
Comprehensive Investigation of Angiogenesis, PASS Score and Immunohistochemical Factors in Risk Assessment of Malignancy for Paraganglioma and Pheochromocytoma


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Tissue Microarray Construction
2.3. Immunohistochemistry
2.4. Morphometry
2.5. Determination of Intratumoral MVD
2.6. Clinical Data
2.7. Statistical Analysis
3. Results
3.1. Clinical and Macroscopic Findings
3.2. Microscopic and Immunohistochemical Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mete, O.; Asa, S.L.; Gill, A.J.; Kimura, N.; de Krijger, R.R.; Tischler, A. Overview of the 2022 WHO Classification of Paragangliomas and Pheochromocytomas. Endocr. Pathol. 2022, 33, 90–114. [Google Scholar] [PubMed]
- Lam, A.K.-Y. Update on Adrenal Tumors in 2017 World Health Organisation (WHO) of Endocrine Tumours. Endocr. Pathol. 2017, 28, 213–227. [Google Scholar] [PubMed]
- Lloyd, R.V.; Osamura, R.Y.; Kloppel, G.; Rosai, J. Tumors of the adrenal medulla and extra-adrenal paraganglia. In WHO Classification of Tumours of Endocrine Organs: Pathology and Genetics of Tumours of Endocrine Organ, 4th ed.; Lloyd, R.V., Osamura, R.Y., Kloppel, G., Rosai, J., Eds.; IARC Press: Lyon, France, 2017; pp. 179–192. [Google Scholar]
- Fishbein, L.; Merrill, S.; Fraker, D.L.; Cohen, D.L.; Nathanson, K.L. Inherited mutations in pheochromocytoma and paraganglioma: Why all patients should be offered genetic testing. Ann. Surg. Oncol. 2013, 20, 1444–1450. [Google Scholar] [PubMed]
- Dahia, P.L.M. Pheochromocytoma and paraganglioma pathogenesis: Learning from genetic heterogeneity. Nat. Rev. Cancer 2014, 14, 108–119. [Google Scholar] [PubMed]
- Lenders, J.W.M.; Duh, Q.-Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.-P.; Grebe, S.K.G.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F., Jr. Pheochromocytoma and paraganglioma: An endocrine society clinical and practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar]
- Grogan, R.H.; Mitmaker, E.J.; Duh, Q.-Y. Changing paradigms in the treatment of malignant pheochromocytoma. Cancer Control 2011, 18, 104–112. [Google Scholar] [PubMed]
- Druce, M.R.; Kaltsas, G.A.; Fraenkel, M.; Gross, D.J.; Grossman, A.B. Novel and evolving therapies in the treatment of malignant pheochromocytoma: Experience with the mTOR inhibitor everolimus (RAD001). Horm. Metab. Res. 2009, 41, 697–702. [Google Scholar] [PubMed]
- Elder, E.E.; Hjelm Skog, A.-L.; Hoog, A.; Hamberger, B. The management of benign and malignant pheochromocytoma and abdominal paraganglioma. Eur. J. Surg. Oncol. 2003, 29, 278–283. [Google Scholar]
- Tischler, A.S. Pheochromocytoma and extra-adrenal paraganlioma: Updates. Arch. Pathol. Lab. Med. 2008, 132, 1272–1284. [Google Scholar]
- Ayala-Ramirez, M.; Feng, L.; Johnson, M.M.; Ejaz, S.; Habra, M.A.; Rich, T.; Busaidy, N.; Cote, G.J.; Perrier, N.; Phan, A.; et al. Clinical risk factors for malignancy and overall survival in patients with pheochromocytomas and sympathetic paragangliomas; primary tumor size and primary tumor location as prognostic indicators. J. Clin. Endocrinol. Metab. 2011, 96, 717–725. [Google Scholar]
- Hamidi, O.; Young, W.F., Jr.; Iniguez-Ariza, N.M.; Kittah, N.E.; Gruber, L.; Bancos, C.; Tamhane, S.; Bancos, I. Malignant Pheochromocytoma and Paraganglioma: 272 Patients Over 55 Years. J. Clin. Endocrinol. Metab. 2017, 102, 3296–3305. [Google Scholar] [PubMed]
