
Advanced Respiratory Failure Requiring Tracheostomy—A Marker of Unfavourable Prognosis after Heart Transplantation
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study
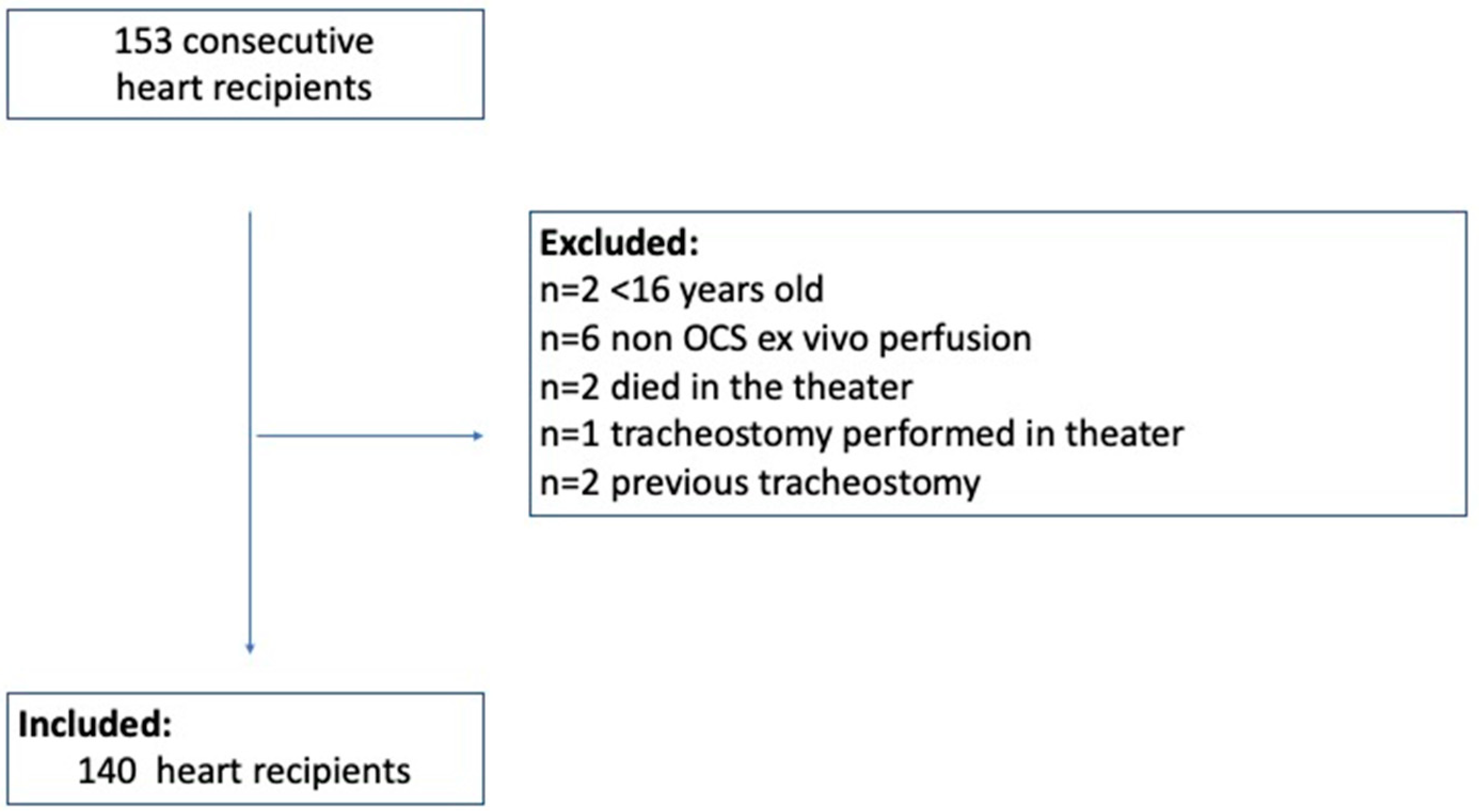
2.2. Population
2.3. Tracheostomy
2.4. Data Collection
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Cardiac index |
| CPB | Cardiopulmonary bypass |
| cf-LVAD | continuous flow left ventricle assist devices |
| ECMO | extra-corporeal membrane oxygenation |
| LVAD | left ventricular assist devices |
| IQR | interquartile range |
| ITU | Intensive therapy unit |
| MCS | Mechanical Circulatory Support |
| OCS | Organ Care System |
| SOFA | Sequential Organ Failure Assessment score |
| SD | standard deviation |
| TT | tracheostomy |
| UK | United Kingdom |
References
- De Leyn, P.; Bedert, L.; Delcroix, M.; Depuydt, P.; Lauwers, G.; Sokolov, Y.; Van Meerhaeghe, A.; Van Schil, P. Tracheotomy: Clinical review and guidelines. EJCTS 2007, 32, 412–421. [Google Scholar]
- Ben-Avi, R.; Ben-Nun, A.; Levin, S.; Simansky, D.; Zeitlin, N.; Sternik, L.; Raanani, E.; Kogan, A. Tracheostomy after cardiac surgery: Timing of tracheostomy as a risk factor for mortality. J. Cardiothorac. Vasc. Anesth. 2014, 28, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Wang, S.; Du, Y.; Song, Y.; Le, S.; Wang, H.; Zhang, A.; Huang, X.; Wu, L.; Du, X. A Predictive Scoring Model for Postoperative Tracheostomy in Patients Who Underwent Cardiac Surgery. Front. Cardiovasc. Med. 2022, 8, 799605. [Google Scholar] [CrossRef] [PubMed]
- Pilarczyk, K.; Carstens, H.; Heckmann, J.; Lubarski, J.; Marggraf, G.; Jakob, H.; Pizanis, N.; Kamler, M. Safety and Efficiency of Percutaneous Dilatational Tracheostomy with Direct Bronchoscopic Guidance for Thoracic Transplant Recipients. Respir. Care 2016, 61, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Załęska-Kocięcka, M.; Dutton, J.; Morosin, M.; Garda, R.F.; Piotrowska, K.; Lees, N.; Aw, T.; Sáez, D.G.; Simon, A.R.; Stock, U.; et al. Prognostic significance of serum lactate following cardiac transplantation. Biomark. Med. 2022, 16, 599–611. [Google Scholar] [CrossRef] [PubMed]
