
Predictive Factors for Pediatric Craniopharyngioma Recurrence: An Extensive Narrative Review

 , , , , ,
, , , , ,  ,
,  and
and 
Abstract
:1. Introduction
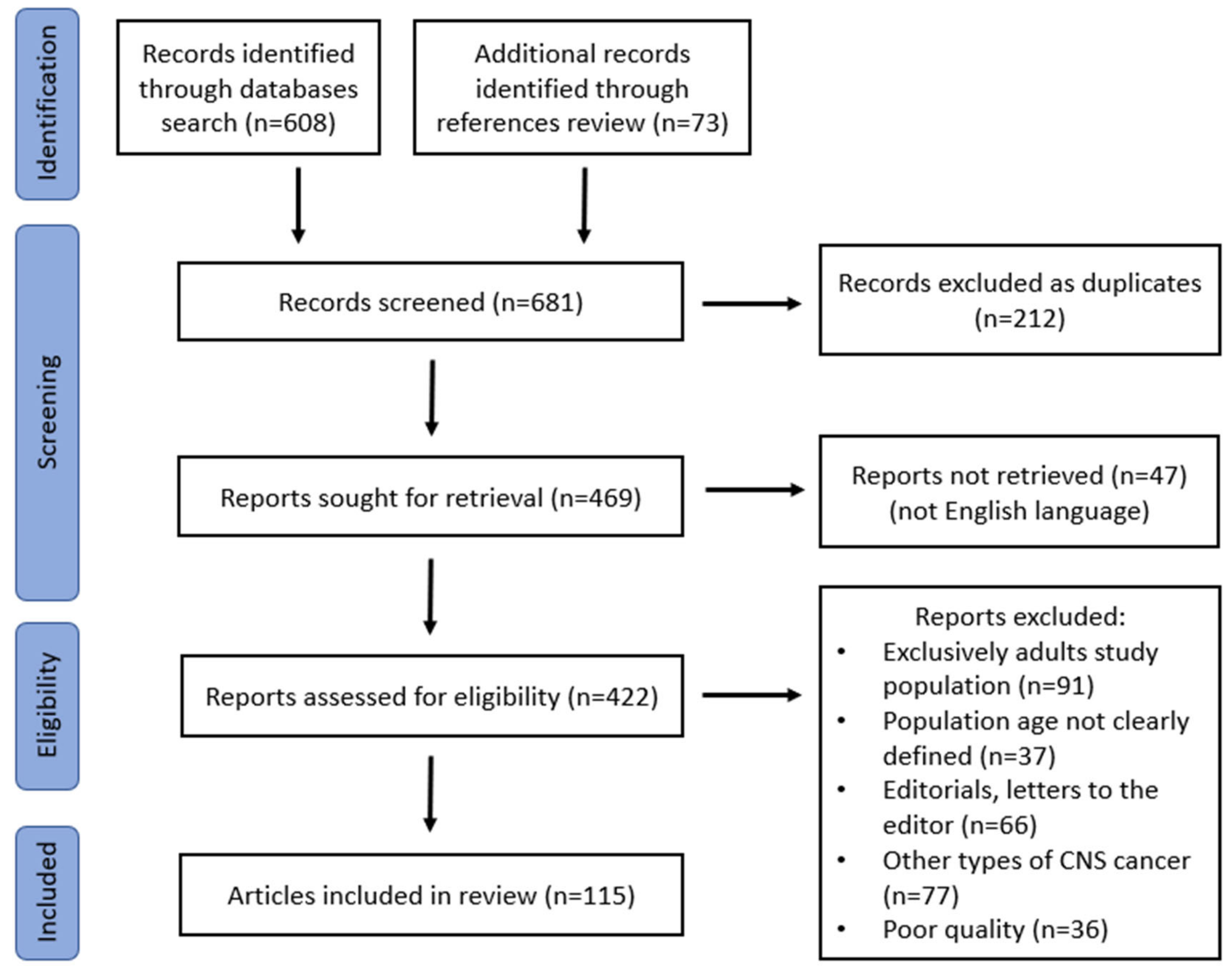
2. Materials and Methods
3. Results
4. Discussion
4.1. Epidemiological Characteristics and Recurrence
4.2. Morphological Features of the Tumor and Recurrence Rate

{kind=link}
| Category | Risk Factor | Association Found | Study |
|---|---|---|---|
| Epidemiological features | Younger age | Increases the risk | Rajan et al. [25], De Vile et al. [23] Fisher et al. [40], Gautier et al. [24], Šteňo et al. [46], Drimtzias et al. [47] |
| No association | Duff et al. [32], Lena et al. [48], Al Shail et al. [49] | ||
| Male sex | Increases the risk | Gautier et al. [24], Mortini et al. [22] | |
| No association | Kim et al. [14], Lena et al. [48], Tena-Suck et al. [30], Tomita et al. [29], Al Shail et al. [49] | ||
| Morphological features | Large size | Increases the risk | Hetelekidis et al. [19], de Vile et al. [23], Elliot et al. [15] Gupta et al. [26], Shi et al. [41], Weiner et al. [27], Yosef et al. [50], Kobayashi et al. [51] |
| Tumor location [e.g., third ventricle involvement] | Increases the risk | Kim et al. [14], Fahlbusch et al. [28], Tomita et al. [29], Van Effenterre et al. [18], Kim et al. [14] | |
| Tumor adherence to surrounding tissues | Increases the risk | Fahlbusch et al. [28], Tomita et al. [29], Karavitaki et al. [1], Pan et al. [57], Pascual et al. [55], Pascual et al. [58], Shi et al. [41], Effenterre et al. [18] | |
| Cystic tumor consistency | Increases the risk | Gupta et al. [26], Lee et al. [60], Prieto et al. [16] | |
| Clinical presentation | Hydrocephalus (increased ICP) | Increases the risk | Prieto et al. [16], DeVile et al. [23], Gautier et al. [24] |
| Some association | Kim et al. [14], Tomita et al. [29], Gupta et al. [26], Al Shail et al. [49], Poretti et al. [9], Liubinas et al. [61], Fahlbusch et al. [28] | ||
| No association | Duff et al. [32], Karavitaki et al. [1], Kim et al. [14], Puget et al. [44] | ||
| Visual disturbances at presentation | Increases the risk | Duff et al. [32], Lee et al. [62] | |
| No association | Shail et al. [49], Tena-Suck et al. [30], Drimtzias et al. [47] | ||
| Hypothalamic involvement | Some association | Vinchon et al. [33], De Vile et al. [23], Poretti et al. [9] | |
| Decreases the risk | Gautier et al. [24] | ||
| Hormonal-related symptoms | Increases the risk | Tena-suck et al. [30], Rogers et al. [63], Erfurth et al. [64] | |
| Better outcome | Gautier et al. [24] | ||
| Histological features | Adamantinomatous vs. papillary CP | Adamantinomatous increases recurrence risk | Adamson et al. [65], Szeifert et al. [66], Crotty et al. [67], Tavangar et al. [68] |
| No difference between the two types | Duff et al. [32], Eldevik et al. [69], Gupta et al. [26], Kim et al. [14], Minamida et al. [70], Tena-Suck et al. [30], Weiner et al. [27], Prieto et al. [16], Agozzino et al. [35], Zygourakis et al. [71] | ||
| Presence of finger-like epithelial protrusions | Increases the risk | Adamson et al. [65], Weiner et al. [27] | |
| No association | Duff et al. [32], Gupta et al. [26], Tena-Suck et al. [30] | ||
| Presence of whorl-like arrays | Increases the risk | Stache et al. [31], Tena-Suck et al. [30], | |
| Intense reactive peritumoral gliosis | Possible risk increase | Pascual et al. [58], Qi et al. [57], Weiner et al. [27], Bartlett [72] | |
| Possible positive effect on number of recurrences | Vile et al. [23], Minamida et al. [70], Tomita et al. [29], Weiner et al. [27], Adamson et al. [65], Prieto et al. [16] | ||
| Molecular features | High Ki-67 expression | Increases the risk | Nishi et al. [73], Rodriguez et al. [34], Prieto et al. [16], Raghavan et al. [74], Izumoto et al. [75], Anegawa et al. [76], Guadagno et al. [77], Xu et al. [78] |
| No association | Agozzino et al. [35], Kim et al. [14], Park et al. [79], Losa et al. [80], Duo et al. [81], Raghavan et al. [74], Yalçın et al. [82], Moszczyńska et al. [83] | ||
| p53 gene loss of function | Increases the risk | Tena-Suck et al. [30] | |
| Possible association | Ishida et al. [36], Lefranc et al. [39], Prieto et al. [16], Ujifuku et al. [84] | ||
| No association | Momota et al. [85], Yalcin et al. [82] | ||
| Vascular endothelial growth factor (VEGF) | Increases the risk | Liu et al. [86], Sun et al. [87], Agozzino et al. [35], Xia et al. [88], Elmaci et al. [37] | |
| No association | Xu et al. [89] | ||
| Expression of RAR isotypes and cathepsins | RARγ increases the risk | Lubansu et al. [38], Lefranc et al. [39] | |
| Hormones and their receptors | Possible association | Hofmann et al. [90], Li et al. [91] | |
| No association | Martínez-Ortega et al. [92] | ||
| Therapeutic approach | Presence of tumor remnants after excision | Increases the risk | Amendola et al. [93], Baskin et al. [94], Cabezudo et al. [95], Carmel et al. [96], Crotty et al. [67], De Vile et al. [23], Duff et al. [32], Elliot et al. [15], Fahlbusch et al. [28], Eldevik et al. [69], Gautier et al. [24], Gupta et al. [26], Hetelekidis et al. [19], Hoffman et al. [13], Karavitaki et al. [1], Khafaga et al. [97], Lena et al. [48], Mortini et al. [22], Puget et al. [44], Schoenfeld et al. [20], Shi et al. [41], Tena-Suck et al. [30], Thompson et al. [98], Tomita et al. [29], Van Effenterre et al. [18], Weiner et al. [27], Yasargil et al. [99], Zuccaro et al. [100] |
| Neurosurgical team expertise | Affects the recurrence rate | Mortini et al. [101], Bao et al. [102], Yosef et al. [50], Zygourakis et al. [71], Prieto et al. [16], Tavangar et al. [68] | |
| Use of radiotherapy after subtotal surgical removal | Decreases the risk | Baskin et al. [94], Cabezudo et al. [95], Carmel et al. [96], Crotty et al. [67], De Vile et al. [23], Duff et al. [32], Eldevik et al. [69], Fisher et al. [40], Hetelekidis et al. [19], Karavitaki et al. [1], Khafaga et al. [97], Mortini et al. [22], Richmond et al. [103], Schoenfeld et al. [20], Stahnke et al. [104], Thompson et al. [98], Tomita et al. [29], Thomsett et al. [105], Weiss et al. [106], Wen et al. [107], Amendola et al. [93], Enayet et al. [108], Stripp et al. [109] | |
