
Comparative Analysis of Examination Methods for Periapical Lesion Diagnostics: Assessing Cone-Beam Computer Tomography, Ultrasound, and Periapical Radiography
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Inclusion and Exclusion Criteria
2.3. Examination
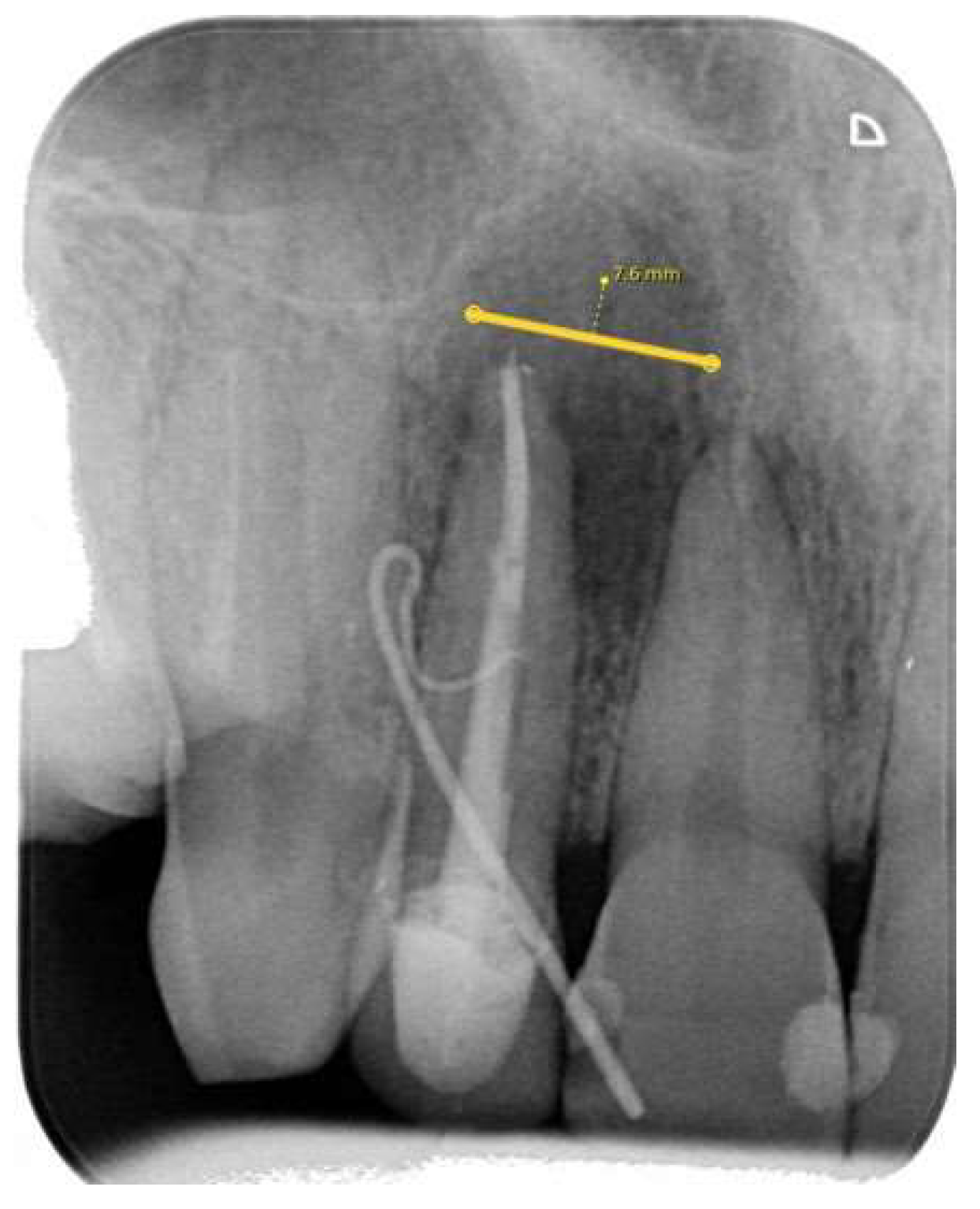
2.3.1. Periapical (PA) Radiography Examination and Evaluation
- Category 1: no discernible periapical lesion was identified;
- Category 2: a periapical lesion was possibly present, however, the distinction was not unequivocal;
- Category 3: a periapical lesion was definitively observed.