- NHS Blood and Transplant Organ Donation and Transplantation. Available online: https://www.odt.nhs.uk/transplantation/tools-policies-and-guidance/policies-and-guidance (accessed on 1 March 2019).
- Sharma, V.; Rao, V.; Manlhiot, C.; Boruvka, A.; Fremes, S.; Wąsowicz, M. A derived and validated score to predict prolonged mechanical ventilation in patients undergoing cardiac surgery. J. Thorac. Cardiovasc. Surg. 2017, 153, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Shenkman, Z.; Shir, Y.; Weiss, Y.G.; Bleiberg, B.; Gross, D. The effects of cardiac surgery on early and late pulmonary functions. Acta Anaesthesiol. Scand. 1997, 41, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Westerdahl, E.; Jonsson, M.; Emtner, M. Pulmonary function and health-related quality of life 1-year follow up after cardiac surgery. J. Cardiothorac. Surg. 2016, 11, 99. [Google Scholar] [CrossRef] [PubMed]
- Krebs, E.D.; Chancellor, W.Z.; Beller, J.P.; Mehaffey, J.H.; Hawkins, R.B.; Sawyer, R.G.; Yarboro, L.T.; Ailawadi, G.; Teman, N.R. Long-term Implications of Tracheostomy in Cardiac Surgery Patients: Decannulation and Mortality. Ann. Thorac. Surg. 2021, 111, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef]
- Hernández-Hernández, M.A.; Sánchez-Moreno, L.; Orizaola, P.; Iturbe, D.; Álvaréz, C.; Fernández-Rozas, S.; González-Novoa, V.; Llorca, J.; Hernández, J.L.; Fernández-Torre, J.L.; et al. A prospective evaluation of phrenic nerve injury after lung transplantation: Incidence, risk factors, and analysis of the surgical procedure. J. Heart Lung Transplant. 2022, 41, 50–60. [Google Scholar] [CrossRef]
- Wang, D.; Wang, S.; Song, Y.; Wang, H.; Zhang, A.; Wu, L.; Huang, X.; Ye, P.; Du, X. Predictors and outcomes of postoperative tracheostomy in patients undergoing acute type A aortic dissection surgery. BMC Cardiovasc. Disord. 2022, 22, 94. [Google Scholar] [CrossRef] [PubMed]
