
Development of a Machine Learning Algorithm to Correlate Lumbar Disc Height on X-rays with Disc Bulging or Herniation

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
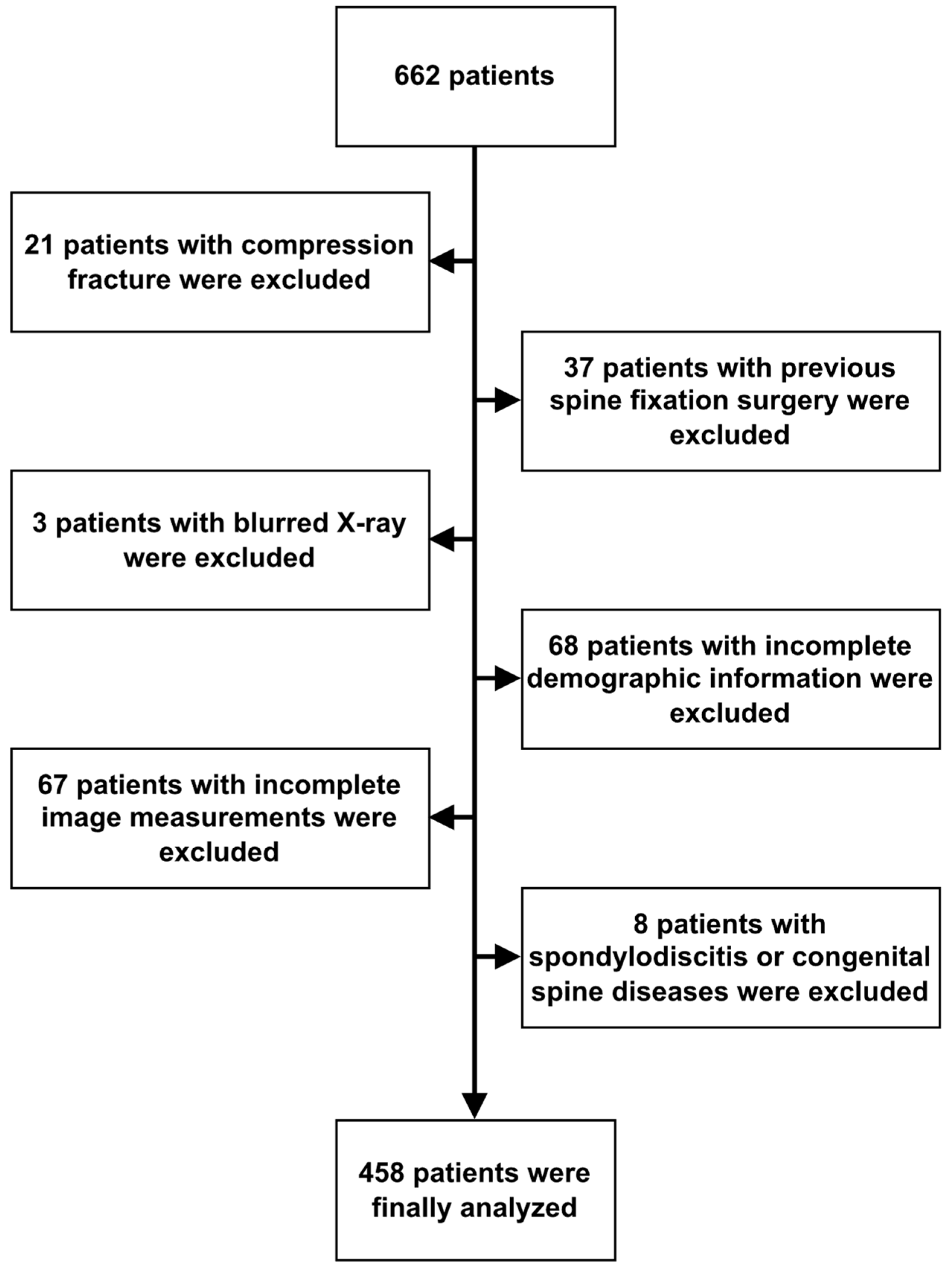
2.1. Participants and Study Design
2.2. Definition of Disc Bulging, Protrusion, and Herniated Disc
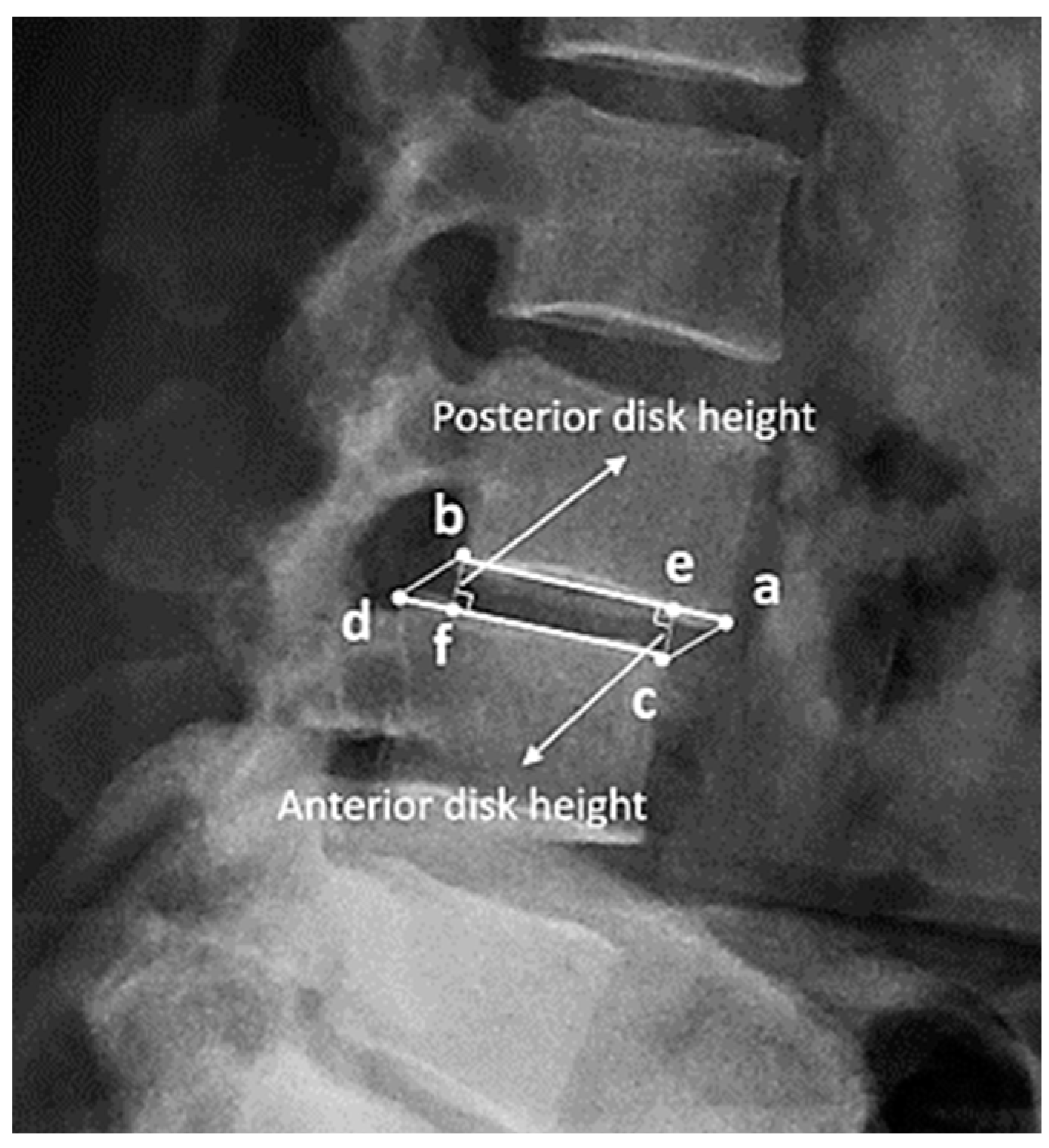
2.3. Definition and Measurement of Disc Height
Measurement of Disc Height with BiLuNet
2.4. Statistical Analysis
2.4.1. LASSO
2.4.2. MARS
2.4.3. Decision Tree
2.4.4. Random Forest
2.4.5. Extreme Gradient Boosting
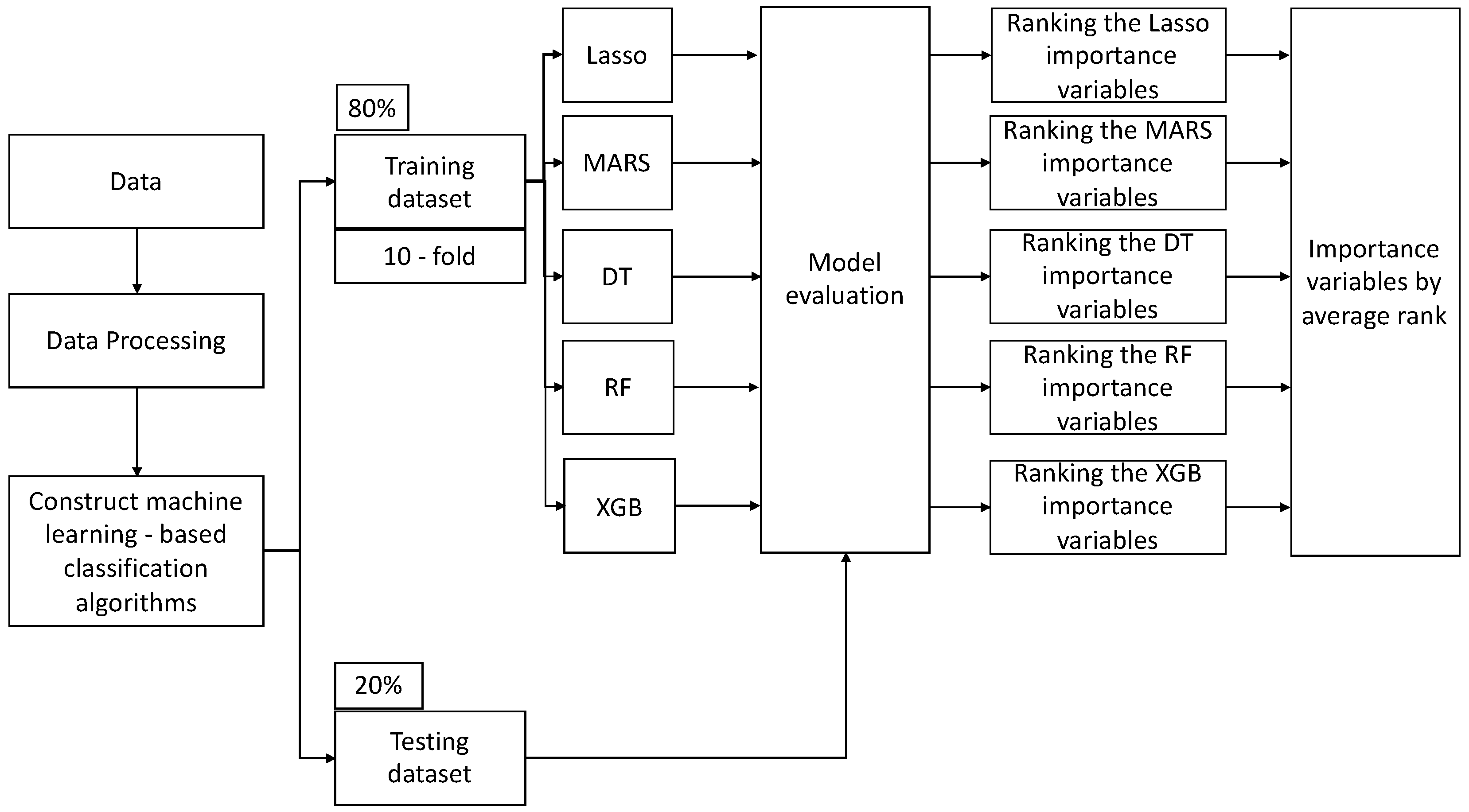
2.4.6. ML Workflow and Implementation Details
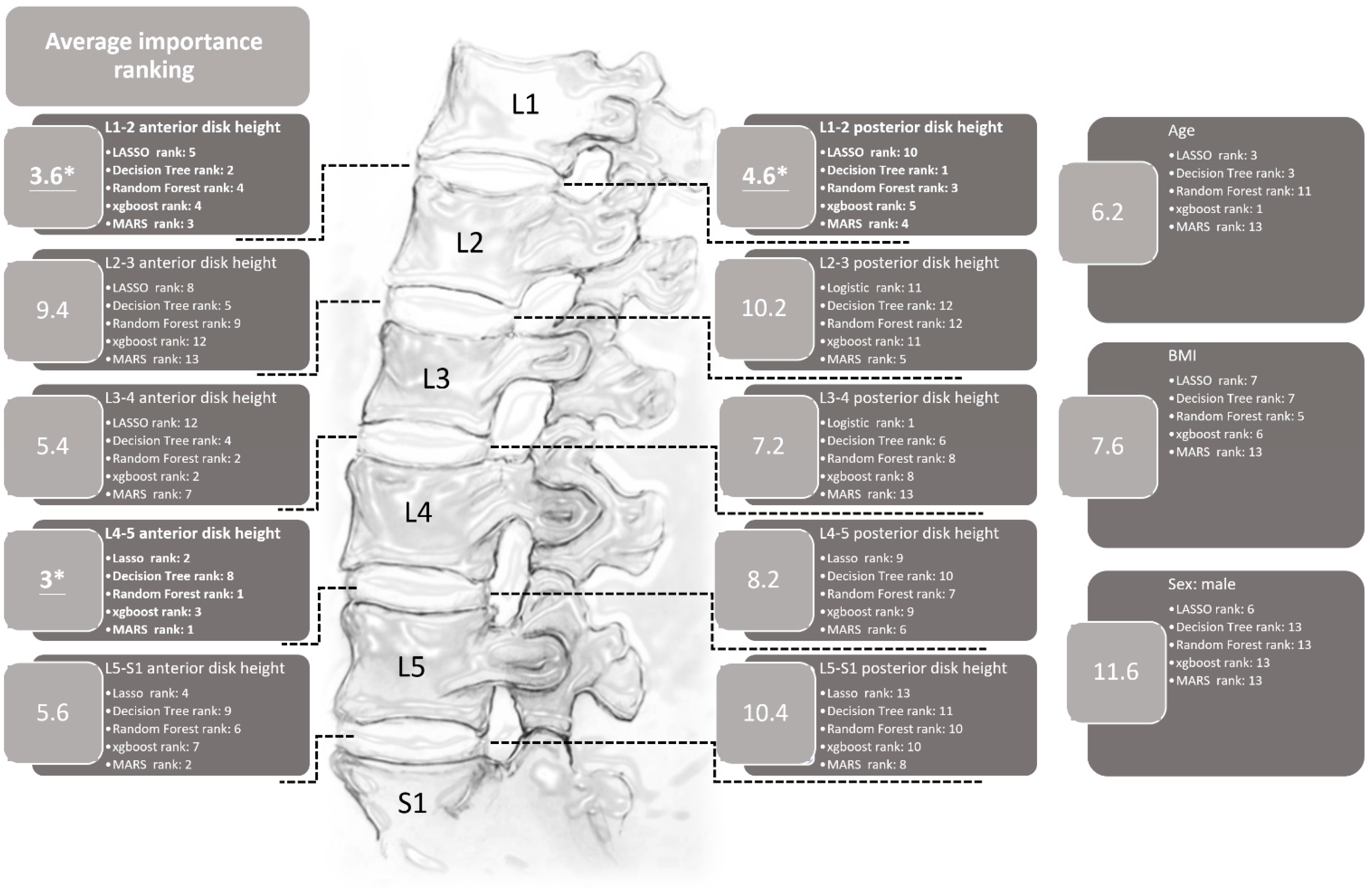
3. Results
4. Discussion
4.1. Clinical Implications
4.2. Limitations and Work in Progress
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deyo, R.A.; Loeser, J.D.; Bigos, S.J. Herniated lumbar intervertebral disk. Ann. Intern. Med. 1990, 112, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Barber, R.M.; Foreman, K.J.; Abbasoglu Ozgoren, A.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Abraham, J.P.; Abubakar, I.; Abu-Raddad, L.J.; et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015, 386, 2145–2191. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, S.C.; Eck, J.C. Clinical evaluation and treatment options for herniated lumbar disc. Am. Fam. Physician 1999, 59, 575–582, 578–587. [Google Scholar] [PubMed]
- Takahashi, K.; Kagechika, K.; Takino, T.; Matsui, T.; Miyazaki, T.; Shima, I. Changes in epidural pressure during walking in patients with lumbar spinal stenosis. Spine 1995, 20, 2746–2749. [Google Scholar] [CrossRef] [PubMed]
- Rydevik, B. Neurophysiology of cauda equina compression. Acta Orthop. Scand. Suppl. 1993, 251, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.R.; Collins, T.A.; Porter, R.W.; Kidd, C. Laser Doppler study of porcine cauda equina blood flow. The effect of electrical stimulation of the rootlets during single and double site, low pressure compression of the cauda equina. Spine 1995, 20, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Ooi, Y.; Mita, F.; Satoh, Y. Myeloscopic study on lumbar spinal canal stenosis with special reference to intermittent claudication. Spine 1990, 15, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Wassenaar, M.; van Rijn, R.M.; van Tulder, M.W.; Verhagen, A.P.; van der Windt, D.A.; Koes, B.W.; de Boer, M.R.; Ginai, A.Z.; Ostelo, R.W. Magnetic resonance imaging for diagnosing lumbar spinal pathology in adult patients with low back pain or sciatica: A diagnostic systematic review. Eur. Spine J. 2012, 21, 220–227. [Google Scholar] [CrossRef]
- Ikawa, M.; Atsuta, Y.; Tsunekawa, H. Ectopic firing due to artificial venous stasis in rat lumbar spinal canal stenosis model: A possible pathogenesis of neurogenic intermittent claudication. Spine 2005, 30, 2393–2397. [Google Scholar] [CrossRef]
- Kaiser, M.C.; Capesius, P.; Roilgen, A.; Sandt, G.; Poos, D.; Gratia, G. Epidural venous stasis in spinal stenosis. CT appearance. Neuroradiology 1984, 26, 435–438. [Google Scholar] [CrossRef]
- Jarvik, J.G.; Deyo, R.A. Diagnostic evaluation of low back pain with emphasis on imaging. Ann. Intern. Med. 2002, 137, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.A.; Bussières, A. Diagnostic imaging for spinal disorders in the elderly: A narrative review. Chiropr. Man. Ther. 2012, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Jarvik, J.G.; Hollingworth, W.; Martin, B.; Emerson, S.S.; Gray, D.T.; Overman, S.; Robinson, D.; Staiger, T.; Wessbecher, F.; Sullivan, S.D.; et al. Rapid magnetic resonance imaging vs radiographs for patients with low back pain: A randomized controlled trial. JAMA 2003, 289, 2810–2818. [Google Scholar] [CrossRef] [PubMed]
- Steurer, J.; Roner, S.; Gnannt, R.; Hodler, J. Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: A systematic literature review. BMC Musculoskelet. Disord. 2011, 12, 175. [Google Scholar] [CrossRef]
- Deyo, R.A.; Bigos, S.J.; Maravilla, K.R. Diagnostic imaging procedures for the lumbar spine. Ann. Intern. Med. 1989, 111, 865–867. [Google Scholar] [CrossRef]
- Mostofi, K.; Karimi Khouzani, R. Reliability of the Path of the Sciatic Nerve, Congruence between Patients’ History and Medical Imaging Evidence of Disc Herniation and Its Role in Surgical Decision Making. Asian Spine J. 2015, 9, 200–204. