
Lung Ultrasound in the Early Diagnosis and Management of the Mild Form of Meconium Aspiration Syndrome: A Case Report
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Cases Study
4. Discussion
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- American Academy of Pediatrics; American Heart Association. Textbook of Neonatal Resuscitation, 6th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2011. [Google Scholar]
- Parkash, A.; Haider, N.; Khoso, Z.A.; Shaikh, A.S. Frequency, causes and outcome of neonates with respiratory distress admitted to Neonatal Intensive Care Unit, National Institute of Child Health, Karachi. JPMA 2015, 65, 771–775. [Google Scholar]
- Edwards, M.O.; Kotecha, S.J.; Kotecha, S. Respiratory distress of the term newborn infant. Paediatr. Respir. Rev. 2013, 14, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Hermansen, C.L.; Mahajan, A. Newborn respiratory distress. Am. Fam. Physician 2015, 92, 994–1002. [Google Scholar] [PubMed]
- Reuter, S.; Moser, C.; Baack, M. Respiratory distress in the newborn. Pediatr. Rev. 2014, 35, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef]
- Sweet, L.R.; Keech, C.; Klein, N.P.; Marshall, H.S.; Tagbo, B.N.; Quine, D.; Kaur, P.; Tikhonov, I.; Nisar, M.I.; Kochhar, S.; et al. Respiratory distress in the neonate: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine 2017, 35 Pt A, 6506–6517. [Google Scholar]
- Olicker, A.L.; Raffay, T.M.; Ryan, R.M. Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome. Children 2021, 8, 246. [Google Scholar] [CrossRef]
- Martin, R.J.; Fanaroff, A.A.; Walsh, M.C. Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant, 11th ed.; Elsevier: Philadeplhia, PA, USA, 2020. [Google Scholar]
- Fanaroff, A.A.; Fanaroff, J.M.; Klaus, M.H. Klaus & Fanaroff’s Care of the High-Risk Neonate, 6th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2013; p. xiv. 626p. [Google Scholar]
- Vain, N.E.; Szyld, E.G.; Prudent, L.M.; Wiswell, T.E.; Aguilar, A.M.; Vivas, N.I. Oropharyngeal and nasopharyngeal suctioning of meconium- stained neonates before delivery of their shoulders: Multicentre, randomised controlled trial. Lancet 2004, 364, 597–602. [Google Scholar] [CrossRef]
