


Corifolitropin-Alfa plus Five Days Letrozole Versus Daily Recombinant-FSH in Expected Normo-Responder Patients: A Retrospective Comparative Study


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. M-COH Protocols
2.4. Oocyte Insemination and Embryo Transfer
2.5. Data Collection and Reproductive Follow-Up
2.6. Outcomes Measures
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Ovarian Stimulation Parameters
3.3. Oocyte Retrieval and Embryo Culture
3.4. Embryo Transfer Outcome
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, V.; Osianlis, T.; Vollenhoven, B. Prevention of Ovarian Hyperstimulation Syndrome: A Review. Obstet. Gynecol. Int. 2015, 2015, 514519. [Google Scholar] [CrossRef] [PubMed]
- Gianaroli, L.; Vitagliano, A.; Ferraretti, A.P.; Azzena, S.; Terzuoli, G.; Perruzza, D.; Ambrosini, G.; Tabanelli, C.; Magli, M.C. IVF Lite: A smart IVF programme based on mild ovarian stimulation for good prognosis patients. Reprod. Biomed. Online 2022, 45, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Hadziosmanovic, N.; Berglund, L.; Holte, J. Using the ovarian sensitivity index to define poor, normal, and high response after controlled ovarian hyperstimulation in the long gonadotropin-releasing hormone-agonist protocol: Suggestions for a new principle to solve an old problem. Fertil. Steril. 2013, 100, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Lambalk, C.B.; Banga, F.R.; Huirne, J.A.; Toftager, M.; Pinborg, A.; Homburg, R.; van der Veen, F.; van Wely, M. GnRH antagonist versus long agonist protocols in IVF: A systematic review and meta-analysis accounting for patient type. Hum. Reprod. Update 2017, 23, 560–579. [Google Scholar] [CrossRef] [Green Version]
- Blockeel, C.; Sterrenburg, M.D.; Broekmans, F.J.; Eijkemans, M.J.; Smitz, J.; Devroey, P.; Fauser, B.C. Follicular phase endocrine characteristics during ovarian stimulation and GnRH antagonist cotreatment for IVF: RCT comparing recFSH initiated on cycle day 2 or 5. J. Clin. Endocrinol. Metab. 2011, 96, 1122–1128. [Google Scholar] [CrossRef]
- Sterrenburg, M.D.; Veltman-Verhulst, S.M.; Eijkemans, M.J.; Hughes, E.G.; Macklon, N.S.; Broekmans, F.J.; Fauser, B.C. Clinical outcomes in relation to the daily dose of recombinant follicle-stimulating hormone for ovarian stimulation in in vitro fertilization in presumed normal responders younger than 39 years: A meta-analysis. Hum. Reprod. Update 2011, 17, 184–196. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Guo, Q.; Wu, X.H.; Zhang, L.N.; Ge, J.; Xu, M.L.; Feng, Z.L.; Wu, X.Q. Does the additional use of clomiphene citrate or letrozole for in vitro fertilization deserve more attention? BMC Pregnancy Childbirth 2021, 21, 275. [Google Scholar] [CrossRef]
- Haas, J.; Casper, R.F. In vitro fertilization treatments with the use of clomiphene citrate or letrozole. Fertil. Steril. 2017, 108, 568–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rombauts, L.; Talmor, A. Corifollitropin alfa for female infertility. Expert Opin. Biol. Ther. 2012, 12, 107–112. [Google Scholar] [CrossRef]
