Use of Biomarkers in Ongoing Research Protocols on Alzheimer’s Disease

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
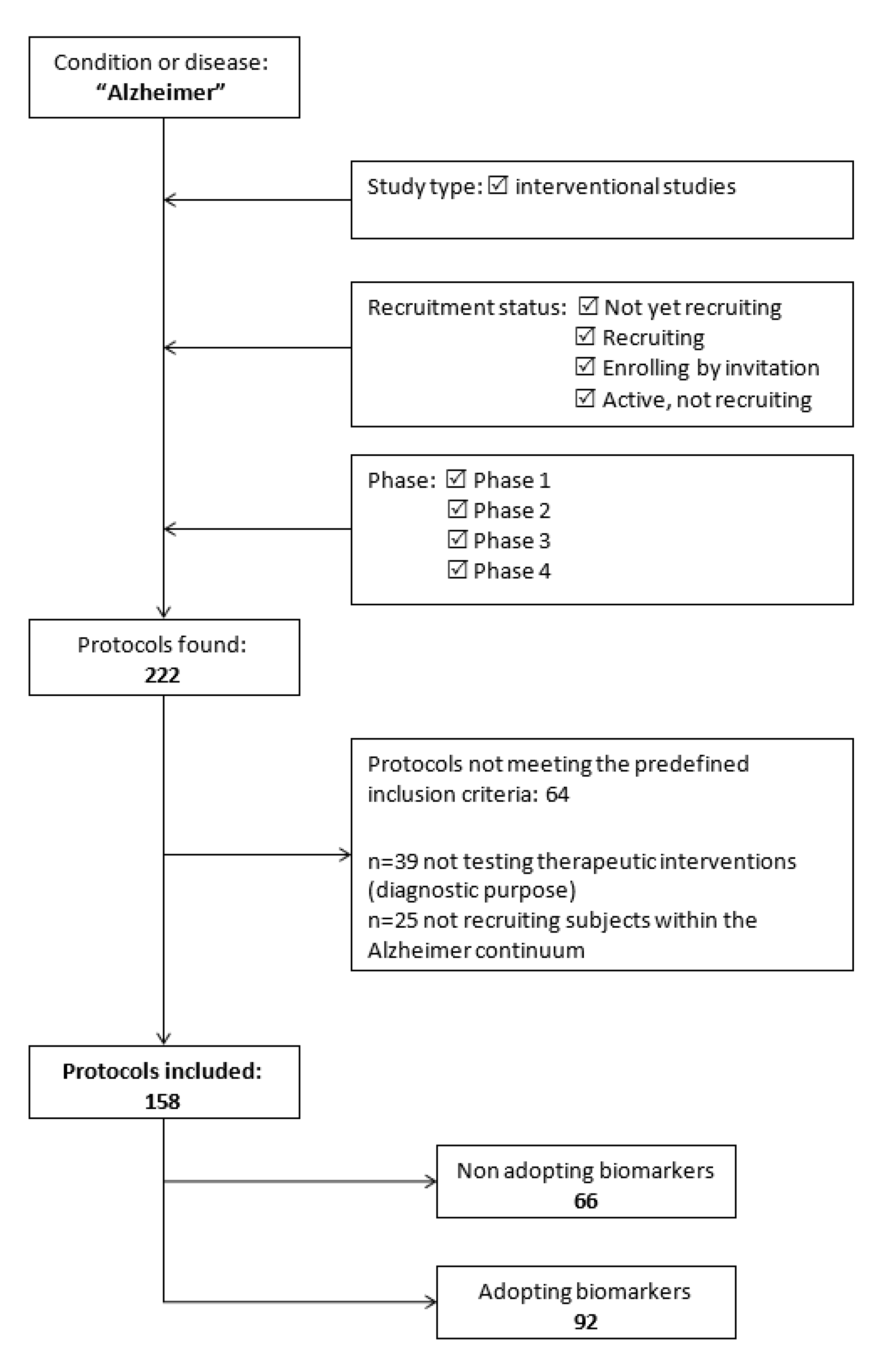
2.1. Data Source and Search Strategy
- i)
- Enrolling subjects with clinical disturbances and/or preclinical diagnoses falling within the AD continuum (i.e., preclinical AD, subjective cognitive decline, mild cognitive impairment, prodromal AD, and AD dementia) [3];
- ii)
- Testing the efficacy and/or safety/tolerability of a therapeutic (both pharmacological and non-pharmacological) intervention.
