
Systematic Review on Diagnostic Reference Levels for Computed Tomography Examinations in Radiation Therapy Planning
 ,
,  ,
, 
Abstract
:1. Introduction
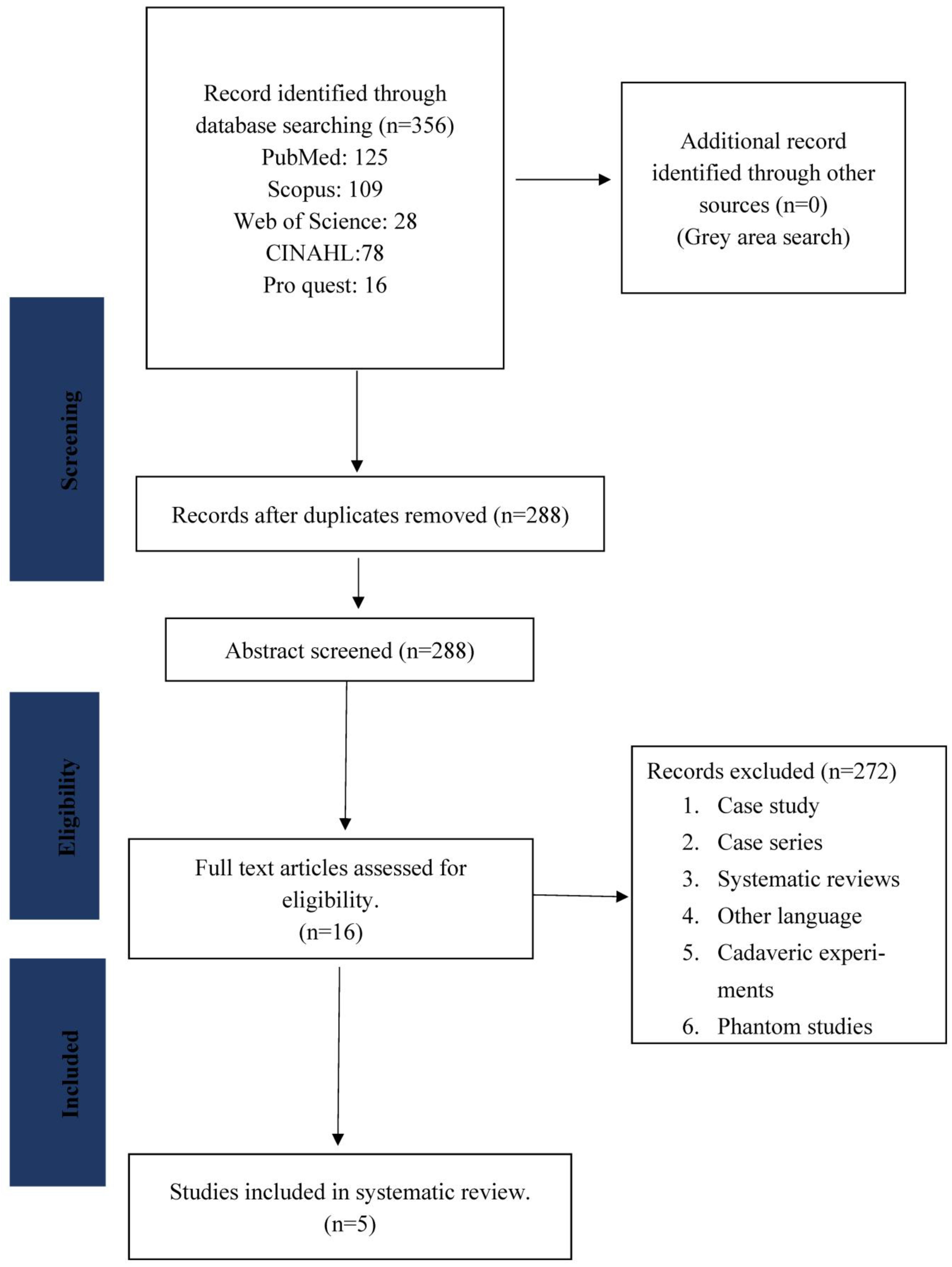
2. Survey Methodology
2.1. Keyword Builds and Search Strategy
2.2. Type of Study
2.3. Data Collection and Analysis
2.4. Removing Duplicates
2.5. Level 1: Article Screening
2.6. Level 2: Abstract Review
2.7. Level 3: Full-Text Review
2.8. Level 4: Reference List Search
2.9. Data Extraction and Management
2.9.1. General Information
2.9.2. Participant-Related Data
2.10. Quality Assessment
3. Results
4. Characteristics of Included Studies
- Type of the study design (phantom, human, or both).
