Long Term Survival in Patients Suffering from Glio-blastoma Multiforme: A Single-Center Observational Cohort Study

 ,
,  ,
, 
Abstract
:1. Introduction
1.1. Background and Rationale
1.2. Purpose of the Present Investigation
2. Patients and Methods
2.1. Participants and Eligibility
- Patients were included in the study if their pre- and post-operative MR imaging was either performed at our institution or available on the picture archiving and communication system (PACS) for review.
- Patients were included if, in the postoperative period, they could undergo a standard Stupp protocol starting from the 30th–35th day after surgery as follows: Radiotherapy (60 Gy delivered in 30 fractions of 2 Gy/day, 5 days a week for 6 weeks) and concomitant oral chemotherapy with temozolomide (75 mg/m2 of body surface 7 days a week, from first to last day of radiotherapy, no more than 49 days). After a break of 20–25 days, about 12 cycles of Temozolomide (200 mg/m2 for 5 days every 28 days) were administered [9].
- Patients were included if they received standard conformational planning with a linear accelerator (LINAC), no stereotactic radiosurgical treatment was performed.
- Once the progression of the disease was noticed, the patient and the relevant imaging were referred again to our attention, to evaluate the feasibility of a second surgery or to address the patient to a second line of adjuvant treatment.
- The estimated target of the surgical procedure was the total or subtotal resection of the lesions: no biopsies were included.
- All the patients included in the study were newly diagnosed GBM at their first surgery; operating on recurrences makes a complete difference.
- Incomplete or wrong data on clinical, radiological and surgical records and/or lost to follow-up.
- Patients classified as LTS: experiencing an OS of at least 24 months or longer.
- Patients classified as short term survivors (STS): experiencing an OS of less than 24 months.
- The white matter appeared free of disease in any aspect of the surgical cavity.
- Despite a directly visualized or navigation proven remnant, neuromonitoring or intraoperative neuropsychological testing outlined a risk for postoperative motor morbidity.
3. Data Sources and Quantitative Variables