- Jasim, S.; Jimenez, C. Metastatic pheochromocytoma and paraganglioma: Management of endocrine manifestations, surgery and ablative procedures, and systemic therapies. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101354. [Google Scholar] [PubMed]
- Eisenhofer, G.; Tischler, A.S.; de Krijger, R.R. Diagnostic tests and biomarkers for pheochromocytoma and extra-adrenal paraganglioma: From routine laboratory methods to disease stratification. Endocr. Pathol. 2012, 23, 4–14. [Google Scholar] [PubMed]
- Thompson, L.D.R. Pheochromocytoma of the Adrenal gland Scaled Score (PASS) to separate benign from malignant neoplasms: A clinicopathologic and immunophenotypic study of 100 cases. Am. J. Surg. Pathol. 2002, 26, 551–566. [Google Scholar] [PubMed]
- Gao, X.; Yamazaki, Y.; Pecori, A.; Tezuka, Y.; Ono, Y.; Omata, K.; Morimoto, R.; Nakamura, Y.; Satoh, F.; Sasano, H. Histopatological Analysis of Tumor Microinviroment and Angiogenesis in Pheochromocytoma. Front. Endocrinol. 2020, 11, 587779. [Google Scholar]
- Wu, D.; Tischler, A.S.; Lloyd, R.V.; DeLellis, R.A.; de Krijger, R.; van Nederveen, F.; Nose, V. Observer variation in the application of the Pheochromocytoma of the Adrenal Gland Scaled Score. Am. J. Surg. Pathol. 2009, 33, 599–608. [Google Scholar] [PubMed]
- Strong, V.E.; Kennedy, T.; Al-Ahmadie, H.; Tang, L.; Coleman, J.; Fong, Y.; Brennan, M.; Ghossein, R.A. Prognostic indicators of malignancy in adrenal pheochromocytomas: Clinical, histopathologic and cell cycle/apoptosis gene expression analysis. Surgery 2008, 143, 759–768. [Google Scholar] [PubMed]
- Folkman, J.; Shing, Y. Angiogenesis. J. Biol. Chem. 1992, 267, 10931–10934. [Google Scholar]
- Liu, Q.; Djuricin, G.; Staren, E.D.; Gattuso, P.; Gould, V.E.; Shen, J.; Saclarides, T.; Rubin, D.B.; Prinz, R.A. Tumor angiogenesis in pheochromocytomas and paragangliomas. Surgery 1996, 120, 938–942; discussion 942–943. [Google Scholar]
- Ohji, H.; Sasagawa, I.; Iciyanagi, O.; Suzuki, Y.; Nakada, T. Tumour angiogenesis and Ki67 expression in phaeochromocytoma. BJU Int. 2001, 87, 381–385. [Google Scholar]
- Jimenez, C.; Junsheng, M.; Gonzalez, A.R.; Varghese, J.; Zhang, M.; Perrier, N.; Habra, M.A.; Graham, P.; Waguespack, S.G. TNM Staging and Overall Survival in Patients With Pheochromocytoma and Sympathetic Paraganglioma. J. Clin. Endocrinol. Metab. 2023, 108, 1132–1142. [Google Scholar] [PubMed]
- Skacel, M.; Skilton, B.; Pettay, J.D.; Tubbs, R.R. Tissue microarrays: A powerful tool for high-throughput analysis of clinical specimens: A review of the method with validation data. Appl. Immunohistochem. Mol. Morphol. 2002, 10, 1–6. [Google Scholar]
- Taylor, C.R.; Rudbeck, L. The Staining Proscess. In Immunohistochemical Staining Methods, 6th ed.; Taylor, C.R., Rudbeck, L., Eds.; Dako Denmark A/S: Glostrup, Denmark, 2013; pp. 20–91. [Google Scholar]
- Schnidein, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar]
- Cell Counts: Histology Guidance (SXHL288). Available online: https://www.studocu.com/en-gb/document/the-open-university/cell-biology/cell-counts-histology-guidance-sxhl288/6880909 (accessed on 20 November 2021).
- Exercise 3—Biology 105 Estimating the Size of Cells Using a Compound Light Microscope. Available online: https://pdf4pro.com/view/exercise-3-biology-105-estimating-the-size-of-cells-4aac9.html (accessed on 20 November 2021).
