
Spontaneous Intracranial Hypotension: Case Report and Update on Diagnosis and Treatment

Abstract
:1. Introduction
2. Case Report
2.1. Clinical Data
2.2. Initial Evaluation and Treatment
2.3. Follow-Up
2.4. Management
2.5. Discussion
3. Update on the Etiology, Diagnosis, and Management of Spontaneous Intracranial Hypotension
3.1. Clinical Presentation
3.1.1. Headache
3.1.2. Neck and Back Pain
3.1.3. Auditory Disturbances
3.1.4. Ocular Findings
3.1.5. Other Cranial Nerve Symptoms
3.1.6. Altered Mental Status
3.1.7. Motor Abnormalities
3.1.8. Other Symptoms
3.2. Evaluation
3.2.1. Lumbar Puncture
3.2.2. Imaging of the Brain
- -
- Diffuse pachymeningeal enhancement is detected in 73–83% of cases [19,32]. The dural thickening is typically diffuse and non-nodular. It needs to be differentiated from immunoglobulin 4 (IgG4)-related pachymeningitis [33], neurosarcoidosis (pachymeningeal and/or leptomeningeal enhancement is most prominent at the skull base) [34], infectious meningitis (in tuberculous meningitis the leptomeninges is usually also involved, while in syphilitic, cryptococcal meningitis or Lyme disease the involvement of other organs and systems may provide useful clues to diagnosis [35], or a series of immune-mediated conditions, such as rheumatoid arthritis, temporal arteritis, polyangiitis with granulomatosis, in which the dural enhancement is rather nodular [32].
- -
