
Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Clinical Information
2.3. Histopathological Staining and Examination
2.4. p16INK4a Immunohistochemical Study
2.5. Scoring of the p16 Immunostaining
2.6. Ethical Approval
2.7. Statistical Analysis
3. Results
3.1. Demographic Data Comparison
3.2. Clinical Data Comparison
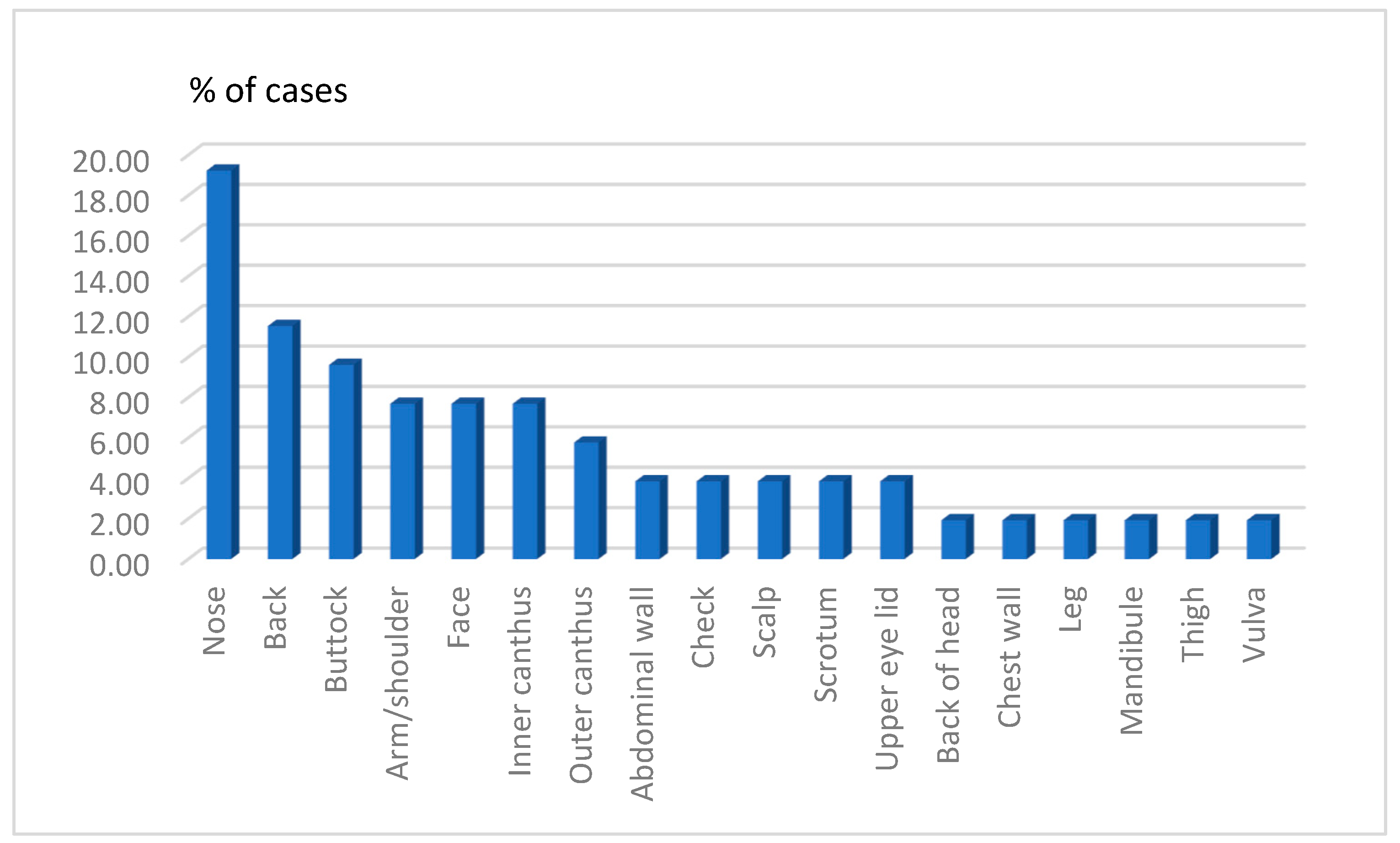
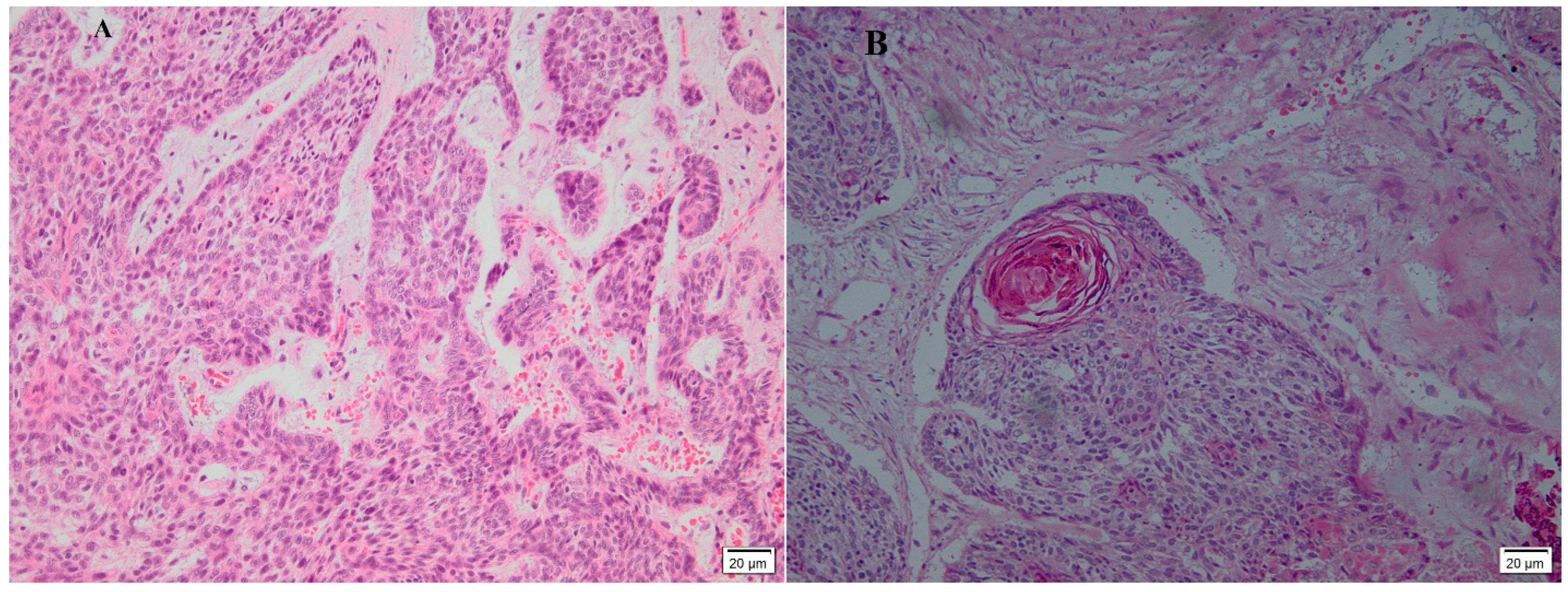
3.3. Histological Features
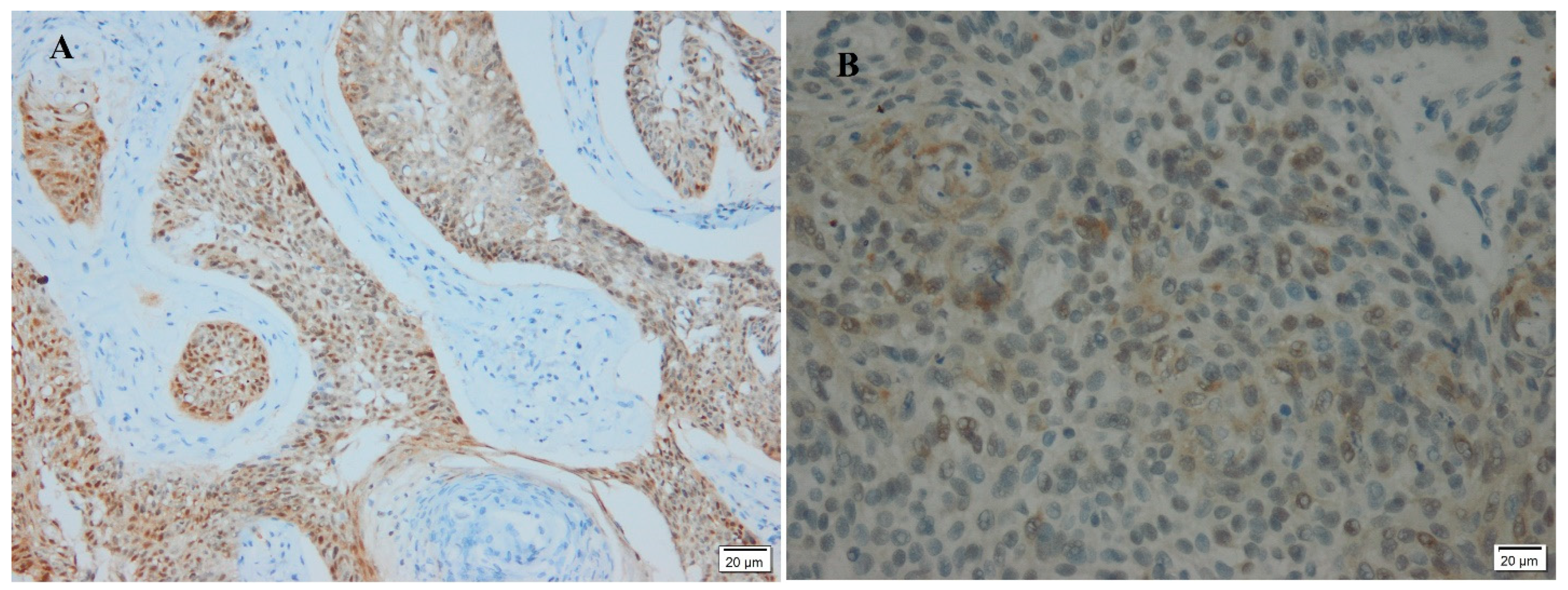
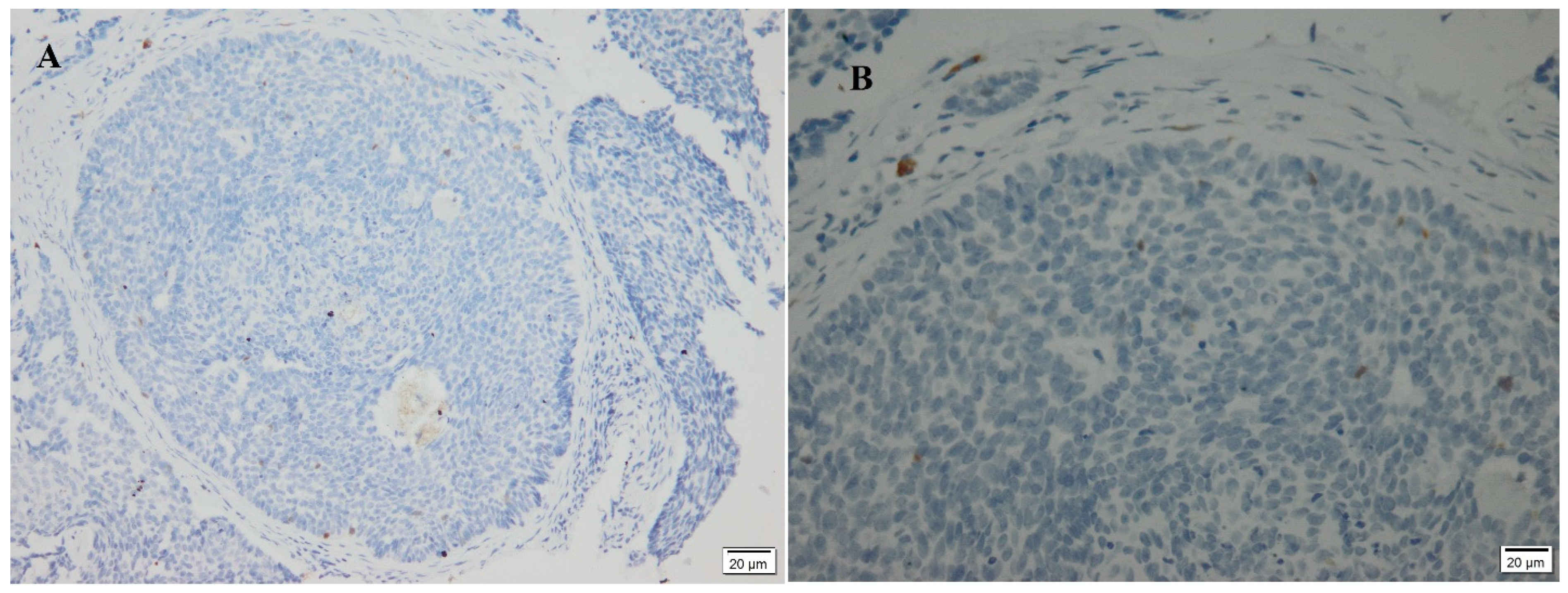
3.4. P16 Immunostaining
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sobjanek, M.; Zabłotna, M.; Szczerkowska-Dobosz, A.; Ruckemann-Dziurdzińska, K.; Sokolowska-Wojdylo, M.; Nowicki, R. –2518 A/G MCP-1 but not –403 G/A RANTES gene polymorphism is associated with enhanced risk of basal cell carcinoma. Postep. Dermatol. Allergol. 2016, 33, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Eshkoor, S.A.; Ismail, P.; Rahman, S.A.; Oshkour, S.A. p16 Gene Expression in Basal Cell Carcinoma. Arch. Med. Res. 2008, 39, 668–673. [Google Scholar] [CrossRef]
- Gallagher, R.P.; Hill, G.B.; Bajdik, C.D.; Fincham, S.; Coldman, A.J.; McLean, D.I.; Threlfall, W.J. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer: I. Basal cell carcinoma. Arch. Dermatol. 1995, 131, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Neale, R.E.; Davis, M.; Pandeya, N.; Whiteman, D.C.; Green, A.C. Basal cell carcinoma on the trunk is associated with excessive sun exposure. J. Am. Acad. Dermatol. 2007, 56, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, M.; Whiteman, D.C.; Rosendahl, C.; Johns, R.; Hackett, T.; Cameron, A.; Waterhouse, M.; Lucas, R.M.; Kimlin, M.G.; Neale, R.E. NHMRC Centre of Research Excellence in Sun and Health. Basal cell carcinomas on sun-protected vs. sun-exposed body sites: A comparison of phenotypic and environmental risk factors. Photodermatol. Photoimmunol. Photomed. 2015, 31, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Donati, P.; Paolino, G.; Panetta, C.; Cota, C.; Zaccarini, M.; Muscardin, L. Another point of view on p16 and Ki67 expression in melanocytic and non-melanocytic cutaneous lesions. Acta Dermatovenerol. Croat. 2013, 21, 149–154. [Google Scholar]