- A standard early (maximum 24 h after surgery) postoperative volumetric brain MRI.
- At approximately one month from surgery (25–35 days) a volumetric brain MRI scan was repeated for a first-step follow-up control and to provide information for the radiation treatment planning.
- After the end of irradiation, a volumetric brain MRI scan was performed every three months.
3.1. Statistical Methods
3.2. Potential Source of Bias and Study Size
4. Results
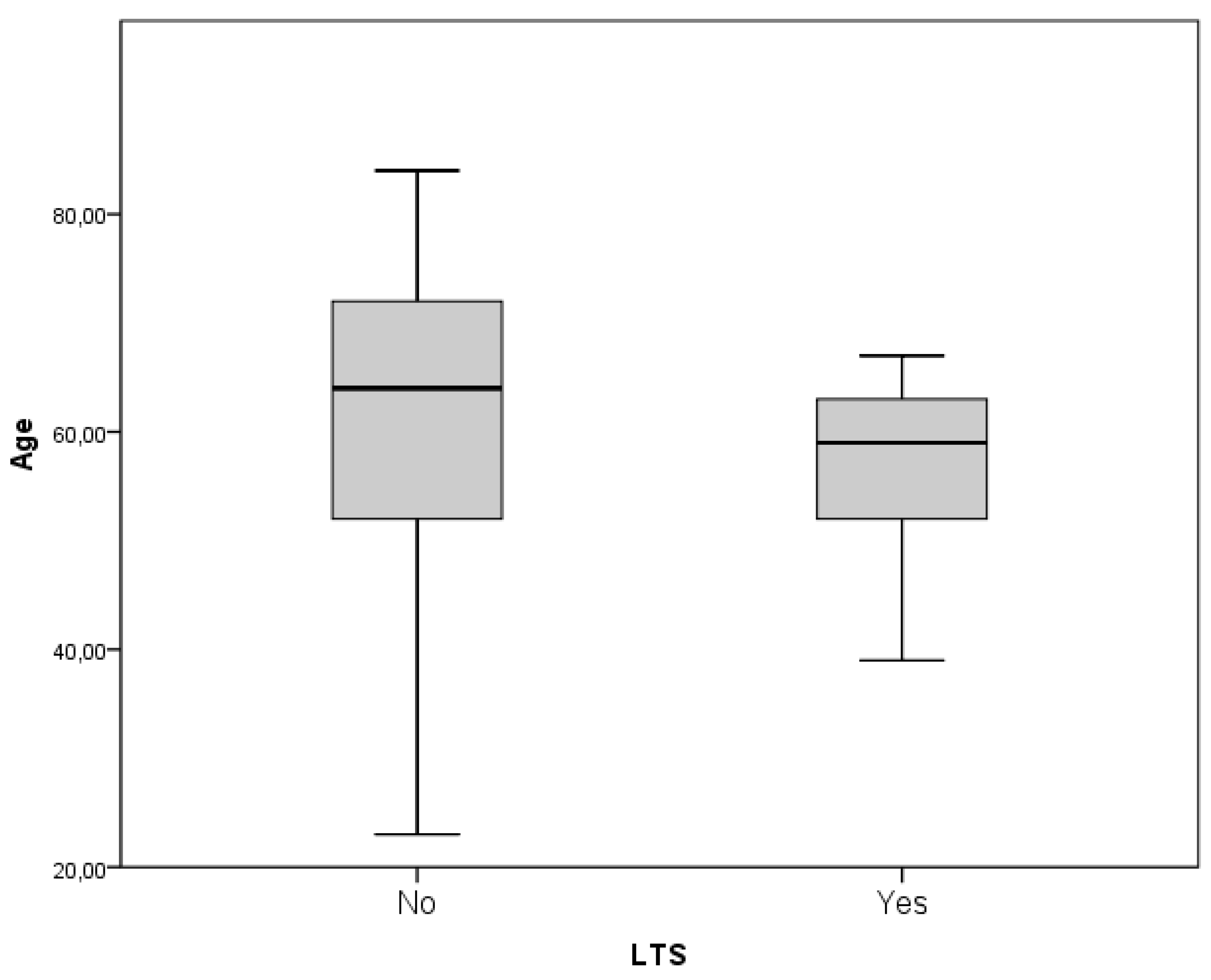
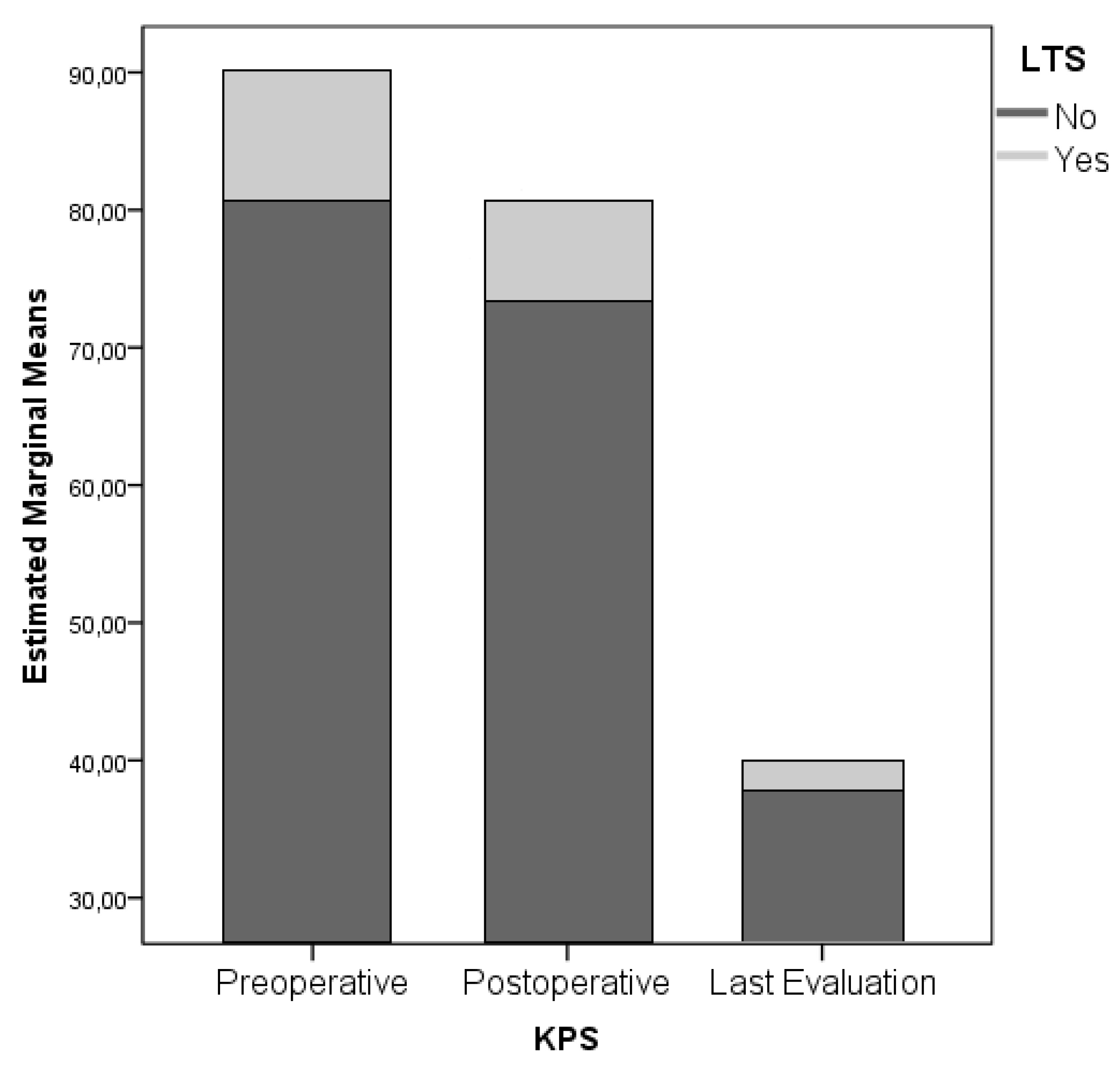
4.1. Patient-Related Factors
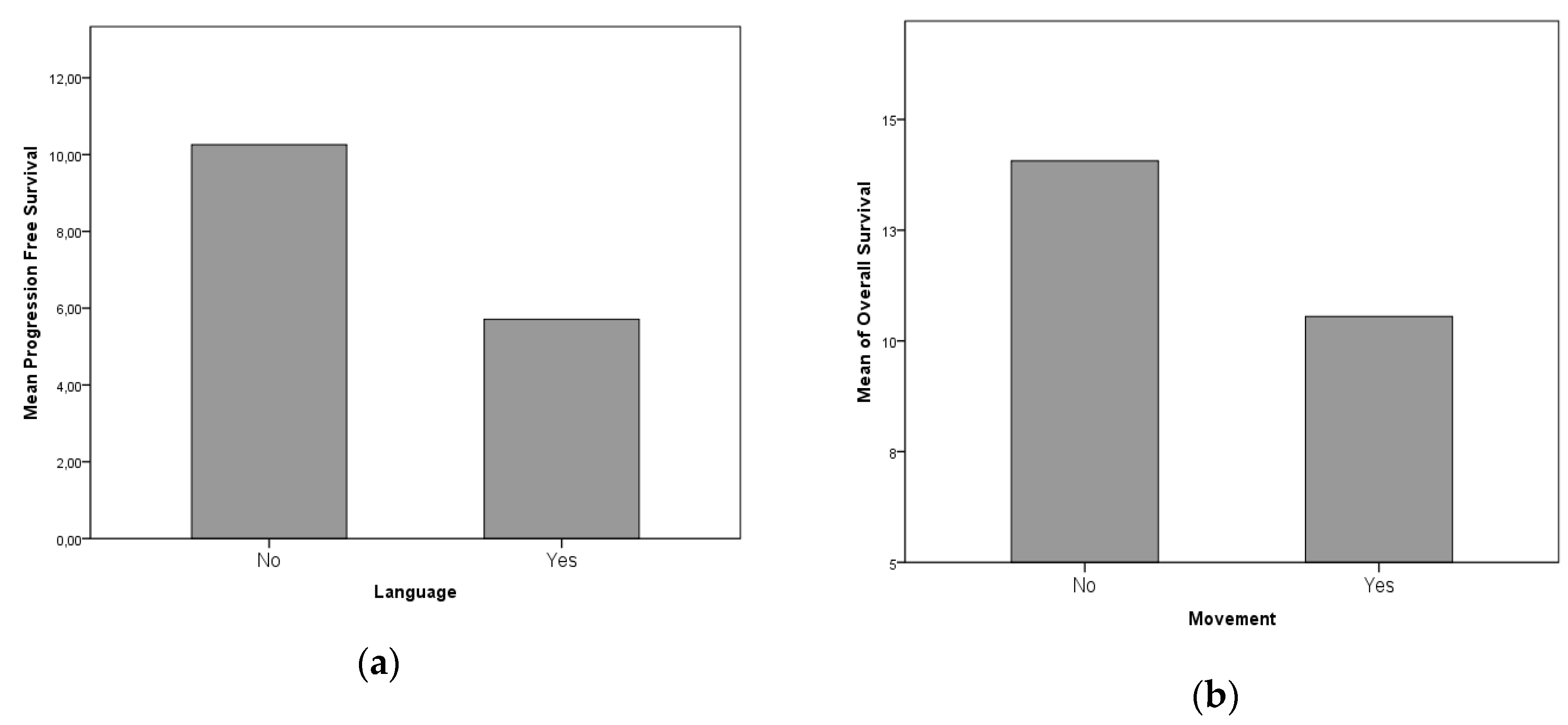
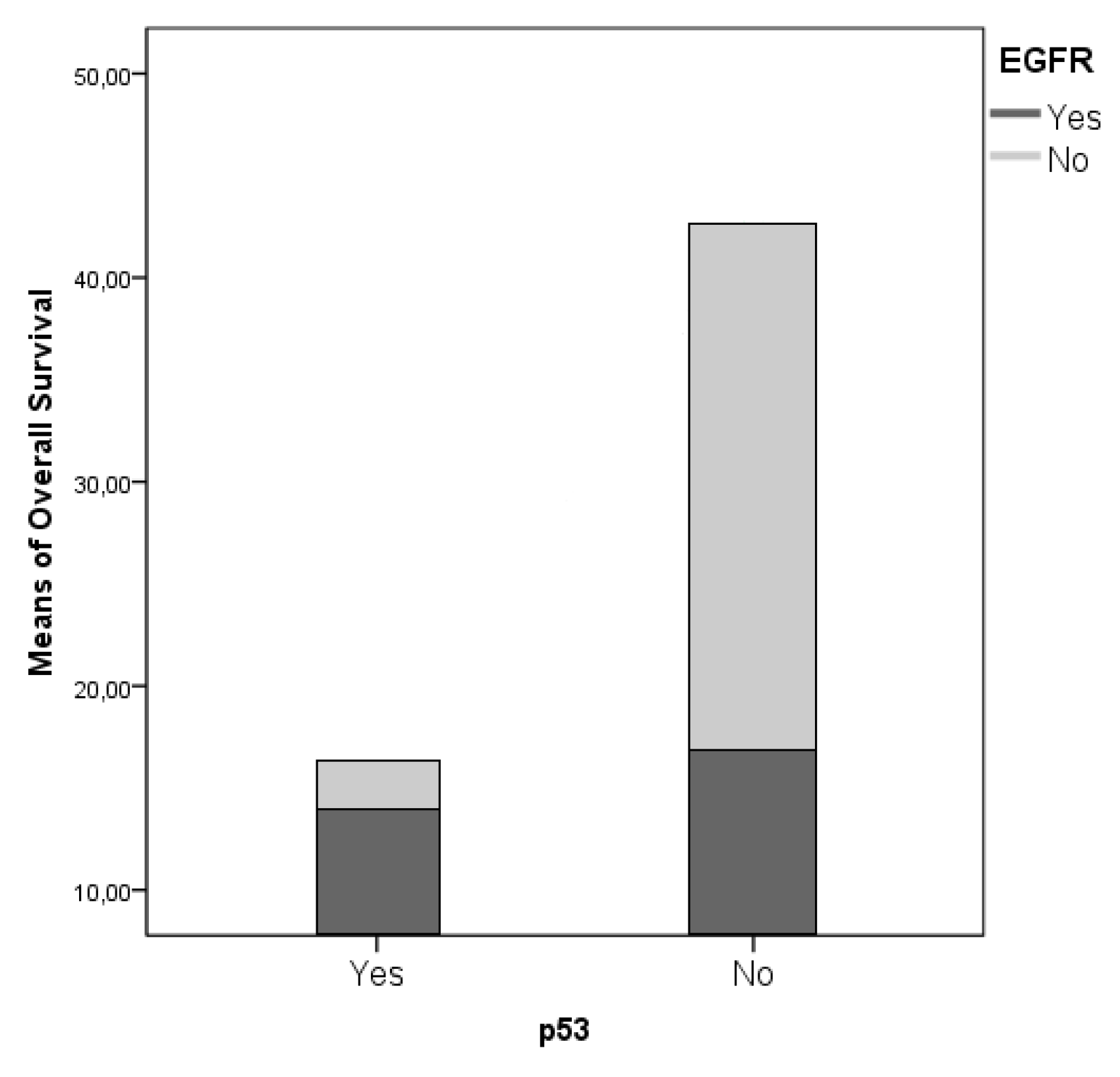
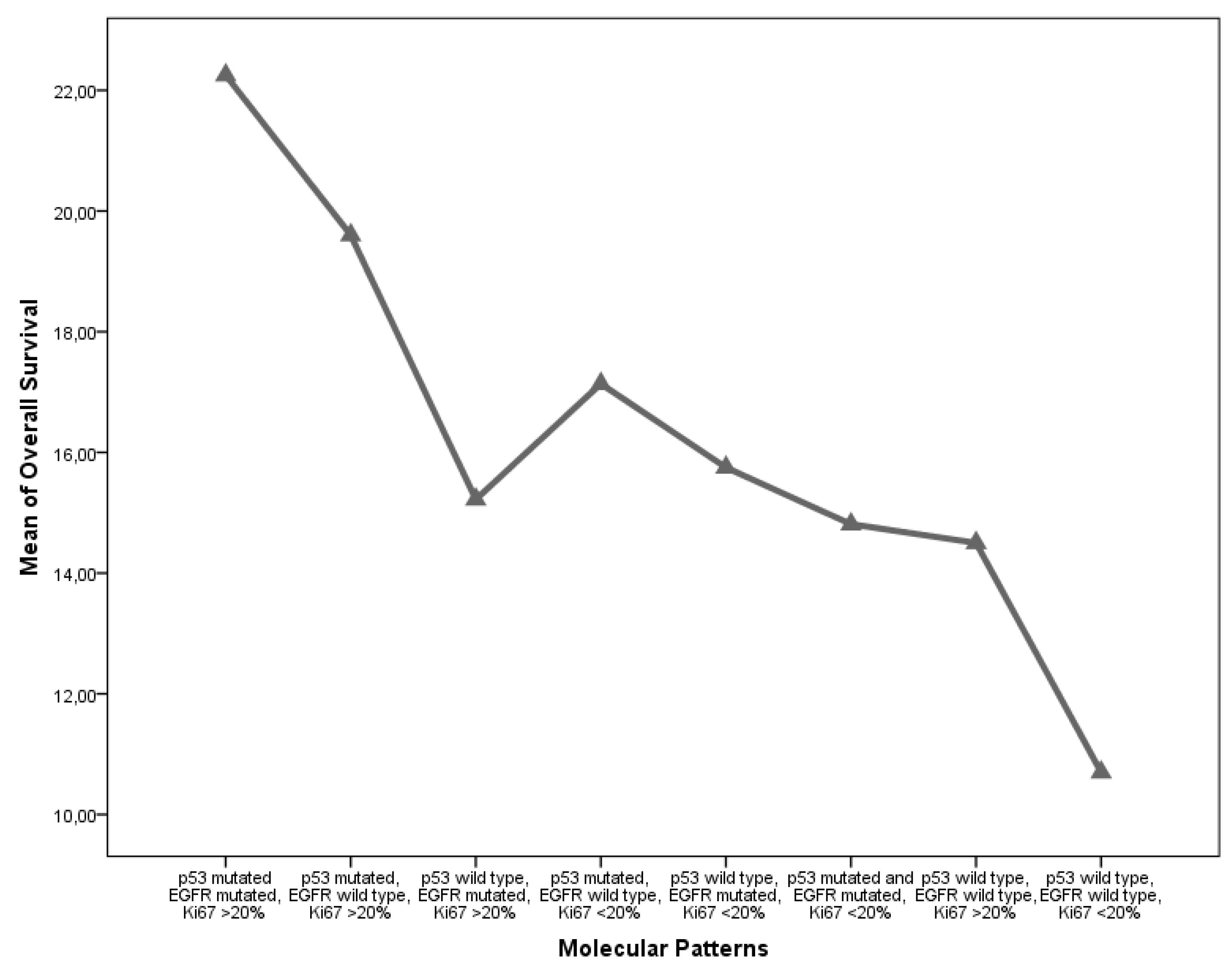
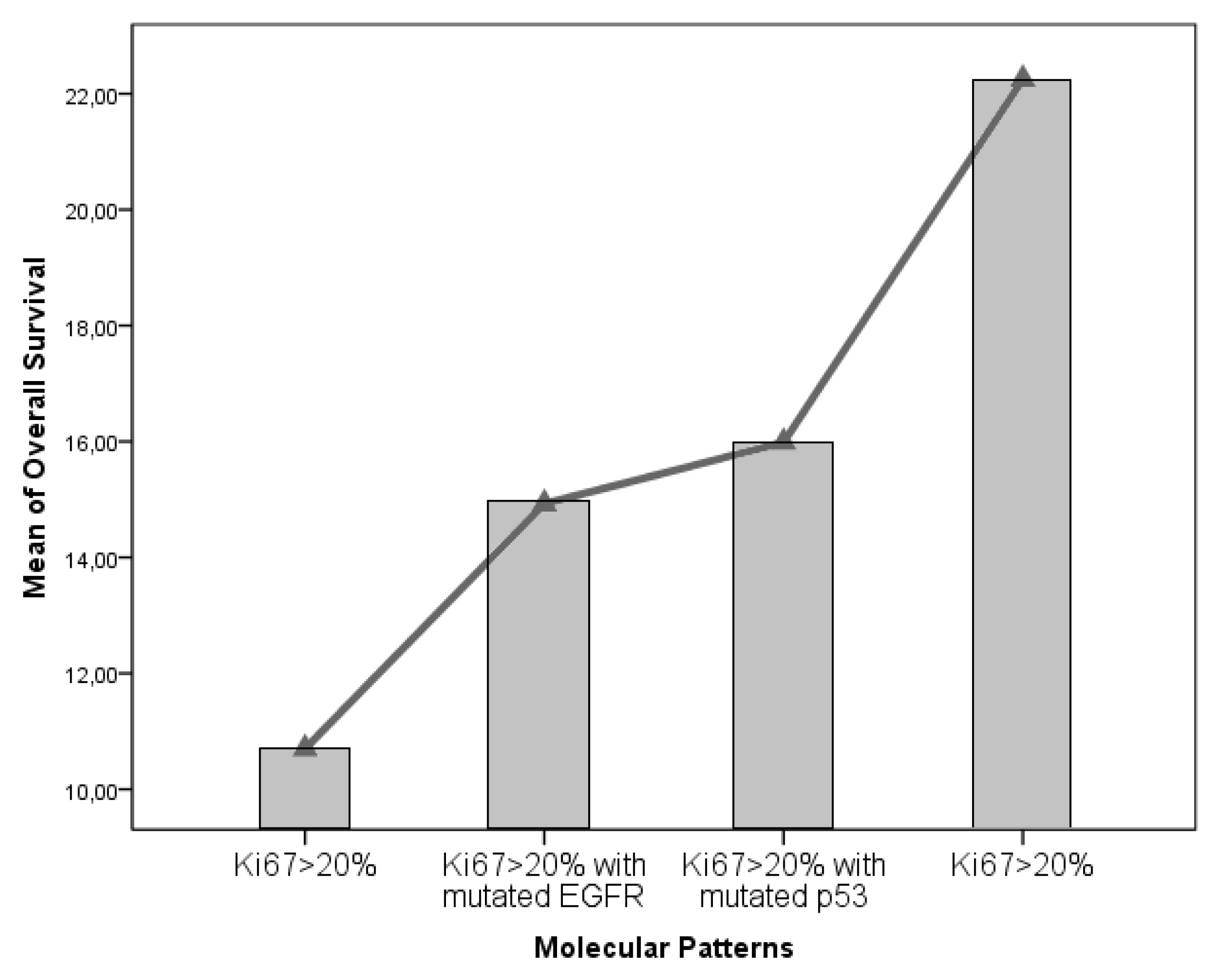
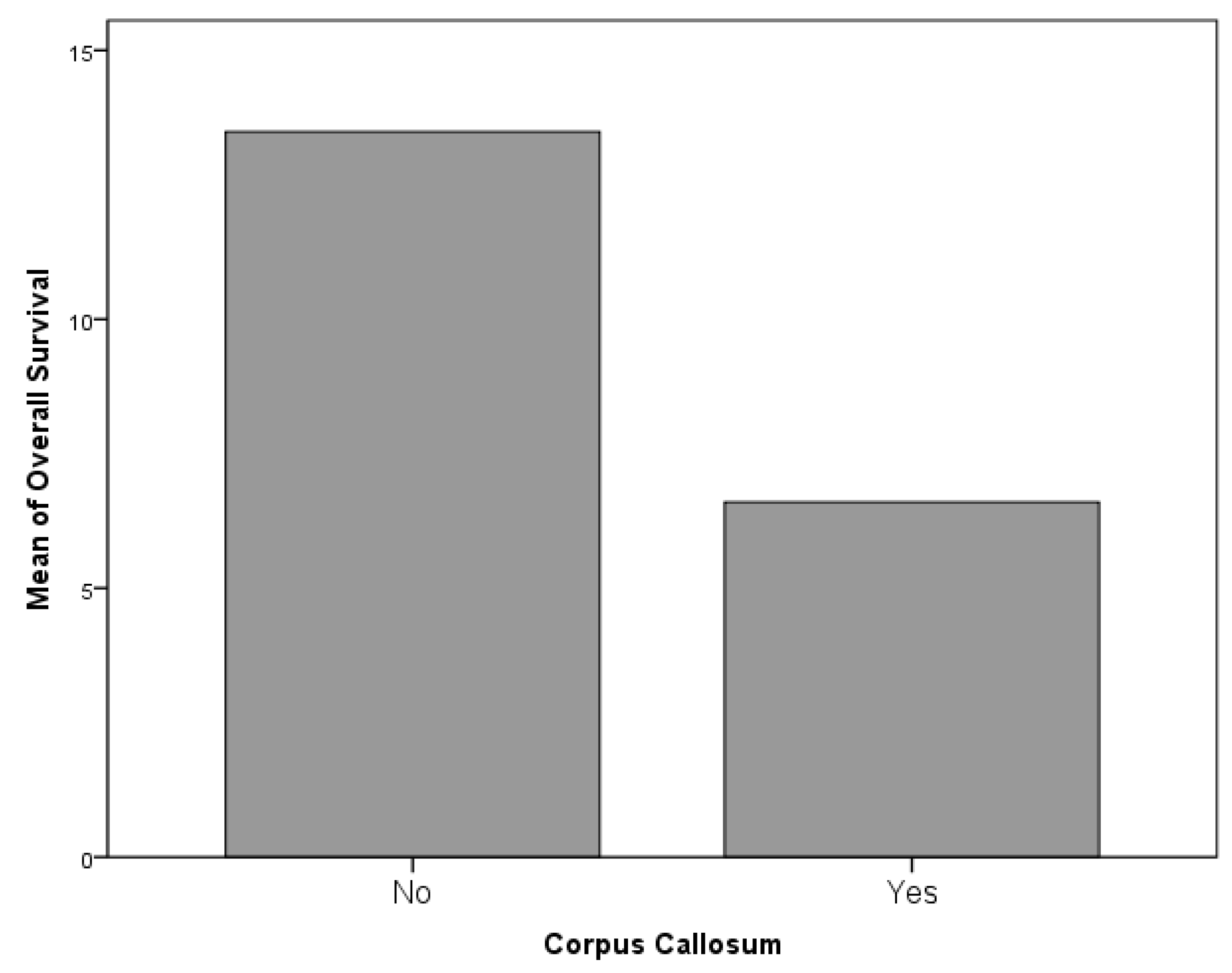
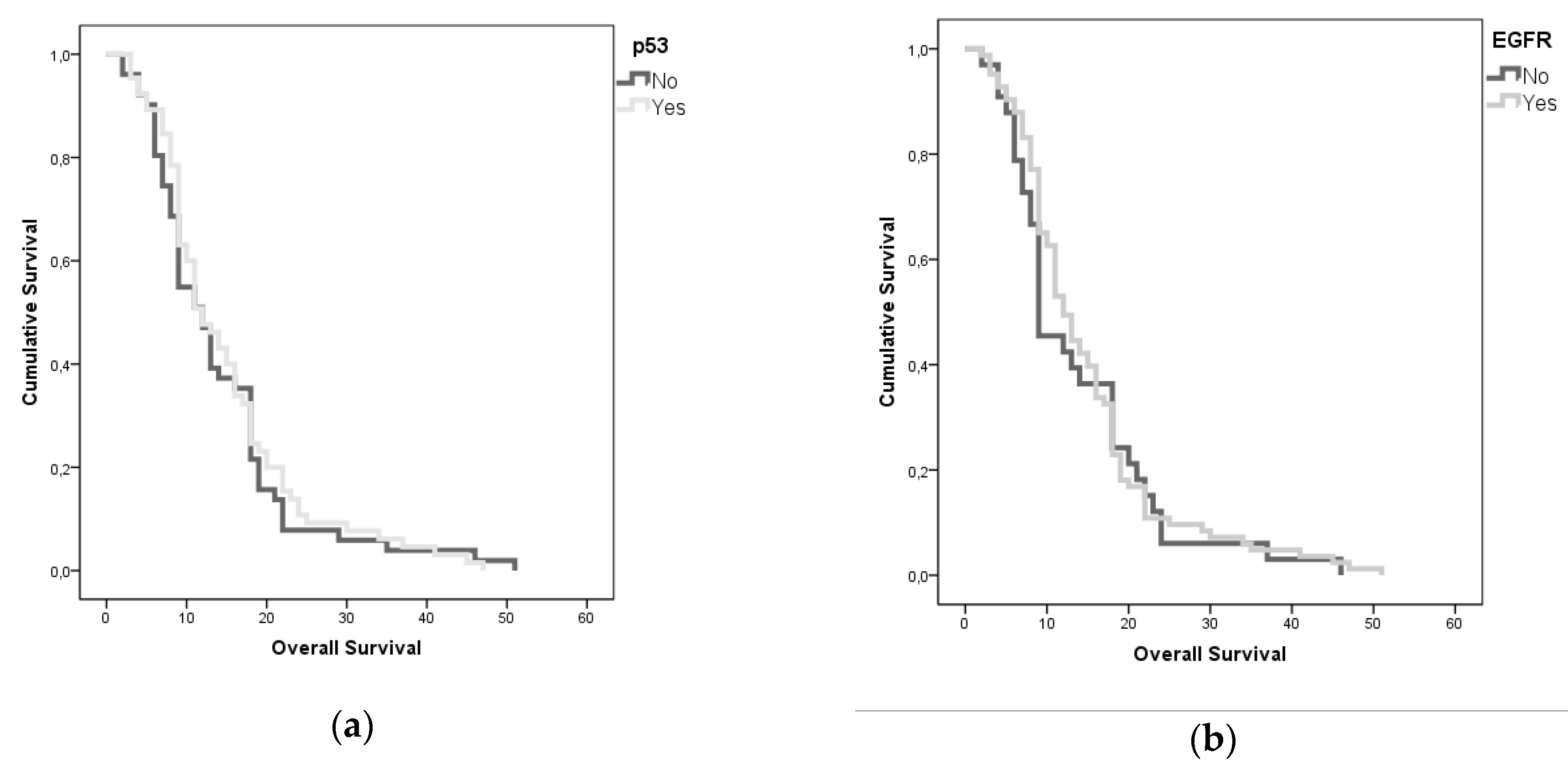
4.2. Tumor-Related Factors
- p53 mutated EGFR mutated, Ki67 >20%.
- p53 mutated and EGFR mutated, Ki67 <20%.
- p53 mutated, EGFR wild-type, Ki67 <20%.
- p53 wild-type, EGFR mutated, Ki67 <20%.
- p53 wild-type, EGFR mutated, Ki67 >20%.
- p53 mutated, EGFR wild-type, Ki67 >20%.
- p53 wild-type, EGFR wild-type, Ki67 >20%.
- p53 wild-type, EGFR wild-type, Ki67 <20%.
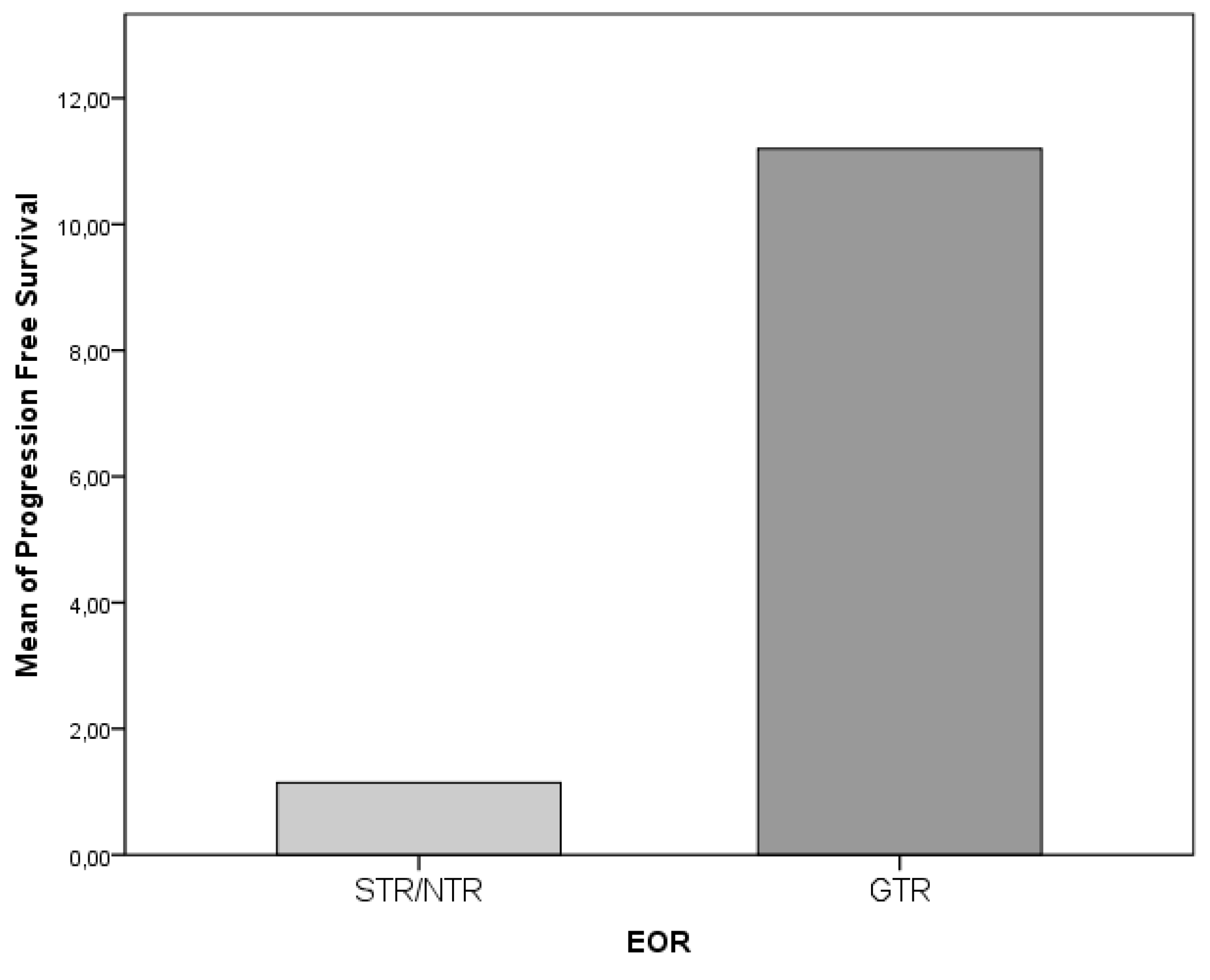
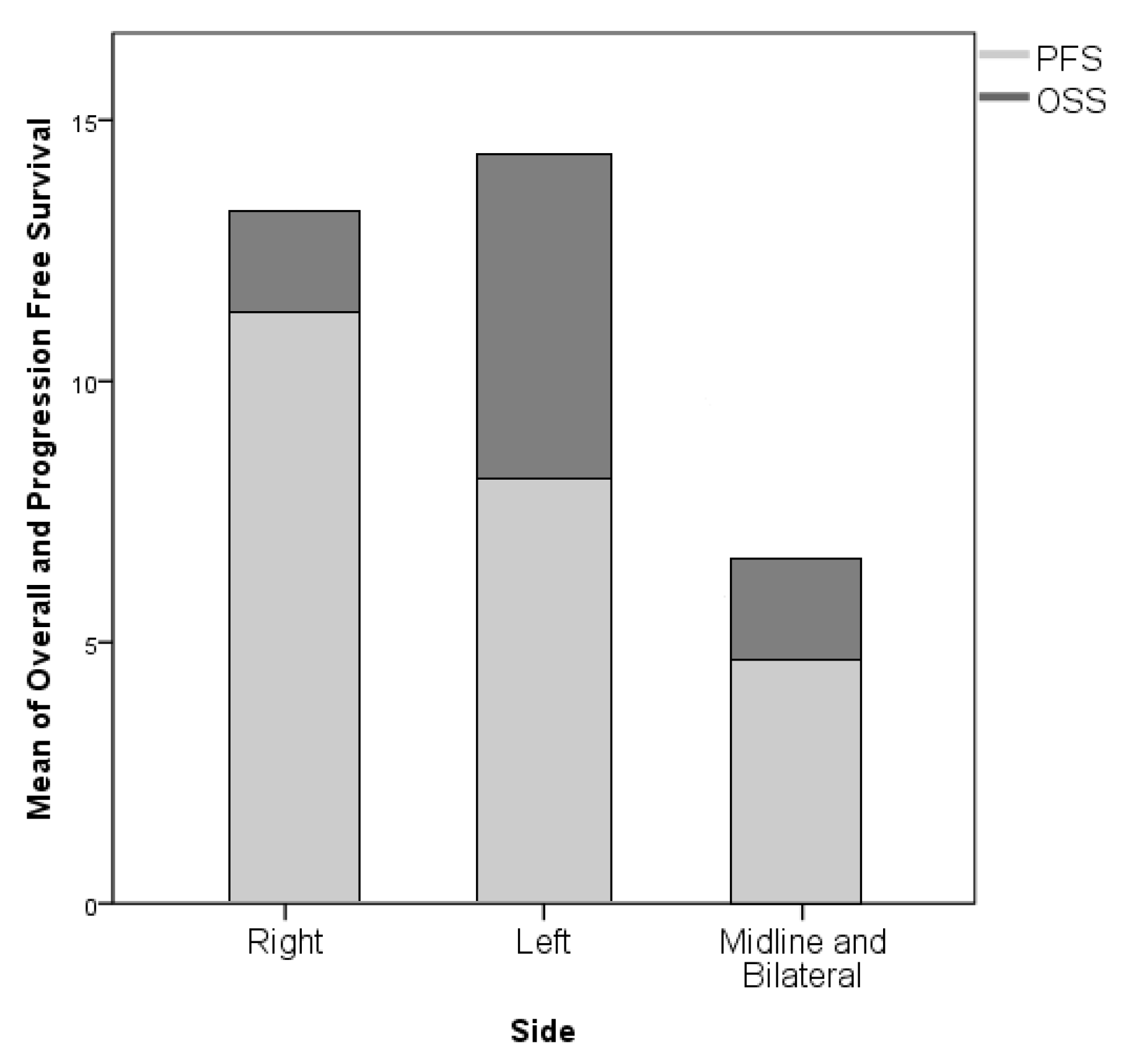
4.3. Surgery-Related Factors
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| LTS | Long Term Survivors |
| STS | Short Term Survivors |
| DTI | Diffusion Tensor Imaging |
| DWI: | Diffusion-Weighted Imaging |
| EGFR | Epidermal Growth Factor Receptor |
| EOR | Extent of Resection |
| FLAIR | Fluid Attenuated Inversion recovery |
| fMRI | Functional Magnetic Resonance Imaging |
| GBM | Glioblastoma |
| GTR | Gross Total Resection |
| HGG | High-Grade Gliomas |
| IDH | Isocitrate Dehydrogenase |
| IoN | Intraoperative Neurophysiological monitoring |
| IoNT | Intraoperative Neuropsychological testing |
| LGG | Low-Grade Gliomas |
| KPS | Karnofsky Performance Status |
| MPRAGE | Magnetization-Prepared Rapid Gradient-Echo |
| MRI | Magnetic Resonance Imaging |
| NTR | Near-Total Resection |
| STR | Subtotal Resection |
| OS | Overall Survival |
| PFS | Progression-Free Survival |
References
