
Perfusion Computed Tomography May Help in Discriminating Gastrointestinal Tuberculosis and Crohn’s Disease


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Data
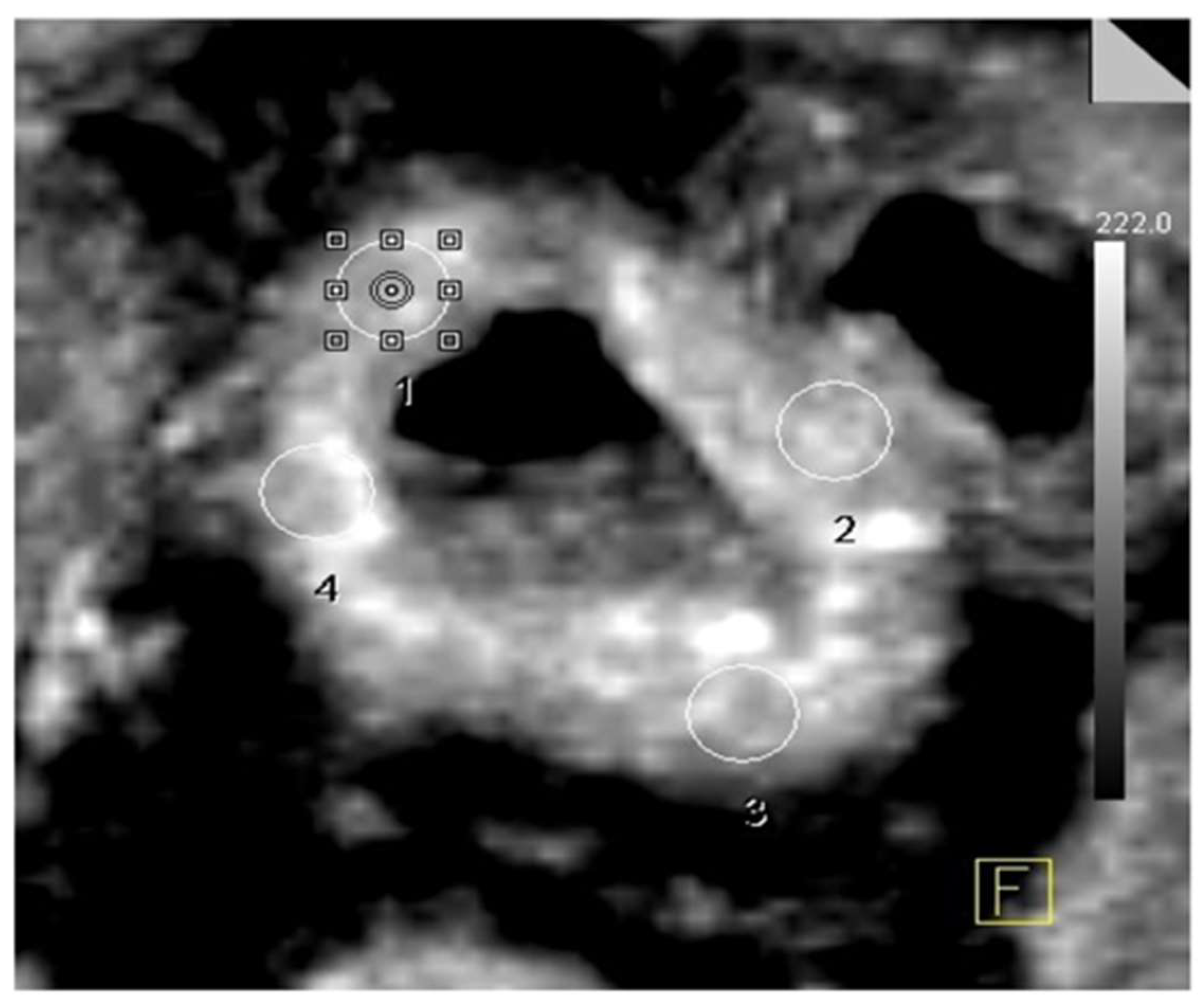
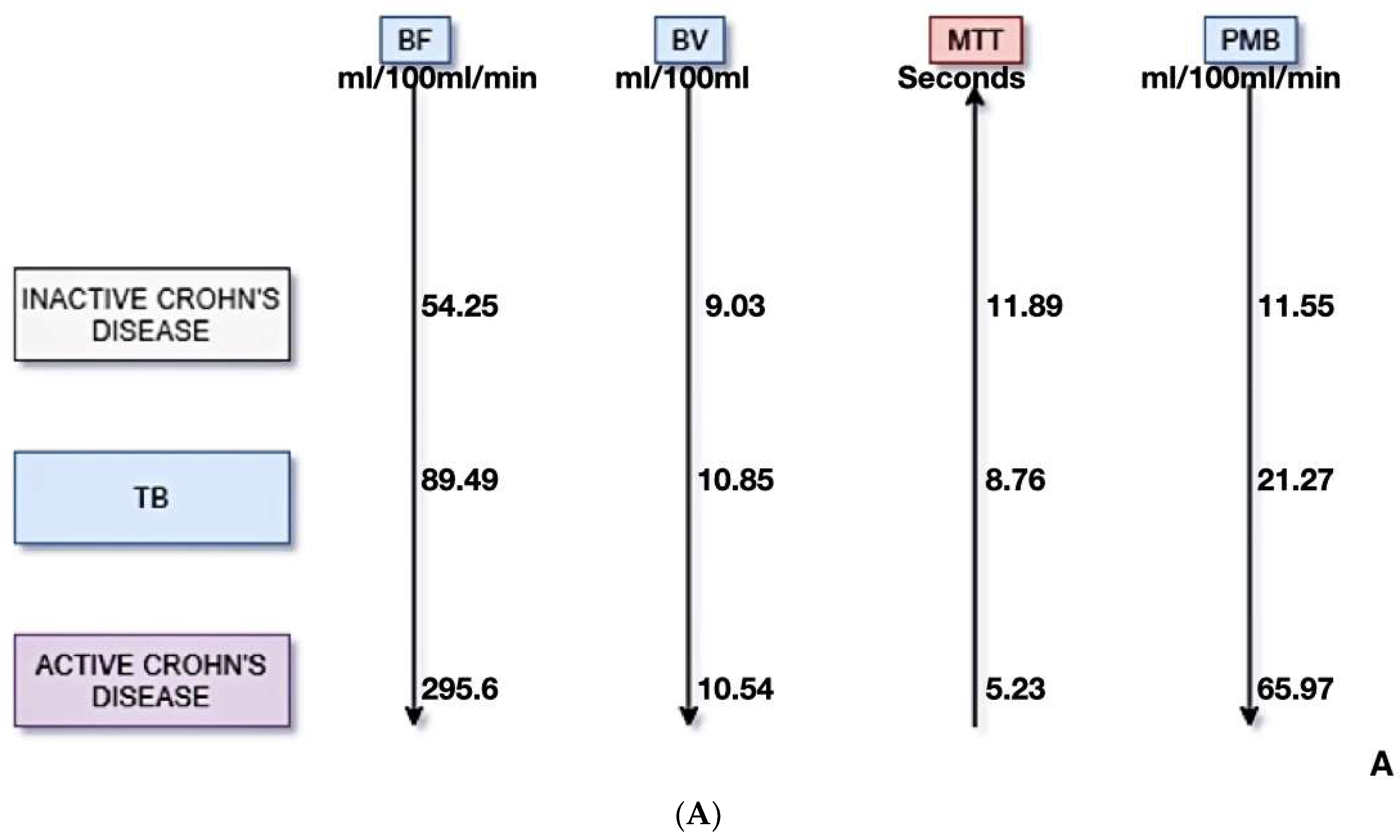
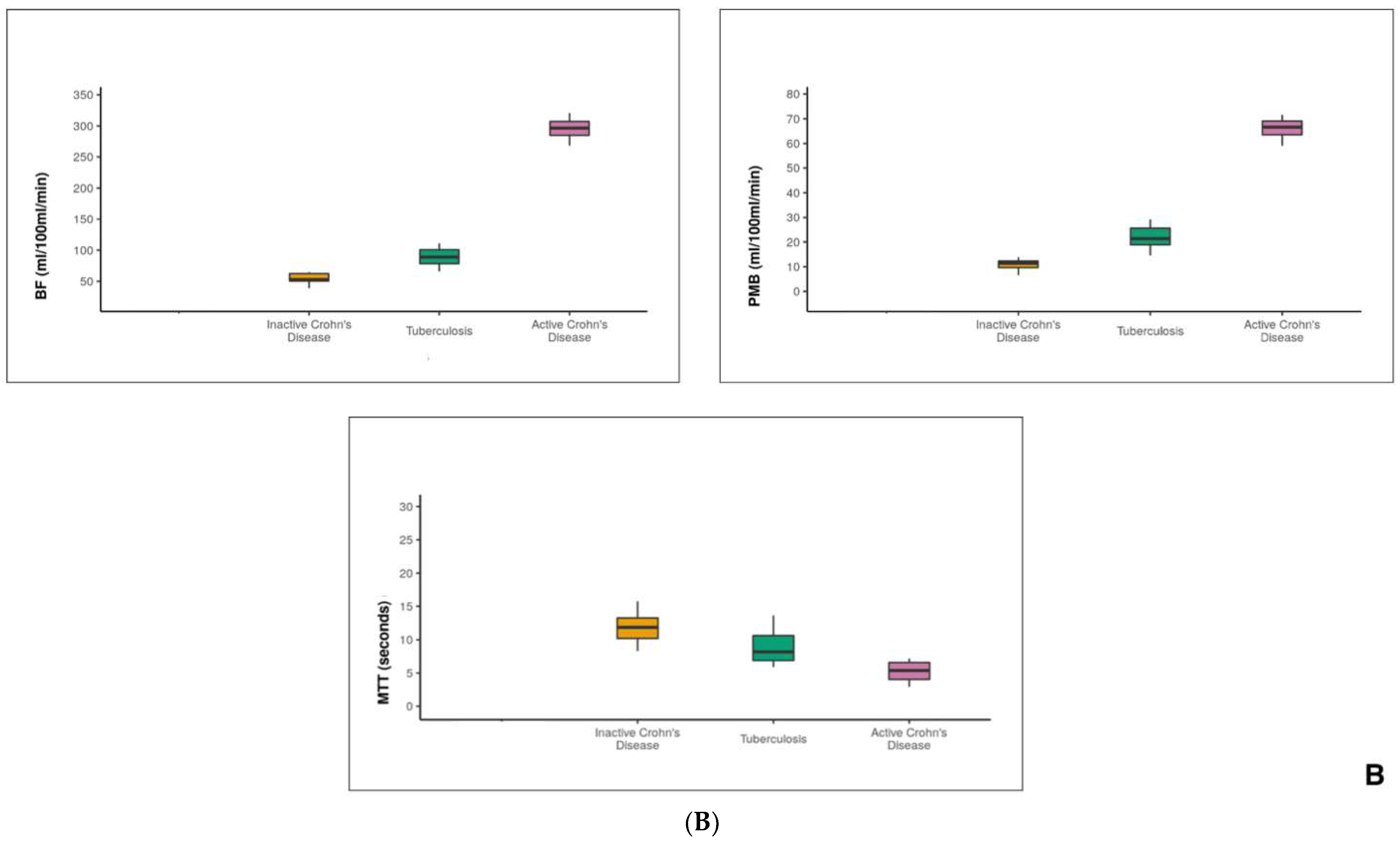
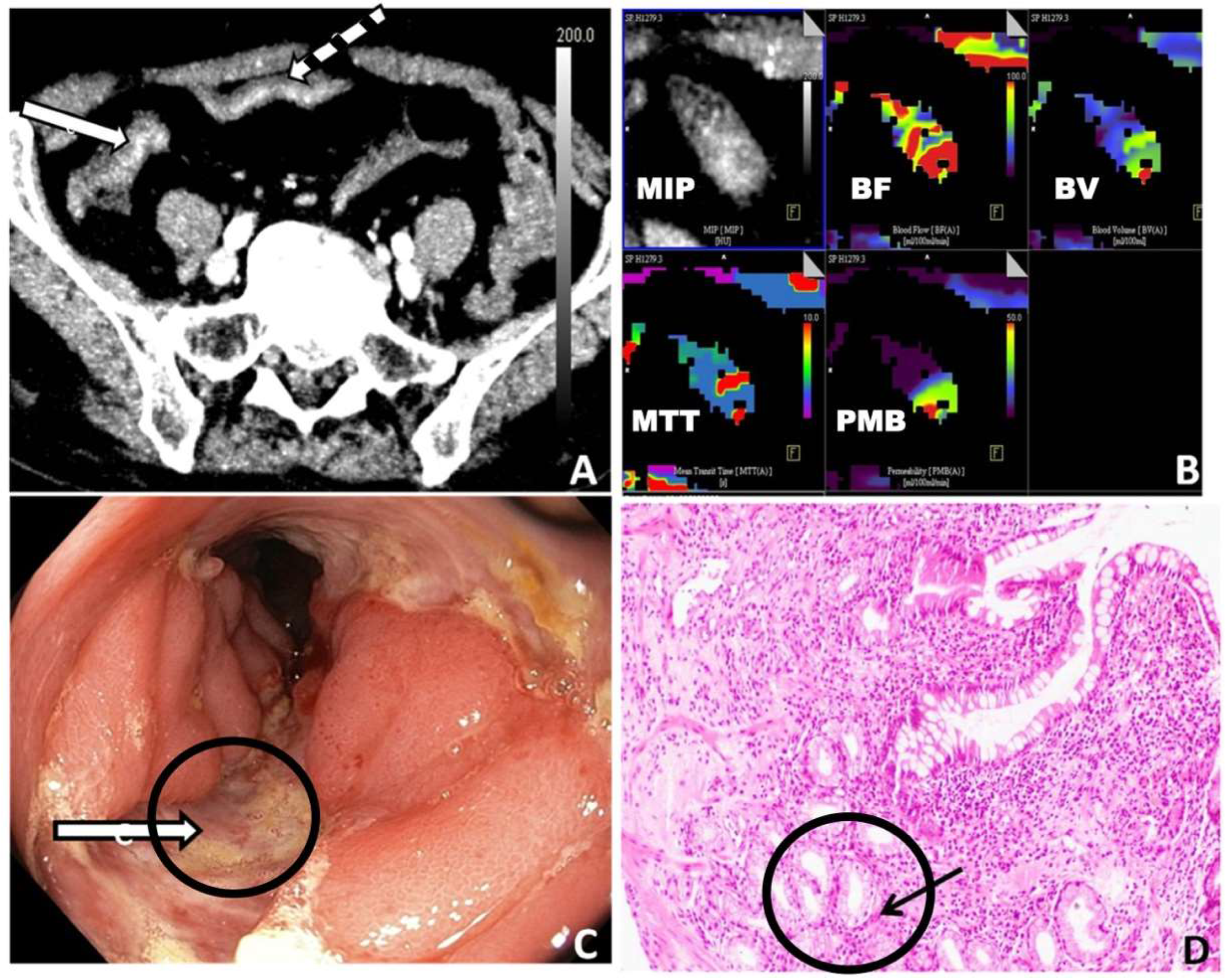
3.2. PCT Parameters
3.3. Diagnostic Performance of PCT
3.4. Interobserver Agreement
3.5. Radiation Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goyal, P.; Shah, J.; Gupta, S.; Gupta, P.; Sharma, V. Imaging in discriminating intestinal tuberculosis and Crohn’s disease: Past, present and the future. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 995–1007. [Google Scholar] [CrossRef]
- Pulimood, A.B.; Amarapurkar, D.N.; Ghoshal, U.; Phillip, M.; Pai, C.G.; Reddy, D.N.; Nagi, B.; Ramakrishna, B.S. Differentiation of Crohn’s disease from intestinal tuberculosis in India in 2010. World J. Gastroenterol. 2011, 17, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Pulimood, A.B.; Peter, S.; Ramakrishna, B.; Chacko, A.; Jeyamani, R.; Jeyaseelan, L.; Kurian, G. Segmental colonoscopic biopsies in the differentiation of ileocolic tuberculosis from Crohn’s disease. J. Gastroenterol. Hepatol. 2005, 20, 688–696. [Google Scholar] [CrossRef]
- Dhali, A.; Das, K.; Dhali, G.K.; Ghosh, R.; Sarkar, A.; Misra, D. Abdominal tuberculosis: Clinical profile and outcome. Int. J. Mycobacteriol. 2021, 10, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Cui, M.Y.; Chan, T.; Mao, R.; Luo, Y.; Barua, I.; Chen, M.; Li, Z.-P.; Feng, S.