
Photon-Counting Detector CT Virtual Monoenergetic Images in Cervical Trauma Imaging—Optimization of Dental Metal Artifacts and Image Quality

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Imaging Protocol
2.3. Objective Image Analysis
2.4. Subjective Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Population Data
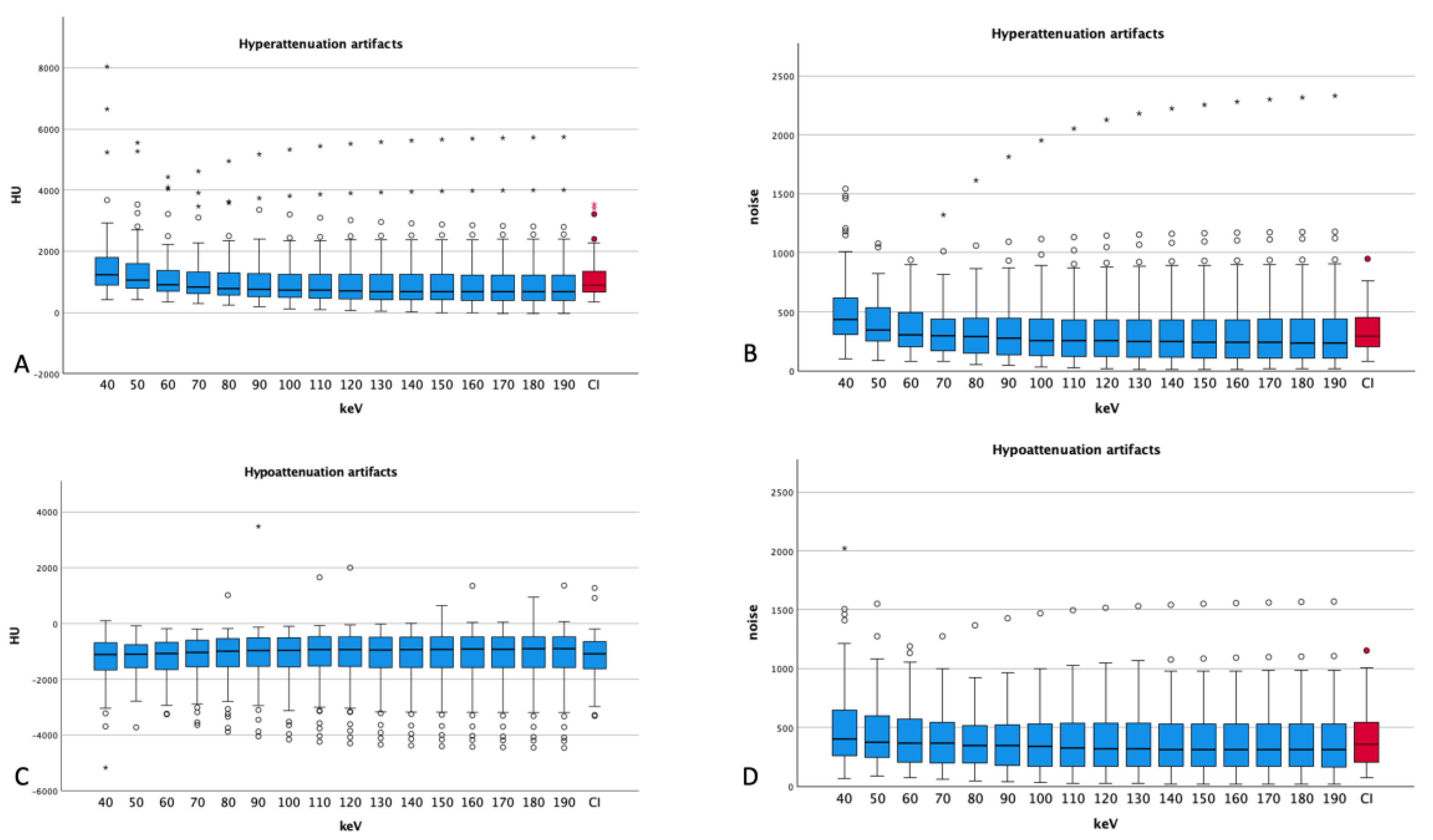
3.2. Hyperattenuation Artifacts
3.3. Hypoattenuation Artifacts
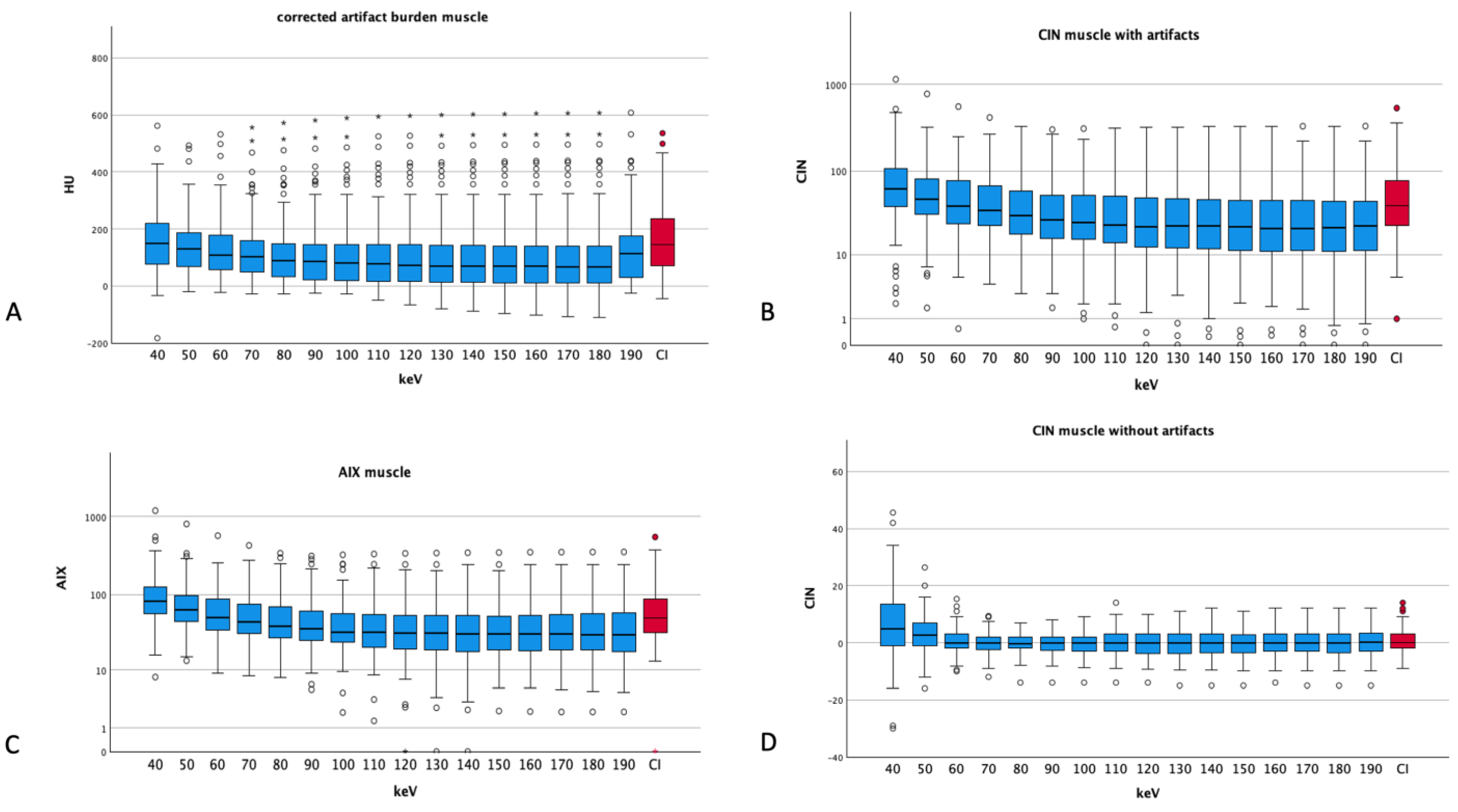
3.4. Artifacts and Noise in Muscle
3.5. Artifacts and Noise in Vessels
3.6. Comparison of Muscle and Vessels
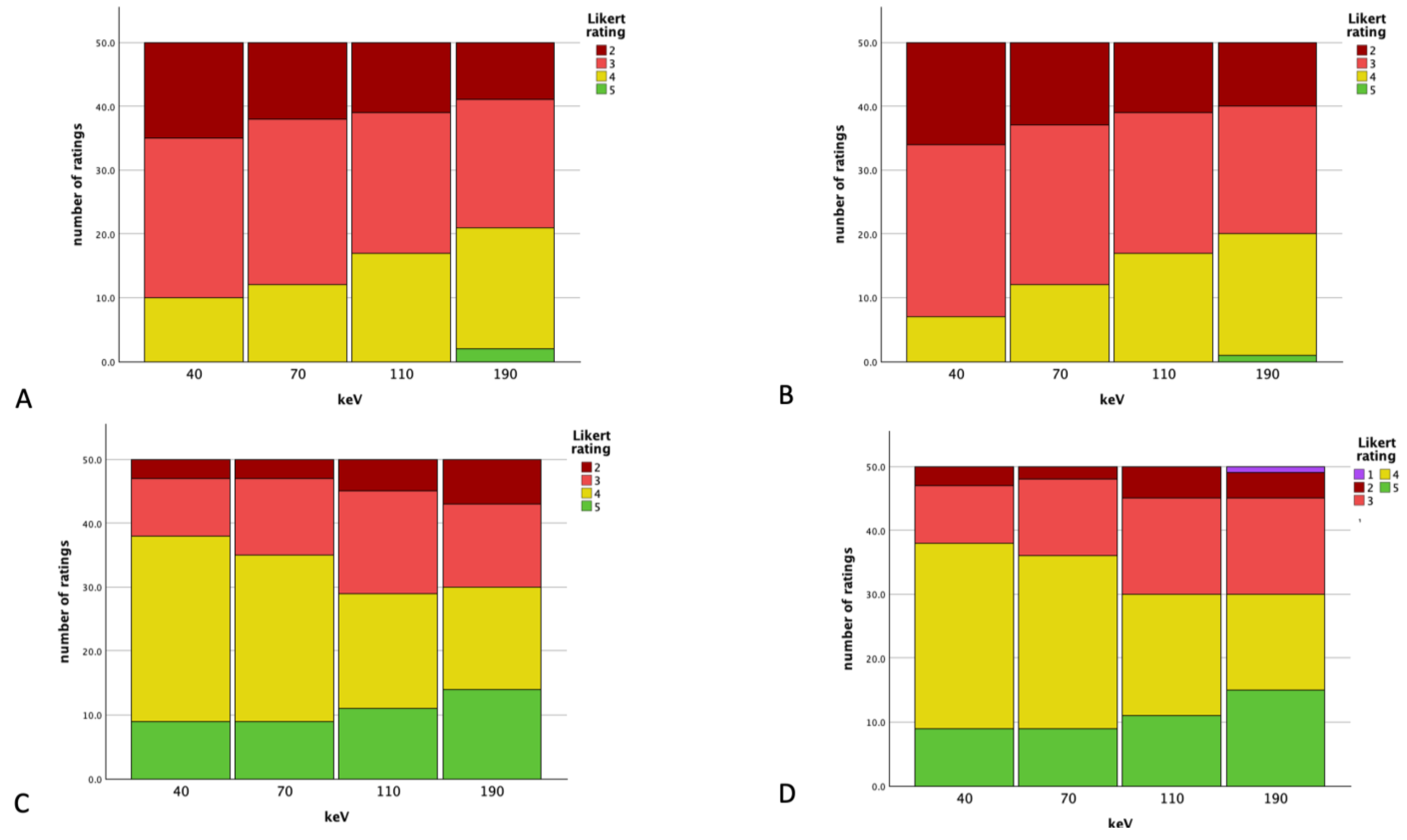
3.7. Subjective Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huber-Wagner, S.; Lefering, R.; Qvick, L.M.; Korner, M.; Kay, M.V.; Pfeifer, K.J.; Reiser, M.; Mutschler, W.; Kanz, K.-G. Effect of whole-body CT during trauma resuscitation on survival: A retrospective, multicentre study. Lancet 2009, 373, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.A.; Di Chiro, G. Beam hardening in x-ray reconstructive tomography. Phys. Med. Biol. 1976, 21, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Joseph, P.M.; Spital, R.D. The effects of scatter in x-ray computed tomography. Med. Phys. 1982, 9, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Komlosi, P.; Grady, D.; Smith, J.S.; Shaffrey, C.I.; Goode, A.R.; Judy, P.G.; Shaffrey, M.; Wintermark, M. Evaluation of monoenergetic imaging to reduce metallic instrumentation artifacts in computed tomography of the cervical spine. J. Neurosurg. Spine 2015, 22, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Mori, I.; Machida, Y.; Osanai, M.; Iinuma, K. Photon starvation artifacts of X-ray CT: Their true cause and a solution. Radiol. Phys. Technol. 