| Presence of calcifications | Increases the risk | Fahlbusch et al. [28], Fisher et al. [40], Zhang et al. 2008 [110], Cheng et al. [111] | |
| No association | Elliott et al. [42], Drimtzias et al. [47] | ||
| Use of GH replacement therapy | Increases the risk | Taguchi et al. [112], Niu et al. [113] | |
| No association | Arslanian et al. [114], Olsson et al. [115], Kanev et al. [116], Moshang [43], Karavitaki et al. [117], Rohrer et al. [118], Boekhoff et al. [119], Boguszewski et al. [120], Puget et al. [44], Kim et al. [14], Elliott et al. [15], Clayton et al. [121], Child et al. [122], Darendeliler et al. [45], Moshang et al. [123], Price et al. [124], Smith et al. [125] | ||
| Decreases the risk | Alotaibi et al. [126] |
4.3. Clinical Presentation at Initial Diagnosis and Recurrence
4.4. Histological Features of the Tumor and Recurrence
4.5. Molecular Features of the Tumor and Recurrence
4.6. Therapeutic Approach and Tumor Recurrence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karavitaki, N.; Brufani, C.; Warner, J.T.; Adams, C.B.T.; Richards, P.; Ansorge, O.; Shine, B.; Turner, H.E.; Wass, J.A.H. Craniopharyngiomas in children and adults: Systematic analysis of 121 cases with long-term follow-up. Clin. Endocrinol. 2005, 62, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Larkin, S.; Karavitaki, N. Recent advances in molecular pathology of craniopharyngioma. F1000Research 2017, 6, 1202. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Karavitaki, N.; Wass, J.A.H. Craniopharyngiomas. Endocrinol. Metab. Clin. N. Am. 2008, 37, 173–193. [Google Scholar] [CrossRef]
- Marszałek, A.; Szylberg, L.; Wiśniewski, S. Pathologic aspects of skull base tumors. Rep. Pract. Oncol. Radiother. 2016, 21, 288–303. [Google Scholar] [CrossRef]
- Gong, J.; Zhang, H.; Xing, S.; Li, C.; Ma, Z.; Jia, G.; Hu, W. High expression levels of CXCL12 and CXCR4 predict recurrence of adamanti-nomatous craniopharyngiomas in children. Cancer Biomark. 2014, 14, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.L.; Merchant, T.E.; Warmuth-Metz, M.; Martinez-Barbera, J.P.; Puget, S. Craniopharyngioma. Nat. Rev. Dis. Primers 2019, 5, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Sughrue, M.E.; Yang, I.; Kane, A.J.; Fang, S.; Clark, A.J.; Aranda, D.; Barani, I.J.; Parsa, A.T. Endocrinologic, neurologic, and visual morbidity after treatment for craniopharyngioma. J. Neuro-Oncol. 2010, 101, 463–476. [Google Scholar] [CrossRef]
- Poretti, A.; Grotzer, M.A.; Ribi, K.; Schönle, E.; Boltshauser, E. Outcome of craniopharyngioma in children: Long-term complications and quality of life. Dev. Med. Child Neurol. 2004, 6, 220–229. [Google Scholar]
- Yuen, K.C.J.; Mattsson, A.F.; Burman, P.; Erfurth, E.-M.; Camacho-Hubner, C.; Fox, J.L.; Verhelst, J.; Geffner, M.E.; Abs, R. Relative Risks of Contributing Factors to Morbidity and Mortality in Adults with Craniopharyngioma on Growth Hormone Replacement. J. Clin. Endocrinol. Metab. 2018, 103, 768–777. [Google Scholar] [CrossRef]
- Wijnen, M.; Olsson, D.S.; Van Den Heuvel-Eibrink, M.M.; Hammarstrand, C.; Janssen, J.A.M.J.L.; van der Lely, A.J.; Johannsson, G.; Neggers, S.J.C.M.M. Excess morbidity and mortality in patients with craniopharyngioma: A hospital-based retrospective cohort study. Eur. J. Endocrinol. 2018, 178, 93–102. [Google Scholar] [CrossRef]
- Cohen, M.; Guger, S.; Hamilton, J. Long Term Sequelae of Pediatric Craniopharyngioma—Literature Review and 20 Years of Experience. Front. Endocrinol. 2011, 2, 81. [Google Scholar] [CrossRef]
- Hoffman, H.J.; De Silva, M.; Humphreys, R.P.; Drake, J.M.; Smith, M.L.; Blaser, S.I. Aggressive surgical management of craniopharyngiomas in children. J. Neurosurg. 1992, 76, 47–52. [Google Scholar] [CrossRef]
- Kim, S.-K.; Wang, K.-C.; Shin, S.-H.; Choe, G.; Chi, J.G.; Cho, B.-K. Radical excision of pediatric craniopharyngioma: Recurrence pattern and prognostic factors. Child’s Nerv. Syst. 2001, 17, 531–536. [Google Scholar] [CrossRef]
- Elliott, R.E.; Hsieh, K.; Hochman, T.; Belitskaya-Levy, I.; Wisoff, J.; Wisoff, J.H. Efficacy and safety of radical resection of primary and recurrent craniopharyngiomas in 86 children. J. Neurosurg. Pediatr. 2010, 5, 30–48. [Google Scholar] [CrossRef] [PubMed]
- Prieto, R.; Pascual, J.M.; Subhi-Issa, I.; Jorquera, M.; Yus, M.; Martínez, R. Predictive Factors for Craniopharyngioma Recurrence: A Systematic Review and Illustrative Case Report of a Rapid Recurrence. World Neurosurg. 2013, 79, 733–749. [Google Scholar] [CrossRef] [PubMed]
- Coury, J.R.; Davis, B.N.; Koumas, C.P.; Manzano, G.S.; Dehdashti, A.R. Histopathological and molecular predictors of growth patterns and recurrence in craniopharyngiomas: A systematic review. Neurosurg. Rev. 2020, 43, 41–48. [Google Scholar] [CrossRef]
- Van Effenterre, R.; Boch, A.-L. Craniopharyngioma in adults and children: A study of 122 surgical cases. J. Neurosurg. 2002, 97, 3–11. [Google Scholar] [CrossRef]
- Hetelekidis, S.; Barnes, P.D.; Tao, M.L.; Fischer, E.G.; Schneider, L.; Scott, R.; Tarbell, N.J. 20-Year experience in childhood craniopharyngioma. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.; Pekmezci, M.; Barnes, M.J.; Tihan, T.; Gupta, N.; Lamborn, K.R.; Banerjee, A.; Mueller, S.; Chang, S.; Berger, M.S.; et al. The superiority of conservative resection and adjuvant radiation for craniopharyngiomas. J. Neuro-Oncol. 2012, 108, 133–139. [Google Scholar] [CrossRef]
