Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context
2.2. Study Participants
2.3. Study Protocol
2.4. Measured Outcomes
2.4.1. Patient-Reported Outcomes (Profile)
2.4.2. Patient-Reported Outcomes (PROs)
2.4.3. Technology-Reported Outcomes (TechROs)
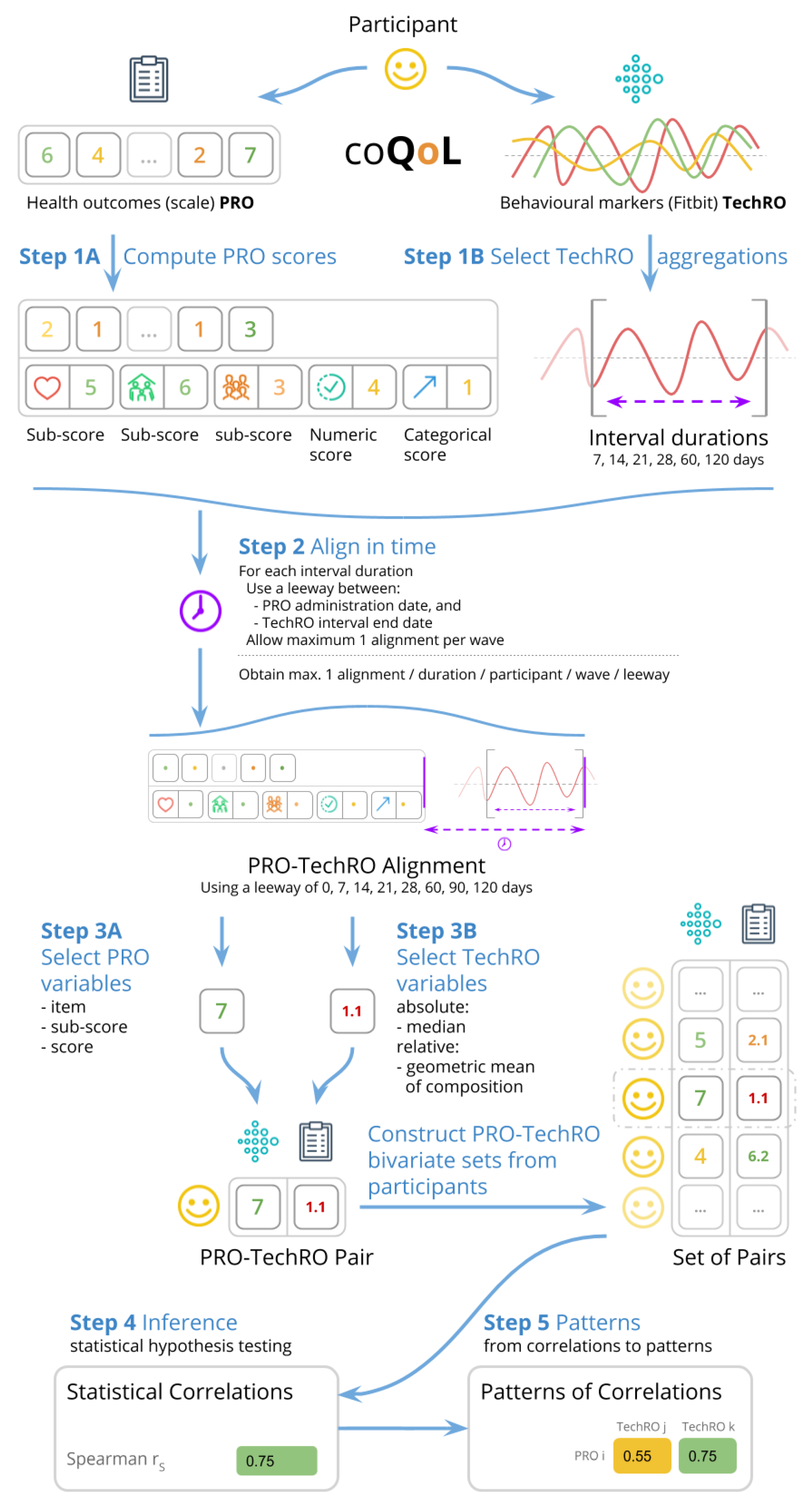
2.4.4. Co-Calibration (PROs vs. TechROs)
2.5. Data Analysis
2.5.1. Descriptive Analysis (PROs and TechROs)
2.5.2. Inferential Analysis (PROs vs. TechROs)
2.5.3. Pattern Analysis (PROs vs. TechROs)
3. Results
3.1. Study Participants
3.2. Descriptive Analysis (PROs and TechROs)
3.2.1. Patient-Reported Outcomes (Questionnaires)
3.2.2. Technology-Reported Outcomes (Fitbit)
3.3. Inferential Analysis (PROs vs. TechROs)
3.4. Pattern Analysis (PROs vs. TechROs)
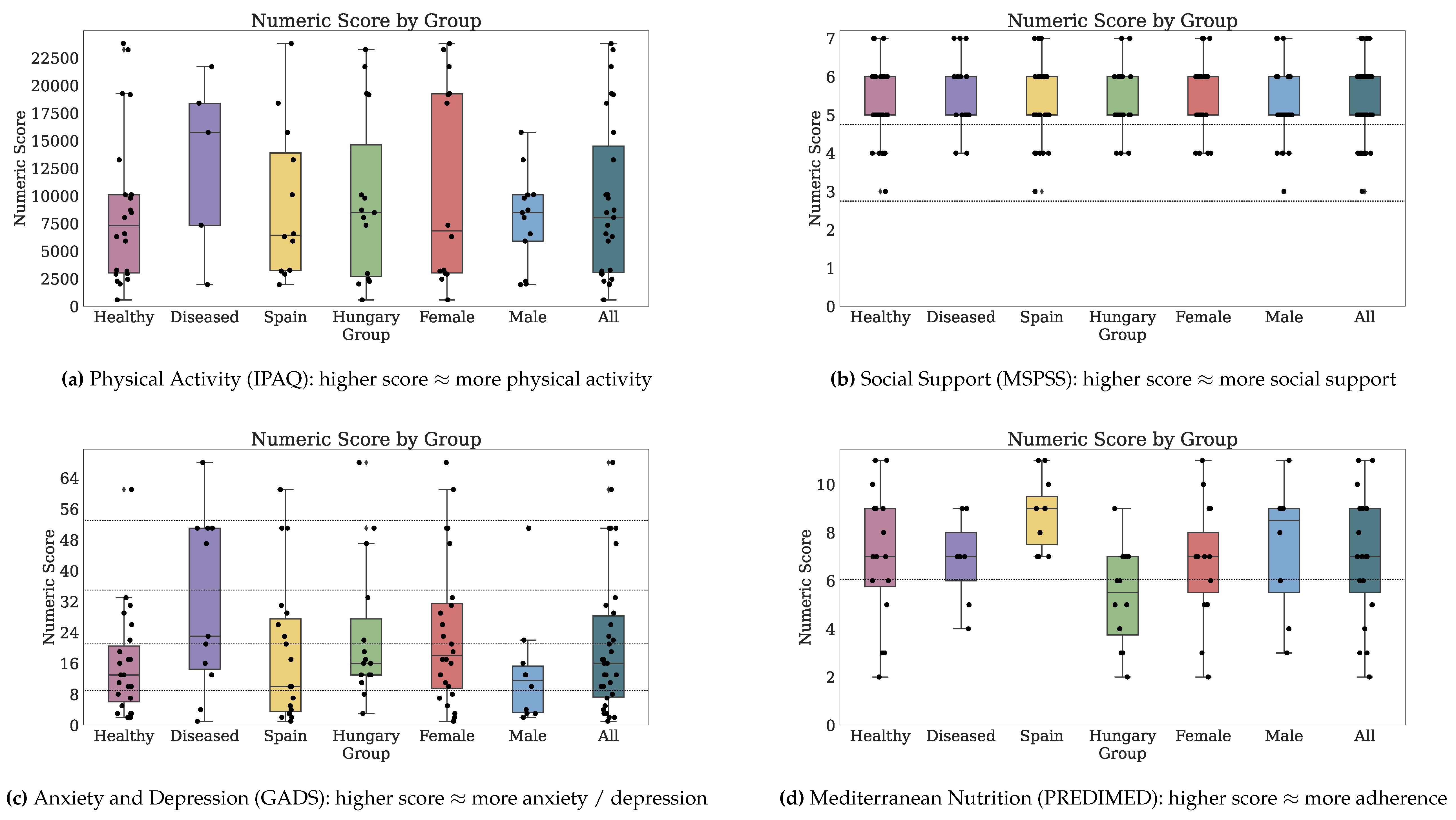