2013, 6, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, V.; Grosse Hokamp, N.; Abdullayev, N.; Rau, R.; Mpotsaris, A.; Maintz, D.; Borggrefe, J. Metal artifact reduction by dual-layer computed tomography using virtual monoenergetic images. Eur. J. Radiol. 2017, 93, 143–148. [Google Scholar] [CrossRef]
- Zatz, L.M.; Alvarez, R.E. An inaccuracy in computed tomography: The energy dependence of CT values. Radiology 1977, 124, 91–97. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, S.; Lee, S.A.; Song, H.T.; Huh, Y.M.; Kim, D.H.; Han, S.H.; Suh, J.-S. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics 2007, 27, 791–803. [Google Scholar] [CrossRef]
- Bamberg, F.; Dierks, A.; Nikolaou, K.; Reiser, M.F.; Becker, C.R.; Johnson, T.R. Metal artifact reduction by dual energy computed tomography using monoenergetic extrapolation. Eur. Radiol. 2011, 21, 1424–1429. [Google Scholar] [CrossRef] [PubMed]
- Barreto, I.; Pepin, E.; Davis, I.; Dean, C.; Massini, T.; Rees, J.; Olguin, C.; Quails, N.; Correa, N.; Rill, L.; et al. Comparison of metal artifact reduction using single-energy CT and dual-energy CT with various metallic implants in cadavers. Eur. J. Radiol. 2020, 133, 109357. [Google Scholar] [CrossRef] [PubMed]
- Huflage, H.; Grunz, J.P.; Hackenbroch, C.; Halt, D.; Luetkens, K.S.; Alfred Schmidt, A.M.; Patzer, T.; Ergün, S.; Bley, T.; Kunz, A. Metal artefact reduction in low-dose computed tomography: Benefits of tin prefiltration versus postprocessing of dual-energy datasets over conventional CT imaging. Radiography 2022, 28, 690–696. [Google Scholar] [CrossRef]