- Clark, A.J.; Cage, T.A.; Aranda, D.; Parsa, A.T.; Sun, P.P.; Auguste, K.I.; Gupta, N. A systematic review of the results of surgery and radiotherapy on tumor control for pediatric craniopharyngioma. Child’s Nerv. Syst. 2012, 29, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Mortini, P.; Losa, M.; Pozzobon, G.; Barzaghi, R.; Riva, M.; Acerno, S.; Angius, D.; Weber, G.; Chiumello, G.; Giovanelli, M.; et al. Neurosurgical treatment of craniopharyngioma in adults and children: Early and long-term results in a large case series. J. Neurosurg. 2011, 114, 1350–1359. [Google Scholar] [CrossRef]
- De Vile, C.J.; Grant, D.B.; Kendall, B.E.; Neville, B.G.R.; Stanhope, R.; Watkins, K.E.; Hayward, R.D. Management of childhood craniopharyngioma: Can the morbidity of radical surgery be predicted? J. Neurosurg. 1996, 85, 73–81. [Google Scholar] [CrossRef]
- Gautier, A.; Godbout, A.; Grosheny, C.; Tejedor, I.; Coudert, M.; Courtillot, C.; Jublanc, C.; De Kerdanet, M.; Poirier, J.-Y.; Riffaud, L.; et al. Markers of Recurrence and Long-Term Morbidity in Craniopharyngioma: A Systematic Analysis of 171 Patients. J. Clin. Endocrinol. Metab. 2012, 97, 1258–1267. [Google Scholar] [CrossRef]
- Rajan, B.; Ashley, S.; Gorman, C.; Jose, C.; Horwich, A.; Bloom, H.; Marsh, H.; Brada, M. Craniopharyngioma—A long-term results following limited surgery and radiotherapy. Radiother. Oncol. 1993, 26, 1–10. [Google Scholar] [CrossRef]
- Gupta, D.K.; Ojha, B.K.; Sarkar, C.; Mahapatra, A.K.; Sharma, B.S.; Mehta, V.S. Recurrence in pediatric craniopharyngiomas: Analysis of clinical and histological features. Child’s Nerv. Syst. 2006, 22, 50–55. [Google Scholar] [CrossRef]
- Weiner, H.L.; Wisoff, J.H.; Rosenberg, M.E.; Kupersmith, M.J.; Cohen, H.; Zagzag, D.; Shiminski-Maher, T.; Flamm, E.S.; Epstein, F.J.; Miller, D.C. Craniopharyngiomas: A clinicopathological analysis of factors predictive of recurrence and functional outcome. Neurosurgery 1994, 35, 1001–1011. [Google Scholar] [CrossRef]
- Fahlbusch, R.; Honegger, J.; Paulus, W.; Huk, W.; Buchfelder, M. Surgical treatment of craniopharyngiomas: Experience with 168 patients. J. Neurosurg. 1999, 90, 237–250. [Google Scholar] [CrossRef]
- Tomita, T.; Bowman, R.M. Craniopharyngiomas in children: Surgical experience at Children’s Memorial Hospital. Child’s Nerv. Syst. 2005, 21, 729–746. [Google Scholar] [CrossRef] [PubMed]
- Tena-Suck, M.L.; Salinas-Lara, C.; Arce-Arellano, R.I.; Rembao-Bojórquez, D.; Morales-Espinosa, D.; Sotelo, J.; Arrieta, O. Clinico-pathological and immunohistochemical characteristics associated to recurrence/regrowth of craniopharyngiomas. Clin. Neurol. Neurosurg. 2006, 108, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Stache, C.; Hölsken, A.; Schlaffer, S.-M.; Hess, A.; Metzler, M.; Frey, B.; Fahlbusch, R.; Flitsch, J.; Buchfelder, M.; Buslei, R. Insights into the Infiltrative Behavior of Adamantinomatous Craniopharyngioma in a New Xenotransplant Mouse Model. Brain Pathol. 2015, 25, 1–10. [Google Scholar] [CrossRef]
- Duff, J.M.; Meyer, F.B.; Ilstrup, D.M.; Laws, E.R.; Schleck, C.D.; Scheithauer, B.W. Long-term Outcomes for Surgically Resected Craniopharyngiomas. Neurosurgery 2000, 46, 291–305. [Google Scholar] [CrossRef]
- Vinchon, M.; Dhellemmes, P. Craniopharyngiomas in children: Recurrence, reoperation and outcome. Child’s Nerv. Syst. 2008, 24, 211–217. [Google Scholar] [CrossRef]
- Rodriguez, F.J.; Scheithauer, B.W.; Tsunoda, S.; Kovacs, K.; Vidal, S.; Piepgras, D.G. The Spectrum of Malignancy in Craniopharyngioma. Am. J. Surg. Pathol. 2007, 31, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Agozzino, L.; Ferraraccio, F.; Accardo, M.; Esposito, S.; Agozzino, M.; Cuccurullo, L. Morphological and Ultrastructural Findings of Prognostic Impact in Craniopharyngiomas. Ultrastruct. Pathol. 2006, 30, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Ishida, M.; Hotta, M.; Tsukamura, A.; Taga, T.; Kato, H.; Ohta, S.; Takeuchi, Y.; Nakasu, S.; Okabe, H. Malignant transformation in craniopharyngioma after radiation therapy: A case report and review of the literature. Clin. Neuropathol. 2010, 29, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Elmaci, L.; Kurtkaya-Yapicier, O.; Ekinci, G.; Sav, A.; Pamir, M.N.; Vidal, S.; Kovacs, K.; Scheithauer, B.W. Metastatic papillary craniopharyngioma: Case study and study of tumor angiogenesis. Neuro-Oncology 2002, 4, 123–128. [Google Scholar] [CrossRef]
- Lubansu, A.; Ruchoux, M.-M.; Brotchi, J.; Salmon, I.; Kiss, R.; Lefranc, F. Cathepsin B, D and K expression in adamantinomatous craniopharyngiomas relates to their levels of differentiation as determined by the patterns of retinoic acid receptor expression. Histopathology 2003, 43, 563–572. [Google Scholar] [CrossRef]
- Lefranc, F.; Mijatovic, T.; Decaestecker, C.; Kaltner, H.; André, S.; Brotchi, J.; Salmon, I.; Gabius, H.-J.; Kiss, R. Monitoring the Expression Profiles of Integrins and Adhesion/Growth-regulatory Galectins in Adamantinomatous Craniopharyngiomas: Their Ability to Regulate Tumor Adhesiveness to Surrounding Tissue and Their Contribution to Prognosis. Neurosurgery 2005, 56, 763–775. [Google Scholar] [CrossRef]
- Fisher, P.G.; Jenab, J.; Goldthwaite, P.T.; Tihan, T.; Wharam, M.D.; Foer, D.R.; Burger, P.C. Outcomes and failure patterns in childhood craniopharyngiomas. Child’s Nerv. Syst. 1998, 14, 558–563. [Google Scholar] [CrossRef]
- Shi, X.-E.; Wu, B.; Fan, T.; Zhou, Z.-Q.; Zhang, Y.-L. Craniopharyngioma: Surgical experience of 309 cases in China. Clin. Neurol. Neurosurg. 2008, 110, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.E.; Moshel, Y.A.; Wisoff, J.H. Minimal residual calcification and recurrence after gross-total resection of craniopharyngioma in children. J. Neurosurg. Pediatr. 2009, 3, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Moshang, T. Is brain tumor recurrence increased following growth hormone treatment? Trends Endocrinol. Metab. 1995, 6, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Puget, S.; Garnett, M.; Wray, A.; Grill, J.; Habrand, J.-L.; Bodaert, N.; Zerah, M.; Bezerra, M.; Renier, D.; Pierre-Kahn, A.; et al. Pediatric craniopharyngiomas: Classification and treatment according to the degree of hypothalamic involvement. J. Neurosurg. Pediatr. 2007, 106, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Darendeliler, F.; Karagiannis, G.; Wilton, P.; Ranke, M.B.; Albertsson-Wikland, K.; Price, D.A. Recurrence of brain tumours in patients treated with growth hormone: Analysis of KIGS [Pfizer International Growth Database]. Acta Paediatr. 2006, 95, 1284–1290. [Google Scholar] [CrossRef]
