

Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
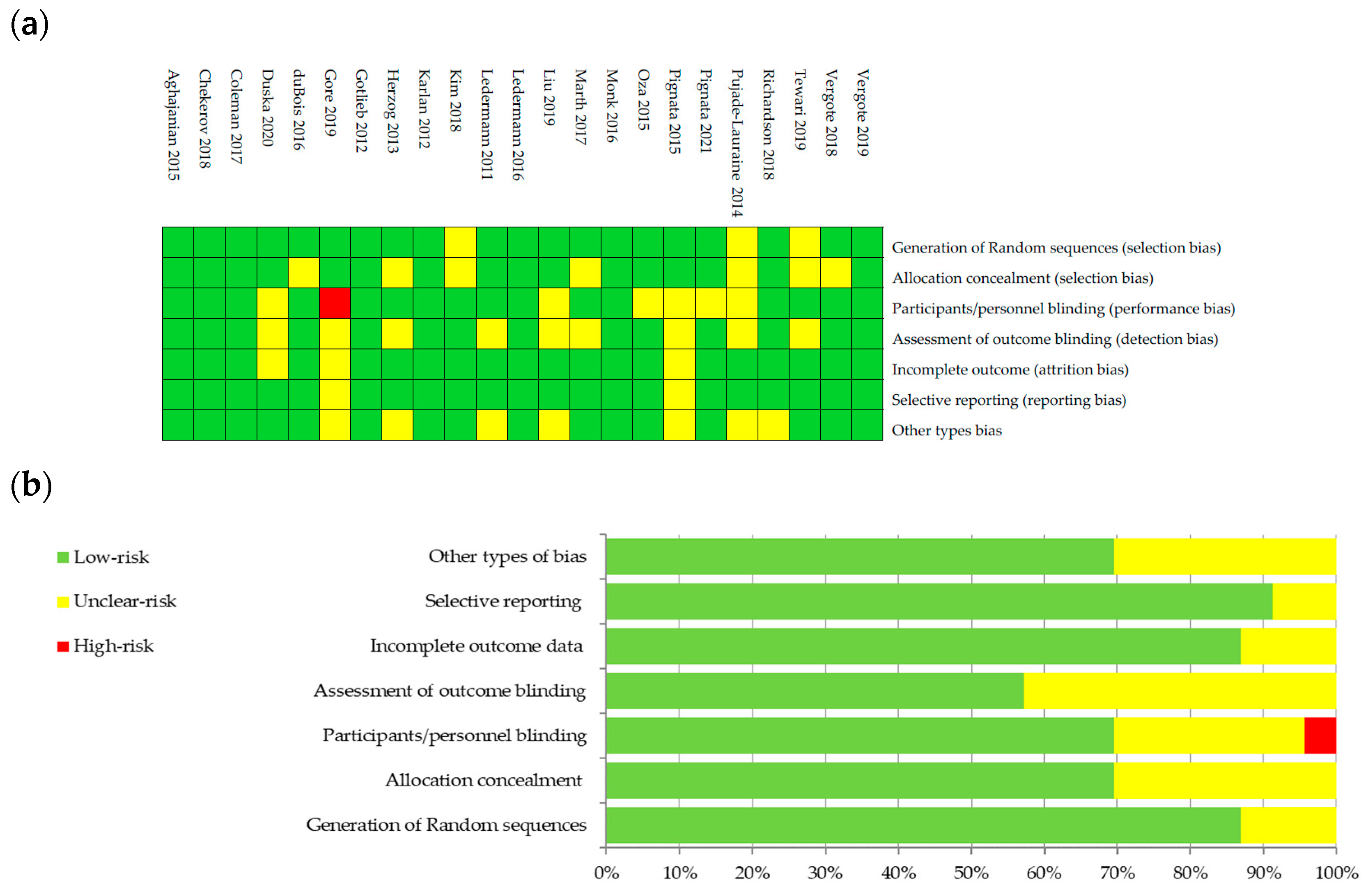
2.4. Assessment of the Bias Risk
2.5. Statistical Analysis
3. Results
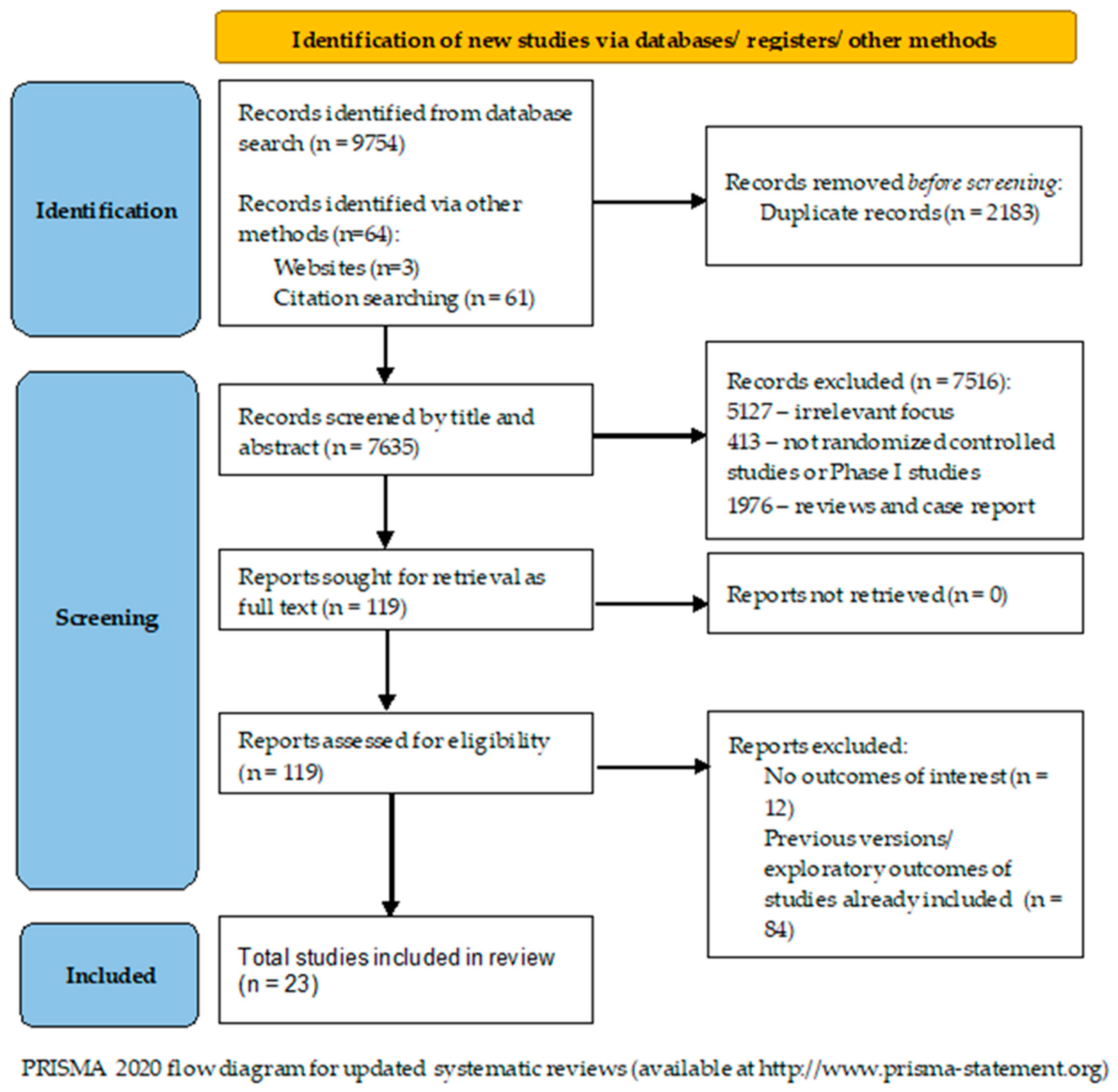
3.1. Literature Search
3.2. Studies Characteristics
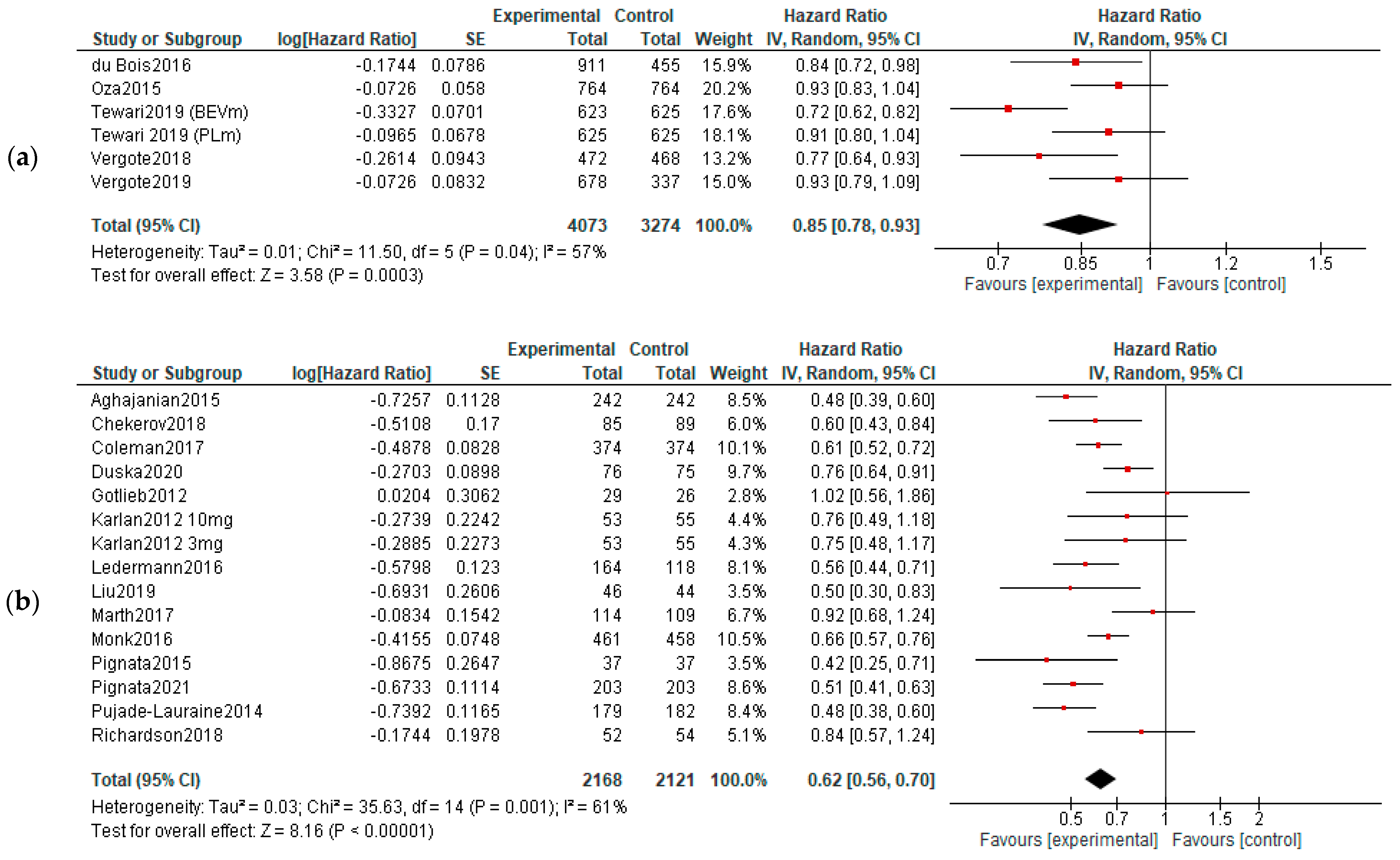
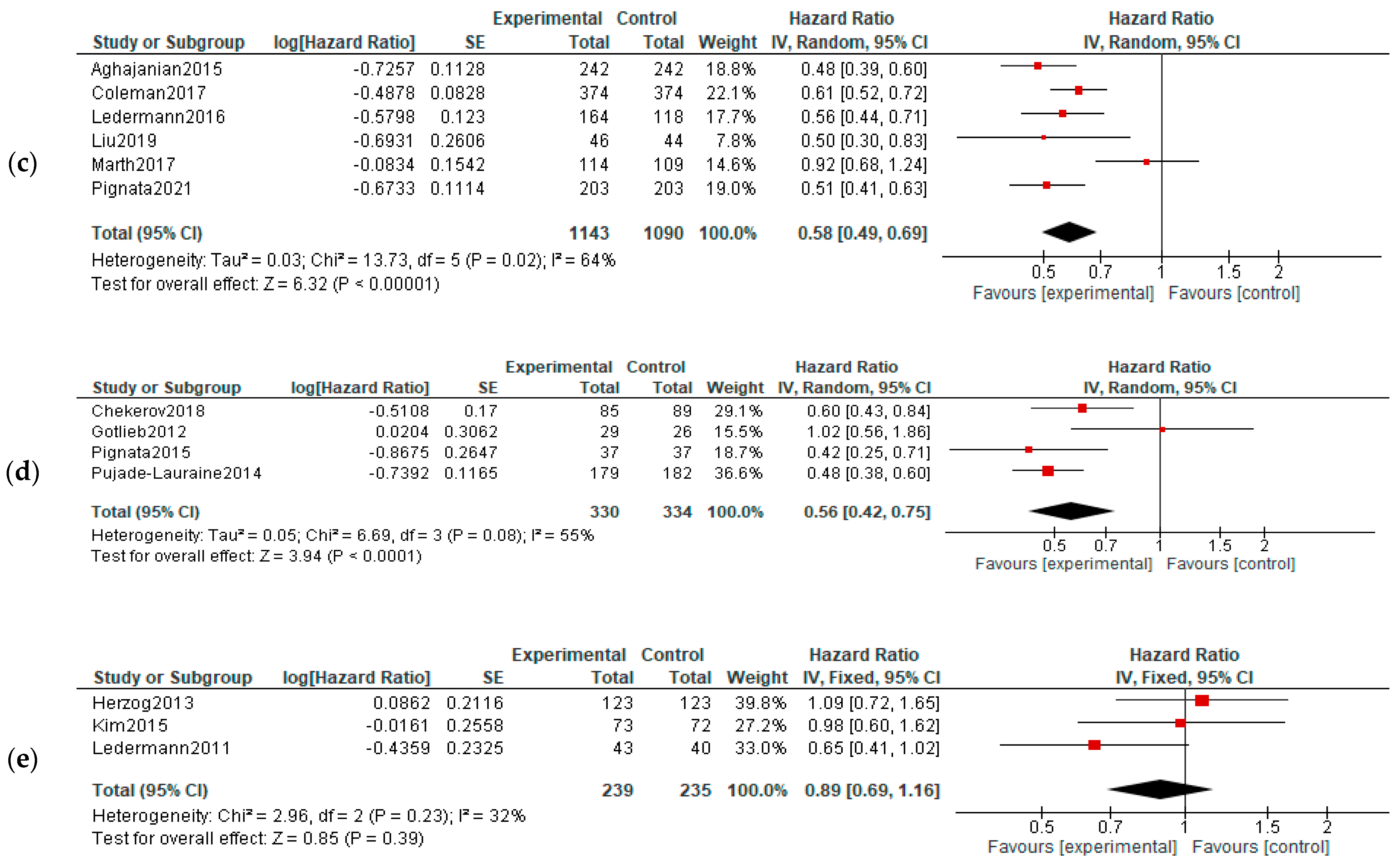
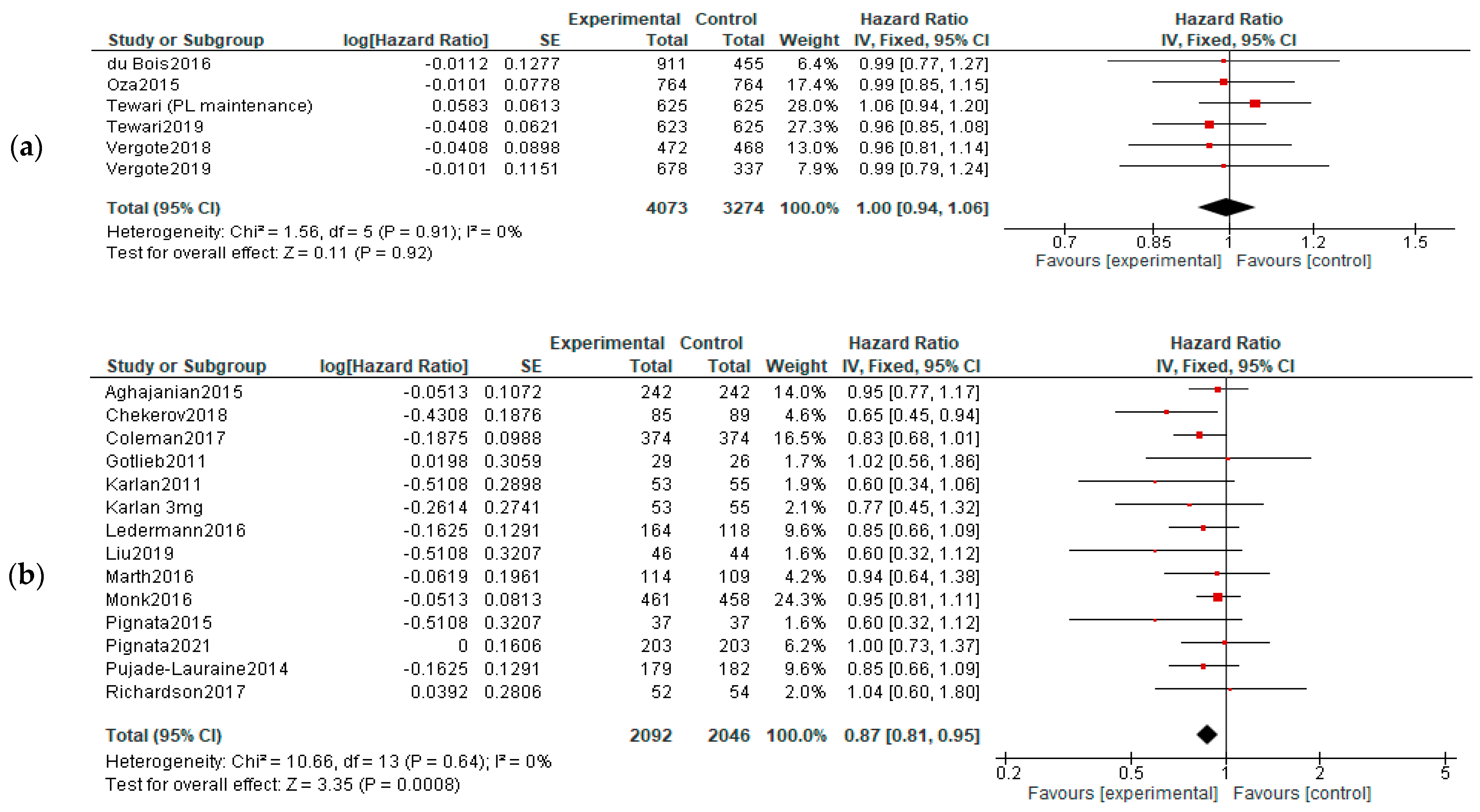
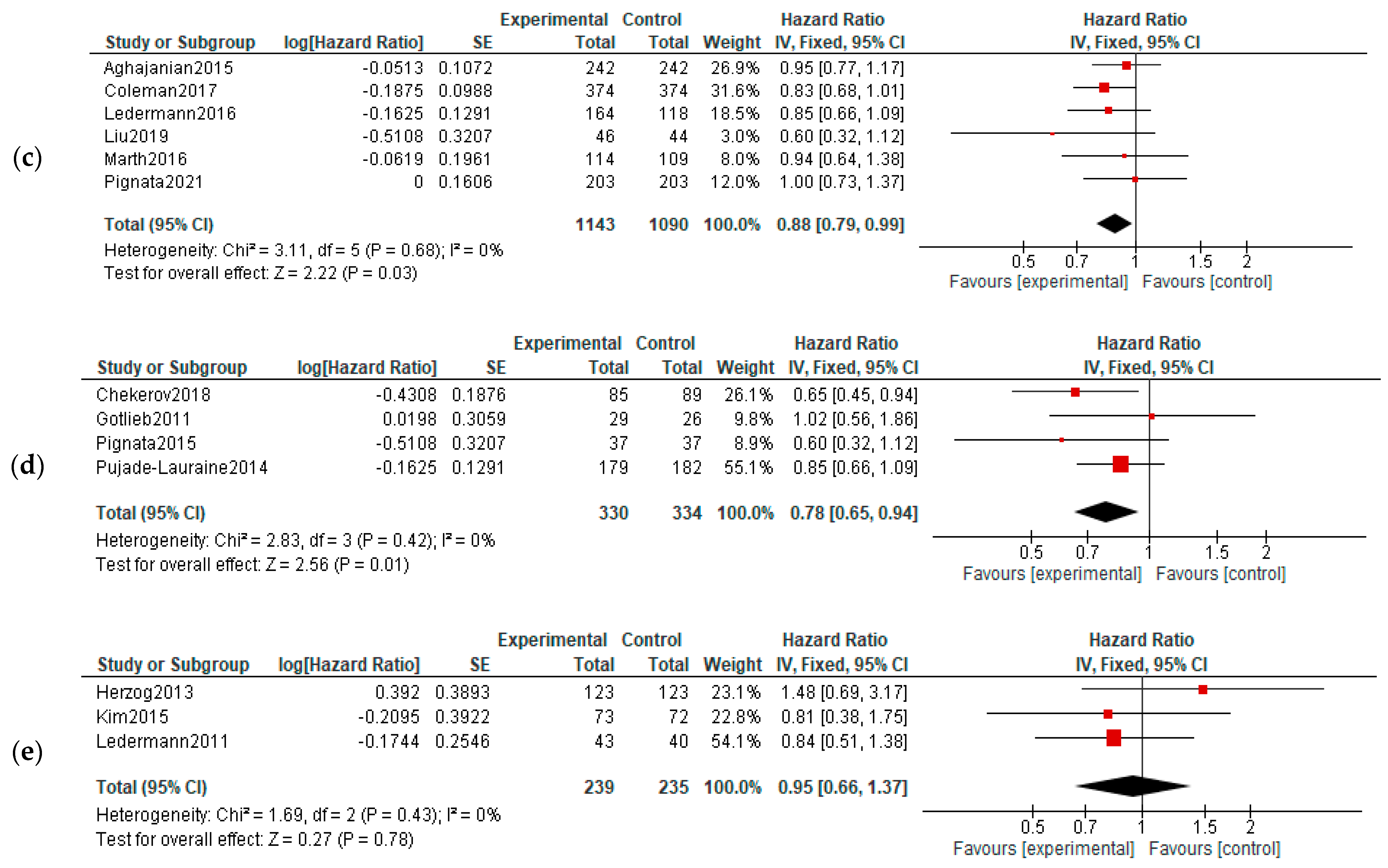
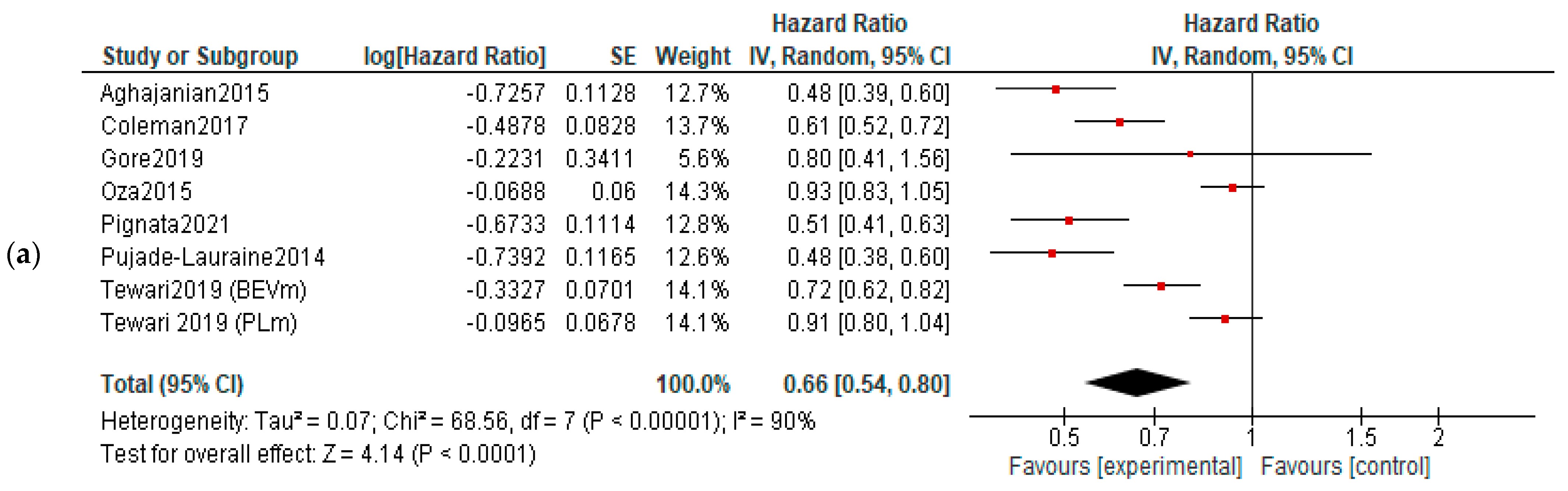
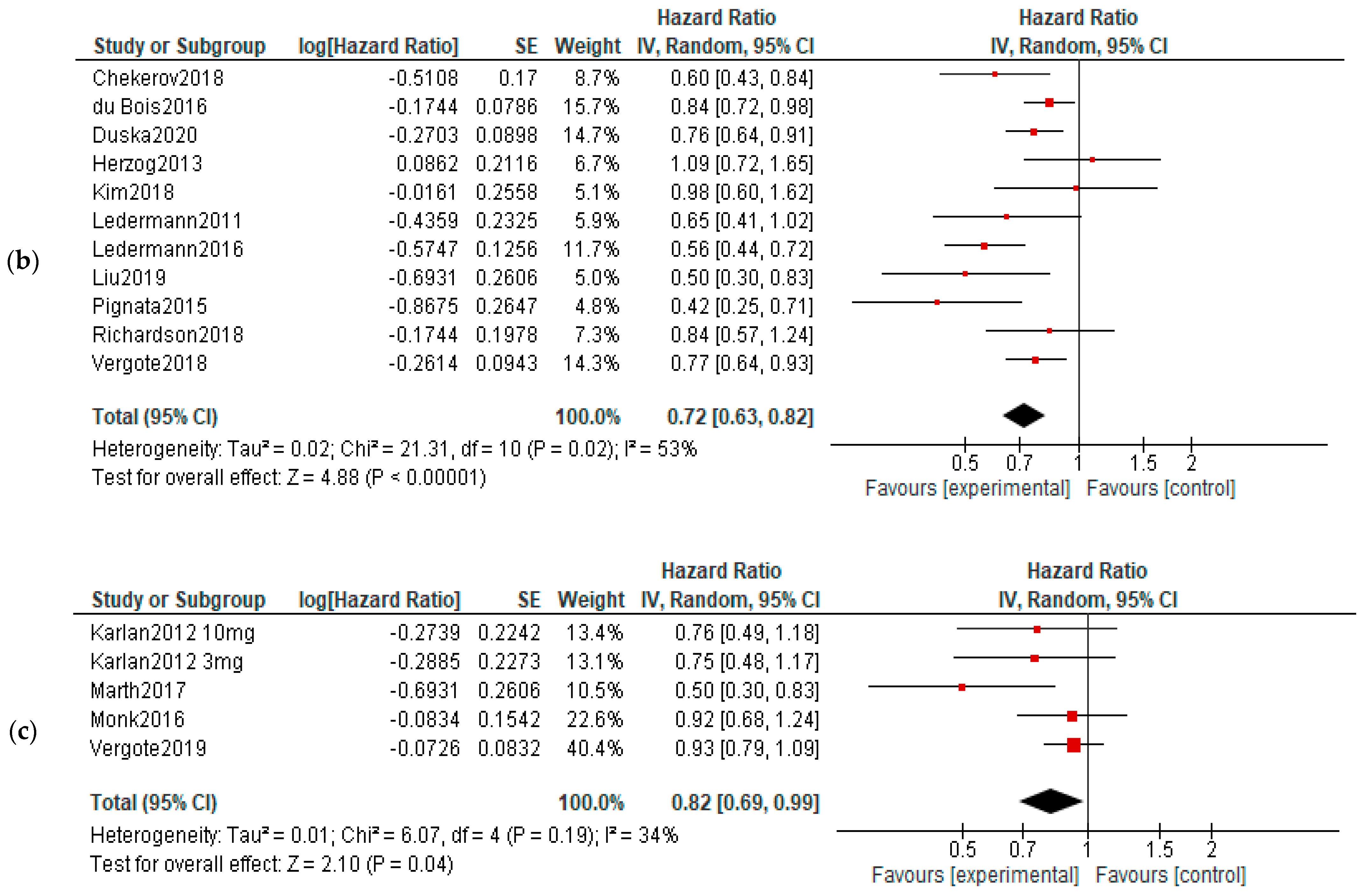
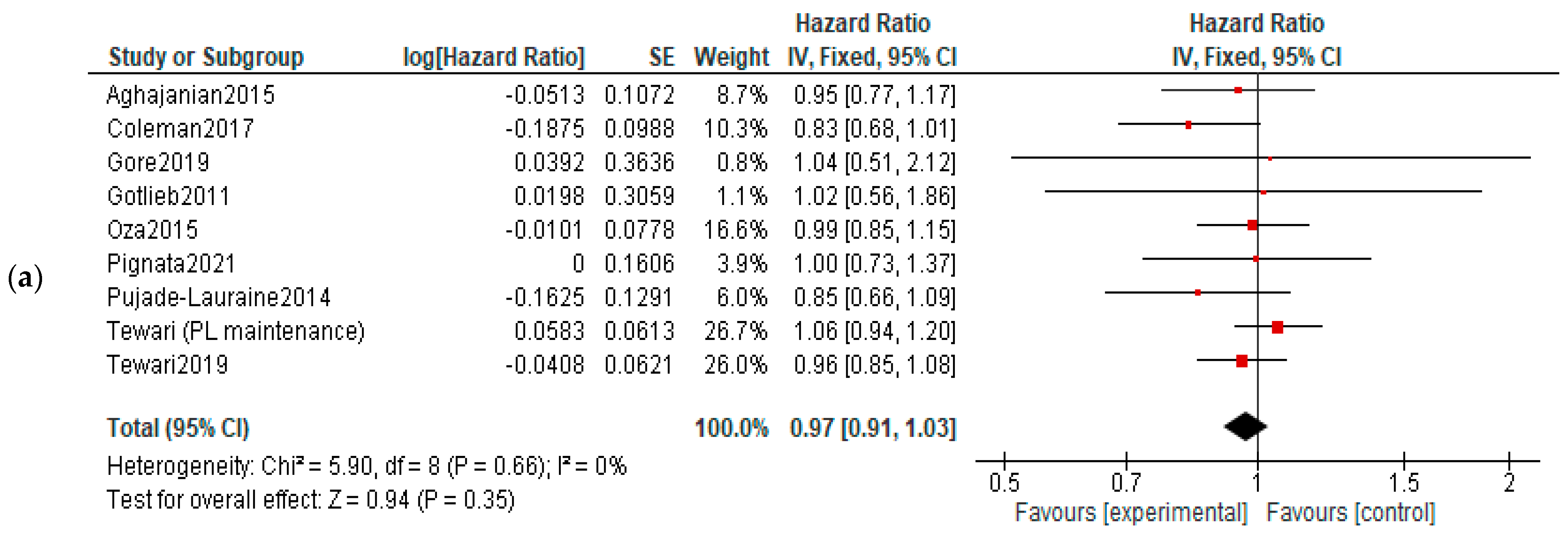
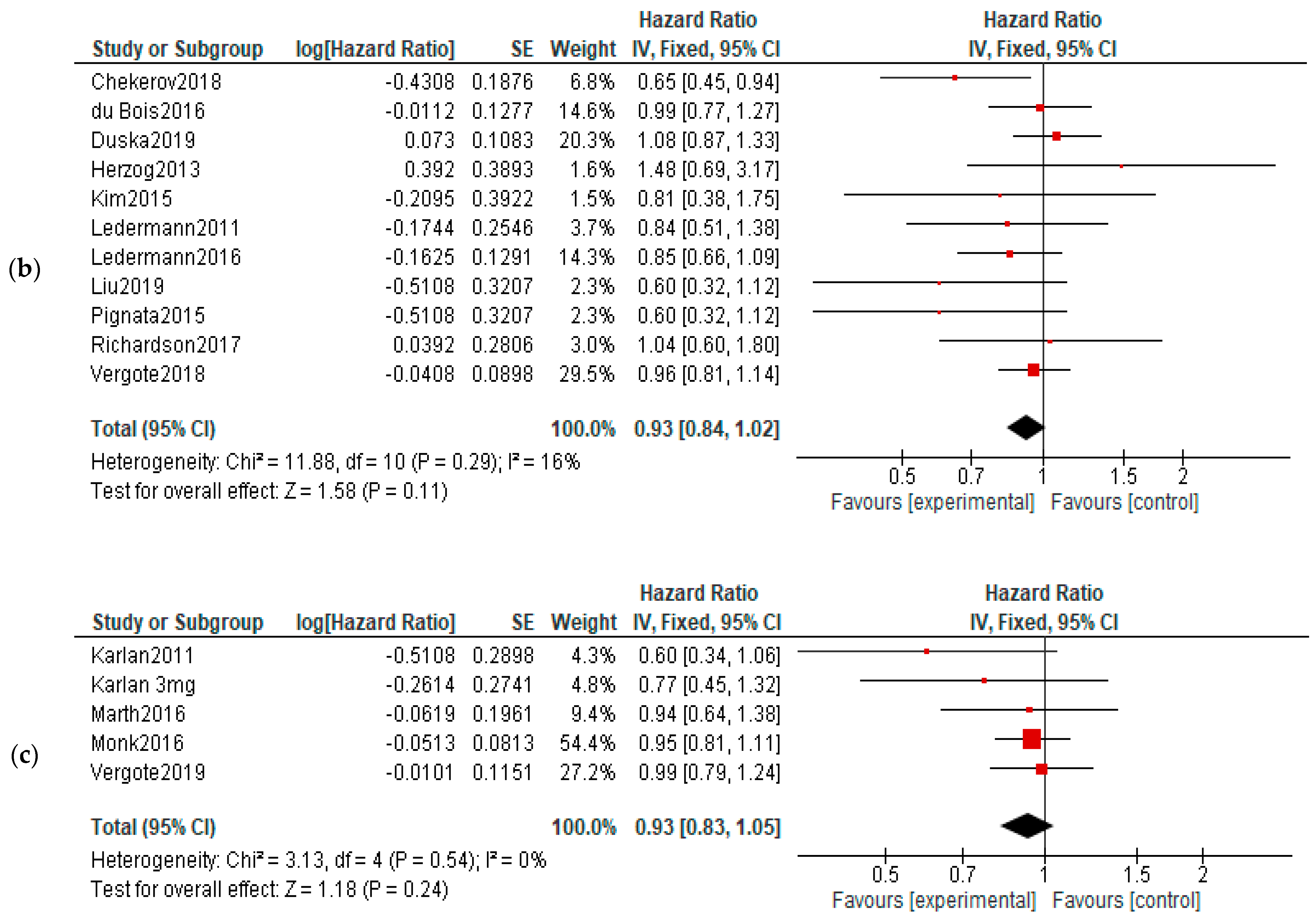
3.3. Analysis of Survival: Overall and Progression-Free
- Treatment settings analysis:
- Analysis by type of drugs used:
- Heterogeneity and publication bias:
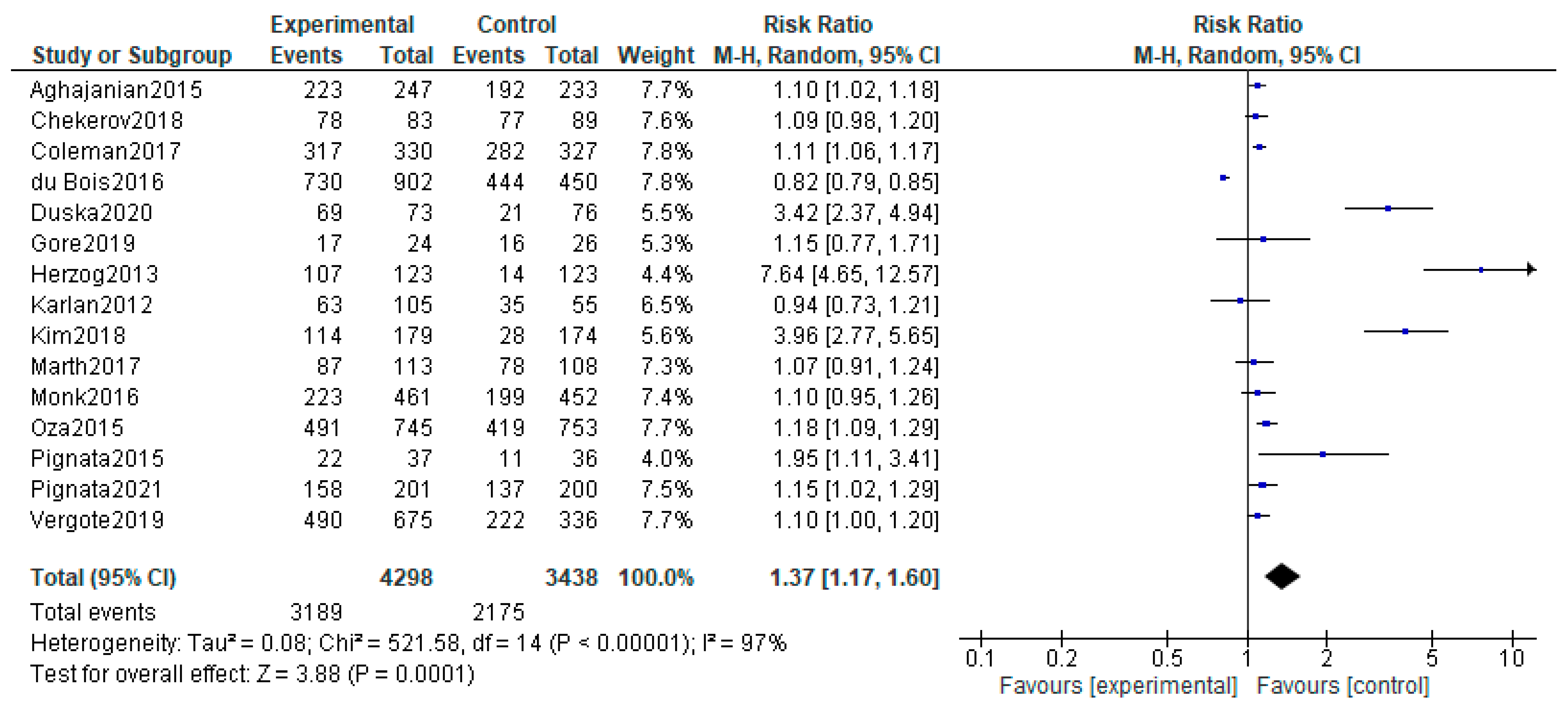
3.4. Adverse Events
4. Discussion
4.1. Interpretation of Results
4.2. Comparison with Other Studies
4.3. Strengths and Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ovary-Fact-Sheet. 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/25-Ovary-fact-sheet.pdf (accessed on 2 January 2023).
- Luvero, D.; Milani, A.; Ledermann, J.A. Treatment Options in Recurrent Ovarian Cancer: Latest Evidence and Clinical Potential. Ther. Adv. Med. Oncol. 