
Utility of Dual-Energy Computed Tomography in Clinical Conundra

 , , , ,
, , , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Principles of Attenuation
3. Principles of DECT
4. DECT Systems
4.1. Dual-Source
4.2. Single-Source with Fast Kilovoltage Switching
4.3. Single-Source with Dual-Layer Detector
4.4. Single-Source with Twin-Beam Filtration
4.5. Single-Source with Sequential (Dual-Spin) Acquisition
5. DECT Applications
5.1. Examples in the Gastrointestinal System
5.1.1. Bowel
5.1.2. Appendix
5.2. Examples in the Genitourinary System
5.2.1. Urolithiasis
5.2.2. Inflammation, Neoplasm and Hemorrhage
5.3. Examples in the Biliary System
5.3.1. Cholelithiasis
5.3.2. Cholecystitis
5.4. Examples in the Musculoskeletal System
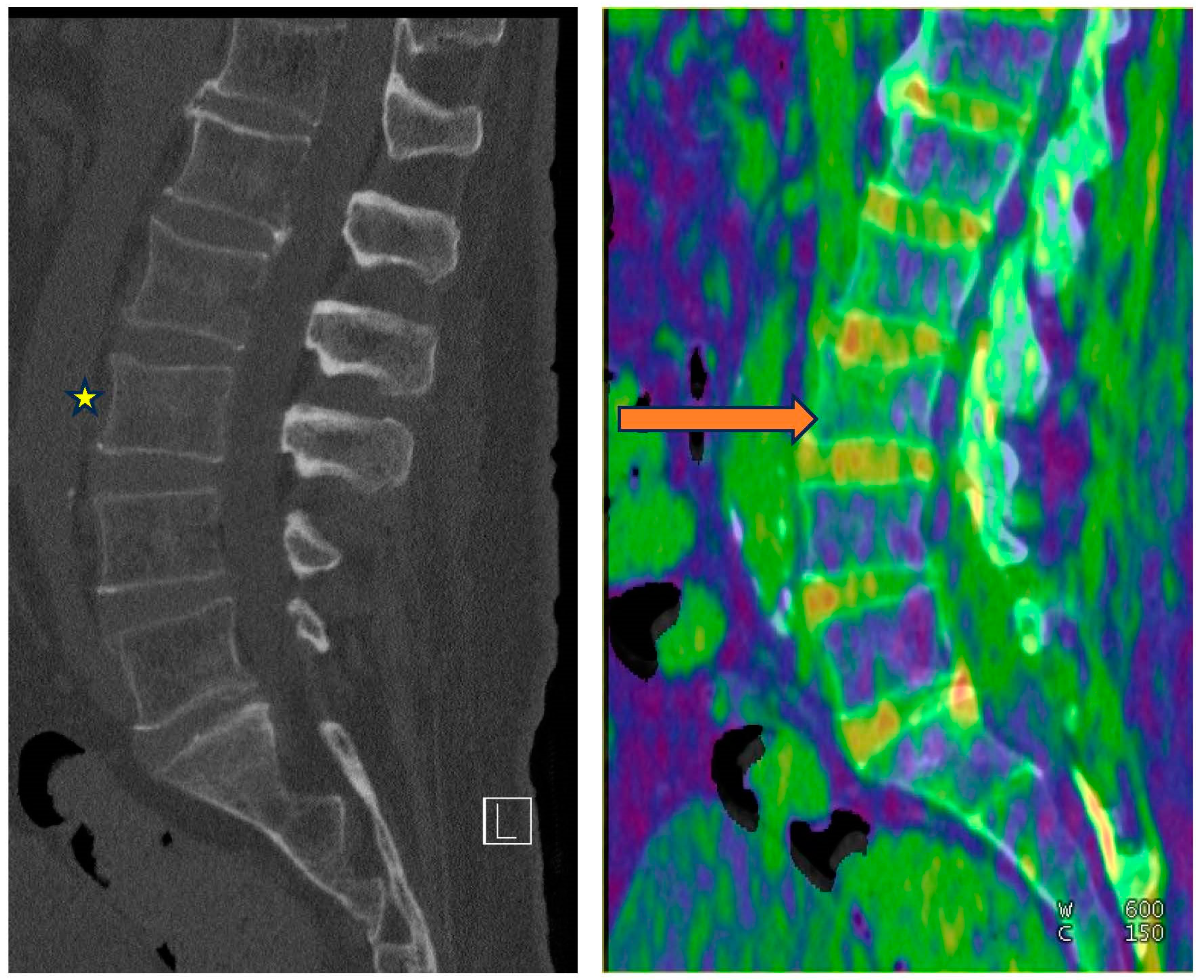
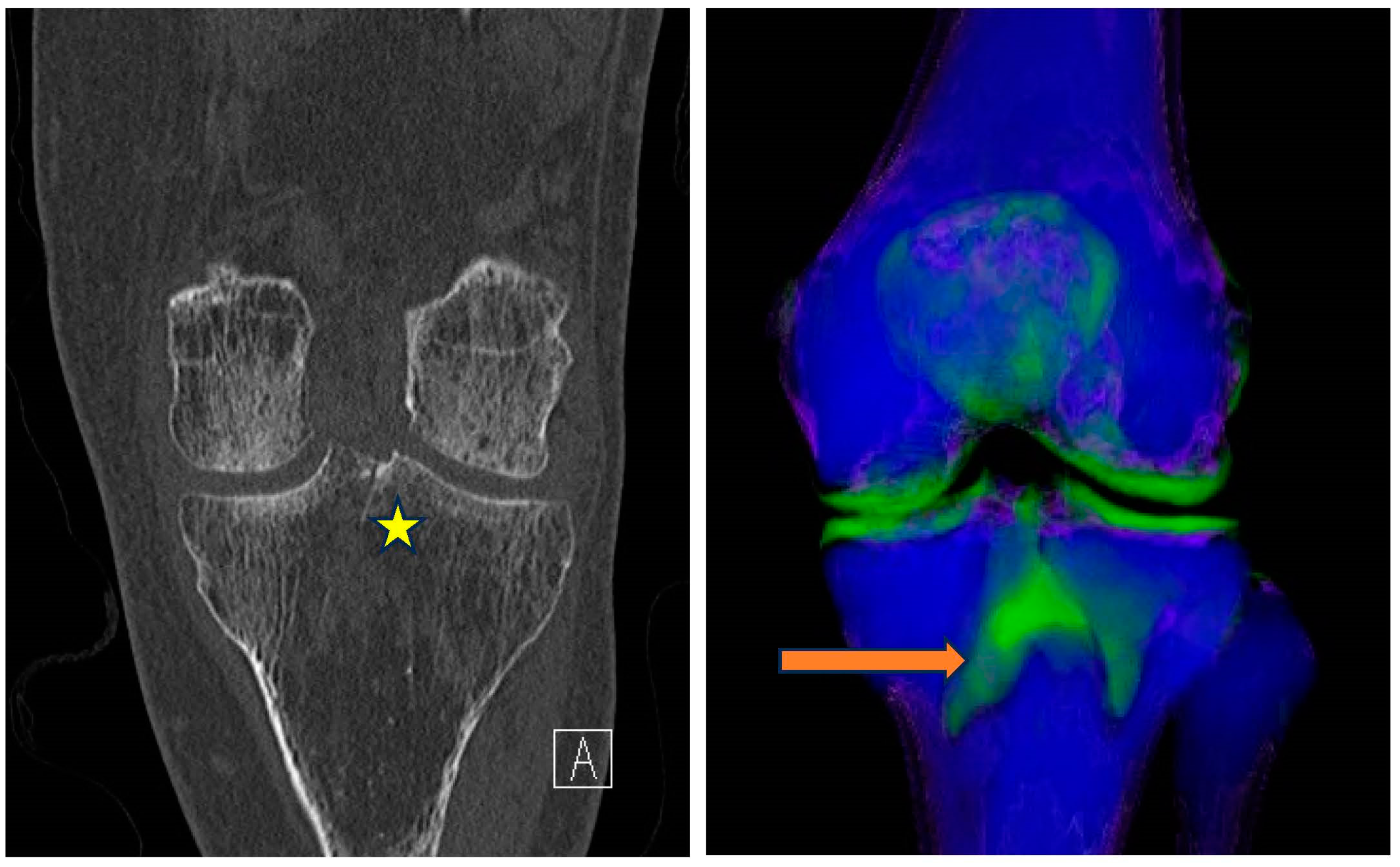
5.4.1. Bone Marrow Edema (BME)
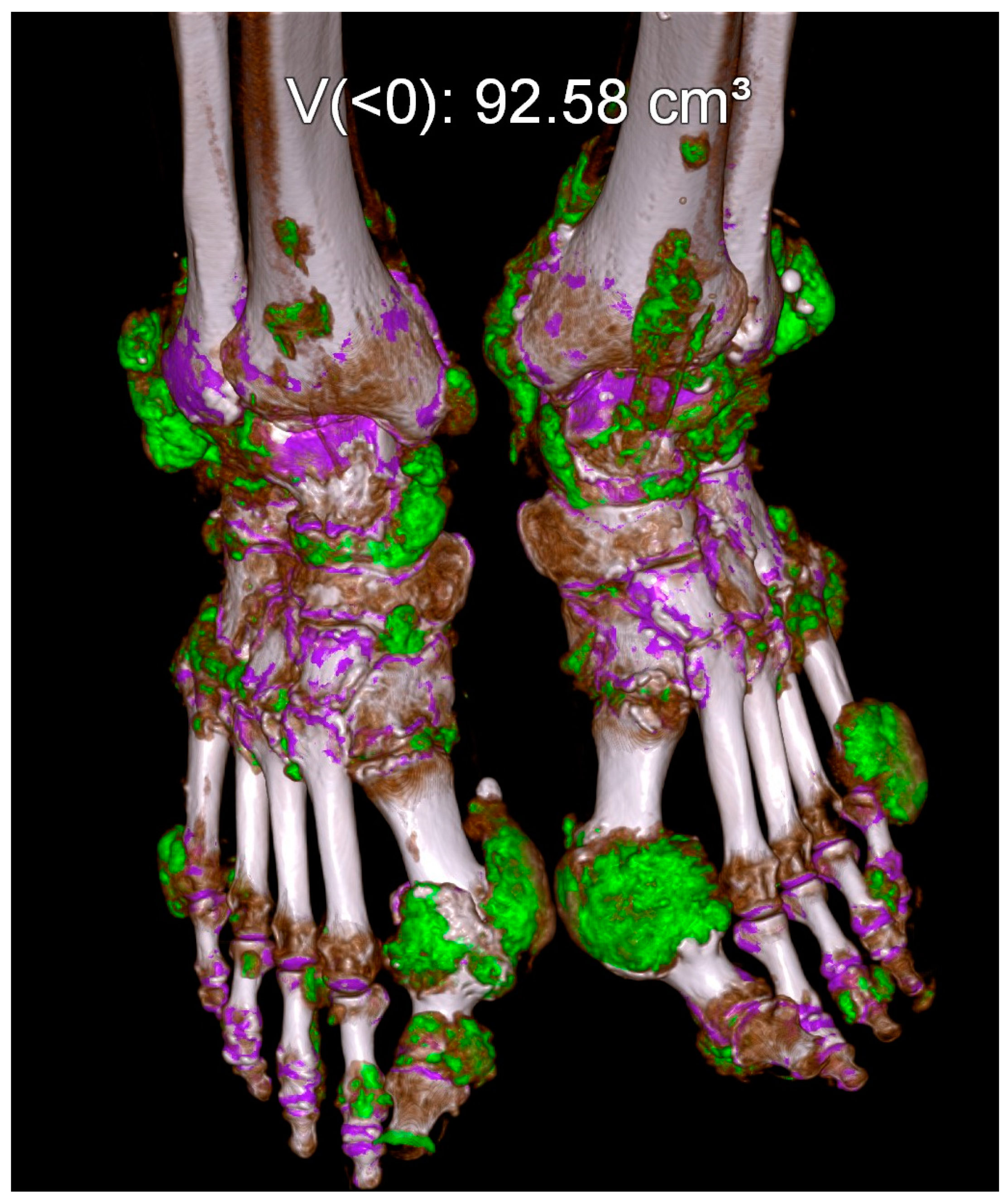
5.4.2. Gout
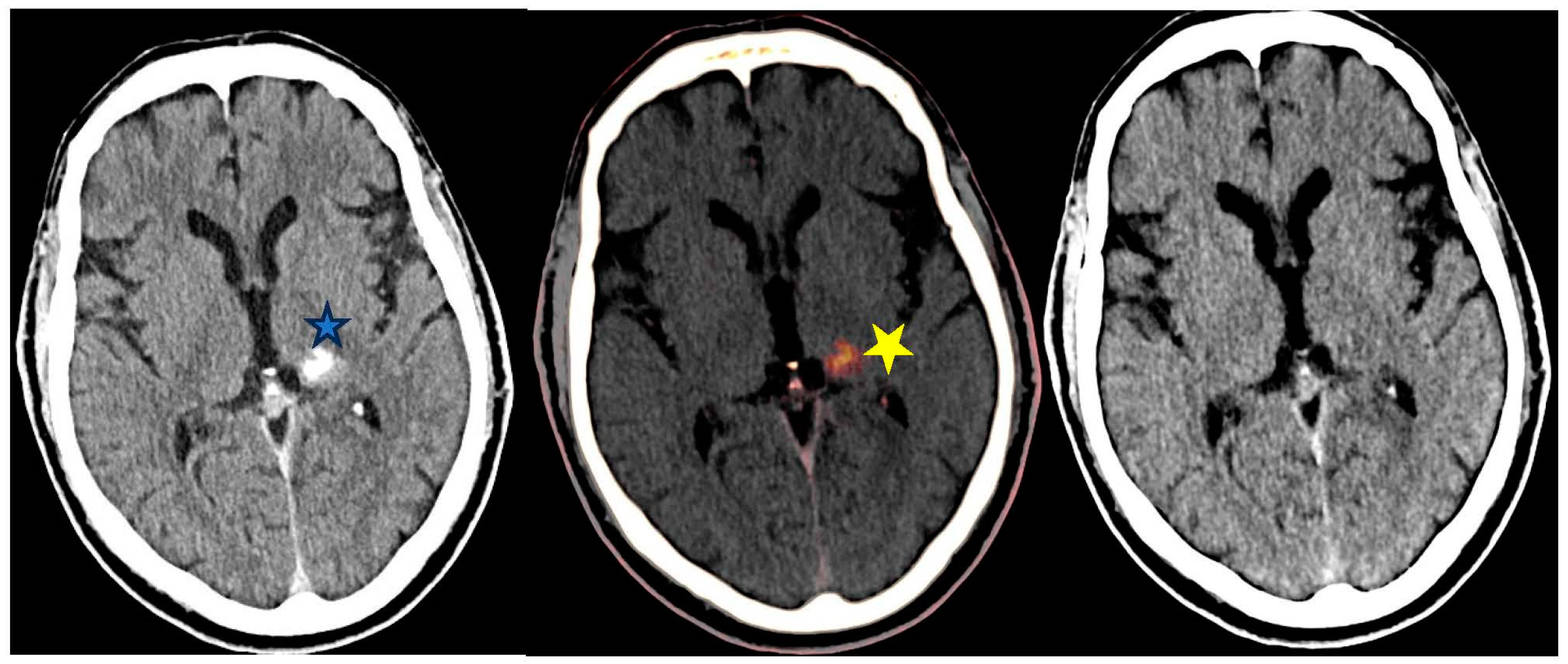
5.5. Examples in Neuroradiology
Post Endovascular Thrombectomy (EVT)
5.6. Pulmonary Examples
5.7. Cardiac Evaluation
5.8. Vascular Examples
5.9. Oncology Examples
6. Challenges and Pitfalls
7. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Stoker, J.; van Randen, A.; Laméris, W.; Boermeester, M.A. Imaging patients with acute abdominal pain. Radiology 2009, 253, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Coursey, C.A.; Nelson, R.C.; Boll, D.T.; Paulson, E.K.; Ho, L.M.; Neville, A.M.; Marin, D.; Gupta, R.T.; Schindera, S.T. Dual-energy multidetector CT: How does it work, what can it tell us, and when can we use it in abdominopelvic imaging? Radiographics 2010, 30, 1037–1055. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.F.; Fischer, R.H.; Novelline, R.A.; Kim, J.; Nagurney, J.T. The role of abdominal computed tomography scanning in patients with non-traumatic abdominal symptoms. Eur. J. Emerg. Med. 2002, 9, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Macari, M.; Spieler, B.; Kim, D.; Graser, A.; Megibow, A.J.; Babb, J.; Chandarana, H. Dual-source dual-energy MDCT of pancreatic adenocarcinoma: Initial observations with data generated at 80 kVp and at simulated weighted-average 120 kVp. Am. J. Roentgenol. 2010, 194, W27–W32. [Google Scholar] [CrossRef] [PubMed]
- Bushberg, J.T.; Seibert, J.A.; Leidholdt, E.M., Jr.; Boone, J.M. The Essential Physics of Medical Imaging, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Gupta, A.K.; Chowdhury, V.; Khandelwal, N. (Eds.) Diagnostic Radiology: Recent Advances and Applied Physics in Imaging, 2nd ed.; Jaypee Brothers Medical: New Delhi, India, 2013. [Google Scholar]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G.; Jacobsen, M.C.; Schellingerhout, D.; Wood, C.A.; Tamm, E.P.; Godoy, M.C.; Sun, J.; et al. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.J.; Kaza, R.K.; Bolus, D.N.; Boll, D.T.; Rofsky, N.M.; De Cecco, C.N.; Foley, W.D.; Morgan, D.E.; Schoepf, U.J.; Sahani, D.V.; et al. White paper of the Society of Computed Body Tomography and Magnetic Resonance on dual-energy CT, Part 1: Technology and terminology. J. Comput. Assist. Tomogr. 2016, 40, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Tatsugami, F.; Higaki, T.; Nakamura, Y.; Honda, Y.; Awai, K. Dual-energy CT: Minimal essentials for radiologists. Jpn. J. Radiol. 2022, 40, 547–559. [Google Scholar] [CrossRef] [PubMed]
