


Diaphragm Ultrasound in Critically Ill Patients on Mechanical Ventilation—Evolving Concepts
Abstract
:1. Introduction
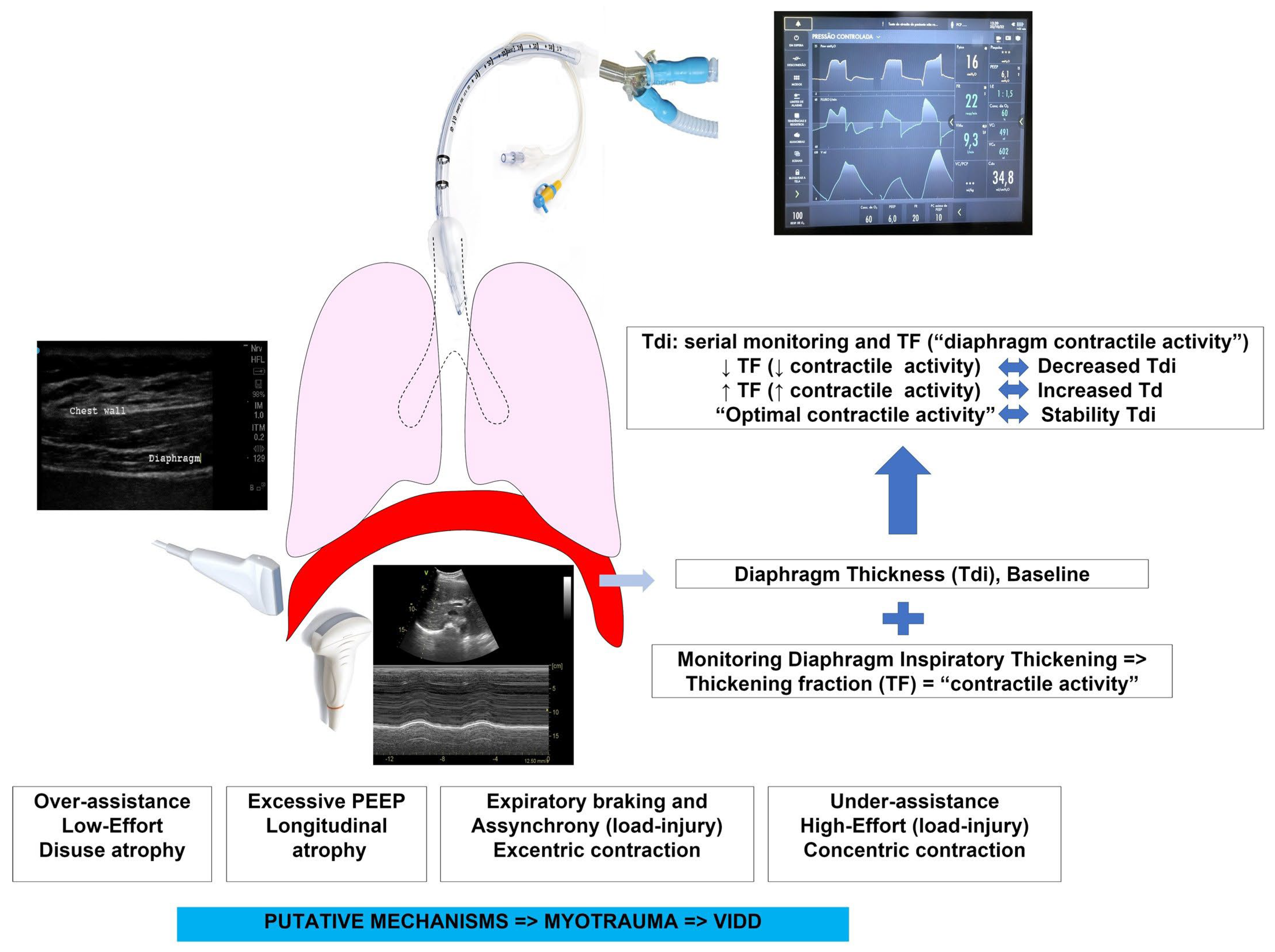
2. Diaphragm Myotrauma-Mechanisms
- Over-assistance myotrauma (disuse atrophy) represents the effect of excessive respiratory support and reduced respiratory drive/effort, resulting in disuse atrophy and weakness. It is the best documented form of myotrauma, in both experimental studies [30,31] and clinical studies reporting histological [24,32,33], functional [7], and imaging evidence of disuse atrophy [23,34,35,36]. It is important to emphasize that disuse atrophy can occur even in assisted ventilation modes [37].
- Under-assistance myotrauma (load-induced, concentric contraction) is a recognized form of muscle injury that occurs when ventilatory support is insufficient or unable to reduce the load on the diaphragm during increased respiratory drive (load-induced diaphragm injury). The persistence of high levels of respiratory efforts during under-assistance results in high muscle tension during concentric contraction [23,38]. In experimental models, the diaphragmatic injury is characterized by an inflammatory infiltration and the disruption of sarcomere and sarcolemma.
- Eccentric myotrauma (load-induced, eccentric contraction) occurs when there is contractile activity of the diaphragm during fiber lengthening instead of shortening. Eccentric contraction is observed in the expiratory phases of ventilation: (1) when the diaphragm exerts an expiratory brake to preserve the end-expiratory lung volume [39]; (2) in some forms of asynchrony (reverse triggering, early cycling, ineffective effort) [40,41,42].
- Expiratory myotrauma—in experimental models, it was observed that the use of high PEEP reduces the final expiratory length of the diaphragm and can cause loss of sarcomeres, resulting in longitudinal atrophy with impairment of the length-tension ratio of the diaphragm [43].
3. Diaphragm Dysfunction-Recognition
4. Diaphragm Ultrasound-DUS
4.1. Ultrasound of Diaphragm–Brief Review of the Technique
- -
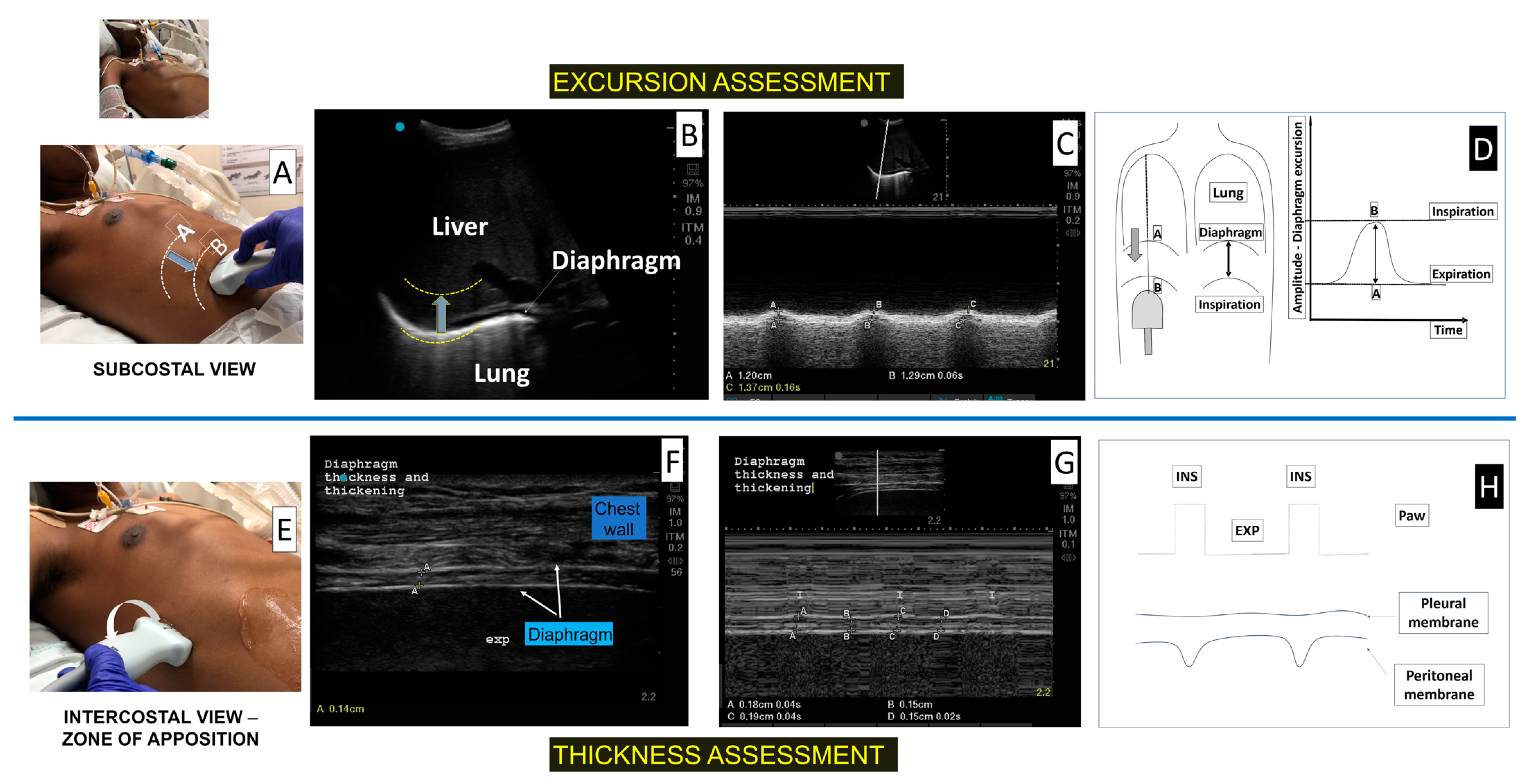
- In the subcostal region, the diaphragm is seen as a deep curved structure that separates the thorax from the abdomen;
- -
- In the mid-axillary intercostal region, in the zone of apposition (ZA), the diaphragm is identified as a three-layer structure; a hypoechoic inner muscle layer surrounded by two hyperechoic outer membranes (the peritoneum and pleura).