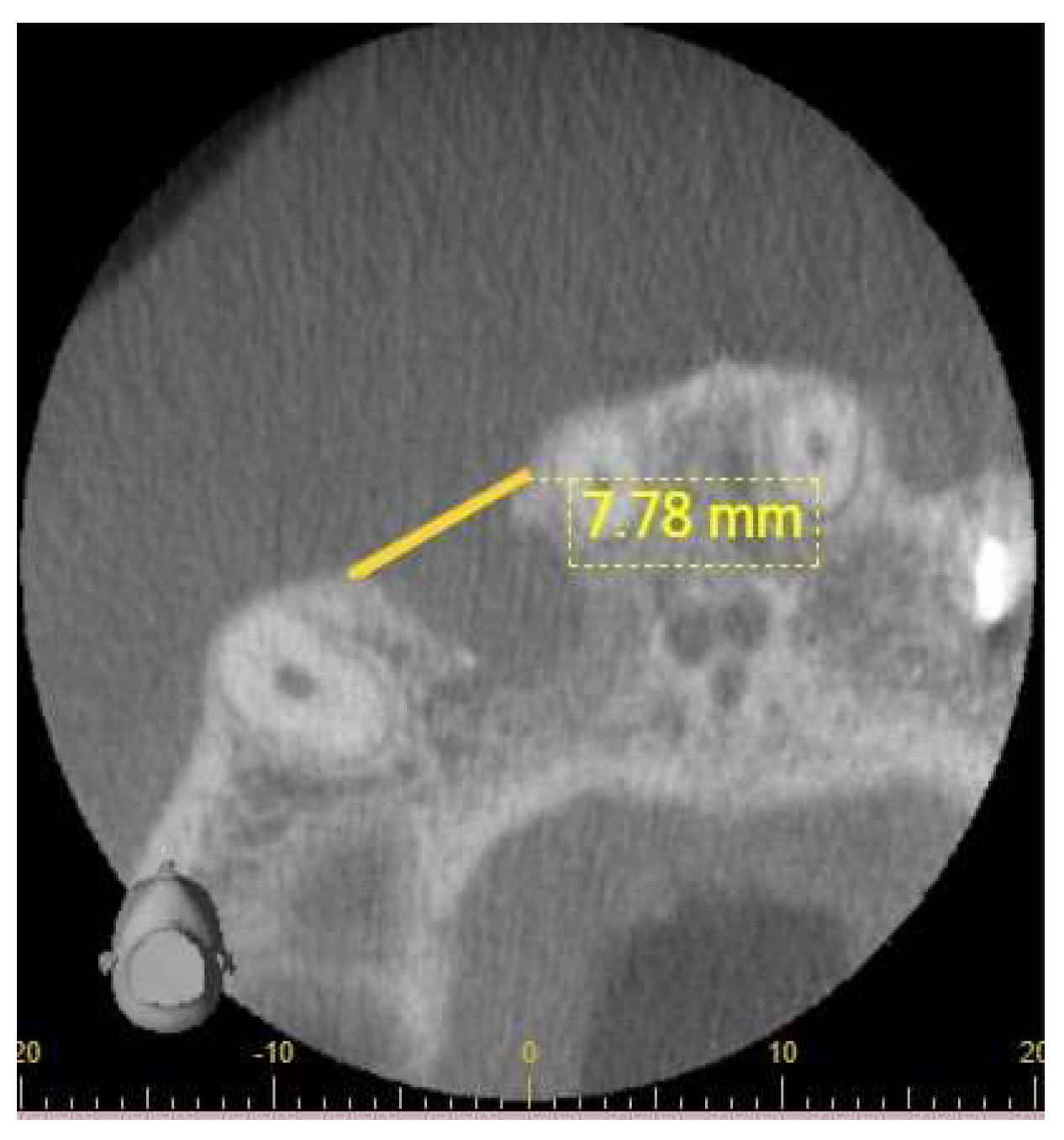
2.3.2. Cone-Beam Computer Tomography (CBCT) Radiographic Examination and Evaluation
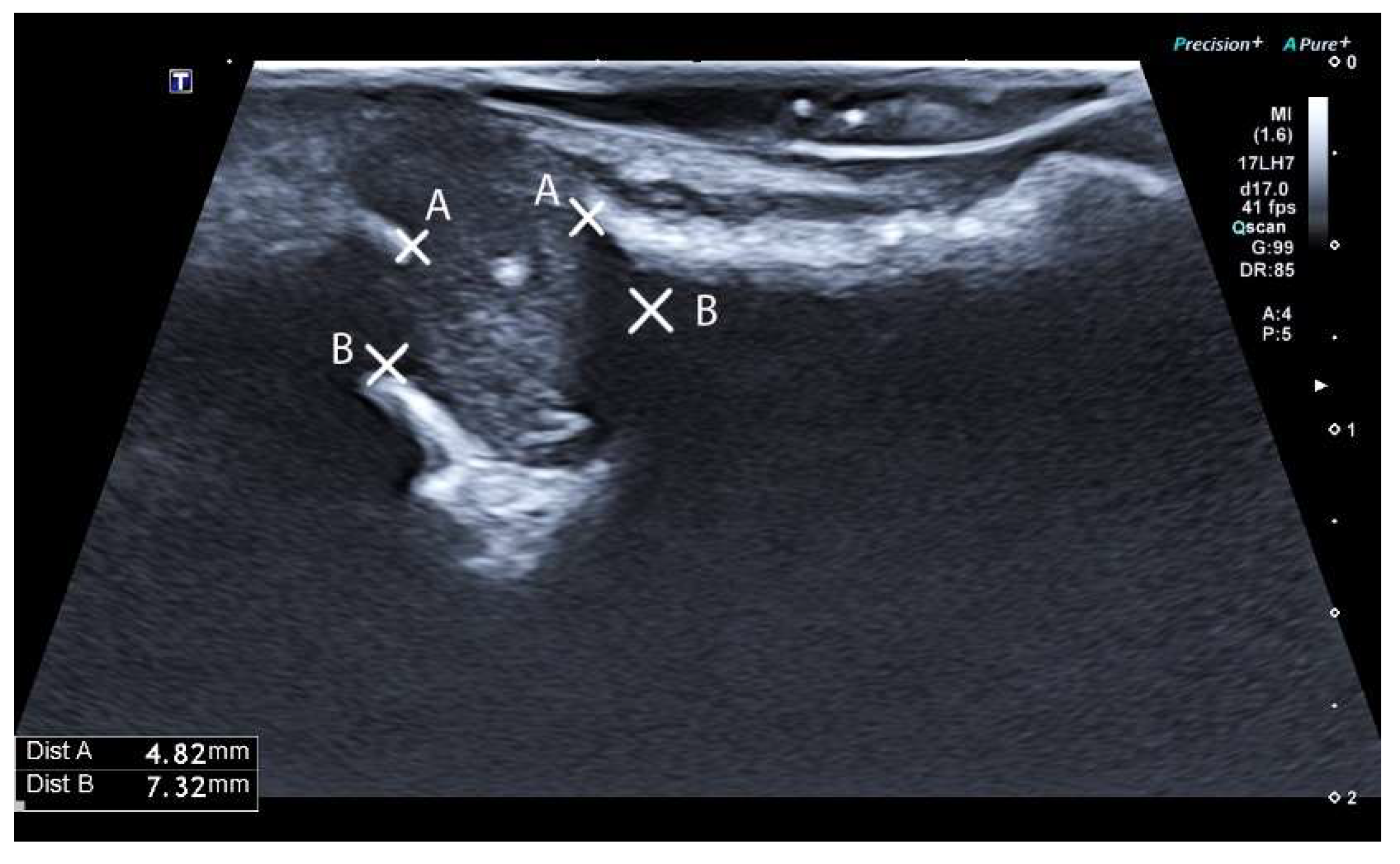
2.3.3. Ultrasound Examination and Evaluation
2.4. Statistical Analysis
3. Results
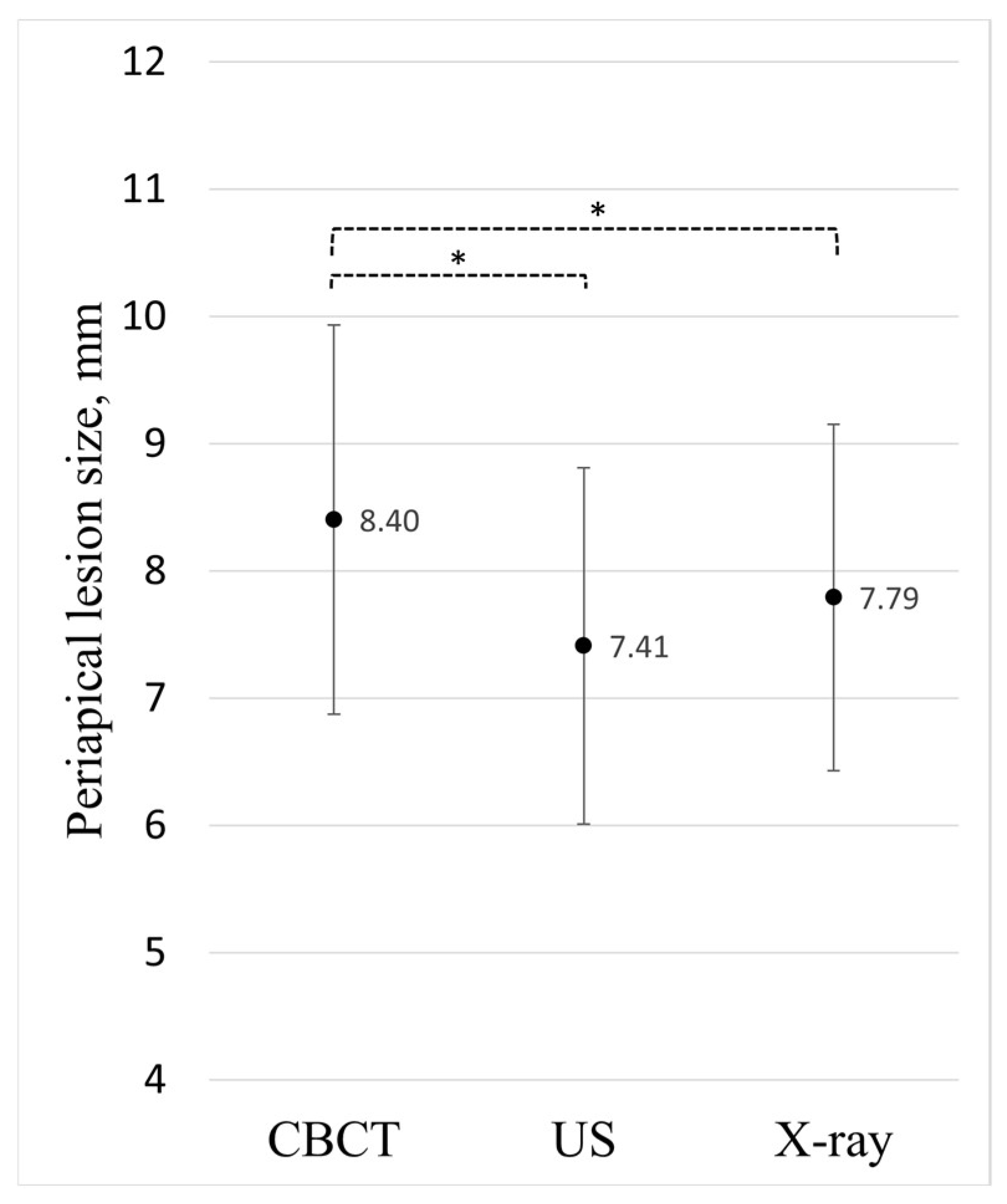
3.1. Comparison of Examination Methods
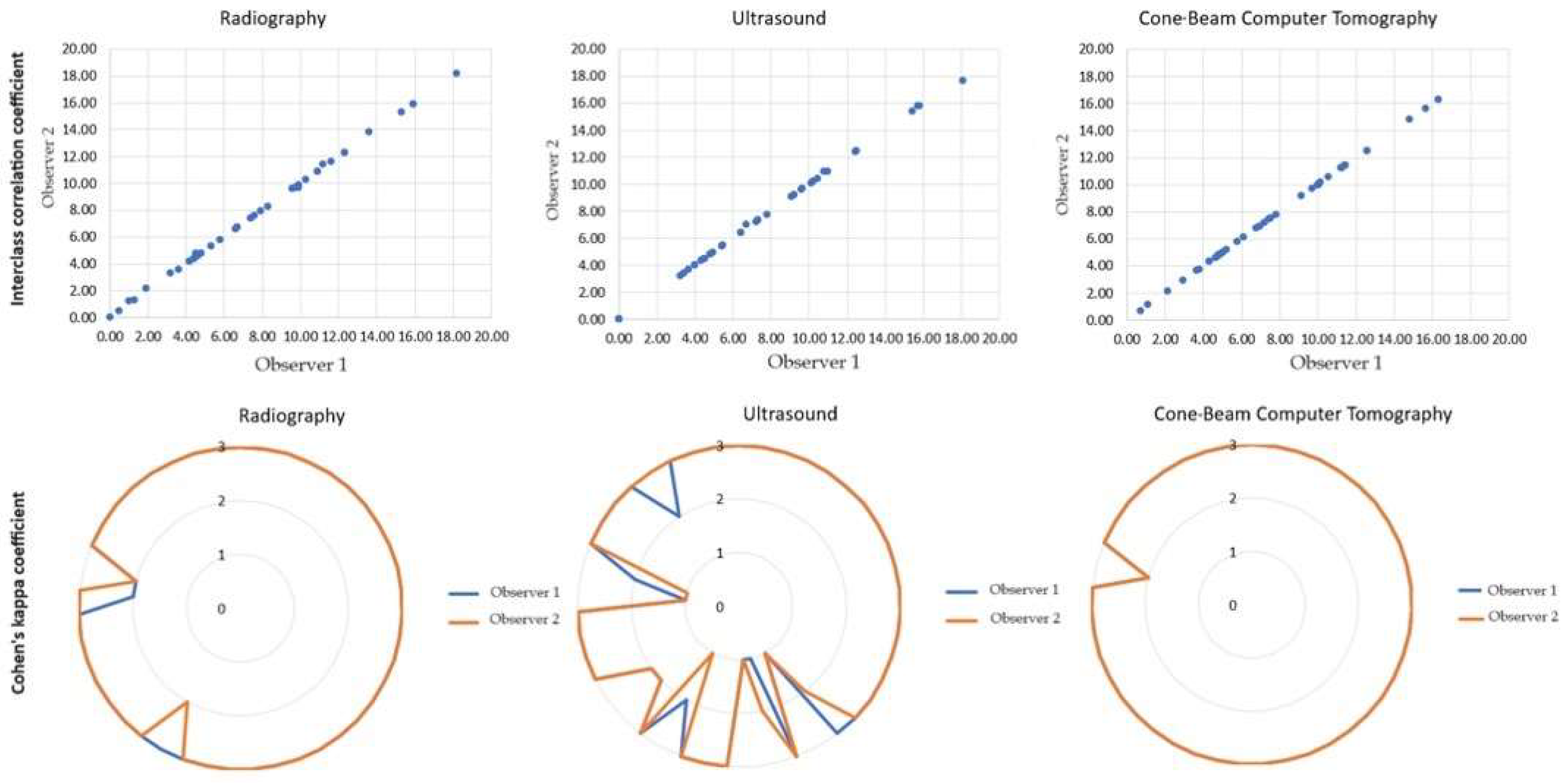
3.2. Observers’ Agreement: Assessing Periapical Lesions through Qualitative and Quantitative Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur. Endod. J. 2020, 5, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Reit, C.; Petersson, K.; Molven, O.P.K.M.O.; Reit, C. Textbook of Endodontology. In Diagnosis of Pulpal and Periradicular Disease, 1st ed.; Blackwell Publishing Ltd.: Oxford, UK, 2003. [Google Scholar]
- Weber, A.L. Imaging of the paranasal sinuses and oromaxillofacial region imaging of cysts and odontogenic tumors of the jaw. Definition and classification. Radiol. Clin. N. Am. 1993, 31, 101–120. [Google Scholar] [CrossRef] [PubMed]
- Shah, N. Recent advances in imaging technologies in dentistry. World J. Radiol. 2014, 6, 794. [Google Scholar] [CrossRef] [PubMed]
- Musu, D.; Rossi-Fedele, G.; Campisi, G.; Cotti, E. Ultrasonography in the diagnosis of bone lesions of the jaws: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, e19–e29. [Google Scholar] [CrossRef]