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, P.C.; Krause, J.; Peng, L. How to Read Articles That Use Machine Learning: Users’ Guides to the Medical Literature. JAMA 2019, 322, 1806–1816. [Google Scholar] [CrossRef] [PubMed]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Qadri, S.F.; Lin, H.; Shen, L.; Ahmad, M.; Qadri, S.; Khan, S.; Khan, M.; Zareen, S.S.; Akbar, M.A.; Bin Heyat, M.B.; et al. CT-Based Automatic Spine Segmentation Using Patch-Based Deep Learning. Int. J. Intell. Syst. 2023, 2023, 2345835. [Google Scholar] [CrossRef]
- Ahmad, M.; Ding, Y.; Furqan Qadri, S.; Yang, J. Convolutional-neural-network-based feature extraction for liver segmentation from CT images. In Proceedings of the Eleventh International Conference on Digital Image Processing (ICDIP 2019), Guangzhou, China, 10–13 May 2019; p. 159. [Google Scholar]
- Katsos, K.; Johnson, S.E.; Ibrahim, S.; Bydon, M. Current Applications of Machine Learning for Spinal Cord Tumors. Life 2023, 13, 520. [Google Scholar] [CrossRef]
- Chang, M.; Canseco, J.A.; Nicholson, K.J.; Patel, N.; Vaccaro, A.R. The Role of Machine Learning in Spine Surgery: The Future Is Now. Front. Surg. 2020, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Chen, S.; Jiang, N.; Hu, H. An Effective WSSENet-Based Similarity Retrieval Method of Large Lung CT Image Databases. KSII Trans. Internet Inf. Syst. 2022, 16, 2359–2376. [Google Scholar] [CrossRef]
- Cao, Z.; Wang, Y.; Zheng, W.; Yin, L.; Tang, Y.; Miao, W.; Liu, S.; Yang, B. The algorithm of stereo vision and shape from shading based on endoscope imaging. Biomed. Signal Process. Control 2022, 76, 103658. [Google Scholar] [CrossRef]
- Liu, Y.; Tian, J.; Hu, R.; Yang, B.; Liu, S.; Yin, L.; Zheng, W. Improved Feature Point Pair Purification Algorithm Based on SIFT During Endoscope Image Stitching. Front. Neurorobot. 2022, 16, 840594. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yang, B.; Wang, Y.; Tian, J.; Yin, L.; Zheng, W. 2D/3D Multimode Medical Image Registration Based on Normalized Cross-Correlation. Appl. Sci. 2022, 12, 2828. [Google Scholar] [CrossRef]
- Amin, A.; Abbas, M.; Salam, A.A. Automatic Detection and classification of Scoliosis from Spine X-rays using Transfer Learning. In Proceedings of the 2022 2nd International Conference on Digital Futures and Transformative Technologies (ICoDT2), Rawalpindi, Pakistan, 24–26 May 2022; pp. 1–6. [Google Scholar]