2014, 6, 229–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matulonis, U.A.; Sood, A.K.; Fallowfield, L.; Howitt, B.E.; Sehouli, J.; Karlan, B.Y. Ovarian Cancer. Nat. Rev. Dis. Prim. 2016, 2, 16061. [Google Scholar] [CrossRef]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian Cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor Angiogenesis: Therapeutic Implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Jászai, J.; Schmidt, M.H.H. Trends and Challenges in Tumor Anti-Angiogenic Therapies. Cells 2019, 8, 1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akaza, H.; Nakagawa, M.; Tsuruo, T.; Saijo, N.; Sone, S.; Yamamoto, N.; Kakeji, Y.; Nakamura, S.; Kurebayashi, J.; Isonishi, S.; et al. Anti-Angiogenesis: New Concept for Therapy of Solid Tumors. Ann. Surg. 1972, 175, 409–416. [Google Scholar] [CrossRef]
- Carmeliet, P. VEGF as a Key Mediator of Angiogenesis in Cancer. Oncology 2005, 69, 4–10. [Google Scholar] [CrossRef]
- Dancey, J.; Sausville, E.A. Issues and Progress with Protein Kinase Inhibitors for Cancer Treatment. Nat. Rev. Drug Discov. 2003, 2, 296–313. [Google Scholar] [CrossRef]
- Ferrara, N. VEGF and the Quest for Tumour Angiogenesis Factors. Nat. Rev. Cancer 2002, 2, 795–803. [Google Scholar] [CrossRef]
- Ferrara, N.; Adamis, A.P. Ten Years of Anti-Vascular Endothelial Growth Factor Therapy. Nat. Rev. Drug Discov. 2016, 15, 385–403. [Google Scholar] [CrossRef] [Green Version]
