
Skin Lesions with Loss of Tissue and Cutaneous-Onset Sepsis: The Skin Infection–Sepsis Relationship


 , , ,
, , ,  and
and
Abstract
:1. Introduction
Study Aims
2. Materials and Methods
2.1. Study Coordinates; Inclusion and Exclusion Criteria
- group A—infected skin lesions and sepsis;
- group B—infected lesions without sepsis;
- group C—non-infected skin lesions (negative bacteriological examination results).
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. General Demographic Characteristics
3.2. Clinical Manifestations—Cutaneous and Systemic, Including Conscious State
3.3. Main Acute Skin Conditions and the Etiological Agents Responsible for Infections
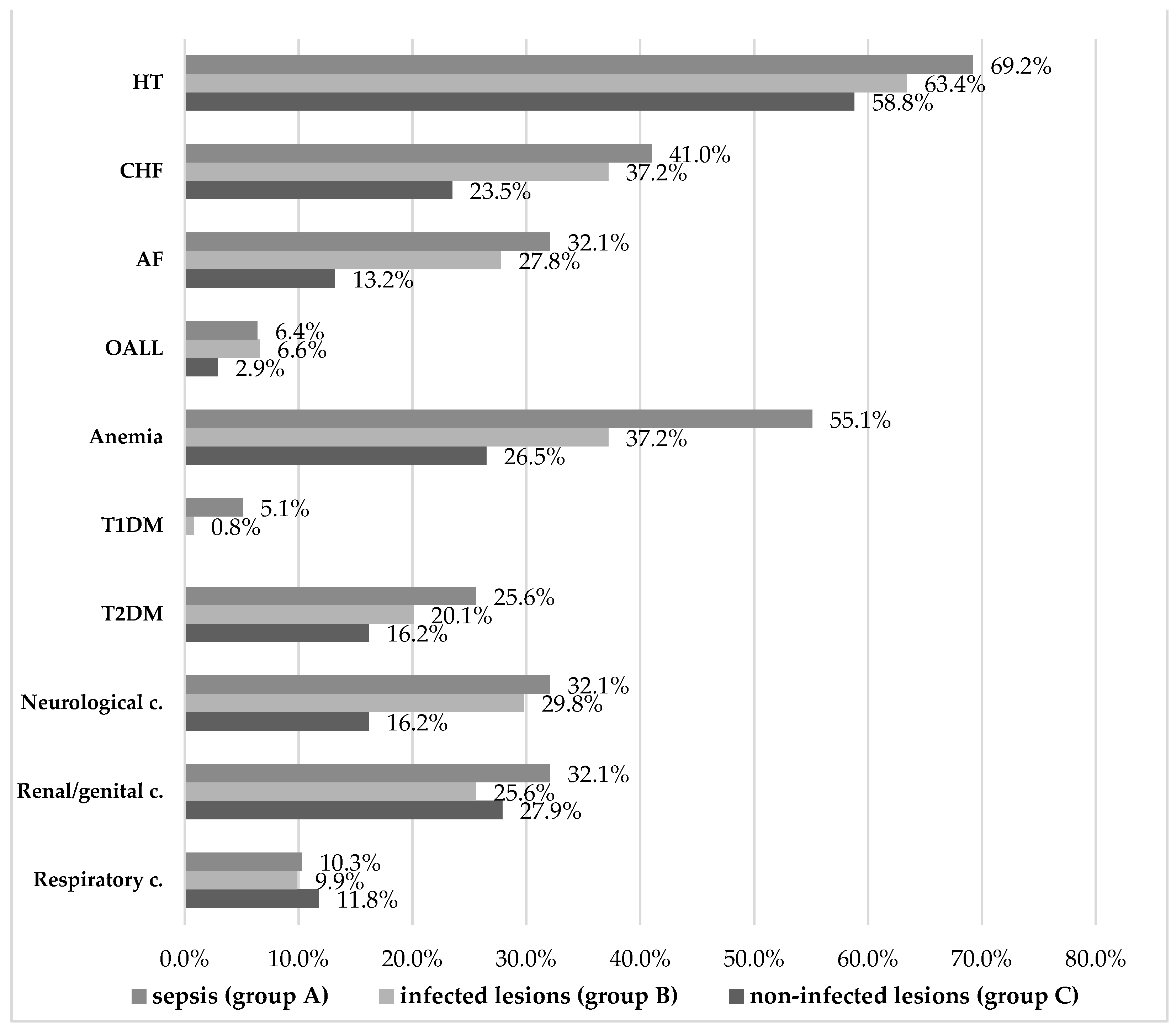
3.4. Comorbidities
3.5. Multivariate Logistic Regression Analyses of Risk Factors for Infection and Sepsis
4. Discussion
4.1. Study Results Overview and General Considerations
4.2. In-Depth Discussion of Studied Lesions
4.3. The Role of Comorbidities in Acute Skin Infections and Related Sepsis
4.4. Further Comments on the Predictive Role of Mildly Altered Mental Status
4.5. Study Limitations and Further Research Opportunities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patrascu, A.I.; Temelie-Olinici, D.; Vata, D.; Halip, I.A.; Hancu, M.F.; Asavei, T.A.; Padure-Costin, A.; Urzica, T.A.; Puha, M.; Gheuca-Solovastru, L. Diagnostic and Treatment Strategies in Cutaneous Sepsis. Dermato. Venerol. 2021, 66, 35–40. Available online: https://www.revistasrd.ro/magazine/Volume-66_53/content (accessed on 4 December 2023).
- Pant, A.; Mackraj, I.; Govender, T. Advances in sepsis diagnosis and management: A paradigm shift towards nanotechnology. J. Biomed. Sci. 2021, 28, 6. [Google Scholar] [CrossRef]
- Jeakrl, D.W.; Lee, S.; Kim, M.; Kim, Y.; Woo, S.H.; Lee, W.J. Procalcitonin as a prognostic marker for sepsis based on SEPSIS-3. J. Clin. Lab. Anal. 2019, 33, e22996. [Google Scholar] [CrossRef]
- Fortini, A.; Faraone, A.; Meini, S.; Bettucchi, M.; Longo, B.; Valoriani, B.; Forni, S. Validity of “SEPSIS-3” criteria in identifying patients with community-onset sepsis in Internal Medicine wards; a prospective, multicenter study. Eur. J. Intern. Med. 2021, 85, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Dimic, N.; Duric, M.; Nenadic, I.; Bobos, M.; Bojic, S.; Vukotic, T.; Simeunovic, G.M.; Gojgic, M.; Stevanovic, P.; Bojovic, K. Development of the Definition of Sepsis. Serbian J. Med. Chamb. 2023, 4, 75–81. Available online: https://www.smj.rs/en/volume-4-no-1/development-of-the-definition-of-sepsis (accessed on 4 December 2023).