- Cozzolino, M.; Vitagliano, A.; Cecchino, G.N.; Ambrosini, G.; Garcia-Velasco, J.A. Corifollitropin alfa for ovarian stimulation in in vitro fertilization: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2019, 111, 722–733. [Google Scholar] [CrossRef]
- Wang, A.; Letourneau, J.M.; Juarez-Hernandez, F.; Abel, M.K.; Mok-Lin, E.; Rosen, M.P. Hormone concentrations of dominant follicles in the TALES randomized controlled trial comparing letrozole with tamoxifen. J. Assist. Reprod. Genet. 2022, 39, 2617–2624. [Google Scholar] [CrossRef] [PubMed]
- Marin, L.; Vitagliano, A.; Capobianco, G.; Dessole, F.; Ambrosini, G.; Andrisani, A. Which is the optimal timing for starting chemoprotection with gonadotropin-releasing hormone agonists after oocyte cryopreservation? Reflections on a critical case of ovarian hyperstimulation syndrome. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101815. [Google Scholar] [CrossRef]
- Bülow, N.S.; Dreyer Holt, M.; Skouby, S.O.; Birch Petersen, K.; Englund, A.L.M.; Pinborg, A.; Macklon, N.S. Co-treatment with letrozole during ovarian stimulation for IVF/ICSI: A systematic review and meta-analysis. Reprod. Biomed. Online 2022, 44, 717–736. [Google Scholar] [CrossRef]
- Bülow, N.S.; Skouby, S.O.; Warzecha, A.K.; Udengaard, H.; Andersen, C.Y.; Holt, M.D.; Grøndahl, M.L.; Nyboe Andersen, A.; Sopa, N.; Mikkelsen, A.L.E.; et al. Impact of letrozole co-treatment during ovarian stimulation with gonadotrophins for IVF: A multicentre, randomized, double-blinded placebo-controlled trial. Hum. Reprod. 2022, 37, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Haas, J.; Bassil, R.; Meriano, J.; Samara, N.; Barzilay, E.; Gonen, N.; Casper, R.F. Does daily co-administration of letrozole and gonadotropins during ovarian stimulation improve IVF outcome? Reprod. Biol. Endocrinol. 2017, 15, 70. [Google Scholar] [CrossRef] [PubMed]
- Moini, A.; Lavasani, Z.; Kashani, L.; Mojtahedi, M.F.; Yamini, N. Letrozole as co-treatment agent in ovarian stimulation antagonist protocol in poor responders: A double-blind randomized clinical trial. Int. J. Reprod. Biomed. 2019, 17, 653–660. [Google Scholar] [CrossRef]
- Nelson, S.M.; Yates, R.W.; Lyall, H.; Jamieson, M.; Traynor, I.; Gaudoin, M.; Mitchell, P.; Ambrose, P.; Fleming, R. Anti-Müllerian hormone-based approach to controlled ovarian stimulation for assisted conception. Hum. Reprod. 2009, 24, 867–875. [Google Scholar] [CrossRef] [Green Version]
- Ecemis, T.; Tasci, Y.; Caglar, G.S. Controlled ovarian hyperstimulation with sequential letrozole co-treatment in normo/high responders. Gynecol. Endocrinol. 2016, 32, 206–209. [Google Scholar] [CrossRef]