- Zhang, B.; Yu, K.; Ning, Z.; Wang, K.; Dong, Y.; Liu, X.; Liu, S.; Wang, J.; Zhu, C.; Yu, Q.; et al. Deep learning of lumbar spine X-ray for osteopenia and osteoporosis screening: A multicenter retrospective cohort study. Bone 2020, 140, 115561. [Google Scholar] [CrossRef] [PubMed]
- Adankon, M.M.; Dansereau, J.; Labelle, H.; Cheriet, F. Non invasive classification system of scoliosis curve types using least-squares support vector machines. Artif. Intell. Med. 2012, 56, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.K.; Hassanpour, S.; Heagerty, P.J.; Rundell, S.D.; Suri, P.; Huhdanpaa, H.T.; James, K.; Carrell, D.S.; Langlotz, C.P.; Organ, N.L.; et al. Comparison of Natural Language Processing Rules-based and Machine-learning Systems to Identify Lumbar Spine Imaging Findings Related to Low Back Pain. Acad. Radiol. 2018, 25, 1422–1432. [Google Scholar] [CrossRef]
- Jin, M.; Schröder, M.; Staartjes, V.E. 15—Artificial Intelligence and Machine Learning in Spine Surgery. In Robotic and Navigated Spine Surgery; Veeravagu, A., Wang, M.Y., Eds.; Elsevier: New Delhi, India, 2023; pp. 213–229. [Google Scholar]
- Masood, R.F.; Taj, I.A.; Khan, M.B.; Qureshi, M.A.; Hassan, T. Deep Learning based Vertebral Body Segmentation with Extraction of Spinal Measurements and Disorder Disease Classification. Biomed. Signal Process. Control 2022, 71, 103230. [Google Scholar] [CrossRef]
- Jujjavarapu, C.; Pejaver, V.; Cohen, T.A.; Mooney, S.D.; Heagerty, P.J.; Jarvik, J.G. A Comparison of Natural Language Processing Methods for the Classification of Lumbar Spine Imaging Findings Related to Lower Back Pain. Acad. Radiol. 2022, 29 (Suppl. 3), S188–S200. [Google Scholar] [CrossRef]
- Nam, K.H.; Seo, I.; Kim, D.H.; Lee, J.I.; Choi, B.K.; Han, I.H. Machine Learning Model to Predict Osteoporotic Spine with Hounsfield Units on Lumbar Computed Tomography. J. Korean Neurosurg. Soc. 2019, 62, 442–449. [Google Scholar] [CrossRef] [PubMed]
- D’Antoni, F.; Russo, F.; Ambrosio, L.; Vollero, L.; Vadalà, G.; Merone, M.; Papalia, R.; Denaro, V. Artificial Intelligence and Computer Vision in Low Back Pain: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10909. [Google Scholar] [CrossRef] [PubMed]