- teňo, J.; Bízik, I.; Šteňo, A.; Matejčík, V. Recurrent craniopharyngiomas in children and adults: Long-term recurrence rate and management. Acta Neurochir. [Wien.] 2014, 156, 113–122. [Google Scholar]
- Drimtzias, E.; Falzon, K.; Picton, S.; Jeeva, I.; Guy, D.; Nelson, O.; Simmons, I. The ophthalmic natural history of paediatric craniopharyngioma: A long-term review. J. Neuro-Oncol. 2014, 120, 651–656. [Google Scholar] [CrossRef]
- Lena, G.; Paredes, A.P.; Scavarda, D.; Giusiano, B. Craniopharyngioma in children: Marseille experience. Child’s Nerv. Syst. 2005, 21, 778–784. [Google Scholar] [CrossRef]
- Al Shail, E.; Al-Shenkiti, A.; Alotaibi, M.T.; Siddiqui, K.; Al-Kofide, A. Excision of pediatric craniopharyngioma: Pattern of recurrence in 35 patients at a tertiary care hospital in Saudi Arabia. Child’s Nerv. Syst. 2020, 36, 297–304. [Google Scholar] [CrossRef]
- Yosef, L.; Ekkehard, K.M.; Shalom, M. Giant craniopharyngiomas in children: Short- and long-term implications. Child’s Nerv. Syst. 2016, 32, 79–88. [Google Scholar] [CrossRef]
- Kobayashi, T.; Tsugawa, T.; Hatano, M.; Hashizume, C.; Mori, Y.; Shibamoto, Y. Gamma knife radiosurgery of craniopharyngioma: Results of 30 cases treated at Nagoya Radiosurgery Center. Nagoya J. Med. Sci. 2015, 77, 447–454. [Google Scholar] [PubMed]
- Pascual, J.M.; Prieto, R. Craniopharyngioma and the Third Ventricle: This Inescapable Topographical Relationship. Front. Oncol. 2022, 12, 872689. [Google Scholar] [CrossRef]
- Müller, H.L.; Gebhardt, U.; Teske, C.; Faldum, A.; Zwiener, I.; Warmuth-Metz, M.; Pietsch, T.; Pohl, F.; Sörensen, N.; Calaminus, G. Post-operative hypothalamic lesions and obesity in childhood craniopharyngioma: Results of the multinational prospective trial KRANIOPHARYNGEOM 2000 after 3-year follow-up. Eur. J. Endocrinol. 2011, 165, 17–24. [Google Scholar] [CrossRef]
- Müller, H.L.; Gebhardt, U.; Faldum, A.; Warmuth-Metz, M.; Pietsch, T.; Pohl, F.; Calaminus, G.; Sörensen, N.; Kraniopharyngeom 2000 Study Committee. Xanthogranuloma, Rathke’s cyst, and childhood craniopharyngioma: Results of prospective multinational studies of children and adolescents with rare sellar malformations. J. Clin. Endocrinol. Metab. 2012, 97, 3935–3943. [Google Scholar] [CrossRef]
- Pascual, J.M.; Prieto, R.; Carrasco, R. Infundibulo-tuberal or not strictly intraventricular craniopharyngioma: Evidence for a major topographical category. Acta Neurochir. 2011, 153, 2403–2425. [Google Scholar] [CrossRef]
- Prieto, R.; Pascual, J.M.; Hofecker, V.; Winter, E.; Castro-Dufourny, I.; Carrasco, R.; Barrios, L. Craniopharyngioma adherence: A reappraisal of the evidence. Neurosurg. Rev. 2020, 43, 453–472. [Google Scholar] [CrossRef]
- Pan, J.; Qi, S.; Lu, Y.; Fan, J.; Zhang, X.; Zhou, J.; Peng, J. Intraventricular craniopharyngioma: Morphological analysis and outcome evaluation of 17 cases. Acta Neurochir. 2011, 153, 773–784. [Google Scholar] [CrossRef]
- Pascual, J.M.; González-Llanos, F.; Barrios, L.; Roda, J.M. Intraventricular craniopharyngiomas: Topographical classification and surgical approach selection based on an extensive overview. Acta Neurochir. 2004, 146, 785–800. [Google Scholar] [CrossRef]
- Prieto, R.; Pascual, J.M.; Rosdolsky, M.; Castro-Dufourny, I.; Carrasco, R.; Strauss, S.; Barrios, L. Craniopharyngioma adherence: A comprehensive topographical categorization and outcome-related risk stratification model based on the methodical examination of 500 tumors. Neurosurg. Focus 2016, 41, E13. [Google Scholar] [CrossRef]
- Lee, E.J.; Cho, Y.H.; Hong, S.H.; Kim, J.H.; Kim, C.J. Is the Complete Resection of Craniopharyngiomas in Adults Feasible Considering Both the Oncologic and Functional Outcomes? J. Korean Neurosurg. Soc. 2015, 58, 432–441. [Google Scholar] [CrossRef]
- Liubinas, S.V.; Munshey, A.S.; Kaye, A.H. Management of recurrent craniopharyngioma. J. Clin. Neurosci. 2011, 18, 451–457. [Google Scholar] [CrossRef]
- Lee, M.J.; Hwang, J.M. Initial visual field as a predictor of recurrence and postoperative visual outcome in children with craniopharyngioma. J. Pediatr. Ophthalmol. Strabismus 2012, 49, 38–42. [Google Scholar] [CrossRef]
- Rogers, M.; Davies, D.-M.; Halliday, J.; Pal, A.; Marland, A.; Foord, T.; Jafar-Mohammadi, B. Characterisation of paediatric craniopharyngiomas in a single centre study—Analysis of factors affecting recurrence rates. Endocr. Abstr. 2018, 59, 133. [Google Scholar] [CrossRef]
- Erfurth, E.M. Endocrine aspects and sequel in patients with craniopharyngioma. J. Pediatr. Endocrinol. Metab. 2015, 28, 19–26. [Google Scholar] [CrossRef]
- Adamson, T.E.; Wiestler, O.D.; Kleihues, P.; Yaşargil, M.G. Correlation of clinical and pathological features in surgically treated craniopharyngiomas. J. Neurosurg. 1990, 73, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Szeifert, G.T.; Sipos, L.; Horváth, M.; Sarker, M.H.; Major, O.; Salomváry, B.; Czirják, S.; Bálint, K.; Slowik, F.; Kolonics, L. Pathological characteristics of surgically removed craniopharyngiomas: Analysis of 131 cases. Acta Neurochir. 1993, 124, 139–143. [Google Scholar] [CrossRef]
- Crotty, T.B.; Scheithauer, B.W.; Young, W.F.; Davis, D.H.; Shaw, E.G.; Miller, G.M.; Burger, P.C. Papillary craniopharyngioma: A clinicopathological study of 48 cases. J. Neurosurg. 1995, 83, 206–214. [Google Scholar] [CrossRef]
- Tavangar, S.M.; Larijani, B.; Mahta, A.; Hosseini, S.M.A.; Mehrazine, M.; Bandarian, F. Craniopharyngioma: A Clinicopathological Study of 141 Cases. Endocr. Pathol. 2004, 15, 339–344. [Google Scholar] [CrossRef]
