
Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Interventions
2.3. Study Outcomes
2.4. Variables and Statistical Analysis
3. Results
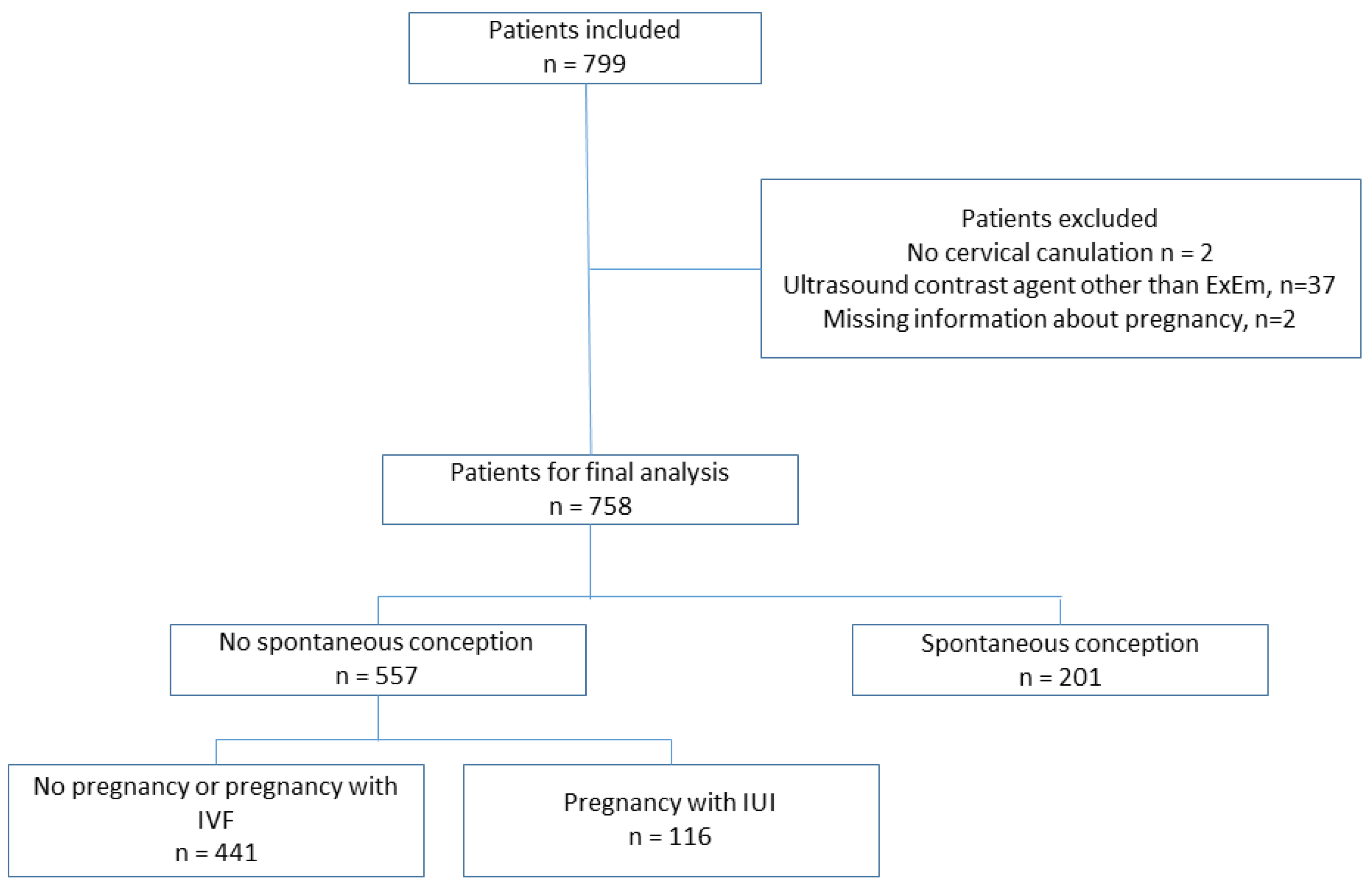
3.1. General Data
3.2. Patients’ Characteristics and Fertility Parameters
3.3. Characteristics Related to HyFoSy Procedure and Findings
3.4. Multivariable Analysis for SC after HyFoSy Examination
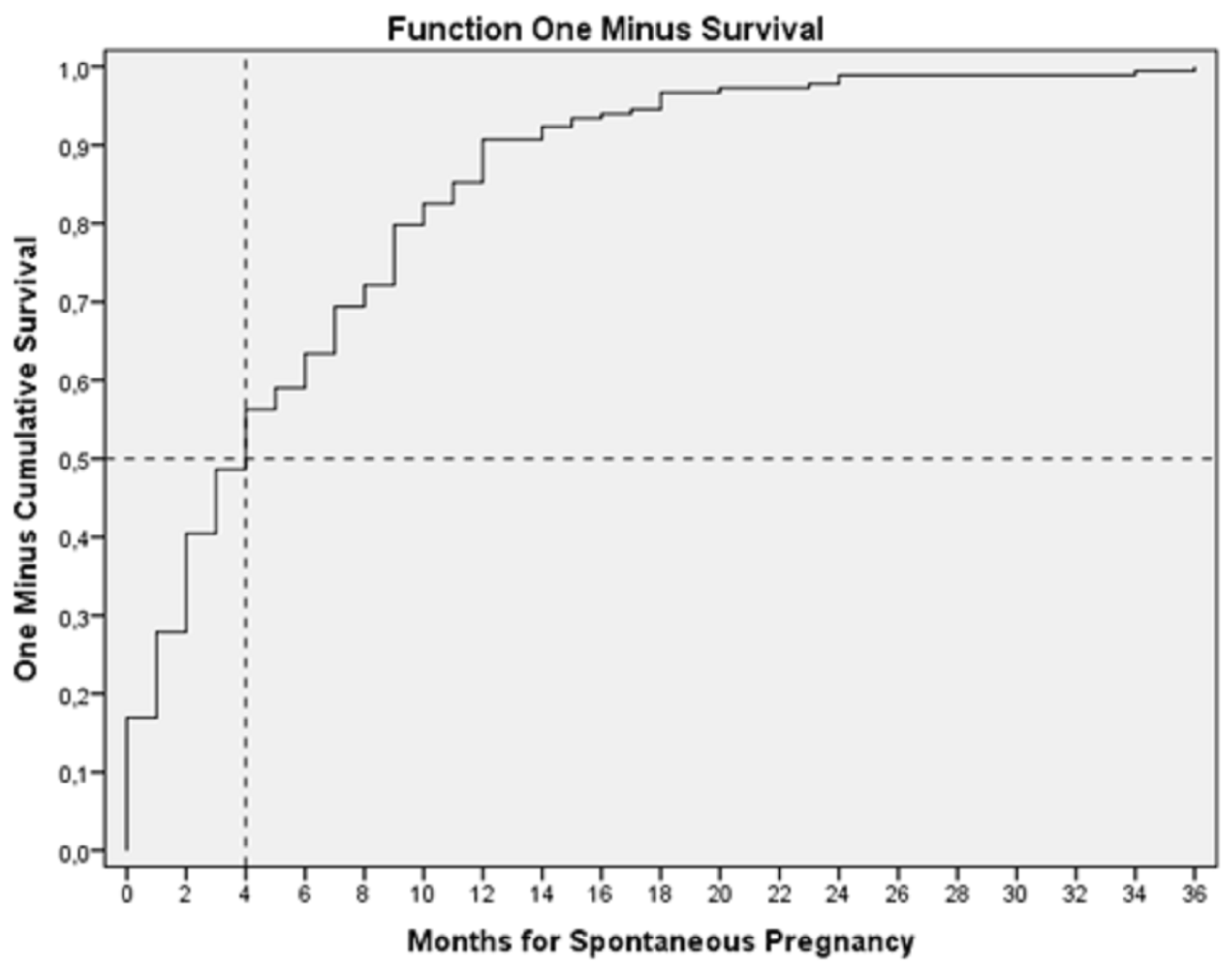
3.5. Perinatal Outcomes of SC after the Procedure
4. Discussion
4.1. Summary of Findings
4.2. Interpretation of Results
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [CrossRef]
- Vander, B.M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.A.; Kallen, A.N. Diagnosis and Management of Infertility: A Review. JAMA 2021, 326, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.D.; Shwayder, J.M.; Nakajima, S.T. Current methods of tubal patency assessment. Fertil. Steril. 2011, 95, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Hamed, H.O.; Shahin, A.Y.; Elsamman, A.M. Hysterosalpingo-contrast sonography versus radiographic hysterosalpingography in the evaluation of tubal patency. Int. J. Gynaecol. Obstet. 2009, 105, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Exalto, N.; Emanuel, M.H. Clinical Aspects of HyFoSy as Tubal Patency Test in Subfertility Workup. Biomed. Res. Int. 2019, 2019, 4827376. [Google Scholar] [CrossRef] [Green Version]
- Vitale, S.G.; Carugno, J.; Riemma, G.; Török, P.; Cianci, S.; De Franciscis, P.; Parry, J.P. Hysteroscopy for Assessing Fallopian Tubal Obstruction: A Systematic Review and Diagnostic Test Accuracy Meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 769–778. [Google Scholar] [CrossRef]
- Ludwin, I.; Ludwin, A.; Nastri, C.O.; Neto, M.A.C.; Kottner, J.; Martins, W.P. Inter-Rater Reliability of Air/Saline HyCoSy, HyFoSy and HyFoSy Combined With Power Doppler for Screening Tubal Patency. Ultraschall Med. 2019, 40, 47–54. [Google Scholar] [CrossRef]
- Lim, S.L.; Jung, J.J.; Yu, S.L.; Rajesh, H. A comparison of hysterosalpingo-foam sonography [HyFoSy] and hysterosalpingo-contrast sonography with saline medium [HyCoSy] in the assessment of tubal patency. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 168–172. [Google Scholar] [CrossRef]