- Cretnik, M.; Poje, G.; Musani, V.; Kruslin, B.; Ozretic, P.; Tomas, D.; Situm, M.; Levanat, S. Involvement of p16 and PTCH in pathogenesis of melanoma and basal cell carcinoma. Int. J. Oncol. 2009, 34, 1045–1050. [Google Scholar]
- Ramezani, M.; Abdali, E.; Khazaei, S.; Vaisi-Raygani, A.; Sadeghi, M. P16INK4a Immunostaining but Lack of Human Papilloma Virus Type 16 in Cutaneous Squamous Cell Carcinoma and Basal Cell Carcinoma: A Report from West Iran. Asian Pac. J. Cancer Prev. 2016, 17, 1093–1096. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.S.; Karnezis, A.N.; Jordan, S.; Singh, N.; McAlpine, J.N.; Gilks, C.B. p16 Immunostaining Allows for Accurate Subclassification of Vulvar Squamous Cell Carcinoma into HPV-Associated and HPV-Independent Cases. Int. J. Gynecol. Pathol. 2016, 35, 385–393. [Google Scholar] [CrossRef]
- Sherr, C.J. The INK4a/ARF network in tumor suppression. Nat. Rev. Mol. Cell Biol. 2001, 2, 731–737. [Google Scholar] [CrossRef]
- Bernard, H.U.; Burk, R.D.; Chen, Z.; van Doorslaer, K.; zur Hausen, H.; de Villiers, E.M. Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments. Virology 2010, 401, 70–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jablonska, S.; Dobrowolski, J.; Jakubowicz, K. Epidermodysplasia Verruciformis as a model in studies on the role of papillo-maviruses in oncogenesis. Cancer Res. 1972, 32, 583–589. [Google Scholar] [PubMed]
- Zakrzewska, K.; Regalbuto, E.; Pierucci, F.; Arvia, R.; Mazzoli, S.; Gori, A.; de Giorgi, V. Pattern of HPV infection in basal cell carcinoma and in perilesional skin biopsies from immunocompetent patients. Virol. J. 2012, 9, 309. [Google Scholar] [CrossRef] [Green Version]