- Eldevik, O.P.; Blaivas, M.; Gabrielsen, T.O.; Hald, J.K.; Chandler, W.F. Craniopharyngioma: Radiologic and histologic findings and recurrence. Am. J. Neuroradiol. 1996, 17, 1427–1439. [Google Scholar] [PubMed]
- Minamida, Y.; Mikami, T.; Hashi, K.; Houkin, K. Surgical management of the recurrence and regrowth of craniopharyngiomas. J. Neurosurg. 2005, 103, 224–232. [Google Scholar] [CrossRef]
- Zygourakis, C.C.; Kaur, G.; Kunwar, S.; McDermott, M.W.; Madden, M.; Oh, T.; Parsa, A.T. Modern treatment of 84 newly diagnosed craniopharyngiomas. J. Clin. Neurosci. 2014, 21, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.R. Craniopharyngiomas. An analysis of some aspects of symptomatology, radiology and histology. Brain 1971, 94, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Nishi, T.; Kuratsu, J.; Takeshima, H.; Saito, Y.; Kochi, M.; Ushio, Y. Prognostic significance of the MIB-1 labeling index for patient with craniopharyngioma. Int. J. Mol. Med. 1999, 3, 157–161. [Google Scholar] [CrossRef]
- Raghavan, R.; Dickey, W.T.; Margraf, L.R.; White, C.L.; Coimbra, C.; Hynan, L.S.; Rushing, E.J. Proliferative activity in craniopharyngiomas: Clinicopathological correlations in adults and children. Surg. Neurol. 2000, 54, 241–248. [Google Scholar] [CrossRef]
- Izumoto, S.; Suzuki, T.; Kinoshita, M.; Hashiba, T.; Kagawa, N.; Wada, K.; Fujimoto, Y.; Hashimoto, N.; Saitoh, Y.; Maruno, M.; et al. Immunohistochemical detection of female sex hormone receptors in craniopharyngiomas: Correlation with clinical and histologic features. Surg. Neurol. 2005, 63, 520–525. [Google Scholar] [CrossRef]
- Anegawa, S.; Hayashi, T.; Nakagawa, S.; Furukawa, Y.; Tomokiyo, M. Craniopharyngioma with rapid regrowth--role of MIB-1 labeling index. No Shinkei Geka 2001, 29, 727–733. [Google Scholar]
- Guadagno, E.; De Divitiis, O.; Solari, D.; Borrelli, G.; Bracale, U.M.; Di Somma, A.; Cappabianca, P.; Caro, M.D.B.D. Can recurrences be predicted in craniopharyngiomas? β-catenin coexisting with stem cells markers and p-ATM in a clinicopathologic study of 45 cases. J. Exp. Clin. Cancer Res. 2017, 36, 95–106. [Google Scholar] [CrossRef]
- Xu, C.; Ge, S.; Cheng, J.; Gao, H.; Zhang, F.; Han, A. Pathological and Prognostic Characterization of Craniopharyngioma Based on the Expression of TrkA, β-Catenin, Cell Cycle Markers, and BRAF V600E Mutation. Front. Endocrinol. 2022, 13, 859381. [Google Scholar] [CrossRef]
- Park, H.J.; Dho, Y.S.; Kim, J.H.; Kim, J.W.; Park, C.K.; Kim, Y.H. Recurrence Rate and Prognostic Factors for the Adult Craniopharyngiomas in Long-Term Follow-Up. World Neurosurg. 2020, 133, e211–e217. [Google Scholar] [CrossRef]
- Losa, M.; Vimercati, A.; Acerno, S.; Barzaghi, R.L.; Mortini, P.; Mangili, F.; Terreni, M.R.; Santambrogio, G.; Giovanelli, M. Correlation between clinical characteristics and proliferative activity in patients with craniopharyngioma. J. Neurol. Neurosurg. Psychiatry 2004, 75, 889–892. [Google Scholar] [CrossRef]
- Duò, D.; Gasverde, S.; Benech, F.; Zenga, F.; Giordana, M.T. MIB-1 immunoreactivity in craniopharyngiomas: A clinico-pathological analysis. Clin. Neuropathol. 2003, 22, 229–234. [Google Scholar] [PubMed]
- Yalcin, N.; Akbulut, M.; Sedat, C.; Bir, F.; Demirtaş, E. Prognostic significance of the Ki-67 labeling index and p53 protein expression for patient with craniopharyngioma. J. Neurol. Sci. 2009, 26, 286–291. [Google Scholar]
- Moszczyńska, E.; Prokop-Piotrkowska, M.; Bogusz-Wójcik, A.; Grajkowska, W.; Szymańska, S.; Szalecki, M. Ki67 as a prognostic factor of craniopharyngioma’s recurrence in paediatric population. Child’s Nerv. Syst. 2020, 36, 1461–1469. [Google Scholar] [CrossRef]
- Ujifuku, K.; Matsuo, T.; Takeshita, T.; Hayashi, Y.; Hayashi, K.; Kitagawa, N.; Hayashi, T.; Suyama, K.; Nagata, I. Malignant Transformation of Craniopharyngioma Associated with Moyamoya Syndrome. Neurol. Med. Chir. 2010, 50, 599–603. [Google Scholar] [CrossRef]
- Momota, H.; Ichimiya, S.; Ikeda, T.; Yamaki, T.; Kikuchi, T.; Houkin, K.; Sato, N. Immunohistochemical analysis of the p53 family members in human craniopharyngiomas. Brain Tumor Pathol. 2003, 20, 73–77. [Google Scholar] [CrossRef]
- Liu, H.; Liu, Z.; Li, J.; Li, Q.; You, C.; Xu, J. Relative quantitative expression of hypoxia-inducible factor 1α messenger ribonucleic acid in recurrent craniopharyngiomas. Neurol. India 2014, 62, 53–56. [Google Scholar]
- Sun, H.I.; Akgun, E.; Bicer, A.; Ozkan, A.; Bozkurt, S.U.; Kurtkaya, O.; Koc, D.Y.; Pamir, M.N.; Kilic, T. Expression of angiogenic factors in craniopharyngiomas: Implications for tumor recurrence. Neurosurgery 2010, 66, 744–750. [Google Scholar] [CrossRef]
- Xia, Z.; Liu, W.; Li, S.; Jia, G.; Zhang, Y.; Li, C.; Ma, Z.; Tian, J.; Gong, J. Expression of Matrix Metalloproteinase-9, Type IV Collagen and Vascular Endothelial Growth Factor in Adamantinous Craniopharyngioma. Neurochem. Res. 2011, 36, 2346–2351. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, S.; You, C.; Wang, X.; Zhou, Q. Microvascular density and vascular endothelial growth factor have little correlation with prognosis of craniopharyngioma. Surg. Neurol. 2006, 66, S30–S34. [Google Scholar] [CrossRef]
- Hofmann, B.M.; Hoelsken, A.; Fahlbusch, R.; Blümcke, I.; Buslei, R. Hormone receptor expression in craniopharyngiomas: A clinicopathological correlation. Neurosurgery 2010, 67, 617–625. [Google Scholar] [CrossRef]
- Li, Q.; You, C.; Liu, L.; Rao, Z.; Sima, X.; Zhou, L.; Xu, J. Craniopharyngioma cell growth is promoted by growth hormone [GH] and is inhibited by tamoxifen: Involvement of growth hormone receptor [GHR] and IGF-1 receptor [IGF-1R]. J. Clin. Neurosci. 2013, 20, 153–157. [Google Scholar] [CrossRef]
- Martínez-Ortega, A.; Flores-Martinez, Á.; Venegas-Moreno, E.; Dios, E.; Del Can, D.; Rivas, E.; Kaen, A.; Ruiz-Valdepeñas, E.C.; Fajardo, E.; Roldán, F.; et al. Sex Hormone Receptor Expression in Craniopharyngiomas and Association with Tumor Aggressiveness Characteristics. J. Clin. Med. 2022, 11, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Amendola, B.E.; Gebarski, S.S.; Bermudez, A.G. Analysis of treatment results in craniopharyngioma. J. Clin. Oncol. 1985, 3, 252–258. [Google Scholar] [CrossRef]
