
Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction

2. Methodological Shortcomings of the Development Procedure of Systemic Exercise Intolerance Disease (SEID)
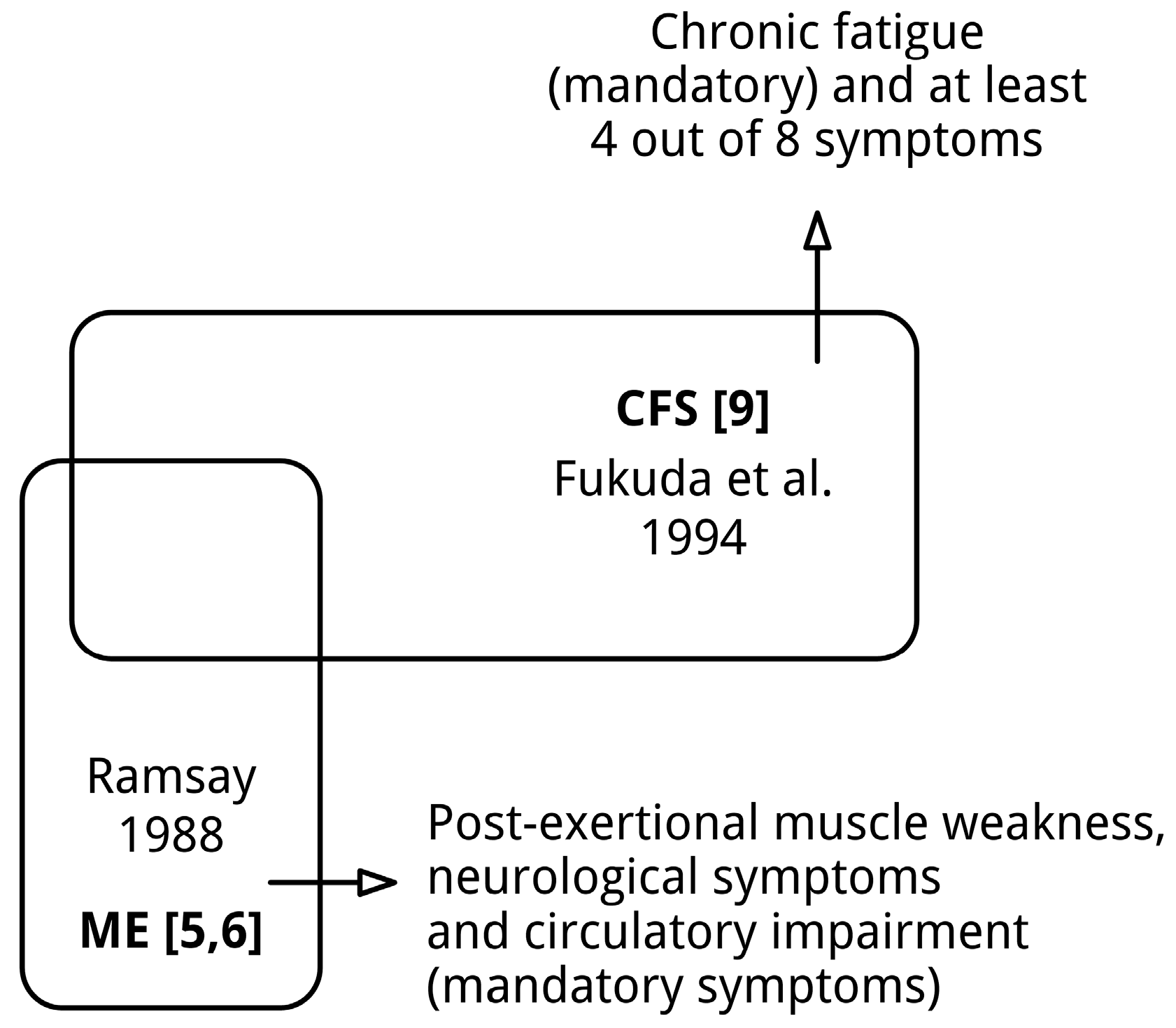
2.1. The Pre-Assumption that Myalgic Encephalomyelitis (ME) and Chronic Fatigue Syndrome (CFS) Denote “Similar Conditions” Is Invalid
- A unique form of muscle fatiguability: prolonged muscle weakness (and myalgia), lasting for days, even after a minor degree of physical effort (*1).