- Yao, Y.; Pan, Y.; Chen, J.; Sun, X.; Qiu, Y.; Ding, Y. Endoglin (CD105) expression in angiogenesis of primary hepatocellular carcinomas: Analysis using tissue microarrays and comparisons with CD34 and VEGF. Ann. Clin. Lab. Sci. 2007, 37, 39–48. [Google Scholar] [PubMed]
- Tanigawa, N.; Lu, C.; Mitsui, T.; Miura, S. Quantitation of sinusoid-like vessels in hepatocellular carcinoma: Its clinical and prognostic significance. Hepatology 1997, 26, 1216–1223. [Google Scholar] [PubMed]
- Weidner, N. Current pathologic methods for measuring intratumoral microvessel density within breast carcinoma and other solid tumors. Breast Cancer Res. Treat. 1995, 36, 169–180. [Google Scholar] [PubMed]
- Schlumberger, M.; Gicquel, C.; Lumbroso, J.; Tenenbaum, F.; Comoy, E.; Bosq, J.; Fonseca, E.; Ghillani, P.P.; Aubert, B.; Travagli, J.P.; et al. Malignant pheochromocytoma: Clinical, biological, histologic and therapeutic data in a series of 20 patients with distant metastases. J. Endocrinol. Investig. 1992, 15, 631–642. [Google Scholar]
- Pattarino, F.; Bouloux, P.M. The diagnosis of malignancy in phaeochromocytoma. Clin. Endocrinol. 1996, 44, 239–241. [Google Scholar]
- Bialas, M.; Dyduch, G.; Dudala, J.; Bereza-Buziak, M.; Hubalewska-Dydejczyk, A.; Budzynski, A.; Okon, K. Study of microvessel density and the expression of vascular endothelial growth factors in adrenal gland pheochromocytomas. Int. J. Endocrinol. 2014, 2014, 104129. [Google Scholar]
- Favier, J.; Plouin, P.-F.; Corvol, P.; Gasc, J.-M. Angiogenesis and vascular architecture in pheochromocytomas: Distinctive traits in malignant tumors. Am. J. Pathol. 2002, 161, 1235–1246. [Google Scholar]
- Oudijk, L.; van Nederveen, F.; Badoual, C.; Tissier, F.; Tischler, A.S.; Smid, M.; Gaal, J.; Lepoutre-Lussey, C.; Gimenez-Roqueplo, A.-P.; Dinjens, W.N.M.; et al. Vascular pattern analysis for the prediction of clinical behaviour in pheochromocytomas and paragangliomas. PLoS ONE 2015, 10, e0121361. [Google Scholar]
- Seon, B.K.; Matsuno, F.; Haruta, Y.; Kondo, M.; Barcos, M. Long-lasting complete inhibition of human solid tumors in SCID mice by targeting endothelial cells of tumor vasculature with antihuman endoglin immunotoxin. Clin. Cancer Res. 1997, 3, 1031–1044. [Google Scholar] [PubMed]
- Westphal, J.R.; Willems, H.W.; Schalkwijk, C.J.; Ruiter, D.J.; de Waal, R.M. Characteristics and possible function of endoglin, a TGF-beta binding protein. Behring Inst. Mitt. 1993, 92, 15–22. [Google Scholar]
