
A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database

 ,
,  ,
,  ,
, 
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participating Centers
3.2. Dataset Characteristics
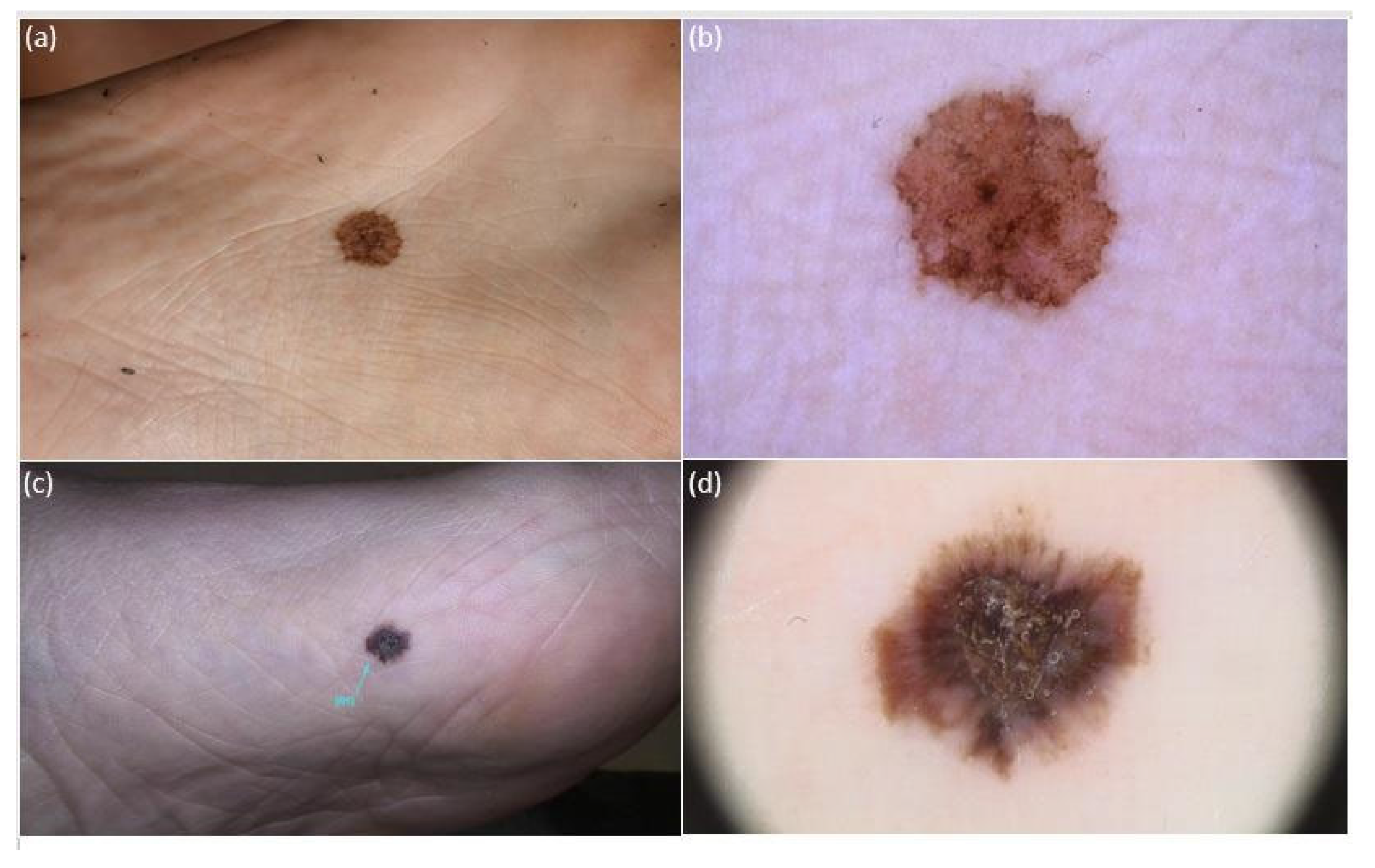
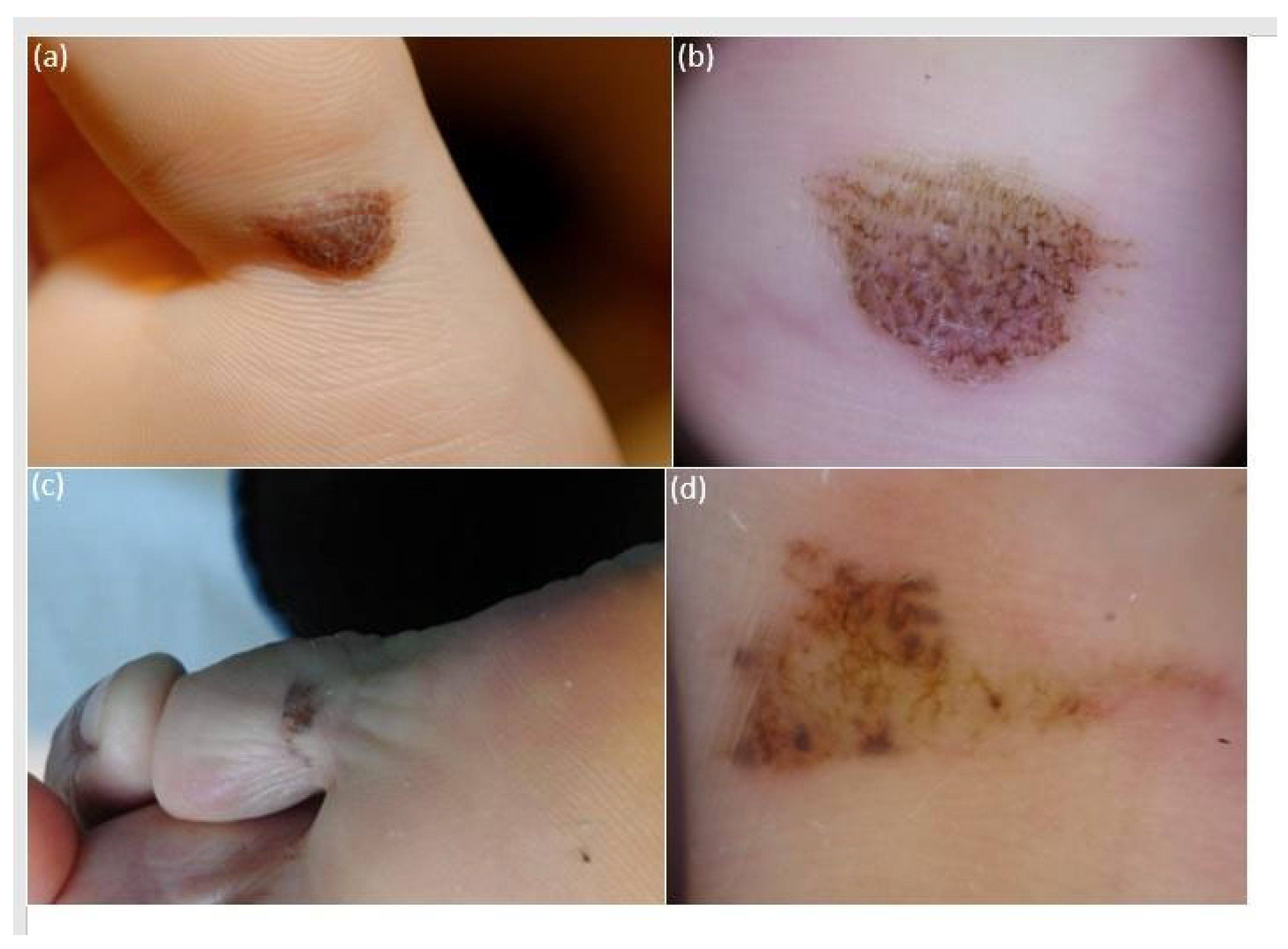
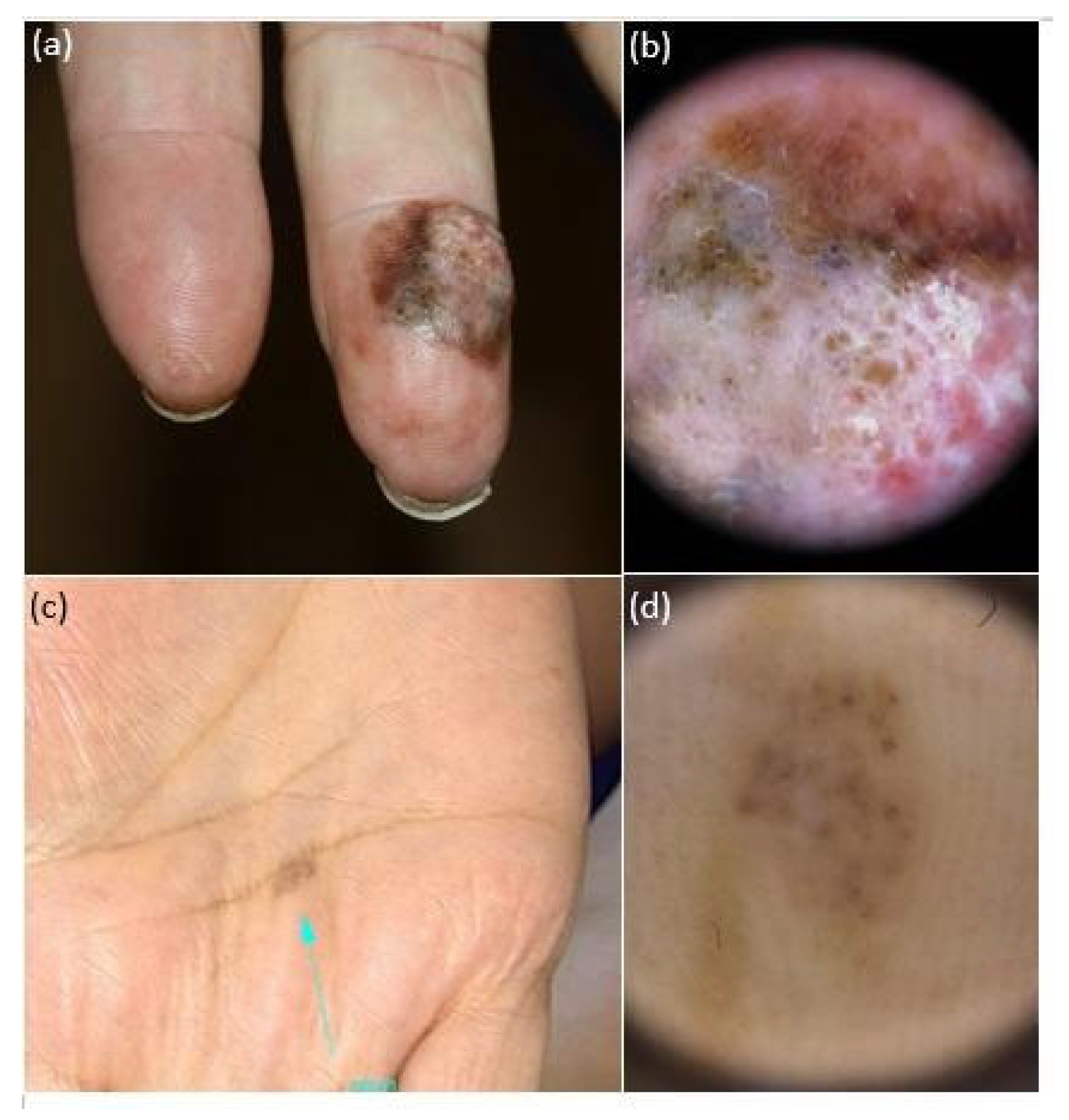
3.3. Lesion Morphological Features
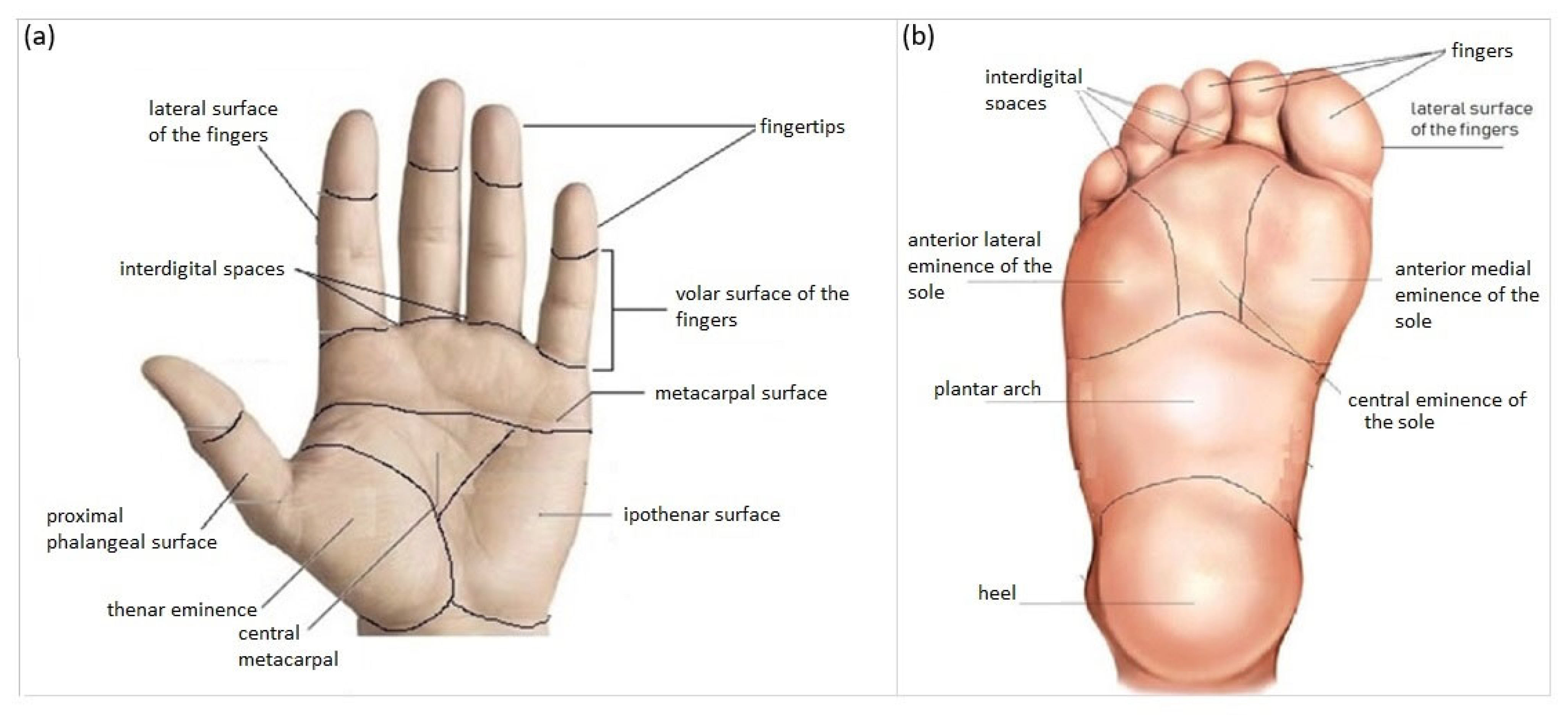
3.4. Lesion Location
3.4.1. All aMPPLs
3.4.2. Malignant aMPPLs
3.4.3. Benign aMPPLs
3.5. Patient Data
3.5.1. Age
3.5.2. Sex
3.6. Patient Optional Data
3.6.1. Anamnestic Data/Risk Factors
3.6.2. Phenotypic Traits
3.7. Device for Image Acquisition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernardes, S.S.; Ferreira, I.; Elder, D.E.; Nobre, A.B.; Martínez-Said, H.; Adams, D.J.; Robles-Espinoza, C.D.; Possik, P.A. More than just acral melanoma: The controversies of defining the disease. J. Pathol. Clin. Res. 2021, 7, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Saida, T. Heterogeneity of the site of origin of malignant melanoma in ungual areas: “subungual” malignant melanoma may be a misnomer. Br. J. Dermatol. 1992, 126, 529. [Google Scholar] [CrossRef] [PubMed]
- Phan, A.; Touzet, S.; Dalle, S.; Ronger-Savlé, S.; Balme, B.; Thomas, L. Acral lentiginous melanoma: A clinicoprognostic study of 126 cases. Br. J. Dermatol. 2006, 155, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Madankumar, R.; Gumaste, P.V.; Martires, K.; Schaffer, P.R.; Choudhary, S.; Falto-Aizpurua, L.; Arora, H.; Kallis, P.J.; Patel, S.; Damanpour, S.; et al. Acral melanocytic lesions in the United States: Prevalence, awareness, and dermoscopic patterns in skin-of-color and non-Hispanic white patients. J. Am. Acad. Dermatol. 2016, 74, 724–730.e1. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yun, S.