
Psychological Outcomes on Anxiety and Depression after Interventions for Temporomandibular Disorders: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Summary of Eligible Criteria
2.3. Search Strategy
2.4. Data Management
2.5. Assessment of Risk of Bias and Quality Evaluation
2.6. Data Analysis
2.7. Meta-Analyses including Only Studies with Control Groups
2.8. Assessment of Heterogeneity
2.9. Narrative Analysis including All Studies
3. Results
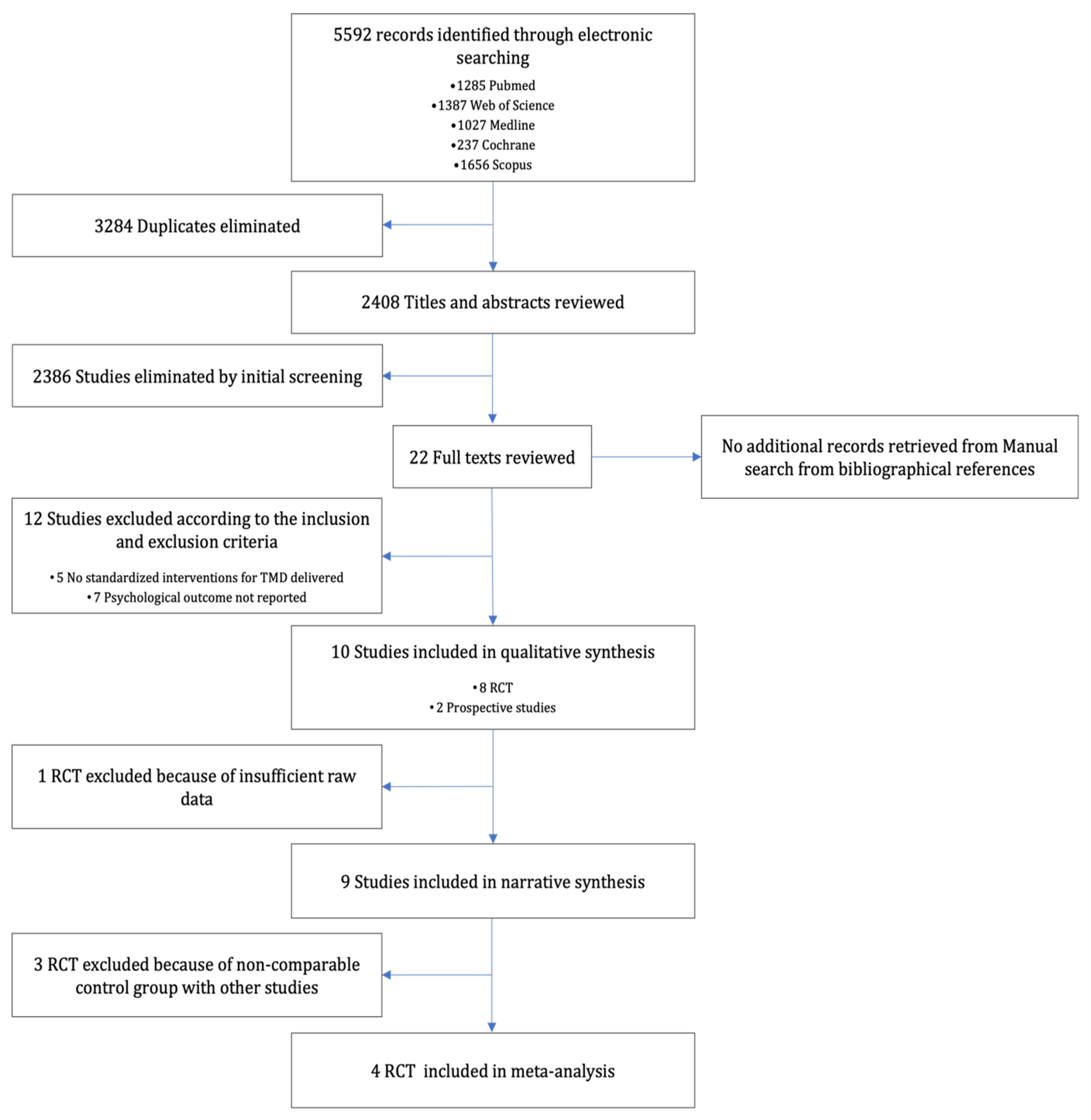
3.1. Literature Search
3.2. Study Characteristics
3.3. Quality of Studies
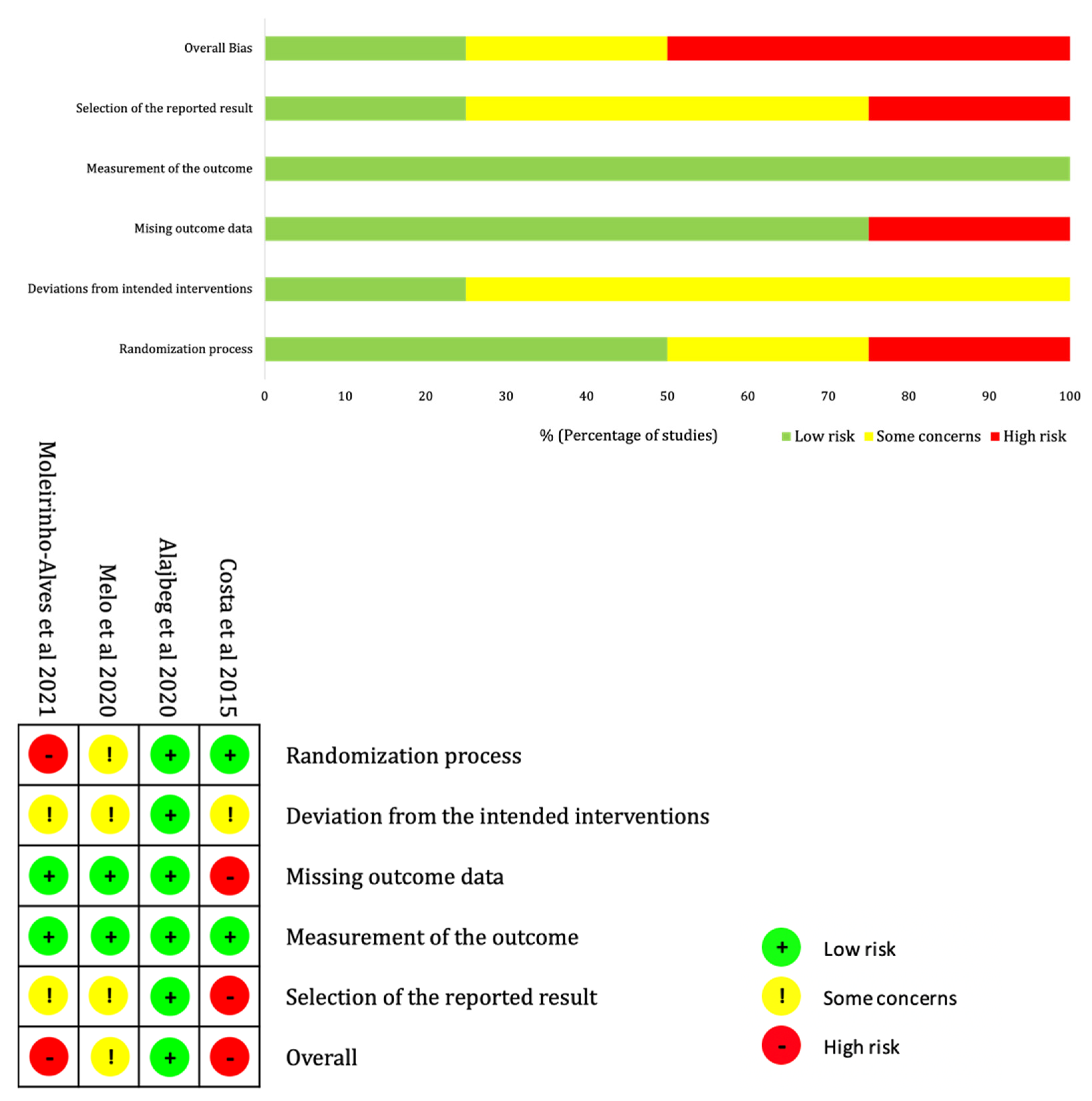
3.4. Risk of Bias in Studies Included in the Meta-Analysis
3.5. Narrative Analysis
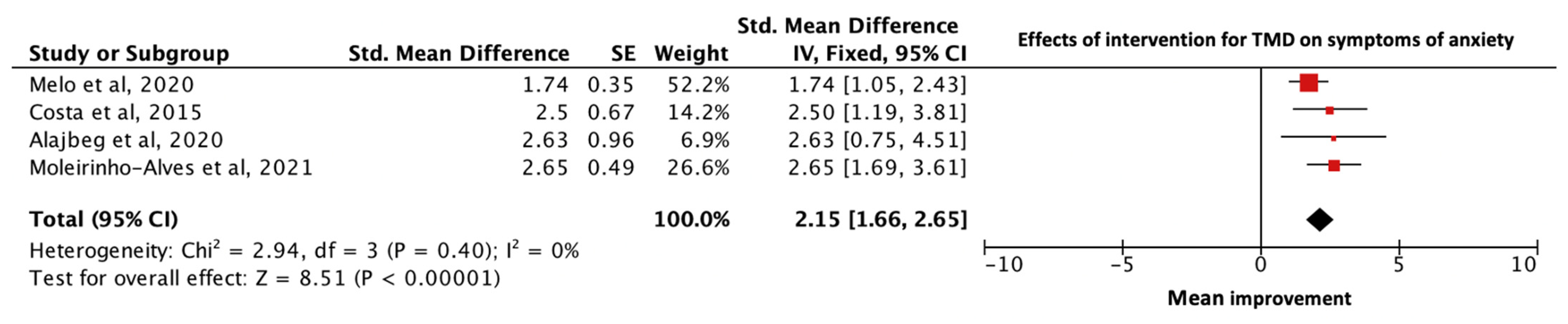
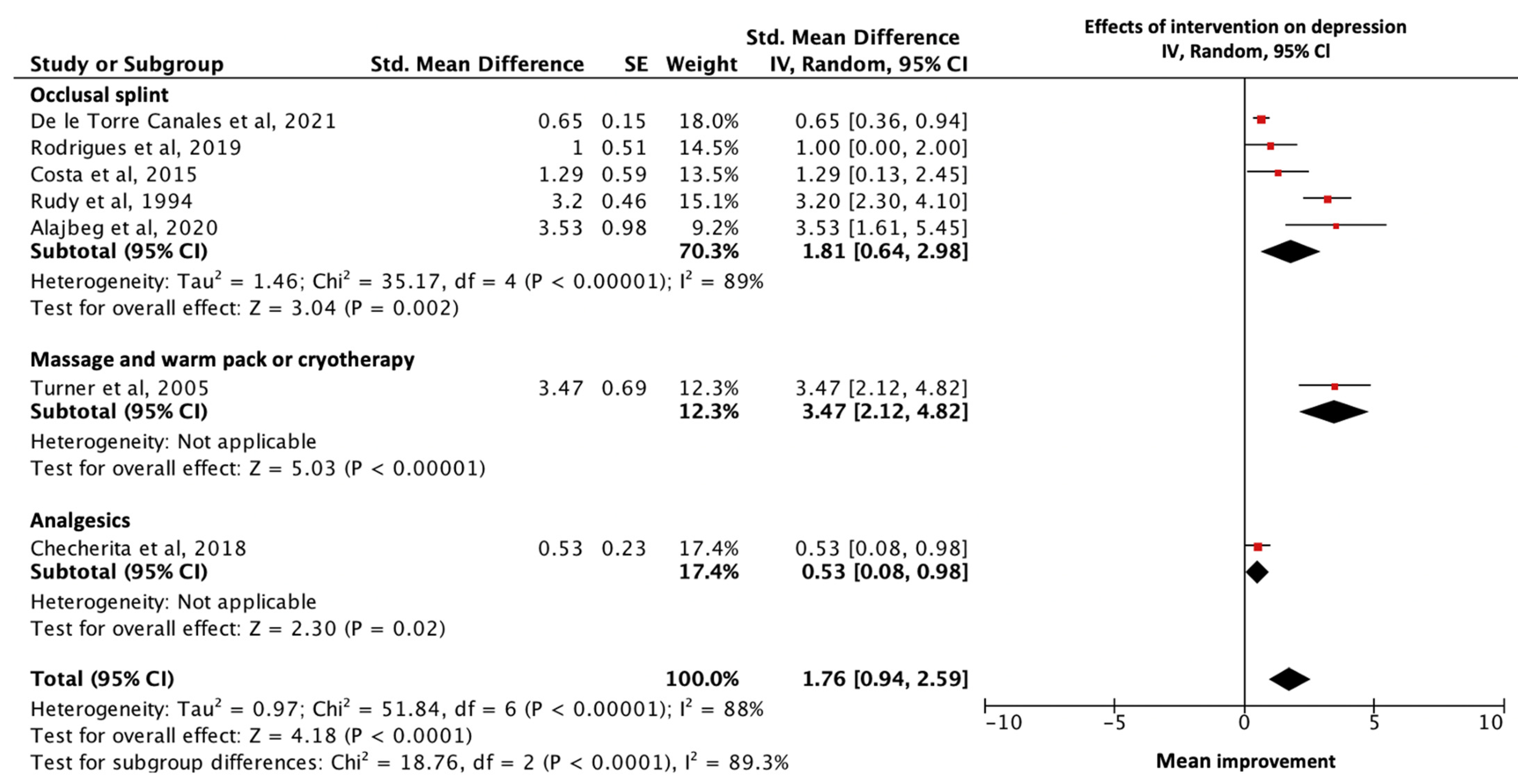
3.6. Meta-Analysis
4. Discussion
4.1. Summary of the Findings
4.2. Role of Interventions for TMD in Improving Anxiety and Depression
4.3. Statistical Significance Not Found in Treatment Effect When Compared to Control Group
4.4. Implication for Clinical Practice
4.5. Implication for Future Research
4.6. Strengths and Limitations of This Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Representativeness of the sample.