- Saad, R.S.; Jasnosz, K.M.; Tung, M.Y.; Silverman, J.F. Endoglin (CD105) expression in endometrial carcinoma. Int. J. Gynecol. Pathol. 2003, 22, 248–253. [Google Scholar]
- Behrem, S.; Zarkovic, K.; Eskinja, N.; Jonjic, N. Endoglin is a better marker than CD31 in evaluation of angiogenesis in glioblastoma. Croat. Med. J. 2005, 46, 417–422. [Google Scholar]
- Birdsey, G.M.; Dryden, N.H.; Amsellem, V.; Gebhardt, F.; Sahnan, K.; Haskard, D.O.; Dejana, E.; Mason, J.C.; Randi, A.M. Transcription factor Erg regulates angiogenesis and endothelial apoptosis through VE-cadherin. Blood 2008, 111, 3498–3506. [Google Scholar]
- Favier, J.; Gimenez-Roqueplo, A.-P. Pheochromocytomas: The (pseudo)-hypoxia hypothesis. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 957–968. [Google Scholar] [PubMed]
- Amorim-Pires, D.; Peixoto, J.; Lima, J. Hypoxia Pathway Mutations in Pheochromocytomas and Paragangliomas. Cytogenet. Genome Res. 2016, 150, 227–241. [Google Scholar]
- De Wailly, P.; Oragano, L.; Rade, F.; Beaulieu, A.; Arnault, V.; Levillain, P.; Kraimps, J.L. Malignant pheochromocytoma: New malignancy criteria. Langenbecks Arch. Surg. 2012, 397, 239–246. [Google Scholar]
- Nagura, S.; Katoh, R.; Kawaoi, A.; Kobayashi, M.; Obara, T.; Omata, K. Immunohistohemical estimation of growth activity to predict biological behavior of pheochromocytomas. Mod. Pathol. 1999, 12, 1107–1111. [Google Scholar]
- August, C.; August, K.; Schroeder, S.; Bahn, H.; Hinze, R.; Baba, H.A.; Kersting, C.; Buerger, H. CGH and CD44/MIB-1 immunohistochemisty are helpful to distinguish metastasized from nonmetastasized sporadic pheochromocytomas. Mod. Pathol. 2004, 17, 1119–1128. [Google Scholar] [PubMed]
- Elder, E.E.; Xu, D.; Hoog, A.; Enberg, U.; Hou, M.; Pisa, P.; Gruber, A.; Larsson, C.; Backdahl, M. KI67 AND hTERT expression can aid in distinction between malignant and benign pheochromocytoma and paraganglioma. Mod. Pathol. 2003, 16, 246–255. [Google Scholar] [PubMed]
- Tavangar, S.M.; Shojaee, A.; Tabriz, M.H.; Haghpanah, V.; Larijani, B.; Heshmat, R.; Lashkari, A.; Azimi, S. Immunohistochemical expression of Ki-67, c-erbB-2, and c-kit antigens in benign and malignant pheochromocytoma. Pathol. Res. Pract. 2010, 206, 305–309. [Google Scholar] [PubMed]
- Liu, T.-H.; Chen, Y.-J.; Wu, S.-F.; Gao, J.; Jiang, W.-J.; Lu, Z.-H.; Guan, J.; Wei, S.-Z.; Luo, Y.-F.; Cao, J.-L.; et al. Distinction between benign and malignant pheochromocytomas. Zhonghua Bing Li Xue Za Zhi 2004, 33, 198–202. [Google Scholar]
- Unger, P.; Hoffman, K.; Pertsemlidis, D.; Thung, S.; Wolfe, D.; Kaneko, M. S100 protein-positive sustentacular cells in malignant and locally aggressive adrenal pheochromocytomas. Arch. Pathol. Lab. Med. 1991, 115, 484–487. [Google Scholar] [PubMed]