- Levy, M.M.; Artigas, A.; Phillips, G.S.; Rhodes, A.; Beale, R.; Osborn, T.; Vincent, J.L.; Townsend, S.; Lemeshow, S.; Dellinger, P. Outcomes of the surviving sepsis campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 2012, 12, 919–924. [Google Scholar] [CrossRef]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelforf, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional and national sepsis incidence and mortality, 1990-2017: Analysis of the global burden of disease study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Pulido-Perez, A.; Bergon-Sendin, M.; Suarez-Fernandez, R.; Munoz-Martin, P.; Bouza, E. Skin and sepsis: Contribution of dermatology to a rapid diagnosis. Infection 2021, 49, 617–629. [Google Scholar] [CrossRef]
- Golan, Y. Current treatment options for acute skin and skin-structure infections. Clin. Infect. Dis. 2019, 68, 206–212. [Google Scholar] [CrossRef]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with coronavirus disease COVID-19. Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevranscky, J.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit. Care Med. 2018, 46, 925–928. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.L.; Chambers, H.F.; Maselli, J.H.; Gonzales, R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch. Intern. Med. 2008, 168, 1585–1591. [Google Scholar] [CrossRef]
- Edelsberg, J.; Taneja, C.; Zervos, M.; Haque, N.; Moore, C.; Reyes, K.; Spalding, J.; Jiang, J.; Oster, G. Trends in US hospital admissions for skin and soft tissue infections. Emerg. Infect. Dis. 2009, 9, 1516–1518. [Google Scholar] [CrossRef]
- Llopis, F.; González-Castillo, J.; Julián-Jiménez, A.; Ferré, C.; Gamazo-Río, J.J.; Martínez, M. Análisis de 1.250 episodios de infección de piel y partes blandas registrados en 49 servicios de Urgencias hospitalarios [Review of 1.250 episodes of skin and soft tissue infections attended at 49 hospital emergency departments]. Rev. Esp. Quimioter. 2014, 27, 115–121. [Google Scholar]
- Moet, G.J.; Jones, R.N.; Biedenbach, D.J.; Stilwell, M.G.; Fritsche, T.R. Contemporary causes of skin and soft tissue infections in North America, Latin America, and Europe: Report from the SENTRY Antimicrobial Surveillance Program (1998–2004). Diagn. Microbiol. Infect. Dis. 2007, 57, 7–13. [Google Scholar] [CrossRef]
- Wardi, G.; Tainter, C.R.; Ramnath, V.R.; Brennan, J.J.; Tolia, V.; Castillo, E.M.; Hsia, R.Y.; Malhotra, A.; Schmidt, U.; Meier, A. Age-related incidence and outcomes of sepsis in California, 2008–2015. J. Crit. Care. 2021, 62, 212–217. [Google Scholar] [CrossRef]
- Bouza, C.; Lopez-Cuadrado, T. Epidemiology and Trends of Sepsis in Young Adults Aged 20-44 Years: A Nationwide Population-Based Study. J. Clin. Med. 2020, 9, 77. [Google Scholar] [CrossRef]
- Matthaeus-Kraemer, C.T.; Norman, R.; Spoden, M.; Pletz, M.W.; Reinhart, K.; Fleischmann-Struzek, C. Urban-Rural Disparities in Case Fatality of Community-acquired sepsis in Germany: A retrospective cohort study. Int. J. Environ. Res. Public Health. 2023, 20, 5867. [Google Scholar] [CrossRef]
- Burian, E.A.; Karlsmark, T.; Franks, P.J.; Keeley, V.; Quere, I.; Moffatt, C.J. Cellulitis in chronic oedema of the lower leg: An international cross-sectional study. Br. J. Dermatol. 2021, 185, 110–118. [Google Scholar] [CrossRef]
- Bonnetblanc, J.; Bedane, C. Erysipelas. Am. J. Clin. Dermatol. 2003, 4, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Ramelet, A.A. Disease of veins. In Braun-Falco’s Dermatology, 3rd ed.; Burgdorf, W.H.C., Plewig, G., Wolff, H.H., Landthaler, M., Eds.; Springer: Heidelberg/Berlin, Germany, 2009; pp. 910–925. [Google Scholar]
- Pătraşcu, A.I.; Gheucă-Solovăstru, L.; Vâţă, D.; Zbranca, A.; Stătescu, L.; Botnariu, G.; Temelie-Olinici, D.; Halip, I.A.; Stîncanu, A.; Dobre, C. Dermatologia pas cu pas. Urgenţe Cutaneo-Mucoase; “Gr. T. Popa” Publishing House: Iaşi, Romania, 2022; pp. 39–58. [Google Scholar]
- Ruocco, V.; Ruocco, E.; Lo Schiavo, A.; Brunetti, G.; Guerrera, L.P.; Wolf, R. Pemphigus: Etiology, pathogenesis, and inducing or triggering factors: Facts and controversies. Clin. Dermatol. 2013, 31, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Kridin, K.; Zelber-Sagi, S.; Bergman, R. Pemphigus vulgaris and pemphigus foliaceus:differences in epidemiology and mortality. Acta Derm. Venereol. 2017, 97, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Baigrie, D.; Nookala, V. Bullous Pemphigoid. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, CA, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK535374 (accessed on 4 December 2023).
- Kirksey, K.H. Erythroderma. In Life-Threatening Rashes. An Illustrated Practical Guide, 1st ed.; Rose, E., Ed.; Springer: Los Angeles, CA, USA, 2018; pp. 265–277. Available online: https://link.springer.com/chapter/10.1007/978-3-319-75623-3_19 (accessed on 4 December 2023).