- (a)
- Truly representative of the average in patients with TMD (Random sampling/population based sampling)*.
- (b)
- Somewhat representative of the average in patients with TMD (non-random sampling)*.
- (c)
- Selected group of patients, e.g., volunteer, students, hospital staffs, restricted by gender, etc.
- (d)
- No description of the sampling strategy.
- Sample size.
- (a)
- Justified and satisfactory, that is, to have a clear description of algorithm, the required sample size is derived*.
- (b)
- Not justified.
- Ascertainment of intervention.
- (a)
- Protocol of intervention is clearly described. Attempts are made to ensure the intervention is accurately carried out*.
- (b)
- Protocol of intervention is somewhat described, but no confirmation of whether the intervention is accurately carried out.
- (c)
- No description of intervention or no attempt to ascertain information on how accurate the intervention is carried out.
- (a)
- Presence of a control or comparable group, e.g., placebo, no treatment, or other non-standardised interventions for TMD*.
- Assessment of outcome
- (a)
- Independent blind assessment*
- (b)
- Record linkage*
- (c)
- Self-report*
- (d)
- No description
- Was follow-up long enough for outcomes to occur
- (a)
- Yes (length of intervention and follow-up was at least 6 months)*
- (b)
- No
- Adequacy of follow-up
- (a)
- Complete follow up—all subjects accounted for*
- (b)
- Number of subjects lost to follow-up is more and unlikely to introduce bias (<20%), or description of those lost is clearly reported*
- (c)
- >20% of subjects lost to follow-up and no description of those lost
References
- Cascone, P.; Gennaro, P.; Gabriele, G.; Chisci, G.; Mitro, V.; De Caris, F.; Iannetti, G. Temporomandibular synovial chondromatosis with numerous nodules. J. Craniofac. Surg. 2014, 25, 1114–1115. [Google Scholar] [CrossRef] [PubMed]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Li, D.T.S.; Leung, Y.Y. Temporomandibular Disorders: Current Concepts and Controversies in Diagnosis and Management. Diagnostics 2021, 11, 459. [Google Scholar] [CrossRef] [PubMed]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.K.; Ma, X.C.; Gao, S.; Gu, Z.Y.; Fu, K.Y. Studies on contributing factors in temporomandibular disorders. Chin. J. Dent. Res. 1999, 2, 7–20. [Google Scholar]
- Global Health Data Exchange. Institute of Health Metrics and Evaluation 2019. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 8 June 2022).
- Florjański, W.; Orzeszek, S. Role of mental state in temporomandibular disorders: A review of the literature. Dent. Med. Probl. 2021, 58, 127–133. [Google Scholar] [CrossRef]
- World Health Organization. Mental Disorders. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed on 12 June 2022).
- De La Torre Canales, G.; Câmara-Souza, M.B.; Muñoz Lora, V.R.M.; Guarda-Nardini, L.; Conti, P.C.R.; Rodrigues Garcia, R.M.; Del Bel Cury, A.A.; Manfredini, D. Prevalence of psychosocial impairment in temporomandibular disorder patients: A systematic review. J. Oral Rehabil. 2018, 45, 881–889. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Reade, P.C.; Kemppainen, P.; Könönen, M.; Dworkin, S.F. Review of aetiological concepts of temporomandibular pain disorders: Towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur. J. Pain 2005, 9, 613–633. [Google Scholar] [CrossRef]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.; Oleszek-Listopad, J.; Marczak, M.; Szymanska, J. Psychological aspects of temporomandibular disorders–literature review. Curr. Issues Pharm. Med. Sci. 2015, 28, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 8 June 2022).
- Murad, M.; Montori, V.; Ioannidis, J.; Prasad, K.; Cook, D.; Guyatt, G. Fixed-Effects and Random-Effects Models. Users’ Guide to the Medical Literature. A Manual for Evidence-Based Clinical Practice, 3rd ed.; McGraw-Hill: New York, NY, USA, 2015. [Google Scholar]
- Tufanaru, C.; Munn, Z.; Stephenson, M.; Aromataris, E. Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. JBI Evid. Implement. 2015, 13, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Costa, Y.M.; Porporatti, A.L.; Stuginski-Barbosa, J.; Bonjardim, L.R.; Conti, P.C. Additional effect of occlusal splints on the improvement of psychological aspects in temporomandibular disorder subjects: A randomized controlled trial. Arch. Oral Biol. 2015, 60, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Alajbeg, I.Z.; Vrbanović, E.; Lapić, I.; Alajbeg, I.; Vuletić, L. Effect of occlusal splint on oxidative stress markers and psychological aspects of chronic temporomandibular pain: A randomized controlled trial. Sci. Rep. 2020, 10, 10981. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Melo, R.A.; de Resende, C.; Rêgo, C.R.F.; Bispo, A.S.L.; Barbosa, G.A.S.; de Almeida, E.O. Conservative therapies to treat pain and anxiety associated with temporomandibular disorders: A randomized clinical trial. Int. Dent. J. 2020, 70, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis forthe Behavioural Sciences; Baskı: Hillsdale, NJ, USA, 1988. [Google Scholar]
- GRADE Handbook. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 12 June 2022).