- Exacoustos, C.; Di Giovanni, A.; Szabolcs, B.; Romeo, V.; Romanini, M.E.; Luciano, D.; Zupi, E.; Arduini, D. Automated three-dimensional coded contrast imaging hysterosalpingo-contrast sonography: Feasibility in office tubal patency testing. Ultrasound Obstet. Gynecol. 2013, 41, 328–335. [Google Scholar] [CrossRef]
- Engels, V.; Medina, M.; Antolín, E.; Ros, C.; Amaro, A.; De-Guirior, C.; Manzour, N.; Sotillo, L.; De la Cuesta, R.; Rodríguez, R.; et al. Feasibility, tolerability, and safety of hysterosalpingo-foam sonography (HyFoSy) multicenter, prospective Spanish study. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102004. [Google Scholar] [CrossRef] [PubMed]
- Crosignani, P.G.; Rubin, B.L. Optimal use of infertility diagnostic tests and treatments. The ESHRE Capri Workshop Group. Hum. Reprod. 2000, 15, 723–732. [Google Scholar] [PubMed]
- Dreyer, K.; van Eekelen, R.; Tjon-Kon-Fat, R.I.; van der Steeg, J.W.; Steures, P.; Eijkemans, M.; van der Veen, F.; Hompes, P.; Mol, B.; van Geloven, N. The therapeutic effect of hysterosalpingography in couples with unexplained subfertility: A post-hoc analysis of a prospective multi-centre cohort study. Reprod. Biomed. Online 2019, 38, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Chua, J.; Cincotta, R.; Ballard, E.L.; Duncombe, G. Hysterosalpingo-foam sonography [HyFoSy]: Tolerability, safety and the occurrence of pregnancy post-procedure. Aust. N. Z. J. Obstet. Gynaecol. 2018, 58, 114–118. [Google Scholar] [CrossRef]
- Lindborg, L.; Thorburn, J.; Bergh, C.; Strandell, A. Influence of HyCoSy on spontaneous pregnancy: A randomized controlled trial. Hum. Reprod. 2009, 24, 1075–1079. [Google Scholar] [CrossRef] [PubMed]
- Van Schoubroeck, D.; Van den Bosch, T.; Ameye, L.; Boes, A.S.; D’Hooghe, T.; Timmerman, D. Pain during Fallopian-tube patency testing by hysterosalpingo-foam sonography. Ultrasound Obstet. Gynecol. 2015, 45, 346–350. [Google Scholar] [CrossRef] [Green Version]