- Toia, G.V.; Mileto, A.; Wang, C.L.; Sahani, D.V. Quantitative dual-energy CT techniques in the abdomen. Abdom. Imaging 2021, 47, 3003–3018. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.; Darras, K.E.; Walstra, F.E.; Mohammed, M.F.; McLaughlin, P.D.; Nicolaou, S. Dual-Energy CT in Evaluation of the Acute Abdomen. RadioGraphics 2019, 39, 264–286. [Google Scholar] [CrossRef]
- Graser, A.; Johnson, T.R.; Hecht, E.M.; Becker, C.R.; Leidecker, C.; Staehler, M.; Stief, C.G.; Hildebrandt, H.; Godoy, M.C.B.; Finn, M.E.; et al. Dual-energy CT in patients suspected of having renal masses: Can virtual nonenhanced images replace true nonenhanced images? Radiology 2009, 252, 433–440. [Google Scholar] [CrossRef]
- Vlahos, I.; Godoy, M.C.; Naidich, D.P. Dual-energy computed tomography imaging of the aorta. J. Thorac. Imaging 2010, 25, 289–300. [Google Scholar] [CrossRef]
- Rajiah, P.; Parakh, A.; Kay, F.; Baruah, D.; Kambadakone, A.R.; Leng, S. Update on multienergy CT: Physics, principles, and applications. RadioGraphics 2020, 40, 1284–1308. [Google Scholar] [CrossRef] [PubMed]
- Baliyan, V.; Shaqdan, K.; Hedgire, S.; Ghoshhajra, B. Vascular computed tomography angiography technique and indications. Cardiovasc. Diagn. Ther. 2019, 9 (Suppl. S1), S14–S27. [Google Scholar] [CrossRef]
- Sun, H.; Hou, X.-Y.; Xue, H.-D.; Li, X.-G.; Jin, Z.-Y.; Qian, J.-M.; Yu, J.-C.; Zhu, H.-D. Dual-source dual-energy CT angiography with virtual non-enhanced images and iodine map for active gastrointestinal bleeding: Image quality, radiation dose and diagnostic performance. Eur. J. Radiol. 2015, 84, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Stolzmann, P.; Frauenfelder, T.; Pfammatter, T.; Peter, N.; Scheffel, H.; Lachat, M.; Schmidt, B.; Marincek, B.; Alkadhi, H.; Schertler, T. Endoleaks after endovascular abdominal aortic aneurysm repair: Detection with dual-energy dual-source CT. Radiology 2008, 249, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Chandarana, H.; Godoy, M.C.B.; Vlahos, I.; Graser, A.; Babb, J.; Leidecker, C.; Macari, M. Abdominal aorta: Evaluation with dual-source dual-energy multidetector CT after endovascular repair of aneurysms—Initial observations. Radiology 2008, 249, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.M.; Yoshizumi, T.T.; Hurwitz, L.M.; Nelson, R.C.; Marin, D.; Toncheva, G.; Schindera, S.T. Dual energy versus single energy MDCT: Measurement of radiation dose using adult abdominal imaging protocols. Acad. Radiol. 2009, 16, 1400–1407. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.; Dane, B.; Yeh, B.M.; Morgan, D.E.; Sahani, D.V.; Kambadakone, A. Dual-energy computed tomography: Technological considerations. Radiol. Clin. N. Am. 2023, 61, 945–961. [Google Scholar] [CrossRef]
- Megibow, A.J.; Sahani, D. Best practice: Implementation and use of abdominal dual-energy CT in routine patient care. Am. J. Roentgenol. 2012, 199 (Suppl. S5), S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.D.; Oliveira, G.R.; Kalva, S.P.; Pinho, D.F.; Arellano, R.S.; Sahani, D.V. Prospective comparison of reduced-iodine-dose virtual monochromatic imaging dataset from dual-energy CT angiography with standard-iodine-dose single-energy CT angiography for abdominal aortic aneurysm. Am. J. Roentgenol. 2016, 207, W125–W132. [Google Scholar] [CrossRef] [PubMed]
