
Differentiation of Salivary Gland and Salivary Gland Tumor Tissue via Raman Imaging Combined with Multivariate Data Analysis

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Parotid Tissue Sample Preparation
2.2. Confocal Raman Imaging
2.3. Data Pre-Treatment and Multivariate Data Analysis
3. Results
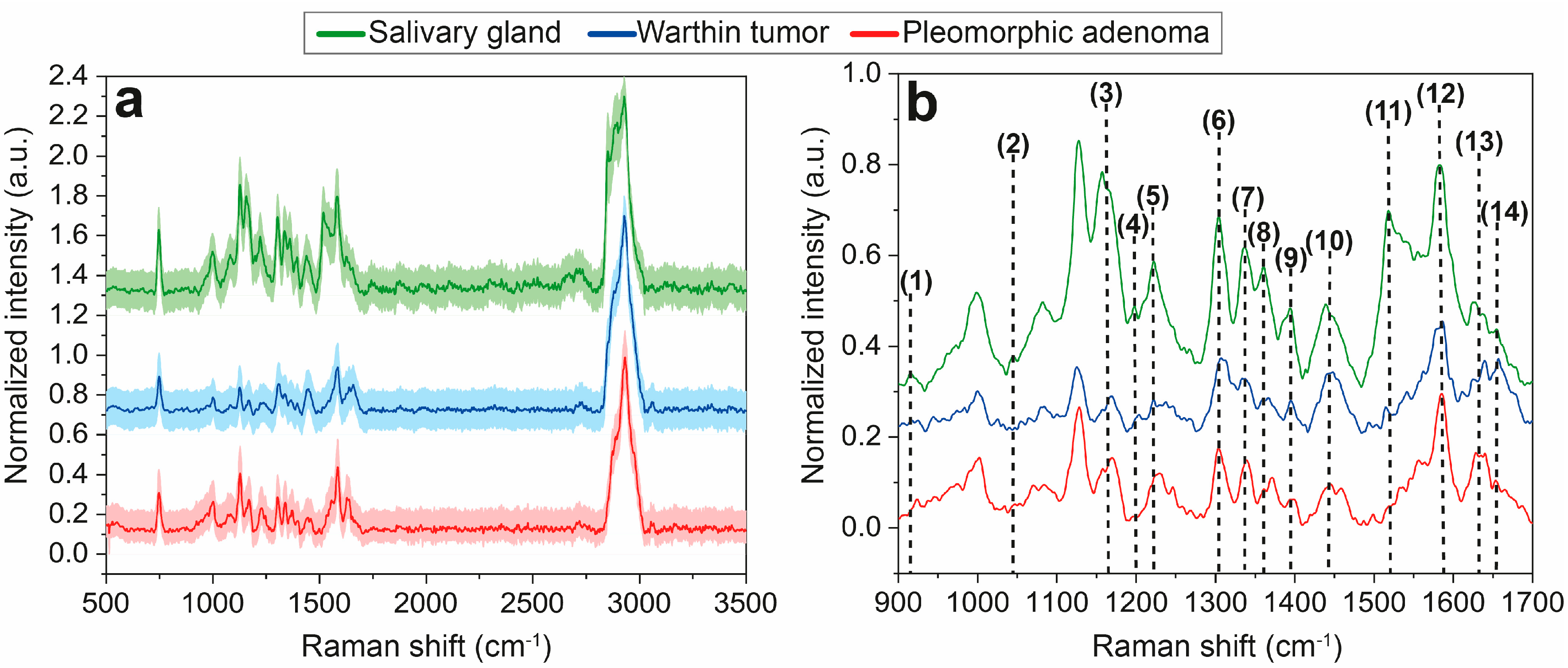
3.1. Raman Mean Spectra Analysis
3.2. Raman Data Analysis via PCA-DA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Israel, Y.; Rachmiel, A.; Ziv, G.; Nagler, R. Benign and Malignant Salivary Gland Tumors—Clinical and Demographic Characteristics. Anticancer Res. 2016, 36, 4151–4154. [Google Scholar] [PubMed]
- Fu, J.-Y.; Wu, C.-X.; Shen, S.-K.; Zheng, Y.; Zhang, C.-P.; Zhang, Z.-Y. Salivary gland carcinoma in Shanghai (2003–2012): An epidemiological study of incidence, site and pathology. BMC Cancer 2019, 19, 350. [Google Scholar] [CrossRef] [PubMed]
- Franzen, A.; Buchali, A.; Lieder, A. The rising incidence of parotid metastases: Our experience from four decades of parotid gland surgery. Acta Otorhinolaryngol. Ital. 2017, 37, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Zhan, K.Y.; Khaja, S.F.; Flack, A.B.; Day, T.A. Benign Parotid Tumors. Otolaryngol. Clin. N. Am. 2016, 49, 327–342. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; International Agency for Research on Cancer: Lyon, France, 2017; Volume 9, p. 347. [Google Scholar]
- Paluszkiewicz, C.; Roman, M.; Piergies, N.; Pięta, E.; Woźniak, M.; Guidi, M.C.; Miśkiewicz-Orczyk, K.; Marków, M.; Ścierski, W.; Misiołek, M.; et al. Tracking of the biochemical changes upon pleomorphic adenoma progression using vibrational microspectroscopy. Sci. Rep. 2021, 11, 18010. [Google Scholar] [CrossRef] [PubMed]
- Postema, R.J.; van Velthuysen, M.-L.F.; van den Brekel, M.W.M.; Balm, A.J.M.; Peterse, J.L. Accuracy of fine-needle aspiration cytology of salivary gland lesions in the netherlands cancer institute. Head Neck 2004, 26, 418–424. [Google Scholar] [CrossRef]
- Dostalova, L.; Kalfert, D.; Jechova, A.; Koucky, V.; Novak, S.; Kuchar, M.; Zabrodsky, M.; Novakova Kodetova, D.; Ludvikova, M.; Kholova, I.; et al. The role of fine-needle aspiration biopsy (FNAB) in the diagnostic management of parotid gland masses with emphasis on potential pitfalls. Eur. Arch. Otorhinolaryngol. 2020, 277, 1763–1769. [Google Scholar] [CrossRef] [PubMed]
- Psychogios, G.; Bohr, C.; Constantinidis, J.; Canis, M.; Vander Poorten, V.; Plzak, J.; Knopf, A.; Betz, C.; Guntinas-Lichius, O.; Zenk, J. Review of surgical techniques and guide for decision making in the treatment of benign parotid tumors. Eur. Arch. Otorhinolaryngol. 2021, 278, 15–29. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Velegrakis, S.; Iro, H. Unexpected Detection of Parotid Gland Malignancy during Primary Extracapsular Dissection. Otolaryngol.–Head Neck Surg. 2015, 152, 1042–1047. [Google Scholar] [CrossRef]