-J. Acral Melanocytic Neoplasms: A Comprehensive Review of Acral Nevus and Acral Melanoma in Asian Perspective. Dermatopathology 2022, 9, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Roncati, L.; Piscioli, F.; Pusiol, T. SAMPUS, MELTUMP and THIMUMP—Diagnostic Categories Characterized by Uncertain Biological Behavior. Klin. Onkol. 2017, 30, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, C.; Kyrgidis, A.; Ilut, P.A.; Gkentsidi, T.; Manoli, S.-M.; Camela, E.; Apalla, Z.; Lallas, A. Acral Melanocytic Nevi in a High-Risk Population: Prevalence, Clinical Characteristics and Dermatoscopic Patterns. Dermatology 2023, 239, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, A.; Koga, H.; Saida, T. Dermoscopic characteristics of congenital melanocytic nevi affecting acral volar skin. Arch. Dermatol. 2011, 147, 809–813. [Google Scholar] [CrossRef]
- Gumaste, P.V.; Fleming, N.H.; Silva, I.; Shapiro, R.L.; Berman, R.S.; Zhong, J.; Osman, I.; Stein, J.A. Analysis of recurrence patterns in acral versus nonacral melanoma: Should histologic subtype influence treatment guidelines? J. Natl. Compr. Cancer Netw. JNCCN 2014, 12, 1706–1712. [Google Scholar] [CrossRef]
- Saida, T.; Yoshida, N.; Ikegawa, S.; Ishihara, K.; Nakajima, T. Clinical guidelines for the early detection of plantar malignant melanoma. J. Am. Acad. Dermatol. 1990, 23, 37–40. [Google Scholar] [CrossRef]
- Phan, A.; Dalle, S.; Touzet, S.; Ronger-Savlé, S.; Balme, B.; Thomas, L. Dermoscopic features of acral lentiginous melanoma in a large series of 110 cases in a white population. Br. J. Dermatol. 2010, 162, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Mun, J.-H.; Jo, G.; Darmawan, C.C.; Park, J.; Bae, J.M.; Jin, H.; Kim, W.-I.; Kim, H.-S.; Ko, H.-C.; Kim, B.-S.; et al. Association between Breslow thickness and dermoscopic findings in acral melanoma. J. Am. Acad. Dermatol. 2018, 79, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Darmawan, C.C.; Jo, G.; Montenegro, S.E.; Kwak, Y.; Cheol, L.; Cho, K.H.; Mun, J.-H. Early detection of acral melanoma: A review of clinical, dermoscopic, histopathologic, and molecular characteristics. J. Am. Acad. Dermatol. 2019, 81, 805–812. [Google Scholar] [CrossRef]