- Pinho, D.F.; Kulkarni, N.M.; Krishnaraj, A.; Kalva, S.P.; Sahani, D.V. Initial experience with single-source dual-energy CT abdominal angiography and comparison with single-energy CT angiography: Image quality, enhancement, diagnosis and radiation dose. Eur. Radiol. 2013, 23, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Patino, M.; Parakh, A.; Lo, G.C.; Agrawal, M.; Kambadakone, A.R.; Oliveira, G.R.; Sahani, D.V. Virtual monochromatic dual-energy aortoiliac CT angiography with reduced iodine dose: A prospective randomized study. Am. J. Roentgenol. 2019, 212, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Shuman, W.P.; Chan, K.T.; Busey, J.M.; Mitsumori, L.M.; Koprowicz, K.M. Dual-energy CT aortography with 50% reduced iodine dose versus single-energy CT aortography with standard iodine dose. Acad. Radiol. 2016, 23, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Shuman, W.P.; Mileto, A.; Busey, J.M.; Desai, N.; Koprowicz, K.M. Dual-energy CT Urography with 50% reduced iodine dose versus single-energy CT urography with standard iodine dose. Am. J. Roentgenol. 2019, 212, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Rotzinger, D.C.; Si-Mohamed, S.A.; Yerly, J.; Boccalini, S.; Becce, F.; Boussel, L.; Meuli, R.A.; Qanadli, S.D.; Douek, P.C. Reduced-iodine-dose dual-energy coronary CT angiography: Qualitative and quantitative comparison between virtual monochromatic and polychromatic CT images. Eur. Radiol. 2021, 31, 7132–7142. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.P.; Antunes, C.; Curvo-Semedo, L. Pros and Cons of Dual-Energy CT Systems: “One Does Not Fit All”. Tomography 2023, 9, 195–216. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Pomerleau, M.; Gupta, A.; Soto, J.A.; Anderson, S.W. Accuracy of dual-energy CT virtual unenhanced and material-specific images: A phantom study. Am. J. Roentgenol. 2020, 215, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Abu-Omar, A.; Murray, N.; Ali, I.T.; Khosa, F.; Barrett, S.; Sheikh, A.; Nicolaou, S.; O’neill, S.B. The Role of Dual-Energy CT in Solid Organ Injury. Can. Assoc. Radiol. J. 2023, 8465371231215669, online ahead of print. [Google Scholar] [CrossRef]
- Forghani, R.; De Man, B.; Gupta, R. Dual-energy computed tomography: Physical principles, approaches to scanning, usage, and implementation: Part 1. Neuroimaging Clin. N. Am. 2017, 27, 371–384. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Nicolaou, S. Spectral computed tomography: Fundamental principles and recent developments. Korean J. Radiol. 2021, 22, 86–96. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Boedeker, K.; Cody, D.; Duan, X.; Flohr, T.; Halliburton, S.S.; Hsieh, J.; Layman, R.R.; Pelc, N.J. Principles and applications of multienergy CT: Report of AAPM task group 291. Med. Phys. 2020, 47, e881–e912. [Google Scholar] [CrossRef] [PubMed]
- Agostini, A.; Borgheresi, A.; Mari, A.; Floridi, C.; Bruno, F.; Carotti, M.; Schicchi, N.; Barile, A.; Maggi, S.; Giovagnoni, A. Dual-energy CT: Theoretical principles and clinical applications. Radiol. Med. 2019, 124, 1281–1295. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.R.C. Dual-energy CT: General principles. Am. J. Roentgenol. 2012, 199 (Suppl. S5), S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Fulwadhva, U.P.; Wortman, J.R.; Sodickson, A.D. Use of dual-energy CT and iodine maps in evaluation of bowel disease. RadioGraphics 2016, 36, 393–406. [Google Scholar] [CrossRef]
- Lee, S.M.; Kim, S.H.; Ahn, S.J.; Kang, H.J.; Kang, J.H.; Han, J.K. Virtual monoenergetic dual-layer, dual-energy CT enterog-raphy: Optimization of keV settings and its added value for Crohn’s disease. Eur. Radiol. 2018, 28, 2525–2534. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.A.; Collins, J.M.; Olden, K.W. Spontaneous intramural small-bowel hematoma: Imaging findings and outcome. Am. J. Roentgenol. 2002, 179, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Im, A.L.; Lee, Y.H.; Bang, D.H.; Yoon, K.H.; Park, S.H. Dual energy CT in patients with acute abdomen: Is it possible for virtual non-enhanced images to replace true non-enhanced images? Emerg. Radiol. 2013, 20, 475–483. [Google Scholar] [CrossRef]