- Baskin, D.S.; Wilson, C.B. Surgical management of craniopharyngiomas. A review of 74 cases. J. Neurosurg. 1986, 65, 22–27. [Google Scholar] [CrossRef]
- Cabezudo, J.M.; Vaquero, J.; Areitio, E.; Martinez, R.; de Sola, R.G.; Bravo, G. Craniopharyngiomas: A critical approach to treatment. J. Neurosurg. 1981, 55, 371–375. [Google Scholar] [CrossRef]
- Carmel, P.W.; Antunes, J.L.; Chang, C.H. Craniopharyngiomas in children. Neurosurgery 1982, 11, 382–389. [Google Scholar] [CrossRef]
- Khafaga, Y.; Jenkin, D.; Kanaan, I.; Hassounah, M.; Al Shabanah, M.; Gray, A. Craniopharyngioma in children. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 601–606. [Google Scholar] [CrossRef]
- Thompson, D.; Phipps, K.; Hayward, R. Craniopharyngioma in childhood: Our evidence-based approach to management. Child’s Nerv. Syst. 2005, 21, 660–668. [Google Scholar] [CrossRef]
- Yaşargil, M.G.; Curcic, M.; Kis, M.; Siegenthaler, G.; Teddy, P.J.; Roth, P. Total removal of craniopharyngiomas. Approaches and long-term results in 144 patients. J. Neurosurg. 1990, 73, 355–357. [Google Scholar] [CrossRef]
- Zuccaro, G. Radical resection of craniopharyngioma. Child’s Nerv. Syst. 2005, 21, 679–690. [Google Scholar] [CrossRef]
- Mortini, P.; Gagliardi, F.; Boari, N.; Losa, M. Surgical strategies and modern therapeutic options in the treatment of craniopharyngiomas. Crit. Rev. Oncol. 2013, 88, 514–529. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Qiu, B.; Qi, S.; Pan, J.; Lu, Y.; Peng, J. Influence of previous treatments on repeat surgery for recurrent craniopharyngiomas in children. Child’s Nerv. Syst. 2016, 32, 485–491. [Google Scholar] [CrossRef]
- Richmond, I.L.; Wara, W.M.; Wilson, C.B. Role of Radiation Therapy in the Management of Craniopharyngiomas in Children. Neurosurgery 1980, 6, 513–517. [Google Scholar] [CrossRef]
- Stahnke, N.; Grubel, G.; Lagenstein, I.; Willig, R.P. Long-term follow-up of children with craniopharyngioma. Eur. J. Pediatr. 1984, 142, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Thomsett, M.; Conte, F.; Kaplan, S.; Grumbach, M. Endocrine and neurologic outcome in childhood craniopharyngioma: Review of effect of treatment in 42 patients. J. Pediatr. 1980, 97, 728–735. [Google Scholar] [CrossRef]
- Weiss, M.; Sutton, L.; Marcial, V.; Fowble, B.; Packer, R.; Zimmerman, R.; Schut, L.; Bruce, D.; D’Angio, G. The role of radiation therapy in the management of childhood craniopharyngioma. Int. J. Radiat. Oncol. Biol. Phys. 1989, 17, 1313–1321. [Google Scholar] [CrossRef]
- Wen, B.-C.; Hussey, D.H.; Staples, J.; Hitchon, P.W.; Jani, S.K.; Vigliotti, A.P.; Doornbos, J. A comparison of the roles of surgery and radiation therapy in the management of craniopharyngiomas. Int. J. Radiat. Oncol. Biol. Phys. 1989, 16, 17–24. [Google Scholar] [CrossRef]
- Enayet, A.E.R.; Atteya, M.M.E.; Taha, H.; Zaghloul, M.S.; Refaat, A.; Maher, E.; Abdelaziz, A.; El Beltagy, M.A. Management of pediatric craniopharyngioma: 10-year experience from high-flow center. Child’s Nerv. Syst. 2021, 37, 391–401. [Google Scholar] [CrossRef]
- Stripp, D.C.; Maity, A.; Janss, A.J.; Belasco, J.B.; Tochner, Z.A.; Goldwein, J.W.; Moshang, T.; Rorke, L.B.; Phillips, P.C.; Sutton, L.N.; et al. Surgery with or without radiation therapy in the management of craniopharyngiomas in children and young adults. Int. J. Radiat. Oncol. Biol Phys. 2004, 58, 714–720. [Google Scholar] [CrossRef]
- Zhang, Y.Q.; Ma, Z.Y.; Wu, Z.B.; Luo, S.Q.; Wang, Z.C. Radical Resection of 202 Pediatric Craniopharyngiomas with Special Reference to the Surgical Approaches and Hypothalamic Protection. Pediatr. Neurosurg. 2008, 44, 435–443. [Google Scholar] [CrossRef]
- Cheng, J.; Shao, Q.; Pan, Z.; You, J. Analysis and Long-Term Follow-Up of the Surgical Treatment of Children With Craniopharyngioma. J. Craniofacial Surg. 2016, 27, e763–e766. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, T.; Takao, T.; Iwasaki, Y.; Pooh, K.; Okazaki, M.; Hashimoto, K.; Terada, Y. Rapid recurrence of craniopharyngioma following recombinant human growth hormone replacement. J. Neuro-Oncol. 2010, 100, 321–322. [Google Scholar] [CrossRef]
- Niu, D.-M.; Guo, W.-Y.; Pan, H.-C.; Wong, T.-T. Rapid enlargement of a residual craniopharyngioma during short-term growth hormone replacement. Child’s Nerv. Syst. 2002, 18, 164–165. [Google Scholar] [CrossRef] [PubMed]
- Arslanian, S.A.; Becker, D.J.; Lee, P.A.; Drash, A.L.; Foley, T.P. Growth Hormone Therapy and Tumor Recurrence: Findings in Children With Brain Neoplasms and Hypopituitarism. Am. J. Dis. Children 1985, 139, 347–350. [Google Scholar] [CrossRef]
- Olsson, D.S.; Buchfelder, M.; Wiendieck, K.; Kremenevskaja, N.; Bengtsson, B.Å.; Jakobsson, K.-E.; Jarfelt, M.; Johannsson, G.; Nilsson, A.G. Tumour recurrence and enlargement in patients with craniopharyngioma with and without GH replacement therapy during more than 10 years of follow-up. Eur. J. Endocrinol. 2012, 166, 1061–1068. [Google Scholar] [CrossRef]
- Kanev, P.M.; Lefebvre, J.F.; Mauseth, R.S.; Berger, M.S.; Alotaibi, N.M.; Noormohamed, N.; Cote, D.J.; Alharthi, S.; Doucette, J.; Zaidi, H.A.; et al. Growth hormone deficiency following radiation therapy of primary brain tumors in children. J. Neurosurg. 1991, 74, 743–748. [Google Scholar] [CrossRef]
- Karavitaki, N.; Warner, J.T.; Marland, A.; Shine, B.; Ryan, F.; Arnold, J.; Turner, H.E.; Wass, J.A.H. GH replacement does not increase the risk of recurrence in patients with craniopharyngioma. Clin. Endocrinol. 2006, 64, 556–560. [Google Scholar] [CrossRef]
- Rohrer, T.R.; Langer, T.; Grabenbauer, G.G.; Buchfelder, M.; Glowatzki, M.; Dörr, H.G. Growth Hormone Therapy and the Risk of Tumor Recurrence after Brain Tumor Treatment in Children. J. Pediatr. Endocrinol. Metab. 2010, 23, 935–942. [Google Scholar] [CrossRef]