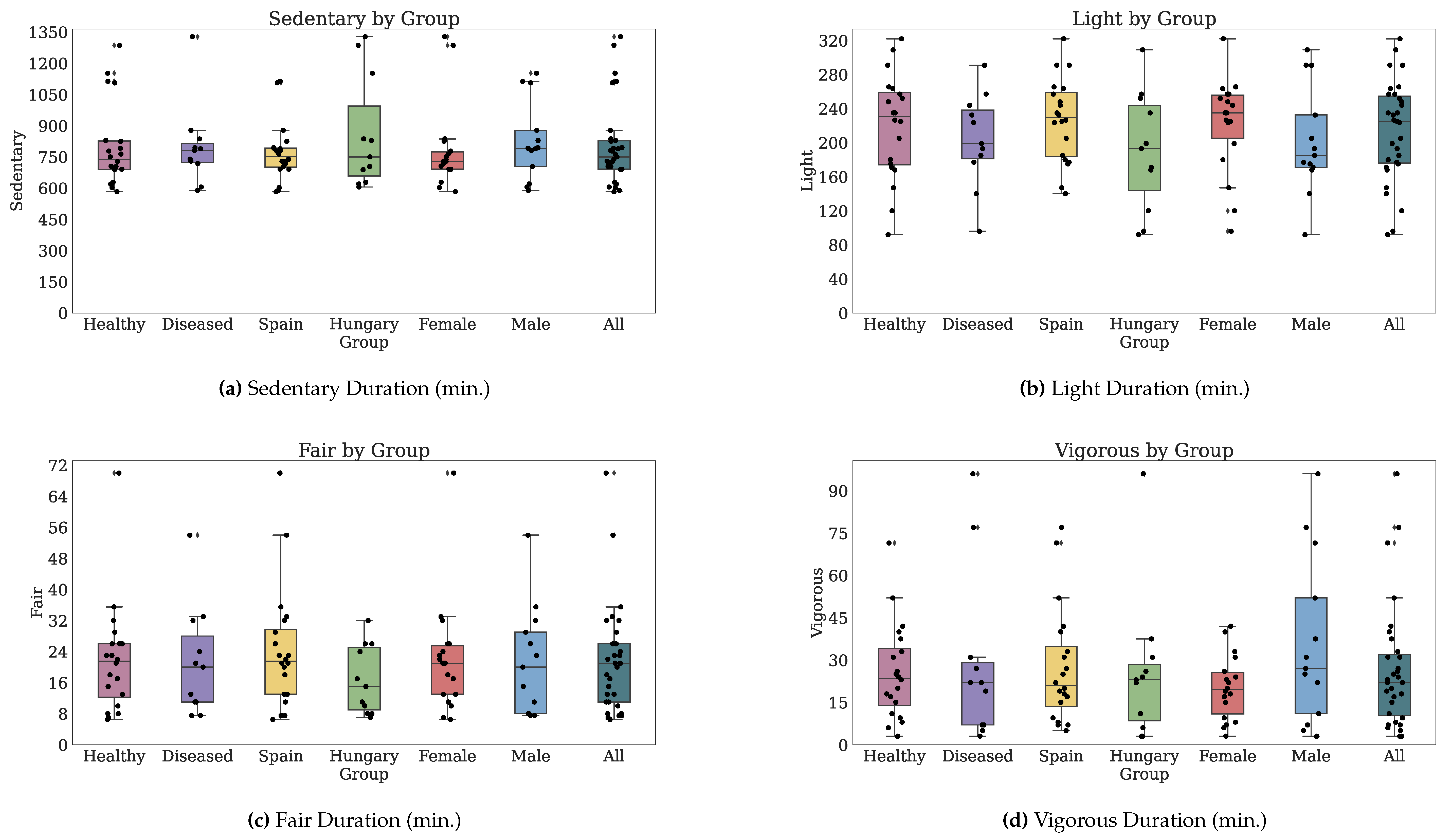
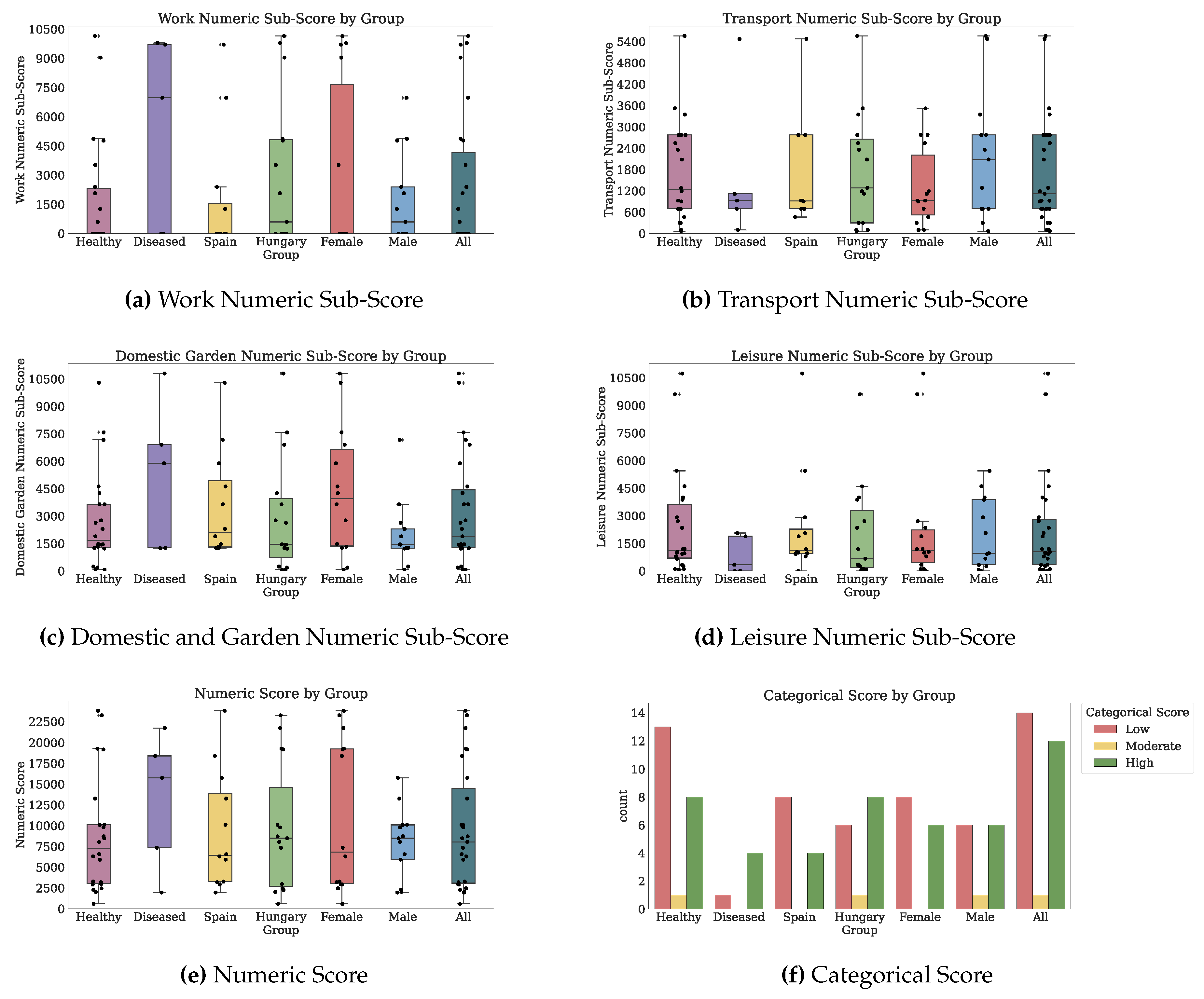
3.4.1. coQoL for Physical Activity (IPAQ vs. Fitbit)
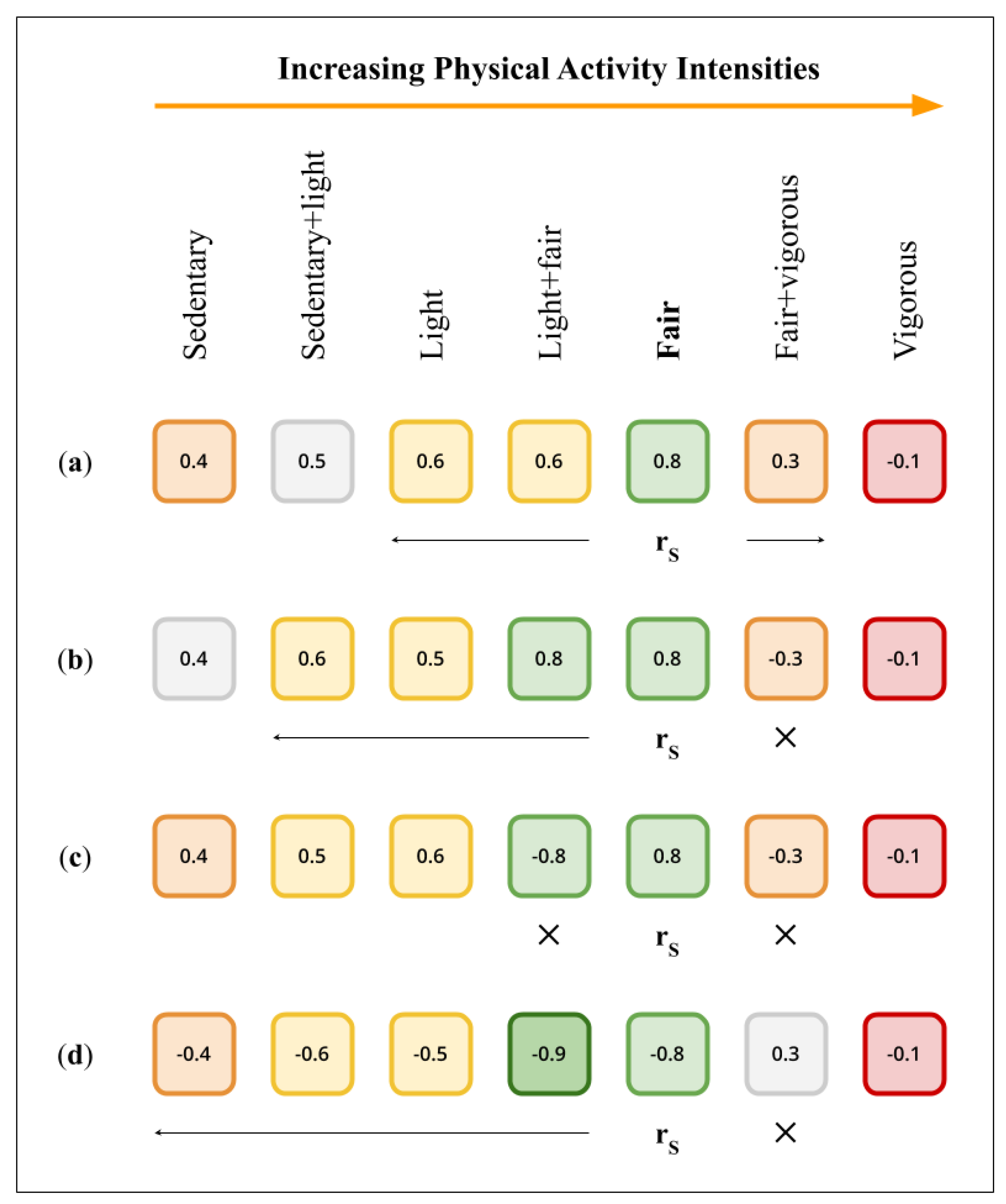
Physical Activity Outcomes by Total Numbers of Correlations
Physical Activity Outcomes by Contours of Correlations
Physical Activity Outcomes Highlighted by Both Metrics
Physical Activity Outcomes Interpretation
3.4.2. coQoL for Social Support (MSPSS vs. Fitbit)
Social Support Outcomes by Total Numbers of Correlations
Social Support Outcomes by Contours of Correlations
Social Support Outcomes Highlighted by Both Metrics
Social Support Outcomes Interpretation
3.4.3. coQoL for Anxiety and Depression (GADS vs. Fitbit)
Anxiety and Depression Outcomes by Total Numbers of Correlations
Anxiety and Depression Outcomes by Contours of Correlations