- Niemann, T.; Kollmann, T.; Bongartz, G. Diagnostic performance of low-dose CT for the detection of urolithiasis: A meta-analysis. Am. J. Roentgenol. 2008, 191, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.; Sindel, T.; Arslan, G.; Özkaynak, C.; Karaali, K.; Kabaalioğlu, A.; Lüleci, E. Renal colic: Comparison of spiral CT, US and IVU in the detection of ureteral calculi. Eur. Radiol. 1998, 8, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Long, B.; Koyfman, A. The evaluation and management of urolithiasis in the ED: A review of the literature. Am. J. Emerg. Med. 2018, 36, 699–706. [Google Scholar] [CrossRef]
- Abou-Elela, A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review. J. Adv. Res. 2017, 8, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Kambadakone, A.R.; Eisner, B.H.; Catalano, O.A.; Sahani, D.V. New and evolving concepts in the imaging and management of urolithiasis: Urologists’ perspective. RadioGraphics 2010, 30, 603–623. [Google Scholar] [CrossRef] [PubMed]
- Motley, G.; Dalrymple, N.; Keesling, C.; Fischer, J.; Harmon, W. Hounsfield unit density in the determination of urinary stone composition. Urology 2001, 58, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Stolzmann, P.; Kozomara, M.; Chuck, N.; Müntener, M.; Leschka, S.; Scheffel, H.; Alkadhi, H. In vivo identification of uric acid stones with dual-energy CT: Diagnostic performance evaluation in patients. Abdom. Imaging 2010, 35, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Graser, A.; Johnson, T.R.C.; Bader, M.; Staehler, M.; Haseke, N.; Nikolaou, K.; Reiser, M.F.; Stief, C.G.; Becker, C.R. Dual energy CT characterization of urinary calculi: Initial in vitro and clinical experience. Investig. Radiol. 2008, 43, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Mangold, S.; Thomas, C.; Fenchel, M.; Vuust, M.; Krauss, B.; Ketelsen, D.; Tsiflikas, I.; Claussen, C.D.; Heuschmid, M. Virtual nonenhanced dual-energy CT urography with tin-filter technology: Determinants of detection of urinary calculi in the renal collecting system. Radiology 2012, 264, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.W.; Park, B.K.; Kim, C.K.; Park, S.Y. Evaluation of virtual unenhanced CT obtained from dual-energy CT urography for detecting urinary stones. Br. J. Radiol. 2012, 85, e176–e181. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Davis, D.; Choudhury, K.R.; Patel, B.; Gupta, R.T.; Mileto, A.; Nelson, R.C. Characterization of small focal renal lesions: Diagnostic accuracy with single-phase contrast-enhanced dual-energy CT with material attenuation analysis compared with conventional attenuation measurements. Radiology 2017, 284, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Bova, J.G.; Schwesinger, W.H.; Kurtin, W.E. In vivo analysis of gallstone composition by computed tomography. Gastrointest. Radiol. 1992, 17, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.P.; Darras, K.E.; Nicolaou, S.; McLaughlin, P.D. Emergency abdominal applications of DECT. Curr. Radiol. Rep. 2016, 4, 54. Available online: https://link.springer.com/article/10.1007/s40134-016-0177-5 (accessed on 26 March 2024).