- Circulatory impairment, implicated by cold extremities and hypersensitivity to climatic change, but above all an ashen-grey facial pallor approximately 20 or 30 min before the patient complains of feeling ill.
- Cerebral dysfunction: impairment of memory and concentration and emotional lability, alterations of sleep rhythm (*2), vivid dreams (*2), episodic sweating and orthostatic tachycardia as cardinal features (the latter two not always present).
- Variability and fluctuation of both symptoms and physical findings over the day.
- A tendency to become chronic.
List 2. The diagnostic criteria of CFS [9].
- Severe chronic_fatigue for 6 or more consecutive months, that is not due to ongoing exertion or other medical conditions associated with fatigue and significantly interferes with daily activities and work,
- Accompanied by at least 4 or more of the following 8 symptoms:
- post-exertional malaise lasting more than 24 h (*1);
- unrefreshing sleep (*2);
- significant impairment of short-term memory or concentration;
- muscle pain;
- joint pain without swelling or redness;
- headaches of a new type, pattern, or severity;
- tender lymph nodes in the neck or armpit; and
- a sore throat that is frequent or recurring.
- chronic fatigue for 6 or more consecutive months;
- unrefreshing sleep;
- significant impairment of short-term memory or concentration;
- headaches of a new type, pattern, or severity; and
- a sore throat that is frequent or recurring.
- prolonged muscle weakness and muscle pain after minimal exertion;