- Emanuel, M.H.; van Vliet, M.; Weber, M.; Exalto, N. First experiences with hysterosalpingo-foam sonography [HyFoSy] for office tubal patency testing. Hum. Reprod. 2012, 27, 114–117. [Google Scholar] [CrossRef] [Green Version]
- Giugliano, E.; Cagnazzo, E.; Bazzan, E.; Patella, A.; Marci, R. Hysterosalpingo-contrast sonography: Is possible to quantify the therapeutic effect of a diagnostic test? Clin. Exp. Reprod. Med. 2012, 39, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Chunyan, G.; Bin, P.; Ping, Y.; Yue, Z.; Yang, X.; Hongju, T.; Li, S.; Xi, X. Assessment of the Influence on Spontaneous Pregnancy of Hysterosalpingo-Contrast Sonography. Biomed. Res. Int. 2018, 2018, 4901281. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Sharma, R.; Harlev, A.; Esteves, S.C. Effect of varicocele on semen characteristics according to the new 2010 World Health Organization criteria: A systematic review and meta-analysis. Asian J. Androl. 2016, 18, 163–170. [Google Scholar] [CrossRef]
- Holz, K.; Becker, R.; Schürmann, R. Ultrasound in the investigation of tubal patency. A meta-analysis of three comparative studies of Echovist-200 including 1007 women. Zent. Gynakol. 1997, 119, 366–373. [Google Scholar]
- Eijkemans, M.J.; van Poppel, F.; Habbema, D.F.; Smith, K.R.; Leridon, H.; te Velde, E.R. Too old to have children? Lessons from natural fertility populations. Hum. Reprod. 2014, 29, 1304–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascarenhas, M.N.; Flaxman, S.R.; Boerma, T.; Vanderpoel, S.; Stevens, G.A. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012, 9, e1001356. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Wahby, O.; Sobrero, A.J.; Epstein, J.A. Hysterosalpingography in relation to pregnancy and its outcome in infertile women. Fertil. Steril. 1966, 17, 520–530. [Google Scholar] [CrossRef]
- Wang, R.; Watson, A.; Johnson, N.; Cheung, K.; Fitzgerald, C.; Mol, B.W.J.; Mohiyiddeen, L. Tubal flushing for subfertility. Cochrane Database Syst. Rev. 2020, 10, CD003718. [Google Scholar]
- Grigovich, M.; Kacharia, V.S.; Bharwani, N.; Hemingway, A.; Mijatovic, V.; Rodgers, S.K. Evaluating Fallopian Tube Patency: What the Radiologist Needs to Know. Radiographics 2021, 41, 1876–18961. [Google Scholar] [CrossRef] [PubMed]