- Cuellar-Barboza, A.; Ocampo-Candiani, J.; Herz-Ruelas, M.E. A Practical Approach to the Diagnosis and Treatment of Adult Erythroderma. Actas Dermosifiliogr. 2018, 109, 777–790. Available online: https://www.actasdermo.org/es-pdf-S1578219018303536 (accessed on 4 December 2023). [CrossRef] [PubMed]
- Grant-Kels, J.M.; Fedeles, F.; Rothe, M.J. Exfoliative Dermatitis. In Fitzpatrick’s Dermatology in General Medicine, 8th ed.; Goldsmith, L.A., Katz, S.I., Gilchrest, B.A., Paller, A.S., Leffell, D.J., Wolff, K., Eds.; McGraw Hill: New York, NY, USA, 2012; Available online: https://accessmedicine.mhmedical.com/book.aspx?bookid=392#41138703 (accessed on 4 December 2023).
- Heinecke, G.; Lebwohl, M. Erythroderma. In Buka’s Emergencies in Dermatology; Buka, B., Uliasz, A., Krishnamurthy, K., Eds.; Springer: New York, NY, USA, 2013; pp. 133–145. [Google Scholar] [CrossRef]
- Chebl, R.B.; Berbari, I.; Safa, R.; Shami, A.; Sabra, M.; Jamali, S.; Makki, M.; Tamim, H.; Dagher, G.A. Clinical outcome of septic patients with heart failure with preserved ejection fraction presenting to the Emergency Department of a tertiary hospital: A retrospective cohort study. Front. Med. 2020, 7, 517999. [Google Scholar] [CrossRef] [PubMed]
- Afzal, B.; Ali, S.A.; Jamil, B. Outcome of Atrial Fibrillation in Patients WithSepsis. Cureus 2021, 13, e19159. [Google Scholar] [CrossRef]
- Velez-Gimon, M. Atrial Fibrillation during septic Shock. In Infections and Sepsis Development; Neri, V., Huang, L., Li, J., Eds.; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Piotr, F.; Czempik, P.F.; Wiorek, A. Iron deficiency in sepsis patients based on reticulocyte hemoglobin and hepcidin concentration: A prospective cohort study. Arch. Med. Sci. 2023, 19, 805–809. [Google Scholar] [CrossRef]
- Ekregbesi, P.; Shanlar-Hari, M.; Bottomley, C.; Viley, E.M.; Mooney, J.P. Relationship between Anaemia, Haemolysis, Inflammation and Haem Oxygenase-1 at Admission with Sepsis: A pilot study. Sci. Rep. 2018, 8, 11198. [Google Scholar] [CrossRef]
- Constantin, E.; Carlin, M.; Porta, M.; Brizzi, M.F. Type 2 diabetes mellitus and sepsis: State of the art, certainties and missing evidence. Acta Diabetol. 2021, 58, 1139–1151. [Google Scholar] [CrossRef]
- Falcone, M.; Meier, J.J.; Marini, M.G.; Caccialanza, R.; Menichetti, F. Diabetes and acute bacterial skin and skin structure infections. Diabetes Res. Clin. Pract. 2021, 174, 108732. [Google Scholar] [CrossRef]
- Jiang, L.; Cheng, M. Impact of diabetes mellitus on outcomes of patients with sepsis: An updated systematic review and meta-analysis. Diabetol. Metab. Syndr. 2022, 14, 39. [Google Scholar] [CrossRef] [PubMed]
- Willis, A. Altered Mental Status and Coma. Available online: https://www.amboss.com/us/knowledge/altered-mental-status-and-coma (accessed on 4 December 2023).
- Piva, S.; Bertoni, M.; Gitti, N.; Rasulo, F.A.; Latronico, N. Neurological complications of sepsis. Curr. Opin. Crit. Care 2023, 29, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Sonneville, R.; de Montmollin, E.; Poujade, J.; Garrouste-Orgeas, M.; Souweine, B.; Darmon, M.; Mariotte, E.; Argaud, L.; Barbier, F.; Goldgran-Toledano, D.; et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. 2017, 43, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Mostel, Z.; Perl, A.; Marck, M.; Mehdi, S.; Lowell, B.; Bathija, S.; Santosh, R.; Pavlov, V.; Chavan, S.; Roth, J. Post-sepsis syndrome-an evolving entity that afflicts survivors of sepsis. Mol. Med. 2019, 26, 6. [Google Scholar] [CrossRef] [PubMed]
- Gofton, T.E.; Young, G.B. Sepsis associated encephalopathy. Nat. Rev. Neurol. 2012, 8, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Young, G.B.; Bolton, C.F.; Austin, T.W.; Archibald, Y.M.; Gonder, J.; Wells, G.A. The encephalopaty associated with septic illness. Clin. Investig. Med. 1990, 13, 297–304. [Google Scholar]
- Ely, E.W.; Shintani, A.; Truman, B.; Speroff, T.; Gordon, S.M.; Harell, F.E., Jr.; Inouye, S.K.; Bernard, G.R.; Dittus, R. Delirium as predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004, 291, 1753–1762. [Google Scholar] [CrossRef]