2.2. Data Extraction
- -
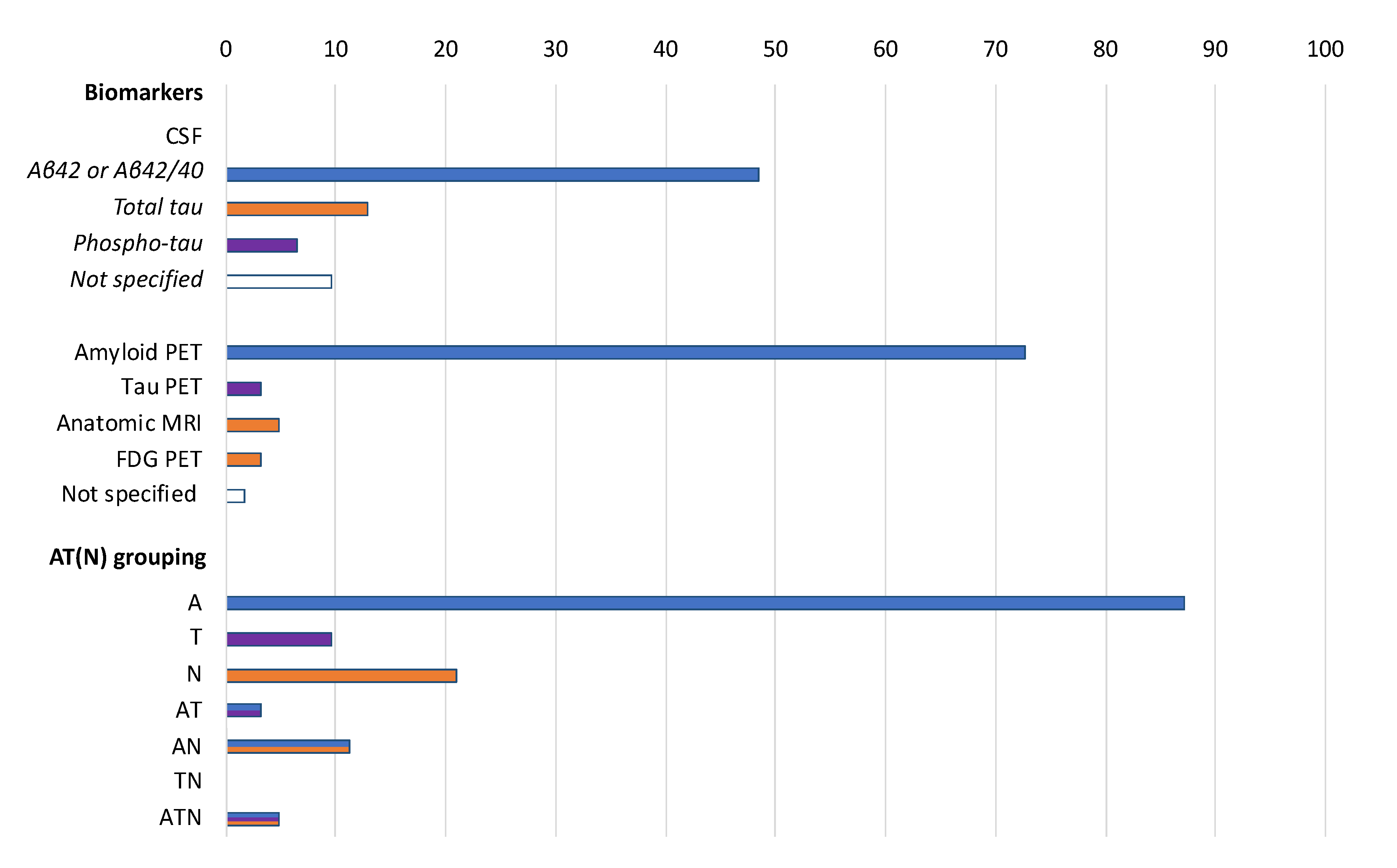
- A, amyloid deposition: (i) low cerebrospinal fluid (CSF) Aβ42 or Aβ42/Aβ40 ratio; and (ii) positive amyloid positron emission tomography (PET) scan;
- -
- T, tau pathology: (i) elevated CSF phospho-tau (p-tau); and (ii) positive tau PET scan;
- -
- N, neurodegeneration: (i) atrophy on anatomic magnetic resonance imaging (MRI); (ii) elevated CSF total tau (t-tau); and (iii) fluorodeoxyglucose (FDG) PET hypometabolism.