4.2. Diaphragm Ultrasound in Respiratory Muscle Monitoring in Critically Ill Patients
4.2.1. To Diagnose Diaphragmatic Dysfunction
4.2.2. Ultrasound of Diaphragm to Monitor Diaphragm Atrophy
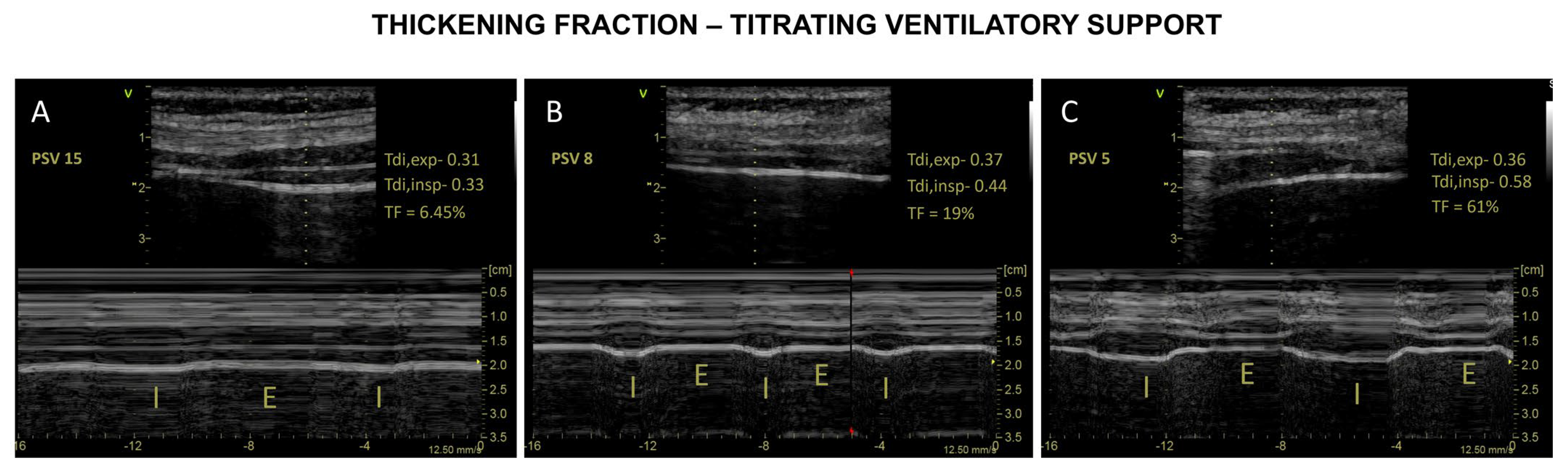
4.2.3. DUS to Monitor Effort–Diaphragm Protective Ventilation
5. Patient–Ventilator Asynchrony (PVA)
6. Role of Ultrasound of the Diaphragm in the Assessment of Weaning
- -
- To identify patients at high risk of weaning failure, DUS is performed before SBT.
- -
- To predict the weaning outcome or to diagnose the cause of weaning failure, DUS is best performed after initiation and/or completion of an SBT.
7. Novel Techniques and Future Developments for Functional Imaging and Quantification of Tissue Properties
7.1. Tissue Doppler Imaging
7.2. Speckle Tracking Ultrasound (STUS)
7.3. Shear Wave Elastography
8. Limitations
9. Future Directions
- -
- Histological findings of the muscle,
- -
- Interaction with other respiratory muscles,
- -
- Reference tools for PVA detection, and
- -
- Baseline measures of respiratory effort (such as work of breathing, PTP) and fatigue (such as TTI and relaxation rate).