- Special Committee to Revise the Joint AAE/AAOMR Position Statement on use of CBCT in Endodontics. AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Chugal, N.; Assad, H.; Markovic, D.; Mallya, S.M. Applying the American Association of Endodontists and American Academy of Oral and Maxillofacial Radiology guidelines for cone-beam computed tomography prescription: Impact on endodontic clinical decisions. J. Am. Dent. Assoc. 2024, 155, 48–58. [Google Scholar] [CrossRef]
- American Association of Endodontists. The Impact of Cone Beam Computer Tomography in Endodontics: A New Era in Diagnosis and Treatment Planning; American Association of Endodontists: Chicago, IL, USA, 2018. [Google Scholar]
- Natkin, R.J.; Oswald, L.; Seattle, W. The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas. Oral Surg. Oral Med. Oral Pathol. 1984, 57, 82–94. [Google Scholar] [CrossRef]
- Valizadeh, S.; Tavakkoli, M.A.; Vasigh, H.K.; Azizi, Z.; Zarrabian, T. Evaluation of Cone Beam Computed Tomography (CBCT) System: Comparison with Intraoral Periapical Radiography in Proximal Caries Detection. J. Dent. Res. Dent. Clin. Dent. Prospect. 2012, 6, 1–5. [Google Scholar] [CrossRef]
- De Vos, W.; Casselman, J.; Swennen, G.R.J. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: A systematic review of the literature. Int. J. Oral Maxillofac. Surg. 2009, 38, 609–625. [Google Scholar] [CrossRef]