- Barichello, T.; Sayana, P.; Giridharan, V.V.; Arumanayagam, A.S.; Narendran, B.; Della Giustina, A.; Petronilho, F.; Quevedo, J.; Dal-Pizzol, F. Long-term cognitive outcomes after sepsis: A translational systematic review. Mol. Neurobiol. 2019, 56, 186–251. [Google Scholar] [CrossRef]
- Semmler, A.; Widmann, C.N.; Okulla, T.; Urbach, H.; Kaiser, M.; Widman, G.; Mormann, F.; Weide, J.; Fliessbach, K.; Hoeft, A.; et al. Persistent cognitive impairment, hippocampal atrophy and EEG changes in sepsis survivors. J. Neurol. Neurosurg. Psychiatry 2013, 84, 62–69. [Google Scholar] [CrossRef]
- Henriquez-Camacho, C.; Losa, J. Biomarkers for sepsis. Review article. BioMed Res. Int. 2014, 7, 547818. [Google Scholar] [CrossRef]
- Toker, A.K.; Kose, S.; Turken, M. Comparison of Sofa Score, SIRS, q SOF and qSOFA + L Criteria in the Diagnosis and Prognosis of Sepsis. Eurasian J. Med. 2021, 53, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Alalawi, M.S.M.; Aljabran, H.A.M.; Alkhamri, A.M.; Alwahbi, A.M.; AlQarrash, Z.I.; Iraqi, H.A.M.; Alonazi, M.S.M.; Alotaibi, A.R.N.; Alahmari, M.A.M.; Alnuwaiser, A.A.A.; et al. Glasgow Coma Scale in Anticipation of Sepsis and Septic Shock: Review Article. Egypt. J. Hosp. Med. 2017, 69, 2663–2666. [Google Scholar] [CrossRef]
- Atterton, B.; Paulino, M.C.; Povoa, P.; Martin-Loeches, I. Sepsis associated delirum. Medicina 2020, 56, 240. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Group | N | Mean | St. Dev. | St. Error | Min | Max | Median |
|---|---|---|---|---|---|---|---|
| A—confirmed sepsis | 78 | 61.33 | 15.022 | 1.701 | 18 | 88 | 62.0 |
| B—infection without sepsis | 363 | 65.23 | 14.056 | 0.738 | 18 | 92 | 65.0 |
| C—non-infected lesions | 68 | 62.13 | 17.075 | 2.071 | 20 | 90 | 65.5 |
| Total | 509 | 64.22 | 14.699 | 0.652 | 18 | 92 | 65.0 |
| Total | Sepsis | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Sex | 0.519 | 0.471 | - | ||||||
| male | 248 | 56.2% | 41 | 52.6% | 207 | 57.0% | |||
| female | 193 | 43.8% | 37 | 47.4% | 156 | 43.0% | |||
| Background | 0.481 | 0.488 | - | ||||||
| urban | 188 | 42.6% | 36 | 46.2% | 152 | 41.9% | |||
| rural | 253 | 57.4% | 42 | 53.8% | 211 | 58.1% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Sepsis | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Ulcerations, erosions, fissures, excoriations | 11.907 | 0.003 * | 0.197 (0.072 ÷ 0.543) | ||||||
| present | 425 | 96.4% | 70 | 89.7% | 355 | 97.8% | |||
| absent | 16 | 3.6% | 8 | 10.3% | 8 | 2.2% | |||
| Bullae, vesicles | 1.751 | 0.186 | - | ||||||
| present | 123 | 27.9% | 17 | 21.8% | 106 | 29.2% | |||
| absent | 318 | 72.1% | 61 | 78.2% | 257 | 70.8% | |||
| Pruritus | 25.131 | <0.001 * | 0.272 (0.160 ÷ 0.462) | ||||||
| present | 243 | 55.1% | 23 | 29.5% | 220 | 60.6% | |||
| absent | 198 | 44.9% | 55 | 70.5% | 143 | 39.4% | |||
| Tumefaction | 1.983 | 0.159 | - | ||||||
| present | 386 | 87.5% | 72 | 92.3% | 314 | 86.5% | |||
| absent | 55 | 12.5% | 6 | 7.7% | 49 | 13.5% | |||
| Edema | 12.786 | <0.001 ** | 2.891 (1.586 ÷ 5.272) | ||||||
| present | 278 | 63.0% | 63 | 80.8% | 215 | 59.2% | |||
| absent | 163 | 37.0% | 15 | 19.2% | 148 | 40.8% | |||
| Fever, chills | 99.762 | <0.001 ** | 14.622 (7.906 ÷ 27.044) | ||||||
| present | 144 | 32.7% | 63 | 80.8% | 81 | 22.3% | |||
| absent | 297 | 67.3% | 15 | 19.2% | 282 | 77.7% | |||
| Pain | 3.754 | 0.053 | - | ||||||
| present | 398 | 90.2% | 75 | 96.2% | 323 | 89.0% | |||
| absent | 43 | 9.8% | 3 | 3.8% | 40 | 11.0% | |||
| Adenopathy | 14.992 | <0.001 ** | 3.961 (1.889 ÷ 8.302) | ||||||
| present | 33 | 7.5% | 14 | 17.9% | 19 | 5.2% | |||
| absent | 408 | 92.5% | 64 | 82.1% | 344 | 94.8% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Infection | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group B) | No (Group C) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Ulcerations, erosions, fissures, excoriations | 1.123 | 0.391 | - | ||||||
| present | 420 | 97.4% | 355 | 97.8% | 65 | 95.6% | |||
| absent | 11 | 2.6% | 8 | 2.2% | 3 | 4.4% | |||
| Bullae, vesicles | 0.078 | 0.780 | - | ||||||