- Auner, G.W.; Koya, S.K.; Huang, C.; Broadbent, B.; Trexler, M.; Auner, Z.; Elias, A.; Mehne, K.C.; Brusatori, M.A. Applications of Raman spectroscopy in cancer diagnosis. Cancer Metastasis Rev. 2018, 37, 691–717. [Google Scholar] [CrossRef]
- Bellisola, G.; Sorio, C. Infrared spectroscopy and microscopy in cancer research and diagnosis. Am. J. Cancer Res. 2012, 2, 1–21. [Google Scholar] [PubMed]
- Kong, K.; Kendall, C.; Stone, N.; Notingher, I. Raman spectroscopy for medical diagnostics—From in-vitro biofluid assays to in-vivo cancer detection. Adv. Drug Del. Rev. 2015, 89, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Kaznowska, E.; Depciuch, J.; Szmuc, K.; Cebulski, J. Use of FTIR spectroscopy and PCA-LDC analysis to identify cancerous lesions within the human colon. J. Pharm. Biomed. Anal. 2017, 134, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Devi, S.; Panigrahi, P.; Pradhan, A. Detecting cervical cancer progression through extracted intrinsic fluorescence and principal component analysis. J. Biomed. Opt. 2014, 19, 127003. [Google Scholar] [CrossRef] [PubMed]
- Francisco, A.L.N.; Correr, W.R.; Azevedo, L.H.; Kern, V.G.; Pinto, C.A.L.; Kowalski, L.P.; Kurachi, C. Fluorescence spectroscopy for the detection of potentially malignant disorders and squamous cell carcinoma of the oral cavity. Photodiagnosis Photodyn. Ther. 2014, 11, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Aaboubout, Y.; Nunes Soares, M.R.; Bakker Schut, T.C.; Barroso, E.M.; van der Wolf, M.; Sokolova, E.; Artyushenko, V.; Bocharnikov, A.; Usenov, I.; van Lanschot, C.G.F.; et al. Intraoperative assessment of resection margins by Raman spectroscopy to guide oral cancer surgery. Analyst 2023, 148, 4116–4126. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.-X.; Xie, X.S. Vibrational spectroscopic imaging of living systems: An emerging platform for biology and medicine. Science 2015, 350, aaa8870. [Google Scholar] [CrossRef]
- Gao, L.; Smith, R.T. Optical hyperspectral imaging in microscopy and spectroscopy—A review of data acquisition. J. Biophotonics 2015, 8, 441–456. [Google Scholar] [CrossRef]
- Halicek, M.; Fabelo, H.; Ortega, S.; Callico, G.M.; Fei, B. In-Vivo and Ex-Vivo Tissue Analysis through Hyperspectral Imaging Techniques: Revealing the Invisible Features of Cancer. Cancers 2019, 11, 756. [Google Scholar] [CrossRef]
- Anderson, N.G.; Butler, A.P. Clinical applications of spectral molecular imaging: Potential and challenges. Contrast Media Mol. Imaging 2014, 9, 3–12. [Google Scholar] [CrossRef]
- Boldrini, B.; Kessler, W.; Rebner, K.; Kessler, R.W. Hyperspectral Imaging: A Review of Best Practice, Performance and Pitfalls for in-line and on-line Applications. J. Near Infrared Spectrosc. 2012, 20, 483–508. [Google Scholar] [CrossRef]