- Onishi, F.J.; de Paiva Neto, M.A.; Cavalheiro, S.; Centeno, R.S. Morphometric analysis of 900 lumbar intervertebral discs: Anterior and posterior height analysis and their ratio. Interdiscip. Neurosurg. 2019, 18, 100523. [Google Scholar] [CrossRef]
- Hung, I.Y.-J.; Shih, T.T.-F.; Chen, B.-B.; Guo, Y.L. Prediction of Lumbar Disc Bulging and Protrusion by Anthropometric Factors and Disc Morphology. Int. J. Environ. Res. Public Health 2021, 18, 2521. [Google Scholar] [CrossRef] [PubMed]
- Wáng, J.Q.; Kaplar, Z.; Deng, M.; Griffith, J.F.; Leung, J.C.; Kwok, A.W.; Kwok, T.; Leung, P.C.; Wáng, Y.X. Thoracolumbar intervertebral disc area morphometry in elderly Chinese men and women: Radiographic quantifications at baseline and changes at year-4 follow-up. bioRxiv 2017, 139402. [Google Scholar] [CrossRef] [PubMed]
- Muellner, M.; Wang, Z.; Hu, Z.; Hardt, S.; Pumberger, M.; Becker, L.; Haffer, H. Hip replacement improves lumbar flexibility and intervertebral disc height—A prospective observational investigation with standing and sitting assessment of patients undergoing total hip arthroplasty. Int. Orthop. 2022, 46, 2195–2203. [Google Scholar] [CrossRef]
- Lv, X.; Liu, Y.; Zhou, S.; Wang, Q.; Gu, H.; Fu, X.; Ding, Y.; Zhang, B.; Dai, M. Correlations between the feature of sagittal spinopelvic alignment and facet joint degeneration: A retrospective study. BMC Musculoskelet. Disord. 2016, 17, 341. [Google Scholar] [CrossRef]
- Kumar, N.; Shah, S.M.; Ng, Y.H.; Pannierselvam, V.K.; Dasde, S.; Shen, L. Role of coflex as an adjunct to decompression for symptomatic lumbar spinal stenosis. Asian Spine J. 2014, 8, 161–169. [Google Scholar] [CrossRef]
- Tran, V.L.; Lin, H.Y.; Liu, H.W.; Jang, F.J.; Tseng, C.H. BiLuNet: A Multi-path Network for Semantic Segmentation on X-ray Images. In Proceedings of the 2020 25th International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021; pp. 10034–10041. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Kwon, S.; Lee, S.; Na, O. Tuning parameter selection for the adaptive LASSO in the autoregressive model. J. Korean Stat. Soc. 2017, 46, 285–297. [Google Scholar] [CrossRef]
- Tsai, M.H.; Jhou, M.J.; Liu, T.C.; Fang, Y.W.; Lu, C.J. An integrated machine learning predictive scheme for longitudinal laboratory data to evaluate the factors determining renal function changes in patients with different chronic kidney disease stages. Front. Med. 2023, 10, 1155426. [Google Scholar] [CrossRef]