-T. Evaluation of intestinal tuberculosis by multi-slice computed tomography enterography. BMC Infect. Dis. 2015, 15, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.C.; Feng, Q.; Zhu, J.; Shen, J.; Qiao, Y.Q.; Xu, J.R.; Ran, Z.H. Usefulness of spectral computed tomography for evaluation of intestinal activity and severity in ileocolonic Crohn’s disease. Ther. Adv. Gastroenterol. 2016, 9, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Kalra, N.; Gulati, A.; Gupta, P.; Dhaka, N.; Sehgal, S.; Singh, S.; Gupta, V.; Sharma, K.; Vaiphei, K.; Rajwanshi, A.; et al. Comparison of virtual computed tomography enteroscopy using carbon dioxide with small-bowel enteroclysis and capsule endoscopy in patients with small-bowel tuberculosis. Eur. Radiol. 2020, 31, 3297–3305. [Google Scholar] [CrossRef]
- Singh, A.K.; Kumar, R.; Gupta, P.; Kumar, M.P.; Mishra, S.; Mandavdhare, H.S.; Singh, H.; Prasad, K.K.; Dutta, U.; Sharma, V. FDG-PET-CT Enterography Helps Determine Clinical Significance of Suspected Ileocecal Thickening: A Prospective Study. Dig. Dis. Sci. 2021, 66, 1620–1630. [Google Scholar] [CrossRef]
- Kedia, S.; Sharma, R.; Nagi, B.; Mouli, V.P.; Aananthakrishnan, A.; Dhingra, R.; Srivastava, S.; Kurrey, L.; Ahuja, V. Computerized tomography-based predictive model for differentiation of Crohn’s disease from intestinal tuberculosis. Indian J. Gastroenterol. 2015, 34, 135–143. [Google Scholar] [CrossRef]
- Yadav, D.P.; Madhusudhan, K.S.; Kedia, S.; Sharma, R.; Pratap Mouli, V.; Bopanna, S.; Dhingra, R.; Pradhan, R.; Goyal, S.; Sreenivas, V.; et al. Development and validation of visceral fat quantification as a surrogate marker for differentiation of Crohn’s disease and intestinal tuberculosis. J. Gastroenterol. Hepatol. 2017, 32, 420–426. [Google Scholar] [CrossRef]