- Abdi, H.; Williams, L.J. Principal component analysis. WIREs Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Wold, S.; Esbensen, K.; Geladi, P. Principal component analysis. Chemom. Intellig. Lab. Syst. 1987, 2, 37–52. [Google Scholar] [CrossRef]
- Gajjar, K.; Heppenstall, L.D.; Pang, W.; Ashton, K.M.; Trevisan, J.; Patel, I.I.; Llabjani, V.; Stringfellow, H.F.; Martin-Hirsch, P.L.; Dawson, T.; et al. Diagnostic segregation of human brain tumours using Fourier-transform infrared and/or Raman spectroscopy coupled with discriminant analysis. Anal. Methods 2013, 5, 89–102. [Google Scholar] [CrossRef]
- Croce, A.C.; Bottiroli, G. Autofluorescence spectroscopy and imaging: A tool for biomedical research and diagnosis. Eur. J. Histochem. 2014, 58, 2461. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Zhang, S.; Yue, S. Raman Spectroscopy and Imaging for Cancer Diagnosis. J. Healthc. Eng. 2018, 2018, 8619342. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, J.; Chen, G.; Li, C.; Lin, S.; Shao, Y.; Feng, S.; Huang, Z.; Xie, S.; Zeng, H.; et al. Micro-Raman spectroscopy study of cancerous and normal nasopharyngeal tissues. J. Biomed. Opt. 2013, 18, 027003. [Google Scholar] [CrossRef]
- Ghassemi, K.M.; Barzegari, S.; Hajian, P.; Zham, H.; Mirzaei, H.R.; Shirazi, F.H. Diagnosis of normal and malignant human gastric tissue samples by FTIR spectra combined with mathematical models. J. Mol. Struct. 2021, 1229, 129493. [Google Scholar] [CrossRef]
- Argov, S.; Ramesh, J.; Salman, A.; Sinelnikov, I.; Goldstein, J.; Guterman, H.; Mordechai, S. Diagnostic potential of FTIR microspectroscopy and advanced computational methods in colon cancer patients. J. Biomed. Opt. 2002, 7, 248–254. [Google Scholar] [CrossRef]
- Bergner, N.; Romeike, B.F.M.; Reichart, R.; Kalff, R.; Krafft, C.; Popp, J. Tumor margin identification and prediction of the primary tumor from brain metastases using FTIR imaging and support vector machines. Analyst 2013, 138, 3983–3990. [Google Scholar] [CrossRef]
- Dong, L.; Sun, X.; Chao, Z.; Zhang, S.; Zheng, J.; Gurung, R.; Du, J.; Shi, J.; Xu, Y.; Zhang, Y.; et al. Evaluation of FTIR spectroscopy as diagnostic tool for colorectal cancer using spectral analysis. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2014, 122, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Surmacki, J.; Musial, J.; Kordek, R.; Abramczyk, H. Raman imaging at biological interfaces: Applications in breast cancer diagnosis. Mol. Cancer 2013, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- Scheer, M.; Fuss, J.; Derman, M.A.; Kreppel, M.; Neugebauer, J.; Rothamel, D.; Drebber, U.; Zoeller, J.E. Autofluorescence imaging in recurrent oral squamous cell carcinoma. Oral Maxillofac. Surg. 2016, 20, 27–33. [Google Scholar] [CrossRef] [PubMed]