- circulatory impairment, e.g., indicated by cold extremities, disturbed thermoregulation, low body temperature, and orthostatic tachycardia; and
- cognitive impairment and other symptoms indicating neurological dysfunction.
2.2. The Literature Analyzed by the Medicine (IOM) Committee Largely Relates to CFS Research
2.3. Consensus on “an Unclear Picture of the Symptoms” in a Heterogeneous Patient Group Does Not Guarantee a Good Solution
3. Diagnostic Shortcomings of the New Definition for “ME/CFS”: SEID
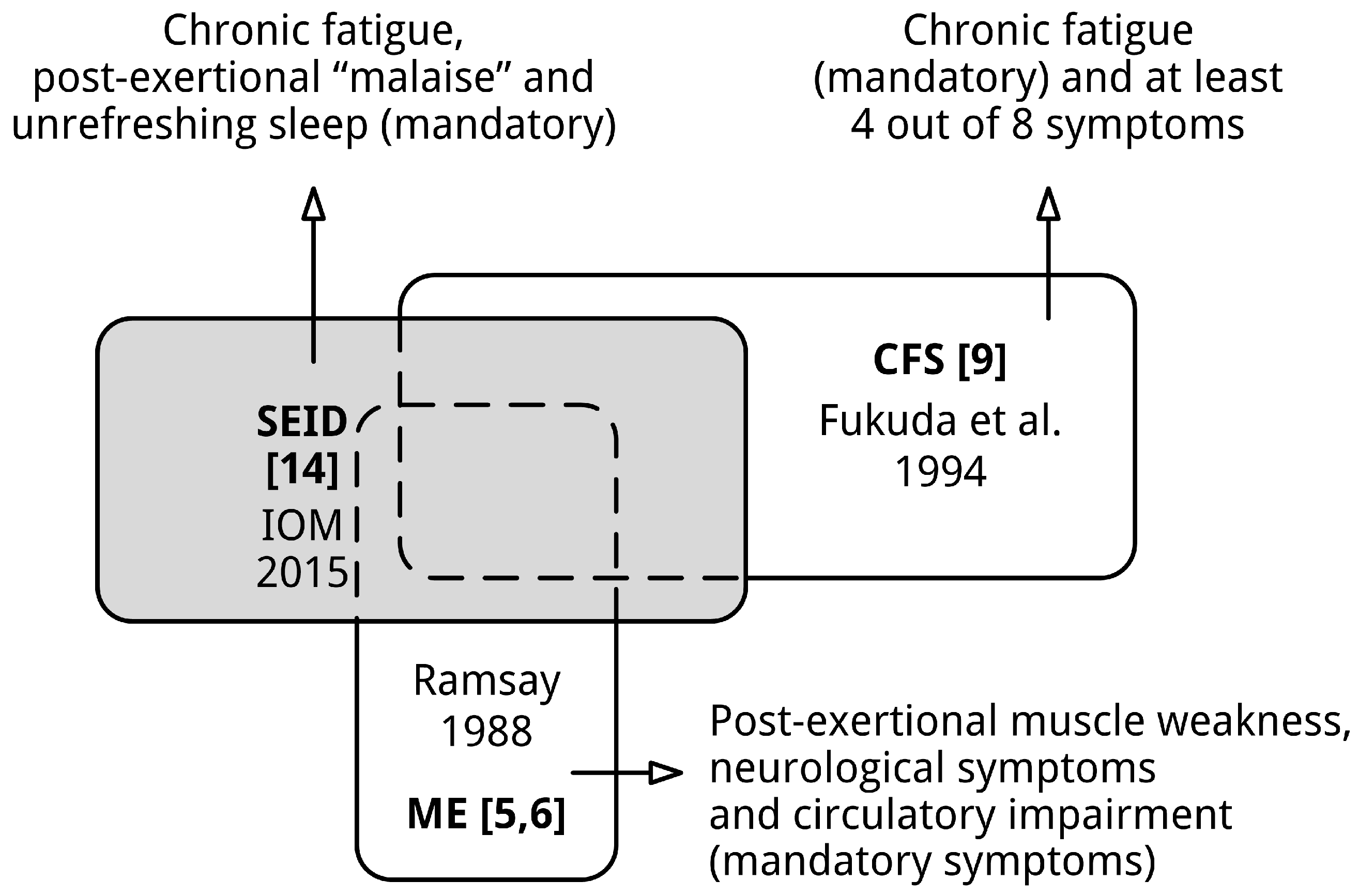
List 5. Proposed diagnostic criteria for SEID [14] (p. 6).
- a substantial reduction or impairment in the ability to engage in pre-illness levels of occupational, educational, social, or personal activities, that persists for more than 6 months and is accompanied by fatigue, which is often profound, is of new or definite onset (not lifelong), is not the result of ongoing excessive exertion, and is not substantially alleviated by rest;
- post-exertional malaise (*1); and
- unrefreshing sleep (*1)
- cognitive impairment (*1); or
- orthostatic intolerance
3.1. Neither ME nor CFS Is Covered by the Diagnostic Criteria of SEID

3.2. The Abstract and Ill-Defined Symptoms of SEID Cannot Be Assessed by Self-Report
3.3. The SEID Criteria Do Not Seem Reduce the Heterogeneity of the CFS Patient Population
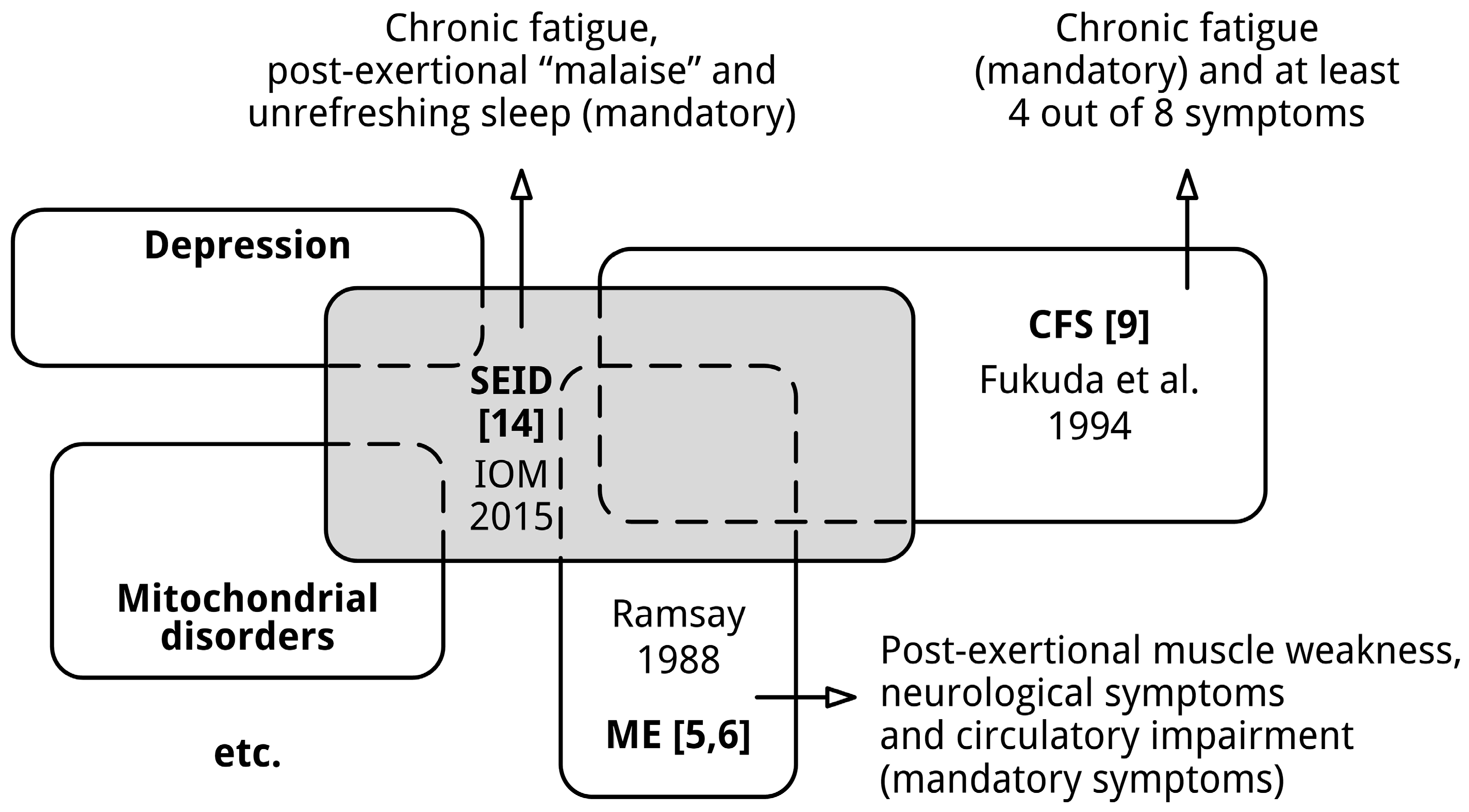
3.4. The Definition of SEID Includes People with Other Conditions

4. Proposal for a Methodological Solution for the Current “Diagnostic Impasse”