- Sahani, D.V.; Holalkere, N.S.; Mueller, P.R.; Zhu, A.X. Advanced hepatocellular carcinoma: CT perfusion of liver and tumor tissue—Initial experience. Radiology 2007, 243, 736–743. [Google Scholar] [CrossRef]
- Sahani, D.V.; Kalva, S.P.; Hamberg, L.M.; Hahn, P.F.; Willett, C.G.; Saini, S.; Mueller, P.R.; Lee, T.-Y. Assessing tumor perfusion and treatment response in rectal cancer with multisection CT: Initial observations. Radiology 2005, 234, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Sitek, A.; Sheiman, R.G. Small-bowel perfusion measurement: Feasibility with single-compartment kinetic model applied to dynamic contrast-enhanced CT. Radiology 2005, 237, 670–674. [Google Scholar] [CrossRef]
- Kuwajerwala, N.K.; Bapat, R.D.; Joshi, A.S. Mesenteric vasculopathy in intestinal tuberculosis. Indian J. Gastroenterol. 1997, 16, 134–136. [Google Scholar] [PubMed]
- Pober, J.S.; Sessa, W.C. Inflammation and the Blood Microvascular System. Cold Spring Harb. Perspect. Biol. 2015, 7, 5–9. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4292166/ (accessed on 5 June 2020). [CrossRef]
- Deban, L.; Correale, C.; Vetrano, S.; Malesci, A.; Danese, S. Multiple Pathogenic Roles of Microvasculature in Inflammatory Bowel Disease: A Jack of All Trades. Am. J. Pathol. 2008, 172, 1457–1466. [Google Scholar] [CrossRef] [Green Version]