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tremblay, L.N.; Slutsky, A.S. Ventilator-induced lung injury: From the bench to the bedside. Intensive Care Med. 2006, 32, 24–33. [Google Scholar] [CrossRef]
- Bates, J.H.; Smith, B.J. Ventilator-induced lung injury and lung mechanics. Ann. Transl. Med. 2018, 6, 378. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Goligher, E.C.; Brochard, L.J.; Reid, W.D.; Fan, E.; Saarela, O.; Slutsky, A.S.; Kavanagh, B.P.; Rubenfeld, G.D.; Ferguson, N.D. Diaphragmatic myotrauma: A mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respir. Med. 2019, 7, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T.; Petrof, B.J. Ventilator-induced diaphragmatic dysfunction. Am. J. Respir. Crit. Care Med. 2004, 169, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Petrof, B.J.; Jaber, S.; Matecki, S. Ventilator-induced diaphragmatic dysfunction. Curr. Opin. Crit. Care 2010, 16, 19–25. [Google Scholar] [CrossRef]
- Jaber, S.; Petrof, B.J.; Jung, B.; Chanques, G.; Berthet, J.P.; Rabuel, C.; Bouyabrine, H.; Courouble, P.; Koechlin-Ramonatxo, C.; Sebbane, M.; et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am. J. Respir. Crit. Care Med. 2011, 183, 364–371. [Google Scholar] [CrossRef]
- Demoule, A.; Jung, B.; Prodanovic, H.; Molinari, N.; Chanques, G.; Coirault, C.; Matecki, S.; Duguet, A.; Similowski, T.; Jaber, S. Diaphragm dysfunction on admission to the intensive care unit. Prevalence, risk factors, and prognostic impact—A prospective study. Am. J. Respir. Crit. Care Med. 2013, 188, 213–219. [Google Scholar] [CrossRef]
- Jung, B.; Moury, P.H.; Mahul, M.; de Jong, A.; Galia, F.; Prades, A.; Albaladejo, P.; Chanques, G.; Molinari, N.; Jaber, S. Diaphragmatic dysfunction in patients with ICU-acquired weakness and its impact on extubation failure. Intensive Care Med. 2016, 42, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Dubé, B.P.; Mayaux, J.; Delemazure, J.; Reuter, D.; Brochard, L.; Similowski, T.; Demoule, A. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am. J. Respir. Crit. Care Med. 2017, 195, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.Y.; Suh, H.J.; Hong, S.-B.; Koh, Y.; Lim, C.-M. Diaphragm dysfunction assessed by ultrasonography: Influence on weaning from mechanical ventilation. Crit. Care Med. 2011, 39, 2627–2630. [Google Scholar] [CrossRef]
- Demoule, A.; Molinari, N.; Jung, B.; Prodanovic, H.; Chanques, G.; Matecki, S.; Mayaux, J.; Similowski, T.; Jaber, S. Patterns of diaphragm function in critically ill patients receiving prolonged mechanical ventilation: A prospective longitudinal study. Ann. Intensive Care 2016, 6, 75. [Google Scholar] [CrossRef] [Green Version]
- Jung, B.; Nougaret, S.; Conseil, M.; Coisel, Y.; Futier, E.; Chanques, G.; Molinari, N.; Lacampagne, A.; Matecki, S.; Jaber, S. Sepsis is associated with a preferential diaphragmatic atrophy: A critically ill patient study using tridimensional computed tomography. Anesthesiology 2014, 120, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- Sassoon, C.S.; Zhu, E.; Fang, L.; Ramar, K.; Jiao, G.Y.; Caiozzo, V.J. Interactive effects of corticosteroid and mechanical ventilation on diaphragm muscle function. Muscle Nerve 2011, 43, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Supinski, G.S.; Ann Callahan, L. Diaphragm weakness in mechanically ventilated critically ill patients. Crit. Care 2013, 17, R120. [Google Scholar] [CrossRef] [Green Version]
- Adler, D.; Dupuis-Lozeron, E.; Richard, J.-C.; Janssens, J.-P.; Brochard, L. Does inspiratory muscle dysfunction predict readmission after intensive care unit discharge? Am. J. Respir. Crit. Care Med. 2014, 190, 347–350. [Google Scholar] [CrossRef]
- Medrinal, C.; Prieur, G.; Frenoy, É.; Robledo Quesada, A.; Poncet, A.; Bonnevie, T.; Gravier, F.E.; Lamia, B.; Contal, O. Respiratory weakness after mechanical ventilation is associated with one-year mortality—A prospective study. Crit. Care 2016, 20, 231. [Google Scholar] [CrossRef] [Green Version]
- Heunks, L.; Ottenheijm, C. Diaphragm-protective mechanical ventilation to improve outcomes in ICU patients? Am. J. Respir. Crit. Care Med. 2018, 197, 150–152. [Google Scholar] [CrossRef]
- Schepens, T.; Dianti, J. Diaphragm protection: What should we target? Curr. Opin. Crit. Care 2020, 26, 35–40. [Google Scholar] [CrossRef]
- Schepens, T.; Dres, M.; Heunks, L.; Goligher, E.C. Diaphragm-protective mechanical ventilation. Curr. Opin. Crit. Care 2019, 25, 77–85. [Google Scholar] [CrossRef]
- Jaber, S.; Jung, B.; Matecki, S.; Petrof, B.J. Clinical review: Ventilator-induced diaphragmatic dysfunction-human studies confirm animal model findings! Crit. Care 2011, 15, 206. [Google Scholar] [CrossRef] [Green Version]
- Goligher, E.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Vorona, S.; Sklar, M.C.; Rittayamai, N.; Lanys, A.; et al. Mechanical ventilation–induced diaphragm atrophy strongly impacts clinical outcomes. Am. J. Respir. Crit. Care Med. 2018, 197, 204–213. [Google Scholar] [CrossRef]
- Goligher, E.C.; Fan, E.; Herridge, M.S.; Murray, A.; Vorona, S.; Brace, D.; Rittayamai, N.; Lanys, A.; Tomlinson, G.; Singh, J.M.; et al. Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am. J. Respir. Crit. Care Med. 2015, 192, 1080–1088. [Google Scholar] [CrossRef]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef]
- Jiang, T.-X.; Reid, W.D.; Belcastro, A.; Road, J.D. Load dependence of secondary diaphragm inflammation and injury after acute inspiratory loading. Am. J. Respir. Crit. Care Med. 1998, 157, 230–236. [Google Scholar] [CrossRef]
- Liang, F.; Emeriaud, G.; Rassier, D.E.; Shang, D.; Gusev, E.; Hussain, S.N.A.; Sage, M.; Crulli, B.; Fortin-Pellerin, E.; Praud, J.P.; et al. Mechanical ventilation causes diaphragm dysfunction in newborn lambs. Crit. Care 2019, 23, 123. [Google Scholar] [CrossRef] [Green Version]
- Radell, P.J.; Remahl, S.; Nichols, D.G.; Eriksson, L.I. Effects of prolonged mechanical ventilation and inactivity on piglet diaphragm function. Intensive Care Med. 2002, 28, 358–364. [Google Scholar] [CrossRef]
- Anzueto, A.; Peters, J.I.; Tobin, M.J.; de los Santos, R.; Seidenfeld, J.J.; Moore, G.; Cox, W.J.; Coalson, J.J. Effects of prolonged controlled mechanical ventilation on diaphragmatic function in healthy adult baboons. Crit. Care Med. 1997, 25, 1187–1190. [Google Scholar] [CrossRef]
- Futier, E.; Constantin, J.M.; Combaret, L.; Mosoni, L.; Roszyk, L.; Sapin, V.; Attaix, D.; Jung, B.; Jaber, S.; Bazin, J.E. Pressure support ventilation attenuates ventilator-induced protein modifications in the diaphragm. Crit. Care 2008, 12, R116. [Google Scholar] [CrossRef] [Green Version]
- Sassoon, C.S.; Caiozzo, V.J.; Manka, A.; Sieck, G.C. Altered diaphragm contractile properties with controlled mechanical ventilation. J. Appl. Physiol. 2002, 92, 2585–2595. [Google Scholar] [CrossRef]