- Whether DRLs were established on third quartile or mean.
- Countries are indicating where the studies were conducted.
- Sample size reported in several scanners or patients or hospitals.
- DRLs in terms of radiation dose indices: volume computed tomography dose index (CTDIvol), weighted computed tomography dose index (CTDIw), dose length product (DLP), effective dose (ED), specific size dose estimate (SSDE).
- Whether the articles reported that the scanners had undergone prior quality control (QC) tests.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goske, M.J. Diagnostic reference ranges and the American College of Radiology Dose Index Registry: The pediatric experience. Pediatr. Radiol. 2014, 44, 506–510. [Google Scholar] [CrossRef]
- Božanić, A.; Šegota, D.; Debeljuh, D.D.; Kolacio, M.; Radojčić, S.; Ružić, K.; Budanec, M.; Kasabašić, M.; Hrepić, D.; Zujić, P.V.; et al. National reference levels of CT procedures dedicated for treatment planning in radiation oncology. Phys. Med. 2022, 96, 123–129. [Google Scholar] [CrossRef]
- Aroua, A.; Samara, E.-T.; Bochud, F.O.; Meuli, R.; Verdun, F.R. Exposure of the Swiss population to computed tomography. BMC Med. Imaging 2013, 13, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrimpton, P.C.; Hillier, M.C.; Lewis, M.A.; Dunn, M. National survey of doses from CT in the UK: 2003. Br. J. Radiol. 2006, 79, 968–980. [Google Scholar] [CrossRef] [PubMed]
- Bernier, M.-O.; Baysson, H.; Pearce, M.; Moissonnier, M.; Cardis, E.; Hauptmann, M.; Struelens, L.; Dabin, J.; Johansen, C.; Journy, N.; et al. Cohort Profile: The EPI-CT study: A European pooled epidemiological study to quantify the risk of radiation-induced cancer from paediatric CT. Leuk. Res. 2018, 48, 379–381g. [Google Scholar] [CrossRef]
- Brenner, D.J.; Elliston, C.D.; Hall, E.J.; Berdon, W.E. Estimated Risks of Radiation-Induced Fatal Cancer from Pediatric CT. AJR. 2001. Available online: www.ajronline.org (accessed on 23 January 2023).
- United Nations Report of the United Nations Scientific Committee on the Effects of Atomic Radiation. Sixty-Fifth Session (11–14 June 2018). Available online: https://www.unscear.org/docs/GAreports/2018/A-73-46-e-V1804724.pdf (accessed on 2 February 2023).
- Martin, C.; Kron, T.; Vassileva, J.; Wood, T.; Joyce, C.; Ung, N.; Small, W.; Gros, S.; Roussakis, Y.; Plazas, M.; et al. An international survey of imaging practices in radiotherapy. Phys. Med. 2021, 90, 53–65. [Google Scholar] [CrossRef]
- Introduction of Image Guided Radiotherapy into Clinical Practice. Available online: http://www.iaea.org/Publications/index.html (accessed on 25 January 2023).
- Mackie, T.R.; Kapatoes, J.; Ruchala, K.; Lu, W.; Wu, C.; Olivera, G.; Forrest, L.; Tomé, W.; Welsh, J.; Jeraj, R.; et al. Image guidance for precise conformal radiotherapy. Int. J. Radiat. Oncol. 2003, 56, 89–105. [Google Scholar] [CrossRef]
- Vanõ, E.; Miller, D.; Martin, C.; Rehani, M.; Kang, K.; Rosenstein, M.; Ortiz-Lopez, P.; Mattsson, S.; Padovani, R.; Rogers, A. Diagnostic Reference Levels in Medical Imaging. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef] [PubMed]
- Roch, P.; Célier, D.; Dessaud, C.; Etard, C. Using diagnostic reference levels to evaluate the improvement of patient dose optimisation and the influence of recent technologies in radiography and computed tomography. Eur. J. Radiol. 2018, 98, 68–74. [Google Scholar] [CrossRef]
- Zalokar, N.; Žager Marciuš, V.; Mekiš, N. Establishment of national diagnostic reference levels for radiotherapy computed tomography sim-ulation procedures in Slovenia. Eur. J. Radiol. 2020, 127, 108979. [Google Scholar] [CrossRef] [PubMed]
- Vassileva, J.; Rehani, M. Diagnostic reference levels. AJR Am. J. Roentgenol. 2015, 204, W1–W3. [Google Scholar] [CrossRef]
- Nam, S.; Park, H.; Kwon, S.; Cho, P.K.; Yoon, Y.; Yoon, S.W.; Kim, G. Updated National Diagnostic Reference Levels and Achievable Doses for CT Protocols: A National Survey of Korean Hospitals. Tomography 2022, 8, 2450–2459. [Google Scholar] [CrossRef]
- Clarke, R.H.; Dunster, C.H.J.; KGuskova, L.A.; Jacobi, M.W.; Li, N.D.; Liniecki, T.J. Annals of the ICRP Published on behalf of the lnternational Commission on Radiological Protection Members of the Main Commission of the ICRP. Available online: https://www.icrp.org/docs/The%20History%20of%20ICRP%20and%20the%20Evolution%20of%20its%20Policies.pdf (accessed on 2 February 2023).