- Correa, R.M.; Vladimirsky, S.; Heideman, D.A.; Coringrato, M.; Abeldaño, A.; Olivares, L.; Del Aguila, R.; Alonio, L.V.; Snijders, P.J.; Picconi, M.A. Cutaneous human papillomavirus genotypes in different kinds of skin lesions in Argentina. J. Med. Virol. 2017, 89, 352–357. [Google Scholar] [CrossRef]
- Mesbah, A.; Rajabi, P.; Rajabi, M.A.; Chehrei, A.; Mougouei, K.; Mokhtari, M. Determination of the relationship between basal cell carcinoma and human papilloma virus, based on immunohistochemistry staining method. Indian J. Dermatol. 2009, 54, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Roewert-Huber, J.; Lange-Asschenfeldt, B.; Stockfleth, E.; Kerl, H. Epidemiology and etiology of basal cell carcinoma. Br. J. Derm. 2007, 157, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Bartoš, V. Expression of p16 Protein in Cutaneous Basal Cell Carcinoma: Still Far from Being Clearly Understood. Acta Dermatovenerol. Croat. 2020, 28, 43–44. [Google Scholar]
- Conscience, I.; Jovenin, N.; Coissard, C.; Lorenzato, M.; Durlach, A.; Grange, F.; Birembaut, P.; Clavel, C.; Bernard, P. P16 is overexpressed in cutaneous carcinomas located on sun-exposed areas. Eur. J. Dermatol. 2006, 16, 518–522. [Google Scholar]
- Paolini, F.; Carbone, A.; Benevolo, M.; Silipo, V.; Rollo, F.; Covello, R.; Piemonte, P.; Frascione, P.; Capizzi, R.; Catricalà, C.; et al. Human Papillomaviruses, p16INK4a and Akt expression in basal cell carcinoma. J. Exp. Clin. Cancer Res. 2011, 30, 108. [Google Scholar] [CrossRef] [Green Version]
- Villada, G.; Kryvenko, O.N.; Campuzano-Zuluaga, G.; Kovacs, C.; Chapman, J.; Gomez-Fernandez, C. A limited immunohisto-chemical panel to distinguish basal cell carcinoma of cutaneous origin from basaloid squamous cell carcinoma of the head and neck. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 126–131. [Google Scholar] [CrossRef]
- Nindl, I.; Meyer, T.; Schmook, T.; Ulrich, C.; Ridder, R.; Audring, H.; Sterry, W.; Stockfleth, E. Human papillomavirus and overex-pression of P16INK4a in nonmelanoma skin cancer. Dermol. Surg 2004, 30, 409–414. [Google Scholar]