- Subdural fluid collections—mostly bilateral hygromas—are described in 43–50% of patients [5,19]. Hygromas occur because of the enlargement of the subdural space secondary to the loss of the CSF, while subdural hematomas may be caused by tearing of the abnormally engorged and dilated cortical veins [32]. Drainage of these collections will not resolve them successfully if the CSF leak is not identified and treated [36].
- -
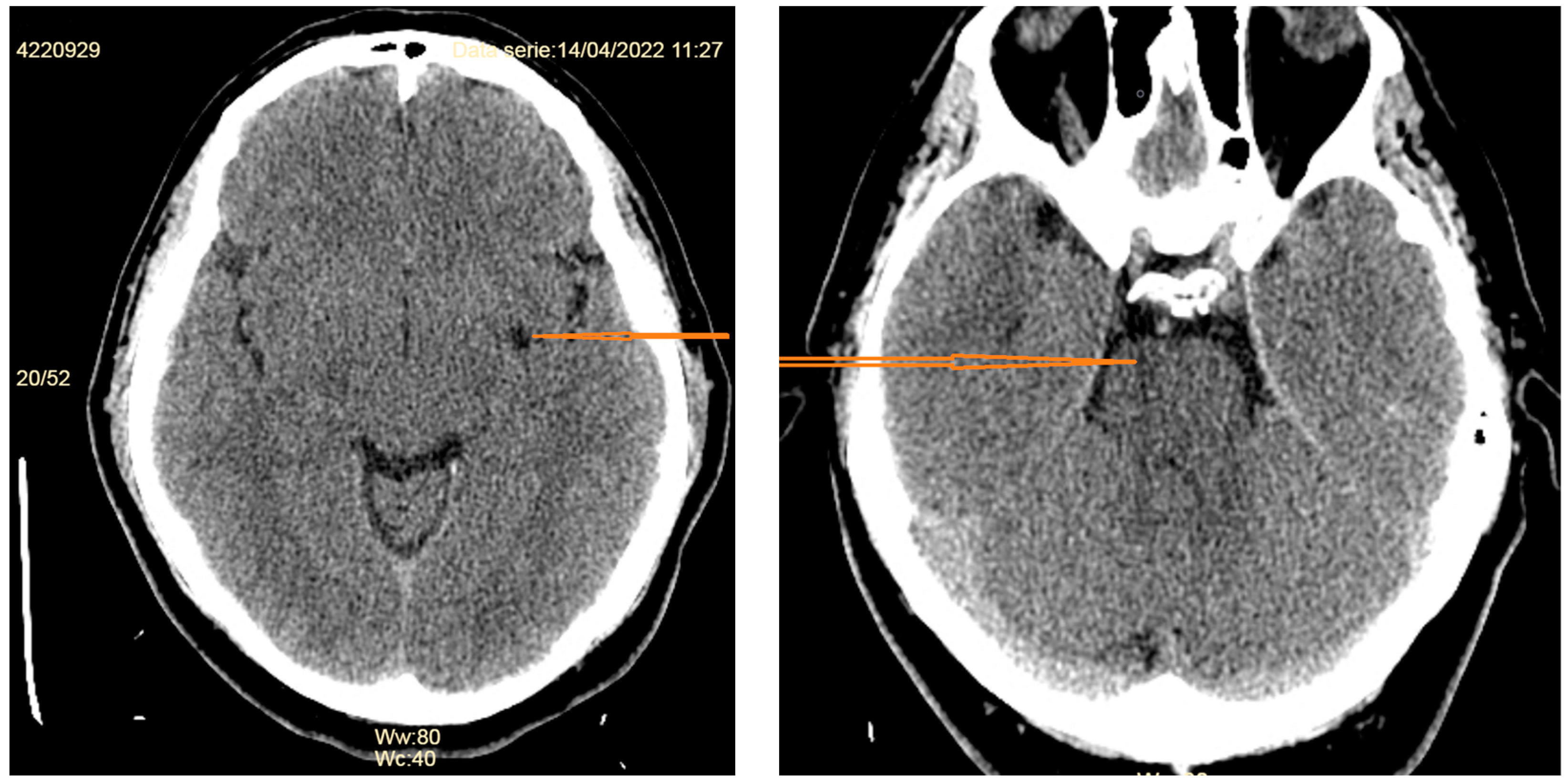
- Signs of brain sagging include flattening of the ventral pons, effacement of the prepontine and perichiasmatic cisterns, or downward displacement of the cerebellar tonsils and brain stem [5,8], which may mimic Chiari type 1 malformation. However, in SIH, the tonsils maintain normal shape and do not descend more than 5 mm below the foramen magnum [37]. Moreover, the findings associated with syringomyelia would argue for the diagnosis of Chiari type 1 malformation [32].
- -
- Dural venous sinus engorgement appears usually as a dilation of the transverse sinuses, which is subtle and often diagnosed retrospectively, by comparison of pre- and post-treatment images [5].
- -
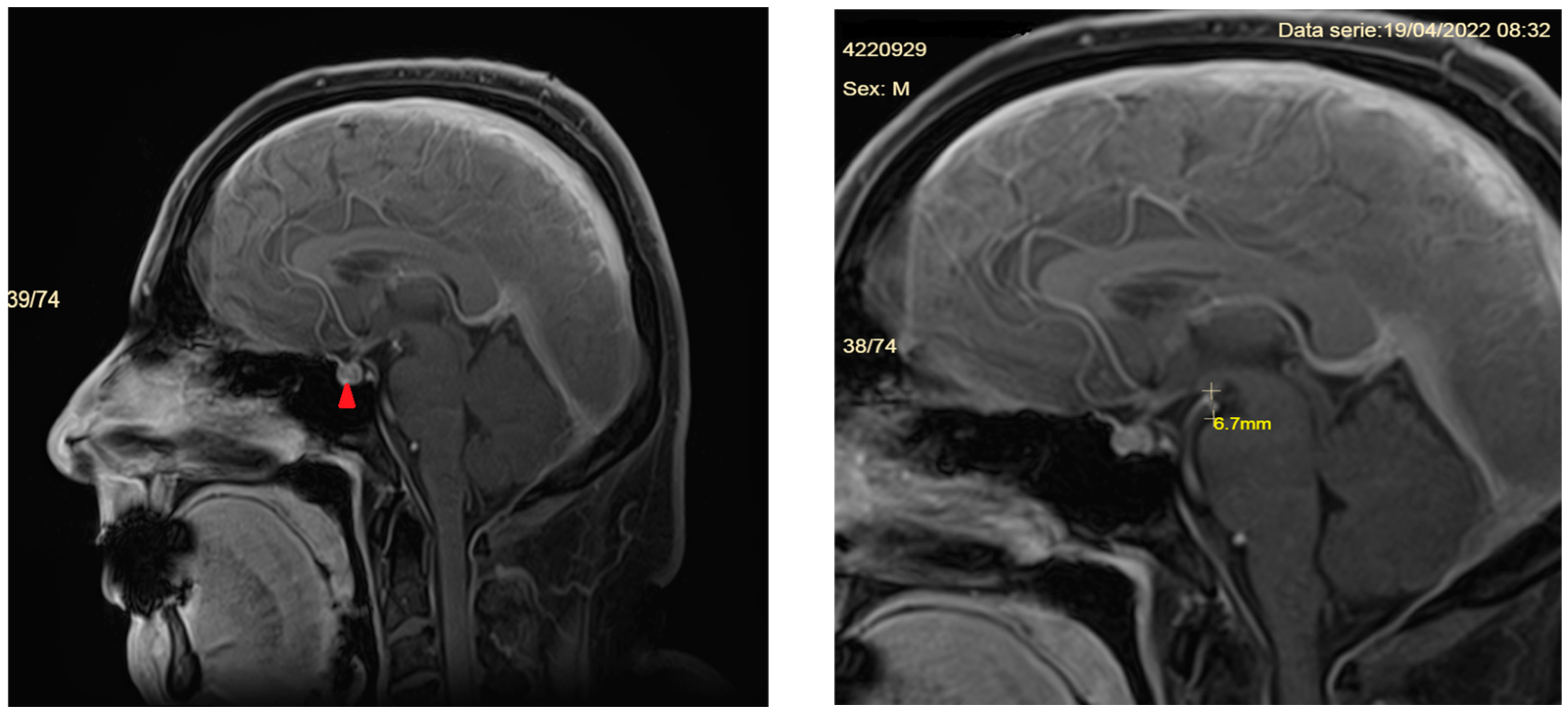
- Pituitary gland hyperemia leads to enlargement of the gland and can be mistaken for a pituitary adenoma [5].
- -
- Reduced optic nerve sheath diameter and thickness (normal—4.4 mm; reduced to a mean of 3.4 mm) is best measured on coronal T2-weighted images or with transorbital ultrasonography [38].
3.2.3. Imaging of the Spine
- A.
- MR imaging of the spine
- -
- Cervical pachymeningeal enhancement
- -
- Non-compressive spinal epidural fluid collections
- -
- Engorgement of the epidural venous plexus
- -
- Meningeal diverticula, dilated nerve root sleeves, that can be nonspecific unless very large and irregular [40]