- Che, D.; Liu, Q.; Rasheed, K.; Tao, X. Decision tree and ensemble learning algorithms with their applications in bioinformatics. Adv. Exp. Med. Biol. 2011, 696, 191–199. [Google Scholar] [CrossRef]
- Sarica, A.; Cerasa, A.; Quattrone, A. Random Forest Algorithm for the Classification of Neuroimaging Data in Alzheimer’s Disease: A Systematic Review. Front. Aging Neurosci. 2017, 9, 329. [Google Scholar] [CrossRef] [PubMed]
- Torlay, L.; Perrone-Bertolotti, M.; Thomas, E.; Baciu, M. Machine learning-XGBoost analysis of language networks to classify patients with epilepsy. Brain Inform. 2017, 4, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Burns, J.E.; Yao, J.; Summers, R.M. Vertebral Body Compression Fractures and Bone Density: Automated Detection and Classification on CT Images. Radiology 2017, 284, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Bar, A.; Wolf, L.; Bergman Amitai, O.; Toledano, E.; Elnekave, E. Compression fractures detection on CT. In Proceedings of the Society of Photo-Optical Instrumentation Engineers (SPIE) Conference Series, Orlando, FL, USA, 1 March 2017; p. 1013440. [Google Scholar]
- Frighetto-Pereira, L.; Rangayyan, R.M.; Metzner, G.A.; de Azevedo-Marques, P.M.; Nogueira-Barbosa, M.H. Shape, texture and statistical features for classification of benign and malignant vertebral compression fractures in magnetic resonance images. Comput. Biol. Med. 2016, 73, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Karhade, A.V.; Thio, Q.; Ogink, P.T.; Shah, A.A.; Bono, C.M.; Oh, K.S.; Saylor, P.J.; Schoenfeld, A.J.; Shin, J.H.; Harris, M.B.; et al. Development of Machine Learning Algorithms for Prediction of 30-Day Mortality After Surgery for Spinal Metastasis. Neurosurgery 2019, 85, E83–E91. [Google Scholar] [CrossRef]
- Ogink, P.T.; Karhade, A.V.; Thio, Q.; Gormley, W.B.; Oner, F.C.; Verlaan, J.J.; Schwab, J.H. Predicting discharge placement after elective surgery for lumbar spinal stenosis using machine learning methods. Eur. Spine J. 2019, 28, 1433–1440. [Google Scholar] [CrossRef]