Anxiety and Depression Outcomes Highlighted by Both Metrics
Anxiety and Depression Outcomes Interpretation
3.4.4. coQoL for Mediterranean Nutrition (PREDIMED vs. Fitbit)
Mediterranean Nutrition Outcomes by Total Numbers of Correlations
Mediterranean Nutrition Outcomes by Contours of Correlations
Mediterranean Nutrition Outcomes Highlighted by Both Metrics
Mediterranean Nutrition Outcomes Interpretation
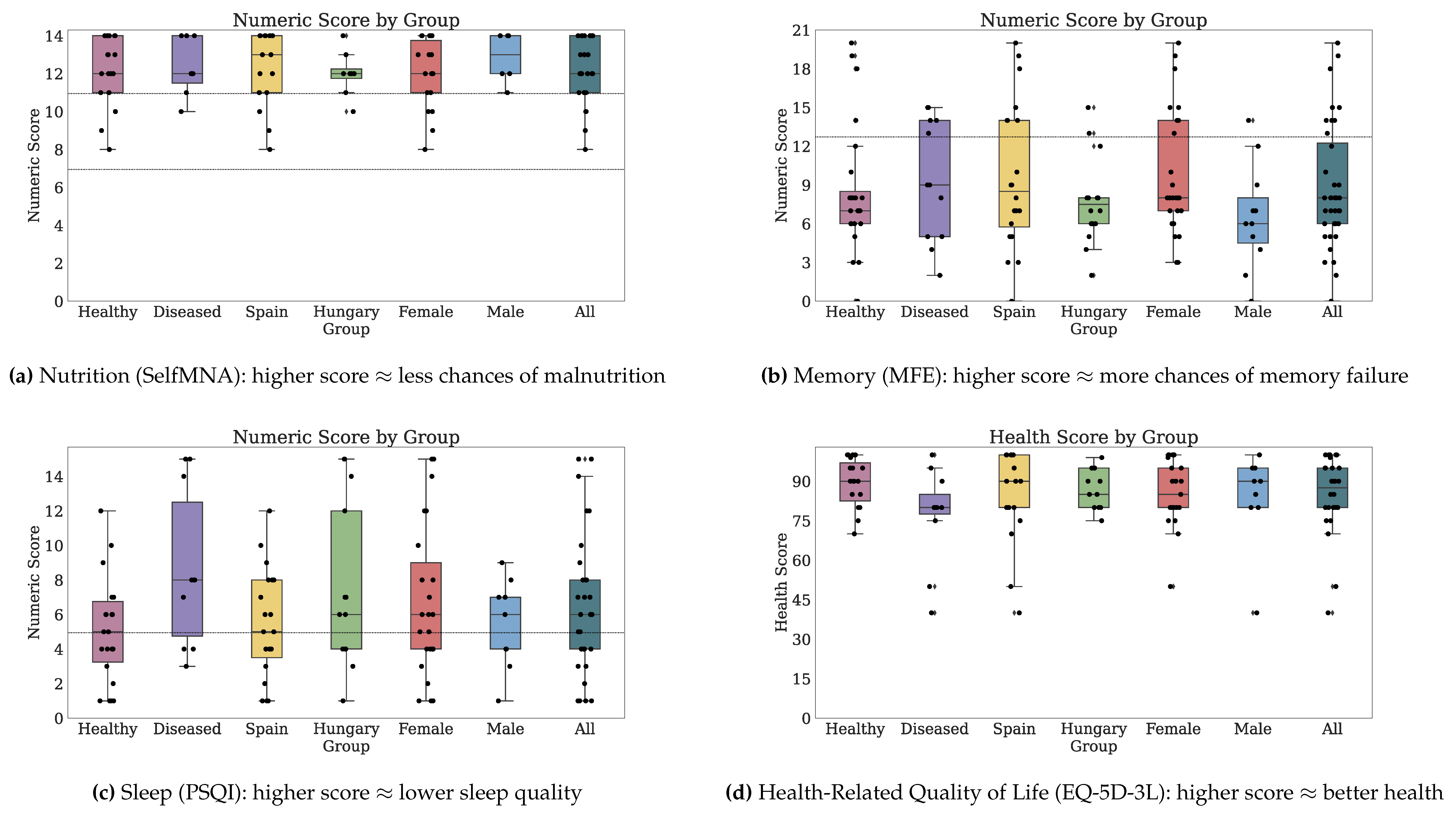
3.4.5. coQoL for Nutrition (SelfMNA vs. Fitbit)
Nutrition Outcomes by Total Numbers of Correlations
Nutrition Outcomes by Contours of Correlations
Nutrition Outcomes Highlighted by Both Metrics
Nutrition Outcomes Interpretation
3.4.6. coQoL for Memory (MFE vs. Fitbit)
Memory Outcomes by Total Numbers of Correlations
Memory Outcomes by Contours of Correlations