- Signorelli, L.; Patcas, R.; Peltomäki, T.; Schätzle, M. Radiation dose of cone-beam computed tomography compared to conventional radiographs in orthodontics. J. Orofac. Orthop. 2016, 77, 9–15. [Google Scholar] [CrossRef]
- Li, G. Patient radiation dose and protection from cone-beam computed tomography. Imaging Sci. Dent. 2013, 43, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Simon, J.H.; Sedghizadeh, P.; Soliman, O.N.; Chapman, T.; Enciso, R. Evaluation of the reliability and accuracy of using cone-beam computed tomography for diagnosing periapical cysts from granulomas. J. Endod. 2013, 39, 1485–1490. [Google Scholar] [CrossRef] [PubMed]
- Theodorakou, C.; Walker, A.; Horner, K.; Pauwels, R.; Bogaerts, R.; Jacobs, R. Estimation of paediatric organ and effective doses from dental cone beam CT using anthropomorphic phantoms. Br. J. Radiol. 2012, 85, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Stokes, K.; Thieme, R.; Jennings, E.; Sholapurkar, A. Cone beam computed tomography in dentistry: Practitioner awareness and attitudes. A scoping review. Aust. Dent. J. 2021, 66, 234–245. [Google Scholar] [CrossRef]
- Kruse, C.; Spin-Neto, R.; Wenzel, A.; Kirkevang, L.L. Cone beam computed tomography and periapical lesions: A systematic review analysing studies on diagnostic efficacy by a hierarchical model. Int. Endod. J. 2015, 48, 815–828. [Google Scholar] [CrossRef]