- Categories in the Iaea Safety Series. Available online: https://www-pub.iaea.org/MTCD/publications/PDF/Pub1227_web.pdf (accessed on 2 February 2023).
- The 2007 Recommendations of the International Commission on Radiological Protection. Available online: http://www.elsevier.com/wps/find/bookdescription.cws_home/713998/description#description/ (accessed on 5 December 2022).
- Strauss, K.J. Developing patient-specific dose protocols for a CT scanner and exam using diagnostic reference levels. Pediatr. Radiol. 2014, 44, 479–488. [Google Scholar] [CrossRef]
- Perić, J.; Mekiš, N.; Žontar, D. Establishment of typical adult CT dose indicators for PET-CT scans in Slovenia. J. Radiol. Prot. 2021, 41, 552–563. [Google Scholar] [CrossRef]
- Zamani, H.; Parach, A.; Razavi, S.; Shabani, M.; Ataei, G.; Zare, M. Estimating the radiation surface dose and measuring the dose area product to provide the diagnostic reference level in panoramic radiography. Intern. J. Radiat. Res. 2021, 19, 963–970. [Google Scholar] [CrossRef]
- Garba, I.; Zarb, F.; McEntee, M.; Fabri, S. Computed tomography diagnostic reference levels for adult brain, chest and abdominal examinations: A systematic review. Radiography 2021, 27, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Elmagarmid, A.; Fedorowicz, Z.; Hammady, H.; Ilyas, I.; Khabsa, M.; Ouzzani, M. Rayyan: A systematic reviews web app for exploring and filtering searches for eligible studies for Cochrane Reviews. In Abstracts of the 22nd Cochrane Colloquium; John Wiley & Sons: Hoboken, NJ, USA, 2014; p. 9. [Google Scholar]
- Clerkin, C.; Brennan, S.; Mullaney, L.M. Establishment of national diagnostic reference levels (DRLs) for radiotherapy localisation computer tomography of the head and neck. Rep. Pract. Oncol. Radiother. 2018, 23, 407–412. [Google Scholar] [CrossRef]
- Connor, S.O.; Mc Ardle, O.; Mullaney, L. Establishment of national diagnostic reference levels for breast cancer CT protocols in radiation therapy. Br. J. Radiol. 2016, 89, 20160428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toroi, P.; Kaijaluoto, S.; Bly, R. Patient exposure levels in radiotherapy CT simulations in Finland. Radiat. Prot. Dosim. 2014, 167, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Alhailiy, A.B.; Brennan, P.C.; McEntee, M.F.; Kench, P.L.; Ryan, E.A. Diagnostic Reference Levels in Cardiac Computed Tomography Angiography: A Systematic Review. Radiat. Prot. Dosim. 2017, 178, 63–72. [Google Scholar] [CrossRef]
- Priyanka; Kadavigere, R.; Sukumar, S.; Pendem, S. Diagnostic reference levels for computed tomography examinations in pediatric population—A systematic review. J. Cancer Res. Ther. 2021, 17, 845–852. [Google Scholar] [PubMed]
- Sanderud, A.; England, A.; Hogg, P.; Fosså, K.; Svensson, S.; Johansen, S. Radiation dose differences between thoracic radiotherapy planning CT and thoracic diagnostic CT scans. Radiography 2016, 22, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Cody, D.D.; Dillon, C.M.; Fisher, T.S.; Liu, X.; McNitt-Gray, M.F.; Patel, V. AAPM Medical Physics Practice Guideline 1.b: CT protocol management and review practice guideline. J. Appl. Clin. Med. Phys. 2021, 22, 4–10. [Google Scholar] [CrossRef]
