


ReClassification of Patients with Ambiguous CA125 for Optimised Pre-Surgical Triage

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Risk Prediction Models
3. Results
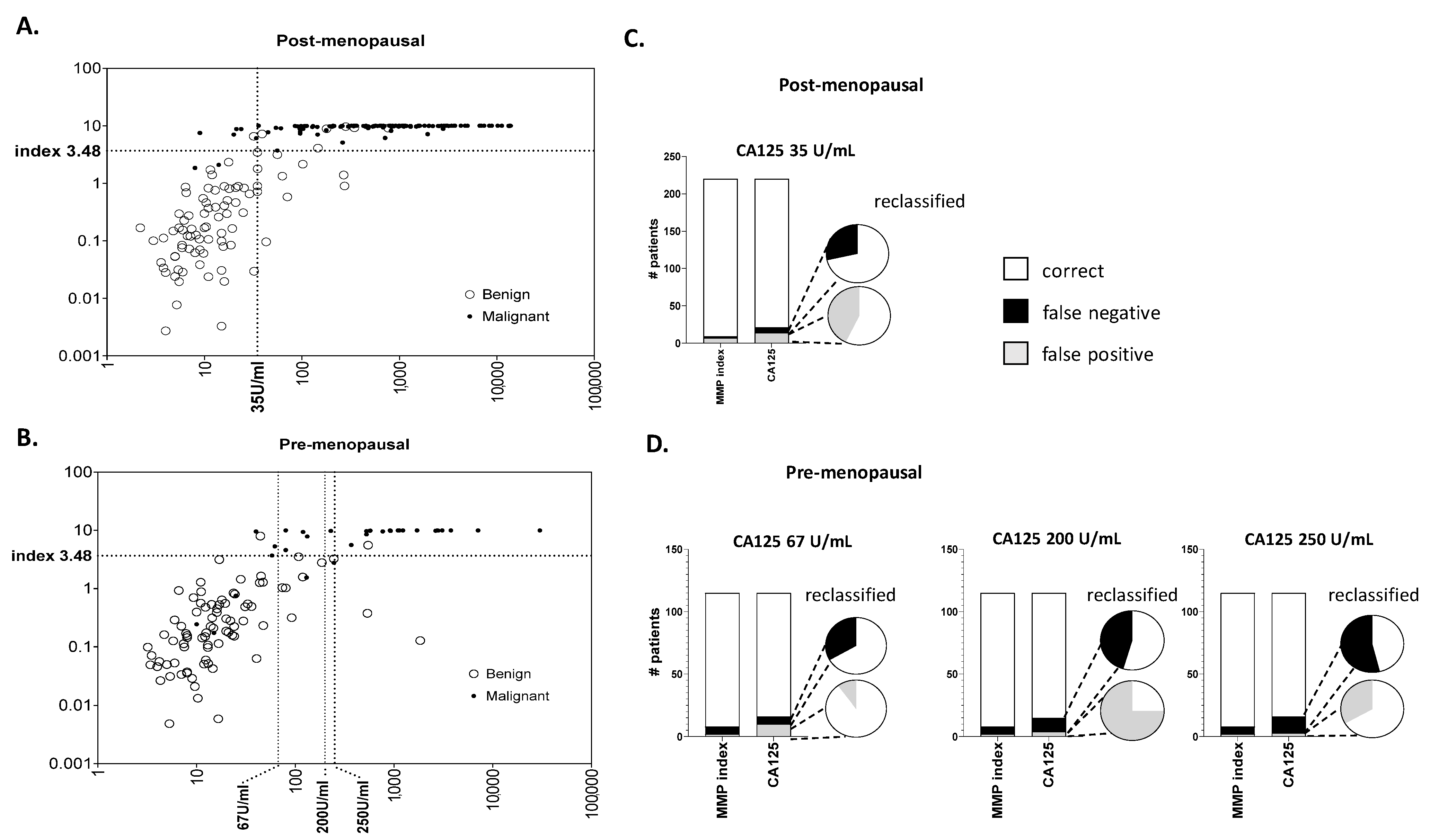
3.1. Use of MMP Index Successfully Rescues Samples Mis-Classified by CA125
3.2. Net Re-Classification Analysis Improves Case/Control Assignment at Clinical Thresholds
3.2.1. Re-Classification of Post-Menopausal Patients
3.2.2. Reclassification of Pre-Menopausal Patients
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabasag, C.J.; Fagan, P.J.; Ferlay, J.; Vignat, J.; Laversanne, M.; Liu, L.; van der Aa, M.A.; Bray, F.; Soerjomataram, I. Ovarian cancer today and tomorrow: A global assessment by world region and Human Development Index using GLOBOCAN 2020. Int. J. Cancer 2022, 151, 1535–1541. [Google Scholar] [CrossRef]
- Henderson, J.T.; Webber, E.M.; Sawaya, G.F. Screening for Ovarian Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, M. Investigation and management of an ovarian mass. Aust. Fam. Physician 2015, 44, 48–52. [Google Scholar] [PubMed]
- The American College of Obstetricians and Gynecologists; Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet. Gynecol. 2016, 128, e210–e226. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Ovarian Cancer: The Recognition and Initial Management of Ovarian Cancer; National Institute for Health and Care Excellence: London, UK, 2011. [Google Scholar]
- Dearking, A.C.; Aletti, G.D.; McGree, M.E.; Weaver, A.L.; Sommerfield, M.K.; Cliby, W.A. How relevant are ACOG and SGO guidelines for referral of adnexal mass? Obstet. Gynecol. 2007, 110, 841–848. [Google Scholar] [CrossRef]
- Skates, S.J.; Mai, P.; Horick, N.K.; Piedmonte, M.; Drescher, C.W.; Isaacs, C.; Armstrong, D.K.; Buys, S.S.; Rodriguez, G.C.; Horowitz, I.R.; et al. Large prospective study of ovarian cancer screening in high-risk women: CA125 cut-point defined by menopausal status. Cancer Prev. Res. 2011, 4, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Sopik, V.; Rosen, B.; Giannakeas, V.; Narod, S.A. Why have ovarian cancer mortality rates declined? Part III. Prospects for the future. Gynecol. Oncol. 2015, 138, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Nustad, K.; Bast, R.C., Jr.; Brien, T.J.; Nilsson, O.; Seguin, P.; Suresh, M.R.; Saga, T.; Nozawa, S.; Bormer, O.P.; de Bruijn, H.W.; et al. Specificity and affinity of 26 monoclonal antibodies against the CA 125 antigen: First report from the ISOBM TD-1 workshop. International Society for Oncodevelopmental Biology and Medicine. Tumour Biol. 1996, 17, 196–219. [Google Scholar] [CrossRef]
- Carney, M.E.; Lancaster, J.M.; Ford, C.; Tsodikov, A.; Wiggins, C.L. A population-based study of patterns of care for ovarian cancer: Who is seen by a gynecologic oncologist and who is not? Gynecol. Oncol. 2002, 84, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Earle, C.C.; Schrag, D.; Neville, B.A.; Yabroff, K.R.; Topor, M.; Fahey, A.; Trimble, E.L.; Bodurka, D.C.; Bristow, R.E.; Carney, M.; et al. Effect of surgeon specialty on processes of care and outcomes for ovarian cancer patients. J. Natl. Cancer Inst. 2006, 98, 172–180. [Google Scholar] [CrossRef]