- -
- Fluid collection in soft tissues near the C1–C2 vertebrae (but which sometimes may be a false CSF leak localizing sign)
- B.
- Computed tomography imaging of the spine
3.3. Diagnostic Criteria
- A.
- Any headache fulfilling criterion C
- B.
- Either or both of the following:
- I.
- Low cerebrospinal fluid (CSF) pressure (<60 mm H2O)
- II.
- Evidence of CSF leakage on imaging
- C.
- Headache has developed in temporal relation to the low CSF pressure or CSF leakage or led to its discovery
- D.
- Not better accounted for by another ICHD-3 diagnosis
- Headache attributed to low cerebrospinal fluid (CSF) pressure is usually but not invariably orthostatic. Headache that significantly worsens soon after sitting upright or standing and/or improves after lying horizontally is likely to be caused by low CSF pressure, but this cannot be relied upon as a diagnostic criterion.
- Brain imaging shows brain sagging or pachymeningeal enhancement, or spine imaging (spine MRI or MRI, CT, or digital subtraction myelography) showing extradural CSF.
- Evidence of causation may depend upon onset in temporal relation to the presumed cause, together with exclusion of other diagnoses.
3.4. Differential Diagnosis
3.4.1. Clinical Differential Diagnosis
3.4.2. Imagistic Differential Diagnosis
3.5. Treatment
3.5.1. Conservative Therapy
3.5.2. Epidural Blood Patch
3.5.3. Surgery
3.5.4. Complications of Treatment
4. Concluding Remarks
- Despite the general belief, SIH is not a rare disease, and even the incidence rate of 5/100,000/year is believed by some physicians to be an underestimation.