- Exacoustos, C.; Tiberio, F.; Szabolcs, B.; Romeo, V.; Romanini, E.; Zupi, E. Can Tubal Flushing With Hysterosalpingo-Foam Sonography [HyFoSy] Media Increase Women’s Chances of Pregnancy? J. Minim. Invasive Gynecol. 2015, 22, S238. [Google Scholar] [CrossRef]
- Exalto, N.; Stassen, M.; Emanuel, M.H. Safety aspects and side-effects of Exem-gel and foam for uterine cavity distension and tubal patency testing. Reprod. Biomed. Online 2014, 29, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Aanesen, A.; Westerbotn, M. Prospective study of a Swedish infertile cohort 2005-08: Population characteristics, treatments and pregnancy rates. Fam. Pract. 2014, 31, 290–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schoubroeck, D.; Van den Bosch, T.; Van Tornout, K.; D’Hooghe, T.; Timmerman, D. Spontaneous conception after hysterosalpingo-foam sonography [HyFoSy]. Ultrasound Obstet. Gynecol. 2015, 46 (Suppl. 1), 53. [Google Scholar] [CrossRef]
- Collins, J.A.; Burrows, E.A.; Wilan, A.R. The prognosis for live birth among untreated infertile couples. Fertil. Steril. 1995, 64, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Gleicher, N.; VanderLaan, B.; Pratt, D.; Karande, V. Background pregnancy rates in an infertile population. Hum. Reprod. 1996, 11, 1011–1012. [Google Scholar] [CrossRef]
- Gnoth, C.; Godehardt, D.; Godehardt, E.; Frank-Herrmann, P.; Freundl, G. Time to pregnancy: Results of the German prospective study and impact on the management of infertility. Hum. Reprod. 2003, 18, 1959–1966. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Martinez, A.; Duarte, M.; Welly, A.; Marín, A.; Calle, A.; Garrido, R.; Pascual, M.A.; Guerriero, S. Two-dimensional hysterosalpingo-contrast-sonography compared to three/four-dimensional hysterosalpingo-contrast-sonography for the assessment of tubal occlusion in women with infertility/subfertility: A systematic review with meta-analysis. Hum. Fertil. 2022, 25, 43–55. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total, Patients | No Spontaneous Conception (NSC) | Spontaneous Conception (SC) | p-Value | |