- van Lanschot, C.; Schut, T.B.; Barroso, E.; Sewnaik, A.; Hardillo, J.; Monserez, D.; Meeuwis, C.; Keereweer, S.; de Jong, R.B.; Puppels, G.; et al. Raman spectroscopy to discriminate laryngeal squamous cell carcinoma from non-cancerous surrounding tissue. Lasers Med. Sci. 2023, 38, 193. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Li, Y.; Yang, G.; Wen, Z.-N.; Li, M.-L.; Li, L.-J. Discrimination of parotid neoplasms from the normal parotid gland by use of Raman spectroscopy and support vector machine. Oral Oncol. 2011, 47, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Czaplicka, M.; Kowalska, A.A.; Nowicka, A.B.; Kurzydłowski, D.; Gronkiewicz, Z.; Machulak, A.; Kukwa, W.; Kamińska, A. Raman spectroscopy and surface-enhanced Raman spectroscopy (SERS) spectra of salivary glands carcinoma, tumor and healthy tissues and their homogenates analyzed by chemometry: Towards development of the novel tool for clinical diagnosis. Anal. Chim. Acta 2021, 1177, 338784. [Google Scholar] [CrossRef] [PubMed]
- Brozek-Pluska, B.; Kopec, M.; Niedzwiecka, I.; Morawiec-Sztandera, A. Label-free determination of lipid composition and secondary protein structure of human salivary noncancerous and cancerous tissues by Raman microspectroscopy. Analyst 2015, 140, 2107–2113. [Google Scholar] [CrossRef]
- Meyer, T.J.; Gerhard-Hartmann, E.; Lodes, N.; Scherzad, A.; Hagen, R.; Steinke, M.; Hackenberg, S. Pilot study on the value of Raman spectroscopy in the entity assignment of salivary gland tumors. PLoS ONE 2021, 16, e0257470. [Google Scholar] [CrossRef]
- Mukherjee, A.; Lorenz, A.; Brecht, M. Determination and Monitoring of Quality Parameters: A Detailed Study of Optical Elements of a Lens-Based Raman Spectrometer. Appl. Spectrosc. 2022, 76, 199–206. [Google Scholar] [CrossRef]
- Ostertag, E.; Stefanakis, M.; Rebner, K.; Kessler, R.W. Elastic and inelastic light scattering spectroscopy and its possible use for label-free brain tumor typing. Anal. Bioanal. Chem. 2017, 409, 6613–6623. [Google Scholar] [CrossRef]
- Stefanakis, M.; Lorenz, A.; Bartsch, J.W.; Bassler, M.C.; Wagner, A.; Brecht, M.; Pagenstecher, A.; Schittenhelm, J.; Boldrini, B.; Hakelberg, S.; et al. Formalin Fixation as Tissue Preprocessing for Multimodal Optical Spectroscopy Using the Example of Human Brain Tumour Cross Sections. J. Spectrosc. 2021, 2021, 5598309. [Google Scholar] [CrossRef]
- Bassler, M.C.; Stefanakis, M.; Sequeira, I.; Ostertag, E.; Wagner, A.; Bartsch, J.W.; Roeßler, M.; Mandic, R.; Reddmann, E.F.; Lorenz, A.; et al. Comparison of Whiskbroom and Pushbroom darkfield elastic light scattering spectroscopic imaging for head and neck cancer identification in a mouse model. Anal. Bioanal. Chem. 2021, 413, 7363–7383. [Google Scholar] [CrossRef]
- Talari, A.C.S.; Movasaghi, Z.; Rehman, S.; Rehman, I.u. Raman Spectroscopy of Biological Tissues. ApSRv 2015, 50, 46–111. [Google Scholar] [CrossRef]