- Yang, C.-B.; Zhang, S.; Jia, Y.-J.; Duan, H.-F.; Ma, G.-M.; Zhang, X.-R.; Yu, Y.; He, T.-P. Clinical application of dual-energy spectral computed tomography in detecting cholesterol gallstones from surrounding bile. Acad. Radiol. 2017, 24, 478–482. [Google Scholar] [CrossRef]
- Li, H.; He, D.; Lao, Q.; Chen, X.; Liu, M.; Yin, B.; Zhao, K.; Wang, R.; Chen, L. Clinical value of spectral CT in diagnosis of negative gallstones and common bile duct stones. Abdom. Imaging 2015, 40, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.C.; Morse, B.G.; Hara, A.K.; Paden, R.G.; Hongo, N.; Pavlicek, W. Dual-energy (spectral) CT: Applications in abdominal imaging. RadioGraphics 2011, 31, 1031–1046; discussion 1047–1050. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Kukla, C.; Breitenseher, M.; Trattnig, S.; Mittlboeck, M.; Vecsei, V. Magnetic resonance imaging of occult scaphoid fractures. J. Trauma 1996, 41, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, S.; Mutlu, H.; Kömür, B.; Guler, O.; Yucel, B.; Parmaksızoğlu, A. Magnetic Resonance imaging-based diagnosis of occult osseous injuries in traumatic knees. Open Orthop. J. 2015, 9, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Wong, M.; Kutschera, P.; Lau, K. Dual-energy CT in musculoskeletal trauma. Clin. Radiol. 2021, 76, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Al-Arfaj, A.M.; Eftekhari, A.; Munk, P.L.; Shojania, K.; Reid, G.; Nicolaou, S. Dual energy computed tomography in tophaceous gout. Ann. Rheum. Dis. 2009, 68, 1609–1612. [Google Scholar] [CrossRef]
- Choi, H.K.; Burns, L.C.; Shojania, K.; Koenig, N.; Reid, G.; Abufayyah, M.; Law, G.; Kydd, A.S.; Ouellette, H.; Nicolaou, S. Dual energy CT in gout: A prospective validation study. Ann. Rheum. Dis. 2012, 71, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Choi, H.K. Dual-energy computed tomography for gout diagnosis and management. Curr. Rheumatol. Rep. 2013, 15, 301. [Google Scholar] [CrossRef]
- Neogi, T.; A. Jansen, T.L.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Rajiah, P.; Sundaram, M.; Subhas, N. Dual-Energy CT in Musculoskeletal Imaging: What Is the Role Beyond Gout? Am. J. Roentgenol. 2019, 213, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; E House, M.; Aati, O.; Tan, P.; Franklin, C.; Horne, A.; Gamble, G.D.; Stamp, L.K.; Doyle, A.J.; McQueen, F.M. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: A dual energy CT study. Ann. Rheum. Dis. 2015, 74, 908–911. [Google Scholar] [CrossRef]
- Saini, V.; Guada, L.; Yavagal, D.R. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology 2021, 97, S6–S16. [Google Scholar] [CrossRef] [PubMed]
- Wassélius, J.; Arnberg, F.; von Euler, M.; Wester, P.; Ullberg, T. Endovascular Thrombectomy for Acute Ischemic Stroke. J. Int. Med. 2022, 291, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Perrella, A.; Bagnacci, G.; Di Meglio, N.; Di Martino, V.; Mazzei, M.A. Thoracic Diseases: Technique and Applications of Dual-Energy CT. Diagnostics 2023, 13, 2440. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, H.; Takayanagi, T.; Ishikawa, T.; Katada, Y.; Fukui, R.; Yamamoto, Y.; Suzuki, S. New Fast kVp Switching Dual-Energy CT: Reduced Severity of Beam Hardening Artifacts and Improved Image Quality in Reduced-Iodine Virtual Monochromatic Imaging. Acad. Radiol. 2020, 27, 1586–1593. [Google Scholar] [CrossRef]
- Mellander, H.; Fransson, V.; Ydström, K.; Lätt, J.; Ullberg, T.; Wassélius, J.; Ramgren, B. Metal artifact reduction by virtual monoenergetic reconstructions from spectral brain CT. Eur. J. Radiol. Open 2023, 10, 100479. [Google Scholar] [CrossRef] [PubMed]
- McComiskey, D.M.; Erdenebold, U.-E.M.; McInnes, M.D.M.; Salameh, J.-P.M.; Chatelain, R.R.; Torres, C.M.; Chakraborty, S.M.; Zakhari, N.M. The Impact of Virtual Monoenergetic Imaging on Visualization of the Cervical Spinal Canal. J. Comput. Assist. Tomogr. 2023, 47, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Thieme, S.F.; Johnson, T.R.C.; Lee, C.; McWilliams, J.; Becker, C.R.; Reiser, M.F.; Nikolaou, K. Dual-energy CT for the assessment of contrast material distribution in the pulmonary parenchyma. Am. J. Roentgenol. 2009, 193, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Pontana, F.; Faivre, J.-B.; Remy-Jardin, M.; Flohr, T.; Schmidt, B.; Tacelli, N.; Pansini, V.; Remy, J. Lung perfusion with dual-energy multidetector-row CT (MDCT): Feasibility for the evaluation of acute pulmonary embolism in 117 consecutive patients. Acad. Radiol. 2008, 15, 1494–1504. [Google Scholar] [CrossRef] [PubMed]
- Thieme, S.F.; Hoegl, S.; Nikolaou, K.; Fisahn, J.; Irlbeck, M.; Maxien, D.; Reiser, M.F.; Becker, C.R.; Johnson, T.R.C. Pulmonary ventilation and perfusion imaging with dual-energy CT. Eur. Radiol. 2010, 20, 2882–2889. [Google Scholar] [CrossRef] [PubMed]
- Geyer, L.L.; Scherr, M.; Körner, M.; Wirth, S.; Deak, P.; Reiser, M.F.; Linsenmaier, U. Imaging of acute pulmonary embolism using a dual energy CT system with rapid kVp switching: Initial results. Eur. J. Radiol. 2012, 81, 3711–3718. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.; Johnson, T.R.; Michaely, H.J.; Morhard, D.; Becker, C.; Reiser, M.; Nikolaou, K. Dual-energy CT angiography of the lung in patients with suspected pulmonary embolism: Initial results. RöFo 2008, 180, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Leithner, D.; Wichmann, J.L.; Vogl, T.J.; Trommer, J.; Martin, S.S.; Scholtz, J.-E.; Bodelle, B.; De Cecco, C.N.; Duguay, T.; Nance, J.W.; et al. Virtual monoenergetic imaging and iodine perfusion maps improve diagnostic accuracy of dual-energy computed tomography pulmonary angiography with suboptimal contrast attenuation. Investig. Radiol. 2017, 52, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Sudarski, S.; Hagelstein, C.; Weis, M.; Schoenberg, S.O.; Apfaltrer, P. Dual-energy snap-shot perfusion CT in suspect pulmonary nodules and masses and for lung cancer staging. Eur. J. Radiol. 2015, 84, 2393–2400. [Google Scholar] [CrossRef]