- Oktay, K.; Hourvitz, A.; Sahin, G.; Oktem, O.; Safro, B.; Cil, A.; Bang, H. Letrozole reduces estrogen and gonadotropin exposure in women with breast cancer undergoing ovarian stimulation before chemotherapy. J. Clin. Endocrinol. Metab. 2006, 91, 3885–3890. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Cortvrindt, R.; Smitz, J. Effects of aromatase inhibition on in vitro follicle and oocyte development analyzed by early preantral mouse follicle culture. Mol. Reprod. Dev. 2002, 61, 549–559. [Google Scholar] [CrossRef]
- Ortega, I.; Sokalska, A.; Villanueva, J.A.; Cress, A.B.; Wong, D.H.; Stener-Victorin, E.; Stanley, S.D.; Duleba, A.J. Letrozole increases ovarian growth and Cyp17a1 gene expression in the rat ovary. Fertil. Steril. 2013, 99, 889–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrisani, A.; Marin, L.; Ragazzi, E.; Donà, G.; Bordin, L.; Dessole, F.; Armanini, D.; Esposito, F.; Vitagliano, A.; Sabbadin, C.; et al. Is corifollitropin alfa effective in controlled ovarian stimulation among all poor ovarian responders? A retrospective comparative study. Gynecol. Endocrinol. 2019, 35, 894–898. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Chen, G.Y.; Shieh, M.L.; Li, H.Y. An extremely patient-friendly and efficient stimulation protocol for assisted reproductive technology in normal and high responders. Reprod. Biol. Endocrinol. 2018, 16, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulsen, L.C.; Warzecha, A.K.; Bülow, N.S.; Bungum, L.; Macklon, N.S.; Yding Andersen, C.; Skouby, S.O. Effects of letrozole cotreatment on endocrinology and follicle development in women undergoing ovarian stimulation in an antagonist protocol. Hum. Reprod. 2022, 37, 1557–1571. [Google Scholar] [CrossRef]
- Lawrenz, B.; Coughlan, C.; Melado, L.; Digma, S.; Sibal, J.; Jean, A.; Fatemi, H.M. Step-Down of FSH- Dosage During Ovarian Stimulation—Basic Lessons to Be Learnt From a Randomized Controlled Trial. Front. Endocrinol. 2021, 12, 661707. [Google Scholar] [CrossRef]
- Venetis, C.A.; Kolibianakis, E.M.; Bosdou, J.K.; Tarlatzis, B.C. Progesterone elevation and probability of pregnancy after IVF: A systematic review and meta-analysis of over 60,000 cycles. Hum. Reprod. Update 2013, 19, 433–457. [Google Scholar] [CrossRef] [Green Version]
- Riva, A.; Buzzaccarini, G.; Vitagliano, A.; Laganà, A.S.; Cucinella, G.; Gullo, G. Progesterone: The key to success? Clin. Exp. Obstet. Gynecol. 2022, 49, 36. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Group_A (n = 91) | Group_B (n = 91) | |
|---|---|---|---|
| Age (years) | 32.42 (±2.34) | 31.90 (±2.59) ° | |
| BMI (kg/h2) | 22.3 (±3.0) | 22.0 (±2.9) ° | |
| Spontaneous miscarriage | 0.2 (±0.4) | 0.4 (±0.3) ° | |
| Cause of infertility | Unexplained | 33% (30) | 38.5% (35) ° |
| Mild male factor | 19.8% (18) | 23.1% (21) ° | |
| Tubal factor | 38.5% (35) | 33% (30) ° | |
| Endometriosis | 8.8% (8) | 5.5% (5) ° | |
| Duration of infertility (months) | 18.0 (±9.2) | 21.3 (±8.5) ° | |
| AFC | 11.31 (±3.16) | 11.14 (±2.04) ° | |
| FSH (iU/mL) | 7.08 (±1.4) | 6.95 (±1.4) ° | |
| LH (iU/mL) | 4.9 (±1.60) | 5.8 (±2.10) * | |