| present | 127 | 29.5% | 106 | 29.2% | 21 | 30.9% | |||
| absent | 304 | 70.5% | 257 | 70.8% | 47 | 69.1% | |||
| Pruritus | 1.760 | 0.185 | - | ||||||
| present | 267 | 61.9% | 220 | 60.6% | 47 | 69.1% | |||
| absent | 164 | 38.1% | 143 | 39.4% | 21 | 30.9% | |||
| Tumefaction | 5.842 | 0.016 * | 2.136 (1.142 ÷ 3.995) | ||||||
| present | 365 | 84.7% | 314 | 86.5% | 51 | 75% | |||
| absent | 66 | 15.3% | 49 | 13.5% | 17 | 25% | |||
| Edema | 18.575 | <0.001 ** | 3.251 (1.866 ÷ 5.666) | ||||||
| present | 236 | 54.8% | 215 | 59.2% | 21 | 30.9% | |||
| absent | 195 | 45.2% | 148 | 40.8% | 47 | 69.1% | |||
| Fever, chills | 0.099 | 0.753 | - | ||||||
| present | 95 | 22% | 81 | 22.3% | 14 | 20.6% | |||
| absent | 336 | 78% | 282 | 77.7% | 54 | 79.4% | |||
| Pain | 32.712 | <0.001 ** | 4.999 (2.773 ÷ 9.010) | ||||||
| present | 365 | 84.7% | 323 | 89% | 42 | 61.8% | |||
| absent | 66 | 15.3% | 40 | 11% | 26 | 38.2% | |||
| Adenopathy | 2.587 | 0.158 | - | ||||||
| present | 26 | 6% | 19 | 5.2% | 7 | 10.3% | |||
| absent | 405 | 94% | 344 | 94.8% | 61 | 89.7% | |||
| Total | 431 | 100% | 363 | 100% | 68 | 100% | |||
| Glasgow Score 13–14 | Total | Sepsis | Pearson Chi-Squared | OR 95% CI | |||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| present | 13 | 2.9% | 7 | 9% | 6 | 1.7% | 12.030 | 0.003 * | 5.866 (1.914 ÷ 17.975) |
| absent | 428 | 97.1% | 71 | 91% | 357 | 98.3% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Sepsis | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Venous ulcers | 0.110 | 0.740 | - | ||||||
| present | 301 | 68.3% | 52 | 66.7% | 249 | 68.6% | |||
| absent | 140 | 31.7% | 26 | 33.3% | 114 | 31.4% | |||
| Microbial eczema | 42.227 | <0.001 ** | 0.189 (0.111 ÷ 0.323) | ||||||
| present | 273 | 61.9% | 23 | 29.5% | 250 | 68.9% | |||
| absent | 168 | 38.1% | 55 | 70.5% | 113 | 31.1% | |||
| Cellulitis | 43.470 | <0.001 ** | 5.320 (3.136 ÷ 9.026) | ||||||
| present | 93 | 21.1% | 38 | 48.7% | 55 | 15.2% | |||
| absent | 348 | 78.9% | 40 | 51.3% | 308 | 84.8% | |||
| Superinfected bullous dermatoses | 1.149 | 0.284 | - | ||||||
| present | 29 | 6.6% | 3 | 3.8% | 26 | 7.2% | |||
| absent | 412 | 93.4% | 75 | 96.2% | 337 | 92.8% | |||
| Erysipelas | 5.548 | 0.038 * | 2.849 (1.152 ÷ 7.048) | ||||||
| present | 22 | 5% | 8 | 10.3% | 14 | 3.9% | |||
| absent | 419 | 95% | 70 | 89.7% | 349 | 96.1% | |||
| Erythroderma | 4.518 | 0.056 | 3.870 (1.015 ÷ 14.757) | ||||||
| present | 9 | 2% | 4 | 5.1% | 5 | 1.4% | |||
| absent | 432 | 98% | 74 | 94.9% | 358 | 98.6% | |||
| Other dermatoses featuring loss of tissue or the disruption of the skin barrier | 2.801 | 0.094 | - | ||||||
| present | 119 | 27% | 27 | 34.6% | 92 | 25.3% | |||
| absent | 322 | 73% | 51 | 65.4% | 271 | 74.7% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Infection | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group B) | No (Group C) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Venous ulcers | 73.049 | <0.001 ** | 14.319 (6.862 ÷ 29.878) | ||||||
| present | 258 | 59.9% | 249 | 68.6% | 9 | 13.2% | |||
| absent | 173 | 40.1% | 114 | 31.4% | 59 | 86.8% | |||
| Microbial eczema | 40.897 | <0.001 ** | 5.706 (3.213 ÷ 10.134) | ||||||
| present | 269 | 62.4% | 250 | 68.9% | 19 | 27.9% | |||
| absent | 162 | 37.6% | 113 | 31.1% | 49 | 72.1% | |||
| Cellulitis | 9.482 | 0.002 * | 11.964 (1.627 ÷ 87.988) | ||||||
| present | 56 | 13.0% | 55 | 15.2% | 1 | 1.5% | |||
| absent | 375 | 87.0% | 308 | 84.8% | 67 | 98.5% | |||
| Superinfected bullous dermatoses | 0.230 | 0.632 | - | ||||||
| present | 32 | 7.4% | 26 | 7.2% | 6 | 8.8% | |||
| absent | 399 | 92.6% | 337 | 92.8% | 62 | 91.2% | |||
| Erysipelas | 19.214 | <0.001 ** | 0.187 (0.082 ÷ 0.425) | ||||||
| present | 26 | 6.0% | 14 | 3.9% | 12 | 17.6% | |||
| absent | 405 | 94.0% | 349 | 96.1% | 56 | 82.4% | |||
| Erythroderma | 0.877 | 0.305 | - | ||||||
| present | 7 | 1.6% | 5 | 1.4% | 2 | 2.9% | |||
| absent | 424 | 98.4% | 358 | 98.6% | 66 | 97.1% | |||
| Other dermatoses featuring loss of tissue or the disruption of the skin barrier | 27.735 | <0.001 ** | 0.252 (0.148 ÷ 0.431) | ||||||