- Moon, K.R.; Choi, Y.D.; Kim, J.M.; Jin, S.; Shin, M.-H.; Shim, H.-J.; Lee, J.-B.; Yun, S.J. Genetic Alterations in Primary Acral Melanoma and Acral Melanocytic Nevus in Korea: Common Mutated Genes Show Distinct Cytomorphological Features. J. Investig. Dermatol. 2018, 138, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Smalley, K.S.M.; Teer, J.K.; Chen, Y.A.; Wu, J.-Y.; Yao, J.; Koomen, J.M.; Chen, W.-S.; Rodriguez-Waitkus, P.; Karreth, F.A.; Messina, J.L. A Mutational Survey of Acral Nevi. JAMA Dermatol. 2021, 157, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Choi, Y.D.; Seon, H.J.; Lee, J.-B.; Yun, S.J. Anatomic mapping and clinicopathologic analysis of benign acral melanocytic neoplasms: A comparison between adults and children. J. Am. Acad. Dermatol. 2017, 77, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, A.; Omodaka, T.; Okuyama, R. Melanomas and Mechanical Stress Points on the Plantar Surface of the Foot. N. Engl. J. Med. 2016, 374, 2404–2406. [Google Scholar] [CrossRef]
- Costello, C.M.; Pittelkow, M.R.; Mangold, A.R. Acral Melanoma and Mechanical Stress on the Plantar Surface of the Foot. N. Engl. J. Med. 2017, 377, 395–396. [Google Scholar] [CrossRef]
- Thomas, L.; Phan, A.; Pralong, P.; Poulalhon, N.; Debarbieux, S.; Dalle, S. Special locations dermoscopy: Facial, acral, and nail. Dermatol. Clin. 2013, 31, 615–624. [Google Scholar] [CrossRef]
- Yun, S.J.; Bastian, B.C. Melanocytic tumours in acral skin. In WHO Classification of Skin Tumours; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; World Health Organization Classification of Tumours; International Agency for Research on Cancer: Lyon, France, 2018; Chapter 2; ISBN 978-92-832-2440-2. [Google Scholar]