- Forghani, R.; Levental, M.; Gupta, R.; Lam, S.; Dadfar, N.; Curtin, H. Different spectral hounsfield unit curve and high-energy virtual monochromatic image characteristics of squamous cell carcinoma compared with nonossified thyroid cartilage. Am. J. Neuroradiol. 2015, 36, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Frellesen, C.; Kaup, M.; Wichmann, J.L.; Hüsers, K.; Scholtz, J.-E.; Albrecht, M.H.; Metzger, S.C.; Bauer, R.W.; Kerl, J.M.; Lehnert, T.; et al. Noise-optimized advanced image-based virtual monoenergetic imaging for improved visualization of lung cancer: Comparison with traditional virtual monoenergetic imaging. Eur. J. Radiol. 2016, 85, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.; Tan, T.C. Dual-phase computed tomography imaging in acute chest pain: Emerging protocols and potential future implications. Eur. Hear. J. Case Rep. 2021, 5, ytab178. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.H.; De Cecco, C.N.; Schoepf, U.J.; Spandorfer, A.; Eid, M.; De Santis, D.; Varga-Szemes, A.; van Assen, M.; von Knebel-Doeberitz, P.L.; Tesche, C.; et al. Dual-energy CT of the heart current and future status. Eur. J. Radiol. 2018, 105, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Varga-Szemes, A.; Meinel, F.G.; De Cecco, C.N.; Fuller, S.R.; Bayer, R.R.; Schoepf, U.J. CT myocardial perfusion imaging. Am. J. Roentgenol. 2014, 204, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.H.; Scholtz, J.-E.; Hüsers, K.; Beeres, M.; Bucher, A.M.; Kaup, M.; Martin, S.S.; Fischer, S.; Bodelle, B.; Bauer, R.W.; et al. Advanced image-based virtual monoenergetic dual-energy CT angiography of the abdomen: Optimization of kiloelectron volt settings to improve image contrast. Eur. Radiol. 2016, 26, 1863–1870. [Google Scholar] [CrossRef]
- Kumar, V.; Min, J.K.; He, X.; Raman, S.V. Computation of calcium score with dual-energy computed tomography: A phantom study. J. Comput. Assist. Tomogr. 2017, 41, 156–158. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Schoepf, U.J.; Steinbach, L.; Boll, D.T.; Foley, W.D.; Kaza, R.K.; Bolus, D.N.; Morgan, D.E.; Sahani, D.V.; Shuman, W.P.; et al. White paper of the society of computed body tomography and magnetic resonance on dual-energy CT, part 3: Vascular, cardiac, pulmonary, and musculoskeletal applications. J. Comput. Assist. Tomogr. 2017, 41, 1–7. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Harris, B.S.; Schoepf, U.J.; Silverman, J.R.; McWhite, C.B.; Krazinski, A.W.; Bayer, R.R.; Meinel, F.G. Incremental value of pharmacological stress cardiac dual-energy CT over coronary CT angiography alone for the assessment of coronary artery disease in a high-risk population. Am. J. Roentgenol. 2014, 203, W70–W77. [Google Scholar] [CrossRef] [PubMed]
- Weininger, M.; Schoepf, U.J.; Ramachandra, A.; Fink, C.; Rowe, G.W.; Costello, P.; Henzler, T. Adenosine-stress dynamic real-time myocardial perfusion CT and adenosine-stress first-pass dual-energy myocardial perfusion CT for the assessment of acute chest pain: Initial results. Eur. J. Radiol. 2012, 81, 3703–3710. [Google Scholar] [CrossRef] [PubMed]
- Ruzsics, B.; Lee, H.; Zwerner, P.L.; Gebregziabher, M.; Costello, P.; Schoepf, U.J. Dual-energy CT of the heart for diagnosing coronary artery stenosis and myocardial ischemia-initial experience. Eur. Radiol. 2008, 18, 2414–2424. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Yu, W.; Wang, Y.; He, Y.; Yang, L.; Bi, T.; Jiao, J.; Wang, Q.; Chi, L.; Yu, Y.; et al. Incremental value of dual-energy CT to coronary CT angiography for the detection of significant coronary stenosis: Comparison with quantitative coronary angiography and single photon emission computed tomography. Int. J. Cardiovasc. Imaging 2011, 27, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, J.L.; Bauer, R.W.; Doss, M.; Stock, W.; Lehnert, T.; Bodelle, B.; Frellesen, C.; Vogl, T.J.; Kerl, J.M. Diagnostic accuracy of late iodine–enhancement dual-energy computed tomography for the detection of chronic myocardial infarction compared with late gadolinium–enhancement 3-T magnetic resonance imaging. Investig. Radiol. 2013, 48, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Deseive, S.; Bauer, R.W.; Lehmann, R.; Kettner, M.; Kaiser, C.; Korkusuz, H.; Christa, T.; Alf, T.; Volker, S.; Joseph, S.U.; et al. Dual-energy computed tomography for the detection of late enhancement in reperfused chronic infarction: A comparison to magnetic resonance imaging and histopathology in a porcine model. Investig. Radiol. 2011, 46, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Meinel, F.G.; De Cecco, C.N.; Schoepf, U.J.; Nance, J.W., Jr.; Silverman, J.R.; Flowers, B.A.; Henzler, T. First–arterial-pass dual-energy CT for assessment of myocardial blood supply: Do We need rest, stress, and delayed acquisition? Comparison with SPECT. Radiology 2014, 270, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Beeres, M.; Trommer, J.; Frellesen, C.; Nour-Eldin, N.E.A.; Scholtz, J.E.; Herrmann, E.; Vogl, T.J.; Wichmann, J.L. Evaluation of different keV-settings in dual-energy CT angiography of the aorta using advanced image-based virtual monoenergetic imaging. Int. J. Cardiovasc. Imaging 2014, 32, 137–144. [Google Scholar] [CrossRef]