- Shanely, R.A.; Zergeroglu, M.A.; Lennon, S.L.; Sugiura, T.; Yimlamai, T.; Enns, D.; Belcastro, A.; Powers, S.K. Mechanical ventilation–induced diaphragmatic atrophy is associated with oxidative injury and increased proteolytic activity. Am. J. Respir. Crit. Care Med. 2002, 166, 1369–1374. [Google Scholar] [CrossRef] [Green Version]
- Hooijman, P.E.; Beishuizen, A.; Witt, C.C.; de Waard, M.C.; Girbes, A.R.; Spoelstra-de Man, A.M.; Niessen, H.W.; Manders, E.; van Hees, H.W.; van den Brom, C.E.; et al. Diaphragm muscle fiber weakness and ubiquitin-proteasome activation in critically ill patients. Am. J. Respir. Crit. Care Med. 2015, 191, 1126–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, M.; Hooijman, P.E.; Beishuizen, A.; de Waard, M.C.; Paul, M.A.; Hartemink, K.J.; van Hees, H.W.H.; Lawlor, M.W.; Brocca, L.; Bottinelli, R.; et al. Diaphragm atrophy and weakness in the absence of mitochondrial dysfunction in the critically ill. Am. J. Respir. Crit. Care Med. 2017, 196, 1544–1558. [Google Scholar] [CrossRef]
- Grosu, H.B.; Im Lee, Y.; Lee, J.; Eden, E.; Eikermann, M.; Rose, K.M. Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 2012, 142, 1455–1460. [Google Scholar] [CrossRef]
- Schepens, T.; Verbrugghe, W.; Dams, K.; Corthouts, B.; Parizel, P.M.; Jorens, P.G. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: A longitudinal cohort study. Crit. Care 2015, 19, 422. [Google Scholar] [CrossRef] [Green Version]
- Zambon, M.; Beccaria, P.; Matsuno, J.; Gemma, M.; Frati, E.; Colombo, S.; Cabrini, L.; Landoni, G.; Zangrillo, A. Mechanical ventilation and diaphragmatic atrophy in critically ill patients: An ultrasound study. Crit. Care Med. 2016, 44, 1347–1352. [Google Scholar] [CrossRef]
- Marin-Corral, J.; Dot, I.; Boguña, M.; Cecchini, L.; Zapatero, A.; Gracia, M.P.; Pascual-Guardia, S.; Vilà, C.; Castellví, A.; Pérez-Terán, P.; et al. Structural differences in the diaphragm of patients following controlled vs assisted and spontaneous mechanical ventilation. Intensive Care Med. 2019, 45, 488–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, W.; Huang, J.; Bryson, S.; Walker, D.; Belcastro, A. Diaphragm injury and myofibrillar structure induced by resistive loading. J. Appl. Physiol. 1994, 76, 176–184. [Google Scholar] [CrossRef]
- Pellegrini, M.; Hedenstierna, G.; Roneus, A.; Segelsjö, M.; Larsson, A.; Perchiazzi, G. The diaphragm acts as a brake during expiration to prevent lung collapse. Am. J. Respir. Crit. Care Med. 2017, 195, 1608–1616. [Google Scholar] [CrossRef]
- Akoumianaki, E.; Lyazidi, A.; Rey, N.; Matamis, D.; Perez-Martinez, N.; Giraud, R.; Mancebo, J.; Brochard, L.; Richard, J.M. Mechanical ventilation-induced reverse-triggered breaths: A frequently unrecognized form of neuromechanical coupling. Chest 2013, 143, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Dres, M.; Patel, B.K.; Sahetya, S.K.; Beitler, J.R.; Telias, I.; Yoshida, T.; Vaporidi, K.; Grieco, D.L.; Schepens, T.; et al. Lung-and diaphragm-protective ventilation. Am. J. Respir. Crit. Care Med. 2020, 202, 950–961. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Jonkman, A.H.; Dianti, J.; Vaporidi, K.; Beitler, J.R.; Patel, B.K.; Yoshida, T.; Jaber, S.; Dres, M.; Mauri, T.; et al. Clinical strategies for implementing lung and diaphragm-protective ventilation: Avoiding insufficient and excessive effort. Intensive Care Med. 2020, 46, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, J.; van den Berg, M.; van der Pijl, R.; Hooijman, P.E.; Beishuizen, A.; Elshof, J.; de Waard, M.; Girbes, A.; Spoelstra-de Man, A.; Shi, Z.H.; et al. Positive end-expiratory pressure ventilation induces longitudinal atrophy in diaphragm fibers. Am. J. Respir. Crit. Care Med. 2018, 198, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Telias, I.; Spadaro, S. Techniques to monitor respiratory drive and inspiratory effort. Curr. Opin. Crit. Care 2020, 26, 3–10. [Google Scholar] [CrossRef]
- Goligher, E.C.; Laghi, F.; Detsky, M.E.; Farias, P.; Murray, A.; Brace, D.; Brochard, L.J.; Bolz, S.S.; Rubenfeld, G.D.; Kavanagh, B.P.; et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: Feasibility, reproducibility and validity. Intensive Care Med. 2015, 41, 642–649. [Google Scholar] [CrossRef]
- Matamis, D.; Soilemezi, E.; Tsagourias, M.; Akoumianaki, E.; Dimassi, S.; Boroli, F.; Richard, J.C.; Brochard, L. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013, 39, 801–810. [Google Scholar] [CrossRef]
- Santana, P.V.; Cardenas, L.Z.; de Albuquerque, A.L.P.; de Carvalho, C.R.R.; Caruso, P. Diaphragmatic ultrasound: A review of its methodological aspects and clinical uses. J. Bras. Pneumol. 2020, 46. [Google Scholar] [CrossRef]
- Haaksma, M.E.; Smit, J.M.; Boussuges, A.; Demoule, A.; Dres, M.; Ferrari, G.; Formenti, P.; Goligher, E.C.; Heunks, L.; Lim, E.H.T.; et al. EXpert consensus On Diaphragm UltraSonography in the critically ill (EXODUS): A Delphi consensus statement on the measurement of diaphragm ultrasound-derived parameters in a critical care setting. Crit. Care 2022, 26, 99. [Google Scholar] [CrossRef]
- Tuinman, P.R.; Jonkman, A.H.; Dres, M.; Shi, Z.H.; Goligher, E.C.; Goffi, A.; de Korte, C.; Demoule, A.; Heunks, L. Respiratory muscle ultrasonography: Methodology, basic and advanced principles and clinical applications in ICU and ED patients—A narrative review. Intensive Care Med. 2020, 46, 594–605. [Google Scholar] [CrossRef] [Green Version]
- Zambon, M.; Greco, M.; Bocchino, S.; Cabrini, L.; Beccaria, P.F.; Zangrillo, A. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: A systematic review. Intensive Care Med. 2017, 43, 29–38. [Google Scholar] [CrossRef]
- Boussuges, A.; Gole, Y.; Blanc, P. Diaphragmatic motion studied by m-mode ultrasonography: Methods, reproducibility, and normal values. Chest 2009, 135, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.; Soldati, G.; Giannuzzi, R.; Berardi, S.; Portale, G.; Silveri, N.G. Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med. Biol. 2011, 37, 44–52. [Google Scholar] [CrossRef]
- Schepens, T.; Fard, S.; Goligher, E.C. Assessing diaphragmatic function. Respir. Care 2020, 65, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Formenti, P.; Longhi, D.; Galimberti, A.; Piva, I.; Pezzi, A.; Mistraletti, G.; Marini, J.J.; Iapichino, G. Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: A pilot clinical study. Crit. Care 2015, 19, 161. [Google Scholar] [CrossRef] [Green Version]
- Lerolle, N.; Guérot, E.; Dimassi, S.; Zegdi, R.; Faisy, C.; Fagon, J.Y.; Diehl, J.L. Ultrasonographic diagnostic criterion for severe diaphragmatic dysfunction after cardiac surgery. Chest 2009, 135, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Boon, A.J.; Harper, C.J.; Ghahfarokhi, L.S.; Strommen, J.A.; Watson, J.C.; Sorenson, E.J. Two-dimensional ultrasound imaging of the diaphragm: Quantitative values in normal subjects. Muscle Nerve 2013, 47, 884–889. [Google Scholar] [CrossRef]