- The diagnosis is based on increased awareness and the correct interpretation of the ever-broadening spectrum of symptoms and signs, which should prompt imagistic evaluation, preferably contrast-enhanced magnetic resonance imaging of the brain.
- Diffuse, smooth dural enhancement detected on brain MRI is highly suggestive of SIH and should be rapidly followed by spinal imaging to detect the CSF leak.
- Although conservative treatment is the first step as therapy, it often fails to relieve the symptoms, and patients need to be referred to a neurosurgeon.
- Failure of 2–3 non-targeted epidural blood patches indicates the need for targeted approaches (epidural blood patch or fibrin glue) or surgical repair of the dural tear.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schievink, W.I. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA 2006, 295, 2286–2296. [Google Scholar] [CrossRef]
- Schievink, W.I.; Maya, M.M.; Moser, F.G.; Simon, P.; Nuño, M. Incidence of spontaneous intracranial hypotension in a community: Beverly Hills, California, 2006–2020. Cephalalgia 2022, 42, 312–316. [Google Scholar] [CrossRef]
- Schievink, W.I.; Maya, M.M.; Moser, F.; Tourje, J.; Torbati, S. Frequency of spontaneous intracranial hypotension in the emergency department. J. Headache Pain 2007, 8, 325–328. [Google Scholar] [CrossRef]
- Urbach, H.; Fung, C.; Dovi-Akue, P.; Lützen, N.; Beck, J. Spontaneous Intracranial Hypotension. Dtsch. Arztebl. Int. 2020, 117, 480–487. [Google Scholar] [CrossRef]
- Ferrante, E.; Trimboli, M.; Rubino, F. Spontaneous intracranial hypotension: Review and expert opinion. Acta Neurol. Belg. 2019, 120, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.P.; Zhang, S.D.; He, F.F.; Liu, M.J.; Ma, X.X. The status of diagnosis and treatment to intracranial hypotension, including SIH. J. Headache Pain 2017, 18, 4. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Lantéri-Minet, M.; Michel, M.C.; Peres, M.; Shibata, M.; Straube, A.; Wijeratne, T.; Ebel-Bitoun, C.; Constantin, L.; Hitier, S. 21st century headache: Mapping new territory. J. Headache Pain 2021, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W. Misdiagnosis of spontaneous intracranial hypotension. Arch Neurol. 2003, 60, 1713–1718. [Google Scholar] [CrossRef] [PubMed]
- Shah, L.M.; McLean, L.A.; Heilbrun, M.E.; Salzman, K.L. Intracranial hypotension: Improved MRI detection with diagnostic intracranial angles. AJR Am. J. Roentgenol. 2013, 200, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Kariev, G.M.; Asadullaev, U.M.; Duschanov, T.A.; Rasulov, S.O.; Mamadaliev, D.M.V.; Khodjimetov, D.N. The importance of measuring mamillopontine distance as a diagnostic criterion of hydrocephalus degrees. Asian J. Neurosurg. 2019, 14, 166. [Google Scholar] [CrossRef]
- Ljubisavljevic, S. Postdural puncture headache as a complication of lumbar puncture: Clinical manifestations, pathophysiology, and treatment. Neurol. Sci. 2020, 41, 3563–3568. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I.; Maya, M.M.; Jean-Pierre, S.; Nuño, M.; Prasad, R.S.; Moser, F.G. A classification system of spontaneous spinal CSF leaks. Neurology 2016, 87, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Kranz, P.G.; Malinzak, M.D.; Amrhein, T.J.; Gray, L. Update on the diagnosis and treatment of spontaneous intracranial hypotension. Curr. Pain Headache Rep. 2017, 21, 37. [Google Scholar] [CrossRef] [PubMed]