2.3. Data Analysis
3. Results
3.1. Search Results
3.2. Characteristics of Protocols Adopting Biomarkers
3.3. Use of Biomarkers in the Selection of Participants
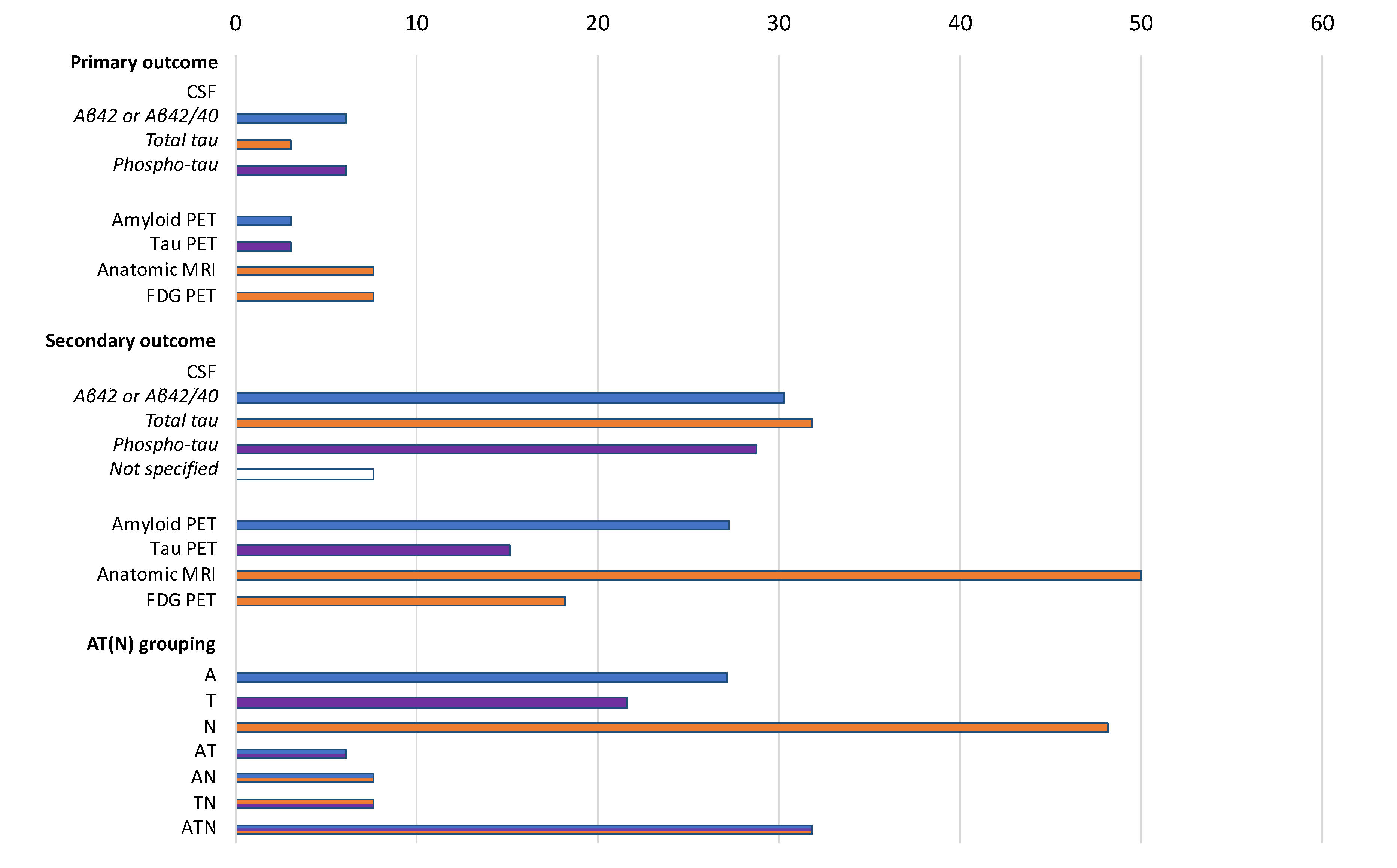
3.4. Use of Biomarkers as Study Outcomes
3.5. Use of Biomarkers Both as Eligibility Criteria and Study Outcomes
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R.; Albert, M.S.; Knopman, D.S.; McKhann, G.M.; Sperling, R.A.; Carrillo, M.C.; Thies, B.; Phelps, C.H. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Feldman, H.H.; Frisoni, G.B.; Hampel, H.; Jagust, W.J.; Johnson, K.A.; Knopman, D.S.; et al. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 2016, 87, 539–547. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Frisoni, G.B.; Boccardi, M.; Barkhof, F.; Blennow, K.; Cappa, S.; Chiotis, K.; Démonet, J.-F.; Garibotto, V.; Giannakopoulos, P.; Gietl, A.; et al. Strategic roadmap for an early diagnosis of Alzheimer’s disease based on biomarkers. Lancet Neurol. 2017, 16, 661–676. [Google Scholar] [CrossRef] [Green Version]
- Sancesario, G.M.; Toniolo, S.; Chiasserini, D.; Di Santo, S.G.; Zegeer, J.; Bernardi, G.; Musicco, M.; Caltagirone, C.; Parnetti, L.; Bernardini, S. The Clinical Use of Cerebrospinal Fluid Biomarkers for Alzheimer’s Disease Diagnosis: The Italian Selfie. J. Alzheimers Dis. 2017, 55, 1659–1666. [Google Scholar] [CrossRef]
- Canevelli, M.; Bacigalupo, I.; Gervasi, G.; Lacorte, E.; Massari, M.; Mayer, F.; Vanacore, N.; Cesari, M. Methodological Issues in the Clinical Validation of Biomarkers for Alzheimer’s Disease: The Paradigmatic Example of CSF. Front. Aging Neurosci. 2019, 11. [Google Scholar] [CrossRef]
- Brookmeyer, R.; Abdalla, N. Estimation of lifetime risks of Alzheimer’s disease dementia using biomarkers for preclinical disease. Alzheimers Dement. 2018, 14, 981–988. [Google Scholar] [CrossRef]
- Cummings, J. The Role of Biomarkers in Alzheimer’s Disease Drug Development. Adv. Exp. Med. Biol. 2019, 1118, 29–61. [Google Scholar] [CrossRef]
- Rothwell, P.M. External validity of randomised controlled trials: “To whom do the results of this trial apply?”. Lancet 2005, 365, 82–93. [Google Scholar] [CrossRef]
- Cummings, J.; Lee, G.; Ritter, A.; Sabbagh, M.; Zhong, K. Alzheimer’s disease drug development pipeline: 2019. Alzheimers Dement. 2019, 5, 272–293. [Google Scholar] [CrossRef] [PubMed]