- Perry, A.; Louis, D.N.; Scheithauer, B.W.; Budka, H.; von Deimling, A.; Ohgaki, H.; Cavenee, W.K. World Health Organization Classification of Tumours of the Central Nervous System; IARC Press: Lyon, France, 2007. [Google Scholar]
- Sonoda, Y.; Kumabe, T.; Watanabe, M.; Nakazato, Y.; Inoue, T.; Kanamori, M.; Tominaga, T. Long-term survivors of glioblastoma: Clinical features and molecular analysis. Acta Neurochir. 2009, 151, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Cervoni, L.; Artico, M.; Caruso, R.; Gagliardi, F.M. Long-term survival in patients with supratentorial glioblastoma. J. Neuro. Oncol. 1998, 36, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Krex, D.; Klink, B.; Hartmann, C.; von Deimling, A.; Pietsch, T.; Simon, M.; Sabel, M.; Steinbach, J.P.; Heese, O.; Reifenberger, G.; et al. German glioma network Long-Term survival with glioblastoma multiforme. Brain 2007, 130, 2596–2606. [Google Scholar] [CrossRef]
- Deb, P.; Sharma, M.C.; Mahapatra, A.K.; Agarwal, D.; Sarkar, C. Glioblastoma multiforme with long term survival. Neurol. India 2005, 53, 329–332. [Google Scholar]
- McLendon, R.E.; Halperin, E.C. Is the long-term survival of patients with intracranial glioblastoma multiforme overstated? Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 98, 1745–1748. [Google Scholar] [CrossRef]
- Bähr, O.; Herrlinger, U.; Weller, M.; Steinbach, J.P. Very late relapses in glioblastoma long-term survivors. J. Neurol. 2009, 256, 1756–1758. [Google Scholar] [CrossRef]
- Steinbach, J.P.; Blaicher, H.P.; Herrlinger, U.; Wick, W.; Nägele, T.; Meyermann, R.; Tatagiba, M.; Bamberg, M.; Dichgans, J.; Karnath, H.O.; et al. Surviving glioblastoma for more than 5 years: The patient’s perspective. Neurology 2006, 66, 239–242. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. European organisation for research and treatment of cancer brain tumor and radiotherapy groups; national cancer institute of canada clinical trials group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Mellinghoff, I.K.; Wang, M.Y.; Vivanco, I.; Haas-Kogan, D.A.; Zhu, S.; Dia, E.Q.; Riggs, B.L. Molecular determinants of the response of glioblastoma to EGFR kinase inhibitors. N. Engl. J. Med. 2005, 353, 2012–2042. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Formichella, A.I.; D’Elia, A.; Brogna, C.; Frati, A.; Giangaspero, F.; Delfini, R.; Santoro, A. Cerebral Glioblastomas with oligodendroglial component: Analysis of 36 cases. J. Neurooncol. 2009, 94, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the central Nervous System: A summary. Acta Neurpathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Ohgaki, H.; Kleihues, P. The definition of primary and secondary glioblastoma. Clin. Cancer Res. 2013, 19, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Caruso, R.; Pesce, A.; Wierzbicki, V. A very rare case report of long-term survival: A patient operated on in 1994 of glioblastoma multiforme and currently in perfect health. Int. J. Surg. Case Rep. 2017, 33, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Bloch, O.; Han, S.J.; Cha, S.; Sun, M.Z.; Aghi, M.K.; McDermott, M.W.; Berger, M.S.; Parsa, A.T. Impact of extent of resection for recurrent glioblastoma on overall survival: Clinical article. J. Neurosurg. 2012, 117, 1032–1038. [Google Scholar] [CrossRef]
- Malakhov, N.; Lee, A.; Garay, E.; Becker, D.J.; Schreiber, D. Patterns of care and outcomes for glioblastoma in patients with poor performance status. J. Clin. Neurosci. 2018, 52, 66–70. [Google Scholar] [CrossRef]
- Yao, F.; Wang, J.; Yao, J.; Hang, F.; Lei, X.; Cao, Y. Three-dimensional image reconstruction with free open-source OsiriX software in video-assisted thoracoscopic lobectomy and segmentectomy. Int. J. Surg. 2017, 39, 16–22. [Google Scholar] [CrossRef]
- Scott, J.N.; Rewcastle, N.B.; Brasher, P.M.; Fulton, D.; MacKinnon, J.A.; Hamilton, M.; Cairncross, J.G.; Forsyth, P. Which glioblastoma multiforme patient will become a long-term survivor? A population-based study. Ann. Neurol. 1999, 46, 183–188. [Google Scholar] [CrossRef]
- D’Andrea, G.; Palombi, L.; Minniti, G.; Pesce, A.; Marchetti, P. Brain metastases: Surgical treatment and overall survival. World Neurosurg. 2017, 97, 169–177. [Google Scholar] [CrossRef]
- Frati, A.; Pesce, A.; Palmieri, M.; Celniku, M.; Raco, A.; Salvati, M. Surgical treatment of the septuagenarian patients suffering from brain metastases: A large retrospective observational analytic cohort-comparison study. World Neurosurg. 2018, 114, e565–e572. [Google Scholar] [CrossRef]