- Burgess, B.T.; Ueland, F.R. Adnexal tumors in menopausal women: Surgery or surveillance? Menopause 2019, 26, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J. Fertility preservation in women, focusing on cancer, benign diseases and social reasons. Minerva Ginecol. 2018, 70, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Schuring, A.N.; Fehm, T.; Behringer, K.; Goeckenjan, M.; Wimberger, P.; Henes, M.; Henes, J.; Fey, M.F.; von Wolff, M. Practical recommendations for fertility preservation in women by the FertiPROTEKT network. Part I: Indications for fertility preservation. Arch. Gynecol. Obstet. 2018, 297, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Cai, J.; Gao, A.; Wang, Z.; Cai, L. Fertility sparing surgery vs radical surgery for epithelial ovarian cancer: A meta-analysis of overall survival and disease-free survival. BMC Cancer 2020, 20, 320. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Kapp, D.S.; Shin, J.Y.; Husain, A.; Teng, N.N.; Berek, J.S.; Osann, K.; Leiserowitz, G.S.; Cress, R.D.; O’Malley, C. Influence of the gynecologic oncologist on the survival of ovarian cancer patients. Obstet. Gynecol. 2007, 109, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Engelen, M.J.; Kos, H.E.; Willemse, P.H.; Aalders, J.G.; de Vries, E.G.; Schaapveld, M.; Otter, R.; van der Zee, A.G. Surgery by consultant gynecologic oncologists improves survival in patients with ovarian carcinoma. Cancer 2006, 106, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Giede, K.C.; Kieser, K.; Dodge, J.; Rosen, B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol. Oncol. 2005, 99, 447–461. [Google Scholar] [CrossRef]
- Vernooij, F.; Heintz, P.; Witteveen, E.; van der Graaf, Y. The outcomes of ovarian cancer treatment are better when provided by gynecologic oncologists and in specialized hospitals: A systematic review. Gynecol. Oncol. 2007, 105, 801–812. [Google Scholar] [CrossRef]
- Canis, M.; Rabischong, B.; Houlle, C.; Botchorishvili, R.; Jardon, K.; Safi, A.; Wattiez, A.; Mage, G.; Pouly, J.L.; Bruhat, M.A. Laparoscopic management of adnexal masses: A gold standard? Curr. Opin. Obstet. Gynecol. 2002, 14, 423–428. [Google Scholar] [CrossRef]
- Funston, G.; Van Melle, M.; Baun, M.L.; Jensen, H.; Helsper, C.; Emery, J.; Crosbie, E.J.; Thompson, M.; Hamilton, W.; Walter, F.M. Variation in the initial assessment and investigation for ovarian cancer in symptomatic women: A systematic review of international guidelines. BMC Cancer 2019, 19, 1028. [Google Scholar] [CrossRef]