- Hussein, M.; Ahmed, A. Expression Profile of CD10, BCL-2, p63, and EMA in the Normal Skin and Basal Cell Carcinomas: An Immunohistochemical Reappraisal. Actas Dermo-Sifiliogr. 2022, 113, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, N.; Simonacci, F.; Greco, M.P.; Grignaffini, E.; Raposio, E. Single center evidence for the treatment of basal cell carcinoma of the head and neck. Acta Bio-Med. Atenei Parm. 2019, 90, 77. [Google Scholar] [CrossRef]
- Linos, E.; Chren, M.-M. Active Surveillance as a Management Option for Low-risk Basal Cell Carcinoma. JAMA Intern. Med. 2021, 181, 1032–1033. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Rabie, A.; Elhussiny, M.; Nasr, M.; Kamel, M.I.; Hegab, A.; El-Kady, A.S.; Nagaty, M.E.; Seleem, A.; Abbas, M.; et al. Recurrent cutaneous basal cell carcinoma after surgical excision: A retrospective clinicopathological study. Ann. Med. Surg. 2022, 78, 103877. [Google Scholar] [CrossRef]
- Dyalram, D.; Caldroney, S.; Heath, J. Margin Analysis: Cutaneous malignancy of the head and neck. Oral Maxillofac. Surg. Clin. 2017, 29, 341–353. [Google Scholar] [CrossRef]
- Rogers, H.W.; Weinstock, M.A.; Harris, A.R.; Hinckley, M.R.; Feldman, S.; Fleischer, A.B.; Coldiron, B.M. Incidence Estimate of Nonmelanoma Skin Cancer in the United States, 2006. Arch. Dermatol. 2010, 146, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.K.; Kopf, A.W.; Bart, R.S.; Grin, C.M.; Levenstein, M.S. Recurrence rates of treated basal cell carcinomas: Part 3: Surgical excision. J. Dermatol. Surg. Oncol. 1992, 18, 471–476. [Google Scholar] [CrossRef]
- Armstrong, L.T.; Magnusson, M.R.; Guppy, M.P. Risk factors for recurrence of facial basal cell carcinoma after surgical excision: A follow-up analysis. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1738–1745. [Google Scholar] [CrossRef]