- Lizio, G.; Salizzoni, E.; Coe, M.; Gatto, M.R.; Asioli, S.; Balbi, T.; Pelliccioni, G.A. Differential diagnosis between a granuloma and radicular cyst: Effectiveness of magnetic resonance imaging. Int. Endod. J. 2018, 51, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, R.E.; Heiland, M.; Bartel-Friedrich, S. Potentials of ultrasound in the diagnosis of midfacial fractures*. Clin. Oral Investig. 2003, 7, 226–229. [Google Scholar] [CrossRef]
- Cotti, E.; Campisi, G. Advanced radiographic techniques for the detection of lesions in bone. Endod. Top. 2004, 7, 52–72. [Google Scholar] [CrossRef]
- Arslan, Z.B.; Demir, H.; Yıldız, D.B.; Yaşar, F. Diagnostic accuracy of panoramic radiography and ultrasonography in detecting periapical lesions using periapical radiography as a gold standard. Dentomaxillofacial Radiol. 2020, 49, 20190290. [Google Scholar] [CrossRef]
- Jia, W.; Jing, H.; Xia, G.; Angang, D.; Wei, Z.; Pengfei, Z.; Shujun, R.; Mengying, M.; Zhengwei, H.; Shensheng, G. Utility of Ultrasonography for Diagnosing and Differentiating Periapical Granuloma from Radicular Cyst. Acad. Radiol. 2023, 30, 2329–2339. [Google Scholar] [CrossRef]