- Cardenas, L.Z.; Santana, P.V.; Caruso, P.; de Carvalho, C.R.R.; de Albuquerque, A.L.P. Diaphragmatic ultrasound correlates with inspiratory muscle strength and pulmonary function in healthy subjects. Ultrasound Med. Biol. 2018, 44, 786–793. [Google Scholar] [CrossRef]
- Carrillo-Esper, R.; Pérez-Calatayud, Á.A.; Arch-Tirado, E.; Díaz-Carrillo, M.A.; Garrido-Aguirre, E.; Tapia-Velazco, R.; Peña-Pérez, C.A.; Espinoza-de Los Monteros, I.; Meza-Márquez, J.M.; Flores-Rivera, O.I.; et al. Standardization of sonographic diaphragm thickness evaluations in healthy volunteers. Respir. Care 2016, 61, 920–924. [Google Scholar] [CrossRef] [Green Version]
- Cohn, D.; Benditt, J.O.; Eveloff, S.; McCool, F.D. Diaphragm thickening during inspiration. J. Appl. Physiol. 1997, 83, 291–296. [Google Scholar] [CrossRef]
- Gottesman, E.; McCool, F.D. Ultrasound evaluation of the paralyzed diaphragm. Am. J. Respir. Crit. Care Med. 1997, 155, 1570–1574. [Google Scholar] [CrossRef]
- Ueki, J.; De Bruin, P.; Pride, N. In vivo assessment of diaphragm contraction by ultrasound in normal subjects. Thorax 1995, 50, 1157–1161. [Google Scholar] [CrossRef] [Green Version]
- Valette, X.; Seguin, A.; Daubin, C.; Brunet, J.; Sauneuf, B.; Terzi, N.; du Cheyron, D. Diaphragmatic dysfunction at admission in intensive care unit: The value of diaphragmatic ultrasonography. Intensive Care Med. 2015, 41, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Mariani, L.F.; Bedel, J.; Gros, A.; Lerolle, N.; Milojevic, K.; Laurent, V.; Hilly, J.; Troché, G.; Bedos, J.P.; Planquette, B. Ultrasonography for screening and follow-up of diaphragmatic dysfunction in the ICU: A pilot study. J. Intensive Care Med. 2016, 31, 338–343. [Google Scholar] [CrossRef]
- Lu, Z.; Xu, Q.; Yuan, Y.; Zhang, G.; Guo, F.; Ge, H. Diaphragmatic dysfunction is characterized by increased duration of mechanical ventilation in subjects with prolonged weaning. Respir. Care 2016, 61, 1316–1322. [Google Scholar] [CrossRef]
- Dubé, B.-P.; Dres, M.; Mayaux, J.; Demiri, S.; Similowski, T.; Demoule, A. Ultrasound evaluation of diaphragm function in mechanically ventilated patients: Comparison to phrenic stimulation and prognostic implications. Thorax 2017, 72, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Dot, I.; Pérez-Terán, P.; Francés, A.; Díaz, Y.; Vilà-Vilardell, C.; Salazar-Degracia, A.; Chalela, R.; Barreiro, E.; Rodriguez-Fuster, A.; Masclans, J.R.; et al. Association between histological diaphragm atrophy and ultrasound diaphragm expiratory thickness in ventilated patients. J. Intensive Care 2022, 10, 40. [Google Scholar] [CrossRef] [PubMed]
- Urner, M.; Mitsakakis, N.; Vorona, S.; Chen, L.; Sklar, M.C.; Dres, M.; Rubenfeld, G.D.; Brochard, L.J.; Ferguson, N.D.; Fan, E.; et al. Identifying subjects at risk for diaphragm atrophy during mechanical ventilation using routinely available clinical data. Respir. Care 2021, 66, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Mekontso Dessap, A.; Dimassi, S.; Vargas, F.; Lyazidi, A.; Thille, A.W.; Brochard, L. Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation. Intensive Care Med. 2012, 38, 796–803. [Google Scholar] [CrossRef]
- Cala, S.J.; Kenyon, C.M.; Lee, A.; Watkin, K.; Macklem, P.T.; Rochester, D.F. Respiratory ultrasonography of human parasternal intercostal muscle in vivo. Ultrasound Med. Biol. 1998, 24, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Wallbridge, P.; Parry, S.M.; Das, S.; Law, C.; Hammerschlag, G.; Irving, L.; Hew, M.; Steinfort, D. Parasternal intercostal muscle ultrasound in chronic obstructive pulmonary disease correlates with spirometric severity. Sci. Rep. 2018, 8, 15274. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, N.; Oto, J.; Ueno, Y.; Nakataki, E.; Itagaki, T.; Nishimura, M. Change in diaphragm and intercostal muscle thickness in mechanically ventilated patients: A prospective observational ultrasonography study. J. Intensive Care 2019, 7, 56. [Google Scholar] [CrossRef]
- Yoshida, R.; Tomita, K.; Kawamura, K.; Nozaki, T.; Setaka, Y.; Monma, M.; Ohse, H. Measurement of intercostal muscle thickness with ultrasound imaging during maximal breathing. J. Phys. Ther. Sci. 2019, 31, 340–343. [Google Scholar] [CrossRef] [Green Version]
- Umbrello, M.; Formenti, P.; Lusardi, A.C.; Guanziroli, M.; Caccioppola, A.; Coppola, S.; Chiumello, D. Oesophageal pressure and respiratory muscle ultrasonographic measurements indicate inspiratory effort during pressure support ventilation. Br. J. Anaesth. 2020, 125, e148–e157. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Dubé, B.P.; Goligher, E.; Vorona, S.; Demiri, S.; Morawiec, E.; Mayaux, J.; Brochard, L.; Similowski, T.; Demoule, A. Usefulness of parasternal intercostal muscle ultrasound during weaning from mechanical ventilation. Anesthesiology 2020, 132, 1114–1125. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Similowski, T.; Goligher, E.C.; Pham, T.; Sergenyuk, L.; Telias, I.; Grieco, D.L.; Ouechani, W.; Junhasavasdikul, D.; Sklar, M.C.; et al. Dyspnoea and respiratory muscle ultrasound to predict extubation failure. Eur. Respir. J. 2021, 58, 2100002. [Google Scholar] [CrossRef]
- Powers, S.K.; Shanely, R.A.; Coombes, J.S.; Koesterer, T.J.; McKenzie, M.; Van Gammeren, D.; Cicale, M.; Dodd, S.L. Mechanical ventilation results in progressive contractile dysfunction in the diaphragm. J. Appl. Physiol. 2002, 92, 1851–1858. [Google Scholar] [CrossRef] [Green Version]
- Hudson, M.B.; Smuder, A.J.; Nelson, W.B.; Bruells, C.S.; Levine, S.; Powers, S.K. Both high level pressure support ventilation and controlled mechanical ventilation induce diaphragm dysfunction and atrophy. Crit. Care Med. 2012, 40, 1254. [Google Scholar] [CrossRef]
- Sklar, M.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Rittayamai, N.; Harhay, M.O.; Reid, W.D.; Tomlinson, G.; et al. Association of low baseline diaphragm muscle mass with prolonged mechanical ventilation and mortality among critically ill adults. JAMA Netw. Open 2020, 3, e1921520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldwin, C.E.; Paratz, J.D.; Bersten, A.D. Diaphragm and peripheral muscle thickness on ultrasound: Intra-rater reliability and variability of a methodology using non-standard recumbent positions. Respirology 2011, 16, 1136–1143. [Google Scholar] [CrossRef]
- Vivier, E.; Muller, M.; Putegnat, J.B.; Steyer, J.; Barrau, S.; Boissier, F.; Bourdin, G.; Mekontso-Dessap, A.; Levrat, A.; Pommier, C.; et al. Inability of diaphragm ultrasound to predict extubation failure: A multicenter study. Chest 2019, 155, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Dianti, J.; Fard, S.; Wong, J.; Chan, T.C.Y.; Del Sorbo, L.; Fan, E.; Amato, M.B.P.; Granton, J.; Burry, L.; Reid, W.D.; et al. Strategies for lung-and diaphragm-protective ventilation in acute hypoxemic respiratory failure: A physiological trial. Crit. Care 2022, 26, 259. [Google Scholar] [CrossRef] [PubMed]