- Albrecht, M.H.; Trommer, J.; Wichmann, J.L.; Scholtz, J.-E.; Martin, S.S.; Lehnert, T.; Vogl, T.J.; Bodelle, B. Comprehensive comparison of virtual monoenergetic and linearly blended reconstruction techniques in third-generation dual-source dual-energy computed tomography angiography of the thorax and abdomen. Investig. Radiol. 2016, 51, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Lenga, L.; Albrecht, M.H.; Othman, A.E.; Martin, S.S.; Leithner, D.; D’Angelo, T.; Arendt, C.; Scholtz, J.E.; De Cecco, C.N.; Schoepf, U.J.; et al. Monoenergetic dual-energy computed tomographic imaging: Cardiothoracic applications. J. Thorac. Imaging 2017, 32, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Bucher, A.M.; Wichmann, J.L.; Schoepf, U.J.; Wolla, C.D.; Canstein, C.; McQuiston, A.D.; Krazinski, A.W.; De Cecco, C.N.; Meinel, F.G.; Vogl, T.J.; et al. Quantitative evaluation of beam-hardening artefact correction in dual-energy CT myocardial perfusion imaging. Eur. Radiol. 2015, 26, 3215–3222. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, F.; Dierks, A.; Nikolaou, K.; Reiser, M.F.; Becker, C.R.; Johnson, T.R.C. Metal artifact reduction by dual energy computed tomography using monoenergetic extrapolation. Eur. Radiol. 2011, 21, 1424–1429. [Google Scholar] [CrossRef] [PubMed]
- Secchi, F.; De Cecco, C.N.; Spearman, J.V.; Silverman, J.R.; Ebersberger, U.; Sardanelli, F.; Schoepf, U.J. Monoenergetic extrapolation of cardiac dual energy CT for artifact reduction. Acta Radiol. 2015, 56, 413–418. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Jin, K.N.; Schoepf, U.J.; Grant, K.L.; De Cecco, C.N.; Nance, J.W., Jr.; Vogl, T.J.; Laghi, A.; Albrecht, M.H. Heavily calcified coronary arteries: Advanced calcium subtraction improves luminal visualization and diagnostic confidence in dual-energy coronary computed tomography angiography. Investig. Radiol. 2017, 2, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Buerke, B.; Wittkamp, G.; Seifarth, H.; Heindel, W.; Kloska, S.P. Dual-energy CTA with bone removal for transcranial arteries: Intraindividual comparison with standard CTA without bone removal and TOF-MRA. Acad. Radiol. 2009, 16, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Morhard, D.; Fink, C.; Graser, A.; Reiser, M.F.; Becker, C.; Johnson, T.R. Cervical and cranial computed tomographic angiography with automated bone removal: Dual energy computed tomography versus standard computed tomography. Investig. Radiol. 2009, 44, 293–297. [Google Scholar] [CrossRef]
- Schulz, B.; Kuehling, K.; Kromen, W.; Siebenhandl, P.; Kerl, M.J.; Vogl, T.J.; Bauer, R. Automatic bone removal technique in whole-body dual-energy CT angiography: Performance and image quality. Am. J. Roentgenol. 2012, 199, W646–W650. [Google Scholar] [CrossRef] [PubMed]
- Sommer, W.H.; Johnson, T.R.; Becker, C.R.; Arnoldi, E.; Kramer, H.; Reiser, M.F.; Nikolaou, K. The value of dual-energy bone removal in maximum intensity projections of lower extremity computed tomography angiography. Investig. Radiol. 2009, 44, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Korn, A.; Bender, B.; Thomas, C.; Danz, S.; Fenchel, M.; Nägele, T.; Heuschmid, M.; Ernemann, U.; Hauser, T. Dual energy CTA of the carotid bifurcation: Advantage of plaque subtraction for assessment of grade of the stenosis and morphology. Eur. J. Radiol. 2011, 80, e120–e125. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.; Werncke, T.; Hopfenmüller, W.; Raatschen, H.; Wolf, K.-J.; Albrecht, T. Dual energy CT of peripheral arteries: Effect of automatic bone and plaque removal on image quality and grading of stenoses. Eur. J. Radiol. 2008, 68, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Uotani, K.; Watanabe, Y.; Higashi, M.; Nakazawa, T.; Kono, A.K.; Hori, Y.; Fukuda, T.; Kanzaki, S.; Yamada, N.; Itoh, T.; et al. Dual-energy CT head bone and hard plaque removal for quantification of calcified carotid stenosis: Utility and comparison with digital subtraction angiography. Eur. Radiol. 2009, 19, 2060–2065. [Google Scholar] [CrossRef] [PubMed]
- Sommer, W.H.; Graser, A.; Becker, C.R.; Clevert, D.A.; Reiser, M.F.; Nikolaou, K.; Johnson, T.R. Image quality of virtual noncontrast images derived from dual-energy CT angiography after endovascular aneurysm repair. J. Vasc. Interv. Radiol. 2010, 21, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Ascenti, G.; Mazziotti, S.; Lamberto, S.; Bottari, A.; Caloggero, S.; Racchiusa, S.; Mileto, A.; Scribano, E. Dual-energy CT for detection of endoleaks after endovascular abdominal aneurysm repair: Usefulness of colored iodine overlay. Am. J. Roentgenol. 2011, 196, 1408–1414. [Google Scholar] [CrossRef]
- Schabel, C.; Bongers, M.; Sedlmair, M.; Korn, A.; Grosse, U.; Mangold, S.; Claussen, C.D.; Thomas, C. Assessment of the hepatic veins in poor contrast conditions using dual energy CT: Evaluation of a novel monoenergetic extrapolation software algorithm. RöFo 2014, 186, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, N.M.; Sahani, D.V.; Desai, G.S.; Kalva, S.P. Indirect computed tomography venography of the lower extremities using single-source dual-energy computed tomography: Advantage of low-kiloelectron volt monochromatic images. J. Vasc. Interv. Radiol. 2012, 23, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Weiss, J.; Schabel, C.; Othman, A.E.; Bier, G.; Nikolaou, K.; Bamberg, F.; Bongers, M.N. Impact of dual-energy CT post-processing to differentiate venous thrombosis from iodine flux artefacts. Eur. Radiol. 2018, 28, 5076–5082. [Google Scholar] [CrossRef] [PubMed]
- Hamid, S.; Nasir, M.U.; So, A.; Andrews, G.; Nicolaou, S.; Qamar, S.R. Clinical applications of dual-energy CT. Korean J. Radiol. 2021, 22, 970–982. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, J.L.; Nöske, E.M.; Kraft, J.; Iris, B.; Jens, W.; Anne, E.; Claudia, F.; Matthias, K.J.; Ralf W, B.; Boris, B.; et al. Virtual monoenergetic dual-energy computed tomography: Optimization of kiloelectron volt settings in head and neck cancer. Investig. Radiol. 2014, 49, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Husarik, D.B.; Gordic, S.; Desbiolles, L.; Bernhard, K.; Sebastian, L.; Simon, W.; Hatem, A. Advanced virtual monoenergetic computed tomography of hyperattenuating and hypoattenuating liver lesions: Ex-vivo and patient experience in various body sizes. Investig. Radiol. 2015, 50, 695–702. [Google Scholar] [CrossRef]