- Saida, T.; Miyazaki, A.; Oguchi, S.; Ishihara, Y.; Yamazaki, Y.; Murase, S.; Yoshikawa, S.; Tsuchida, T.; Kawabata, Y.; Tamaki, K. Significance of Dermoscopic Patterns in Detecting Malignant Melanoma on Acral Volar Skin: Results of a Multicenter Study in Japan. Arch. Dermatol. 2004, 140, 1233–1238. [Google Scholar] [CrossRef]
- Costello, C.M.; Ghanavatian, S.; Temkit, M.; Buras, M.R.; DiCaudo, D.J.; Swanson, D.L.; Mangold, A.R. Educational and practice gaps in the management of volar melanocytic lesions. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Criscito, M.C.; Stein, J.A. Improving the diagnosis and treatment of acral melanocytic lesions. Melanoma Manag. 2017, 4, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Saida, T.; Koga, H.; Uhara, H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J. Dermatol. 2011, 38, 25–34. [Google Scholar] [CrossRef]
- Ingrassia, J.P.; Stein, J.A.; Levine, A.; Liebman, T.N. Diagnosis and Management of Acral Pigmented Lesions. Dermatol. Surg. 2023, 49, 926–931. [Google Scholar] [CrossRef]
- Huang, K.; Fan, J.; Misra, S. Acral lentiginous melanoma: Incidence and survival in the United States, 2006-2015, an analysis of the SEER registry. J. Surg. Res. 2020, 251, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Bhor, U.; Pande, S. Scoring systems in dermatology. Indian J. Dermatol. Venereol. Leprol. 2006, 72, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; Cevenini, G.; Moscarella, E.; Cinotti, E.; Farnetani, F.; Mahlvey, J.; Perrot, J.L.; Longo, C.; Pellacani, G.; Argenziano, G.; et al. An integrated clinical-dermoscopic risk scoring system for the differentiation between early melanoma and atypical nevi: The iDScore. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2162–2170. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Bertello, M.; Giordani, M.; Cinotti, E.; Cevenini, G.; Rubegni, P. An updated algorithm integrated with patient data for the differentiation of atypical nevi from early melanomas: The idScore 2021. Dermatol. Pract. Concept. 2022, 12, e2022134. [Google Scholar] [CrossRef]
- Rubegni, P.; Tognetti, L.; Argenziano, G.; Nami, N.; Brancaccio, G.; Cinotti, E.; Miracco, C.; Fimiani, M.; Cevenini, G. A risk scoring system for the differentiation between melanoma with regression and regressing nevi. J. Dermatol. Sci. 2016, 83, 138–144. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Żychowska, M.; Savarese, I.; Cinotti, E.; Pizzichetta, M.A.; Moscarella, E.; Longo, C.; Farnetani, F.; Guida, S.; et al. A risk-scoring model for the differential diagnosis of lentigo maligna and other atypical pigmented facial lesions of the face: The facial iDScore. Acad. Dermatol. Venereol. 2023, 37, 2301–2310. [Google Scholar] [CrossRef]
- Tognetti, L.; Cevenini, G.; Moscarella, E.; Cinotti, E.; Farnetani, F.; Lallas, A.; Tiodorovic, D.; Carrera, C.; Puig, S.; Perrot, J.L.; et al. Validation of an integrated dermoscopic scoring method in an European teledermoscopy web platform: The iDScore project for early detection of melanoma. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; Cinotti, E.; Farnetani, F.; Lallas, A.; Paoli, J.; Longo, C.; Pampena, R.; Moscarella, E.; Argenziano, G.; Tiodorovic, D.; et al. Development and Implementation of a Web-Based International Registry Dedicated to Atypical Pigmented Skin Lesions of the Face: Teledermatologic Investigation on Epidemiology and Risk Factors. Telemed. J. E Health 2023, 29, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- EUR-Lex-32016R0679-EN-EUR-Lex Regulation—2016/679—EN—Gdpr—EUR-Lex. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 16 January 2024).