- Testelmans, D.; Nafteux, P.; Van Cromphaut, S.; Vrijsen, B.; Vos, R.; De Leyn, P.; Decaluwé, H.; Van Raemdonck, D.; Verleden, G.M.; Buyse, B. Feasibility of diaphragm pacing in patients after bilateral lung transplantation. Clin. Transplant. 2017, 31, e13134. [Google Scholar] [CrossRef] [PubMed]
- Toeg, H.; French, D.; Gilbert, S.; Rubens, F. Incidence of sternal wound infection after tracheostomy in patients undergoing cardiac surgery: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2017, 153, 1394–1400.e7. [Google Scholar] [CrossRef] [PubMed]
- Ballotta, A.; Kandil, H.; Generali, T.; Menicanti, L.; Pelissero, G.; Ranucci, M. Surgical and Clinical Outcome Research (SCORE) Group. Tracheostomy after cardiac operations: In-hospital and long-term survival. Ann. Thorac. Surg. 2011, 92, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.B.; Walkey, A.J.; Curran-Everett, D.; Douglas, I.S. One-Year Outcomes Following Tracheostomy for Acute Respiratory Failure. Crit. Care Med. 2019, 47, 1572–1581. [Google Scholar] [CrossRef] [PubMed]
- Annual Report on Cardiothoracic Organ Transplantation 2018/2019, NHS Blood and Transplant. Available online: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/16795/nhsbt-annual-report-on-cardiothoracic-organ-transplantation-201819.pdf (accessed on 1 March 2019).
- Whitbread, J.J.; Etchill, E.W.; Giuliano, K.A.; Suarez-Pierre, A.; Lawton, J.S.; Hsu, S.; Sharma, K.; Choi, C.W.; Higgins, R.S.D.; Kilic, A. Posttransplant Long-Term Outcomes for Patients with Ventricular Assist Devices on the Heart Transplant Waitlist. ASAIO J. 2022, 68, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Nakarada-Kordic, I.; Patterson, N.; Wrapson, J.; Reay, S.D. A Systematic Review of Patient and Caregiver Experiences with a Tracheostomy. Patient 2018, 11, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Young, D.; Harrison, D.A.; Cuthbertson, B.H.; Rowan, K.; TracMan Collaborators. Effect of early vs. late tracheostomy placement on survival in patients receiving mechanical ventilation: The TracMan randomized trial. JAMA 2013, 309, 2121–2129. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Watanuki, H.; Masato, T.; Sugiyama, K.; Futamura, Y.; Matsuyama, K. Impact of Tracheostomy Timing on Outcomes After Cardiovascular Surgery. J. Cardiothorac. Vasc. Anesth. 2022, 36, 2335–2338. [Google Scholar] [CrossRef] [PubMed]
- Zochios, V.; Casey, J.; Parhar, K.; Vuylsteke, A. Timing of tracheostomy and associated complications in cardiothoracic intensive care patients. Heart Lung Vessel. 2015, 7, 179–180. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Non-TT (n = 100) | TT (n = 40) | p-Values |
|---|---|---|---|
| Preoperative risk factors | |||
| Age, years (SD) | 44.9 (13.5) | 48.0 (14.4) | 0.235 |
| Sex (female) | 32% | 30% | 0.819 |
| Hypertension | 14% | 13% | 0.817 |
| History of stroke | 10% | 28% | 0.009 |
| Coronary artery disease | 24% | 30% | 0.463 |
| Diabetes | 9% | 5% | 0.427 |
| Smoking | 19% | 8% | 0.091 |
| Previous sternotomy | 33% | 58% | 0.008 |
| PreOHT MCS | 38% | 53% | 0.117 |
| COPD | 5% | 2.5% | 0.509 |
| Creatinine, μmol/L | 95.39 (31.9) | 88.2 (27.12) | 0.212 |
| Pulmonary resistance (woods unit; IQ) | 2.2 (1.4, 3.1) | 2.19 (1.5, 2.9) | 0.739 |
| Long term LVAD | 35% | 34% | 0.913 |
| Transplantation-related risk factors | |||
| OHT urgency: | |||
| Elective | 15% | 5% | 0.102 |
| Urgent | 80% | 85% | 0.492 |
| Emergent | 5% | 10% | 0.276 |
| Donor age, years | 40.8 (12.0) | 39.5 (11.4) | 0.574 |
| Recipient/Donor BSA ratio | 0.96 (0.90,1.02) | 0.99 (0.91,1.05) | 0.063 |
| Organ Care System duration, min (SD) | 259.5 (81.8) | 270.6 (71.9) | 0.456 |
| Cold ischaemia time, min (SD) | 78.8 (13.8) | 84.5 (13.9) | 0.045 |
| Cardiopulmonary bypass time, min (IQ) | 161.0 (142.5, 197.8) | 183.5 (152.5, 255.5) | 0.009 |
| Postoperative risk factors | |||
| Mean RBC transfusion up 72 h, mL (IQ) | 846.0 (612.7, 2185.0) | 1096.67 (784.7, 1706.0) | 0.795 |
| Maximum lactate in 24 h | 10.3 (3.8) | 11.9 (5.0) | 0.033 |
| Maximum lactate in 48 h | 3.26 (2.37) | 3.66 (2.21) | 0.361 |