- Olsson, A.K.; Dimberg, A.; Kreuger, J.; Claesson-Welsh, L. VEGF Receptor Signalling ? In Control of Vascular Function. Nat. Rev. Mol. Cell Biol. 2006, 7, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Elman, M.J.; Aiello, L.P.; Beck, R.W.; Bressler, N.M.; Bressler, S.B.; Edwards, A.R.; Ferris III, F.L.; Friedman, S.M.; Glassman, A.R.; Miller, K.M.; et al. Randomized Trial Evaluating Ranibizumab plus Prompt or Deferred Laser or Triamcinolone plus Prompt Laser for Diabetic Macular Edema. Ophthalmology 2010, 117, 1064–1077.e35. [Google Scholar] [CrossRef] [Green Version]
- CATT Research Group. Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration. N. Engl. J. Med. 2011, 364, 1897–1908. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for Diabetic Macular Edema: Results from 2 Phase III Randomized Trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.-F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal Aflibercept (VEGF Trap-Eye) in Wet Age-Related Macular Degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef]
- Brown, D.M.; Campochiaro, P.A.; Bhisitkul, R.B.; Ho, A.C.; Gray, S.; Saroj, N.; Adamis, A.P.; Rubio, R.G.; Murahashi, W.Y. Sustained Benefits from Ranibizumab for Macular Edema Following Branch Retinal Vein Occlusion: 12-Month Outcomes of a Phase III Study. Ophthalmology 2011, 118, 1594–1602. [Google Scholar] [CrossRef]