- Airede, K.I. Meconium aspiration syndrome—Unusual features. East Afr. Med. J. 1992, 69, 162–164. [Google Scholar]
- Moore, C.S. Meconium aspiration syndrome. Neonatal Netw. 2000, 19, 41–44. [Google Scholar]
- De Cunto, A.; Paviotti, G.; Demarini, S. Neonatal aspiration: Not just meconium. J. Neonatal Perinat. Med. 2013, 6, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, J.; Karotkin, E.; Suresh, G.; Keszler, M. Assisted Ventilation of the Neonate, Evidence-Based Approach to Newborn Respiratory Care, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Liu, J.; Cao, H.Y.; Wang, H.W.; Kong, X.Y. The role of lung ultrasound in diagnosis of respiratory distress syndrome in newborn infants. Iran. J. Pediatr. 2014, 24, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Y.; Fu, W.; Yang, C.S.; Huang, J.J. Diagnosis of neonatal transient tachypnea and its differentiation from respiratory distress syndrome using lung ultrasound. Medicine 2014, 93, e197. [Google Scholar] [CrossRef] [PubMed]
- Cattarossi, L. Lung ultrasound: Its role in neonatology and pediatrics. Early Hum. Dev. 2013, 89 (Suppl. 1), S17–S19. [Google Scholar] [CrossRef] [PubMed]
- Prontera, G.; Perri, A.; Vento, G.; D’Andrea, V. Use of Wireless Ultrasound Probe in Isolated Infants: A Case Report of Two SARS-CoV-2-Positive Mothers’ Newborns. Neonatology 2022, 119, 129–132. [Google Scholar] [CrossRef]
- Chen, S.W.; Fu, W.; Liu, J.; Wang, Y. Routine application of lung ultrasonography in the neonatal intensive care unit. Medicine 2017, 96, e5826. [Google Scholar] [CrossRef] [PubMed]
- Zong, H.; Huang, Z.; Zhao, J.; Lin, B.; Fu, Y.; Lin, Y.; Huang, P.; Sun, H.; Yang, C. The Value of Lung Ultrasound Score in Neonatology. Front. Pediatr. 2022, 10, 791664. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, C.; Michel, F.; Brévaut-Malaty, V.; Hassid, S.; Nicaise, C.; Puech, B.; Thomachot, L.; Vialet, R.; Tosello, B.; Panuel, M. Thoracic ultrasound accuracy for the investigation of initial neonatal respiratory distress. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2019, 26, 459–465. [Google Scholar] [CrossRef]