- Vallone, M.G.; Tell-Marti, G.; Potrony, M.; Rebollo-Morell, A.; Badenas, C.; Puig-Butille, J.A.; Gimenez-Xavier, P.; Carrera, C.; Malvehy, J.; Puig, S. Melanocortin 1 receptor (MC1R) polymorphisms’ influence on size and dermoscopic features of nevi. Pigment Cell Melanoma Res. 2018, 31, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Zocchi, L.; Lontano, A.; Merli, M.; Dika, E.; Nagore, E.; Quaglino, P.; Puig, S.; Ribero, S. Familial Melanoma and Susceptibility Genes: A Review of the Most Common Clinical and Dermoscopic Phenotypic Aspect, Associated Malignancies and Practical Tips for Management. J. Clin. Med. 2021, 10, 3760. [Google Scholar] [CrossRef] [PubMed]
- Quint, K.D.; van der Rhee, J.I.; Gruis, N.A.; Ter Huurne, J.A.; Wolterbeek, R.; van der Stoep, N.; Bergman, W.; Kukutsch, N.A. Melanocortin 1 receptor (MC1R) variants in high melanoma risk patients are associated with specific dermoscopic ABCD features. Acta Derm.-Venereol. 2012, 92, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Ghanavatian, S.; Costello, C.M.; Buras, M.R.; Cumsky, H.J.L.; Pittelkow, M.R.; Swanson, D.L.; Mangold, A.R. Density and distribution of acral melanocytic nevi and acral melanomas on the plantar surface of the foot. J. Am. Acad. Dermatol. 2019, 80, 790–792.e2. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, M.; Yamamoto, Y.; Hara, T.; Okuhira, H.; Inaba, Y.; Kunimoto, K.; Mikita, N.; Kaminaka, C.; Kanazawa, N.; Jinnin, M. Difference in distribution of malignant melanoma and melanocytic nevus in the palm and finger. Biosci. Trends 2019, 13, 361–363. [Google Scholar] [CrossRef]
- Kawabata, Y.; Tamaki, K. Distinctive dermatoscopic features of acral lentiginous melanoma in situ from plantar melanocytic nevi and their histopathologic correlation. J. Cutan. Med. Surg. 1998, 2, 199–204. [Google Scholar] [CrossRef]
- Tan, A.; Stein, J.A. Dermoscopic patterns of acral melanocytic lesions in skin of color. Cutis 2019, 103, 274–276. [Google Scholar]
- González-Ramírez, R.A.; Guerra-Segovia, C.; Garza-Rodríguez, V.; Garza-Báez, P.; Gómez-Flores, M.; Ocampo-Candiani, J. Dermoscopic features of acral melanocytic nevi ina case series from Mexico. Ann. Bras. Dermatol. 2018, 93, 665–670. [Google Scholar] [CrossRef]
- Durbec, F.; Martin, L.; Derancourt, C.; Grange, F. Melanoma of the hand and foot: Epidemiological, prognostic and genetic features. A systematic review. Br. J. Dermatol. 2012, 166, 727–739. [Google Scholar] [CrossRef] [PubMed]
- Metzger, S.; Ellwanger, U.; Stroebel, W.; Schiebel, U.; Rassner, G.; Fierlbeck, G. Extent and consequences of physician delay in the diagnosis of acral melanoma. Melanoma Res. 1998, 8, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kolm, I.; Kamarashev, J.; Kerl, K.; Hafner, J.; Läuchli, S.; French, L.E.; Braun, R.P. Acral melanoma with network pattern: A dermoscopy-reflectance confocal microscopy and histopathology correlation. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2010, 36, 701–703. [Google Scholar] [CrossRef] [PubMed]
- Nagore, E.; Pereda, C.; Botella-Estrada, R.; Requena, C.; Guillén, C. Acral lentiginous melanoma presents distinct clinical profile with high cancer susceptibility. Cancer Causes Control 2009, 20, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Hur, K.; Ohn, J.; Lim, S.S.; Mun, J.-H. Acral lentiginous melanoma in situ: Dermoscopic features and management strategy. Sci. Rep. 2020, 10, 20503. [Google Scholar] [CrossRef] [PubMed]
- Weitao, Y.; Jiaqiang, W.; Peng, Z.; Xin, W.; Xinhui, D.; Xiaohui, N. A Retrospective Study of Acral Melanoma That Happened on Foot. 2020. Available online: https://www.researchsquare.com/article/rs-16460/v1 (accessed on 18 January 2024).
- Jaroonwanichkul, S.; Fan, E.; Matthews, S.; Ho, B.V.; Hall, J.C. Acral Nodular Melanoma at a Site of Trauma. Kans. J. Med. 2023, 16, 187–188. [Google Scholar] [CrossRef] [PubMed]
- Mikoshiba, Y.; Minagawa, A.; Koga, H.; Yokokawa, Y.; Uhara, H.; Okuyama, R. Clinical and Histopathologic Characteristics of Melanocytic Lesions on the Volar Skin Without Typical Dermoscopic Patterns. JAMA Dermatol. 2019, 155, 578–584. [Google Scholar] [CrossRef]