- Chan, J.W.; Taylor, D.S.; Zwerdling, T.; Lane, S.M.; Ihara, K.; Huser, T. Micro-Raman Spectroscopy Detects Individual Neoplastic and Normal Hematopoietic Cells. Biophys. J. 2006, 90, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Bonnier, F.; Byrne, H.J. Understanding the molecular information contained in principal component analysis of vibrational spectra of biological systems. Analyst 2012, 137, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Davis, C.; Cai, W.; He, L.; Chen, X.; Dai, H. Circulation and long-term fate of functionalized, biocompatible single-walled carbon nanotubes in mice probed by Raman spectroscopy. Proc. Natl. Acad. Sci. USA 2008, 105, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Dukor, R.K. Vibrational Spectroscopy in the Detection of Cancer. In Handbook of Vibrational Spectroscopy; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2001. [Google Scholar]
- Schulz, H.; Baranska, M. Identification and quantification of valuable plant substances by IR and Raman spectroscopy. Vib. Spectrosc. 2007, 43, 13–25. [Google Scholar] [CrossRef]
- Gniadecka, M.; Wulf, H.C.; Nymark Mortensen, N.; Faurskov Nielsen, O.; Christensen, D.H. Diagnosis of Basal Cell Carcinoma by Raman Spectroscopy. J. Raman Spectrosc. 1997, 28, 125–129. [Google Scholar] [CrossRef]
- Stone, N.; Kendall, C.; Smith, J.; Crow, P.; Barr, H. Raman spectroscopy for identification of epithelial cancers. Faraday Discuss. 2004, 126, 141–157. [Google Scholar] [CrossRef]
- Cheng, W.-T.; Liu, M.-T.; Liu, H.-N.; Lin, S.-Y. Micro-Raman spectroscopy used to identify and grade human skin pilomatrixoma. Microsc. Res. Tech. 2005, 68, 75–79. [Google Scholar] [CrossRef]
- Silveira, L., Jr.; Sathaiah, S.; Zângaro, R.A.; Pacheco, M.T.T.; Chavantes, M.C.; Pasqualucci, C.A.G. Correlation between near-infrared Raman spectroscopy and the histopathological analysis of atherosclerosis in human coronary arteries. Lasers Surg. Med. 2002, 30, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Ó Faoláin, E.; Hunter, M.B.; Byrne, J.M.; Kelehan, P.; McNamara, M.; Byrne, H.J.; Lyng, F.M. A study examining the effects of tissue processing on human tissue sections using vibrational spectroscopy. Vib. Spectrosc. 2005, 38, 121–127. [Google Scholar] [CrossRef]
- Lau, D.P.; Huang, Z.; Lui, H.; Man, C.S.; Berean, K.; Morrison, M.D.; Zeng, H. Raman spectroscopy for optical diagnosis in normal and cancerous tissue of the nasopharynx—Preliminary findings. Lasers Surg. Med. 2003, 32, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.; Dalal, K.; Naglot, S.; Aggarwal, P.; Murali Krishna, C. Serum Based Diagnosis of Asthma Using Raman Spectroscopy: An Early Phase Pilot Study. PLoS ONE 2013, 8, e78921. [Google Scholar] [CrossRef] [PubMed]