- de Vries, H.J.; Jonkman, A.H.; de Grooth, H.J.; Duitman, J.W.; Girbes, A.R.J.; Ottenheijm, C.A.C.; Schultz, M.J.; van de Ven, P.M.; Zhang, Y.; de Man, A.M.E.; et al. Lung-and diaphragm-protective ventilation by titrating inspiratory support to diaphragm effort: A randomized clinical trial. Crit. Care Med. 2022, 50, 192. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Sigala, I.; Vassilakopoulos, T. Diaphragmatic ultrasound as a monitoring tool in the intensive care unit. Ann. Transl. Med. 2017, 5, 79. [Google Scholar] [CrossRef] [Green Version]
- Summerhill, E.M.; El-Sameed, Y.A.; Glidden, T.J.; McCool, F.D. Monitoring recovery from diaphragm paralysis with ultrasound. Chest 2008, 133, 737–743. [Google Scholar] [CrossRef]
- Oppersma, E.; Hatam, N.; Doorduin, J.; van der Hoeven, J.G.; Marx, G.; Goetzenich, A.; Fritsch, S.; Heunks, L.M.A.; Bruells, C.S. Functional assessment of the diaphragm by speckle tracking ultrasound during inspiratory loading. J. Appl. Physiol. 2017, 123, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Poulard, T.; Bachasson, D.; Fossé, Q.; Niérat, M.C.; Hogrel, J.Y.; Demoule, A.; Gennisson, J.L.; Dres, M. Poor correlation between diaphragm thickening fraction and transdiaphragmatic pressure in mechanically ventilated patients and healthy subjects. Anesthesiology 2022, 136, 162–175. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, I.; Chiodaroli, E.; Gattarello, S.; Cappio Borlino, S.; Chiumello, D. Diaphragmatic ultrasound and esophageal pressure in COVID-19 pneumonia during helmet CPAP. Intensive Care Med. 2022, 48, 1095–1096. [Google Scholar] [CrossRef] [PubMed]
- Holanda, M.A.; Vasconcelos, R.d.S.; Ferreira, J.C.; Pinheiro, B.V. Patient-ventilator asynchrony. J. Bras. Pneumol. 2018, 44, 321–333. [Google Scholar] [CrossRef] [PubMed]
- De Wit, M.; Miller, K.B.; Green, D.A.; Ostman, H.E.; Gennings, C.; Epstein, S.K. Ineffective triggering predicts increased duration of mechanical ventilation. Crit. Care Med. 2009, 37, 2740–2745. [Google Scholar]
- Tobin, M.J.; Jubran, A.; Laghi, F. Patient–ventilator interaction. Am. J. Respir. Crit. Care Med. 2001, 163, 1059–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beitler, J.R.; Sands, S.A.; Loring, S.H.; Owens, R.L.; Malhotra, A.; Spragg, R.G.; Matthay, M.A.; Thompson, B.T.; Talmor, D. Quantifying unintended exposure to high tidal volumes from breath stacking dyssynchrony in ARDS: The BREATHE criteria. Intensive Care Med. 2016, 42, 1427–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonis, H.; Gobert, F.; Tapponnier, R.; Guérin, C. Reverse triggering in a patient with ARDS. Intensive Care Med. 2015, 41, 1711–1712. [Google Scholar] [CrossRef] [PubMed]
- Blanch, L.; Villagra, A.; Sales, B.; Montanya, J.; Lucangelo, U.; Luján, M.; García-Esquirol, O.; Chacón, E.; Estruga, A.; Oliva, J.C.; et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015, 41, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Gilstrap, D.; MacIntyre, N. Patient–ventilator interactions. Implications for clinical management. Am. J. Respir. Crit. Care Med. 2013, 188, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Branson, R.D.; Blakeman, T.C.; Robinson, B.R. Asynchrony and dyspnea discussion. Respir. Care 2013, 58, 973–989. [Google Scholar] [CrossRef] [Green Version]
- Sieck, G.C.; Ferreira, L.F.; Reid, M.B.; Mantilla, C.B. Mechanical properties of respiratory muscles. Compr. Physiol. 2013, 3, 1553. [Google Scholar]
- Thille, A.W.; Rodriguez, P.; Cabello, B.; Lellouche, F.; Brochard, L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006, 32, 1515–1522. [Google Scholar] [CrossRef]
- Doorduin, J.; Van Hees, H.W.; Van Der Hoeven, J.G.; Heunks, L.M. Monitoring of the respiratory muscles in the critically ill. Am. J. Respir. Crit. Care Med. 2013, 187, 20–27. [Google Scholar] [CrossRef]
- Soilemezi, E.; Vasileiou, M.; Spyridonidou, C.; Tsagourias, M.; Matamis, D. Understanding patient–ventilator asynchrony using diaphragmatic ultrasonography. Am. J. Respir. Crit. Care Med. 2019, 200, e27–e28. [Google Scholar] [CrossRef]
- Vivier, E.; Haudebourg, A.F.; Le Corvoisier, P.; Mekontso Dessap, A.; Carteaux, G. Diagnostic accuracy of diaphragm ultrasound in detecting and characterizing patient–ventilator asynchronies during noninvasive ventilation. Anesthesiology 2020, 132, 1494–1502. [Google Scholar] [CrossRef]
- Epstein, S.K.; Ciubotaru, R.L.; Wong, J.B. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997, 112, 186–192. [Google Scholar] [CrossRef]
- Esteban, A.; Anzueto, A.; Frutos, F.; Alía, I.; Brochard, L.; Stewart, T.E.; Benito, S.; Epstein, S.K.; Apezteguía, C.; Nightingale, P.; et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: A 28-day international study. JAMA 2002, 287, 345–355. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, G.A.; Girard, T.D.; Kress, J.P.; Morris, P.E.; Ouellette, D.R.; Alhazzani, W.; Burns, S.M.; Epstein, S.K.; Esteban, A.; Fan, E.; et al. Official executive summary of an American Thoracic Society/American College of Chest Physicians clinical practice guideline: Liberation from mechanical ventilation in critically ill adults. Am. J. Respir. Crit. Care Med. 2017, 195, 115–119. [Google Scholar] [CrossRef]
- Llamas-Alvarez, A.M.; Tenza-Lozano, E.M.; Latour-Perez, J. Diaphragm and lung ultrasound to predict weaning outcome: Systematic review and meta-analysis. Chest 2017, 152, 1140–1150. [Google Scholar] [CrossRef]
- Li, C.; Li, X.; Han, H.; Cui, H.; Wang, G.; Wang, Z. Diaphragmatic ultrasonography for predicting ventilator weaning: A meta-analysis. Medicine 2018, 97, e10968. [Google Scholar] [CrossRef]
- Qian, Z.; Yang, M.; Li, L.; Chen, Y. Ultrasound assessment of diaphragmatic dysfunction as a predictor of weaning outcome from mechanical ventilation: A systematic review and meta-analysis. BMJ Open 2018, 8, e021189. [Google Scholar] [CrossRef] [Green Version]
- DiNino, E.; Gartman, E.J.; Sethi, J.M.; McCool, F.D. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax 2014, 69, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetrugno, L.; Orso, D.; Corradi, F.; Zani, G.; Spadaro, S.; Meroi, F.; D’Andrea, N.; Bove, T.; Cammarota, G.; De Robertis, E.; et al. Diaphragm ultrasound evaluation during weaning from mechanical ventilation in COVID-19 patients: A pragmatic, cross-section, multicenter study. Respir. Res. 2022, 23, 210. [Google Scholar] [CrossRef] [PubMed]
- Mayo, P.; Volpicelli, G.; Lerolle, N.; Schreiber, A.; Doelken, P.; Vieillard-Baron, A. Ultrasonography evaluation during the weaning process: The heart, the diaphragm, the pleura and the lung. Intensive Care Med. 2016, 42, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Cammarota, G.; Boniolo, E.; Tarquini, R.; Vaschetto, R. Diaphragmatic excursion tissue Doppler sonographic assessment. Intensive Care Med. 2020, 46, 1759–1760. [Google Scholar] [CrossRef]