- Frati, A.; Pesce, A.; Palmieri, M.; Iasanzaniro, M.; Familiari, P.; Angelini, A.; Raco, A. Hypnosis-aided awake surgery for the management of intrinsic brain tumors versus standard awake-asleep-awake protocol: A preliminary, promising experience. World Neurosurg. 2019, 121, e882–e891. [Google Scholar] [CrossRef]
- Shinojima, N.; Kochi, M.; Hamada, J.; Nakamura, H.; Yano, S.; Makino, K.; Tsuiki, H.; Tada, K.; Kuratsu, J.; Ishimaru, Y.; et al. The influence of sex and the presence of giant cells on postoperative long-term survival in adult patients with supratentorial glioblastoma multiforme. J. Neurosurg. 2004, 101, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Plunkett, R.J.; Lis, A.; Barone, T.A.; Fronckowiak, M.D.; Greenberg, S.J. Hormonal effects on glioblastoma multiforme in the nude rat model. J. Neurosurg. 1999, 90, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Seki, Y.; Suico, M.A.; Uto, A.; Hisatsune, A.; Shuto, T.; Isohama, Y.; Kai, H. The ETS transcription factor MEF is a candidate tumor suppressor gene on the X chromosome. Cancer Res. 2002, 62, 6579–6586. [Google Scholar] [PubMed]
- Stummer, W.; Reulen, H.J.; Meinel, T.; Pichlmeier, U.; Schumacher, W.; Tonn, J.C.; Rohde, V.; Oppel, F.; Turowski, B.; Woiciechowsky, C.; et al. ALA-Glioma Study Group. Extent of resection and survival in glioblastoma multiforme: Identification of and adjustment for bias. Neurosurgery 2008, 62, 564–576. [Google Scholar]
- Hottinger, A.F.; Yoon, H.; Deangelis, L.M.; Abrey, L.E. Neurological outcome of long-term glioblastoma survivors. J. Neurooncol. 2009, 95, 301–305. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. European organisation for research and treatment of cancer brain tumour and radiation oncology groups; national cancer institute of canada clinical trials group. effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-years analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar]
- Li, H.F.; Kim, J.S.; Waldman, T. Radiation-induced akt activation modulates radioresistance in human glioblastoma cells. Radiat. Oncol. 2009, 4, 43. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Gilbert, M.R.; Chakravarti, A. Chemoradiotherapy in malignant glioma: Standard of care and future directions. J. Clin. Oncol. 2007, 25, 4127–4136. [Google Scholar] [CrossRef]