- Almond, L.M.; Hutchings, J.; Lloyd, G.; Barr, H.; Shepherd, N.; Day, J.; Stevens, O.; Sanders, S.; Wadley, M.; Stone, N.; et al. Endoscopic Raman spectroscopy enables objective diagnosis of dysplasia in Barrett’s esophagus. Gastrointest. Endosc. 2014, 79, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Khristoforova, Y.; Bratchenko, L.; Bratchenko, I. Combination of Raman spectroscopy and chemometrics: A review of recent studies published in the Spectrochimica Acta, Part A: Molecular and Biomolecular Spectroscopy Journal. arXiv 2022, arXiv:2210.10051. [Google Scholar]
- Boehmke, B.; Greenwell, B.M. Hands-on Machine Learning with R; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Kessler, W. Multivariate Datenanalyse: Für die Pharma, Bio-und Prozessanalytik; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Calvo, M.B.; Figueroa, A.; Pulido, E.G.; Campelo, R.G.; Aparicio, L.A. Potential Role of Sugar Transporters in Cancer and Their Relationship with Anticancer Therapy. Int. J. Endocrinol. 2010, 2010, 205357. [Google Scholar] [CrossRef]
- Romero-Garcia, S.; Lopez-Gonzalez, J.S.; B’ez-Viveros, J.L.; Aguilar-Cazares, D.; Prado-Garcia, H. Tumor cell metabolism. Cancer Biol. Ther. 2011, 12, 939–948. [Google Scholar] [CrossRef]
- Ackerman, D.; Simon, M.C. Hypoxia, lipids, and cancer: Surviving the harsh tumor microenvironment. Trends Cell Biol. 2014, 24, 472–478. [Google Scholar] [CrossRef]
- Zaidi, N.; Lupien, L.; Kuemmerle, N.B.; Kinlaw, W.B.; Swinnen, J.V.; Smans, K. Lipogenesis and lipolysis: The pathways exploited by the cancer cells to acquire fatty acids. Prog. Lipid Res. 2013, 52, 585–589. [Google Scholar] [CrossRef]
- Donadio, E.; Giusti, L.; Seccia, V.; Ciregia, F.; da Valle, Y.; Dallan, I.; Ventroni, T.; Giannaccini, G.; Sellari-Franceschini, S.; Lucacchini, A. New Insight into Benign Tumours of Major Salivary Glands by Proteomic Approach. PLoS ONE 2013, 8, e71874. [Google Scholar] [CrossRef] [PubMed]
- Kuhajda, F.P. Fatty-acid synthase and human cancer: New perspectives on its role in tumor biology. Nutrition 2000, 16, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Egeblad, M.; Rasch, M.G.; Weaver, V.M. Dynamic interplay between the collagen scaffold and tumor evolution. Curr. Opin. Cell Biol. 2010, 22, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Cescon, M.; Bonaldo, P. Collagen VI in cancer and its biological mechanisms. Trends Mol. Med. 2013, 19, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Chaplin, A.J.; Darke, P.; Patel, S. Tyrosine-rich crystals in pleomorphic adenomas of parotid glands. J. Oral Pathol. Med. 1983, 12, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Koklesova, L.; Liskova, A.; Samec, M.; Zhai, K.; Abotaleb, M.; Ashrafizadeh, M.; Brockmueller, A.; Shakibaei, M.; Biringer, K.; Bugos, O.; et al. Carotenoids in Cancer Metastasis—Status Quo and Outlook. Biomolecules 2020, 10, 1653. [Google Scholar] [CrossRef] [PubMed]
- Chimento, A.; Casaburi, I.; Avena, P.; Trotta, F.; De Luca, A.; Rago, V.; Pezzi, V.; Sirianni, R. Cholesterol and Its Metabolites in Tumor Growth: Therapeutic Potential of Statins in Cancer Treatment. Front. Endocrinol. 2019, 9, 807. [Google Scholar] [CrossRef]