4.1. Make a Clear Distinction between Patients Meeting the Diagnosis of ME or CFS
4.2. Symptoms Should Be Assessed Objectively If Feasible, Not Only by Self-Report
4.3. Take into Account Confounding Factors
4.4. Use Pattern Recognition Methods to Develop Empiric Definitions for ME, CFS-1 etc.
4.5. Diagnostic Labels Should Preferably Reflect the Clinical Picture

5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gilliam, A.G. Epidemiological Study on an Epidemic, Diagnosed as Poliomyelitis, Occurring among the Personnel of Los Angeles County General Hospital during the Summer of 1934; Public Health Bulletin 240; United States Treasury Department Public Health Service: Washington, DC, USA, 1938; pp. 1–90. [Google Scholar]
- Acheson, E.D. The clinical syndrome variously called benign myalgic encephalomyelitis, Iceland disease and epidemic neuromyasthenia. Am. J. Med. 1959, 26, 569–595. [Google Scholar] [CrossRef]
- Parish, J.G. Early outbreaks of “epidemic neuromyasthenia”. Postgrad. Med. J. 1978, 54, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Acheson, E.D. A new clinical entity? Lancet 1956, 267, 789–790. [Google Scholar]
- Ramsay, A.M. Myalgic Encephalomyelitis and Postviral Fatigue States: The Saga of Royal Free Disease, 2nd ed.; Gower Publishing Corporation: London, UK, 1988. [Google Scholar]
- Ramsay, A.M. The clinical identity of the Myalgic Encephalomyelitis syndrome. ME Assoc. 1988. Available online: http://web.onetel.com/~kickback/THE%20CLINICAL%20IDENTITY%20OF%20ME.html (accessed on 3 February 2016).