- Armstrong, B.K.; Kricker, A. The epidemiology of UV induced skin cancer. J. Photochem. Photobiol. B 2001, 63, 8–18. [Google Scholar] [CrossRef]
- Bernier, M.A.; Rivas-Ruiz, F.; Martín, M.D.T.; Sánchez, N.B. Comparative epidemiological study of non-melanoma skin cancer between Spanish and north and central European residents on the Costa del Sol. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Pyne, J.; Mint, E.; Barr, E.; Clark, S.; Hou, R. Basal cell carcinoma: Variation in invasion depth by subtype, sex, and anatomic site in 4565 cases. Dermatol. Pract. Concept. 2018, 8, 314. [Google Scholar] [CrossRef]
- Subramaniam, P.; Olsen, C.; Thompson, B.; Whiteman, D.; Neale, R.; QSkin Sun and Health Study Investigators. Anatomical Distributions of Basal Cell Carcinoma and Squamous Cell Carcinoma in a Population-Based Study in Queensland, Australia. JAMA Dermatol. 2017, 153, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orth, G. Genetics of epidermodysplasia verruciformis: Insights into host defense against papillomaviruses. Semin. Immunol. 2006, 18, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Lear, J.T.; Smith, A.G.; Bowers, B.; Heagearty, A.H.; Jones, P.W.; Gilford, J.; Alladersea, J.; Strange, R.C.; Fryer, A.A. Truncal Tumor Site Is Associated with High Risk of Multiple Basal Cell Carcinoma and Is Influenced by Glutathione S-Transferase, GSTT1, and Cytochrome P450, CYP1A1 Genotypes, and Their Interaction. J. Investig. Dermatol. 1997, 108, 519–522. [Google Scholar] [CrossRef] [Green Version]
- Scrivener, Y.; Grosshans, E.; Cribier, B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br. J. Dermatol. 2002, 147, 41–47. [Google Scholar] [CrossRef]
- Pelucchi, C.; Di Landro, A.; Naldi, L.; La Vecchia, C. Risk Factors for Histological Types and Anatomic Sites of Cutaneous Basal-Cell Carcinoma: An Italian Case–Control Study. J. Investig. Dermatol. 2007, 127, 935–944. [Google Scholar] [CrossRef] [Green Version]