| present | 131 | 30.4% | 92 | 25.3% | 39 | 57.4% | |||
| absent | 300 | 69.6% | 271 | 74.7% | 29 | 42.6% | |||
| Total | 431 | 100% | 363 | 100% | 68 | 100% | |||
| Total | Sepsis | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| S. aureus | 1.451 | 0.228 | - | ||||||
| present | 191 | 43.3% | 29 | 37.2% | 162 | 44.6% | |||
| absent | 250 | 56.7% | 49 | 62.8% | 201 | 55.4% | |||
| P. aeruginosa | 0.029 | 0.865 | - | ||||||
| present | 149 | 33.8% | 27 | 34.6% | 122 | 33.6% | |||
| absent | 292 | 66.2% | 51 | 65.4% | 241 | 66.4% | |||
| E. coli | 2.125 | 0.145 | - | ||||||
| present | 57 | 12.9% | 14 | 17.9% | 43 | 11.8% | |||
| absent | 384 | 87.1% | 64 | 82.1% | 320 | 88.2% | |||
| K. pneumoniae | 7.237 | 0.007 * | 2.519 (1.262 ÷ 5.031) | ||||||
| present | 43 | 9.8% | 14 | 17.9% | 29 | 8% | |||
| absent | 398 | 90.2% | 64 | 82.1% | 334 | 92% | |||
| S. β-hemolytic | 5.438 | 0.031 * | 2.655 (1.137 ÷ 6.200) | ||||||
| present | 26 | 5.9% | 9 | 11.5% | 17 | 4.7% | |||
| absent | 415 | 94.1% | 69 | 88.5% | 346 | 95.3% | |||
| Other bacterial species | 0.124 | 0.724 | - | ||||||
| present | 134 | 30.4% | 25 | 32.1% | 109 | 30% | |||
| absent | 307 | 69.6% | 53 | 67.9% | 254 | 70% | |||
| Viral agents | 0.033 | 0.855 | - | ||||||
| present | 42 | 9.5% | 7 | 9% | 35 | 9.6% | |||
| absent | 399 | 90.5% | 71 | 91% | 328 | 90.4% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Sepsis | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group A) | No (Group B) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Hypertension | 0.965 | 0.326 | - | ||||||
| present | 284 | 64.4% | 54 | 69.2% | 230 | 63.4% | |||
| absent | 157 | 35.6% | 24 | 30.8% | 133 | 36.6% | |||
| Chronic heart failure | 0.401 | 0.526 | - | ||||||
| present | 167 | 37.9% | 32 | 41% | 135 | 37.2% | |||
| absent | 274 | 62.1% | 46 | 59% | 228 | 62.8% | |||
| Atrial fibrillation | 0.562 | 0.453 | - | ||||||
| present | 126 | 28.6% | 25 | 32.1% | 101 | 27.8% | |||
| absent | 315 | 71.4% | 53 | 67.9% | 262 | 72.2% | |||
| Obliterating arteriopathy of the lower limbs (OALL) | 0.004 | 0.948 | - | ||||||
| present | 29 | 6.6% | 5 | 6.4% | 24 | 6.6% | |||
| absent | 412 | 93.4% | 73 | 93.6% | 339 | 93.4% | |||
| Anemia | 8.583 | 0.003 * | 2.075 (1.266 ÷ 3.402) | ||||||
| present | 178 | 40.4% | 43 | 55.1% | 135 | 37.2% | |||
| absent | 263 | 59.6% | 35 | 44.9% | 228 | 62.8% | |||
| Type 1 diabetes mellitus | 7.606 | 0.021 * | 6.486 (1.422 ÷ 29.590) | ||||||
| present | 7 | 1.6% | 4 | 5.1% | 3 | 0.8% | |||
| absent | 434 | 98.4% | 74 | 94.9% | 360 | 99.2% | |||
| Type 2 diabetes mellitus | 1.180 | 0.277 | - | ||||||
| present | 93 | 21.1% | 20 | 25.6% | 73 | 20.1% | |||
| absent | 348 | 78.9% | 58 | 74.4% | 290 | 79.9% | |||
| Neurological conditions | 0.161 | 0.688 | - | ||||||
| present | 133 | 30.2% | 25 | 32.1% | 108 | 29.8% | |||
| absent | 308 | 69.8% | 53 | 67.9% | 255 | 70.2% | |||
| Renal/genital conditions | 1.355 | 0.244 | - | ||||||
| present | 118 | 26.8% | 25 | 32.1% | 93 | 25.6% | |||
| absent | 323 | 73.2% | 53 | 67.9% | 270 | 74.4% | |||
| Respiratory conditions | 0.008 | 0.928 | - | ||||||
| present | 44 | 10% | 8 | 10.3% | 36 | 9.9% | |||
| absent | 397 | 90% | 70 | 89.7% | 327 | 90.1% | |||
| Total | 441 | 100% | 78 | 100% | 363 | 100% | |||
| Total | Infection | Pearson Chi-Squared | OR 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (Group B) | No (Group C) | ||||||||
| N | % | N | % | N | % | Chi2 | p | ||
| Hypertension | 0.504 | 0.478 | - | ||||||
| present | 270 | 62.6% | 230 | 63.4% | 40 | 58.8% | |||
| absent | 161 | 37.4% | 133 | 36.6% | 28 | 41.2% | |||
| Chronic heart failure | 4.696 | 0.030 * | 1.924 (1.057 ÷ 3.504) | ||||||
| present | 151 | 35.0% | 135 | 37.2% | 16 | 23.5% | |||
| absent | 280 | 65.0% | 228 | 62.8% | 52 | 76.5% | |||
| Atrial fibrillation | 6.412 | 0.011 * | 2.527 (1.208 ÷ 5.286) | ||||||
| present | 110 | 25.5% | 101 | 27.8% | 9 | 13.2% | |||
| absent | 321 | 74.5% | 262 | 72.2% | 59 | 86.8% | |||
| Obliterating arteriopathy of the lower limbs (OALL) | 1.361 | 0.402 | - | ||||||
| present | 26 | 6.0% | 24 | 6.6% | 2 | 2.9% | |||