| Maximum lactate in 72 h | 2.08 (1.14) | 2.29 (1.15) | 0.331 |
| Maximum bilirubin in 24 h | 36.00 (25.3, 48.0) | 40.00 (25.3, 70.0) | 0.206 |
| Maximum bilirubin in 48 h | 22.0 (14.0, 39.0) | 36.00 (18.0, 55.0) | 0.011 |
| Maximum bilirubin in 72 h | 17.0 (11.0, 27.0) | 28.00 (18.0, 44.3) | 0.001 |
| Maximum ALT in 24 h, IU (IQ) | 42.0 (28.0, 70.3) | 72.00 (37.0, 208.8) | 0.001 |
| Maximum ALT in 48 h, IU (IQ) | 42.0 (31.0, 72.0) | 128.00 (41.0, 211.0) | <0.001 |
| Maximum ALT in 72 h, IU (IQ) | 41.0 (27.0, 66.0) | 108.00 (35.3, 237.8) | <0.001 |
| Inotropic score 24 h (IQ) | 10.0 (7.0, 15.0) | 15.00 (10.0, 20.0) | <0.001 |
| Inotropic score 48 h (IQ) | 8.0 (5.0, 12.0) | 12.00 (10.0, 18.0) | <0.001 |
| Inotropic score 72 h (IQ) | 5.0 (2.0, 10.0) | 11.00 (8.5, 16.0) | <0.001 |
| Maximum SOFA score in 24 h (SD) | 15.3 (3.1) | 16.8 (2.4) | 0.007 |
| Maximum SOFA score in 48 h (SD) | 13.1 (4.5) | 16.5 (2.4) | <0.001 |
| Maximum SOFA score in 72 h (SD) | 11.0 (5.5) | 16.0 (2.7) | <0.001 |
| Outcomes | |||
| Primary graft failure | 14% | 52.5% | <0.001 |
| RRT | 67% | 98% | <0.001 |
| Duration of RRT, days (IQ) | 4.5 (1.5, 10) | 30.2 (20.2, 68.6) | <0.001 |
| Duration of mechanical ventilation, days (IQ) | 2.07 (1.4, 4.0) | 22.29 (14.1, 55.2) | <0.001 |
| Duration of ITU stay, days (IQ) | 6.00 (4.0, 8.0) | 28.50 (21.0, 49.8) | <0.001 |
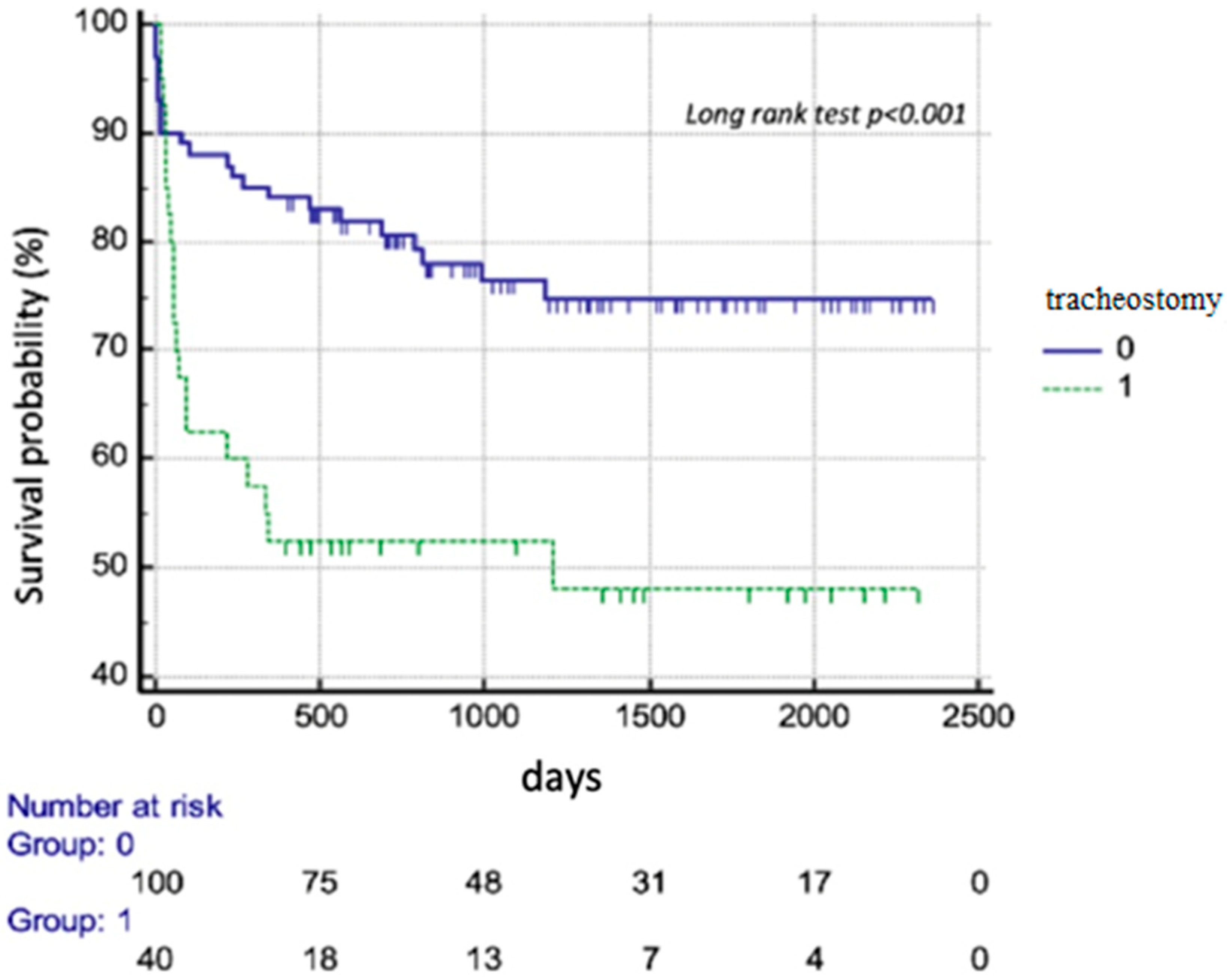
| 30-day mortality | 10% | 13% | 0.666 |
| 90-day mortality | 11% | 35% | <0.001 |
| 1-year mortality | 16% | 50% | <0.001 |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| History of stroke/TIA | 3.41 | 1.32–8.86 | 0.012 |
| Pre-transplant sternotomy | 2.5 | 1.18–5.32 | 0.017 |
| Cardiopulmonary bypass time | 1.01 | 1–1.01 | 0.007 |
| Mean SOFA up to 72 h | 1.50 | 1.23–1.71 | <0.01 |
| RRT in ITU | 19.2 | 2.53–146 | 0.004 |
| Primary graft failure | 6.79 | 2.93–15.71 | <0.001 |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | 0.99 | 0.96–1.03 | 0.758 |
| Female sex | 0.80 | 0.26–2.41 | 0.689 |
| History of stroke/TIA | 2.63 | 0.73–9.43 | 0.138 |