- Badel, T.; Keros, J.; Marotti, M.; Kern, J.; Kocijan, S. Therapy of displaced disk of the temporomandibular joint in relation to anxiety. Period. Biol. 2008, 110, 101–105. [Google Scholar]
- Bouloux, G.F.; Zerweck, A.G.; Celano, M.; Dai, T.; Easley, K.A. Can Preoperative Psychological Assessment Predict Outcomes After Temporomandibular Joint Arthroscopy? J. Oral Maxillofac. Surg. 2015, 73, 2094–2102. [Google Scholar] [CrossRef]
- Huttunen, J.; Qvintus, V.; Suominen, A.L.; Sipilä, K. Role of psychosocial factors on treatment outcome of temporomandibular disorders. Acta Odontol. Scand. 2019, 77, 119–125. [Google Scholar] [CrossRef]
- Krogstad, B.S.; Jokstad, A.; Dahl, B.L.; Soboleva, U. Somatic complaints, psychologic distress, and treatment outcome in two groups of TMD patients, one previously subjected to whiplash injury. J. Orofac. Pain 1998, 12, 136–144. [Google Scholar] [PubMed]
- Manfredini, D.; Favero, L.; Del Giudice, A.; Masiero, S.; Stellini, E.; Guarda-Nardini, L. Axis II psychosocial findings predict effectiveness of TMJ hyaluronic acid injections. Int. J. Oral Maxillofac. Surg. 2013, 42, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, H.; Ekberg, E. Do psychological factors and general health influence the short-term efficacy of resilient appliance therapy in patients with temporomandibular disorder pain? Acta Odontol. Scand. 2010, 68, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Plaza-Manzano, G.; Delgado-de-la-Serna, P.; Díaz-Arribas, M.J.; Rodrigues-de-Souza, D.P.; Fernández-de-Las-Peñas, C.; Alburquerque-Sendín, F. Influence of Clinical, Physical, Psychological, and Psychophysical Variables on Treatment Outcomes in Somatic Tinnitus Associated with Temporomandibular Pain: Evidence From a Randomized Clinical Trial. Pain Pract. 2021, 21, 8–17. [Google Scholar] [CrossRef]
- Abrahamsen, R.; Zachariae, R.; Svensson, P. Effect of hypnosis on oral function and psychological factors in temporomandibular disorders patients. J. Oral Rehabil. 2009, 36, 556–570. [Google Scholar] [CrossRef]
- Fernandes, M.P.; Vidal, C.L.; de Oliveira, T.T.; Botelho, A.L.; Valente, M.; Dos Reis, A.C. Effects of photobiomodulation on auriculotherapy points for sleep disorders, anxiety, and temporomandibular dysfunctions. Cranio 2020, 1–6. [Google Scholar] [CrossRef]
- Iunes, D.H.; Chaves Éde, C.; Moura Cde, C.; Côrrea, B.; Carvalho, L.C.; Silva, A.M.; de Carvalho, E.C. Role of Auriculotherapy in the Treatment of Temporomandibular Disorders with Anxiety in University Students. Evid. Based Complement. Alternat. Med. 2015, 2015, 430143. [Google Scholar] [CrossRef]
- Ivkovic, N.; Mladenovic, I.; Petkoci, S.; Stojic, D. TMD chronic pain and masseter silent period in psychiatric patients on antidepressive therapy. J. Oral Rehabil. 2008, 35, 424–432. [Google Scholar] [CrossRef]
- Rodrigues, J.H.; Marques, M.M.; Biasotto-Gonzalez, D.A.; Moreira, M.S.; Bussadori, S.K.; Mesquita-Ferrari, R.A.; Martins, M.D. Evaluation of pain, jaw movements, and psychosocial factors in elderly individuals with temporomandibular disorder under laser phototherapy. Lasers Med. Sci. 2015, 30, 953–959. [Google Scholar] [CrossRef]
- Brandão, R.; Mendes, C.M.C.; Brandão Filho, R.A.; De Sena, E.P. Isotonic exercises and relaxing techniques in individuals with temporomandibular dysfunction. Cranio 2022, 40, 199–206. [Google Scholar] [CrossRef]