| absent | 405 | 94.0% | 339 | 93.4% | 66 | 97.1% | |||
| Anemia | 2.874 | 0.090 | - | ||||||
| present | 153 | 35.5% | 135 | 37.2% | 18 | 26.5% | |||
| absent | 278 | 64.5% | 228 | 62.8% | 50 | 73.5% | |||
| Type 1 diabetes mellitus | 0.566 | 1.000 | - | ||||||
| present | 3 | 0.7% | 3 | 0.8% | 0% | ||||
| absent | 428 | 99.3% | 360 | 99.2% | 68 | 100% | |||
| Type 2 diabetes mellitus | 0.565 | 0.452 | - | ||||||
| present | 84 | 19.5% | 73 | 20.1% | 11 | 16.2% | |||
| absent | 347 | 80.5% | 290 | 79.9% | 57 | 83.8% | |||
| Neurological conditions | 5.281 | 0.022 * | 2.195 (1.108 ÷ 4.347) | ||||||
| present | 119 | 27.6% | 108 | 29.8% | 11 | 16.2% | |||
| absent | 312 | 72.4% | 255 | 70.2% | 57 | 83.8% | |||
| Renal/genital conditions | 0.160 | 0.689 | - | ||||||
| present | 112 | 26.0% | 93 | 25.6% | 19 | 27.9% | |||
| absent | 319 | 74.0% | 270 | 74.4% | 49 | 72.1% | |||
| Respiratory conditions | 0.213 | 0.644 | - | ||||||
| present | 44 | 10.2% | 36 | 9.9% | 8 | 11.8% | |||
| absent | 387 | 89.8% | 327 | 90.1% | 60 | 88.2% | |||
| Total | 431 | 100% | 363 | 100% | 68 | 100% | |||
| Risk Factors | 95% CI | ||||
|---|---|---|---|---|---|
| (Statistically Significant) | Coef. B | p-Value | Odds Ratio | Lower | Upper |
| Rural background | 1.066 | 0.001 * | 2.903 | 1.521 | 5.538 |
| Neurological conditions | 1.203 | 0.002 * | 3.329 | 1.527 | 7.260 |
| E. coli | 2.368 | 0.026 * | 10.679 | 1.335 | 85.416 |
| Venous ulcers | 2.205 | <0.001 ** | 9.073 | 3.833 | 21.480 |
| Cellulitis | 2.205 | 0.037 * | 9.071 | 1.137 | 72.347 |
| Microbial eczema | 1.130 | 0.002 * | 3.094 | 1.489 | 6.432 |
| Constant | −0.789 | 0.009 | 0.454 | ||
| Rural Residence | Neurological Conditions | E. coli | Venous Ulcers | Cellulitis | Microbial Eczema | Risk of Infection |
|---|---|---|---|---|---|---|
| 0 | 0 | 0 | 0 | 0 | 0 | 0.31 |
| 0 | 0 | 0 | 0 | 0 | 1 | 0.58 |
| 0 | 0 | 0 | 0 | 1 | 0 | 0.80 |
| 0 | 0 | 0 | 0 | 1 | 1 | 0.93 |
| 0 | 0 | 0 | 1 | 0 | 0 | 0.80 |
| 0 | 0 | 0 | 1 | 0 | 1 | 0.93 |
| 0 | 0 | 0 | 1 | 1 | 0 | 0.97 |
| 0 | 0 | 0 | 1 | 1 | 1 | 0.99 |
| 0 | 0 | 1 | 0 | 0 | 0 | 0.83 |
| 0 | 0 | 1 | 0 | 0 | 1 | 0.94 |
| 0 | 0 | 1 | 0 | 1 | 0 | 0.98 |
| 0 | 0 | 1 | 0 | 1 | 1 | 0.99 |
| 0 | 0 | 1 | 1 | 0 | 0 | 0.98 |
| 0 | 0 | 1 | 1 | 0 | 1 | 0.99 |
| 0 | 0 | 1 | 1 | 1 | 0 | 1.00 |
| 0 | 0 | 1 | 1 | 1 | 1 | 1.00 |
| 0 | 1 | 0 | 0 | 0 | 0 | 0.60 |
| 0 | 1 | 0 | 0 | 0 | 1 | 0.82 |
| 0 | 1 | 0 | 0 | 1 | 0 | 0.93 |
| 0 | 1 | 0 | 0 | 1 | 1 | 0.98 |
| 0 | 1 | 0 | 1 | 0 | 0 | 0.93 |
| 0 | 1 | 0 | 1 | 0 | 1 | 0.98 |
| 0 | 1 | 0 | 1 | 1 | 0 | 0.99 |
| 0 | 1 | 0 | 1 | 1 | 1 | 1.00 |
| 0 | 1 | 1 | 0 | 0 | 0 | 0.94 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0.98 |
| 0 | 1 | 1 | 0 | 1 | 0 | 0.99 |
| 0 | 1 | 1 | 0 | 1 | 1 | 1.00 |
| 0 | 1 | 1 | 1 | 0 | 0 | 0.99 |
| 0 | 1 | 1 | 1 | 0 | 1 | 1.00 |
| 0 | 1 | 1 | 1 | 1 | 0 | 1.00 |
| 0 | 1 | 1 | 1 | 1 | 1 | 1.00 |
| 1 | 0 | 0 | 0 | 0 | 0 | 0.57 |
| 1 | 0 | 0 | 0 | 0 | 1 | 0.80 |
| 1 | 0 | 0 | 0 | 1 | 0 | 0.92 |
| 1 | 0 | 0 | 0 | 1 | 1 | 0.97 |
| 1 | 0 | 0 | 1 | 0 | 0 | 0.92 |
| 1 | 0 | 0 | 1 | 0 | 1 | 0.97 |
| 1 | 0 | 0 | 1 | 1 | 0 | 0.99 |
| 1 | 0 | 0 | 1 | 1 | 1 | 1.00 |
| 1 | 0 | 1 | 0 | 0 | 0 | 0.93 |
| 1 | 0 | 1 | 0 | 0 | 1 | 0.98 |
| 1 | 0 | 1 | 0 | 1 | 0 | 0.99 |
| 1 | 0 | 1 | 0 | 1 | 1 | 1.00 |
| 1 | 0 | 1 | 1 | 0 | 0 | 0.99 |
| 1 | 0 | 1 | 1 | 0 | 1 | 1.00 |
| 1 | 0 | 1 | 1 | 1 | 0 | 1.00 |
| 1 | 0 | 1 | 1 | 1 | 1 | 1.00 |
| 1 | 1 | 0 | 0 | 0 | 0 | 0.81 |
| 1 | 1 | 0 | 0 | 0 | 1 | 0.93 |
| 1 | 1 | 0 | 0 | 1 | 0 | 0.98 |
| 1 | 1 | 0 | 0 | 1 | 1 | 0.99 |
| 1 | 1 | 0 | 1 | 0 | 0 | 0.98 |
| 1 | 1 | 0 | 1 | 0 | 1 | 0.99 |
| 1 | 1 | 0 | 1 | 1 | 0 | 1.00 |
| 1 | 1 | 0 | 1 | 1 | 1 | 1.00 |
| 1 | 1 | 1 | 0 | 0 | 0 | 0.98 |
| 1 | 1 | 1 | 0 | 0 | 1 | 0.99 |
| 1 | 1 | 1 | 0 | 1 | 0 | 1.00 |
| 1 | 1 | 1 | 0 | 1 | 1 | 1.00 |
| 1 | 1 | 1 | 1 | 0 | 0 | 1.00 |
| 1 | 1 | 1 | 1 | 0 | 1 | 1.00 |
| 1 | 1 | 1 | 1 | 1 | 0 | 1.00 |
| 1 | 1 | 1 | 1 | 1 | 1 | 1.00 |
| Risk Factors | 95% CI | ||||
|---|---|---|---|---|---|
| (Statistically Significant) | Coef. B | p-Value | Odds Ratio | Lower | Upper |