- Glas, M.; Happold, C.; Rieger, J.; Wiewrodt, D.; Bähr, O.; Steinbach, J.P.; Wick, W.; Kortmann, R.D.; Reifenberger, G.; Weller, M.; et al. Long-term survival of patients with glioblastoma treated with radiotherapy and lomustine plus temozolomide. J. Clin. Oncol. 2009, 27, 1257–1261. [Google Scholar] [CrossRef]
- Liu, Q.; Nguyen, D.H.; Dong, Q.; Shitaku, P.; Chung, K.; Liu, O.Y.; Tso, J.L.; Liu, J.Y.; Konkankit, V.; Cloughesy, T.F.; et al. Molecular properties of CD133+ glioblastoma stem cells derived from treatment-refractory recurrent brain tumors. J. Neurooncol. 2009, 94, 1–19. [Google Scholar] [CrossRef]
- Nishide, K.; Nakatani, Y.; Kiyonari, H.; Kondo, T. Glioblastoma formation from cell population depleted of Prominin1-expressing cells. PLoS ONE 2009, 4, e6869. [Google Scholar] [CrossRef]
- Beier, D.; Hau, P.; Proescholdt, M.; Lohmeier, A.; Wischhusen, J.; Oefner, P.J.; Aigner, L.; Brawanski, A.; Bogdahn, U.; Beier, C.P. CD133(+) and CD133(-) glioblastoma-derived cancer stem cells show differential growth characteristics and molecular profiles. Cancer Res. 2007, 67, 4010–4015. [Google Scholar] [CrossRef] [PubMed]
- Kanu, O.O.; Hughes, B.; Di, C.; Lin, N.; Fu, J.; Bigner, D.D.; Yan, H.; Adamson, C. Glioblastoma Multiforme Oncogenomics and Signaling Pathways. Clin. Med. Oncol. 2009, 3, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Watanabe, T.; Yonekawa, Y.; Kleihues, P.; Ohgaki, H. Promoter methylation of the DNA repair gene MGMT in astrocytomas is frequently associated with G:C→A:T mutations of the TP53 tumor suppressor gene. Carcinogenesis 2001, 22, 1715–1719. [Google Scholar] [CrossRef] [Green Version]
- Pelloski, C.E.; Mahajan, A.; Maor, M.; Chang, E.L.; Woo, S.; Gilbert, M.; Colman, H.; Yang, H.; Ledoux, A.; Blair, H.; et al. YKL-40 expression is associated with poorer response to radiation and shorter overall survival in glioblastoma. Clin. Cancer Res. 2005, 11, 3326–3334. [Google Scholar] [CrossRef] [Green Version]
- Sperduto, C.M.; Chakravarti, A.; Aldape, K.; Burger, P.; Papermaster, G.B.; Sperduto, P. Twenty-Year survival in glioblastoma: A case report and molecular profile. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1162–1165. [Google Scholar] [CrossRef]