- Friedrich, L.; Meyer, R.; Levin, G. Management of adnexal mass: A comparison of five national guidelines. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 265, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Davenport, C.F.; Rai, N.; Sharma, P.; Deeks, J.; Berhane, S.; Mallett, S.; Saha, P.; Solanki, R.; Bayliss, S.; Snell, K.; et al. Diagnostic Models Combining Clinical Information, Ultrasound and Biochemical Markers for Ovarian Cancer: Cochrane Systematic Review and Meta-Analysis. Cancers 2022, 14, 3621. [Google Scholar] [CrossRef] [PubMed]
- Ashmore, A.A.; Gnanachandran, C.; Luqman, I.; Horrocks, K. One-stop clinic for patients with suspected ovarian cancer: Results from a retrospective outcome study of the referral pathway. BMC Womens Health 2021, 21, 429. [Google Scholar] [CrossRef] [PubMed]
- Auekitrungrueng, R.; Tinnangwattana, D.; Tantipalakorn, C.; Charoenratana, C.; Lerthiranwong, T.; Wanapirak, C.; Tongsong, T. Comparison of the diagnostic accuracy of International Ovarian Tumor Analysis simple rules and the risk of malignancy index to discriminate between benign and malignant adnexal masses. Int. J. Gynaecol. Obstet. 2019, 146, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Women’s, I.; Atri, M.; Alabousi, A.; Reinhold, C.; Akin, E.A.; Benson, C.B.; Bhosale, P.R.; Kang, S.K.; Lakhman, Y.; Nicola, R.; et al. ACR Appropriateness Criteria® Clinically Suspected Adnexal Mass, No Acute Symptoms. J. Am. Coll. Radiol. 2019, 16, S77–S93. [Google Scholar] [CrossRef]
- Pelayo, M.; Pelayo-Delgado, I.; Sancho-Sauco, J.; Sanchez-Zurdo, J.; Abarca-Martinez, L.; Corraliza-Galan, V.; Martin-Gromaz, C.; Pablos-Antona, M.J.; Zurita-Calvo, J.; Alcazar, J.L. Comparison of Ultrasound Scores in Differentiating between Benign and Malignant Adnexal Masses. Diagnostics 2023, 13, 1307. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.W.; Rainczuk, A.; Oehler, M.K.; Jobling, T.W.; Plebanski, M.; Stephens, A.N. Active Ratio Test (ART) as a Novel Diagnostic for Ovarian Cancer. Diagnostics 2021, 11, 1048. [Google Scholar] [CrossRef] [PubMed]
- Stephens, A.N.; Hobbs, S.J.; Kang, S.W.; Bilandzic, M.; Rainczuk, A.; Oehler, M.K.; Jobling, T.W.; Plebanski, M.; Allman, R. A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer. Cancers 2023, 15, 5267. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R. Quantifying the added value of new biomarkers: How and how not. Diagn. Progn. Res. 2018, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Dite, G.S.; MacInnis, R.J.; Bickerstaffe, A.; Dowty, J.G.; Allman, R.; Apicella, C.; Milne, R.L.; Tsimiklis, H.; Phillips, K.A.; Giles, G.G.; et al. Breast Cancer Risk Prediction Using Clinical Models and 77 Independent Risk-Associated SNPs for Women Aged Under 50 Years: Australian Breast Cancer Family Registry. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.; Jenkins, V.; Farewell, V.; Menon, U.; Jacobs, I.; Kilkerr, J.; Ryan, A.; Langridge, C.; Fallowfield, L.; Trialists, U. Psychological morbidity associated with ovarian cancer screening: Results from more than 23,000 women in the randomised trial of ovarian cancer screening (UKCTOCS). BJOG 2014, 121, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.R.; Drescher, C.W.; Zheng, Y.; Bowen, D.J.; Wilson, S.; Young, A.; McIntosh, M.; Mahony, B.S.; Lowe, K.A.; Urban, N. Changes