- Mokri, B.; Maher, C.O.; Sencakova, D. Spontaneous CSF leaks: Underlying disorder of connective tissue. Neurology 2002, 58, 814–816. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I.; Meyer, F.B.; Atkinson, J.L.D.; Mokri, B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J. Neurosurg. 1996, 84, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Casanova, A.; Entz, L.; Weinmann, S.; Wanke, I.; Reisch, R. Bilateral subdural hematoma caused by spontaneous intracranial hypotension originating from a discogenic microspur successfully treated with duraplasty: A case report. Brain Spine 2022, 2, 100879. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I.; Moser, F.G.; Maya, M.M. CSF-venous fistula in spontaneous intracranial hypotension. Neurology 2014, 83, 472–473. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I.; Goseland, A.; Cunneen, S. Bariatric surgery as a possible risk factor for spontaneous intracranial hypotension. Neurology 2014, 83, 1819–1822. [Google Scholar] [CrossRef]
- D’Antona, L.; Jaime Merchan, M.A.; Vassiliou, A.; Watkins, L.D.; Davagnanam, I.; Toma, A.K.; Matharu, M.S. Clinical Presentation, Investigation Findings, and Treatment Outcomes of Spontaneous Intracranial Hypotension Syndrome: A Systematic Review and Meta-analysis. JAMA Neurol. 2021, 78, 329–337. [Google Scholar] [CrossRef]
- Perez-Vega, C.; Robles-Romelin, P.; Robles-Romelin, I.; Navarro, V.G. Spontaneous intracranial hypotension: Key features for a frequently misdiagnosed disorder. Neurol. Sci. 2020, 41, 2433–2441. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International headache Society (HIS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Pistacchi, M.; Pezzato, A.; Rudà, R.; Gioulis, M.; Contin, F.; Fragiacomo, F.; Marsala, S.Z. Spontaneous intracranial hypotension: A case series and literature review. Folia Neuropathol. 2023, 61, 225–234. [Google Scholar] [CrossRef]
- Luetzen, N.; Dovi-Akue, P.; Fung, C.; Beck, J.; Urbach, H. Spontaneous intracranial hypotension: Diagnostic and therapeutic workup. Neuroradiology 2021, 63, 1765–1772. [Google Scholar] [CrossRef]
- Idrissi, A.L.; Lacour, J.C.; Klein, O.; Schmitt, E.; Ducrocq, X.; Richard, S. Spontaneous intracranial hypotension: Characteristics of the serious form in a series of 24 patients. World Neurosurg. 2015, 84, 1613–1620. [Google Scholar] [CrossRef]
- Upadhyaya, P.; Ailani, J. A review of spontaneous intracranial hypotension. Curr. Neurol. Neurosci. Rep. 2019, 19, 22. [Google Scholar] [CrossRef]
- Lashkarivand, A.; Eide, P.K. Brain Sagging Dementia-Diagnosis, Treatment, and Outcome: A Review. Neurology 2022, 98, 798–805. [Google Scholar] [CrossRef]
- Schievink, W.I.; Jean-Pierre, S.; Maya, M.M.; Moser, F.G.; Nuño, M. Coma: A serious complication of spontaneous intracranial hypotension. Neurology 2018, 90, E1638–E1645. [Google Scholar] [CrossRef]
- Duvall, J.R.; Robertson, C.E.; Cutsforth-Gregory, J.K.; Carr, C.M.; Atkinson, J.L.D.; Garza, I. Headache due to spontaneous spinal cerebrospinal fluid leak secondary to cerebrospinal fluid-venous fistula: Case series. Cephalalgia 2019, 39, 1847–1854. [Google Scholar] [CrossRef]
- Schievink, W.I.; Nuño, M.; Rozen, T.D.; Maya, M.M.; Mamelak, A.N.; Carmichael, J.; Bonert, V.S. Hyperprolactinemia due to spontaneous intracranial hypotension. J. Neurosurg. 2015, 122, 1020–1025. [Google Scholar] [CrossRef]
- Schievink, W.I.; Chu, R.M.; Maya, M.M.; Johnson, J.P.; Cohen, H.C.M. Spinal manifestations of spontaneous intracranial hypotension: Clinical article. J. Neurosurg. Spine 2013, 18, 96–101. [Google Scholar] [CrossRef]
- Fermo, O.P. Evaluation and management of orthostatic headache in hypermobility disorders. Front. Neurol. 2023, 14, 1321350. [Google Scholar] [CrossRef] [PubMed]
- Bond, K.M.; Benson, J.C.; Cutsforth-Gregory, J.K.; Kim, D.K.; Diehn, F.E.; Carr, C.N. Spontaneous intracranial hypotension: Atypical radiologic appearances, imaging mimickers, and clinical look-alikes. Am. J. Neuroradiol. 2020, 41, 1339–1347. [Google Scholar] [CrossRef]