- Turner, J.A.; Mancl, L.; Aaron, L.A. Short- and long-term efficacy of brief cognitive-behavioral therapy for patients with chronic temporomandibular disorder pain: A randomized, controlled trial. Pain 2006, 121, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.D.F.; Rodrigues, M.L.; Bueno, K.S.; Aroca, J.P.; Camilotti, V.; Busato, M.C.A.; Mendonça, M.J. Effects of low-power laser auriculotherapy on the physical and emotional aspects in patients with temporomandibular disorders: A blind, randomized, controlled clinical trial. Complement. Ther. Med. 2019, 42, 340–346. [Google Scholar] [CrossRef] [PubMed]
- De la Torre Canales, G.; Poluha, R.L.; Alvarez Pinzón, Y.N.; Rodrigues Conti, P.C.; Manfredini, D.; Sánchez-Ayala, A.; Rizzatti-Barbosa, C.M. Effects of Botulinum Toxin Type A on the Psychosocial Features of Myofascial Pain TMD Subjects: A Randomized Controlled Trial. J. Oral Facial Pain Headache 2021, 35, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Checherita, L.E.; Burlea, L.S.; Stamatin, O.; Manuc, D. Impact of Ibruprofen Medication and Prosthetic Esthetical Treatment in Elderly Patients with Temporal Mandibular Joint Disorders and Deppresion. Rev. De Chim. 2018, 69, 831–836. [Google Scholar] [CrossRef]
- Moleirinho-Alves, P.M.M.; Almeida, A.; Exposto, F.G.; Oliveira, R.; Pezarat-Correia, P.L.C. Effects of therapeutic exercise and aerobic exercise programmes on pain, anxiety and oral health-related quality of life in patients with temporomandibular disorders. J. Oral Rehabil. 2021, 48, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Rudy, T.E.; Turk, D.C.; Kubinski, J.A.; Zaki, H.S. Differential treatment responses of TMD patients as a function of psychological characteristics. Pain 1995, 61, 103–112. [Google Scholar] [CrossRef]
- Arola, H.M.; Nicholls, E.; Mallen, C.; Thomas, E. Self-reported pain interference and symptoms of anxiety and depression in community-dwelling older adults: Can a temporal relationship be determined? Eur. J. Pain 2010, 14, 966–971. [Google Scholar] [CrossRef] [PubMed]
- Kindler, S.; Samietz, S.; Houshmand, M.; Grabe, H.J.; Bernhardt, O.; Biffar, R.; Kocher, T.; Meyer, G.; Völzke, H.; Metelmann, H.R.; et al. Depressive and anxiety symptoms as risk factors for temporomandibular joint pain: A prospective cohort study in the general population. J. Pain 2012, 13, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Bradburn, M.J.; Deeks, J.J.; Berlin, J.A.; Russell Localio, A. Much ado about nothing: A comparison of the performance of meta-analytical methods with rare events. Stat. Med. 2007, 26, 53–77. [Google Scholar] [CrossRef]
- Themessl-Huber, M. Weak evidence supports the use of psychosocial interventions for chronic orofacial pain. Evid. Based Dent. 2012, 13, 58. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database Searched | Search Terms | Articles Retrieved |
|---|---|---|
| Pubmed | (“Temporomandibular Joint Disorders” or “Temporomandibular joint disorder” or “TMJ Disorders” or “TMJ Disorder” or “Temporomandibular Disorders” or “Temporomandibular Disorder” or “Temporomandibular Joint Diseases” or “Temporomandibular Joint Disease” or “TMJ Diseases” or “TMJ Disease” or “Temporomandibular joint dysfunction syndrome” or “Temporomandibular joint pain” or “Temporomandibular pain” or “TMD” or “Craniomandibular Disorders” or “Craniomandibular Disorder” or “Orofacial Pain” or “Craniofacial pain”) AND (“Depression” or “depressive disorders” or “depression symptoms” or “anxiety” or “mood disorders” or “psychological distress”) | 1285 |