in cancer worry associated with participation in ovarian cancer screening. Psychooncology 2007, 16, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Hassan, H.; Allen, I.; Sofianopoulou, E.; Walburga, Y.; Turnbull, C.; Eccles, D.M.; Tischkowitz, M.; Pharoah, P.; Antoniou, A.C. Long-term outcomes of hysterectomy with bilateral salpingo-oophorectomy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2023, 230, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.H.; Jacoby, V.; Shoupe, D.; Rocca, W. Effect of bilateral oophorectomy on women’s long-term health. Women’s Health 2009, 5, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Gottschau, M.; Rosthoj, S.; Settnes, A.; Aalborg, G.L.; Viuff, J.H.; Munk, C.; Jensen, A.; Kjaer, S.K.; Mellemkjaer, L. Long-Term Health Consequences After Ovarian Removal at Benign Hysterectomy: A Nationwide Cohort Study. Ann. Intern. Med. 2023, 176, 596–604. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin. Management of adnexal masses. Obstet. Gynecol. 2007, 110, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.R.; Randall, T.C. Adnexal masses in the premenopausal patient. Clin. Obstet. Gynecol. 2015, 58, 47–52. [Google Scholar] [CrossRef]
- Whiteman, M.K.; Kuklina, E.; Jamieson, D.J.; Hillis, S.D.; Marchbanks, P.A. Inpatient hospitalization for gynecologic disorders in the United States. Am. J. Obstet. Gynecol. 2010, 202, 541.e1–546.e6. [Google Scholar] [CrossRef]
- Bolstad, N.; Oijordsbakken, M.; Nustad, K.; Bjerner, J. Human epididymis protein 4 reference limits and natural variation in a Nordic reference population. Tumour Biol. 2012, 33, 141–148. [Google Scholar] [CrossRef]
- Schorge, J.O.; Eisenhauer, E.E.; Chi, D.S. Current surgical management of ovarian cancer. Hematol. Oncol. Clin. N. Am. 2012, 26, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Dunton, C.J.; Hutchcraft, M.L.; Bullock, R.G.; Northrop, L.E.; Ueland, F.R. Salvaging Detection of Early-Stage Ovarian Malignancies When CA125 Is Not Informative. Diagnostics 2021, 11, 1440. [Google Scholar] [CrossRef] [PubMed]
- Vara, J.; Manzour, N.; Chacon, E.; Lopez-Picazo, A.; Linares, M.; Pascual, M.A.; Guerriero, S.; Alcazar, J.L. Ovarian Adnexal Reporting Data System (O-RADS) for Classifying Adnexal Masses: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 3151. [Google Scholar] [CrossRef] [PubMed]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ferrazzi, E.; Ameye, L.; Konstantinovic, M.L.; Van Calster, B.; Collins, W.P.; Vergote, I.; Van Huffel, S.; et al. Logistic regression model to distinguish between the benign and malignant adnexal mass before surgery: A multicenter study by the International Ovarian Tumor Analysis Group. J. Clin. Oncol. 2005, 23, 8794–8801. [Google Scholar] [CrossRef] [PubMed]
- Green–top Guideline No. 62. Management of Suspected Ovarian Masses in Premenopausal Women. In RCOG/BSGE Joint Guideline; BSGE: London, UK, 2011.