- Van Maurik, I.S.; Slot, R.E.R.; Verfaillie, S.C.J.; Zwan, M.D.; Bouwman, F.H.; Prins, N.D.; Teunissen, C.E.; Scheltens, P.; Barkhof, F.; Wattjes, M.P.; et al. Personalized risk for clinical progression in cognitively normal subjects-the ABIDE project. Alzheimers Res. Ther. 2019, 11, 33. [Google Scholar] [CrossRef]
- Rossini, P.M.; Cappa, S.F.; Lattanzio, F.; Perani, D.; Spadin, P.; Tagliavini, F.; Vanacore, N. The Italian INTERCEPTOR Project: From the Early Identification of Patients Eligible for Prescription of Antidementia Drugs to a Nationwide Organizational Model for Early Alzheimer’s Disease Diagnosis. J. Alzheimers Dis. 2019, 72, 373–388. [Google Scholar] [CrossRef] [PubMed]
- Landau, S.M.; Horng, A.; Fero, A.; Jagust, W.J. Alzheimer’s Disease Neuroimaging Initiative Amyloid negativity in patients with clinically diagnosed Alzheimer disease and MCI. Neurology 2016, 86, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Canevelli, M.; Grande, G.; Lacorte, E.; Quarchioni, E.; Cesari, M.; Mariani, C.; Bruno, G.; Vanacore, N. Spontaneous Reversion of Mild Cognitive Impairment to Normal Cognition: A Systematic Review of Literature and Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 943–948. [Google Scholar] [CrossRef]
- Rosenberg, A.; Solomon, A.; Jelic, V.; Hagman, G.; Bogdanovic, N.; Kivipelto, M. Progression to dementia in memory clinic patients with mild cognitive impairment and normal β-amyloid. Alzheimers Res. Ther. 2019, 11, 99. [Google Scholar] [CrossRef] [Green Version]
- Jansen, W.J.; Ossenkoppele, R.; Knol, D.L.; Tijms, B.M.; Scheltens, P.; Verhey, F.R.J.; Visser, P.J.; Amyloid Biomarker Study Group; Aalten, P.; Aarsland, D.; et al. Prevalence of cerebral amyloid pathology in persons without dementia: A meta-analysis. JAMA 2015, 313, 1924–1938. [Google Scholar] [CrossRef]
- Roberts, J.S.; Dunn, L.B.; Rabinovici, G.D. Amyloid imaging, risk disclosure and Alzheimer’s disease: Ethical and practical issues. Neurodegener. Dis. Manag. 2013, 3, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Mattsson, N.; Carrillo, M.C.; Dean, R.A.; Devous, M.D.; Nikolcheva, T.; Pesini, P.; Salter, H.; Potter, W.Z.; Sperling, R.S.; Bateman, R.J.; et al. Revolutionizing Alzheimer’s disease and clinical trials through biomarkers. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2015, 1, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Kern, S.; Zetterberg, H.; Kern, J.; Zettergren, A.; Waern, M.; Höglund, K.; Andreasson, U.; Wetterberg, H.; Börjesson-Hanson, A.; Blennow, K.; et al. Prevalence of preclinical Alzheimer disease. Neurology 2018, 90, e1682–e1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brookmeyer, R.; Abdalla, N.; Kawas, C.H.; Corrada, M.M. Forecasting the prevalence of preclinical and clinical Alzheimer’s disease in the United States. Alzheimers Dement. 2018, 14, 121–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blennow, K.; Hampel, H.; Zetterberg, H. Biomarkers in amyloid-β immunotherapy trials in Alzheimer’s disease. Neuropsychopharmacology 2014, 39, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J. Disease modification and Neuroprotection in neurodegenerative disorders. Transl. Neurodegener. 2017, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Andrieu, S.; Sampaio, C.; Wilcock, G. Disease-modifying trials in Alzheimer’s disease: A European task force consensus. Lancet Neurol. 2007, 6, 56–62. [Google Scholar] [CrossRef]
- Barcikowska, M. European Medicines Agency Guideline on the clinical investigation of medicines for the treatment of Alzheimer’s disease. Lek. POZ 2018, 4, 370–374. [Google Scholar]
- Cummings, J.; Feldman, H.H.; Scheltens, P. The “rights” of precision drug development for Alzheimer’s disease. Alzheimer’s Res. Ther. 2019, 11, 76. [Google Scholar] [CrossRef] [Green Version]
- Wallace, L.M.K.; Theou, O.; Godin, J.; Andrew, M.K.; Bennett, D.A.; Rockwood, K. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer’s disease: A cross-sectional analysis of data from the Rush Memory and Aging Project. Lancet Neurol. 2019, 18, 177–184. [Google Scholar] [CrossRef]
- Sackett, D.L.; Haynes, R.B. The architecture of diagnostic research. BMJ 2002, 324, 539–541. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Adopting Biomarkers (n = 92) | Non Adopting Biomarkers (n = 66) | p | |
|---|---|---|---|
| Participants per study (n) | 120 (43–382) | 133 (43–267) | 0.77 |
| Phases | <0.01 | ||
| Phase 1 and Phase 1–2 | 22 (23.9) | 14 (21.2) | |