- Angerson, W.J.; Allison, M.C.; Baxter, J.N.; Russell, R.I. Neoterminal ileal blood flow after ileocolonic resection for Crohn’s disease. Gut 1993, 34, 1531–1534. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, A.J.; Sankey, A.; Dhillon, A.P.; Sawyerr, A.M.; More, L.; Pittilo, M.; Rowles, P.T.; Hudson, M.; Lewis, A.A.M.; Pounder, R.E. Granulomatous Vasculitis in Crohn’s Disease. Gastroenterology 1991, 100, 1279–1287. [Google Scholar] [CrossRef]
- Shah, P.; Ramakantan, R. Role of vasculitis in the natural history of abdominal tuberculosis—Evaluation by mesenteric angiography. Indian J. Gastroenterol. 1991, 10, 127–130. [Google Scholar] [PubMed]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohns Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.K.; Ryan, H.; Khaparde, S.; Sachdeva, K.S.; Singh, A.D.; Mohan, A.; Sarin, R.; Paramasivan, C.N.; Kumar, P.; Nischal, N.; et al. Index-TB Guidelines: Guidelines on extrapulmonary tuberculosis for India. Indian J. Med. Res. 2017, 145, 448–463. [Google Scholar]
- Sharma, V.; Mandavdhare, H.S.; Dutta, U. Letter: Mucosal response in discriminating intestinal tuberculosis from Crohn’s disease-when to look for it? Aliment. Pharmacol. Ther. 2018, 47, 859–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standard Treatment Workflow (STW) for the Management of ADULT ABDOMINAL TUBERCULOSIS ICD-10-A18.3. Available online: https://stw.icmr.org.in/images/Adult_Extr_Tuberculosis/1_Adult_Abdominal_TB_18032022.pdf (accessed on 18 January 2023).
- Almadi, M.A.; Ghosh, S.; Aljebreen, A.M. Differentiating intestinal tuberculosis from Crohn’s disease: A diagnostic challenge. Am. J. Gastroenterol. 2009, 104, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Amarapurkar, D.N.; Patel, N.D.; Rane, P.S. Diagnosis of Crohn’s disease in India where tuberculosis is widely prevalent. World J. Gastroenterol. 