- Tanwar, M.K.; Gilbert, M.R.; Holland, E.C. Gene expression microarray analysis reveals YKL-40 to be a potential serum marker for malignant character in human glioma. Cancer Res. 2002, 62, 4364–4368. [Google Scholar]
- Adeberg, S.; Bostel, T.; König, L.; Welzel, T.; Debus, J.; Combs, S.E. A comparison of long-term survivors and short-term survivors with glioblastoma, subventricular zone involvement: A predictive factor for survival? Radiat. Oncol. 2014, 9, 95. [Google Scholar] [CrossRef] [Green Version]
- Nafe, R.; Franz, K.; Schlote, W.; Schneider, B. The morphology of perinecrotic tumor cell nuclei in glioblastomas shows a significant relationship with survival time. Oncol. Rep. 2006, 16, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Martinez, R.; Schackert, G.; Yaya-Tur, R.; Rojas-Marcos, I.; Herman, J.G.; Esteller, M. Frequent hypermethylation of the DNA repair gene MGMT in long-term survivors of glioblastoma multiforme. J. Neurooncol. 2007, 83, 91–93. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contents | n = 177 Patients | Patients Collected between 2014–2016 | p Value |
|---|---|---|---|
| Subgroup | LTS = 30 | STS = 147 | |
| Sex | Male n = 20–66.7% Female n = 10–33.3% | Male n = 78, 53.06% Female n = 69, 46.93% | 0.128 |
| Age | 59.4 ± 7.69 | 61.16 ± 11.55 | 0.409 |
| KPS at admission | 89.0 ± 13.70 | 80.4 ± 12.41 | 0.010 |
| Volume in cm3 | 24.2 ± 19.3 | 22.22 ± 18.4 | 0.676 |
| Ki67 (%) | 18.7 ± 10.9 | 26.4 ± 15.4 | 0.061 |
| IDH Mutation status available in 166/177 pts | IDH Mutant 2/166 (6.7%) | IDH Mutant 0/166 | 0.027 |
| EGFR overexpression status available in 149/177 pts | EGFR Overexpressed 9/26 (34.6%) | EGFR Overexpressed 35/124 (28.2%) | 0. 333 |
| MGMT Methylation status available in 53/177 | MGMT Methylated 17 patients | MGMT Methylated 8 patients | 0.397 |
| p53Mutation status available in 150/177 pts | Mutant p53 Normal 18/27 (66.7%) | Mutant p53 66/124 (53.22%) | 0.144 |
| EOR | GTR 28/30patients (93.3%) STR 2/30 patients (6.7%) | GTR 133/147 patients (90.80%) STR 14/147 patients (9.20%) | 0.468 |
| KPS after Surgery | 81.0 ± 25.11 | 73.9 ± 19.9 | 0.163 |
| KPS at last Evaluation | 39.5 ± 15.8 | 37.9 ± 17.6 | 0.721 |