- Kunz, A.S.; Patzer, T.S.; Grunz, J.P.; Luetkens, K.S.; Hartung, V.; Hendel, R.; Fieber, T.; Genest, F.; Ergün, S.; Bley, T.A.; et al. Metal artifact reduction in ultra-high-resolution cone-beam CT imaging with a twin robotic X-ray system. Sci. Rep. 2022, 12, 15549. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Higashigaito, K.; Euler, A.; Eberhard, M.; Flohr, T.G.; Schmidt, B.; Alkadhi, H. Contrast-Enhanced Abdominal CT with Clinical Photon-Counting Detector CT: Assessment of Image Quality and Comparison with Energy-Integrating Detector CT. Acad. Radiol. 2022, 29, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Kaatsch, H.L.; Fulisch, F.; Dillinger, D.; Kubitscheck, L.; Becker, B.V.; Piechotka, J.; Brockmann, M.A.; Froelich, M.F.; Schoenberg, S.O.; Overhoff, D.; et al. Ultra-low-dose photon-counting CT of paranasal sinus: An in vivo comparison of radiation dose and image quality to cone-beam CT. Dentomaxillofacial Radiol. 2023, 53, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Graafen, D.; Muller, L.; Halfmann, M.; Duber, C.; Hahn, F.; Yang, Y.; Emrich, T.; Kloeckner, R. Photon-counting detector CT improves quality of arterial phase abdominal scans: A head-to-head comparison with energy-integrating CT. Eur. J. Radiol. 2022, 156, 110514. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.; Kavanagh, R.G.; Carey, B.W.; Moore, N.; Maher, M.; O’Connor, O.J. Using body mass index to estimate individualised patient radiation dose in abdominal computed tomography. Eur. Radiol. Exp. 2018, 2, 38. [Google Scholar] [CrossRef]
- Grosse Hokamp, N.; Neuhaus, V.; Abdullayev, N.; Laukamp, K.; Lennartz, S.; Mpotsaris, A.; Borggrefe, J. Reduction of artifacts caused by orthopedic hardware in the spine in spectral detector CT examinations using virtual monoenergetic image reconstructions and metal-artifact-reduction algorithms. Skeletal Radiol. 2018, 47, 195–201. [Google Scholar] [CrossRef]