| Web of Science | (“Temporomandibular Joint Disorders” or “Temporomandibular joint disorder” or “TMJ Disorders” or “TMJ Disorder” or “Temporomandibular Disorders” or “Temporomandibular Disorder” or “Temporomandibular Joint Diseases” or “Temporomandibular Joint Disease” or “TMJ Diseases” or “TMJ Disease” or “Temporomandibular joint dysfunction syndrome” or “Temporomandibular joint pain” or “Temporomandibular pain” or “TMD” or “Craniomandibular Disorders” or “Craniomandibular Disorder” or “Orofacial Pain” or “Craniofacial pain”) AND (“Depression” or “depressive disorders” or “depression symptoms” or “anxiety” or “mood disorders” or “psychological distress”) | 1387 |
| Medline | (Temporomandibular Joint Disorders or Temporomandibular joint disorder or TMJ Disorders or TMJ Disorder or Temporomandibular Disorders or Temporomandibular Disorder or Temporomandibular Joint Diseases or Temporomandibular Joint Disease or TMJ Diseases or TMJ Disease or Temporomandibular joint dysfunction syndrome or Temporomandibular joint pain or Temporomandibular pain or TMD or Craniomandibular Disorders or Craniomandibular Disorder or Orofacial Pain or Craniofacial pain) and (Depression or depressive disorders or depression symptoms or anxiety or mood disorders or psychological distress) | 1027 |
| Cochrane | (“Temporomandibular Joint Disorders” or “Temporomandibular joint disorder” or “TMJ Disorders” or “TMJ Disorder” or “Temporomandibular Disorders” or “Temporomandibular Disorder” or “Temporomandibular Joint Diseases” or “Temporomandibular Joint Disease” or “TMJ Diseases” or “TMJ Disease” or “Temporomandibular joint dysfunction syndrome” or “Temporomandibular joint pain” or “Temporomandibular pain” or “TMD” or “Craniomandibular Disorders” or “Craniomandibular Disorder” or “Orofacial Pain” or “Craniofacial pain”) AND (“Depression” or “depressive disorders” or “depression symptoms” or “anxiety” or “mood disorders” or “psychological distress”) | 237 |
| Scopus | (“Temporomandibular Joint Disorders” OR “Temporomandibular joint disorder” OR “TMJ Disorders” OR “TMJ Disorder” OR “Temporomandibular Disorders” OR “Temporomandibular Disorder” OR “Temporomandibular Joint Diseases” OR “Temporomandibular Joint Disease” OR “TMJ Diseases” OR “TMJ Disease” OR “Temporomandibular joint dysfunction syndrome” OR “Temporomandibular joint pain” OR “Temporomandibular pain” OR “TMD” OR “Craniomandibular Disorders” OR “Craniomandibular Disorder” OR “Orofacial Pain” OR “Craniofacial pain”) AND (“depression” OR “depressive disorders” OR “depression symptoms” OR “anxiety” OR “mood disorders” OR “psychological distress”) | 1656 |
| Study | Country | Characteristics of Subjects
| Intervention Groups
| Duration of Follow-Up | Diagnostics Tool of TMD | Outcome Measures of Anxiety or/and Depression | Results | |
|---|---|---|---|---|---|---|---|---|
| Experimental | Control | |||||||
| Brandão et al., 2022 [37] | Brazil |
|
|
|
| RDC/TMD | Depression: RDC/TMD Axis II |
|
| De la Torre Canales et al., 2021 [40] | Brazil |
|
|
|
| RDC/TMD | Depression: SCL-90R |
|
| Moleirinho-Alves et al., 2021 [42] | Portugal |
|
|
|
| DC/TMD | Anxiety: GAD-7 |
|
| Alajbeg et al., 2020 [20] | Croatia |
|
|
|
| DC/TMD | Anxiety: GAD-7Depression: PHQ-9 |
|
| Melo et al., 2020 [22] | Brazil |
|
|
|
| RDC/TMD | Anxiety: HADS, BAI |
|
| Rodrigues et al., 2019 [39] | Brazil |
|
|
|
| RDC/TMD | Depression: SCL-90 |
|
| Checherita et al., 2018 [41] | Romania |
|
|
|