- Abdelsalam, T.A.; Amer, M.E.; Mahrous, A.; Abdelkader, M. Evaluation of oral and maxillofacial swellings using ultrasonographic features. Imaging Sci. Dent. 2019, 49, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Juerchott, A.; Pfefferle, T.; Flechtenmacher, C.; Mente, J.; Bendszus, M.; Heiland, S.; Hilgenfeld, T. Differentiation of periapical granulomas and cysts by using dental MRI: A pilot study. Int. J. Oral Sci. 2018, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Langland, O.E.; Langlais, R.P. Early pioneers of oral and maxiofacial radiology. Oral Surg. Med. Oral Pathol. Oral Radiol. Endod. 1995, 80, 496–511. [Google Scholar] [CrossRef] [PubMed]
- Masthoff, M.; Gerwing, M.; Masthoff, M.; Timme, M.; Kleinheinz, J.; Berninger, M.; Heindel, W.; Wildgruber, M.; Schülke, C. Dental Imaging-A basic guide for the radiologist. RoFo Fortschritte Auf Dem Geb. Rontgenstrahlen Bildgeb. Verfahr. 2019, 191, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Dawood, A.; Whaites, E.; Ford, T.P. New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int. Endod. J. 2009, 42, 447–462. [Google Scholar] [CrossRef] [PubMed]
- Mozzo, P. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Aboudara, C.A.; Hatcher, D.; Nielsen, I.L.; Miller, A. A three-dimensional evaluation of the upper airway in adolescents. Orthod. Craniofac. Res. 2003, 6 (Suppl. 1), 173–175. [Google Scholar] [CrossRef] [PubMed]