- Hao, X.; Yim, J.; Chang, S.; Schwartz, E.; Rubenstein, S.; Friske, C.; Shamim, S.; Masternick, E.; Mirkin, G. Acral Lentiginous Melanoma of Foot and Ankle: A Clinicopathological Study of 7 Cases. Anticancer Res. 2019, 39, 6175–6181. [Google Scholar] [CrossRef]
- Saida, T. Malignant Melanoma on the Sole: How to Detect the Early Lesions Efficiently. Pigment. Cell Res. 2000, 13, 135–139. [Google Scholar] [CrossRef]
- Tognetti, L.; Cartocci, A.; Balistreri, A.; Cataldo, G.; Cinotti, E.; Moscarella, E.; Farnetani, F.; Lallas, A.; Tiodorovic, D.; Carrera, C.; et al. The Comparative Use of Multiple Electronic Devices in the Teledermoscopic Diagnosis of Early Melanoma. Telemed. J. e-Health 2021, 27, 495–502. [Google Scholar] [CrossRef]
- Ozdemir, F.; Karaarslan, I.K.; Akalin, T. Variations in the dermoscopic features of acquired acral melanocytic nevi. Arch. Dermatol. 2007, 143, 1378–1384. [Google Scholar] [CrossRef]
- Barcaui, C.B.; Lima, P.M.O. Application of teledermoscopy in the diagnosis of pigmented lesions. Int. J. Telemed. Appl. 2018, 2018, 1624073. [Google Scholar] [CrossRef] [PubMed]
- Emiroglu, N.; Cengiz, F.P.; Onsun, N. Age and Anatomical Location-Related Dermoscopic Patterns of 210 Acral Melanocytic Nevi in a Turkish Population. J. Cutan. Med. Surg. 2017, 21, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Yang, S.; Kim, W.; Jung, J.; Chung, K.Y.; Lee, S.W.; Oh, B. Acral melanoma detection using a convolutional neural network for dermoscopy images. PLoS ONE 2018, 13, e0193321. [Google Scholar] [CrossRef]
- Tognetti, L.; Bonechi, S.; Andreini, P.; Bianchini, M.; Scarselli, F.; Cevenini, G.; Moscarella, E.; Farnetani, F.; Longo, C.; Lallas, A.; et al. A new deep learning approach integrated with clinical data for the dermoscopic differentiation of early melanomas from atypical nevi. J. Dermatol. Sci. 2021, 101, 115–122. [Google Scholar] [CrossRef]
- Rubegni, P.; Cevenini, G.; Nami, N.; Argenziano, G.; Saida, T.; Burroni, M.; Quaglino, P.; Bono, R.; Hofmann-Wellenhof, R.; Fimiani, M. A simple scoring system for the diagnosis of palmo-plantar pigmented skin lesions by digital dermoscopy analysis. J. Eur. Acad. Dermatol. Venereol. JEADV 2013, 27, e312–e319. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lesion Data | n (%)/Mean ± SD | ||
|---|---|---|---|
| Histological Diagnosis | 542 | ||
| Nevus | 429 (79.2%) | ||
| Malignant melanoma | 113 (20.8%) | ||
| Maximum diameter | 8.83 ± 7.85 | ||
| Four macro-areas of the sole | 490 (90.6%) | ||
| 111 (22.7%) | ||
| 87 (17.8%) | ||
| 229 (46.7%) | ||
| 63 (12.9%) | ||
| Three macro-areas of the palm | 51 (9.4%) | ||
| 12 (23.5%) | ||
| 17 (33.3%) | ||
| 22 (43.1%) | ||
| Patient Data | |||
| Age | 46.33 ± 19.07 | ||
| Male | 195 (36.0%) | ||
| Female | 347 (64.0%) | ||
| ANAMNESTIC DATA/RISK FACTORS | YES | NO | NA |
| Personal/family history of melanoma—1st-degree-relative | 11 (2.0%) | 79 (14.5%) | 452 (83.4%) |
| History of sunburns (>3) in childhood below the age of 14 years | 41 (7.5%) | 75 (13.8%) | 426 (78.5%) |
| Chronic traumatism of palms | 0 (0.0%) | 7 (12.9%) | 44 (86.3%) |
| Chronic traumatism of soles | 10 (1.8%) | 138 (25.4%) | 342 (63.0%) |
| PHENOTYPIC TRAITS | |||
| Presence of >100 common nevi or >10 dysplastic nevi on the body | 24 (4.4%) | 67 (12.3%) | 451 (83.2%) |
| Phototype | 355 (65.5%) | 187 (34.5%) | |
| 94 (17.3%) | ||
| 248 (45.7%) | ||
| 11 (2.0%) | ||
| 2 (0.3%) | ||
| Pheomelanin phenotype | 35 (6.4%) | 65 (11.9%) | 442 (81%) |
| Presence of green/light blue/blue eyes | 51 (9.4%) | 76 (14%) | 415 (76%) |
| Presence of blond hair | 93 (17.1%) | 69 (12.7%) | 380 (70.1%) |
| n (%)/Mean ± SD | |||
|---|---|---|---|
| Lesion Data | MMs (113) | Nevi (429) | p |
| Maximum diameter | 17.39 ± 12.47 | 6.58 ± 3.58 | <0.001 |
| Body site | 0.285 | ||
| Four macro-areas of the sole * | 98 (87.5%) | 392 (91.4%) | |
| 21 (21.4%) | 90 (23.0%) | |
| 21 (21.4%) | 66 (16.8%) | |
| 29 (29.6%) | 200 (51.0%) | |
| 27 (27.6%) | 36 (9.2%) | |
| Three macro-areas of the palm # | 14 (12.5%) | 37 (8.6%) | |
| 3 (21.4%) | 9 (24.3%) | |
| 7 (50.0%) | 10 (27.0%) | |
| 4 (28.6%) | 18 (41.6%) | |
| Patient Data | |||
| Age | 65.30 ± 14.79 | 41.33 ± 16.81 | <0.001 |
| Male | 55 (48.6%) | 140 (32.6%) | |
| Female | 58 (51.3%) | 289 (67.4%) | 0.002 |
| Anamnestic Data/Risk Factors | |||