- Buffet, A.; Burnichon, N.; Favier, J.; Gimenez-Roqueplo, A.-P. An overview of 20 years of genetic studies in pheochromocytoma and paraganglioma. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101416. [Google Scholar] [PubMed]
- Baysal, B.E.; Willett-Brozick, J.E.; Lawrence, E.C.; Drovdlic, C.M.; Savul, S.A.; McLeod, D.R.; Yee, H.A.; Brackmann, D.E.; Slattery, W.H., 3rd; Myers, E.N.; et al. Prevalence of SDHB, SDHC, and SDHD germline mutations in clinic patients with head and neck paragangliomas. J. Med. Genet. 2002, 39, 178–183. [Google Scholar] [PubMed]
- Buffet, A.; Venisse, A.; Nau, V.; Roncellin, I.; Boccio, V.; Le Pottier, N.; Boussion, M.; Travers, C.; Simian, C.; Burnichon, N.; et al. A decade (2001–2010) of genetic testing for pheochromocytoma and paraganglioma. Horm. Metab. Res. 2012, 44, 359–366. [Google Scholar]
- Benn, D.E.; Robinson, B.G.; Clifton-Bligh, R.J. 15 YEARS OF PARAGANGLIOMA: Clinical manifestations of paraganglioma syndromes types 1–5. Endocr. Relat. Cancer 2015, 22, T91–T103. [Google Scholar]
- Plouin, P.F.; Amar, L.; Dekkers, O.M.; Fassnacht, M.; Gimenez-Roqueplo, A.-P.; Lenders, J.W.M.; Lussey-Lepoutre, C.; Steichen, O. European Society of Endocrinology Clinical Practice Guideline for long-term follow-up of patients operated on for a phaeochromocytoma or a paraganglioma. Eur. J. Endocrinol. 2016, 174, G1–G10. [Google Scholar]
- Van Nederveen, F.H.; Gaal, J.; Favier, J.; Korpershoek, E.; Oldenburg, R.A.; de Bruyn, E.M.; Sleddens, H.F.; Derkx, P.; Riviere, J.; Dannenberg, H.; et al. An immunohistochemical procedure to detect patients with paraganglioma and pheochromocytoma with germline SDHB, SDHC, or SDHD gene mutations: A retrospective and prospective analysis. Lancet Oncol. 2009, 10, 764–771. [Google Scholar]
- Goldstein, R.E.; O’Neill, J.A., Jr.; Holcomb, G.W., III; Morgan, W.M., III; Neblett, W.W., III; Oates, J.A.; Brown, N.; Smith, B.; Page, D.L.; Abumrad, N.N.; et al. Clinical experience over 48 years with pheochromocytoma. Ann. Surg. 1999, 229, 755–764. [Google Scholar] [PubMed]
- Ajalle, R.; Plouin, P.F.; Pacak, K.; Lehner, H. Treatment of malignant pheochromocytoma. Horm. Metab. Res. 2009, 41, 687–696. [Google Scholar]
- Amar, L.; Bertherat, J.; Baudin, E.; Ajzenberg, K.; Bressac-de Pillerets, B.; Chabre, O.; Chamontin, B.; Delemer, B.; Giraud, S.; Murat, A.; et al. Genetic testing in pheochromocytoma of functional paraganglioma. J. Clin. Oncol. 2005, 23, 8812–8818. [Google Scholar] [PubMed]