- Ramkumar, P.N.; Karnuta, J.M.; Navarro, S.M.; Haeberle, H.S.; Iorio, R.; Mont, M.A.; Patterson, B.M.; Krebs, V.E. Preoperative Prediction of Value Metrics and a Patient-Specific Payment Model for Primary Total Hip Arthroplasty: Development and Validation of a Deep Learning Model. J. Arthroplasty 2019, 34, 2228–2234.e2221. [Google Scholar] [CrossRef]
- Stopa, B.M.; Robertson, F.C.; Karhade, A.V.; Chua, M.; Broekman, M.L.D.; Schwab, J.H.; Smith, T.R.; Gormley, W.B. Predicting nonroutine discharge after elective spine surgery: External validation of machine learning algorithms. J. Neurosurg. Spine 2019, 31, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Thio, Q.; Karhade, A.V.; Ogink, P.T.; Raskin, K.A.; De Amorim Bernstein, K.; Lozano Calderon, S.A.; Schwab, J.H. Can Machine-learning Techniques Be Used for 5-year Survival Prediction of Patients With Chondrosarcoma? Clin. Orthop. Relat. Res. 2018, 476, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Trinh, G.M.; Shao, H.C.; Hsieh, K.L.; Lee, C.Y.; Liu, H.W.; Lai, C.W.; Chou, S.Y.; Tsai, P.I.; Chen, K.J.; Chang, F.C.; et al. Detection of Lumbar Spondylolisthesis from X-ray Images Using Deep Learning Network. J. Clin. Med. 2022, 11, 5450. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, T.; Cheung, K.M.; Shea, G.K. Application of deep learning upon spinal radiographs to predict progression in adolescent idiopathic scoliosis at first clinic visit. EClinicalMedicine 2021, 42, 101220. [Google Scholar] [CrossRef]
- Brinckmann, P.; Grootenboer, H. Change of disc height, radial disc bulge, and intradiscal pressure from discectomy. An in vitro investigation on human lumbar discs. Spine 1991, 16, 641–646. [Google Scholar] [CrossRef]
- Nachemson, A.L.; Schultz, A.B.; Berkson, M.H. Mechanical properties of human lumbar spine motion segments. Influence of age, sex, disc level, and degeneration. Spine 1979, 4, 1–8. [Google Scholar] [CrossRef]
- Alexandru, D.; So, W. Evaluation and management of vertebral compression fractures. Perm. J. 2012, 16, 46–51. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LDBH n = 259 | Non-LDBH n = 199 | |
|---|---|---|
| Age (mean ± SD) | 60.00 ± 14.00 | 58.98 ± 14.14 |
| Sex = Male (%) | 133 (51.4) | 100 (50.3) |
| BMI (mean ± SD) | 25.76 ± 4.09 | 26.33 ± 4.21 |
| Disc height measurement (mean ± SD) (mm) | ||
| Disc height L1-2 anterior | 9.69 ± 2.12 | 9.36 ± 2.19 |
| Disc height L1-2 posterior | 7.46 ± 1.60 | 7.33 ± 1.50 |