- Yu, H.; Lu, C.; Duan, W.; Dong, Y.; Wang, Z.; Wang, X.; Jian, F. A selected case series of idiopathic hypertrophic pachymeningitis in a single center: Pathological characteristics and case-oriented review. J. Neuroimmunol. 2023, 383, 578191. [Google Scholar] [CrossRef] [PubMed]
- Chakales, P.A.; Herman, M.C.; Chien, L.C.; Hutto, S.K. Pachymeningitis in Biopsy-Proven Sarcoidosis: Clinical Course, Radiographic Findings, Response to Treatment, and Long-term Outcomes. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e200028. [Google Scholar] [CrossRef]
- Bystritsky, R.J.; Chow, F.C. Infectious Meningitis and Encephalitis. Neurol. Clin. 2022, 40, 77–91. [Google Scholar] [CrossRef]
- Chen, H.C.; Chen, P.L.; Chai, J.W.; Teng, C.J. Risk factors for nonresponsive hydration in patients with spinal cerebrospinal fluid leakage. BMC Neurol. 2021, 21, 427. [Google Scholar] [CrossRef]
- Holbrook, J.; Saindane, A.M. Imaging of intracranial pressure disorders. Neurosurgery 2017, 80, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Müller, S.J.; Henkes, E.; Gounis, M.J.; Felber, S.; Ganslandt, O.; Henkes, H. Non-Invasive Intracranial Pressure Monitoring. J. Clin. Med. 2023, 12, 2209. [Google Scholar] [CrossRef]
- Kranz, P.G.; Gray, L.; Malinzak, M.D.; Amrhein, T.J. Spontaneous intracranial hypotension: Pathogenesis, diagnosis, and treatment. Neuroimag. Clin. N. Am. 2019, 29, 581–594. [Google Scholar] [CrossRef]
- Kranz, P.G.; Stinett, S.S.; Huang, K.T.; Gray, L. Spinal meningeal diverticula in spontaneous intracranial hypotension: Analysis of prevalence and myelographic appearance. AJNR Am. J. Neuroradiol. 2013, 34, 1284–1289. [Google Scholar] [CrossRef]
- Dobrocky, T.; Winklehner, A.; Breiding, P.S.; Grunder, L.; Peschi, G.; Häni, L.; Mosimann, P.J.; Branca, M.; Kaesmacher, J.; Mordasini, P.; et al. Spine MRI in Spontaneous Intracranial Hypotension for CSF Leak Detection: Nonsuperiority of Intrathecal Gadolinium to Heavily T2-Weighted Fat-Saturated Sequences. AJNR Am. J. Neuroradiol. 2020, 41, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Mallio, C.A.; Rovira, À.; Parizel, P.M.; Quattrocchi, C.C. Exposure to gadolinium and neurotoxicity: Current status of preclinical and clinical studies. Neuroradiology 2020, 62, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Ayers-Ringler, J.; McDonald, J.S.; Connors, M.A.; Fisher, C.R.; Han, S.; Jakaitis, D.R.; Scherer, B.; Tutor, G.; Wininger, K.M.; Dai, D.; et al. Neurologic Effects of Gadolinium Retention in the Brain after Gadolinium-based Contrast Agent Administration. Radiology 2022, 302, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I.; Maya, M.M.; Moser, F.G.; Prasad, R.S.; Cruz, R.B.; Nuño, M.; Farb, R.I. Lateral decubitus digital subtraction myelography to identify spinal CSF-venous fistulas in spontaneous intracranial hypotension. J. Neurosurg. Spine 2019, 13, 902–905. [Google Scholar] [CrossRef] [PubMed]
- Kranz, P.G.; Amrhein, T.J.; Gray, L. CSF venous fistulas in spontaneous intracranial hypotension: Imaging characteristics on dynamic and CT myelography. AJR Am. J. Roentgenol. 2017, 209, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Lützen, N.; Kremers, N.; Fung, C.; Beck, J.; Urbach, H. The “hyperdense basivertebral vein” sign: Another marker of a CSF-venous fistula. Neuroradiology 2022, 64, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, A.A.; Yu, L.; Brinjikji, W.; Cutsforth-Gregory, J.K.; Schwartz, F.R.; Mark, I.T.; Benson, J.C.; Amrhein, T.J. Utility of Photon-Counting Detector CT Myelography for the Detection of CSF-Venous Fistulas. AJNR Am. J. Neuroradiol. 2023, 44, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A. Postural orthostatic tachycardia syndrome: Clinical presentation, aetiology and management. J. Intern. Med. 2019, 285, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Khurana, R.K. Coat-hanger ache in orthostatic hypotension. Cephalalgia 2012, 32, 731–737. [Google Scholar] [CrossRef]