- Yamazaki, Y.; Gao, X.; Pecori, A.; Nakamura, Y.; Tezuka, Y.; Omata, K.; Ono, Y.; Morimoto, R.; Satoh, F.; Sasano, H. Recent advances in histopathological and molecular diagnosis in pheochromocytoma and paraganglioma: Challenges fo predicting metastasis in individual patients. Front. Endocrinol. 2020, 11, 587769. [Google Scholar]
- Kimura, N.; Takayanagi, R.; Takizawa, N.; Itagaki, E.; Katabarni, T.; Kakoi, N.; Rakugi, H.; Ikeda, Y.; Tanabe, A.; Nigawara, T.; et al. Phaechromocytoma Study Group in Japan. Pathological grading in phaechromocytoma and paraganglioma. Endocr Relat Cancer 2014, 21, 405–414. [Google Scholar]
- Wang, Y.; Li, M.; Deng, H.; Pang, Y.; Liu, L.; Guan, X. The systems of metastatic potential prediction in pheochromocytoma and paraganglioma. Am. J. Cancer 2020, 10, 769–800. [Google Scholar]
- Koh, J.-M.; Ahn, S.H.; Kim, H.; Kim, B.-J.; Sung, T.-Y.; Kim, Y.H.; Hong, S.J.; Song, D.E.; Lee, S.H. Validation of pathological grading systems for predicting metastatic potential in pheochromocytoma and paraganglioma. PLoS ONE 2017, 12, e0187398. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Dilution | Source |
|---|---|---|
| CD31 | 1:100 | BIO SB |
| CD34 | 1:200 | NOVOCASTRA |
| CD105 | 1:100 | Termo Fisher |
| ERG | 1:100 | ABCAM |
| SDHB | 1:50 | ABCAM |
| S-100 | 1:100 | NOVOCASTRA |
| Ki67 | 1:200 | DAKO |
| Feature | PASS < 4 | PASS ≥ 4 | p e |
|---|---|---|---|
| Total number (%) a (m, f) b | 61 (53%) (17 m, 44 f) | 54 (47%) (23 m, 31 f) | |
| Age at resection mean/range | 48.4 (22–78) | 48.8 (19–73) | 0.864 |
| Site of tumor | 0.118 | ||
| Intraadrenal total/percentages | 55 (47.83%) | 52 (45.22%) | |
| extraadrenal total/percentages | 6 (5.22%) | 2 (1.74%) | |
| Tumor weight in grams mean/range | 31.7 (3–159) | 89.7 (2–361) | 0.001 |
| Tumor size in mm mean/range | 44 (4–110) | 61 (20–130) | 0.001 |
| Catecholamines/metabolites | 0.673 | ||
| elevated total/percentages | 47 (40.87%) | 46 (40%) | |
| normal total/percentages | 9 (7.83%) | 7 (6.08%) | |
| unknown data total/percentages | 5 (4.35%) | 1 (0.87%) | |
| Blood pressure/spikes | |||
| elevated total/percentages | 47 (40.87%) | 44 (38.26%) | 0.676 |
| normal total/percentages | 13 (11.3%) | 10 (8.7%) | |
| unknown data total/percentages | 1 (0.87%) | ||
| MIBG scintigraphy | 1.000 | ||
| increased accumulation | 24 (20.87%) | 16 (13.91%) | |
| normal distribution | 8 (6.96%) | 4 (3.49%) | |
| unknown data | 29 (25.22%) | 34 (29.56%) | |
| Genetic testing | 0.843 | ||
| mutation present | 16 (13.91%) | 16 (13.91%) | |