| Disc height L2-3 anterior | 10.74 ± 2.40 | 10.26 ± 2.16 |
| Disc height L2-3 posterior | 8.04 ± 2.04 | 7.68 ± 1.79 |
| Disc height L3-4 anterior | 11.83 ± 2.68 | 11.44 ± 2.78 |
| Disc height L3-4 posterior | 8.96 ± 2.74 | 8.28 ± 2.12 |
| Disc height L4-5 anterior | 12.88 ± 8.90 | 11.47 ± 3.76 |
| Disc height L4-5 posterior | 10.99 ± 9.53 | 9.68 ± 5.99 |
| Disc height L5-S1 anterior | 15.10 ± 7.27 | 14.57 ± 7.92 |
| Disc height L5-S1 posterior | 9.59 ± 9.31 | 8.51 ± 5.28 |
| Method | Avg_Accuracy | Avg_Recall | Avg_Precision | Avg_Specificity | Avg_F1 |
|---|---|---|---|---|---|
| Testing Dataset | |||||
| LASSO Regression | 0.615 | 0.857 | 0.600 | 0.333 | 0.706 |
| MARS | 0.689 | 0.924 | 0.676 | 0.357 | 0.778 |
| Decision Tree | 0.516 | 0.592 | 0.547 | 0.429 | 0.569 |
| Random Forest | 0.655 | 0.794 | 0.675 | 0.458 | 0.729 |
| XGBoost | 0.615 | 0.857 | 0.600 | 0.333 | 0.706 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, P.-C.; Chang, W.-S.; Hsiao, K.-Y.; Liu, H.-M.; Shia, B.-C.; Chen, M.-C.; Hsieh, P.-Y.; Lai, T.-W.; Lin, F.-H.; Chang, C.-C. Development of a Machine Learning Algorithm to Correlate Lumbar Disc Height on X-rays with Disc Bulging or Herniation. Diagnostics 2024, 14, 134. https://doi.org/10.3390/diagnostics14020134
Lin P-C, Chang W-S, Hsiao K-Y, Liu H-M, Shia B-C, Chen M-C, Hsieh P-Y, Lai T-W, Lin F-H, Chang C-C. Development of a Machine Learning Algorithm to Correlate Lumbar Disc Height on X-rays with Disc Bulging or Herniation. Diagnostics. 2024; 14(2):134. https://doi.org/10.3390/diagnostics14020134
Chicago/Turabian StyleLin, Pao-Chun, Wei-Shan Chang, Kai-Yuan Hsiao, Hon-Man Liu, Ben-Chang Shia, Ming-Chih Chen, Po-Yu Hsieh, Tseng-Wei Lai, Feng-Huei Lin, and Che-Cheng Chang. 2024. "Development of a Machine Learning Algorithm to Correlate Lumbar Disc Height on X-rays with Disc Bulging or Herniation" Diagnostics 14, no. 2: 134. https://doi.org/10.3390/diagnostics14020134
APA StyleLin, P. -C., Chang, W. -S., Hsiao, K. -Y., Liu, H. -M., Shia, B. -C., Chen, M. -C., Hsieh, P. -Y., Lai, T. -W., Lin, F. -H., & Chang, C. -C. (2024). Development of a Machine Learning Algorithm to Correlate Lumbar Disc Height on X-rays with Disc Bulging or Herniation. Diagnostics, 14(2), 134. https://doi.org/10.3390/diagnostics14020134