| RDC/TMD | Depression: GDS |
|
| Costa et al., 2015 [19] | Brazil |
|
|
|
| RDC/TMD | Anxiety: HADS, Depression: HADS |
|
| Turner et al., 2006 [38] | USA |
|
|
|
| RDC/TMD | Depression: BD [14] |
|
| Rudy et al., 1995 [43] | USA |
|
|
|
| RDC/TMD | Depression: BDI |
|
| Study | Selection | Comparability | Outcome | Total Score |
|---|---|---|---|---|
| Alajbeg et al., 2020 [20] | *** | * | *** | 7 |
| Melo et al., 2020 [22] | *** | * | ** | 6 |
| Moleirinho-Alves et al., 2021 [42] | *** | * | ** | 6 |
| Costa et al., 2015 [19] | *** | * | * | 5 |
| De la Torre Canales et al., 2021 [40] | ** | * | ** | 5 |
| Rudy et al., 1995 [43] | ** | *** | 5 | |
| Turner et al., 2006 [38] | ** | * | ** | 5 |
| Brandão et al., 2022 [37] | * | * | ** | 4 |
| Rodrigues et al., 2019 [39] | ** | * | * | 4 |
| Checherita et al., 2018 [41] | ** | 2 |
| Number of Studies | Included Studies | Number of Participants (Intervention) | SMD (95% Cl) | p Value | Heterogeneity I2; χ2; P | |
|---|---|---|---|---|---|---|
| Intervention effects | ||||||
| Anxiety | 4 | [19,20,22,42] | 139 | 2.15 (1.66–2.65) | <0.00001 | 0%; 2.94; 0.40 |
| Depression | 7 | [19,20,38,39,40,41,43] | 451 | 1.76 (0.94–2.59) | <0.0001 | 88%; 51.84; <0.00001 |
| Sensitivity analysis (Depression) | ||||||
| Assessed by BDI | 2 | [38,43] | 270 | 3.28 (2.53, 4.03) * | <0.00001 | 0%; 0.11; 0.74 |
| Assessed by SCL-90R | 2 | [39,40] | 31 | 0.68 (0.40, 0.96) * | <0.00001 | 0%; 0.43; 0.51 |
| Number of Studies | Included Studies | Number of Participants (Intervention) | Number of Participants (Control) | SMD (95% Cl) | p Value | Heterogeneity I2; χ2; P | |
|---|---|---|---|---|---|---|---|
| Intervention effects | |||||||
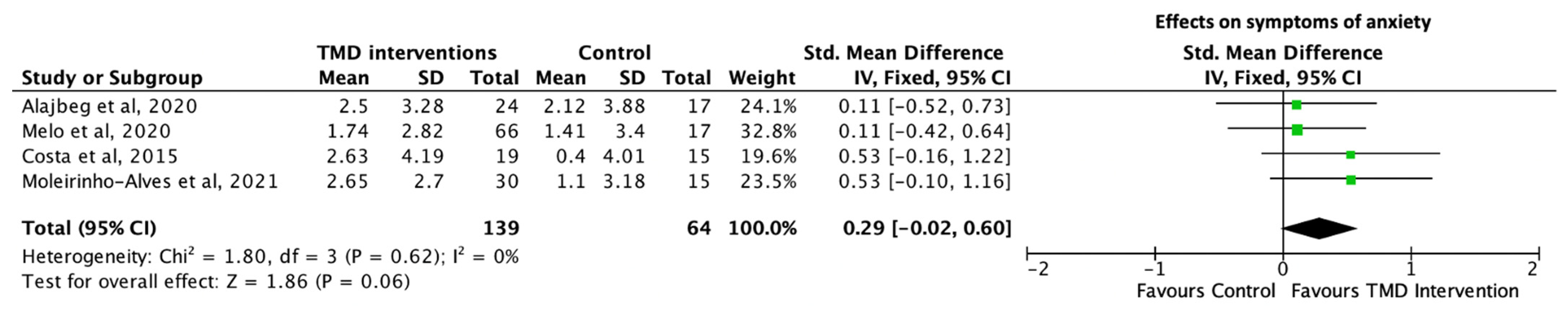
| Anxiety | 4 | [19,20,22,42] | 139 | 64 | 0.29 (0.02–0.6) | 0.06 | 0%; 1.80; 0.62 |
| Depression | 2 | [19,20] | 43 | 32 | 0.40 (−0.06–0.87) | 0.09 | 0%; 0.22; 0.64 |
| Sensitivity analysis (Anxiety) | |||||||
| Higher-quality studies | 2 | [20,22] | 90 | 34 | 0.11 (−0.3–0.51) | 0.06 | 0%; 0.00; 0.99 |
| Occlusal splints | 3 | [19,20,22] | 109 | 49 | 0.22 (−0.13–0.57) | 0.22 | 0%; 1.06; 0.59 |
| Assessed by GAD−7 | 2 | [20,42] | 54 | 32 | 1.07 (−0.37, 2.52) * | 0.15 | 0%; 0.61; 0.44 |
| Assessed by HADS | 2 | [19,22] | 85 | 32 | 0.87 (−0.61, 2.36) * | 0.25 | 23%; 1.29; 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, L.Y.; Lee, J.; Li, K.Y.; Leung, Y.Y.; Li, D.T.S. Psychological Outcomes on Anxiety and Depression after Interventions for Temporomandibular Disorders: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 653. https://doi.org/10.3390/diagnostics13040653
Luo LY, Lee J, Li KY, Leung YY, Li DTS. Psychological Outcomes on Anxiety and Depression after Interventions for Temporomandibular Disorders: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(4):653. https://doi.org/10.3390/diagnostics13040653
Chicago/Turabian StyleLuo, Lai Ying, Johyun Lee, Kar Yan Li, Yiu Yan Leung, and Dion Tik Shun Li. 2023. "Psychological Outcomes on Anxiety and Depression after Interventions for Temporomandibular Disorders: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 4: 653. https://doi.org/10.3390/diagnostics13040653
APA StyleLuo, L. Y., Lee, J., Li, K. Y., Leung, Y. Y., & Li, D. T. S. (2023). Psychological Outcomes on Anxiety and Depression after Interventions for Temporomandibular Disorders: A Systematic Review and Meta-Analysis. Diagnostics, 13(4), 653. https://doi.org/10.3390/diagnostics13040653