- Marin, D.; Ramirez-Giraldo, J.C.; Gupta, S.; Fu, W.; Stinnett, S.S.; Mileto, A.; Bellini, D.; Patel, B.; Samei, E.; Nelson, R.C. Effect of a noise-optimized second-generation monoenergetic algorithm on image noise and conspicuity of hypervascular liver tumors: An in vitro and in vivo study. Am. J. Roentgenol. 2016, 206, 1222–1232. [Google Scholar] [CrossRef] [PubMed]
- Frellesen, C.; Fessler, F.; Hardie, A.D.; Wichmann, J.L.; De Cecco, C.N.; Schoepf, U.J.; Kerl, J.M.; Schulz, B.; Hammerstingl, R.; Vogl, T.J.; et al. Dual-energy CT of the pancreas: Improved carcinoma-to-pancreas contrast with a noise-optimized monoenergetic reconstruction algorithm. Eur. J. Radiol. 2015, 84, 2052–2058. [Google Scholar] [CrossRef]
- McNamara, M.M.; Little, M.D.; Alexander, L.F.; Carroll, L.V.; Beasley, T.M.; Morgan, D.E. Multireader evaluation of lesion conspicuity in small pancreatic adenocarcinomas: Complimentary value of iodine material density and low keV simulated monoenergetic images using multiphasic rapid kVp-switching dual energy CT. Abdom. Imaging 2015, 40, 1230–1240. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Wichmann, J.L.; Pfeifer, S.; Leithner, D.; Lenga, L.; Reynolds, M.A.; D’angelo, T.; Hammerstingl, R.; Gruber-Rouh, T.; Vogl, T.J.; et al. Impact of noise-optimized virtual monoenergetic dual-energy computed tomography on image quality in patients with renal cell carcinoma. Eur. J. Radiol. 2017, 97, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.N.; Farjat, A.; Schabel, C.; Duvnjak, P.; Mileto, A.; Ramirez-Giraldo, J.C.; Marin, D. Energy-specific optimization of attenuation thresholds for low-energy virtual monoenergetic images in renal lesion evaluation. Am. J. Roentgenol. 2018, 210, W205–W217. [Google Scholar] [CrossRef]
- Martin, S.S.; Czwikla, R.; Wichmann, J.L.; Albrecht, M.H.; Lenga, L.; Savage, R.H.; Arendt, C.; Hammerstingl, R.; Vogl, T.J.; Kaltenbach, B. Dual-energy CT-based iodine quantification to differentiate abdominal malignant lymphoma from lymph node metastasis. Eur. J. Radiol. 2018, 105, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.N.; Boltyenkov, A.T.; Martinez, M.G.; Mastrodicasa, D.; Marin, D.; Jeffrey, R.B.; Chung, B.; Pandharipande, P.; Kambadakone, A. Cost-effectiveness of dual-energy CT versus multiphasic single-energy CT and MRI for characterization of incidental indeterminate renal lesions. Abdom. Imaging 2020, 45, 1896–1906. [Google Scholar] [CrossRef]
- Atwi, N.E.; Sabottke, C.F.; Pitre, D.M.; Smith, D.L.; Danrad, R.; Dharaiya, E.; Kambadakone, A.; Pandharipande, P.V.; Toshav, A.M. Follow-up Recommendation Rates Associated with Spectral Detector Dual-Energy CT of the Abdomen and Pelvis: A Retrospective Comparison to Single-Energy CT. J. Am. Coll. Radiol. 2020, 17, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Parakh, A.; Lennartz, S.; An, C.; Rajiah, P.; Yeh, B.M.; Simeone, F.J.; Sahani, D.V.; Kambadakone, A.R. Dual-energy CT images: Pearls and pitfalls. RadioGraphics 2021, 41, 98–119. [Google Scholar] [CrossRef] [PubMed]
- Parakh, A.; An, C.; Lennartz, S.; Rajiah, P.; Yeh, B.M.; Simeone, F.J.; Sahani, D.V.; Kambadakone, A.R. Recognizing and Minimizing Artifacts at Dual-Energy CT. RadioGraphics 2021, 41, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Lennartz, S.; Pisuchpen, N.; Mroueh, N.; Kongboonvijit, S.; Parakh, A.; Sahani, D.V.; Kambadakone, A. Renal Lesion Characterization by Dual-Layer Dual-Energy CT: Comparison of Virtual and True Unenhanced Images. Am. J. Roentgenol. 2022, 219, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Srinivas-Rao, S.; Cao, J.; Marin, D.; Kambadakone, A.R. Dual-Energy Computed Tomography to Photon Counting Computed Tomography: Emerging Technological Innovations. Radiol. Clin. N. Am. 2023, 61, 933–944. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Advantages | Disadvantages |
|---|---|---|
| Dual source | Optimized image quality | Limited temporal and spatial resolution Small FOV * |
| Rapid kVp switching | Good temporal and spatial registration | Limited spectral separation High noise-to-signal ratio of low-energy images Requires specialized hardware |
| Dual layer detectors | Excellent temporal and spatial resolution | High spectral overlap Requires specialized hardware |
| Twin-beam filtration | Cost-effective Full spectral FOV * available for image acquisition | Temporal discrepancy between high- and low-energy data Cross-scatter Intrinsic lower energies due to filtration Overlapping spectra in center and edge of the beam |
| Dual spin | Cost-effective (can be performed on any scanner) Optimized tube current modulation Full spectral FOV * No cross scatter | Spectral distortion secondary to motion artefact |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Omar, A.; Murray, N.; Ali, I.T.; Khosa, F.; Barrett, S.; Sheikh, A.; Nicolaou, S.; Tamburrini, S.; Iacobellis, F.; Sica, G.; et al. Utility of Dual-Energy Computed Tomography in Clinical Conundra. Diagnostics 2024, 14, 775. https://doi.org/10.3390/diagnostics14070775
Abu-Omar A, Murray N, Ali IT, Khosa F, Barrett S, Sheikh A, Nicolaou S, Tamburrini S, Iacobellis F, Sica G, et al. Utility of Dual-Energy Computed Tomography in Clinical Conundra. Diagnostics. 2024; 14(7):775. https://doi.org/10.3390/diagnostics14070775
Chicago/Turabian StyleAbu-Omar, Ahmad, Nicolas Murray, Ismail T. Ali, Faisal Khosa, Sarah Barrett, Adnan Sheikh, Savvas Nicolaou, Stefania Tamburrini, Francesca Iacobellis, Giacomo Sica, and et al. 2024. "Utility of Dual-Energy Computed Tomography in Clinical Conundra" Diagnostics 14, no. 7: 775. https://doi.org/10.3390/diagnostics14070775
APA StyleAbu-Omar, A., Murray, N., Ali, I. T., Khosa, F., Barrett, S., Sheikh, A., Nicolaou, S., Tamburrini, S., Iacobellis, F., Sica, G., Granata, V., Saba, L., Masala, S., & Scaglione, M. (2024). Utility of Dual-Energy Computed Tomography in Clinical Conundra. Diagnostics, 14(7), 775. https://doi.org/10.3390/diagnostics14070775