- Miller, J.W. The Harvard Angiogenesis Story. Surv. Ophthalmol. 2014, 59, 361–364. [Google Scholar] [CrossRef] [Green Version]
- Turcan, N.; Baros, A.; Zugravu, C.; Mergeanu, M.; Sajin, M.; Andreescu, C.V.; Frincu, F.; Carp-Veliscu, A.; Edu, A.; Mehedintu, C.; et al. Trend of Incidence in the Last Five Years of Breast, Cervical, Ovarian and Uterine Cancer in the Main Hospital in Romania. Rom. J. Med. Pract. 2021, 16, 62–68. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Mendeley Reference Manager | Mendeley. Available online: https://www.mendeley.com/reference-management/reference-manager (accessed on 28 January 2023).
- McGuire, W.P.; Hoskins, W.J.; Brady, M.F.; Kucera, P.R.; Partridge, E.E.; Look, K.Y.; Clarke-Pearson, D.L.; Davidson, M. Cyclophosphamide and Cisplatin Compared with Paclitaxel and Cisplatin in Patients with Stage III and Stage IV Ovarian Cancer. N. Engl. J. Med. 1996, 334, 1–6. [Google Scholar] [CrossRef]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) Design as a Framework to Formulate Eligibility Criteria in Systematic Reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RevMan | Cochrane Training. Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 24 January 2023).