| Personal/family history of melanoma—1st-degree relative | 0.520 | ||
| No | 9 (7.9%) | 70 (16.3%) | |
| Yes | 0 (0.0%) | 11 (2.5%) | |
| History of sunburns (>3) in childhood below the age of 14 years | |||
| No | 25 (22.1%) | 50 (11.6%) | |
| Yes | 7 (0.6%) | 34 (7.9%) | |
| Chronic traumatism on soles | |||
| No | 15 (13.2%) | 129 (30.0%) | |
| Yes | 0 (0%) | 10 (23.3%) | |
| Chronic traumatism on palms | |||
| No | 10 (8.8%) | 94 (21.9%) | |
| Yes | 0 (%) | 1 (0.2%) | |
| PHENOTYPIC TRAITS | |||
| Presence of >100 common nevi or >10 dysplastic nevi | 1.000 | ||
| No | 7 (6.1%) | 60 (13.9%) | |
| Yes | 3 (2.6%) | 21 (4,8%) | |
| Phototype (%) | 100% | 100% | 0.717 |
| II | 19 (29.7%) | 75 (25.8%) | |
| III | 44 (68.8%) | 204 (70.1%) | |
| IV | 1 (1.6%) | 10 (3.4%) | |
| V | 0 (0.0%) | 2 (0.7%) | |
| Pheomelanin phenotype | |||
| No | 17 (15.0%) | 48 (11.1%) | 0.610 |
| Yes | 9 (7.9%) | 26 (6.0%) | |
| Presence of green/light blue/blue eyes | |||
| No | 23 (20.3%) | 53 (12.3%) | 0.320 |
| Yes | 18 (15.9%) | 33 (7.6%) | |
| Presence of blond hair | |||
| No | 14 (12.3%) | 55 (12.8%) | 0.430 |
| Yes | 26 (23%) | 67 (15.6%) | |
| Lesion Data | aMPPLs n = 542 | MMs n = 113 | Nevi n = 429 |
|---|---|---|---|
| Eight Subareas of the sole | 490 | 98 (87.5) | 392 (91.4) |
| Anterior lateral eminence of the sole | 21 (3.18%) | 3 (3.1%) | 18 (4.6%) |
| Anterior medial eminence of the sole | 45 (7.85%) | 15 (15.3%) | 30 (7.7%) |
| Central eminence of the sole | 21 (4.46%) | 3 (3.1%) | 18 (4.6%) |
| Heel | 63 (1.21%) | 27 (27.6%) | 36 (9.2%) |
| Interdigital spaces (foot) | 34 (5.73%) | 4 (4.1%) | 30 (7.7%) |
| Lateral surface of the fingers (foot) | 36 (7.21%) | 8 (8.2%) | 28 (7.1%) |
| Plantar arch | 229 (43.9%) | 29 (29.6%) | 200 (51.0%) |
| Plantar surface of the fingers | 41 (7.85%) | 9 (9.2%) | 32 (8.2%) |
| Nine Subareas of the palms | 36 | 14 (12.5%) | 37 (8.6%) |
| Central metacarpal | 2 (5.6%) | 0 (0.0%) | 2 (5.4%) |
| Fingertips (hand) | 2 (5.6%) | 2 (14.3%) | 0 (0.0%) |
| Interdigital spaces | 3 (8.3%) | 0 (0.0%) | 3 (8.1%) |
| Ipothenar surface | 11 (30.6%) | 1 (7.1%) | 10 (27.0%) |
| Lateral surface of the fingers (hand) | 5 (13.9%) | 3 (21.4%) | 2 (5.4%) |
| Metacarpal surface | 11 (30.6%) | 3 (21.4%) | 8 (21.6%) |
| Thenar surface | 10 (27.8%) | 3 (21.4%) | 7 (18.9%) |
| Volar surface of the fingers | 7 (19.4%) | 2 (14.3%) | 5 (13.5%) |
| Proximal phalangeal surface | 0 | 0 | 0 |
| Device Type Used for Image Acquisition/ | aMPPLs | Melanomas | Nevi |
|---|---|---|---|
| n (%) | 542 (100%) | 113 (100%) | 429 (100%) |
| Camera-based system | 254 (46.8%) | 31 (27.4%) | 223 (51.9%) |
| Videodermatoscope | 160 (29.5%) | 51 (45.1%) | 109 (25.4%) |
| Smartphone-based system | 97 (17.8%) | 20 (17.6%) | 77 (17.9%) |
| Unknown/unspecified | 31 (5.7%) | 11 (9.7%) | 20 (4.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tognetti, L.; Cartocci, A.; Lallas, A.; Moscarella, E.; Stanganelli, I.; Nazzaro, G.; Paoli, J.; Fargnoli, M.C.; Broganelli, P.; Kittler, H.; et al. A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database. Diagnostics 2024, 14, 460. https://doi.org/10.3390/diagnostics14050460
Tognetti L, Cartocci A, Lallas A, Moscarella E, Stanganelli I, Nazzaro G, Paoli J, Fargnoli MC, Broganelli P, Kittler H, et al. A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database. Diagnostics. 2024; 14(5):460. https://doi.org/10.3390/diagnostics14050460
Chicago/Turabian StyleTognetti, Linda, Alessandra Cartocci, Aimilios Lallas, Elvira Moscarella, Ignazio Stanganelli, Gianluca Nazzaro, John Paoli, Maria Concetta Fargnoli, Paolo Broganelli, Harald Kittler, and et al. 2024. "A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database" Diagnostics 14, no. 5: 460. https://doi.org/10.3390/diagnostics14050460
APA StyleTognetti, L., Cartocci, A., Lallas, A., Moscarella, E., Stanganelli, I., Nazzaro, G., Paoli, J., Fargnoli, M. C., Broganelli, P., Kittler, H., Perrot, J. -L., Cataldo, G., Cevenini, G., Lo Conte, S., Simone, L., Cinotti, E., & Rubegni, P. (2024). A European Multicentric Investigation of Atypical Melanocytic Skin Lesions of Palms and Soles: The iDScore-PalmoPlantar Database. Diagnostics, 14(5), 460. https://doi.org/10.3390/diagnostics14050460