- Bogduk, N. The neck and headaches. Neurol. Clin. 2014, 32, 471–487. [Google Scholar] [CrossRef]
- Staab, J.P.; Eckhardt-Henn, A.; Horii, A.; Jacob, R.; Strupp, M.; Brandt, T.; Bronstein, A. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society. J. Vestib. Res. 2017, 27, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Matias, T.B.; Cordeiro, R.A.; Duarte, J.A.; de Jarry, V.M.; Appenzeller, S.; Villarinho, L.; Reis, F. Immune-Mediated Hypertrophic Pachymeningitis and its Mimickers: Magnetic Resonance Imaging Findings. Acad. Radiol. 2023, 30, 2696–2706. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, J.; Shimojima, Y.; Yamada, A.; Sekijima, Y. Quantitative evaluation of the thickened dura mater impacting clinical signs in immune-mediated hypertrophic pachymeningitis. J. Neurol. Sci. 2023, 453, 120780. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Ray, B.K.; Pandit, A.; Kumar, K.; Dubey, S. Characteristic Array of Imaging Markers in Central Nervous System Tuberculosis. J. Glob. Infect. Dis. 2023, 15, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.S. Subdural Lesions Linking Additional Intracranial Spaces and Chronic Subdural Hematomas: A Narrative Review with Mutual Correlation and Possible Mechanisms behind High Recurrence. Diagnostics 2023, 13, 235. [Google Scholar] [CrossRef]
- Ducros, A.; Biousse, V. Headache arising from idiopathic changes in CSF pressure. Lancet Neurol. 2015, 14, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Kong, D.-S.; Park, K.; Nam, D.H.; Lee, J.I.; Kim, J.S.; Eoh, W.; Kim, J.H. Clinical features and long-term results of spontaneous intracranial hypotension. Neurosurgery 2005, 57, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Sencakova, D.; Mokri, B.; McClelland, R.L. The efficacy of epidural blood patch in spontaneous CSF leaks. Neurology 2001, 57, 1921–1923. [Google Scholar] [CrossRef] [PubMed]
- Massourou, Z.; Papagiannakis, N.; Mantzikopoulos, G.; Mitsikostas, D.-D.; Theodoraki, K. Treating spontaneous intracranial hypotension with an anesthetic modality: The role of the epidural blood patch. Life 2022, 12, 1109. [Google Scholar] [CrossRef]
- Shin, H.Y. Recent update on epidural blood patch. Anesth. Pain Med. 2022, 17, 12–23. [Google Scholar] [CrossRef]
- Zetlaoui, P.J.; Buchheit, T.; Benhamou, D. Epidural blood patch: A narrative review. Anaesth. Crit. Care Pain Med. 2022, 41, 101138. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Raabe, A.; Schievink, W.I.; Fung, C.; Gralla, J.; Piechowiak, E.; Seidel, K.; Ulrich, C.T. Posterior approach and spinal cord release for 360° repair of dural defects in spontaneous intracranial hypotension. Neurosurgery 2018, 84, E345–E351. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Hubbe, U.; Klingler, J.H.; Roelz, R.; Kraus, L.M.; Volz, F.; Lützen, N.; Urbach, H.; Kieselbach, K.; Fung, C. Minimally invasive surgery for spinal cerebrospinal fluid leaks in spontaneous intracranial hypotension. J. Neurosurg. Spine 2022, 38, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Maresca, L.; Fragale, M.; Petrella, G.; Boeris, D. Management of post blood patch severe rebound intracranial hypertension by the usage of an external ventricular drain. BMJ Case Rep. 2024, 17, e257743. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disorders | Common Features | Distinguishing Features | Ref. |
|---|---|---|---|