- Dong, Y.; Shi, A.J.; Wu, J.L.; Wang, R.X.; Sun, L.F.; Liu, A.L.; Liu, Y.J. Metal artifact reduction using virtual monochromatic images for patients with pedicle screws implants on CT. Eur. Spine J. 2016, 25, 1754–1763. [Google Scholar] [CrossRef]
- Risch, F.; Decker, J.A.; Popp, D.; Sinzinger, A.; Braun, F.; Bette, S.; Jehs, B.; Haerting, M.; Wollny, C.; Scheurig-Muenkler, C.; et al. Artifact Reduction From Dental Material in Photon-Counting Detector Computed Tomography Data Sets Based on High-keV Monoenergetic Imaging and Iterative Metal Artifact Reduction Reconstructions-Can We Combine the Best of Two Worlds? Investig. Radiol. 2023, 58, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Chen, Y.; Yang, J.; Tao, X.; Xi, Y. Evaluation of the dental spectral cone beam CT for metal artefact reduction. Dentomaxillofacial Radiol. 2019, 48, 20180044. [Google Scholar] [CrossRef] [PubMed]
- Laukamp, K.R.; Zopfs, D.; Lennartz, S.; Pennig, L.; Maintz, D.; Borggrefe, J.; Hokamp, N.G. Metal artifacts in patients with large dental implants and bridges: Combination of metal artifact reduction algorithms and virtual monoenergetic images provides an approach to handle even strongest artifacts. Eur. Radiol. 2019, 29, 4228–4238. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Dillinger, D.; Overhoff, D.; Booz, C.; Kaatsch, H.L.; Piechotka, J.; Hagen, A.; Froelich, M.F.; Vogl, T.J.; Waldeck, S. Impact of CT Photon-Counting Virtual Monoenergetic Imaging on Visualization of Abdominal Arterial Vessels. Diagnostics 2023, 13, 938. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.L.; Flohr, T.G.; Krauss, B.; Sedlmair, M.; Thomas, C.; Schmidt, B. Assessment of an advanced image-based technique to calculate virtual monoenergetic computed tomographic images from a dual-energy examination to improve contrast-to-noise ratio in examinations using iodinated contrast media. Investig. Radiol. 2014, 49, 586–592. [Google Scholar] [CrossRef]
- Patzer, T.S.; Kunz, A.S.; Huflage, H.; Gruschwitz, P.; Pannenbecker, P.; Afat, S.; Herrmann, J.; Petritsch, B.; Bley, T.A.; Grunz, J.-P. Combining virtual monoenergetic imaging and iterative metal artifact reduction in first-generation photon-counting computed tomography of patients with dental implants. Eur. Radiol. 2023, 33, 7818–7829. [Google Scholar] [CrossRef]
- Layer, Y.C.; Mesropyan, N.; Kupczyk, P.A.; Luetkens, J.A.; Isaak, A.; Dell, T.; Ernst, B.P.; Attenberger, U.I.; Kuetting, D. Use of virtual monoenergetic images for reduction of extensive dental implant associated artifacts in photon-counting detector CT. Sci. Rep. 2024, 14, 497. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rating | Overall Image Quality/Artifact Burden | Vascular Assessability/Vascular Artifact Burden |
|---|---|---|
| 1 | massive artifacts; very poor image quality/no diagnostic use | no diagnostic assessability of neck vessels |
| 2 | pronounced streaks; poor image quality/very limited diagnostic assessability | Severe impairment of the diagnostic assessability |
| 3 | intermediate streaks; intermediate image quality/restricted diagnostic assessability | Moderate impairment, but sufficient diagnostic assessability |
| 4 | minimal streaks; good image quality/sufficient diagnostic assessability | minor impairment |
| 5 | no artifacts; excellent image quality/diagnostic assessability | excellent assessability |