- Wanderley, V.A.; Leite, A.F.; de Faria Vasconcelos, K.; Pauwels, R.; Mueller-Garcia, F.; Becker, K.; Oliveira, M.L.; Jacobs, R. Impact of metal artefacts on subjective perception of image quality of 13 CBCT devices. Clin. Oral Investig. 2022, 26, 4457–4466. [Google Scholar] [CrossRef]
- Chan, F.; Brown, L.F.; Parashos, P. CBCT in contemporary endodontics. Aust. Dent. J. 2023, 68, S39–S55. [Google Scholar] [CrossRef]
- Preston, D.L.; Cullings, H.; Suyama, A.; Funamoto, S.; Nishi, N.; Soda, M.; Mabuchi, K.; Kodama, K.; Kasagi, F.; Shore, R.E. Solid Cancer Incidence in Atomic Bomb Survivors Exposed In Utero or as Young Children. J. Natl. Cancer Inst. 2008, 100, 428–436. [Google Scholar] [CrossRef]
- Zielinski, J.M.; Ashmore, P.J.; Band, P.R.; Jiang, H.; Shilnikova, N.S.; Tait, V.K.; Krewski, D. Low dose ionizing radiation exposure and cardiovascular disease mortality: Cohort study based on Canadian national dose registry of radiation workers. Int. J. Occup. Med. Environ. Health 2009, 22, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J.; Brenner, D.J. Cancer risks from diagnostic radiology. Br. J. Radiol. 2008, 81, 362–378. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Doll, R.; Goodhead, D.T.; Hall, E.J.; Land, C.E.; Little, J.B.; Lubin, J.H.; Preston, D.L.; Preston, R.J.; Puskin, J.S.; et al. Cancer Risks Attributable to Low Doses of Ionizing Radiation: Assessing What We Really Know. 2003. Available online: www.pnas.orgcgidoi10.1073pnas.2235592100 (accessed on 10 November 2003).