2008, 14, 741–746. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Wang, F.; Chen, Y.; Chen, H.; Wu, S.; Farris, A.B.; Jiang, Y.; Kong, J. Virtual liver needle biopsy from reconstructed three-dimensional histopathological images: Quantification of sampling error. Comput. Biol. Med. 2022, 147, 105764. [Google Scholar] [CrossRef]
- Jin, T.; Fei, B.; Zhang, Y.; He, X. The Diagnostic Value of Polymerase Chain Reaction for Mycobacterium tuberculosis to Distinguish Intestinal Tuberculosis from Crohn’s Disease: A Meta-analysis. Saudi J. Gastroenterol. 2017, 23, 3–10. [Google Scholar] [PubMed]
- Kumar, S.; Bopanna, S.; Kedia, S.; Mouli, P.; Dhingra, R.; Padhan, R.; Kohli, M.; Chaubey, J.; Sharma, R.; Das, P.; et al. Evaluation of Xpert MTB/RIF assay performance in the diagnosis of abdominal tuberculosis. Intestig. Res. 2017, 15, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Da Rocha, E.L.; Pedrassa, B.C.; Bormann, R.L.; Kierszenbaum, M.L.; Torres, L.R.; D’Ippolito, G. Abdominal tuberculosis: A radiological review with emphasis on computed tomography and magnetic resonance imaging findings. Radiol. Bras. 2015, 48, 181–191. [Google Scholar] [CrossRef]
- Kalra, N.; Agrawal, P.; Mittal, V.; Kochhar, R.; Gupta, V.; Nada, R.; Singh, R.; Khandelwal, N. Spectrum of imaging findings on MDCT enterography in patients with small bowel tuberculosis. Clin. Radiol. 2014, 69, 315–322. [Google Scholar] [CrossRef]
- Sharma, R.; Madhusudhan, K.S.; Ahuja, V. Intestinal tuberculosis versus crohn’s disease: Clinical and radiological recommendations. Indian J. Radiol. Imaging 2016, 26, 161. [Google Scholar] [CrossRef]