- Ibrahim, M.; Omran, A.; AbdAllah, N.B.; Ibrahim, M.; El-Sharkawy, S. Lung ultrasound in early diagnosis of neonatal transient tachypnea and its differentiation from other causes of neonatal respiratory distress. J. Neo-Natal-Perinat. Med. 2018, 11, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Hiles, M.; Culpan, A.M.; Watts, C.; Munyombwe, T.; Wolstenhulme, S. Neonatal respiratory distress syndrome: Chest X-ray or lung ultrasound? A systematic review. Ultrasound 2017, 25, 80–91. [Google Scholar] [CrossRef]
- Rachuri, H.; Oleti, T.P.; Murki, S.; Subramanian, S.; Nethagani, J. Diagnostic Performance of Point of Care Ul-trasonography in Identifying the Etiology of Respiratory Distress in Neonates. Indian J. Pediatr. 2017, 84, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Czarnecki, Ł.M. Assessment of chest X-ray images in newborns with respiratory disorders. Kardiochirurgia Torakochirurgia Pol. = Pol. J. Cardio-Thorac. Surg. 2015, 12, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Piastra, M.; Yousef, N.; Brat, R.; Manzoni, P.; Mokhtari, M.; De Luca, D. Lung ultrasound findings in meconium aspiration syndrome. Early Hum. Dev. 2014, 90 (Suppl. 2), S41–S43. [Google Scholar] [CrossRef]
- Liu, J.; Cao, H.Y.; Fu, W. Lung ultrasonography to diagnose meconium aspiration syndrome of the newborn. J. Int. Med. Res. 2016, 44, 1534–1542. [Google Scholar] [CrossRef] [Green Version]
- Dell’Orto, V.; Centorrino, R.; De Luca, D. Ultrasound-guided lung lavage for life-threatening bronchial obstruction due to meconium plug. J. Clin. Ultrasound 2021, 49, 405–407. [Google Scholar] [CrossRef]
- Monfredini, C.; Cavallin, F.; Villani, P.E.; Paterlini, G.; Allais, B.; Trevisanuto, D. Meconium Aspiration Syndrome: A Narrative Review. Children 2021, 8, 230. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| GA | 39 + 6 | 40 + 2 | 39 + 6 | 39 + 3 | 41 + 0 | 39 + 4 |
| BW(g) | 3590 | 3330 | 2965 | 2840 | 3100 | 3835 |
| Delivery | Vaginal delivery | Vaginal delivery | Vaginal delivery | Vaginal delivery | Cesarean section (CTG type 2) | Vaginal delivery |
| Maternal desease | Gestational diabetes | Gestational diabetes | - | - | - | - |
| Apgar index 1′-5′ | 8–9 | 9–9 | 7–8 | 8–9 | 5–8 | 9–10 |
| Delivery room assistance | - | - | FiO2 0.40 | FiO2 0.35 | CPAP 6 cmH2O, FiO2 0.80 | - |