- Sampathila, N.; Chadaga, K.; Goswami, N.; Chadaga, R.P.; Pandya, M.; Prabhu, S.; Bairy, M.G.; Katta, S.S.; Bhat, D.; Upadya, S.P. Customized Deep Learning Classifier for Detection of Acute Lymphoblastic Leukemia Using Blood Smear Images. Healthcare 2022, 10, 1812. [Google Scholar] [CrossRef] [PubMed]
- Micucci, M.; Iula, A. Recent Advances in Machine Learning Applied to Ultrasound Imaging. Electronics 2022, 11, 1800. [Google Scholar] [CrossRef]
- Acharya, V.; Dhiman, G.; Prakasha, K.; Bahadur, P.; Choraria, A.; Sushobhitha, M.; Sowjanya, J.; Prabhu, S.; Chadaga, K.; Viriyasitavat, W.; et al. AI-Assisted Tuberculosis Detection and Classification from Chest X-Rays Using a Deep Learning Normalization-Free Network Model. Comput. Intell. Neurosci. 2022, 2022, 2399428. [Google Scholar] [CrossRef]
- Krishnadas, P.; Chadaga, K.; Sampathila, N.; Rao, S.; Swathi, K.S.; Prabhu, S. Classification of Malaria Using Object Detection Models. Informatics 2022, 9, 76. [Google Scholar] [CrossRef]
- Li, H.; Lee, C.H.; Chia, D.; Lin, Z.; Huang, W.; Tan, C.H. Machine Learning in Prostate MRI for Prostate Cancer: Current Status and Future Opportunities. Diagnostics 2022, 12, 289. [Google Scholar] [CrossRef]
- Alrehily, F. Diagnostic Reference Levels of Radiographic and Ct Examinations in Saudi Arabia: A Systematic Review. Radiat. Prot. Dosim. 2022, 198, 1451–1461. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Database | Number of Studies | Total |
|---|---|---|
| PubMed | 125 | 356 |
| Scopus | 109 | |
| Web of Science | 28 | |
| FINAL | 78 | |
| ProQuest | 16 |
| Sl. No. | Search |
|---|---|
| 1 | “Reference level” OR “Diagnostic reference levels” |
| 2 | “CT scan” OR “Computed Tomography” OR “CAT scan” OR “computed axial tomography” |
| 3 | “Radiotherapy Dosage” OR “Radiotherapy” |
| No. | Study | Year | Country | Design | Sample | Dose Indices | DRLs | QC | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Celine et al. [24] | 2018 | Ireland | Prospective | 25 | CTDIvol and DLP | 75th percentile | Yes | M |
| 2 | Nika et al. [13] | 2020 | Slovenia | Retrospective | 1631 | CTDIvol and DLP | 3rd quartile | Yes | M |
| 3 | Sean et al. [25] | 2016 | Ireland | Prospective | 60 | CTDIvol and DLP | 3rd quartile | yes | M |
| 4 | Toroi et al. [26] | 2014 | Finland | Prospective | 13 hospitals | CTDIvol | 3rd quartile | Yes | M |
| 5 | Alhailiy et al. [27] | 2018 | Saudi Arabia | Retrospective | 197 | CTDIvol and DLP | 75, median and 25th percentile | Yes | M |
| Articles | Year | CTDIvol (mGy) | DLP (mGy.cm) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Head and Neck | Breast | Thorax | Abdomen | Head and Neck | Breast | Thorax | Abdomen | ||
| Celine et al. [24] | 2018 | 21 | ---- | ---- | ---- | 882m | ---- | ---- | ---- |
| Nika [13] | 2020 | (n = 278) 16.9 | (n = 298) 11.2 | (n = 289) 19.2 | (n = 128) 18.2 | (n = 278) 969.2 | (n = 298) 606.6 | (n = 289) 832.4 | (n = 128) 1116.2 |
| Sean et al. [25] | 2016 | ---- | 26 | ---- | ---- | ---- | 732 | ---- | ---- |
| Toroi et al. [26] | 2014 | 29 | 24 | 13 (whole brain) | ---- | ---- | ---- | ----- | ---- |
| Article | Year | Scan Type | CTDIvol | DLP | ||||
|---|---|---|---|---|---|---|---|---|
| 75th | Median | 25th | 75th | Median | 25th | |||
| Alhailiy et al. [27] | 2018 | Mixed models | 43 | 37 | 27 | 808 | 554.5 | 359 |
| PGM | 29 | 24 | 19 | 393 | 343 | 313 | ||