- Goh, V.; Halligan, S.; Hugill, J.A.; Bassett, P.; Bartram, C.I. Quantitative Assessment of Colorectal Cancer Perfusion Using MDCT: Inter- and Intraobserver Agreement. Am. J. Roentgenol. 2005, 185, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Goh, V.; Dattani, M.; Farwell, J.; Shekhdar, J.; Tam, E.; Patel, S.; Juttla, J.; Simcock, I.; Stirling, J.; Mandeville, H.; et al. Radiation dose from volumetric helical perfusion CT of the thorax, abdomen or pelvis. Eur. Radiol. 2011, 21, 974–981. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Inactive Crohn’s Disease (n = 9) | Gastrointestinal Tuberculosis (n = 11) | Active Crohn’s Disease (n = 6) | p |
|---|---|---|---|---|
| Blood Flow (mL/100 mL/min) | 54.25 ± 9.15 | 89.49 ± 15.73 | 295.60 ± 21.92 | 0.001 |
| Blood Volume (mL/100 mL) | 9.03 ± 2.00 | 10.85 ± 3.74 | 10.54 ± 0.81 | 0.417 |
| Mean Transit Time (s) | 11.89 ± 2.33 | 8.76 ± 2.57 | 5.23 ± 1.95 | 0.001 |
| Permeability (mL/100 mL/min) | 11.55 ± 3.28 | 21.27 ± 6.43 | 65.97 ± 5.32 | 0.001 |
| Parameters | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | Diagnostic Accuracy (95% CI) | AUC |
|---|---|---|---|---|---|---|
| Gastrointestinal tuberculosis vs. Crohn’s disease | ||||||
| Blood Flow (mL/100 mL/min) (cut-off: 64.64 mL/100 mL/min) | 69.2% (39–91) | 100.0% (69–100) | 100.0% (66–100) | 71.4% (42–92) | 82.6% (61–95) | 0.692 |
| Blood Volume (mL/100 mL) (cut-off: 12.68 mL/100 mL)) | 100.0% (75–100) | 30.0% (7–65) | 65.0% (41–85) | 100.0% (29–100) | 69.6% (47–87) | 0.558 |