| Postural orthostatic tachycardia syndrome (POTS) | Headache worsening in the upright posture | Increasing heart rate on standing from supine position with negligible changes in blood pressure | [48] |
| Orthostatic hypotension (etiologies: autonomic failure, hypovolemia, medication adverse effects) | Orthostatic headache, worsened by Valsalva maneuvers, + pain in the neck and shoulders (“coat-hanger” pain) caused by ischemia of the paraspinal muscles, +/− tinnitus | Fall in systolic blood pressure (>20 mm Hg) and/or diastolic blood pressure (>10 mm Hg) during standing from seating or supine position, or on the head-up tilt test | [49] |
| Cervicogenic headache (etiology: osteoarthritis of the atlanto-occipital junction and/or upper cervical spine) | Headache worsens in upright posture (due to axial loading of the spine) + neck pain | Usually unilateral, movement of the neck worsens neck pain; digital pressure on neck muscles may augment the neck pain | [50] |
| Persistent postural perceptual dizziness | Unsteadiness, nausea +/− headache in upright posture | Nausea and unsteadiness more prominent, headache occurs only occasional | [51] |
| Condition | Common Features | Distinguishing Features | Ref. |
|---|---|---|---|
| IgG4-related hypertrophic pachymeningitis | Thickened, enhancing dura extending into the cervical canal | Increased IgG4, fibrosis can manifest in many organs, leading to a variety of presentations | [33] |
| Neurosarcoidosis | Pachymeningeal enhancement, clinical picture of cranial nerve damage | Pachymeningeal and/or leptomeningeal enhancement more prominent along the skull base, increased serum angiotensin convertase | [52] |
| Autoimmune diseases (rheumatoid arthritis, polyangiitis with granulomatosis, temporal arteritis) | Dural thickening and enhancement | Typical serologic findings | [53] |
| Tuberculous meningitis | Dural thickening and enhancement | Can also affect the leptomeninges, form intracranial tuberculomas, may associate spinal tuberculous arachnoiditis | [54] |
| Other infectious causes of pachymeningitis (syphilis, Cryptococcus, Lyme disease) | Pachymeningeal enhancement | Affect multiple organ systems beyond the nervous system, serologic findings | [32] |
| Chiari malformation type 1 | Cerebellar tonsillar descent | In Chiari malformation the cerebellar tonsils are inferiorly pointed and descend more than 5 mm below the foramen magnus, whereas in SIH they maintain normal shape and descent in the foramen magnus is <5 mm; midbrain descent presents in SIH | [37] |
| Subdural fluid collections | Mostly unilateral, occurring after trauma or in elderly, precipitated by anticoagulation, whereas in SIH they are usually bilateral, accompanied by dural enhancement and signs of brain sagging | [55] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurcau, M.C.; Jurcau, A.; Hogea, V.O.; Diaconu, R.G. Spontaneous Intracranial Hypotension: Case Report and Update on Diagnosis and Treatment. Diagnostics 2024, 14, 881. https://doi.org/10.3390/diagnostics14090881
Jurcau MC, Jurcau A, Hogea VO, Diaconu RG. Spontaneous Intracranial Hypotension: Case Report and Update on Diagnosis and Treatment. Diagnostics. 2024; 14(9):881. https://doi.org/10.3390/diagnostics14090881
Chicago/Turabian StyleJurcau, Maria Carolina, Anamaria Jurcau, Vlad Octavian Hogea, and Razvan Gabriel Diaconu. 2024. "Spontaneous Intracranial Hypotension: Case Report and Update on Diagnosis and Treatment" Diagnostics 14, no. 9: 881. https://doi.org/10.3390/diagnostics14090881
APA StyleJurcau, M. C., Jurcau, A., Hogea, V. O., & Diaconu, R. G. (2024). Spontaneous Intracranial Hypotension: Case Report and Update on Diagnosis and Treatment. Diagnostics, 14(9), 881. https://doi.org/10.3390/diagnostics14090881