|---|---|---|---|---|---|
| n (%) | 758 | 557 (73.5) | 201 (26.5) | ||
| BMI (median, IQR) | 22.9 (20.6–25.6) | 23.0 (20.0–27.0) | N.S. | ||
| Age, years (median, IQR) | 34 (31–36) | 34 (30–36) | N.S. | ||
| Age < 35 years | 324 (58.2%) | 132 (65.6%) | 0.0754 | ||
| Time of sterility, months (median, IQR) | 18 (12–24) | 18 (12–24) | 0.0034 | ||
| Time of sterility < 18 months | 306 (55.9%) | 139 (69.1%) | 0.0006 | ||
| Sterility etiology | Unexplained * Ovulatory ** Mild or moderate male factor ** Tubal factor ** Others(endocrinology, uterine…) ** Mixed factor ** | 228/652 (35.0) 113/652 (17.3) 114/652 (17.5) 52/652 (8.0) 70/652 (10.7) 75/652 (11.5) | 151/469 (32.2) 94/469 (20.0) 85/469 (18.1) 32/469 (6.8) 46/469 (9.8) 61/469 (13.0) | 77/183 (42.1) 19/183 (10.4) 29/183 (15.8) 20/183 (10.9) 24/183 (13.1) 14/183 (7.7) | * 0.017 ** N.S. |
| Characteristic | Total | No Spontaneous Conception | Spontaneous Conception | p-Value | |
|---|---|---|---|---|---|
| 758 | 557 (73.5) | 201 (26.5) | |||
| Contrast volume (CC) (median, IQR) | 5.0 (3.0–7.0) | 5.0 (3.0–7.0) | 5.0 (3.0–8.0) | 0.314 | |
| Tubal patency | Both tubes patent One tube patent Bilateral occlusion Not valuable | 576/755 (76.3) 146/755 (19.3) 32/755 (4.2) 1/755 (0.1) | 422/554 (76.2) 108/554 (19.5) 23/554 (4.2) 1/554 (0.2) | 154 (76.6) 38 (18.9) 9 (4.5) 0 (0.0) | 0.934 |
| PAIN (VAS score) | Mild (0–3) Moderate (4–7) Severe ( > 8) | 456/712 (64.0) 227/712 (31.9) 29/712 (4.1) | 331/521 (63.5) 169/521 (32.4) 21/521 (4.0) | 125/191 (65.4) 58/191 (30.4) 8/191 (4.2) | 0.871 |
| Initial Maximal Model | Final Estimation Model | Variables Conserved in the Model | p-Value | OR (95% CI) |
|---|---|---|---|---|
| Spontaneous pregnancy = interaction (cause of sterility + age categorized) + time of sterility categorized | Spontaneous pregnancy = interaction (cause of sterility + age categorized) + time of sterility categorized | Time of sterility categorized | <0.001 | 1.93 (1.34–2.81) |
| Age categorized | 0.216 | |||
| Unknown sterility | 0.830 | |||