| Mean Transit Time (s) (cut-off: 9.51 s) | 61.5% (32–86) | 70.0% (35–93) | 72.7% (39–94) | 58.3% (28–85) | 65.2% (43–84) | 0.600 |
| Permeability (mL/100 mL/min) (cut-off: 13.9 mL/100 mL/min) | 61.5% (32–86) | 90.0% (55–100) | 88.9% (52–100) | 64.3% (35–87) | 73.9% (52–90) | 0.623 |
| Gastrointestinal tuberculosis vs. active Crohn’s disease | ||||||
| Blood Flow (mL/100 mL/min) (cut-off: 268.5 mL/100 mL/min) | 100.0% (40–100) | 100.0% (69–100) | 100.0% (40–100) | 100.0% (69–100) | 100.0% (77–100) | 1 |
| Blood Volume (mL/100 mL) (cut-off: 9.8 mL/100 mL) | 100.0% (40–100) | 50.0% (19–81) | 44.4% (14–79) | 100.0% (48–100) | 64.3% (35–87) | 0.562 |
| Mean Transit Time (s) (cut-off: 7.2 s) | 100.0% (40–100) | 70.0% (35–93) | 57.1% (18–90) | 100.0% (59–100) | 78.6% (49–95) | 0.875 |
| Permeability (mL/100 mL/min) (cut-off: 59.1 mL/100 mL/min) | 100.0% (40–100) | 100.0% (69–100) | 100.0% (40–100) | 100.0% (69–100) | 100.0% (77–100) | 1 |
| Gastrointestinal tuberculosis vs. inactive Crohn’s disease | ||||||
| Blood Flow (mL/100 mL/min) (cut-off: 65.95 mL/100 mL/min) | 100.0% (69–100) | 100.0% (66–100) | 100.0% (69–100) | 100.0% (66–100) | 100.0% (82–100) | 1 |
| Blood Volume (mL/100 mL) (cut-off: 12.79 mL/100 mL) | 30.0% (7–65) | 100.0% (66–100) | 100.0% (29–100) | 56.2% (30–80) | 63.2% (38–84) | 0.611 |
| Mean Transit Time (s) (cut-off: 8.5 s) | 70.0% (35–93) | 88.9% (52–100) | 87.5% (47–100) | 72.7% (39–94) | 78.9% (54–94) | 0.811 |
| Permeability (mL/100 mL/min) (cut-off: 18.81 mL/100 mL/min) | 80.0% (44–97) | 100.0% (66–100) | 100.0% (63–100) | 81.8% (48–98) | 89.5% (67–99) | 0.900 |
| Active vs. inactive Crohn’s disease | ||||||