- Boekhoff, S.; Bogusz, A.; Sterkenburg, A.S.; Eveslage, M.; Müller, H.L. Long-term effects of growth hormone replacement therapy in childhood-onset craniopharyngioma: Results of the German Craniopharyngioma Registry [HIT-Endo]. Eur. J. Endocrinol. 2018, 179, 331–341. [Google Scholar] [CrossRef]
- Boguszewski, M.C.S.; Cardoso-Demartini, A.A.; Boguszewski, C.L.; Chemaitilly, W.; Higham, C.E.; Johannsson, G.; Yuen, K.C.J. Safety of growth hormone [GH] treatment in GH deficient children and adults treated for cancer and non-malignant intracranial tumors—A review of research and clinical practice. Pituitary 2021, 24, 810–827. [Google Scholar] [CrossRef]
- Clayton, P.E.; Price, D.A.; Shalet, S.M.; Gattemaneni, H.R. Craniopharyngioma Recurrence and Growth Hormone Therapy. Lancet 1988, 331, 642. [Google Scholar] [CrossRef] [PubMed]
- Child, C.J.; Conroy, D.; Zimmermann, A.G.; Woodmansee, W.W.; Erfurth, E.M.; Robison, L.L. Incidence of primary cancers and intracranial tumour recurrences in GH-treated and untreated adult hypopituitary patients: Analyses from the Hypopituitary Control and Complications Study. Eur. J. Endocrinol. 2015, 172, 779–790. [Google Scholar] [CrossRef]
- Moshang, T.; Rundle, A.C.; Graves, D.A.; Nickas, J.; Johanson, A.; Meadows, A. Brain tumor recurrence in children treated with growth hormone: The National Cooperative Growth Study experience. J. Pediatr. 1996, 128, S4–S7. [Google Scholar] [CrossRef]
- Price, D.; Wilton, P.; Jönsson, P.; Albertsson-Wikland, K.; Chatelain, P.; Cutfield, W.; Ranke, M. Efficacy and Safety of Growth Hormone Treatment in Children with Prior Craniopharyngioma: An Analysis of the Pharmacia and Upjohn International Growth Database [KIGS] from 1988 to 1996. Horm. Res. Paediatr. 1998, 49, 91–97. [Google Scholar] [CrossRef]
- Smith, T.R.; Cote, D.J.; Jane, J.A.; Laws, E.R. Physiological growth hormone replacement and rate of recurrence of craniopharyngioma: The Genentech National Cooperative Growth Study. J. Neurosurg. Pediatr. 2016, 18, 408–412. [Google Scholar] [CrossRef]
- Alotaibi, N.M.; Noormohamed, N.; Cote, D.J.; Alharthi, S.; Doucette, J.; Zaidi, H.A.; Mekary, R.A.; Smith, T.R. Physiologic Growth Hormone–Replacement Therapy and Craniopharyngioma Recurrence in Pediatric Patients: A Meta-Analysis. World Neurosurg. 2018, 109, 487–496. [Google Scholar] [CrossRef]
- Drapeau, A.; Walz, P.C.; Eide, J.G.; Rugino, A.J.; Shaikhouni, A.; Mohyeldin, A.; Carrau, R.L.; Prevedello, D.M. Pediatric craniopharyngioma. Child’s Nerv. Syst. 2019, 35, 2133–2145. [Google Scholar] [CrossRef]
- Steinbok, P. Craniopharyngioma in Children: Long-term Outcomes. Neurol. Med. Chir. 2015, 55, 722–726. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Taylor-Weiner, A.; Manley, P.E.; Jones, R.T.; Dias-Santagata, D.; Thorner, A.R.; Lawrence, M.S.; Rodriguez, F.J.; A Bernardo, L.; Schubert, L.; et al. Exome sequencing identifies BRAF mutations in papillary craniopharyngiomas. Nat. Genet. 2014, 46, 161–165. [Google Scholar] [CrossRef]
- Buslei, R.; Hölsken, A.; Hofmann, B.; Kreutzer, J.; Siebzehnrubl, F.; Hans, V.; Oppel, F.; Buchfelder, M.; Fahlbusch, R.; Blümcke, I. Nuclear beta-catenin accumulation associates with epithelial morphogenesis in craniopharyngiomas. Acta Neuropathol. 2007, 113, 585–590. [Google Scholar] [CrossRef]
- Hölsken, A.; Stache, C.; Schlaffer, S.M.; Flitsch, J.; Fahlbusch, R.; Buchfelder, M.; Oppel, F.; Buchfelder, M.; Fahlbusch, R.; Blümcke, I. Adamantinomatous craniopharyngiomas express tumor stem cell markers in cells with activated Wnt signaling: Further evidence for the existence of a tumor stem cell niche? Pituitary 2014, 17, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Wang, Y.; Liu, H.; Qi, X.; Zhou, Z.; Wang, X.; Lin, Z. Molecular biological features of cyst wall of adamantinomatous craniopharyngioma. Sci. Rep. 2023, 13, 3049. [Google Scholar] [CrossRef] [PubMed]
- Khakh, B.S.; Sofroniew, M.V. Diversity of astrocyte functions and phenotypes in neural circuits. Nat. Neurosci. 2015, 18, 942–952. [Google Scholar] [CrossRef]
- Qi, S.; Lu, Y.; Pan, J.; Zhang, X.; Long, H.; Fan, J. Anatomic relations of the arachnoidea around the pituitary stalk: Relevance for surgical removal of craniopharyngiomas. Acta Neurochir. 2011, 153, 785–796. [Google Scholar] [CrossRef]
- Scholzen, T.; Gerdes, J. The Ki-67 protein: From the known and the unknown. J. Cell. Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Mrouj, K.; Andrés-Sánchez, N.; Dubra, G.; Singh, P.; Sobecki, M.; Chahar, D.; Al Ghoul, E.; Aznar, A.B.; Prieto, S.; Pirot, N.; et al. Ki-67 regulates global gene expression and promotes sequential stages of carcinogenesis. Proc. Natl. Acad. Sci. USA 2021, 118, e2026507118. [Google Scholar] [CrossRef]
- Sengupta, S.; Chatterjee, U.; Banerjee, U.; Ghosh, S.; Chatterjee, S.; Ghosh, A.K. A study of histopathological spectrum and expression of Ki-67, TP53 in primary brain tumors of pediatric age group. Indian J. Med. Paediatr. Oncol. 2012, 33, 25–31. [Google Scholar] [CrossRef]
- Prieto, R.; Pascual, J.M. Can tissue biomarkers reliably predict the biological behavior of craniopharyngiomas? A comprehensive overview. Pituitary 2018, 21, 431–442. [Google Scholar] [CrossRef]
- Broggi, G.; Franzini, A.; Cajola, L.; Pluchino, F. Cell Kinetic Investigations in Craniopharyngioma: Preliminary Results and Considerations. Pediatr. Neurosurg. 1994, 21, 21–23. [Google Scholar] [CrossRef]
- Kim, S.; An, S.S.A. Role of p53 isoforms and aggregations in cancer. Medicine 2016, 95, e3993. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Santagata, S. Endocrine Tumors: BRAF V600E mutations in papillary craniopharyngioma. Eur. J. Endocrinol. 2016, 174, R139–R144. [Google Scholar] [CrossRef]
- Rao, M.; Bhattacharjee, M.; Shepard, S.; Hsu, S. Newly diagnosed papillary craniopharyngioma with BRAF V600E mutation treated with single-agent selective BRAF inhibitor dabrafenib: A case report. Oncotarget 2019, 10, 6038–6042. [Google Scholar] [CrossRef] [PubMed]