| RGM | 62 | 46 | 40 | 1057 | 808 | 605 | ||
| CS test | 5.8 | 4 | 3.7 | 69 | 8 | 46 | ||
| Study | CTDIvol (mGy) | DLP (mGy.cm) | CS (mGy.cm) |
|---|---|---|---|
| Saudi Arabia | 43 | 808 | 69 |
| Switzerland (2010) | 50 | 1000 | 150 |
| Japan (2012) | - | 1510 | - |
| Netherlands (2013) | - | 671 | - |
| Italy (2014) | 61 | 1280 | 131 |
| France (2014) | (PGM) 26 (RGM) 44 | 370 870 | - |
| - | |||
| Iran (2016) | 66.5 | 1073 | 187 |
| Siemens | Acquisition Type | Voltage (kV) | Reference (mAs) | Collimation (n × mm) | AEC | Rotation Time | Pitch | Slice Thickness | Kernel |
|---|---|---|---|---|---|---|---|---|---|
| HEAD | Helical | 120 | 370 | 20 × 0.6 | On | 1 | 0.55 | 3 | H30s |
| Head and neck | Helical | 120 | 165 | 16 × 1.1 | On | 1 | 0.8 | 2 | B31s |
| Breast | Helical | 120 | 140 | 16 × 1.2 | On | 0.5 | 1 | 3 | B31f |
| Thorax | Helical | 120 | 110 | 16 × 1.2 | On | 0.5 | 1.2 | 3 | B31f |
| Abdomen | Helical | 120 | 180 | 16 × 1.2 | On | 0.5 | 0.6 | 3 | B30f |
| Pelvis | Helical | 120 | 210 | 16 × 1.2 | On | 0.5 | 0.8 | 3 | B30f |
| Spine | Helical | 120 | 330 | 16 × 1.2 | On | 1 | 0.8 | 3 | B30s |
| Siemens | Acquisition Type | Voltage (kV) | Reference (mAs) | Collimation (N × mm) | AEC | Rotation Time | Pitch | Slice Thickness | Kernel |
|---|---|---|---|---|---|---|---|---|---|
| HEAD | Helical | 120 | 350 | 16 × 1.5 | Off | 0.75 | 0.93 | 3 | UB |
| Head and neck | Helical | 120 | 300 | 16 × 0.75 | On | 1 | 0.94 | 2 | A |
| Breast | Helical | 120 | 250 | 16 × 1.5 | On | 0.75 | 0.81 | 3 | C |
| Thorax | Helical | 120 | 300 | 16 × 1.5 | On | 0.75 | 0.81 | 3 | B |
| Abdomen | Helical | 120 | 300 | 16 × 1.5 | On | 0.75 | 0.81 | 3 | B |
| Pelvis | Helical | 120 | 200 | 16 × v1.5 | On | 0.75 | 0.68 | 3 | A |
| Spine | Helical | 120 | 250 | 16 × 1.5 | On | 1 | 0.98 | 3 | A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, S.; Sharan, K.; Sukumar, S.; Chandraguthi, S.G.; Nisha Dsouza, R.; David, L.R.; Ravichandran, S.; Uzun, B.; Kadavigere, R.; Uzun Ozsahin, D. Systematic Review on Diagnostic Reference Levels for Computed Tomography Examinations in Radiation Therapy Planning. Diagnostics 2023, 13, 1072. https://doi.org/10.3390/diagnostics13061072
Rao S, Sharan K, Sukumar S, Chandraguthi SG, Nisha Dsouza R, David LR, Ravichandran S, Uzun B, Kadavigere R, Uzun Ozsahin D. Systematic Review on Diagnostic Reference Levels for Computed Tomography Examinations in Radiation Therapy Planning. Diagnostics. 2023; 13(6):1072. https://doi.org/10.3390/diagnostics13061072
Chicago/Turabian StyleRao, Shreekripa, Krishna Sharan, Suresh Sukumar, Srinidhi Gururajarao Chandraguthi, Rechal Nisha Dsouza, Leena R. David, Sneha Ravichandran, Berna Uzun, Rajagopal Kadavigere, and Dilber Uzun Ozsahin. 2023. "Systematic Review on Diagnostic Reference Levels for Computed Tomography Examinations in Radiation Therapy Planning" Diagnostics 13, no. 6: 1072. https://doi.org/10.3390/diagnostics13061072
APA StyleRao, S., Sharan, K., Sukumar, S., Chandraguthi, S. G., Nisha Dsouza, R., David, L. R., Ravichandran, S., Uzun, B., Kadavigere, R., & Uzun Ozsahin, D. (2023). Systematic Review on Diagnostic Reference Levels for Computed Tomography Examinations in Radiation Therapy Planning. Diagnostics, 13(6), 1072. https://doi.org/10.3390/diagnostics13061072