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard Chemotherapy with or without Bevacizumab for Women with Newly Diagnosed Ovarian Cancer (ICON7): Overall Survival Results of a Phase 3 Randomised Trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef]
- Aghajanian, C.; Goff, B.; Nycum, L.R.; Wang, Y.V.; Husain, A.; Blank, S.V. Final Overall Survival and Safety Analysis of OCEANS, a Phase 3 Trial of Chemotherapy with or without Bevacizumab in Patients with Platinum-Sensitive Recurrent Ovarian Cancer. Gynecol. Oncol. 2015, 139, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotlieb, W.H.; Amant, F.; Advani, S.; Goswami, C.; Hirte, H.; Provencher, D.; Somani, N.; Yamada, D.; Tamby, J.-F.; Vergote, I. Intravenous Afl Ibercept for Treatment of Recurrent Symptomatic Malignant Ascites in Patients with Advanced Ovarian Cancer: A Phase 2, Randomised, Double-Blind, Placebo-Controlled Study. Lancet Oncol. 2012, 13, 154–162. [Google Scholar] [CrossRef]
- Karlan, B.Y.; Oza, A.M.; Richardson, G.E.; Provencher, D.M.; Hansen, V.L.; Buck, M.; Chambers, S.K.; Ghatage, P.; Pippitt, C.H.; Brown, J.V.; et al. Randomized, Double-Blind, Placebo-Controlled Phase II Study of AMG 386 Combined with Weekly Paclitaxel in Patients with Recurrent Ovarian Cancer. J. Clin. Oncol. 2012, 30, 362–371. [Google Scholar] [CrossRef]
- Chekerov, R.; Hilpert, F.; Mahner, S.; El-Balat, A.; Harter, P.; de Gregorio, N.; Fridrich, C.; Markmann, S.; Potenberg, J.; Lorenz, R.; et al. Sorafenib plus Topotecan versus Placebo plus Topotecan for Platinum-Resistant Ovarian Cancer (TRIAS): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Oncol. 2018, 19, 1247–1258. [Google Scholar] [CrossRef]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and Paclitaxel–Carboplatin Chemotherapy and Secondary Cytoreduction in Recurrent, Platinum-Sensitive Ovarian Cancer (NRG Oncology/Gynecologic Oncology Group Study GOG-0213): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Duska, L.R.; Petroni, G.R.; Varhegyi, N.; Brown, J.; Jelovac, D.; Moore, K.N.; McGuire, W.P.; Darus, C.; Barroilhet, L.M.; Secord, A.A. A Randomized Phase II Evaluation of Weekly Gemcitabine plus Pazopanib versus Weekly Gemcitabine Alone in the Treatment of Persistent or Recurrent Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Carcinoma. Gynecol. Oncol. 2020, 157, 585–592. [Google Scholar] [CrossRef]
- du Bois, A.; Kristensen, G.; Ray-Coquard, I.; Reuss, A.; Pignata, S.; Colombo, N.; Denison, U.; Vergote, I.; del Campo, J.M.; Ottevanger, P.; et al. Standard First-Line Chemotherapy with or without Nintedanib for Advanced Ovarian Cancer (AGO-OVAR 12): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet Oncol. 2016, 17, 78–89. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Cibula, D.; Mirza, M.R.; Reuss, A.; Ricci, C.; Colombo, N.; Koch, H.; Goffin, F.; González-Martin, A.; Ottevanger, P.B.; et al. Final Results from GCIG/ENGOT/AGO-OVAR 12, a Randomised Placebo-Controlled Phase III Trial of Nintedanib Combined with Chemotherapy for Newly Diagnosed Advanced Ovarian Cancer. Int. J. Cancer 2020, 146, 439–448. [Google Scholar] [CrossRef]
- Gore, M.; Hackshaw, A.; Brady, W.E.; Penson, R.T.; Zaino, R.; McCluggage, W.G.; Ganesan, R.; Wilkinson, N.; Perren, T.; Montes, A.; et al. An International, Phase III Randomized Trial in Patients with Mucinous Epithelial Ovarian Cancer (MEOC/GOG 0241) with Long-Term Follow-up: And Experience of Conducting a Clinical Trial in a Rare Gynecological Tumor. Gynecol. Oncol. 2019, 153, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Herzog, T.J.; Scambia, G.; Kim, B.G.; Lhommé, C.; Markowska, J.; Ray-Coquard, I.; Sehouli, J.; Colombo, N.; Shan, M.; Petrenciuc, O.; et al. A Randomized Phase II Trial of Maintenance Therapy with Sorafenib in Front-Line Ovarian Carcinoma. Gynecol. Oncol. 2013, 130, 25–30. [Google Scholar] [CrossRef]
- Kim, J.W.; Mahner, S.; Wu, L.Y.; Shoji, T.; Kim, B.G.; Zhu, J.Q.; Takano, T.; Park, S.Y.; Kong, B.H.; Wu, Q.; et al. Pazopanib Maintenance Therapy in East Asian Women with Advanced Epithelial Ovarian Cancer: Results from AGO-OVAR16 and an East Asian Study. Int. J. Gynecol. Cancer 2018, 28, 2–10. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Hackshaw, A.; Kaye, S.; Jayson, G.; Gabra, H.; McNeish, I.; Earl, H.; Perren, T.; Gore, M.; Persic, M.; et al. Randomized Phase II Placebo-Controlled Trial of Maintenance Therapy Using the Oral Triple Angiokinase Inhibitor BIBF 1120 after Chemotherapy for Relapsed Ovarian Cancer. J. Clin. Oncol. 2011, 29, 3798–3804. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Embleton-Thirsk, A.C.; Perren, T.J.; Jayson, G.C.; Rustin, G.J.S.; Kaye, S.B.; Hirte, H.; Oza, A.; Vaughan, M.; Friedlander, M.; et al. Cediranib in Addition to Chemotherapy for Women with Relapsed Platinum-Sensitive Ovarian Cancer (ICON6): Overall Survival Results of a Phase III Randomised Trial. ESMO Open 2021, 6, 100043. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Embleton, A.C.; Raja, F.; Perren, T.J.; Jayson, G.C.; Rustin, G.J.S.; Kaye, S.B.; Hirte, H.; Eisenhauer, E.; Vaughan, M.; et al. Cediranib in Patients with Relapsed Platinum-Sensitive Ovarian Cancer (ICON6): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet 2016, 387, 1066–1074. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.F.; Barry, W.T.; Birrer, M.; Lee, J.M.; Buckanovich, R.J.; Fleming, G.F.; Rimel, B.J.; Buss, M.K.; Nattam, S.R.; Hurteau, J.; et al. Overall Survival and Updated Progression-Free Survival Outcomes in a Randomized Phase II Study of Combination Cediranib and Olaparib versus Olaparib in Relapsed Platinum-Sensitive Ovarian Cancer. Ann. Oncol. 2019, 30, 551–557. [Google Scholar] [CrossRef]
- Marth, C.; Vergote, I.; Scambia, G.; Oberaigner, W.; Clamp, A.; Berger, R.; Kurzeder, C.; Colombo, N.; Vuylsteke, P.; Lorusso, D.; et al. ENGOT-Ov-6/TRINOVA-2: Randomised, Double-Blind, Phase 3 Study of Pegylated Liposomal Doxorubicin plus Trebananib or Placebo in Women with Recurrent Partially Platinum-Sensitive or Resistant Ovarian Cancer. Eur. J. Cancer 2017, 70, 111–121. [Google Scholar] [CrossRef]
- Monk, B.J.; Poveda, A.; Vergote, I.; Raspagliesi, F.; Fujiwara, K.; Bae, D.S.; Oaknin, A.; Ray-Coquard, I.; Provencher, D.M.; Karlan, B.Y.; et al. Final Results of a Phase 3 Study of Trebananib plus Weekly Paclitaxel in Recurrent Ovarian Cancer (TRINOVA-1): Long-Term Survival, Impact of Ascites, and Progression-Free Survival-2. Gynecol. Oncol. 2016, 143, 27–34. [Google Scholar] [CrossRef]
- Pignata, S.; Lorusso, D.; Joly, F.; Gallo, C.; Colombo, N.; Sessa, C.; Bamias, A.; Salutari, V.; Selle, F.; Frezzini, S.; et al. Carboplatin-Based Doublet plus Bevacizumab beyond Progression versus Carboplatin-Based Doublet Alone in Patients with Platinum-Sensitive Ovarian Cancer: A Randomised, Phase 3 Trial. Lancet Oncol. 2021, 22, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Pignata, S.; Lorusso, D.; Scambia, G.; Sambataro, D.; Tamberi, S.; Cinieri, S.; Mosconi, A.M.; Orditura, M.; Brandes, A.A.; Arcangeli, V.; et al. Pazopanib plus Weekly Paclitaxel versus Weekly Paclitaxel Alone for Platinum-Resistant or Platinum-Refractory Advanced Ovarian Cancer (MITO 11): A Randomised, Open-Label, Phase 2 Trial. Lancet Oncol. 2015, 16, 561–568. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined with Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.L.; Sill, M.W.; Coleman, R.L.; Sood, A.K.; Pearl, M.L.; Kehoe, S.M.; Carney, M.E.; Hanjani, P.; van Le, L.; Zhou, X.C.; et al. Paclitaxel with and without Pazopanib for Persistent or Recurrent Ovarian Cancer: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 196–202. [Google Scholar] [CrossRef]
- Tewari, K.S.; Burger, R.A.; Enserro, D.; Norquist, B.M.; Swisher, E.M.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Huang, H.; Homesley, H.D.; et al. Final Overall Survival of a Randomized Trial of Bevacizumab for Primary Treatment of Ovarian Cancer. J. Clin. Oncol. 2019, 37, 2317–2328. [Google Scholar] [CrossRef]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of Bevacizumab in the Primary Treatment of Ovarian Cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef] [Green Version]
- Vergote, I.; du Bois, A.; Floquet, A.; Rau, J.; Kim, J.W.; del Campo, J.M.; Friedlander, M.; Pignata, S.; Fujiwara, K.; Colombo, N.; et al. Overall Survival Results of AGO-OVAR16: A Phase 3 Study of Maintenance Pazopanib versus Placebo in Women Who Have Not Progressed after First-Line Chemotherapy for Advanced Ovarian Cancer. Gynecol. Oncol. 2019, 155, 186–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- du Bois, A.; Floquet, A.; Kim, J.W.; Rau, J.; del Campo, J.M.; Friedlander, M.; Pignata, S.; Fujiwara, K.; Vergote, I.; Colombo, N.; et al. Incorporation of Pazopanib in Maintenance Therapy of Ovarian Cancer. J. Clin. Oncol. 2014, 32, 3374–3381. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Scambia, G.; O’Malley, D.; van Calster, B.; Park, S.Y.; del Campo, J.M.; Meier, W.; Bamias, A.; Colombo, N.; Wenham, R.M.; et al. Trebananib or Placebo plus Carboplatin and Paclitaxel as First-Line Treatment for Advanced Ovarian Cancer (TRINOVA-3/ENGOT-Ov2/GOG-3001): A Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol. 2019, 20, 862–876. [Google Scholar] [CrossRef]
- El Helali, A.; Wong, C.H.L.; Choi, H.C.W.; Chan, W.W.L.; Dickson, N.; Siu, S.W.K.; Chan, K.K.; Ngan, H.Y.S.; Ngan, R.K.C.; Kennedy, R.D. A Comprehensive Systematic Review and Network Meta-Analysis: The Role of Anti-Angiogenic Agents in Advanced Epithelial Ovarian Cancer. Sci. Rep. 2022, 12, 3803. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef] [PubMed]
- Kay, A.; Higgins, J.; Day, A.G.; Meyer, R.M.; Booth, C.M. Randomized Controlled Trials in the Era of Molecular Oncology: Methodology, Biomarkers, and End Points. Ann. Oncol. 2012, 23, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- A Review of Studies Examining the Relationship between Progression-Free Survival and Overall Survival in Advanced or Metastatic Cancer. Available online: https://pubmed.ncbi.nlm.nih.gov/28481488/ (accessed on 27 January 2023).