- Svensson, S.; Nilsson, K.; Ringberg, A.; Landberg, G. Invade or proliferate? Two contrasting events in malignant behavior gov-erned by p16INK4a and an intact Rb pathway illustrated by a model system of basal cell carcinoma. Cancer Res. 2003, 63, 1737–1742. [Google Scholar]
- Soyer, H.P.; Rigel, D.S.; Wurm, E.M. Dermatology, 3rd ed.; Bolognia, J.L., Jorizzo, J.L., Schaffer, J.V., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2012; pp. 1773–1793. [Google Scholar]
- Straume, O.; Sviland, L.; Akslen, L. Loss of nuclear p16 protein expression correlates with increased tumor cell proliferation (Ki-67) and poor prognosis in patients with vertical growth phase melanoma. Clin. Cancer Res. 2000, 6, 1845–1853. [Google Scholar]
- Bartoš, V.; Pokorný, D.; Zacharová, O.; Haluska, P.; Doboszová, J.; Kullová, M.; Adamicová, K.; Péč, M.; Péč, J. Recurrent basal cell carcinoma: A clinicopathological study and evaluation of histomorphological findings in primary and recurrent lesions. Acta Dermatovenerol. APA 2011, 20, 67–75. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sun-Protected (n = 23) | Sun-Exposed (n = 29) | p-Value | ||
|---|---|---|---|---|
| Demographic data | ||||
| Age, mean (SD) | 67.2 (10.25) | 62.7 (14.35) | 0.216 | |
| Sex, no. (%) | Female | 13 (56.5) | 18 (62) | 0.69 |
| Male | 10 (43.5) | 11 (37.9) | ||
| Clinical data | ||||
| Clinical diagnosis, no. (%) | BCC | 8 (34.8) | 16 (55.2) | 0.17 f |
| Other than BCC | 15 (65.2) | 13 (44.8) | ||
| Tumor size in mm, mean (SD) | 13.1 (8.8) | 13.7 (9.6) | 0.81 | |
| Recurrent state, no. (%) | Recurrent | 1 (4.3) | 3 (10.3) | 0.06 f |
| Not recurrent | 22 (95.7) | 26 (89.7) | ||
| Histopathological examination | ||||
| Histological, variant, no. (%) | BCC nodular | 18 (78.2) | 23 (79.3) | 0.31 m |
| BCC Superficial | 4 (17.4) | 5 (17.3) | ||
| BCC adenoid | 0 (0) | 1 (3.4) | ||
| BCC keratotic | 1 (4.3) | 0 (0) | ||
| P16 status | ||||
| P16 immunostaining, no. (%) | Negative | 9 (39.1) | 15 (51.7) | 0.37 |
| Positive | 14 (60.9) | 14 (48.3) | ||