| NICU respiratory assistance | - | - | CPAP 6 cmH2O | - | - | CPAP 6 cmH2O |
| Hours | - | - | 18 | - | - | 24 |
| FiO2 | 0.27 | 0.25 | 0.28 | 0.30 | 0.30 | 0.40 |
| Hours | 48 | 48 | 24 | 24 | 28 | 24 |
| CO2 (mmHg) | 39 | 51 | 38 | 46 | 41 | 30 |
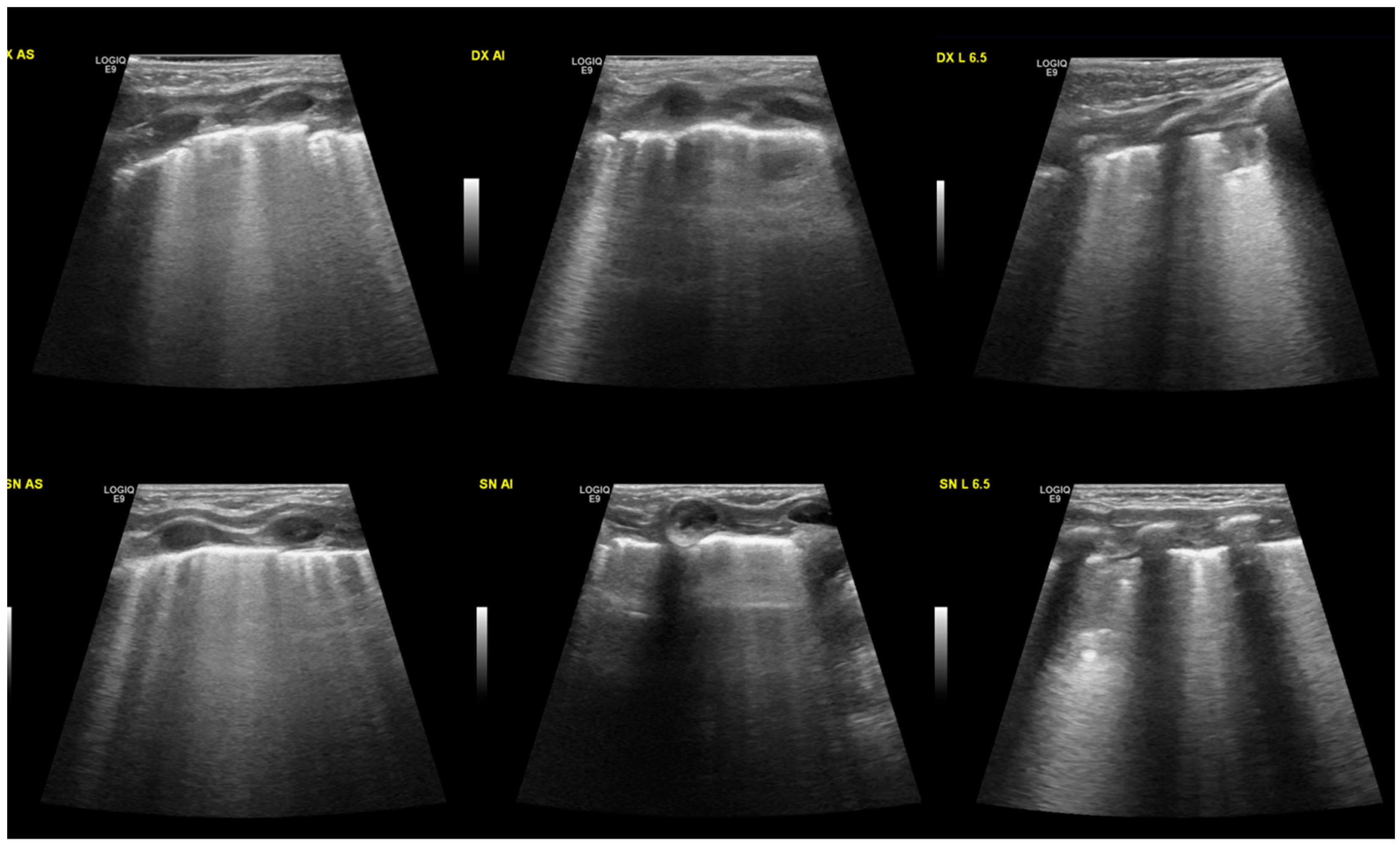
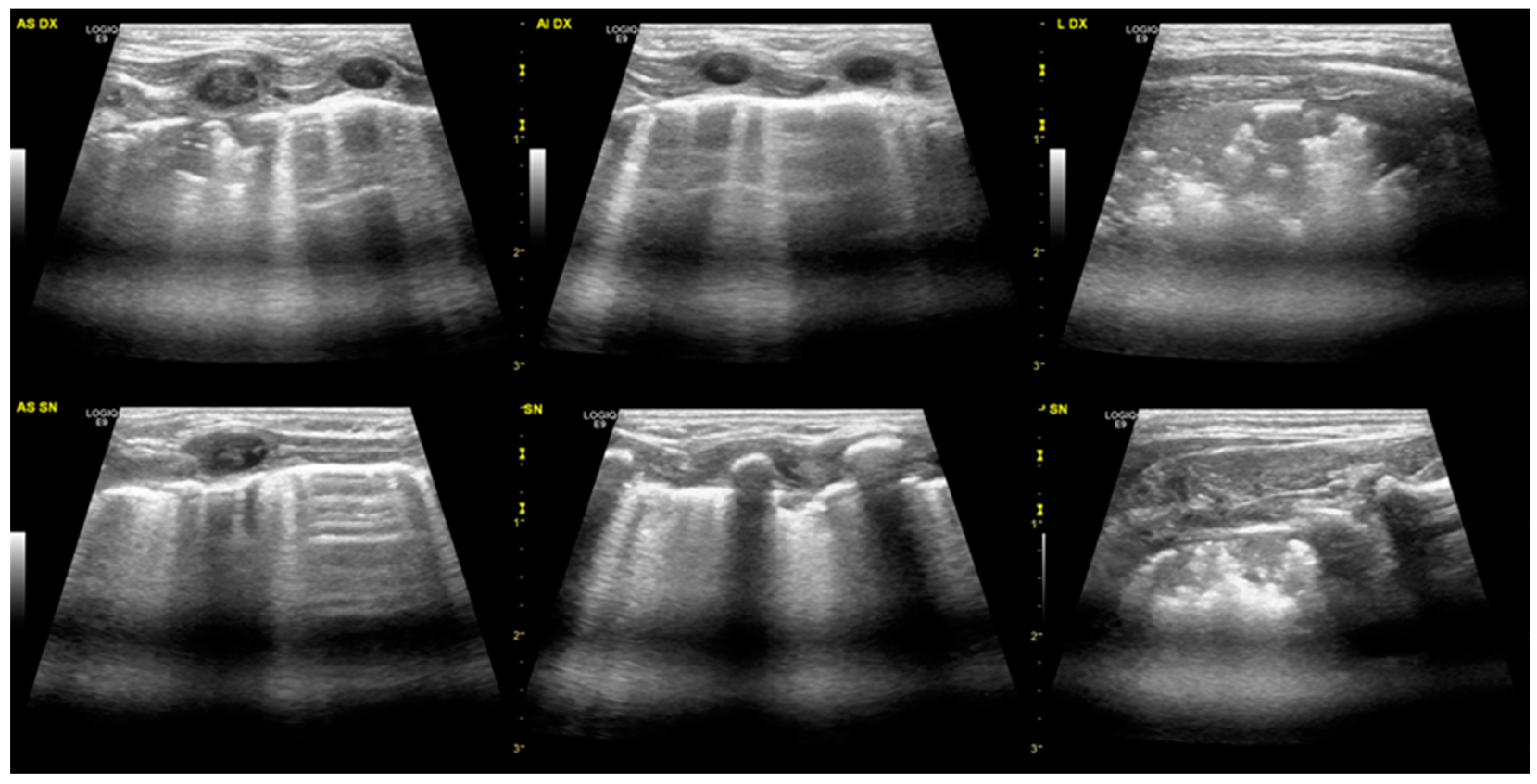
| Lung ultrasound: | ||||||
| Diffuse coalescing B-linee | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Thickening/interruption of pleural line | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Subpleural consolidation | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Largest involvement of the right lung | ✔ | ✗ | ✔ | ✗ | ✔ | ✔ |
| Time of normalisation of lung ultrasound | 3.5 weeks | 2 weeks | 2.5 weeks | 4 weeks | 2 weeks | 4 weeks |
| Chest radiography | diffuse bilateral interstitial involvement | - | diffuse bilateral alveolar-interstitial involvement | - | - | diffuse bilateral interstitial involvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perri, A.; Fattore, S.; Prontera, G.; Patti, M.L.; Sbordone, A.; Tana, M.; D’Andrea, V.; Vento, G. Lung Ultrasound in the Early Diagnosis and Management of the Mild Form of Meconium Aspiration Syndrome: A Case Report. Diagnostics 2023, 13, 719. https://doi.org/10.3390/diagnostics13040719
Perri A, Fattore S, Prontera G, Patti ML, Sbordone A, Tana M, D’Andrea V, Vento G. Lung Ultrasound in the Early Diagnosis and Management of the Mild Form of Meconium Aspiration Syndrome: A Case Report. Diagnostics. 2023; 13(4):719. https://doi.org/10.3390/diagnostics13040719
Chicago/Turabian StylePerri, Alessandro, Simona Fattore, Giorgia Prontera, Maria Letizia Patti, Annamaria Sbordone, Milena Tana, Vito D’Andrea, and Giovanni Vento. 2023. "Lung Ultrasound in the Early Diagnosis and Management of the Mild Form of Meconium Aspiration Syndrome: A Case Report" Diagnostics 13, no. 4: 719. https://doi.org/10.3390/diagnostics13040719
APA StylePerri, A., Fattore, S., Prontera, G., Patti, M. L., Sbordone, A., Tana, M., D’Andrea, V., & Vento, G. (2023). Lung Ultrasound in the Early Diagnosis and Management of the Mild Form of Meconium Aspiration Syndrome: A Case Report. Diagnostics, 13(4), 719. https://doi.org/10.3390/diagnostics13040719