- Bullock, B.; Larkin, L.; Turker, L.; Stampler, K. Management of the Adnexal Mass: Considerations for the Family Medicine Physician. Front. Med. 2022, 9, 913549. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Participants (n=) | All Samples | Pre-Menopausal | Post-Menopausal | ||||
|---|---|---|---|---|---|---|---|
| 334 | 115 | 219 | |||||
| FIGO Stage | # Cases (n=) | CA125 (Median, IQ Range) | # Cases (n=) | CA125 (Median, IQ Range) | # Cases (n=) | CA125 (Median, IQ Range) | |
| Malignant | all | 164 | 724 (213, 1734) | 32 | 549 (110, 1350) | 132 | 797 (259, 1845) |
| stage I | 17 | 178 (62, 527) | 11 | 229 (71, 448) | 6 | 137 (35, 646) | |
| stages II–IV | 147 | 821 (281, 2105) | 21 | 911 (130, 2743) | 126 | 817 (301, 1988) | |
| Benign | n/a | 170 | 13 (7, 25) | 83 | 14 (8, 26) | 87 | 12 (6, 24) |
| Combined Risk Score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Malignant | Benign | ||||||||||
| Menopausal Status | Risk Score CA125 | MMP Index ≤ 3.48 | MMP Index > 3.48 | Up | Down | MMP Index ≤ 3.48 | MMP Index > 3.48 | Up | Down | NRI (95% CI) | p Value |
| post-menopausal | ≤35 U/mL | 2 | 5 | 0.04 | 0 | 72 | 1 | 0.011 | 0.09 | 0.12 (0.04, 0.21) | 0.01 |
| >35 U/mL | 0 | 125 | 8 | 6 | |||||||
| pre-menopausal | ≤67 U/mL | 4 | 2 | 0.06 | 0.063 | 72 | 1 | 0.012 | 0.11 | 0.10 (−0.07, 0.27) | 0.26 |
| >67 U/mL | 2 | 24 | 9 | 1 | |||||||
| ≤200 U/mL | 5 | 6 | 0.18 | 0.03 | 78 | 1 | 0.012 | 0.05 | 0.19 (0.02, 0.37) | 0.03 | |
| >200 U/mL | 1 | 21 | 4 | 1 | |||||||
| ≤250 U/mL | 6 | 7 | 0.22 | 0 | 79 | 1 | 0.01 | 0.02 | 0.23 (0.07, 0.41) | 0.01 | |
| >250 U/mL | 0 | 19 | 2 | 1 | |||||||
| Post-Menopausal | Pre-Menopausal | |||||||
|---|---|---|---|---|---|---|---|---|
| CA125 Threshold 35 U/mL | CA125 Threshold 67 U/mL | CA125 Threshold 200 U/mL | CA125 Threshold 250 U/mL | |||||
| n= | misclassified % | n= | misclassified % | n= | misclassified % | n= | misclassified % | |
| total patients | 80 | 80 | 90 | 95 | ||||
| # cancer misclassified CA125 | 7 | 8.8% | 6 | 7.5% | 11 | 12.2% | 13 | 13.7% |
| # cancer misclassified MMPI | 2 | 2.5% | 4 | 5.0% | 5 | 5.6% | 6 | 6.3% |
| %Δ false negatives | 71.4% | 66.7% | 54.5% | 53.8% | ||||
| total patients | 139 | 36 | 25 | 22 | ||||
| # benign mis-classified CA125 | 14 | 10.1% | 10 | 27.8% | 4 | 16.0% | 3 | 13.6% |
| # benign mis-classified MMPI | 6 | 4.3% | 1 | 2.8% | 1 | 4.0% | 1 | 4.5% |
| %D false positives | 57.1% | 90.0% | 75.0% | 66.7% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stephens, A.N.; Hobbs, S.J.; Kang, S.-W.; Oehler, M.K.; Jobling, T.W.; Allman, R. ReClassification of Patients with Ambiguous CA125 for Optimised Pre-Surgical Triage. Diagnostics 2024, 14, 671. https://doi.org/10.3390/diagnostics14070671
Stephens AN, Hobbs SJ, Kang S-W, Oehler MK, Jobling TW, Allman R. ReClassification of Patients with Ambiguous CA125 for Optimised Pre-Surgical Triage. Diagnostics. 2024; 14(7):671. https://doi.org/10.3390/diagnostics14070671
Chicago/Turabian StyleStephens, Andrew N., Simon J. Hobbs, Sung-Woog Kang, Martin K. Oehler, Tom W. Jobling, and Richard Allman. 2024. "ReClassification of Patients with Ambiguous CA125 for Optimised Pre-Surgical Triage" Diagnostics 14, no. 7: 671. https://doi.org/10.3390/diagnostics14070671
APA StyleStephens, A. N., Hobbs, S. J., Kang, S. -W., Oehler, M. K., Jobling, T. W., & Allman, R. (2024). ReClassification of Patients with Ambiguous CA125 for Optimised Pre-Surgical Triage. Diagnostics, 14(7), 671. https://doi.org/10.3390/diagnostics14070671