Memory Outcomes Highlighted by Both Metrics
Memory Outcomes Interpretation
3.4.7. coQoL for Sleep (PSQI vs. Fitbit)
Sleep Outcomes by Total Numbers of Correlations
Sleep Outcomes by Contours of Correlations
Sleep Outcomes Highlighted by Both Metrics
Sleep Outcomes Interpretation
3.4.8. coQoL for Health-Related Quality of Life (EQ-5D-3L vs. Fitbit)
Health-Related Quality of Life Outcomes by Total Numbers of Correlations
Health-Related Quality of Life Outcomes by Contours of Correlations
Health-Related Quality of Life Outcomes Highlighted by Both Metrics
Health-Related Quality of Life Outcomes Interpretation
3.5. Use Case Examples for coQoL
3.5.1. Longitudinal Data Example
3.5.2. Participant Story Example
4. Discussion
4.1. Overall Methodological Approach in PROomics
4.2. coQoL in Perspective of Past Evidence
4.3. Observations on Data Quality
4.4. Pathways towards Personalized Medicine
4.5. Study Limitations
4.6. Future Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| API | Application Programmable Interface |
| CLR | Centered Log Ratio |
| CLR PA | Centered Log Ratios of Physical Activity |
| CLR PA+S | Centered Log Ratios of Physical Activity and Sleep |
| CoME | Caregiver and Me |
| EQ-5D-3L | EuroQoL with 5 Domains and 3 Levels |
| GADS | Goldberg Anxiety and Depression Scale |
| IPAQ | International Physical Activity Questionnaire |
| MFE | Memory Failures of Everyday |
| MSPSS | Multidimensional Scale of Perceived Social Support |
| PREDIMED | Prevention with Mediterranean Diet |
| PRO | Patient-Reported Outcome |
| PSQI | Pittsburgh Sleep Quality Index |