| Blood Flow (mL/100 mL/min) (cut-off: 268.5 mL/100 mL/min) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (75–100) | 1 |
| Blood Volume (mL/100 mL) (cut-off: 9.57 mL/100 mL) | 100.0% (40–100) | 66.7% (30–93) | 57.1% (18–90) | 100.0% (54–100) | 76.9% (46–95) | 0.722 |
| Mean Transit Time (s) (cut-off: 7.2 s) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (75–100) | 1 |
| Permeability (mL/100 mL/min) (cut-off: 43.54 mL/100 mL/min) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (40–100) | 100.0% (66–100) | 100.0% (75–100) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seth, R.; Gupta, P.; Debi, U.; Prasad, K.K.; Singh, H.; Sharma, V. Perfusion Computed Tomography May Help in Discriminating Gastrointestinal Tuberculosis and Crohn’s Disease. Diagnostics 2023, 13, 1255. https://doi.org/10.3390/diagnostics13071255
Seth R, Gupta P, Debi U, Prasad KK, Singh H, Sharma V. Perfusion Computed Tomography May Help in Discriminating Gastrointestinal Tuberculosis and Crohn’s Disease. Diagnostics. 2023; 13(7):1255. https://doi.org/10.3390/diagnostics13071255
Chicago/Turabian StyleSeth, Raghav, Pankaj Gupta, Uma Debi, Kaushal Kishore Prasad, Harjeet Singh, and Vishal Sharma. 2023. "Perfusion Computed Tomography May Help in Discriminating Gastrointestinal Tuberculosis and Crohn’s Disease" Diagnostics 13, no. 7: 1255. https://doi.org/10.3390/diagnostics13071255
APA StyleSeth, R., Gupta, P., Debi, U., Prasad, K. K., Singh, H., & Sharma, V. (2023). Perfusion Computed Tomography May Help in Discriminating Gastrointestinal Tuberculosis and Crohn’s Disease. Diagnostics, 13(7), 1255. https://doi.org/10.3390/diagnostics13071255