- Cotti, E.; Campisi, G.; Ambu, R.; Dettori, C. Ultrasound real-time imaging in the differential diagnosis of periapical lesions. Int. Endod. J. 2003, 36, 556–563. [Google Scholar] [CrossRef]
- Cotti, E.; Campisi, G.; Garau, V.; Puddu, G. A new technique for the study of periapical bone lesions: Ultrasound real time imaging. Int. Endod. J. 2002, 35, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Raghav, N.; Reddy, S.S.; Giridhar, A.G.; Murthy, S.; Devi, B.Y.; Santana, N.; Rakesh, N.; Kaushik, A. Comparison of the efficacy of conventional radiography, digital radiography, and ultrasound in diagnosing periapical lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2010, 110, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.L.D.; Costa, A.L.F.; Tucunduva, M.J.A.; Tucunduva-Neto, R.R.; Shinohara, E.H.; de Freitas, C.F. Ultrasound evaluation of intra-osseous cavity: A preliminary study in pig mandibles. J. Oral Biol. Craniofac. Res. 2016, 6, S14–S17. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Jacobs, R.; Levring Jäghagen, E.; Lindh, C.; Baksi, G.; Schulze, D.; Schulze, R. Basic training requirements for the use of dental CBCT by dentists: A position paper prepared by the European Academy of Dento Maxillo Facial Radiology. Dentomaxillofacial Radiol. 2014, 43, 20130291. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef]
- Protection Radiation No 172. Cone Beam CT for Dental and Maxillofacial Radiology (Evidence-Based Guidelines). Available online: www.sedentexct.eu (accessed on 12 March 2012).
- Avcı, F.; Etöz, M.; Üstün, Y.; Arslan, T. Evaluation of ultrasonography as a diagnostic tool in the management of periapical cysts and granulomas: A clinical study. Imaging Sci. Dent. 2022, 52, 209. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incisors N (%) | Canines N (%) | Premolars N (%) | Total N (%) | |
|---|---|---|---|---|
| Mandibular | 6 (14%) | 0 (0%) | 1 (2%) | 7 (16%) |
| Maxillary | 29 (68%) | 4 (9%) | 3 (7%) | 36 (84%) |
| Total | 35 (82%) | 4 (9%) | 4 (9%) | 43 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karkle, A.; Slaidina, A.; Zolovs, M.; Vaskevica, A.; Meistere, D.; Bokvalde, Z.; Neimane, L. Comparative Analysis of Examination Methods for Periapical Lesion Diagnostics: Assessing Cone-Beam Computer Tomography, Ultrasound, and Periapical Radiography. Diagnostics 2024, 14, 766. https://doi.org/10.3390/diagnostics14070766
Karkle A, Slaidina A, Zolovs M, Vaskevica A, Meistere D, Bokvalde Z, Neimane L. Comparative Analysis of Examination Methods for Periapical Lesion Diagnostics: Assessing Cone-Beam Computer Tomography, Ultrasound, and Periapical Radiography. Diagnostics. 2024; 14(7):766. https://doi.org/10.3390/diagnostics14070766
Chicago/Turabian StyleKarkle, Aleksandra, Anda Slaidina, Maksims Zolovs, Anete Vaskevica, Dita Meistere, Zanda Bokvalde, and Laura Neimane. 2024. "Comparative Analysis of Examination Methods for Periapical Lesion Diagnostics: Assessing Cone-Beam Computer Tomography, Ultrasound, and Periapical Radiography" Diagnostics 14, no. 7: 766. https://doi.org/10.3390/diagnostics14070766
APA StyleKarkle, A., Slaidina, A., Zolovs, M., Vaskevica, A., Meistere, D., Bokvalde, Z., & Neimane, L. (2024). Comparative Analysis of Examination Methods for Periapical Lesion Diagnostics: Assessing Cone-Beam Computer Tomography, Ultrasound, and Periapical Radiography. Diagnostics, 14(7), 766. https://doi.org/10.3390/diagnostics14070766