- Dowsett, E.G. Myalgic encephalomyelitis, or what? Lancet 1988, 332, 101. [Google Scholar] [CrossRef]
- Holmes, G.P.; Kaplan, J.E.; Gantz, N.M.; Komaroff, A.L.; Schonberger, L.B.; Straus, S.E.; Jones, J.F.; Dubois, R.E.; Cunningham-Rundles, C.; Pahwa, S.; et al. Chronic fatigue syndrome: A working case definition. Ann. Intern. Med. 1988, 108, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.; Dobbins, J.G.; Komaroff, A.L. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.B.; William, A.H.; Strauss, A.C.; Unger, E.R.; Jason, L.; Marshall, G.D.J.; Dimitrakoff, J.D. Chronic fatigue syndrome: The current status and future potentials of emerging biomarkers. Fatigue 2014, 2, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.; Hickie, I.; Hadzi-Pavlovic, D.; Wakefield, D.; Parker, G.; Straus, S.E.; Dale, J.; McCluskey, D.; Hinds, G.; Brickman, A.; et al. What is chronic fatigue syndrome? Heterogeneity within an international multicentre study. Aust. N. Z. J. Psychiatry 2001, 35, 520–527. [Google Scholar] [CrossRef] [PubMed]
- May, M.; Emond, A.; Crawley, E. Phenotypes of chronic fatigue syndrome in children and young people. Arch. Dis. Child. 2010, 95, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N.M. The status of and future research into Myalgic Encephalomyelitis and chronic fatigue syndrome: The need of accurate diagnosis, objective assessment, and acknowledging biological and clinical subgroups. Front. Physiol. 2014, 5, 109. [Google Scholar] [CrossRef] [PubMed]
- IOM (Institute of Medicine). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Haney, E.; Smith, M.E.; McDonagh, M.; Pappas, M.; Daeges, M.; Wasson, N.; Nelson, H.D. Diagnostic methods for Myalgic Encephalomyelitis/chronic fatigue syndrome: A systematic review for a national institutes of health pathways to prevention workshop. Ann. Intern. Med. 2015, 162, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, R.; Guyatt, G.H.; Dellinger, P.; Schünemann, H.; Levy, M.M.; Kunz, R.; Norris, S.; Bion, J.; GRADE-Working-Group. Use of GRADE grid to reach decisions on clinical practice guidelines when consensus is elusive. BMJ 2008, 337, a744. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; Group, G.W. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–946. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Aggarwal, R.; Khanna, D. Methods of formal consensus in classification/diagnostic criteria and guideline development. Semin. Arthritis Rheum. 2011, 41, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Hamm, M.P.; Milne, A.; Vandermeer, B.; Santaguida, P.L.; Ansari, M.; Tsertsvadze, A.; Hempel, S.; Shekelle, P.; Dryden, D.M. Testing the risk of bias tool showed low reliability between individual reviewers and across consensus assessments of reviewer pairs. J. Clin. Epidemiol. 2013, 66, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Vernon, S.D.; Furst, J.D.; Simonis, V. Examining case definition criteria for chronic fatigue syndrome and myalgic encephalomyelitis. Fatigue 2014, 2, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Bou-Holaigah, I.; Rowe, P.C.; Kan, J.; Calkins, H. The relationship between neurally mediated hypotension and the chronic fatigue syndrome. JAMA 1995, 274, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.K.; Lewis, D.P.; Richardson, A.M.; Lidbury, B.A. Comorbidity of postural orthostatic tachycardia syndrome and chronic fatigue syndrome in an Australian cohort. J. Intern. Med. 2014, 275, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Lewis, I.; Pairman, J.; Spickett, G.; Newton, J.L. Clinical characteristics of a novel subgroup of chronic fatigue syndrome patients with postural orthostatic tachycardia syndrome. J. Intern. Med. 2013, 273, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Hoad, A.; Spickett, G.; Elliott, J.; Newton, J. Postural orthostatic tachycardia syndrome is an under-recognized condition in chronic fatigue syndrome. QJM 2008, 101, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Jessen, T.; Porter, N.; Boulton, A.; Gloria-Njoku, M.; Friedberg, F. Examining Types of Fatigue among Individuals with ME/CFS. Available online: http://dsq-sds.org/article/view/938/1113 (accessed on 3 February 2016).