| E2 (pg/mL) | 46.6 (±20.9) | 42.3 (±14.5) ° | |
| AMH (ng/mL) | 2.49 (±0.76) | 2.78 (±0.90) ° | |
| Variables | Group_A (n = 91) | Group_B (n = 91) |
|---|---|---|
| Duration of ovarian stimulation (days) | 11.39 ± 1.66 | 10.98 ± 1.37 ° |
| Daily r-FSH consumption (IU) | 692.7 ± 487.9 | 2396.5 ± 1122.1 * |
| Long acting FSH consumption (IU) | 131.32 ± 24.32 | - |
| GnRH-antagonist injections (number) | 4.06 ± 1.42 | 4.88 ± 1.24 * |
| Day 8 antral follicles (number) | 9.89 ± 4.4 | 5.74 ± 3.87 * |
| Pre-ovulatory follicles (number) | 8.74 ± 3.30 | 7.96 ± 2.61° |
| Serum estradiol on the day of ovulation induction (ng/mL) | 1947.9 ± 1361.1 | 2681.2 ± 1569.2 * |
| Serum progesterone on the day of ovulation induction (ng/mL) | 1.10 ± 0.57 | 1.35 ± 0.92 * |
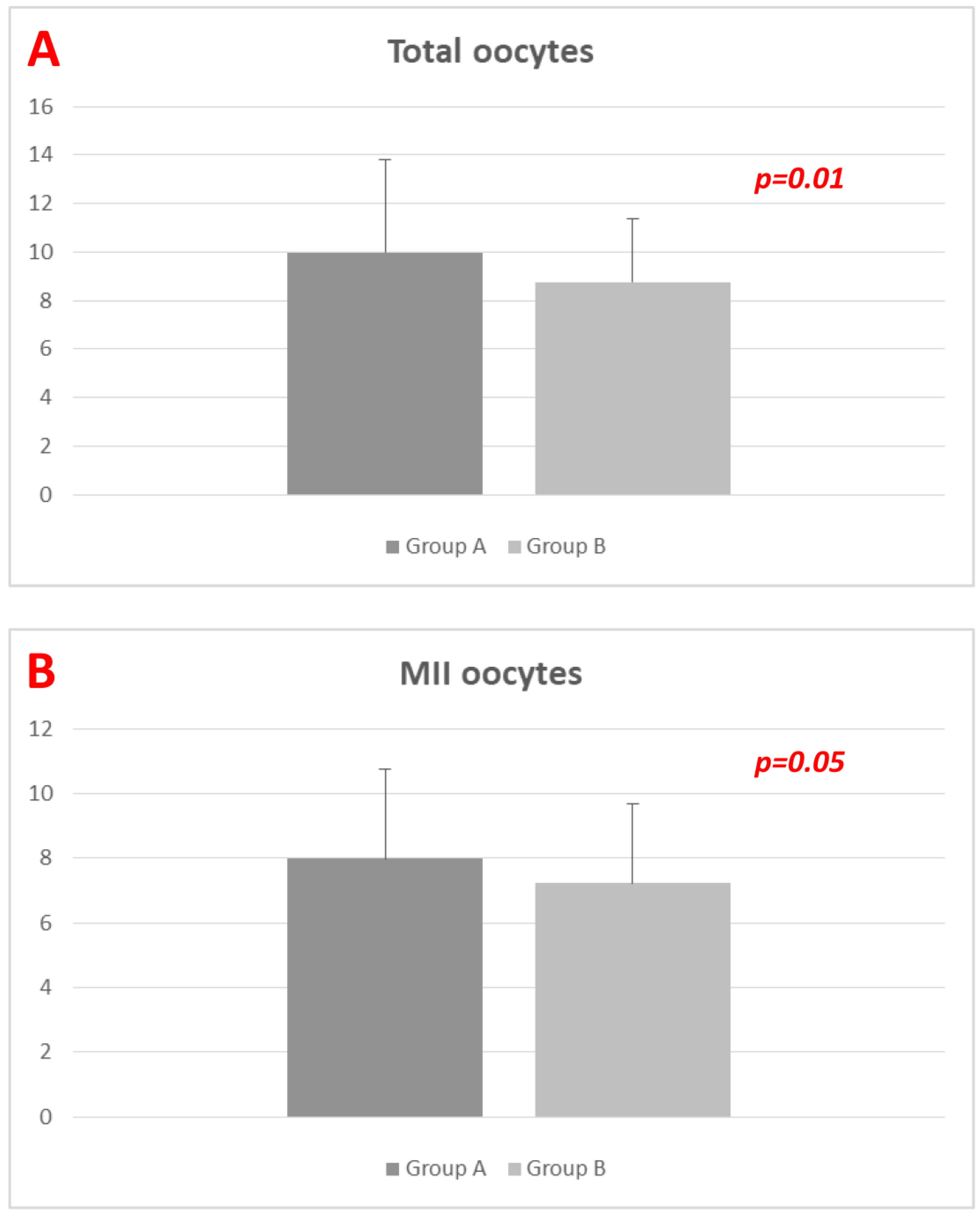
| Total oocytes (number) | 9.97 ± 3.81 | 8.76 ± 2.60 * |
| MII oocytes (number) | 7.98 ± 2.78 | 7.22 ± 2.47 ° |
| Fertilization rate (proportion) | 0.79 ± 0.22 | 0.80 ± 0.19 ° |
| Total embryos (number) | 3.73 ± 2.19 | 3.07 ± 1.22 * |
| Good quality embryos/blastocysts (number) | 2.72 ± 1.03 | 2.87 ± 1.19 ° |
| Fresh transfer (%) | 73.6% | 59.3% * |
| Transferred embryos (number) | 1.52 ± 0.57 | 1.52 ± 0.57 ° |
| Transferred good quality embryos/blastocysts (number) | 1.39 ± 0.62 | 1.41 ± 0.54 ° |
| Positive HCG test (%) | 53.8% | 46.1% ° |
| Implantation rate (%) | 38.4% | 35.5% ° |
| Cinical pregnancy rate (%) | 46.7% | 43.7% ° |
| Miscarriage rate (%) | 16.7% | 11.8% ° |
| Live birth rate (%) | 35.6% | 38.8% ° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amato, G.; Caringella, A.M.; Stanziano, A.; Cantatore, C.; D’Amato, A.; Cicinelli, E.; Vitagliano, A. Corifolitropin-Alfa plus Five Days Letrozole Versus Daily Recombinant-FSH in Expected Normo-Responder Patients: A Retrospective Comparative Study. Diagnostics 2023, 13, 1249. https://doi.org/10.3390/diagnostics13071249
D’Amato G, Caringella AM, Stanziano A, Cantatore C, D’Amato A, Cicinelli E, Vitagliano A. Corifolitropin-Alfa plus Five Days Letrozole Versus Daily Recombinant-FSH in Expected Normo-Responder Patients: A Retrospective Comparative Study. Diagnostics. 2023; 13(7):1249. https://doi.org/10.3390/diagnostics13071249
Chicago/Turabian StyleD’Amato, Giuseppe, Anna Maria Caringella, Antonio Stanziano, Clementina Cantatore, Antonio D’Amato, Ettore Cicinelli, and Amerigo Vitagliano. 2023. "Corifolitropin-Alfa plus Five Days Letrozole Versus Daily Recombinant-FSH in Expected Normo-Responder Patients: A Retrospective Comparative Study" Diagnostics 13, no. 7: 1249. https://doi.org/10.3390/diagnostics13071249
APA StyleD’Amato, G., Caringella, A. M., Stanziano, A., Cantatore, C., D’Amato, A., Cicinelli, E., & Vitagliano, A. (2023). Corifolitropin-Alfa plus Five Days Letrozole Versus Daily Recombinant-FSH in Expected Normo-Responder Patients: A Retrospective Comparative Study. Diagnostics, 13(7), 1249. https://doi.org/10.3390/diagnostics13071249