- Maurizio, R.; Rinaldi, V.E.; Camerini, P.G.; Salvatori, C.; Leonardi, A.; Bini, V. Right diaphragmatic peak motion velocities on pulsed wave tissue Doppler imaging in neonates: Method, reproducibility, and reference values. J. Ultrasound Med. 2019, 38, 2695–2701. [Google Scholar] [CrossRef]
- Soilemezi, E.; Savvidou, S.; Sotiriou, P.; Smyrniotis, D.; Tsagourias, M.; Matamis, D. Tissue Doppler imaging of the diaphragm in healthy subjects and critically ill patients. Am. J. Respir. Crit. Care Med. 2020, 202, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- McCool, F.D.; Tzelepis, G.E. Tissue Doppler imaging of the diaphragm: A new kid on the block? Am. J. Respir. Crit. Care Med. 2020, 202, 921–922. [Google Scholar] [CrossRef]
- Blessberger, H.; Binder, T. Two dimensional speckle tracking echocardiography: Basic principles. Heart 2010, 96, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Hatam, N.; Goetzenich, A.; Rossaint, R.; Karfis, I.; Bickenbach, J.; Autschbach, R.; Marx, G.; Bruells, C.S. A novel application for assessing diaphragmatic function by ultrasonic deformation analysis in noninvasively ventilated healthy young adults. Ultraschall Med.—Eur. J. Ultrasound 2014, 35, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Orde, S.R.; Boon, A.J.; Firth, D.G.; Villarraga, H.R.; Sekiguchi, H. Diaphragm assessment by two dimensional speckle tracking imaging in normal subjects. BMC Anesthesiol. 2015, 16, 43. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Yang, X.; Qian, Y.; Hu, C.; Lu, W.; Cai, S.; Hu, B.; Li, J. Comparison of assessment of diaphragm function using speckle tracking between patients with successful and failed weaning: A multicentre, observational, pilot study. BMC Pulm. Med. 2022, 22, 459. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, S.J.; Hatam, N.; Goetzenich, A.; Marx, G.; Autschbach, R.; Heunks, L.; Bickenbach, J.; Bruells, C.S. Speckle tracking ultrasonography as a new tool to assess diaphragmatic function: A feasibility study. Ultrasonography 2022, 41, 403. [Google Scholar] [CrossRef] [PubMed]
- Chino, K.; Ohya, T.; Katayama, K.; Suzuki, Y. Diaphragmatic shear modulus at various submaximal inspiratory mouth pressure levels. Respir. Physiol. Neurobiol. 2018, 252, 52–57. [Google Scholar] [CrossRef]
- Bachasson, D.; Dres, M.; Niérat, M.C.; Gennisson, J.L.; Hogrel, J.Y.; Doorduin, J.; Similowski, T. Diaphragm shear modulus reflects transdiaphragmatic pressure during isovolumetric inspiratory efforts and ventilation against inspiratory loading. J. Appl. Physiol. 2019, 126, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Aarab, Y.; Flatres, A.; Garnier, F.; Capdevila, M.; Raynaud, F.; Lacampagne, A.; Chapeau, D.; Klouche, K.; Etienne, P.; Jaber, S.; et al. Shear wave elastography, a new tool for diaphragmatic qualitative assessment: A translational study. Am. J. Respir. Crit. Care Med. 2021, 204, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Jonkman, A.H.; de Korte, C.L. Shear wave elastography of the diaphragm: Good vibrations? Am. J. Respir. Crit. Care Med. 2021, 204, 748–750. [Google Scholar] [CrossRef] [PubMed]
- Khurana, J.; Gartner, S.C.; Naik, L.; Tsui, B.C. Ultrasound identification of diaphragm by novices using ABCDE technique. Reg. Anesth. Pain Med. 2018, 43, 161–165. [Google Scholar] [CrossRef]
- Sanchez de Toledo, J.; Munoz, R.; Landsittel, D.; Shiderly, D.; Yoshida, M.; Komarlu, R.; Wearden, P.; Morell, V.O.; Chrysostomou, C. Diagnosis of abnormal diaphragm motion after cardiothoracic surgery: Ultrasound performed by a cardiac intensivist vs. fluoroscopy. Congenit. Heart Dis. 2010, 5, 565–572. [Google Scholar] [CrossRef]
- Garofalo, E.; Bruni, A.; Pelaia, C.; Landoni, G.; Zangrillo, A.; Antonelli, M.; Conti, G.; Biasucci, D.G.; Mercurio, G.; Cortegiani, A.; et al. Comparisons of two diaphragm ultrasound-teaching programs: A multicenter randomized controlled educational study. Ultrasound J. 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirompanich, P.; Romsaiyut, S. Use of diaphragm thickening fraction combined with rapid shallow breathing index for predicting success of weaning from mechanical ventilator in medical patients. J. Intensive Care 2018, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Hellyer, N.J.; Andreas, N.M.; Bernstetter, A.S.; Cieslak, K.R.; Donahue, G.F.; Steiner, E.A.; Hollman, J.H.; Boon, A.J. Comparison of diaphragm thickness measurements among postures via ultrasound imaging. PMR 2017, 9, 21–25. [Google Scholar] [CrossRef]
- Wait, J.L.; Nahormek, P.A.; Yost, W.T.; Rochester, D.P. Diaphragmatic thickness-lung volume relationship in vivo. J. Appl. Physiol. 1989, 67, 1560–1568. [Google Scholar] [CrossRef]
- McKenzie, D.; Gandevia, S.; Gorman, R.; Southon, F. Dynamic changes in the zone of apposition and diaphragm length during maximal respiratory efforts. Thorax 1994, 49, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Sarwal, A.; Walker, F.O.; Cartwright, M.S. Neuromuscular ultrasound for evaluation of the diaphragm. Muscle Nerve 2013, 47, 319–329. [Google Scholar] [CrossRef]
- Saad, M.; Pini, S.; Danzo, F.; Mandurino Mirizzi, F.; Arena, C.; Tursi, F.; Radovanovic, D.; Santus, P. Ultrasonographic assessment of diaphragmatic function and its clinical application in the management of patients with acute respiratory failure. Diagnostics 2023, 13, 411. [Google Scholar] [CrossRef]
- Harris, R.; Giovannetti, M.; Kim, B. Normal ventilatory movement of the right hemidiaphragm studied by ultrasonography and pneumotachography. Radiology 1983, 146, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Gerscovich, E.O.; Cronan, M.; McGahan, J.P.; Jain, K.; Jones, C.D.; McDonald, C. Ultrasonographic evaluation of diaphragmatic motion. J. Ultrasound Med. 2001, 20, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Kantarci, F.; Mihmanli, I.; Demirel, M.K.; Harmanci, K.; Akman, C.; Aydogan, F.; Uysal, O. Normal diaphragmatic motion and the effects of body composition. J. Ultrasound Med. 2004, 23, 255–260. [Google Scholar] [CrossRef]
- Spiesshoefer, J.; Herkenrath, S.; Henke, C.; Langenbruch, L.; Schneppe, M.; Randerath, W.; Boentert, M. Evaluation of respiratory muscle strength and diaphragm ultrasound: Normative values, theoretical considerations, and practical recommendations. Respiration 2020, 99, 369–381. [Google Scholar] [CrossRef]
- Boussuges, A.; Rives, S.; Finance, J.; Chaumet, G.; Vallée, N.; Risso, J.-J.; Brégeon, F. Ultrasound assessment of diaphragm thickness and thickening: Reference values and limits of normality when in a seated position. Front. Med. 2021, 8, 1982. [Google Scholar] [CrossRef] [PubMed]
- Haaksma, M.E.; van Tienhoven, A.J.; Smit, J.M.; Heldeweg, M.L.A.; Lissenberg-Witte, B.I.; Wennen, M.; Jonkman, A.; Girbes, A.R.J.; Heunks, L.; Tuinman, P.R. Anatomical variation in diaphragm thickness assessed with ultrasound in healthy volunteers. Ultrasound Med. Biol. 2022, 48, 1833–1839. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Methods | n | Main Findings | Highlights |