- Kim, C.; Prasad, V. Cancer Drugs Approved on the Basis of a Surrogate End Point and Subsequent Overall Survival: An Analysis of 5 Years of US Food and Drug Administration Approvals. JAMA Intern. Med. 2015, 175, 1992–1994. [Google Scholar] [CrossRef] [Green Version]
- Pasalic, D.; McGinnis, G.J.; Fuller, C.D.; Grossberg, A.J.; Verma, V.; Mainwaring, W.; Miller, A.B.; Lin, T.A.; Jethanandani, A.; Espinoza, A.F.; et al. Progression-Free Survival Is a Suboptimal Predictor for Overall Survival Among Metastatic Solid Tumor Clinical Trials. Eur. J. Cancer 2020, 136, 176. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Kim, C.; Burotto, M.; Vandross, A. The Strength of Association between Surrogate End Points and Survival in Oncology: A Systematic Review of Trial-Level Meta-Analyses. JAMA Intern. Med. 2015, 175, 1389–1398. [Google Scholar] [CrossRef] [Green Version]
- Paoletti, X.; Lewsley, L.A.; Daniele, G.; Cook, A.; Yanaihara, N.; Tinker, A.; Kristensen, G.; Ottevanger, P.B.; Aravantinos, G.; Miller, A.; et al. Assessment of Progression-Free Survival as a Surrogate End Point of Overall Survival in First-Line Treatment of Ovarian Cancer: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2020, 3, e1918939. [Google Scholar] [CrossRef]
- Backen, A.; Renehan, A.G.; Clamp, A.R.; Berzuini, C.; Zhou, C.; Oza, A.; Bannoo, S.; Scherer, S.J.; Banks, R.E.; Dive, C.; et al. The Combination of Circulating Ang1 and Tie2 Levels Predict Progression Free Survival Advantage in Bevacizumab-Treated Ovarian Cancer Patients. Clin. Cancer Res. 2014, 20, 4549. [Google Scholar] [CrossRef] [Green Version]
- Gourley, C.; McCavigan, A.; Perren, T.; Paul, J.; Michie, C.O.; Churchman, M.; Williams, A.; McCluggage, W.G.; Parmar, M.; Kaplan, R.S.; et al. Molecular Subgroup of High-Grade Serous Ovarian Cancer (HGSOC) as a Predictor of Outcome Following Bevacizumab. J. Clin. Oncol. 2014, 32, 5502. [Google Scholar] [CrossRef]
- Collinson, F.; Hutchinson, M.; Craven, R.A.; Cairns, D.A.; Zougman, A.; Wind, T.C.; Gahir, N.; Messenger, M.P.; Jackson, S.; Thompson, D.; et al. Predicting Response to Bevacizumab in Ovarian Cancer: A Panel of Potential Biomarkers Informing Treatment Selection. Clin. Cancer Res. 2013, 19, 5227. [Google Scholar] [CrossRef] [Green Version]
- Jayson, G.C.; Kerbel, R.; Ellis, L.M.; Harris, A.L. Antiangiogenic Therapy in Oncology: Current Status and Future Directions. Lancet 2016, 388, 518–529. [Google Scholar] [CrossRef]
- Birrer, M.J.; Choi, Y.; Brady, M.F.; Mannel, R.S.; Burger, R.A.; WEI, W.; Husain, A.; Bais, C. Retrospective Analysis of Candidate Predictive Tumor Biomarkers (BMs) for Efficacy in the GOG-0218 Trial Evaluating Front-Line Carboplatin–Paclitaxel (CP) ± Bevacizumab (BEV) for Epithelial Ovarian Cancer (EOC). J. Clin. Oncol. 2015, 33, 5505. [Google Scholar] [CrossRef]
- Bais, C.; Mueller, B.; Brady, M.F.; Mannel, R.S.; Burger, R.A.; Wei, W.; Marien, K.M.; Kockx, M.M.; Husain, A.; Birrer, M.J. Tumor Microvessel Density as a Potential Predictive Marker for Bevacizumab Benefit: GOG-0218 Biomarker Analyses. JNCI J. Natl. Cancer Inst. 2017, 109, djx066. [Google Scholar] [CrossRef] [Green Version]
- Secord, A.A.; Burdett, K.B.; Owzar, K.; Tritchler, D.; Sibley, A.B.; Liu, Y.; Starr, M.D.; Chris Brady, J.; Lankes, H.A.; Hurwitz, H.I.; et al. Predictive Blood-Based Biomarkers in Patients with Epithelial Ovarian Cancer Treated with Carboplatin and Paclitaxel with or without Bevacizumab: Results from GOG-0218. Clin. Cancer Res. 2020, 26, 1288–1296. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Yang, X.; Yin, Y.; Zhang, H.; Yin, F.; Guo, P.; Zhang, X.; Sun, C.; Li, S.; Han, Y.; et al. Identifying the Role of Oxidative Stress-Related Genes as Prognostic Biomarkers and Predicting the Response of Immunotherapy and Chemotherapy in Ovarian Cancer. Oxid. Med. Cell. Longev. 2022, 2022, 6575534. [Google Scholar] [CrossRef] [PubMed]
- Chaiswing, L.; Yarana, C.; Clair, W.S.; Tovmasyan, A.; Batinic-Haberle, I.; Spasojevic, I.; St Clair, D. A Redox-Active Mn Porphyrin, MnTnBuOE-2-PyP5+, Synergizes with Carboplatin in Treatment of Chemoresistant Ovarian Cell Line. Oxid. Med. Cell. Longev. 2022, 2022, 9664636. [Google Scholar] [CrossRef] [PubMed]
- Cecerska-Heryć, E.; Surowska, O.; Heryć, R.; Serwin, N.; Napiontek-Balińska, S.; Dołęgowska, B. Are Antioxidant Enzymes Essential Markers in the Diagnosis and Monitoring of Cancer Patients—A Review. Clin. Biochem 2021, 93, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, N.M.; Belotte, J.; Saed, M.G.; Memaj, I.; Diamond, M.P.; Morris, R.T.; Saed, G.M. Specific Point Mutations in Key Redox Enzymes Are Associated with Chemoresistance in Epithelial Ovarian Cancer. Free Radic. Biol. Med. 2017, 102, 122–132. [Google Scholar] [CrossRef]
- Senthil, K.; Aranganathan, S.; Nalini, N. Evidence of Oxidative Stress in the Circulation of Ovarian Cancer Patients. Clin. Chim. Acta 2004, 339, 27–32. [Google Scholar] [CrossRef]
- Rahimian, N.; Razavi, Z.S.; Aslanbeigi, F.; Mirkhabbaz, A.M.; Piroozmand, H.; Shahrzad, M.K.; Hamblin, M.R.; Mirzaei, H. Non-Coding RNAs Related to Angiogenesis in Gynecological Cancer. Gynecol. Oncol. 2021, 161, 896–912. [Google Scholar] [CrossRef]
- Friedlander, M.; Rau, J.; Lee, C.K.; Meier, W.; Lesoin, A.; Kim, J.W.; Poveda, A.; Buck, M.; Scambia, G.; Shimada, M.; et al. Quality of Life in Patients with Advanced Epithelial Ovarian Cancer (EOC) Randomized to Maintenance Pazopanib or Placebo after First-Line Chemotherapy in the AGO-OVAR 16 Trial. Measuring What Matters-Patient-Centered End Points in Trials of Maintenance Therapy. Ann. Oncol. 2018, 29, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Stark, D.; Nankivell, M.; Pujade-Lauraine, E.; Kristensen, G.; Elit, L.; Stockler, M.; Hilpert, F.; Cervantes, A.; Brown, J.; Lanceley, A.; et al. Standard Chemotherapy with or without Bevacizumab in Advanced Ovarian Cancer: Quality-of-Life Outcomes from the International Collaboration on Ovarian Neoplasms (ICON7) Phase 3 Randomised Trial. Lancet Oncol. 2013, 14, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bindra, R.S.; Schaffer, P.J.; Meng, A.; Woo, J.; Måseide, K.; Roth, M.E.; Lizardi, P.; Hedley, D.W.; Bristow, R.G.; Glazer, P.M. Down-Regulation of Rad51 and Decreased Homologous Recombination in Hypoxic Cancer Cells. Mol. Cell. Biol. 2004, 24, 8504–8518. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.R.; Pignata, S.; Ledermann, J.A. Latest Clinical Evidence and Further Development of PARP Inhibitors in Ovarian Cancer. Ann. Oncol. 2018, 29, 1366–1376. [Google Scholar] [CrossRef]
- Bindra, R.S.; Gibson, S.L.; Meng, A.; Westermark, U.; Jasin, M.; Pierce, A.J.; Bristow, R.G.; Classon, M.K.; Glazer, P.M. Hypoxia-Induced down-Regulation of BRCA1 Expression by E2Fs. Cancer Res. 2005, 65, 11597–11604. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, D.; Maltese, G.; Sabatucci, I.; Cresta, S.; Matteo, C.; Ceruti, T.; D’Incalci, M.; Zucchetti, M.; Raspagliesi, F.; Sonetto, C.; et al. Phase I Study of Rucaparib in Combination with Bevacizumab in Ovarian Cancer Patients: Maximum Tolerated Dose and Pharmacokinetic Profile. Target. Oncol. 2021, 16, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Carboplatin-Paclitaxel-Bevacizumab vs Carbo-Pacli-Beva-Rucaparib vs Carbo-Pacli-Ruca, Selected According to HRD Status, in Patients With Advanced Ovarian, Primary Peritoneal and Fallopian Tube Cancer, Preceded by a Phase I Dose Escalation Study on Ruca-Beva Combination—Full Text View—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03462212 (accessed on 27 January 2023).
- Mirza, M.R.; Bergmann, T.K.; Mau-Sørensen, M.; Christensen, R.d.P.; Åvall-Lundqvist, E.; Birrer, M.J.; Jørgensen, M.; Roed, H.; Malander, S.; Nielsen, F.; et al. A Phase I Study of the PARP Inhibitor Niraparib in Combination with Bevacizumab in Platinum-Sensitive Epithelial Ovarian Cancer: NSGO AVANOVA1/ENGOT-OV24. Cancer Chemother. Pharmacol. 2019, 84, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Stapor, P.; Wang, X.; Goveia, J.; Moens, S.; Carmeliet, P. Angiogenesis Revisited-Role and Therapeutic Potential of Targeting Endothelial Metabolism. J. Cell Sci. 2014, 127, 4331–4341. [Google Scholar] [CrossRef] [Green Version]
- de Bock, K.; Cauwenberghs, S.; Carmeliet, P. Vessel Abnormalization: Another Hallmark of Cancer?: Molecular Mechanisms and Therapeutic Implications. Curr. Opin. Genet. Dev. 2011, 21, 73–79. [Google Scholar] [CrossRef]
- Michaelsen, S.R.; Staberg, M.; Pedersen, H.; Jensen, K.E.; Majewski, W.; Broholm, H.; Nedergaard, M.K.; Meulengracht, C.; Urup, T.; Villingshøj, M.; et al. VEGF-C Sustains VEGFR2 Activation under Bevacizumab Therapy and Promotes Glioblastoma Maintenance. Neuro Oncol. 2018, 20, 1462–1474. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.P.; Rodriguez, M.; Adams, K.; Goldenberg, D.M.; Blumenthal, R.D. Altered Tumor Vessel Maturation and Proliferation in Placenta Growth Factor-Producing Tumors: Potential Relationship to Post-Therapy Tumor Angiogenesis and Recurrence. Int. J. Cancer 2003, 105, 158–164. [Google Scholar] [CrossRef]
- Shojaei, F.; Wu, X.; Zhong, C.; Yu, L.; Liang, X.H.; Yao, J.; Blanchard, D.; Bais, C.; Peale, F.V.; van Bruggen, N.; et al. Bv8 Regulates Myeloid-Cell-Dependent Tumour Angiogenesis. Nature 2007, 450, 825–831. [Google Scholar] [CrossRef]
- Shojaei, F.; Wu, X.; Malik, A.K.; Zhong, C.; Baldwin, M.E.; Schanz, S.; Fuh, G.; Gerber, H.-P.; Ferrara, N. Tumor Refractoriness to Anti-VEGF Treatment Is Mediated by CD11b+Gr1+ Myeloid Cells. Nat. Biotechnol. 2007, 25, 911–920. [Google Scholar] [CrossRef]
- Li, D.; Xie, K.; Ding, G.; Li, J.; Chen, K.; Li, H.; Qian, J.; Jiang, C.; Fang, J. Tumor Resistance to Anti-VEGF Therapy through up-Regulation of VEGF-C Expression. Cancer Lett. 2014, 346, 45–52. [Google Scholar] [CrossRef]