- Elasy, T.A.; Gaddy, G. Measuring subjective outcomes: Rethinking reliability and validity. J. Gen. Intern. Med. 1998, 13, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, A.A.; Drinkard, B.M.; Diao, G.; Furst, G.; Dale, J.K.; Straus, S.E.; Gerber, L.H. Exploratory analysis of the relationships between aerobic capacity and self-reported fatigue in patients with rheumatoid arthritis, polymyositis, and chronic fatigue syndrome. PM R 2009, 1, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Wiborg, J.F.; Knoop, H.; Stulemeijer, M.; Prins, J.B.; Bleijenberg, G. How does cognitive behaviour therapy reduce fatigue in patients with chronic fatigue syndrome? The role of physical activity. Psychol. Med. 2010, 40, 1281–1287. [Google Scholar] [PubMed]
- Holgate, S.T.; Komaroff, A.L.; Mangan, D.; Wessely, S. Chronic fatigue syndrome: Understanding a complex illness. Nat. Rev. Neurosci. 2011, 12, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, M. Cognitive behavior therapy for chronic fatigue syndrome: efficacy and implications. Am. J. Med. 1998, 105, 104S–109S. [Google Scholar] [CrossRef]
- Vercoulen, J.H.; Swanink, C.M.; Galama, J.M.; Fennis, J.F.; Jongen, P.J.; Hommes, O.R.; van der Meer, J.W.; Bleijenberg, G. The persistence of fatigue in chronic fatigue syndrome and multiple sclerosis: Development of a model. J. Psychosom. Res. 1998, 45, 507–517. [Google Scholar] [CrossRef]
- Hooper, M. Myalgic encephalomyelitis: A review with emphasis on key findings in biomedical research. J. Clin. Pathol. 2007, 60, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N.M. The 4I hypothesis: A neuro-immunological explanation for characteristic symptoms of Myalgic Encephalomyelitis/chronic fatigue syndrome. Int. J. Neurol. Res. 2015, 1, 20–38. [Google Scholar] [CrossRef]
- Twisk, F.N.M. A definition of recovery in myalgic encephalomyelitis and chronic fatigue syndrome should be based upon objective measures. Qual. Life Res. 2014, 23, 2417–2418. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N.M. Accurate diagnosis of Myalgic Encephalomyelitis and chronic fatigue syndrome based upon objective test methods for characteristic symptoms. World J. Methodol. 2015, 5, 68–87. [Google Scholar] [PubMed]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Newton, J.L.; Strand, E.B.; Vernon, S.D. Chronic fatigue syndrome versus systemic exertion intolerance disease. Fatigue Biomed. Health Behav. 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N.M. A critical analysis of the proposal of the Institute of Medicine to replace myalgic encephalomyelitis and chronic fatigue syndrome by a new diagnostic entity called systemic exertion intolerance disease. Curr. Med. Res. Opin. 2015, 31, 1333–1347. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Sunnquist, M.; Kot, B.; Brown, A.; Reed, J. Unintended consequences of not specifying exclusionary illnesses with systemic exertion intolerance disease. Diagnostics 2015, 5, 272–286. [Google Scholar] [CrossRef]
- Maes, M.; Twisk, F.N.M. Chronic fatigue syndrome: Harvey and Wessely’s (bio)psychosocial model versus a bio(psychosocial) model based on inflammatory and oxidative and nitrosative stress pathways. BMC Med. 2010, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Faro, M.; Sàez-Francás, N.; Castro-Marrero, J.; Aliste, L.; Fernández-de-Sevilla, T.; Alegre, J. Gender differences in chronic fatigue syndrome. Reumatol Clin. 2015. [Google Scholar] [CrossRef]