| Overall Survival | 26.68 ± 7.1 months | 10.8±4.8 months | 0.001 |
| Location | Frontal 14 (46.6%) | Frontal 47 (31.9%) | 0.314 |
| Temporal 11 (36.6%) | Temporal 39 (26.5%) | ||
| Occipital 4 (13.3%) | Occipital 13 (8.8%) | ||
| Parietal 4 (13.3%) | Parietal 34 (23.1%) | ||
| Insular 2 (6.7%) | Insular 8 (5.44%) | ||
| Rolandic 2 (6.7%) | Rolandic 1 (0.7%) | ||
| Corpus Callosum 0 (0.0%) | Corpus Callosum 5 (3.4%) | ||
| Side | Left 18 (60.0%) | Left 69 (46.9%) | 0.743 |
| Right 12 (20.0%) | Right 66 (44.8%) | ||
| Midline 0 (0.0%) | Midline 8 (5.44%) | ||
| Multifocal 0 (0.0%) | Multifocal 1 (0.7%) | ||
| Symptoms | Headache 8 (26.6%) | Headache 25 (17.1%) | 0.115 |
| Seizures 8 (26.6%) | Seizures 41 (27.9%) | 0.544 | |
| Speech Disturbance 0 (0.0%) | Speech Disturbance 27 (18.4%) | 0.531 | |
| Motor Dysfunction 5 (16.6%) | Motor Dysfunction 35 (23.8%) | 0.491 | |
| Sensory Disturbance 6 (20.0%) | Sensory Disturbance 21(14.3%) | 0.600 | |
| Visual Deficit 1 (3.3%) | Visual Deficit 5 (3.4%) | 0.423 | |
| Incidental 2 (6.7%) | Incidental 4 (2.7%) | 0.384 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armocida, D.; Pesce, A.; Di Giammarco, F.; Frati, A.; Santoro, A.; Salvati, M. Long Term Survival in Patients Suffering from Glio-blastoma Multiforme: A Single-Center Observational Cohort Study. Diagnostics 2019, 9, 209. https://doi.org/10.3390/diagnostics9040209
Armocida D, Pesce A, Di Giammarco F, Frati A, Santoro A, Salvati M. Long Term Survival in Patients Suffering from Glio-blastoma Multiforme: A Single-Center Observational Cohort Study. Diagnostics. 2019; 9(4):209. https://doi.org/10.3390/diagnostics9040209
Chicago/Turabian StyleArmocida, Daniele, Alessandro Pesce, Federico Di Giammarco, Alessandro Frati, Antonio Santoro, and Maurizio Salvati. 2019. "Long Term Survival in Patients Suffering from Glio-blastoma Multiforme: A Single-Center Observational Cohort Study" Diagnostics 9, no. 4: 209. https://doi.org/10.3390/diagnostics9040209
APA StyleArmocida, D., Pesce, A., Di Giammarco, F., Frati, A., Santoro, A., & Salvati, M. (2019). Long Term Survival in Patients Suffering from Glio-blastoma Multiforme: A Single-Center Observational Cohort Study. Diagnostics, 9(4), 209. https://doi.org/10.3390/diagnostics9040209