| Unknown sterility in women aged under 35 years | 0.033 | 2.22 (1.07–4.65) |
| Characteristics | Total, Patients | HyFoSy + IUI | HyFoSy | p-Value | |
|---|---|---|---|---|---|
| Pregnancy | Term delivery Preterm delivery miscarriage | 220/267 (82.4) 20/267 (7.5) 27/267 (10.1) | 76/92 (82.6) 10/92 (10.9) 6/92 (6.5) | 144/175 (82.3) 10/175 (5.7) 21/175 (12.0) | 0.140 |
| Evolution of pregnancy | Ongoing pregnancy miscarriage | 240/267 (89.9) 27/267 (10.1) | 86/92 (93.5) 6/92 (6.5) | 154/175 (88.0) 21/175 (12.0) | 0.158 |
| Neonatal weight, grams (median, IQR) | 3176 (2850–3430) | 2998 (2656–3485) | 3205 (3016–3395) | 0.034 * | |
| Fetal malformations | Yes No | 12/192 (6.2) 180/192 (93.8) | 7/73 (9.6) 66/73 (93.8) | 5/119 (4.2) 114/119 (95.8) | 0.217 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engels, V.; Medina, M.; Antolín, E.; Ros, C.; Bermejo, C.; Manzour, N.; Pelayo, I.; Amaro, A.; Martinez-Ten, P.; De-Guirior, C.; et al. Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study. Diagnostics 2023, 13, 504. https://doi.org/10.3390/diagnostics13030504
Engels V, Medina M, Antolín E, Ros C, Bermejo C, Manzour N, Pelayo I, Amaro A, Martinez-Ten P, De-Guirior C, et al. Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study. Diagnostics. 2023; 13(3):504. https://doi.org/10.3390/diagnostics13030504
Chicago/Turabian StyleEngels, Virginia, Margarita Medina, Eugenia Antolín, Cristina Ros, Carmina Bermejo, Nabil Manzour, Irene Pelayo, Ainara Amaro, Pilar Martinez-Ten, Cristian De-Guirior, and et al. 2023. "Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study" Diagnostics 13, no. 3: 504. https://doi.org/10.3390/diagnostics13030504
APA StyleEngels, V., Medina, M., Antolín, E., Ros, C., Bermejo, C., Manzour, N., Pelayo, I., Amaro, A., Martinez-Ten, P., De-Guirior, C., Rodríguez, R., Sotillo, L., Brotons, I., de la Cuesta-Benjumea, R., Martinez, O., Sancho, J., & Alcázar, J. L. (2023). Factors Associated with a Post-Procedure Spontaneous Pregnancy after a Hysterosapingo-Foam-Sonography (HyFoSy): Results from a Multicenter Observational Study. Diagnostics, 13(3), 504. https://doi.org/10.3390/diagnostics13030504