- Crawford, Y.; Kasman, I.; Yu, L.; Zhong, C.; Wu, X.; Modrusan, Z.; Kaminker, J.; Ferrara, N. PDGF-C Mediates the Angiogenic and Tumorigenic Properties of Fibroblasts Associated with Tumors Refractory to Anti-VEGF Treatment. Cancer Cell 2009, 15, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Casanovas, O.; Hicklin, D.J.; Bergers, G.; Hanahan, D. Drug Resistance by Evasion of Antiangiogenic Targeting of VEGF Signaling in Late-Stage Pancreatic Islet Tumors. Cancer Cell 2005, 8, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Xu, T.; Zheng, L.; Li, G. Angiogenesis Inhibitors for the Treatment of Ovarian Cancer: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Gynecol. Cancer 2018, 28, 903–914. [Google Scholar] [CrossRef]
- Guo, C.; Yan, C.; Qu, L.; Du, R.; Lin, J. The Efficacy and Toxicity of Angiogenesis Inhibitors for Ovarian Cancer: A Meta-Analysis of Randomized Controlled Trials. Arch. Gynecol. Obstet. 2021, 303, 285–311. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Chen, H.L. Bevacizumab in the Treatment of Ovarian Cancer: A Meta-Analysis from Four Phase III Randomized Controlled Trials. Arch. Gynecol. Obstet. 2013, 288, 655–666. [Google Scholar] [CrossRef]
- Zhou, M.; Yu, P.; Qu, X.; Liu, Y.; Zhang, J. Phase III Trials of Standard Chemotherapy with or without Bevacizumab for Ovarian Cancer: A Meta-Analysis. PLoS ONE 2013, 8, e81858. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhu, S.; Hong, C.; Cai, H. Angiogenesis Inhibitors for Patients with Ovarian Cancer: A Meta-Analysis of 12 Randomized Controlled Trials. Curr. Med. Res. Opin. 2016, 32, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Shen Wu, Y.; Shui, L.; Shen, D.; Chen, X. Bevacizumab Combined with Chemotherapy for Ovarian Cancer: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Oncotarget 2017, 8, 10703–10713. [Google Scholar]
- Jiang, Y.; Sun, X.; Kong, B.; Jiang, J. Antiangiogenesis Therapy in Ovarian Cancer Patients: An Updated Meta-Analysis for 15 Randomized Controlled Trials. Medicine 2018, 97, e11920. [Google Scholar] [CrossRef]
- Li, J.; Li, S.; Chen, R.; Yu, H.; Lu, X. The Prognostic Significance of Anti-Angiogenesis Therapy in Ovarian Cancer: A Meta-Analysis. J. Ovarian Res. 2015, 8, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchetti, C.; de Felice, F.; Palaia, I.; Musella, A.; di Donato, V.; Gasparri, M.L.; Musio, D.; Muzii, L.; Tombolini, V.; Panici, P.B. Efficacy and Toxicity of Bevacizumab in Recurrent Ovarian Disease: An Update Meta-Analysis on Phase III Trials. Oncotarget 2016, 7, 13221. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Zhou, L.; Chen, X.; Ba, Y. Addition of Bevacizumab to Chemotherapy in Patients with Ovarian Cancer: A Systematic Review and Meta-Analysis of Randomized Trials. Clin. Transl. Oncol. 2015, 17, 673–683. [Google Scholar] [CrossRef]
- Wang, T.S.; Lei, W.; Cui, W.; Wen, P.; Guo, H.F.; Ding, S.G.; Yang, Y.P.; Xu, Y.Q.; Lv, S.W.; Zhu, Y.L. A Meta-Analysis of Bevacizumab Combined with Chemotherapy in the Treatment of Ovarian Cancer. Indian J. Cancer 2014, 51 (Suppl. 3), e95–e98. [Google Scholar] [CrossRef] [PubMed]
- Matulonis, U.A.; Shapira-Frommer, R.; Santin, A.D.; Lisyanskaya, A.S.; Pignata, S.; Vergote, I.; Raspagliesi, F.; Sonke, G.S.; Birrer, M.; Provencher, D.M.; et al. Antitumor Activity and Safety of Pembrolizumab in Patients with Advanced Recurrent Ovarian Cancer: Results from the Phase II KEYNOTE-100 Study. Ann. Oncol. 2019, 30, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.R.; Dehbi, H.M.; Banerjee, S.; Lord, R.; Clamp, A.; Ledermann, J.A.; Nicum, S.; Lilleywhite, R.; Bowen, R.; Michael, A.; et al. A Phase II Randomised, Placebo-Controlled Trial of Low Dose (Metronomic) Cyclophosphamide and Nintedanib (BIBF1120) in Advanced Ovarian, Fallopian Tube or Primary Peritoneal Cancer. Gynecol. Oncol. 2020, 159, 692–698. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, W. The Efficacy and Safety of Angiogenesis Inhibitors for Recurrent Ovarian Cancer: A Meta-analysis. J. Ovarian Res. 2022, 15, 99. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Participants | Adults with confirmed ovarian cancer |
| Intervention | Angiogenesis-inhibitor therapy |
| Comparison | Drug regimens without angiogenesis inhibitors |
| Outcomes | PFS (hazard ratio, HR; confidence interval, 95% CI), OS (HR and 95% CI) and adverse effects (toxicity) |
| Study design | Randomized/controlled trials |
| Study (Reference/Name/Phase) | Drug | Subjects | Sample Size (E/C) | Angiogenesis Inhibitors Group Treatment | Control Group Treatment | Outcomes in Meta-Analysis |
|---|---|---|---|---|---|---|
| Aghajanian2015 (OCEANS/ NCT00434642) Phase III [26] | Bevacizumab | P-S R EOC/fallopian/primary peritoneal carcinoma ECOG performance status PS 0–1 | 242/242 | Cycles 1–6: gemcitabine (1000 mg/m2, days 1 and 8) + carboplatin (AUC 4, day 1) + bevacizumab (15 mg/kg on day 1, 6–10 cycles of 21 days) Cycles 10+: bevacizumab (15 mg/kg) | Cycles 1–6: gemcitabine (1000 mg/m2, days 1 and 8) and carboplatin (AUC4, day 1) + Placebo (15 mg/kg days 1, 6–10 cycles of 21 days) Cycles 10+: placebo (15 mg/kg) | PFS; OS; toxicity |
| Chekerov2018 (TRIAS/ NCT01047891) Phase II [27] | Sorafenib | P-R R EOC/fallopian/peritoneal carcinomas progressing during platinum therapy (platinum refractory) or ≤6 months after completing primary/secondary/ tertiary platinum-based therapy ECOG PS 0–2 | 85/89 | Cycles 1–6: topotecan (1–25 mg/m2 on days 1–5) + sorafenib (400 mg oral bi-daily on days 6–15, every 21 days) Cycles 6+: maintenance sorafenib for up to 1 year daily | Cycles 1–6: topotecan (1–25 mg/m2 on days 1–5) + placebo (bi-daily on days 6–15, every 21 days) Cycles 6+: maintenance Placebo for up to 1 year daily | PFS; OS; toxicity |
| Coleman2017 (GOG-0213/ NCT00565851) Phase III [28] | Bevacizumab | P-S R EOC/fallopian/primary peritoneal cancer GOG PS 0–2 | 337/337 | Cycles 1–6: paclitaxel (175 mg/m2)–carboplatin (AUC 5)) 3-weekly+ bevacizumab (15 mg/kg, 3-weekly) Cycles 6+: bevacizumab (15 mg/kg, 3-weekly) | Cycles 1–6: paclitaxel (175 mg/m2)–carboplatin (AUC 5) 3-weekly | PFS; OS; toxicity |
| Duska2020 (NCT01610206) Phase III [29] | Pazopanib | FIGO II-IV epithelial ovarian, fallopian tube or primary peritoneal carcinoma with less than 3 lines of prior chemotherapy ECOG PS 0–1 | 73/75 | Gemcitabine (1000 mg/m2 every week on days 1 and 8, every 21 days with pazopanib 800 mg daily | Gemcitabine (1000 mg/m2 every week on days 1 and 8, every 21 days | PFS; toxicity |
| duBois2016 (AGO-OVAR12/NCT 01015118) Phase III [30,31] | Nintedanib | Chemo-naive, FIGO IIB-IV EOC/fallopian/primary peritoneal cancer ECOG performance status 0–2 | 911/455 | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin (AUC5 or 6) + nintedanib (200 mg bi-daily, days 2–21), every 3 weeks followed by nintedanib maintenance | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin (AUC5 or 6) + placebo (200 mg, bi-daily, days 2–21, every 3 weeks), followed by placebo maintenance | PFS |
| Gore2019 (GOG-0241/ NCT01081262) Phase III [32] | Bevacizumab | Primary mEOC FIGO II–IV/ recurrence after stage I cancer | 24/26 | Paclitaxel (175 mg/m2) + carboplatin (AUC5/6) + bevacizumab (15 mg/kg, 3-weekly maintenance, 12 cycles). oxaliplatin (130 mg/m2) + capecitabine (850 mg/m2, bi-daily, days 1–14) + bevacizumab (15 mg/kg, 3-weekly maintenance, 12 cycles) | Paclitaxel (175 mg/m2) + carboplatin (AUC 5/6); Oxaliplatin (130 mg/m2) + capecitabine (850 mg/m2, bi-daily, days 1–14) | PFS; OS; toxicity |
| Gotlieb2012 (NCT00327444) Phase II [33] | Aflibercept | Platinum and Topotecan resistant and/or PLD-resistant cancer; Advanced EOC patients with recurrent malignant ascites ECOG Performance status 0–2 | 26/29 | Aflibercept (4 mg/kg, every 2 weeks) | Placebo (4 mg/kg, every 2 weeks) | OS; toxicity |
| Herzog2013 (NCT00791778) Phase II [34] | Sorafenib | FIGO III–IV EOC/primary peritoneal cancers who responded after standard first-line platinum/taxanes containing chemotherapy ECOG Performance status 0–1 | 123/123 | Sorafenib (400 mg bi-daily, every 12 h) | Placebo (400 mg bi-daily, every 12 h) | PFS; OS; toxicity |
| Karlan2012 (10 mg/kg) (NCT00479817) Phase II [35] | Trebananib (AMG 386) | FIGO II-IV recurrent EOC/ fallopian/primary peritoneal cancer ECOG Performance status 0–1 | 53/55 | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + AMG 386 (10 mg/kg, once a week) | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + placebo (10 mg/kg, once a week) | PFS; OS; toxicity |
| Karlan2012 (3 mg/kg) (NCT00479817) Phase II [35] | Trebananib (AMG 386) | FIGO II-IV recurrent EOC/ fallopian/primary peritoneal cancer ECOG Performance status 0–1 | 53/55 | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + AMG 386 (3 mg/kg, once a week) | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + placebo (3 mg/kg, once a week) | PFS; OS; toxicity |
| Kim2018 (East Asian Study/ NCT00866697) Phase III [36] | Pazopanib | Advanced EOC/fallopian/ primary peritoneal carcinoma | 73/72 | Pazopanib 800 mg daily for up to24 months | Placebo 800 mg daily or up to 24 months | PFS; OS |
| Ledermann2011 (NCT00710762) Phase II [37] | Nintedanib (BIBF 1120) | Advanced recurrent serous ovarian/fallopian/primary peritoneal cancer which responded to second-/third-/fourth-line chemotherapy ECOG Performance status 0–1 | 43/40 | Cycles 1–9: BIBF 1120 (250 mg, bi-daily, 28-day cycles) | Cycles 1–9: placebo (250 mg, bi-daily, 28-day cycles) | PFS; OS; toxicity |
| Ledermann2016 (ICON6/ NCT00532194) Phase III [38,39] | Cediranib | P-S R EOC/fallopian/primary peritoneal cancer after first-line platinum-based chemotherapy ECOG Performance status 0–1 | 164/118 | Platinum-based chemotherapy + cediranib (20 mg, daily) and then maintenance cediranib (20 mg, daily) alone | Platinum-based chemotherapy + placebo (20 mg, daily) then maintenance placebo (20 mg, daily) | PFS; OS; toxicity |