| Glasgow score 13, 14 | 1.696 | 0.023 * | 5.451 | 1.268 | 23.432 |
| Fever, chills | 2.251 | <0.001 ** | 9.497 | 4.703 | 19.177 |
| Adenopathy | 1.384 | 0.003 * | 3.993 | 1.594 | 10.003 |
| Type 1 diabetes mellitus | 2.668 | 0.005 * | 14.404 | 2.205 | 94.101 |
| Anemia | 0.678 | 0.026 * | 1.971 | 1.086 | 3.578 |
| Cellulitis | 1.180 | <0.001 ** | 3.253 | 1.652 | 6.404 |
| Constant | −3.703 | <0.001 | 0.025 | ||
| Glasgow Scores 13, 14 | Fever, Chills | Adenopathy | T1DM | Anemia | Cellulitis | Risk of Sepsis |
|---|---|---|---|---|---|---|
| 0 | 0 | 0 | 0 | 0 | 0 | 0.02 |
| 0 | 0 | 0 | 0 | 0 | 1 | 0.07 |
| 0 | 0 | 0 | 0 | 1 | 0 | 0.05 |
| 0 | 0 | 0 | 0 | 1 | 1 | 0.14 |
| 0 | 0 | 0 | 1 | 0 | 0 | 0.26 |
| 0 | 0 | 0 | 1 | 0 | 1 | 0.54 |
| 0 | 0 | 0 | 1 | 1 | 0 | 0.41 |
| 0 | 0 | 0 | 1 | 1 | 1 | 0.69 |
| 0 | 0 | 1 | 0 | 0 | 0 | 0.09 |
| 0 | 0 | 1 | 0 | 0 | 1 | 0.24 |
| 0 | 0 | 1 | 0 | 1 | 0 | 0.16 |
| 0 | 0 | 1 | 0 | 1 | 1 | 0.39 |
| 0 | 0 | 1 | 1 | 0 | 0 | 0.59 |
| 0 | 0 | 1 | 1 | 0 | 1 | 0.82 |
| 0 | 0 | 1 | 1 | 1 | 0 | 0.74 |
| 0 | 0 | 1 | 1 | 1 | 1 | 0.90 |
| 0 | 1 | 0 | 0 | 0 | 0 | 0.19 |
| 0 | 1 | 0 | 0 | 0 | 1 | 0.43 |
| 0 | 1 | 0 | 0 | 1 | 0 | 0.32 |
| 0 | 1 | 0 | 0 | 1 | 1 | 0.60 |
| 0 | 1 | 0 | 1 | 0 | 0 | 0.77 |
| 0 | 1 | 0 | 1 | 0 | 1 | 0.92 |
| 0 | 1 | 0 | 1 | 1 | 0 | 0.87 |
| 0 | 1 | 0 | 1 | 1 | 1 | 0.96 |
| 0 | 1 | 1 | 0 | 0 | 0 | 0.48 |
| 0 | 1 | 1 | 0 | 0 | 1 | 0.75 |
| 0 | 1 | 1 | 0 | 1 | 0 | 0.65 |
| 0 | 1 | 1 | 0 | 1 | 1 | 0.86 |
| 0 | 1 | 1 | 1 | 0 | 0 | 0.93 |
| 0 | 1 | 1 | 1 | 0 | 1 | 0.98 |
| 0 | 1 | 1 | 1 | 1 | 0 | 0.96 |
| 0 | 1 | 1 | 1 | 1 | 1 | 0.99 |
| 1 | 0 | 0 | 0 | 0 | 0 | 0.12 |
| 1 | 0 | 0 | 0 | 0 | 1 | 0.30 |
| 1 | 0 | 0 | 0 | 1 | 0 | 0.21 |
| 1 | 0 | 0 | 0 | 1 | 1 | 0.46 |
| 1 | 0 | 0 | 1 | 0 | 0 | 0.66 |
| 1 | 0 | 0 | 1 | 0 | 1 | 0.86 |
| 1 | 0 | 0 | 1 | 1 | 0 | 0.79 |
| 1 | 0 | 0 | 1 | 1 | 1 | 0.93 |
| 1 | 0 | 1 | 0 | 0 | 0 | 0.35 |
| 1 | 0 | 1 | 0 | 0 | 1 | 0.64 |
| 1 | 0 | 1 | 0 | 1 | 0 | 0.51 |
| 1 | 0 | 1 | 0 | 1 | 1 | 0.77 |
| 1 | 0 | 1 | 1 | 0 | 0 | 0.89 |
| 1 | 0 | 1 | 1 | 0 | 1 | 0.96 |
| 1 | 0 | 1 | 1 | 1 | 0 | 0.94 |
| 1 | 0 | 1 | 1 | 1 | 1 | 0.98 |
| 1 | 1 | 0 | 0 | 0 | 0 | 0.56 |
| 1 | 1 | 0 | 0 | 0 | 1 | 0.81 |
| 1 | 1 | 0 | 0 | 1 | 0 | 0.72 |
| 1 | 1 | 0 | 0 | 1 | 1 | 0.89 |
| 1 | 1 | 0 | 1 | 0 | 0 | 0.95 |
| 1 | 1 | 0 | 1 | 0 | 1 | 0.98 |
| 1 | 1 | 0 | 1 | 1 | 0 | 0.97 |
| 1 | 1 | 0 | 1 | 1 | 1 | 0.99 |
| 1 | 1 | 1 | 0 | 0 | 0 | 0.84 |
| 1 | 1 | 1 | 0 | 0 | 1 | 0.94 |
| 1 | 1 | 1 | 0 | 1 | 0 | 0.91 |
| 1 | 1 | 1 | 0 | 1 | 1 | 0.97 |
| 1 | 1 | 1 | 1 | 0 | 0 | 0.99 |
| 1 | 1 | 1 | 1 | 0 | 1 | 1.00 |
| 1 | 1 | 1 | 1 | 1 | 0 | 0.99 |
| 1 | 1 | 1 | 1 | 1 | 1 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pătrașcu, A.-I.; Vâță, D.; Temelie-Olinici, D.; Mocanu, M.; Guguluș, D.-L.; Marinescu, M.; Stafie, L.; Tarcău, B.-M.; Creţu, I.; Popescu, I.-A.; et al. Skin Lesions with Loss of Tissue and Cutaneous-Onset Sepsis: The Skin Infection–Sepsis Relationship. Diagnostics 2024, 14, 659. https://doi.org/10.3390/diagnostics14060659
Pătrașcu A-I, Vâță D, Temelie-Olinici D, Mocanu M, Guguluș D-L, Marinescu M, Stafie L, Tarcău B-M, Creţu I, Popescu I-A, et al. Skin Lesions with Loss of Tissue and Cutaneous-Onset Sepsis: The Skin Infection–Sepsis Relationship. Diagnostics. 2024; 14(6):659. https://doi.org/10.3390/diagnostics14060659
Chicago/Turabian StylePătrașcu, Adriana-Ionela, Dan Vâță, Doinița Temelie-Olinici, Mădălina Mocanu, Dumitrița-Lenuța Guguluș, Mădălina Marinescu, Liviu Stafie, Bogdan-Marian Tarcău, Ioana Creţu, Ioana-Adriana Popescu, and et al. 2024. "Skin Lesions with Loss of Tissue and Cutaneous-Onset Sepsis: The Skin Infection–Sepsis Relationship" Diagnostics 14, no. 6: 659. https://doi.org/10.3390/diagnostics14060659
APA StylePătrașcu, A. -I., Vâță, D., Temelie-Olinici, D., Mocanu, M., Guguluș, D. -L., Marinescu, M., Stafie, L., Tarcău, B. -M., Creţu, I., Popescu, I. -A., Cimpoeșu, C. -D., & Gheucă-Solovăstru, L. (2024). Skin Lesions with Loss of Tissue and Cutaneous-Onset Sepsis: The Skin Infection–Sepsis Relationship. Diagnostics, 14(6), 659. https://doi.org/10.3390/diagnostics14060659