| QoL | Quality of Life |
| SD | Standard Deviation |
| SelfMNA | Mini Nutritional Assessment |
| TechRO | Technology-Reported Outcome |
Appendix A. Literature Review
Appendix A.1. Literature Review Procedure

Appendix B. Materials and Methods
Appendix B.1. Patient-Reported Outcomes (Questionnaires)
Appendix B.1.1. Questionnaires

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Scale | Administration | Scoring |
|---|---|---|---|
| Profile | - | 27 items assessing: age, gender, ethnicity, profession, education, cohabitants, height, weight, blood pressure, cholesterol, smoking, alcohol, medication (hypertension), personal health history (diabetes, apnea, insomnia, hyperglycemia, stroke, infarct, depression), and family health history (hypertension, diabetes, stroke, infarct, dementia) | - |
| Physical Activity | International Physical Activity Questionnaire (IPAQ) [26] | 27 items of mixed types: yes/no, counts of days of physical activity per week, durations of physical activity per day. Recall: 2 weeks | Numeric score (estimated effort in metabolic equivalent of task). Categorical score with 3 levels: 0 low, 1 moderate, and 2 high. Numeric sub-scores for domains (work, leisure, transport, domestic and garden) and intensities of physical activity (sedentary, low, moderate, and vigorous). |
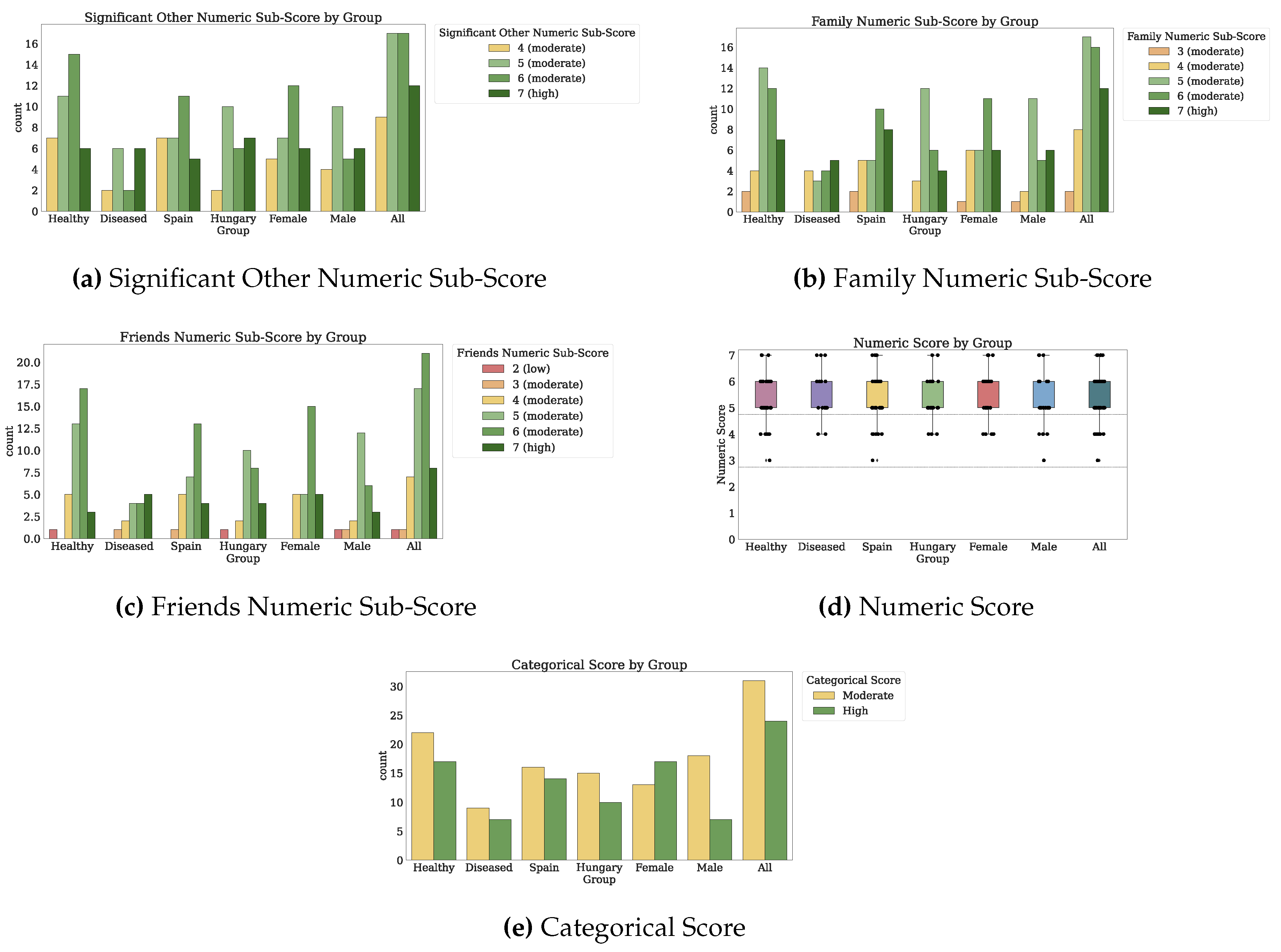
| Social Support | Multi-Dimensional Scale Perceived Social Support (MSPSS) [27] | 12 items on a 7-level Likert scale (Q1–Q12). Recall: indefinite | Numeric score increasing with social support (1–2.9: low, 3–5: moderate, 5.1–7: high). Categorical score