| Pre-transplant sternotomy | 3.14 | 1.15–8.56 | 0.025 |
| Cardiopulmonary bypass time | 0.99 | 0.99–1.00 | 0.169 |
| Mean SOFA up to 72 h | 1.28 | 1.04–1.57 | 0.018 |
| RRT in ITU | 7.92 | 0.86–73.42 | 0.068 |
| Primary graft failure | 4.5 | 1.37–214.77 | 0.013 |
| Variables | HR | 95% CI | p-Value |
|---|---|---|---|
| Tracheostomy | 0.70 | 0.31–1.60 | 0.396 |
| Pre-transplant sternotomy | 1.72 | 0.85–3.50 | 0.133 |
| Cardiopulmonary bypass time | 1.0 | 0.99–1.0 | 0.656 |
| Mean SOFA up to 72 h | 1.05 | 0.90–1.21 | 0.546 |
| RRT in ITU | 1.31 | 0.38–4.53 | 0.667 |
| Primary graft failure | 6.96 | 2.92–16.56 | <0.001 |
| History of stroke | 2.1 | 0.97–4.43 | 0.058 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Załęska-Kocięcka, M.; Morosin, M.; Dutton, J.; Garda, R.F.; Piotrowska, K.; Lees, N.; Aw, T.-C.; Saez, D.G.; Doce, A.H. Advanced Respiratory Failure Requiring Tracheostomy—A Marker of Unfavourable Prognosis after Heart Transplantation. Diagnostics 2024, 14, 851. https://doi.org/10.3390/diagnostics14080851
Załęska-Kocięcka M, Morosin M, Dutton J, Garda RF, Piotrowska K, Lees N, Aw T-C, Saez DG, Doce AH. Advanced Respiratory Failure Requiring Tracheostomy—A Marker of Unfavourable Prognosis after Heart Transplantation. Diagnostics. 2024; 14(8):851. https://doi.org/10.3390/diagnostics14080851
Chicago/Turabian StyleZałęska-Kocięcka, Marta, Marco Morosin, Jonathan Dutton, Rita Fernandez Garda, Katarzyna Piotrowska, Nicholas Lees, Tuan-Chen Aw, Diana Garcia Saez, and Ana Hurtado Doce. 2024. "Advanced Respiratory Failure Requiring Tracheostomy—A Marker of Unfavourable Prognosis after Heart Transplantation" Diagnostics 14, no. 8: 851. https://doi.org/10.3390/diagnostics14080851
APA StyleZałęska-Kocięcka, M., Morosin, M., Dutton, J., Garda, R. F., Piotrowska, K., Lees, N., Aw, T. -C., Saez, D. G., & Doce, A. H. (2024). Advanced Respiratory Failure Requiring Tracheostomy—A Marker of Unfavourable Prognosis after Heart Transplantation. Diagnostics, 14(8), 851. https://doi.org/10.3390/diagnostics14080851