| Phase 2 and Phase 2–3 | 52 (56.5) | 24 (36.4) | |
| Phase 3 | 15 (16.3) | 18 (27.3) | |
| Phase 4 | 3 (3.3) | 10 (15.2) | |
| Condition | 0.21 | ||
| Enrolling participants with AD dementia | 74 (80.4) | 58 (87.9) | |
| Not enrolling participants with AD dementia | 18 (19.6) | 8 (12.1) | |
| Main sponsor | 0.12 | ||
| Industry | 56 (60.9) | 32 (48.5) | |
| Other | 36 (39.1) | 34 (51.5) | |
| Primary outcome | <0.001 | ||
| Safety | 33 (35.9) | 17 (25.8) | |
| Clinical improvement | 38 (41.3) | 47 (71.2) | |
| AD biological change | 21 (14.6) | 2 (3.0) | |
| Intervention | 0.04 | ||
| Pharmacological | 87 (94.6) | 56 (84.8) | |
| Non-pharmacological | 5 (5.4) | 10 (15.2) |
| CSF Cut-Offs | |
|---|---|
| NCT02547818 | Aβ42 ≥ 180 pg/mL and ≤ 690 pg/mL |
| NCT02947893 | Aβ42 < 600 ng/mL |
| NCT03061474 | Aβ42 ≤ 600 pg/mL or t-tau/Aβ42 ratio ≥ 0.39 |
| NCT03069014 | Aβ42 < 550 ng/L or Aβ40/42 ratio < 0.89 |
| NCT04079803 | t-tau/Aβ42 ratio ≥ 0.28 |
| NCT04191486 | Aβ ≤ 1000 pg/mL and p-tau 181 ≥ 19 pg/mL |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canevelli, M.; Remoli, G.; Bacigalupo, I.; Valletta, M.; Toccaceli Blasi, M.; Sciancalepore, F.; Bruno, G.; Cesari, M.; Vanacore, N. Use of Biomarkers in Ongoing Research Protocols on Alzheimer’s Disease. J. Pers. Med. 2020, 10, 68. https://doi.org/10.3390/jpm10030068
Canevelli M, Remoli G, Bacigalupo I, Valletta M, Toccaceli Blasi M, Sciancalepore F, Bruno G, Cesari M, Vanacore N. Use of Biomarkers in Ongoing Research Protocols on Alzheimer’s Disease. Journal of Personalized Medicine. 2020; 10(3):68. https://doi.org/10.3390/jpm10030068
Chicago/Turabian StyleCanevelli, Marco, Giulia Remoli, Ilaria Bacigalupo, Martina Valletta, Marco Toccaceli Blasi, Francesco Sciancalepore, Giuseppe Bruno, Matteo Cesari, and Nicola Vanacore. 2020. "Use of Biomarkers in Ongoing Research Protocols on Alzheimer’s Disease" Journal of Personalized Medicine 10, no. 3: 68. https://doi.org/10.3390/jpm10030068
APA StyleCanevelli, M., Remoli, G., Bacigalupo, I., Valletta, M., Toccaceli Blasi, M., Sciancalepore, F., Bruno, G., Cesari, M., & Vanacore, N. (2020). Use of Biomarkers in Ongoing Research Protocols on Alzheimer’s Disease. Journal of Personalized Medicine, 10(3), 68. https://doi.org/10.3390/jpm10030068