|---|---|---|---|---|
| Ultrasound of diaphragm to diagnose Diaphragm Dysfunction | ||||
| Lerolle, 2009 [55] | # Cardiac ICU # DE, Pdi, and Gilbert index, MV > 7 days # Severe DD = “Best DE < 25 mm (maximal inspiration) | 28 | Best DE discriminated patients with and without severe DD |
|
| Kim, 2011 [11] | # Medical ICU; MV > 48 h; # During SBT on PSV or T Tube # DD = Diaphragm excursion (DE) < 1 cm | 82 |
| DD:
|
| Valette, 2015 [62] | # Medical ICU, # DE during unassisted breathing # DD = DE < 1.0 cm, OR paradoxical OR absent | 10 | DD in 10 patients | ARF and DD: ↑ high mortality rates (60%) |
| Mariani, 2015 [63] | # Medical ICU, MV >7 days and SBT eligible # DE during SBT on T tube # DD = DE < 1.0 cm | 34 | DD prevalence 38% | DD bilateral in 24% DD: was not associated with extubation failure. |
| Lu, 2016 [64] | # Medical ICU, only patients on prolonged MV # TF during SBT on PSV # DD = TF < 20% | 41 | DD prevalence = 34%. | DD:
|
| Jung, 2016 [9] | # Patients with ICUAW, MV > 48 h, at 1st SBT # DD = Ptr,stim < 11 cmH2O. # Thickening fraction # ICUAW = MRC < 48 | 40 |
| Patients with ICUAW on first SBT
|
| Dube, 2017 [65] | # MV <24 h after intubation (‘initiation MV’), under ACV # MV at the switch to PSV (‘switch to PSV’) # Ptr,stim and US variables # DD = Ptr,stim <11 cm H2O. | 112 | At the switch to PSV,
|
|
| Dres M, 2017 [10] | # MV > 24 h, eligible for the 1st SBT # DD = Ptr,stim <11 cm H2O # “ICUAW” = MRC < 48. # TF and DE | 76 | At the first SBT attempt:
|
|
| Ultrasound of diaphragm to assess atrophy | ||||
| Grosu, 2012 [34] | # Daily measurement of Tdi since intubation | 7 |
|
|
| Schepens, 2015 [35] | # Medical ICU # Daily measurement of Tdi since first 24 h MV | 54 |
|
|
| Goligher, 2015 [23] | # Daily measurement of Tdi since OTI-72h of MV # Inspiratory effort = TF | 107 |  |  |
| Zambon, 2016 [36] | # Daily measurement of Tdi since the 1st day of MV # Daily atrophy rate (ΔTdi/d) = % reduction from the previous measurement # MV categorization = 4 classes | 40 |  |
|
| Goligher, 2018 [22] | # Daily measurement of Tdi since intubation until 72h of MV # Inspiratory effort = TF # Primary outcome: time to liberation from MV # 2ary outcomes: complications (reintubation, tracheostomy, prolonged ventilation, or death) | 211 |  | ⇓ Tdi > 10%: associated:
TF 15–30% = shortest duration of ventilation. |
| Dot, 2022 [66] | # Ventilated organ-donors and controls (n = 5) # Diaphragm biopsies (to measure CSA) # DUS to measure Tdi (at end-expiration # Median values of the controls = thresholds | 35 |
| Diaphragm Tdi: able to detect atrophy but cannot rule out atrophy completely
|
| Urner, 2022 [67] | # Clinical variables (RR, ventilator settings, and blood gases), were recorded longitudinally. # Diaphragm atrophy (⇓ Tdi > 10% from baseline) | 191 |
|
|
| Ultrasound of diaphragm to assess effort | ||||
| Lerolle, 2009 [55] | # Cardiac ICU, adult patients > 7 days MV pos-operative # Best DE = DE at maximal inspiratory effort # Pes, Pga, Pdi, # Severe DD = Gilbert index ≤ 0 | 28 |
|
|
| Vivier,2012 [68] | # ICU, adult # Patients under planned NIV post-extubation # During SB and NIV (PS 5, 10, 15) # Pressure–time product (PTPdi) and USD (Tdi and TF) | 12 |
| # TF usefulness
|
| Goligher 2015 [45] | # ICU, adult patients requiring MV # TF at peak and end-inspiration (airway occluded and diaphragm relaxed) in 9 controls (at varying lung volumes). # EAdi and Pdi | 96 |
| TF significantly correlated with EAdi and Pdi (validation study) |
| Umbrello, 2015 [54] | # Surgical ICU, adult patients, after major elective surgery eligible for an SBT with PSV # PSV 0, 5 and 15 cmH2O). #TF and diaphragmatic excursion # Diaphragm and esophageal PTP (PTPdi and PTPes) | 25 |
| TF is a reliable indicator of respiratory effort in patients undergoing AMV DE should not be used to quantitatively assess diaphragm contractile activity. |
| Dube, 2017 [65] | # MV <24 h after intubation (‘initiation MV’), under ACV # MV at the switch to PSV (‘switch to PSV’) # Ptr,stim and US variables were measured in, and compared # DD = Ptr,stim < 11 cm H2O. | 112 | A TFdi < 29% could reliably identify diaphragm dysfunction (sensitivity and specificity of 85% and 88%) |
|
| Ultrasound of intercostal muscles | ||||
| Cala, 1998 [69] | # Healthy subjects # US image of the 2nd interspace during tidal breathing, RV, FRC ant TLC # Inter-rib distance, parasternal IC thickness and motion of the midpoint | 4 |
|
|
| Wallbridge, 2018 [70] | # COPD patients # US measurement of thickness and echogenicity of 2nd and 3rd parasternal IC muscles, pectoralis major, quadriceps, and diaphragm thickness # CT-measured lateral IC mass | 20 |
|
|
| Nakanishi, 2019 [71] | # MV< 48 h # IC muscle thickness measured with US on days 1, 3, 5 and 7 # Change in IC thickness # The relationship of changes in IC thickness with patient characteristics | 80 |
| Decreased IC thickness:
|
| Yoshida, 2019 [72] | # Healthy volunteers # IC thickness measured using US at rest and at maximal breathing # Anterior, lateral and posterior portions of the IC spaces | 12 |
|
|
| Umbrello, 2020 [73] | # MV patients in PSV # Parasternal IC US (thickness and TF) at 3-levels of PSV (baseline, 25% and 50% reduction) # Diaphragm and esophageal PTP (PTPdi and PTPes) and WOB # DUS | 21 |
|
|
| Dres, 2020 [74] | # Evaluation of the parasternal in healthy volunteers # Responsiveness of parasternal to PSV levels in patients # Comparison of parasternal activity in presence or absence of diaphragm dysfunction # Comparison of parasternal activity in case of success/failure of an SBT | 93 |
|
|
| Dres, 2021 [75] | # Patients intubated ≥ 48 h # 2 h after extubation # Dyspnea (MRC) # US TF of the parasternal IC and the diaphragm # Limb muscle strength | 122 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santana, P.V.; Cardenas, L.Z.; Albuquerque, A.L.P.d. Diaphragm Ultrasound in Critically Ill Patients on Mechanical Ventilation—Evolving Concepts. Diagnostics 2023, 13, 1116. https://doi.org/10.3390/diagnostics13061116
Santana PV, Cardenas LZ, Albuquerque ALPd. Diaphragm Ultrasound in Critically Ill Patients on Mechanical Ventilation—Evolving Concepts. Diagnostics. 2023; 13(6):1116. https://doi.org/10.3390/diagnostics13061116
Chicago/Turabian StyleSantana, Pauliane Vieira, Letícia Zumpano Cardenas, and Andre Luis Pereira de Albuquerque. 2023. "Diaphragm Ultrasound in Critically Ill Patients on Mechanical Ventilation—Evolving Concepts" Diagnostics 13, no. 6: 1116. https://doi.org/10.3390/diagnostics13061116
APA StyleSantana, P. V., Cardenas, L. Z., & Albuquerque, A. L. P. d. (2023). Diaphragm Ultrasound in Critically Ill Patients on Mechanical Ventilation—Evolving Concepts. Diagnostics, 13(6), 1116. https://doi.org/10.3390/diagnostics13061116