| Liu2019 (NCT01116648) Phase II [40] | Cediranib | P-S R high-grade serous/ endometrioid/deleterious germline BRCA1/2 mutation ovarian cancer | 46/44 | Olaparib (200 mg, bi-daily) + cediranib (30 mg daily) | Olaparib (400 mg, bi-daily) | PFS; OS; toxicity |
| Marth2017 (TRINOVA-2/ NCT01281254) Phase III [41] | Trebananib (AMG 386) | P-R R EOC/fallopian/primary peritoneal cancer ECOG Performance status 0–2 | 114/109 | Pegylated liposomal doxorubicin (50 mg/m2, every 4 weeks) + trebananib (15 mg/kg, every week) | Pegylated liposomal doxorubicin (50 mg/m2, every 4 weeks) + placebo (15 mg/kg, every week) | PFS; OS; toxicity |
| Monk2016 (TRINOVA-1/ NCT01204749) Phase III [42] | Trebananib (AMG 386) | Recurrent partially platinum-sensitive or—EOC/fallopian/ primary peritoneal cancer GOG Performance status 0–1 | 458/461 | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + trebananib (15 mg/ kg, every week) | Paclitaxel (80 mg/m2 once a week, 3 weeks on/1 week off) + placebo (15 mg/kg, every week) | PFS; OS; toxicity |
| Oza2015 (ICON7/ NCT00483782) Phase III [43] | Bevacizumab | FIGO I–IIA newly diagnosed high risk ovarian cancer/FIGO IIB–IV EOC/fallopian/primary peritoneal cancer ECOG Performance status 0–2 | 764/764 | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin AUC 5 or 6) every 3 weeks + bevacizumab (7.5 mg/kg, every 3 weeks) Cycles 7–18: Bev (7.5 mg/kg, every 3 weeks) | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin AUC 5 or 6) every 3 weeks | PFS; OS; toxicity |
| Pignata2021 (MITO16b/ NCT01802749) Phase II [44] | Bevacizumab | FIGO IIIB-IV recurrent ovarian cancer relapsing ≥ 6 months after last dose of platinum, in patients with bevacizumab during first line treatment ECOG Performance status 0–2 | 203/203 | Cycles 1–6: platinum-based-doublets paclitaxel–carboplatin/carboplatin–gemcitabine/carboplatin–pegylated liposomal doxorubicin + bevacizumab maintenance | Cycles 1–6: platinum-based doublets paclitaxel–carboplatin/carboplatin–gemcitabine/carboplatin–pegylated liposomal doxorubicin | PFS; OS; toxicity |
| Pignata2015 (MITO11/ NCT01644825) Phase II [45] | Pazopanib | Platinum-resistant/refractory EOC ECOG Performance status 0–1 | 37/37 | Paclitaxel (80 mg/m2 on days 1, 8, and 15, every 28 days) + pazopanib 800 mg daily | Paclitaxel (80 mg/m2 on days 1, 8 and 15 every, 28 days) | PFS; OS; toxicity |
| Pujade-Lauraine 2014 (AURELIA/ NCT00976911) Phase III [46] | Bevacizumab | P-R R EOC/fallopian/primary peritoneal cancer ECOG Performance status 0–2 | 182/179 | Cycle 1 to progression: pegylated liposomal doxorubicin (40 mg/m2, day 1 every 4 weeks) or paclitaxel (80 mg/m2, days 1, 8, 15, and 22, every 4 weeks); or topotecan (4 mg/m2, days 1, 8, and 15, every 4 weeks; or 1.25 mg/m2, days 1–5, every 3 weeks); + bevacizumab (10 mg/kg, every 2 weeks or 15 mg/kg, every 3 weeks) | Cycle 1 to progression: pegylated liposomal doxorubicin (40 mg/m2, day 1, every 4 weeks); paclitaxel (80 mg/m2 on days 1, 8, 15 and 22, every 4 weeks); or topotecan (4 mg/m2, days 1, 8, and 15, every 4 weeks; or 1.25 mg/m2, days 1–5, every 3 weeks); | PFS; OS; toxicity |
| Richardson2018 (NCT01468909) Phase II [47] | Pazopanib | Persistent or recurrent EOC/ fallopian/primary peritoneal cancer GOG Performance status 0–1 | 52/54 | Paclitaxel (80 mg/m2 on days 1, 8, and 15 every 28 days) + pazopanib 800 mg daily | Paclitaxel (80 mg/m2 on days 1, 8 and 15 every 28 days) + placebo 800 mg daily | PFS; OS; toxicity |
| Tewari2019 (PLm) (GOG-0218/ NCT00262847) Phase III [48,49] | Bevacizumab | Newly diagnosed EOC/ fallopian/primary peritoneal cancer | 625/625 | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin (AUC 6) + bevacizumab (15 mg/kg; cycle 2 +) every 21 days Cycles 7–22: placebo maintenance every 21 days | Cycles 1–6: paclitaxel (175 mg/ m2) + carboplatin (AUC6) + PL (cycle 2 +) every 21 days Cycles 7–22: placebo maintenance every 21 days | PFS; OS; toxicity |
| Tewari2019 (BEVm) (GOG-0218/ NCT00262847) Phase III [48,49] | Bevacizumab | Newly diagnosed EOC/ fallopian/primary peritoneal cancer | 623/625 | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin (AUC 6) + bevacizumab (15 mg/kg; cycle 2 +) every 21 days Cycles 7–22: bevacizumab maintenance (15 mg/kg) every 21 days | Cycles 1–6: paclitaxel (175 mg/m2) + carboplatin (AUC 6) Placebo (cycle 2+) every 21 days Cycles 7–22: placebo every 21 days | PFS; OS; toxicity |
| Vergote2018 (AGO-OVAR16/ NCT00866697) Phase III [50,51] | Pazopanib | Newly diagnosed advanced ovarian cancer | 472/468 | Pazopanib 800 mg daily for up to 24 months | Placebo 800 mg daily for up to 24 months | PFS; OS; toxicity |
| Vergote2019 (TRINOVA-3/NCT01493505) Phase III [52] | Trebananib (AMG 386) | FIGO III–IV EOC/fallopian/ primary peritoneal cancer ECOG Performance status 0–1 | 678/337 | Cycles 1–6: Pac (175 mg/m2)- carboplatin ((AUC 5/6) every 3 weeks) + trebananib (15 mg/kg) Cycles 6+: trebananib for up to 18 more months | Cycles 1–6: paclitaxel (175 mg/m2)–carboplatin ((AUC5/6) every 3 weeks) + placebo (15 mg/kg) Cycles 6+: placebo for up to 18 more months | PFS; OS; toxicity |
| Study | Line | Size | Arms | PFS | OS | ||
|---|---|---|---|---|---|---|---|
| Median (in Months) | Hazard Ratio (95% CI) | Median (in Months) | Hazard Ratio (95% CI) | ||||
| Aghajanian 2015 [26] | P-S R | 484 | GC + Pl + bevacizumab(m) GC + PL | 12.4 8.4 | 0.484 (0.388–0.605) | 33.6 32.9 | 0.95 (0.77–1.77) |
| Chekerov 2018 [27] | P-R R | 174 | Topotecan + sorafenib + sorafenib(m) PL + PL(m) | 6.7 4.4 | 0.60 (0.43–0.83) | 17.1 10.1 | 0.65 (0.45–0.93) |
| Coleman 2017 [28] | P-S R | 674 | GC + PL + bevacizumab(m) TC | 13.8 10.4 | 0.628 (0.534–0.739) | 42.2 37.3 | 0.829 (0.683–1.005) |
| Du Bois 2016 [30] | F | 1366 | TC +nintedanib + nintedanib(m) TC + PL + PL(m) | 17.2 16.6 | 0.84 (0.72–0.98) | 34 32.8 | 0.99 (0.77–1.27) |
| Duska 2020 [29] | R | 148 | Pazopanib PL | 5.3 2.9 | 1.50 (0.76–2.94) | NA | NA |
| Gore 2019 [32] | F or R | 50 | TC/Oxal–Cape + Bev TC/Oxal–Cape | 18.1 8.8 | 0.80 (0.41–1.57) | 27.7 32.7 | 1.04 (0.51–2.10) |
| Gotlieb 2012 [33] | R | 55 | Aflibercept PL | 6.3 w 7.3 w | NA | 12.9 w 16.0 w | 1.02 (0.56–1.86) |
| Herzog 2013 [34] | M | 246 | Sorafenib PL | 12.7 15.7 | 1.09 (0.72–1.63) | NA | 1.48 (0.69–3.23) |
| Karlan 2012 [35] (10 mg/kg) | R | 108 | Pac + trebananib Pac + PL | 7.2 4.6 | 0.76 (0.49–1.18) | 22.5 20.9 | 0.60 (0.34–1.06) |
| Karlan 2012 [35] (3 mg/kg) | R | 108 | Pac + trebananib Pac + PL | 5.7 4.6 | 0.75 (0.48–1.17) | 20.4 20.9 | 0.77 (0.45–1.31) |
| Kim 2018 [36] | M | 145 | Pazopanib PL | 18.1 18.1 | 0.984 (0.596–1.626) | NA | 0.811 (0.376–1.751) |
| Ledermann 2016 [38,39] | P-S R | 282 | TC or GC or Carbo + cediranib + cediranib(m) TC or GC or Carbo + PL +PL(m) | 11.0 8.7 | 0.56 (0.44–0.72) | 27.3 19.9 | 0.85 (0.66–1.10) |
| Ledermann 2011 [37] | M | 83 | Nintedanib PL | NA | 0.65 (0.41–1.02) | NA | 0.84 (0.51–1.39) |
| Liu 2019 [40] | P-S R | 90 | Olaparib + cediranib Olaparib | 16.5 8.2 | 0.5 (0.3–0.83) | 44.2 33.3 | 0.64 (0.36–1.11) |
| Marth 2017 [41] | P-S R | 223 | PLD + trebananib PLD + PL | 7.6 7.2 | 0.92 (0.68–1.24) | 19.4 17.0 | 0.94 (0.64–1.39) |
| Monk 2016 [42] | R | 919 | Pac + trebananib Pac + PL | 7.2 5.4 | 0.66 (0.57–0.77) | 19.3 18.3 | 0.95 (0.81–1.11) |
| Oza 2015 [43] | F | 1528 | TC + Bev + Bev(m) TC | 19.9 17.5 | 0.93 (0.83–1.05) | 58.0 58.6 | 0.99 (0.85–1.14) |
| Pignata 2015 [45] | P-R R | 73 | Pac + pazopanib Pac + PL | 6.35 3.49 | 0.42 (0.25–0.69) | 19.1 13.7 | 0.60 (0.32–1.13) |
| Pignata 2021 [44] | P-S R | 406 | TC/GC/Carbo–PLD + Bev TC/GC/Carbo–PLD | 11.8 8.8 | 0.51 (0.41–0.64) | 26.7 27.1 | 1.00 (0.73–1.39) |
| Pujade-Lauraine 2014 [46] | P-R R | 361 | PLD/Pac/TOP + Bev PLD/Pac/TOP | 6.7 3.4 | 0.48 (0.38–0.60) | 16.6 13.3 | 0.85 (0.66–1.08) |
| Richardson 2018 [47] | R | 106 | Paclitaxel + pazopanib Paclitaxel + PL | 7.5 6.2 | 0.84 (0.57–1.22) | 20.7 23.3 | 1.04 (0.60–1.79) |
| Tewari 2019 [48] (PLm) | F | 1250 | TC + bevacizumab + PL(m) TC + PL | 11.2 10.3 | 0.908 (0.795–1.040) | 40.8 41.1 | 1.06 (0.94–1.20) |
| Tewari 2019 [48] (BEV-m) | F | 1248 | TC + bevacizumab + bevacizumab(m) TC + PL | 14.1 10.3 | 0.717 (0.625–0.824) | 43.4 41.1 | 0.96 (0.85–1.09) |
| Vergote 2018 [50] | F | 940 | Pazopanib PL | 17.9 12.3 | 0.77 (0.64–0.91) | 59.1 64.0 | 0.96 (0.805–1.145) |
| Vergote 2019 [52] | F | 1015 | TC + trebananib + trebananib(m) TC + placebo + placebo (m) | 15.9 15.0 | 0.93 (0.79–1.09) | 46.6 43.6 | 0.99 (0.79–1.25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simion, L.; Rotaru, V.; Cirimbei, C.; Stefan, D.-C.; Gherghe, M.; Ionescu, S.; Tanase, B.C.; Luca, D.C.; Gales, L.N.; Chitoran, E. Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 1040. https://doi.org/10.3390/diagnostics13061040
Simion L, Rotaru V, Cirimbei C, Stefan D-C, Gherghe M, Ionescu S, Tanase BC, Luca DC, Gales LN, Chitoran E. Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(6):1040. https://doi.org/10.3390/diagnostics13061040
Chicago/Turabian StyleSimion, Laurentiu, Vlad Rotaru, Ciprian Cirimbei, Daniela-Cristina Stefan, Mirela Gherghe, Sinziana Ionescu, Bogdan Cosmin Tanase, Dan Cristian Luca, Laurentia Nicoleta Gales, and Elena Chitoran. 2023. "Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 6: 1040. https://doi.org/10.3390/diagnostics13061040
APA StyleSimion, L., Rotaru, V., Cirimbei, C., Stefan, D. -C., Gherghe, M., Ionescu, S., Tanase, B. C., Luca, D. C., Gales, L. N., & Chitoran, E. (2023). Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis. Diagnostics, 13(6), 1040. https://doi.org/10.3390/diagnostics13061040