| mutation excluded | 8 (6.96%) | 8 (6.09%) | |
| unknown data | 37 (32.17%) | 31 (26.96%) | |
| TNM | 0.001 | ||
| T1 tumor < 5 cm c | 37 | 13 | |
| T2 tumor ≥ 5 cm d | 22 | 24 | |
| T3 tumor of any size with invasion | 2 | 16 |
| Antibody | PASS < 4 | PASS ≥ 4 | p b |
|---|---|---|---|
| CD31 mean/SD a | 274.31/206.41 | 242.41/204.15 | 0.336 |
| CD105 mean/SD a | 132.31/149.85 | 83.81/82.86 | 0.088 |
| ERG mean/SD a | 358.87/321.36 | 234.46/179.92 | 0.071 |
| CD34 mean/SD a | 429.28/324.73 | 319.50/226.88 | 0.077 |
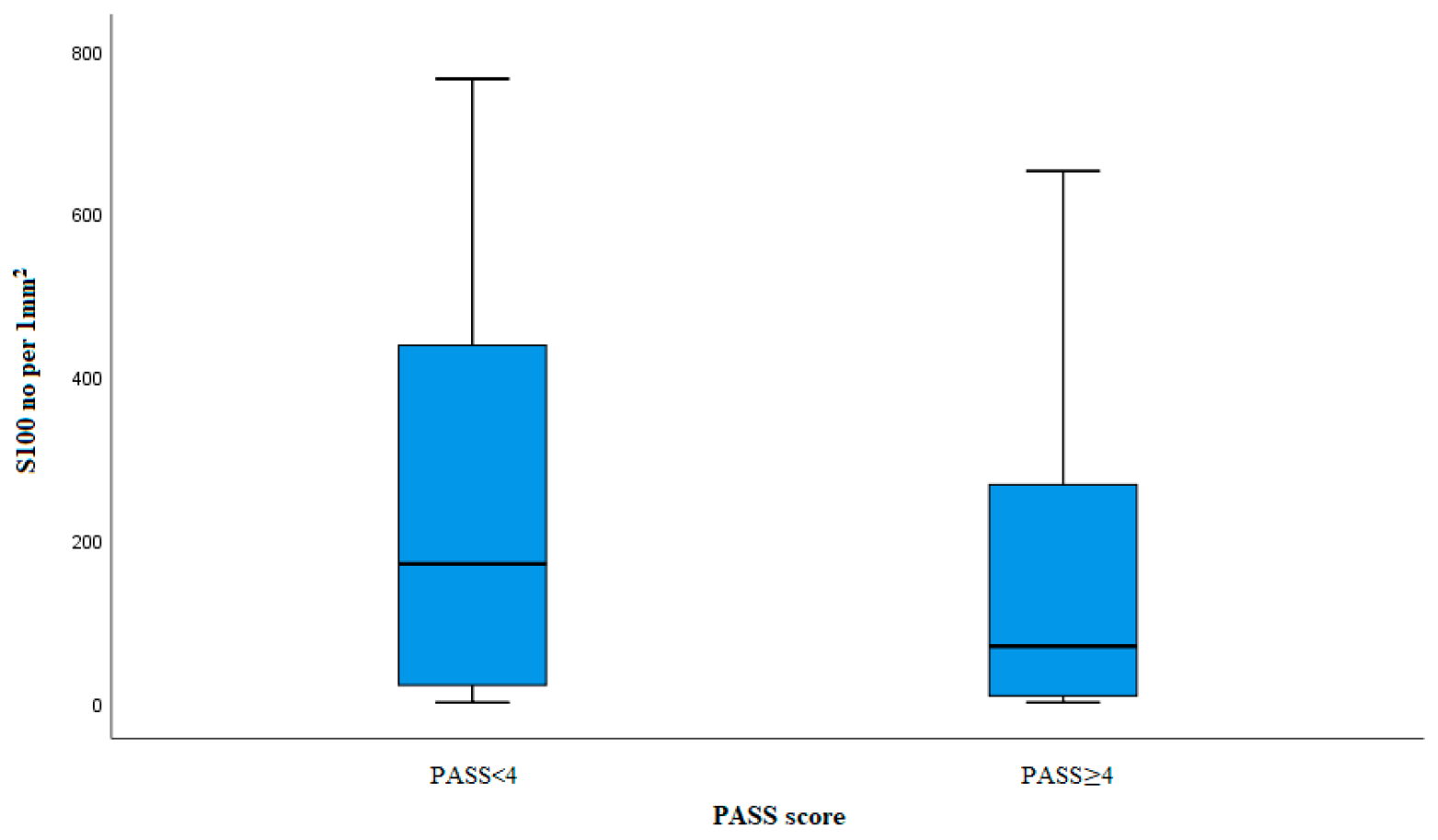
| S100 mean/SD a | 243.11/242.73 | 158.61/187.27 | 0.062 |
| Ki67 mean/SD a | 1.02/0.93 | 1.22/1.47 | 0.598 |
| SDHB positive/negative | 57/4 | 52/2 | 0.683 |
| Syndrome | Number (m, f) x | Age Mean/Range | PASS Mean/Range |
|---|---|---|---|
| VHL | 10 (6 m, 4 f) | 37.7 (19–55) | 4.2 (1–12) |
| MEN2a | 17 (6 m; 11 f) | 42.6 (22–64) | 3.1 (1–8) |
| NF1 | 4 (1 m; 3 f) | 44.3 (34–53) | 6.3 (4–9) |
| SDHB | 1 (1 f) | 51 | 9 |
| Without mutation | 15 (3 m; 11 f) | 45 (29–64) | 5.1 (1–10) |
| Not available | 68 (24 m; 44 f) | 52.5 (23–78) | 3.7 (1–10) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milinkovic, M.; Soldatovic, I.; Zivaljevic, V.; Bozic, V.; Zivotic, M.; Tatic, S.; Dundjerovic, D. Comprehensive Investigation of Angiogenesis, PASS Score and Immunohistochemical Factors in Risk Assessment of Malignancy for Paraganglioma and Pheochromocytoma. Diagnostics 2024, 14, 849. https://doi.org/10.3390/diagnostics14080849
Milinkovic M, Soldatovic I, Zivaljevic V, Bozic V, Zivotic M, Tatic S, Dundjerovic D. Comprehensive Investigation of Angiogenesis, PASS Score and Immunohistochemical Factors in Risk Assessment of Malignancy for Paraganglioma and Pheochromocytoma. Diagnostics. 2024; 14(8):849. https://doi.org/10.3390/diagnostics14080849
Chicago/Turabian StyleMilinkovic, Marija, Ivan Soldatovic, Vladan Zivaljevic, Vesna Bozic, Maja Zivotic, Svetislav Tatic, and Dusko Dundjerovic. 2024. "Comprehensive Investigation of Angiogenesis, PASS Score and Immunohistochemical Factors in Risk Assessment of Malignancy for Paraganglioma and Pheochromocytoma" Diagnostics 14, no. 8: 849. https://doi.org/10.3390/diagnostics14080849
APA StyleMilinkovic, M., Soldatovic, I., Zivaljevic, V., Bozic, V., Zivotic, M., Tatic, S., & Dundjerovic, D. (2024). Comprehensive Investigation of Angiogenesis, PASS Score and Immunohistochemical Factors in Risk Assessment of Malignancy for Paraganglioma and Pheochromocytoma. Diagnostics, 14(8), 849. https://doi.org/10.3390/diagnostics14080849