- DeLuca, J.; Johnson, S.K.; Ellis, S.P.; Natelson, B.H. Sudden vs. gradual onset of chronic fatigue syndrome differentiates individuals on cognitive and psychiatric measures. J. Psychiatr. Res. 1997, 31, 83–90. [Google Scholar] [CrossRef]
- Hornig, M.; Montoya, J.G.; Klimas, N.G.; Levine, S.; Felsenstein, D.; Bateman, L.; Peterson, D.L.; Gottschalk, C.G.; Schultz, A.F.; Che, X.; et al. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. Sci. Adv. 2015, 1, e1400121. [Google Scholar] [CrossRef] [PubMed]
- Natelson, B.H.; Weaver, S.A.; Tseng, C.L.; Ottenweller, J.E. Spinal fluid abnormalities in patients with chronic fatigue syndrome. Clin. Diagn. Lab. Immunol. 2005, 12, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R.; Petty, R.; Burke, B.; Gough, J.; Fear, D.; Sinclair, L.I.; Mattey, D.L.; Richards, S.C.; Montgomery, J.; Baldwin, D.A.; et al. Gene expression subtypes in patients with chronic fatigue syndrome/myalgic encephalomyelitis. J. Infect. Dis. 2008, 197, 1171–1184. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R.; Burke, B.; Petty, R.; Gough, J.; Fear, D.; Mattey, D.L.; Axford, J.S.; Dalgleish, A.G.; Nutt, D.J. Seven genomic subtypes of chronic fatigue syndrome/myalgic encephalomyelitis: A detailed analysis of gene networks and clinical phenotypes. J. Clin. Pathol. 2008, 61, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, J.W.M.; Lloyd, A.R. A controversial consensus—Comment on article by Broderick et al. J. Intern. Med. 2012, 271, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van de Sande, M.I.; de Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Nakatomi, Y.; Mizuno, K.; Ishii, A.; Wada, Y.; Tanaka, M.; Tazawa, S.; Onoe, K.; Fukuda, S.; Kawabe, J.; Takahashi, K.; et al. Neuroinflammation in patients with chronic fatigue syndrome/Myalgic Encephalomyelitis: An 11C-(R)-PK11195 PET study. J. Nucl. Med. 2014, 55, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Hornig, M.; Gottschalk, G.; Peterson, D.L.; Knox, K.K.; Schultz, A.F.; Eddy, M.L.; Che, X.; Lipkin, W.I. Cytokine network analysis of cerebrospinal fluid in myalgic encephalomyelitis/chronic fatigue syndrome. Mol. Psychiatry 2015. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Diseases, 8th Revision ed.; (ICD-8); Code 323; WHO: Geneva, Switzerland, 1967; p. 158. [Google Scholar]
- Green, C.R.; Cowan, P.; Elk, R.; O’Neil, K.M.; Rasmussen, A.L. National Institutes of Health pathways to prevention workshop: Advancing the research on Myalgic Encephalomyelitis/chronic fatigue syndrome. Ann. Intern. Med. 2015, 162, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L. Myalgic Encephalomyelitis/chronic fatigue syndrome: A real illness. Ann. Intern. Med. 2015, 162, 871–872. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Twisk, F.N.M. Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward. Diagnostics 2016, 6, 10. https://doi.org/10.3390/diagnostics6010010
Twisk FNM. Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward. Diagnostics. 2016; 6(1):10. https://doi.org/10.3390/diagnostics6010010
Chicago/Turabian StyleTwisk, Frank N.M. 2016. "Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward" Diagnostics 6, no. 1: 10. https://doi.org/10.3390/diagnostics6010010
APA StyleTwisk, F. N. M. (2016). Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward. Diagnostics, 6(1), 10. https://doi.org/10.3390/diagnostics6010010