- Himes, B.T.; Ruff, M.W.; Van Gompel, J.J.; Park, S.S.; Galanis, E.; Kaufmann, T.J.; Uhm, J.H. Recurrent papillary craniopharyngioma with BRAF V600E mutation treated with dabrafenib: Case report. J. Neurosurg. 2018, 130, 1299–1303. [Google Scholar] [CrossRef]
- Fasano, M.; Della Corte, C.M.; Caterino, M.; Pirozzi, M.; Rauso, R.; Troiani, T.; Martini, G.; Napolitano, S.; Morgillo, F.; Ciardiello, F. Dramatic Therapeutic Response to Dabrafenib Plus Trametinib in BRAF V600E Mutated Papillary Craniopharyngiomas: A Case Report and Literature Review. Front. Med. 2022, 8, 652005. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Shankar, G.M.; Gill, C.M.; Taylor-Weiner, A.; Nayyar, N.; Panka, D.J.; Sullivan, R.J.; Frederick, D.T.; Abedalthagafi, M.; Jones, P.S.; et al. Dramatic Response of BRAF V600E Mutant Papillary Craniopharyngioma to Targeted Therapy. Gynecol. Oncol. 2015, 108, djv310. [Google Scholar] [CrossRef]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef]
- Jun, J.C.; Rathore, A.; Younas, H.; Gilkes, D.; Polotsky, V.Y. Hypoxia-Inducible Factors and Cancer. Curr. Sleep Med. Rep. 2017, 3, 1–10. [Google Scholar] [CrossRef]
- Vidal, S.; Kovacs, K.; Lloyd, R.V.; Meyer, F.B.; Scheithauer, B.W. Angiogenesis in patients with craniopharyngiomas: Correlation with treatment and outcome. Cancer 2002, 94, 738–745. [Google Scholar] [CrossRef]
- Flitsch, J.; Müller, H.L.; Burkhardt, T. Surgical Strategies in Childhood Craniopharyngioma. Front. Endocrinol. 2011, 2, 96. [Google Scholar] [CrossRef]
- Yamada, S.; Fukuhara, N.; Yamaguchi-Okada, M.; Nishioka, H.; Takeshita, A.; Takeuchi, Y.; Inoshita, N.; Ito, J. Therapeutic outcomes of transsphenoidal surgery in pediatric patients with craniopharyngiomas: A single-center study. J. Neurosurg. Pediatr. 2018, 21, 549–562. [Google Scholar] [CrossRef]
- Yang, I.; Sughrue, M.E.; Rutkowski, M.J.; Kaur, R.; Ivan, M.E.; Aranda, D.; Barani, I.J.; Parsa, A.T. Craniopharyngioma: A comparison of tumor control with various treatment strategies. Neurosurg. Focus 2010, 28, E5. [Google Scholar] [CrossRef] [PubMed]
- Jalali, R.; Gupta, T.; Goda, J.S.; Goswami, S.; Shah, N.; Dutta, D.; Uday, K.; Jayita, D.; Padmavathy, M.; Sadhana, K.; et al. Efficacy of Stereotactic Conformal Radiotherapy vs Conventional Radiotherapy on Benign and Low-Grade Brain Tumors: A Randomized Clinical Trial. JAMA Oncol. 2017, 3, 1368–1376. [Google Scholar] [CrossRef]
- Klimo, P.; Venable, G.T.; Boop, F.A.; Merchant, T.E. Recurrent craniopharyngioma after conformal radiation in children and the burden of treatment. J. Neurosurg. Pediatr. 2015, 15, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, T.; Kamada, K.; Izumo, T.; Nagata, I. Indication and Limitations of Endoscopic Extended Transsphenoidal Surgery for Craniopharyngioma. Neurol. Med. Chir. 2014, 54, 974–982. [Google Scholar] [CrossRef] [PubMed]
- de Divitiis, E.; Cappabianca, P.; Cavallo, L.M.; Esposito, F.; de Divitiis, O.; Messina, A. Extended Endoscopic Transsphenoidal Approach for Extrasellar Craniopharyngiomas. Neurosurgery 2007, 61, 219–228. [Google Scholar] [CrossRef]
- Koutourousiou, M.; Fernandez-Miranda, J.C.; Wang, E.W.; Snyderman, C.H.; Gardner, P.A. The limits of transsellar/transtuberculum surgery for craniopharyngioma. J. Neurosurg. Sci. 2018, 62, 301–309. [Google Scholar] [CrossRef]
- Taylor, D.G.; Jane, J.A. Editorial. Endoscopic endonasal surgery for pediatric craniopharyngiomas. J. Neurosurg. Pediatr. 2018, 21, 546–548. [Google Scholar] [CrossRef]
- Maira, G.; Anile, C.; Albanese, A.; Cabezas, D.; Pardi, F.; Vignati, A. The role of transsphenoidal surgery in the treatment of craniopharyngiomas. J. Neurosurg. 2004, 100, 445–451. [Google Scholar] [CrossRef]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.M.; Anand, V.K.; Schwartz, T.H. Endoscopic Endonasal Compared with Microscopic Transsphenoidal and Open Transcranial Resection of Craniopharyngiomas. World Neurosurg. 2012, 77, 329–341. [Google Scholar] [CrossRef]
- Ogawa, Y.; Kudo, M.; Watanabe, M.; Tominaga, T. Heterogeneity of Growth Hormone Receptor Expression in Craniopharyngioma—Implications for Surgical Strategy. World Neurosurg. 2020, 138, 89–92. [Google Scholar] [CrossRef]
- Losa, M.; Castellino, L.; Pagnano, A.; Rossini, A.; Mortini, P.; Lanzi, R. Growth Hormone Therapy Does Not Increase the Risk of Craniopharyngioma and Nonfunctioning Pituitary Adenoma Recurrence. J. Clin. Endocrinol. Metab. 2020, 105, 1573–1580. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serbis, A.; Tsinopoulou, V.R.; Papadopoulou, A.; Kolanis, S.; Sakellari, E.I.; Margaritis, K.; Litou, E.; Ntouma, S.; Giza, S.; Kotanidou, E.P.; et al. Predictive Factors for Pediatric Craniopharyngioma Recurrence: An Extensive Narrative Review. Diagnostics 2023, 13, 1588. https://doi.org/10.3390/diagnostics13091588
Serbis A, Tsinopoulou VR, Papadopoulou A, Kolanis S, Sakellari EI, Margaritis K, Litou E, Ntouma S, Giza S, Kotanidou EP, et al. Predictive Factors for Pediatric Craniopharyngioma Recurrence: An Extensive Narrative Review. Diagnostics. 2023; 13(9):1588. https://doi.org/10.3390/diagnostics13091588
Chicago/Turabian StyleSerbis, Anastasios, Vasiliki Rengina Tsinopoulou, Anastasia Papadopoulou, Savvas Kolanis, Eleni I. Sakellari, Kosmas Margaritis, Eleni Litou, Stergianna Ntouma, Styliani Giza, Eleni P. Kotanidou, and et al. 2023. "Predictive Factors for Pediatric Craniopharyngioma Recurrence: An Extensive Narrative Review" Diagnostics 13, no. 9: 1588. https://doi.org/10.3390/diagnostics13091588
APA StyleSerbis, A., Tsinopoulou, V. R., Papadopoulou, A., Kolanis, S., Sakellari, E. I., Margaritis, K., Litou, E., Ntouma, S., Giza, S., Kotanidou, E. P., & Galli-Tsinopoulou, A. (2023). Predictive Factors for Pediatric Craniopharyngioma Recurrence: An Extensive Narrative Review. Diagnostics, 13(9), 1588. https://doi.org/10.3390/diagnostics13091588