- Llaverias, G.; Danilo, C.; Mercier, I.; Daumer, K.; Capozza, F.; Williams, T.M.; Sotgia, F.; Lisanti, M.P.; Frank, P.G. Role of Cholesterol in the Development and Progression of Breast Cancer. Am. J. Pathol. 2011, 178, 402–412. [Google Scholar] [CrossRef]
- Yue, S.; Li, J.; Lee, S.Y.; Lee, H.J.; Shao, T.; Song, B.; Cheng, L.; Masterson, T.A.; Liu, X.; Ratliff, T.L.; et al. Cholesteryl Ester Accumulation Induced by PTEN Loss and PI3K/AKT Activation Underlies Human Prostate Cancer Aggressiveness. Cell Metab. 2014, 19, 393–406. [Google Scholar] [CrossRef]
- Czamara, K.; Majzner, K.; Pacia, M.Z.; Kochan, K.; Kaczor, A.; Barańska, M. Raman spectroscopy of lipids: A review. J. Raman Spectrosc. 2015, 46, 4–20. [Google Scholar] [CrossRef]
- Warnecke, P.M.; Bestor, T.H. Cytosine methylation and human cancer. Curr. Opin. Oncol. 2000, 12, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Lunt, S.Y.; Heiden, M.G.V. Aerobic Glycolysis: Meeting the Metabolic Requirements of Cell Proliferation. Annu. Rev. Cell Dev. Biol. 2011, 27, 441–464. [Google Scholar] [CrossRef] [PubMed]
- Badawy, A.A.-B. Targeting tryptophan availability to tumors: The answer to immune escape? Immunol. Cell Biol. 2018, 96, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Betz, V.; Schneckenburger, H.; Alleroeder, H.; Sybrecht, G.; Meyer, J.-U. Evaluation of Changes in the NADH Level between Carcinogenic and Normal Tissue Samples by Use of Fluorescence Spectroscopy; SPIE: Bellingham, WA, USA, 1995; Volume 2324. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Raman Shift/cm−1 | Assignment | Cause | Reference [44] |
|---|---|---|---|---|
| (1) | 915; 920 | -; C-C stretch | Ribose RNA; collagen | [45,46] |
| (2) | 1043 | ring stretching | Collagen proline | [46] |
| (3) | 1158; 1168 | C-N stretching; ν(C=C); ν(C-C) | Proteins/lipids | [47,48] |
| (4) | 1197; 1204 | Antisymmetric phosphate vibrations; amide III, CH2 wagging vibrations | Glycine backbone or proline side chains | [48,49] |
| (5) | 1222; 1228 | C-N stretching and N-H bending, thymine, adenine stretch | Amide III, proteins, DNA/RNA | [47,50] |
| (6) | 1304 | CH2/CH3 deformation, twisting or bending | Lipids, collagen | [46,51] |
| (7) | 1337 | CH2/CH3 wagging, twisting and/or bending mode | Collagens, lipids, amide III (proteins) | [45,48,52] |
| (8) | 1360 | - | Tryptophan | [44] |
| (9) | 1396 | - | β-carotene | [44] |
| (10) | 1443; 1454 | CH2 deformation; CH2 stretching/CH3 asymmetric deformation | Lipids, proteins, triglycerides (fatty acids); elastin, collagen, phospholipids | [51,53,54,55] |
| (11) | 1517 | C-C stretch mode | β-Carotene accumulation | [53] |
| (12) | 1585 | C=C olefinic stretch | Proteins | [54,56] |
| (13) | 1628; 1640 | Cα=Cα stretch; - | Proteins; amide I (proteins) | [44,57] |