| Overall | Male | Female | |
|---|---|---|---|
| Age (years) | 63 ± 16 | 59 ± 14 | 70 ± 18 |
| DLP (mGy·cm) | 318 ± 40 | 334 ± 28 | 291 ± 43 |
| CTDIvol (mGy) | 7.77 ± 0.74 | 8.00 ± 0.50 | 7.34 ± 0.89 |
| Deff (mm) | 306 ± 53 | 311 ± 42 | 297 ± 69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dillinger, D.; Overhoff, D.; Froelich, M.F.; Kaatsch, H.L.; Booz, C.; Hagen, A.; Vogl, T.J.; Schönberg, S.O.; Waldeck, S. Photon-Counting Detector CT Virtual Monoenergetic Images in Cervical Trauma Imaging—Optimization of Dental Metal Artifacts and Image Quality. Diagnostics 2024, 14, 626. https://doi.org/10.3390/diagnostics14060626
Dillinger D, Overhoff D, Froelich MF, Kaatsch HL, Booz C, Hagen A, Vogl TJ, Schönberg SO, Waldeck S. Photon-Counting Detector CT Virtual Monoenergetic Images in Cervical Trauma Imaging—Optimization of Dental Metal Artifacts and Image Quality. Diagnostics. 2024; 14(6):626. https://doi.org/10.3390/diagnostics14060626
Chicago/Turabian StyleDillinger, Daniel, Daniel Overhoff, Matthias F. Froelich, Hanns L. Kaatsch, Christian Booz, Achim Hagen, Thomas J. Vogl, Stefan O. Schönberg, and Stephan Waldeck. 2024. "Photon-Counting Detector CT Virtual Monoenergetic Images in Cervical Trauma Imaging—Optimization of Dental Metal Artifacts and Image Quality" Diagnostics 14, no. 6: 626. https://doi.org/10.3390/diagnostics14060626
APA StyleDillinger, D., Overhoff, D., Froelich, M. F., Kaatsch, H. L., Booz, C., Hagen, A., Vogl, T. J., Schönberg, S. O., & Waldeck, S. (2024). Photon-Counting Detector CT Virtual Monoenergetic Images in Cervical Trauma Imaging—Optimization of Dental Metal Artifacts and Image Quality. Diagnostics, 14(6), 626. https://doi.org/10.3390/diagnostics14060626