| P16 expression, categories, no. (%) | Strong positive | 1 (4.3) | 4 (13.8) | 0.27 m |
| Moderate | 12 (52.2) | 9 (31.1) | ||
| Weak | 1 (4.3) | 1 (3.4) | ||
| None | 9 (39.2) | 15 (51.7) | ||
| P16+ | P16− | p-Value | ||
|---|---|---|---|---|
| Age | <50 years old | 3 | 2 | 0.1 f |
| ≥50 years old | 25 | 22 | ||
| Total | 28 | 24 | 52 | |
| Sex | Female | 17 | 14 | 0.86 |
| Male | 11 | 10 | ||
| Total | 28 | 24 | 52 | |
| Recurrence | Yes | 0 | 4 | 0.039 * f |
| No | 28 | 20 | ||
| Total | 28 | 24 | 52 | |
| Tumor size | <20 mm | 21 | 20 | 0.46 m |
| ≥20 mm | 7 | 4 | ||
| Total | 28 | 24 | 52 | |
| Histological variant | Nodular | 22 | 13 | 0.061 |
| Non-nodular | 6 | 11 | ||
| Total | 28 | 24 | 52 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasan, A.; Kandil, A.M.; Al-Ghamdi, H.S.; Alghamdi, M.A.; Nasr, M.; Naeem, S.A.; Abd-Elhay, W.M.; Mohamed, O.K.E.; Ibrahim, H.S.A.; Ahmed, E.M.; et al. Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining. Diagnostics 2023, 13, 1271. https://doi.org/10.3390/diagnostics13071271
Hasan A, Kandil AM, Al-Ghamdi HS, Alghamdi MA, Nasr M, Naeem SA, Abd-Elhay WM, Mohamed OKE, Ibrahim HSA, Ahmed EM, et al. Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining. Diagnostics. 2023; 13(7):1271. https://doi.org/10.3390/diagnostics13071271
Chicago/Turabian StyleHasan, Abdulkarim, Ahmad M. Kandil, Hasan S. Al-Ghamdi, Mohammad A. Alghamdi, Mohamed Nasr, Suhaib Alsayed Naeem, Wagih M. Abd-Elhay, Osama Khalil E. Mohamed, Hany Sabry A. Ibrahim, Eman Mohamed Ahmed, and et al. 2023. "Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining" Diagnostics 13, no. 7: 1271. https://doi.org/10.3390/diagnostics13071271
APA StyleHasan, A., Kandil, A. M., Al-Ghamdi, H. S., Alghamdi, M. A., Nasr, M., Naeem, S. A., Abd-Elhay, W. M., Mohamed, O. K. E., Ibrahim, H. S. A., Ahmed, E. M., Abdrabo, A. E. M., & Elgohary, S. A. (2023). Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining. Diagnostics, 13(7), 1271. https://doi.org/10.3390/diagnostics13071271