| (14) | 1654 | C-C stretch, C=O stretching mode | Amide I (proteins), collagen, lipids | [46,48,51] |
| Entity | Total Spectra | Correctly Assigned | Correctly Assigned/% | Accuracy /% | Sensitivity /% | Specificity /% | Precision /% |
|---|---|---|---|---|---|---|---|
| Salivary gland tissue | 94 | 91 | 97 | 94 | 94 | 95 | 94 |
| Pleomorphic adenoma | 35 | 31 | 89 | ||||
| Warthin tumor | 47 | 43 | 91 |
| Entity | Prediction Spectra | Model Classified as | HE Diagnosed as |
|---|---|---|---|
| Salivary gland tissue | 1 | Salivary gland tissue | Salivary gland tissue |
| 2 | Salivary gland tissue | Salivary gland tissue | |
| 3 | Salivary gland tissue | Salivary gland tissue | |
| 4 | Salivary gland tissue | Salivary gland tissue | |
| 5 | Salivary gland tissue | Salivary gland tissue | |
| Pleomorphic adenoma | 1 | Pleomorphic adenoma | Pleomorphic adenoma |
| 2 | Pleomorphic adenoma | Pleomorphic adenoma | |
| 3 | Pleomorphic adenoma | Salivary gland tissue | |
| 4 | Pleomorphic adenoma | Pleomorphic adenoma | |
| 5 | Pleomorphic adenoma | Pleomorphic adenoma | |
| Warthin tumor | 1 | Warthin tumor | Warthin tumor |
| 2 | Warthin tumor | Warthin tumor | |
| 3 | Warthin tumor | Warthin tumor | |
| 4 | Warthin tumor | Warthin tumor | |
| 5 | Warthin tumor | Warthin tumor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassler, M.C.; Knoblich, M.; Gerhard-Hartmann, E.; Mukherjee, A.; Youssef, A.; Hagen, R.; Haug, L.; Goncalves, M.; Scherzad, A.; Stöth, M.; et al. Differentiation of Salivary Gland and Salivary Gland Tumor Tissue via Raman Imaging Combined with Multivariate Data Analysis. Diagnostics 2024, 14, 92. https://doi.org/10.3390/diagnostics14010092
Bassler MC, Knoblich M, Gerhard-Hartmann E, Mukherjee A, Youssef A, Hagen R, Haug L, Goncalves M, Scherzad A, Stöth M, et al. Differentiation of Salivary Gland and Salivary Gland Tumor Tissue via Raman Imaging Combined with Multivariate Data Analysis. Diagnostics. 2024; 14(1):92. https://doi.org/10.3390/diagnostics14010092
Chicago/Turabian StyleBassler, Miriam C., Mona Knoblich, Elena Gerhard-Hartmann, Ashutosh Mukherjee, Almoatazbellah Youssef, Rudolf Hagen, Lukas Haug, Miguel Goncalves, Agmal Scherzad, Manuel Stöth, and et al. 2024. "Differentiation of Salivary Gland and Salivary Gland Tumor Tissue via Raman Imaging Combined with Multivariate Data Analysis" Diagnostics 14, no. 1: 92. https://doi.org/10.3390/diagnostics14010092
APA StyleBassler, M. C., Knoblich, M., Gerhard-Hartmann, E., Mukherjee, A., Youssef, A., Hagen, R., Haug, L., Goncalves, M., Scherzad, A., Stöth, M., Ostertag, E., Steinke, M., Brecht, M., Hackenberg, S., & Meyer, T. J. (2024). Differentiation of Salivary Gland and Salivary Gland Tumor Tissue via Raman Imaging Combined with Multivariate Data Analysis. Diagnostics, 14(1), 92. https://doi.org/10.3390/diagnostics14010092