with 3 levels: 0 low, 1 moderate, and 2 high. Numeric sub-scores (1–7) for three sources of social support: significant other, family, and friends. |
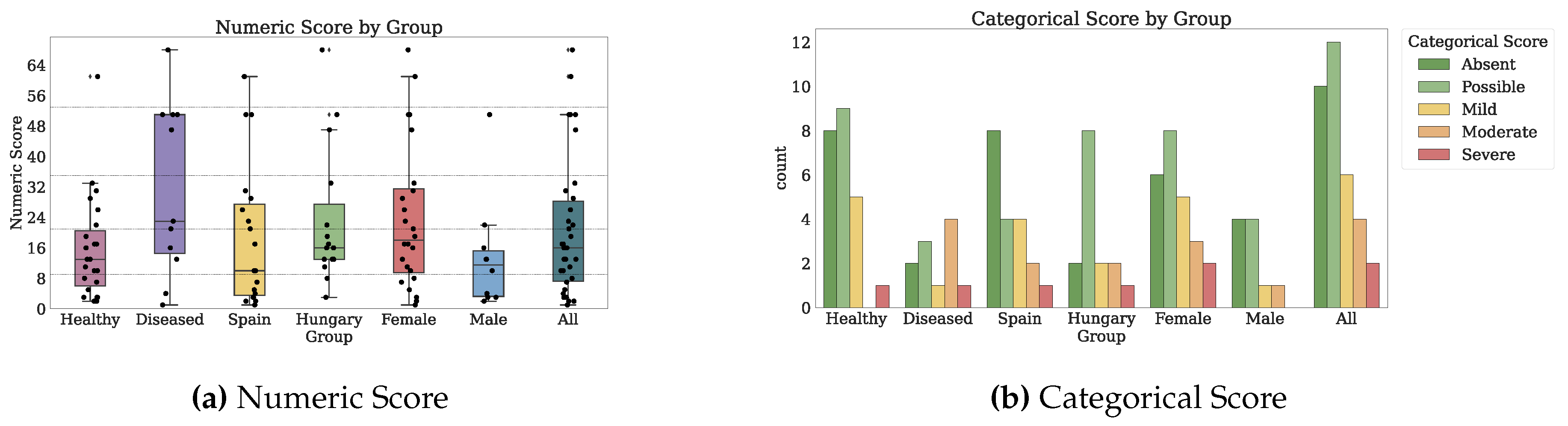
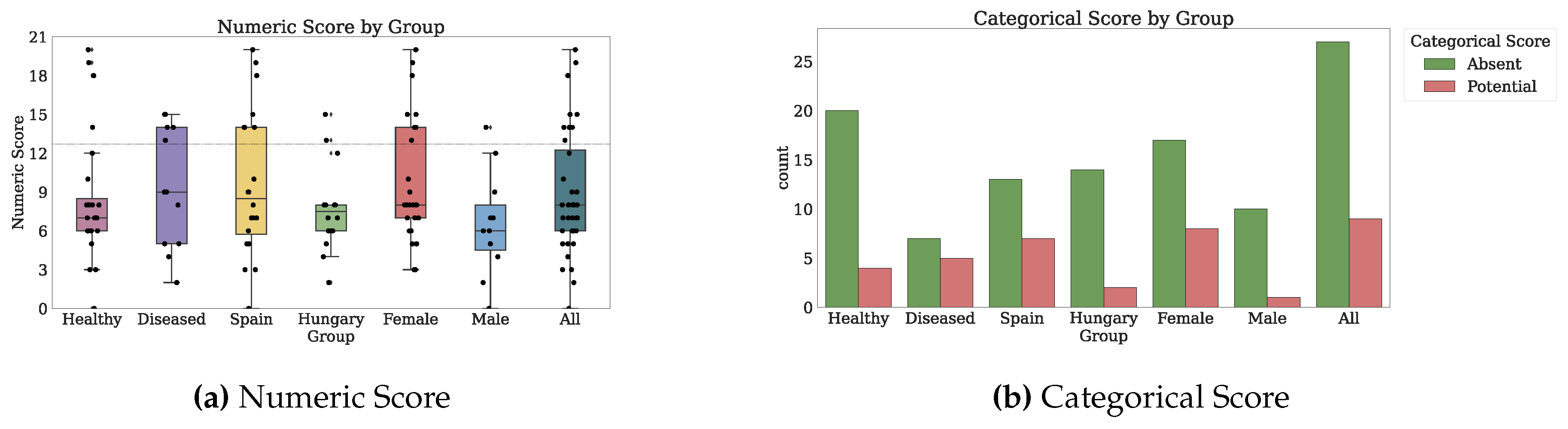
| Anxiety and Depression | Goldberg depression and anxiety scale (GADS) [28] | 18 items: 9 for Anxiety (denoted Q1A–Q9A), 9 for Depression (Q1D-Q9D), all on a 6-level Likert scale. The original answers were on a 2-level Likert scale. The collected answers are on a 6-level Likert scale. Recall: 1 month | Numeric score increasing with depression and anxiety: 0–9 no depression, 10–21 possible depression, 22–35 mild depression, 36–53 moderate depression, and 54–90 severe depression. Categorical score with 5 levels: 0 absent, 1 possible, 2 mild, 3 moderate, 4 severe. |
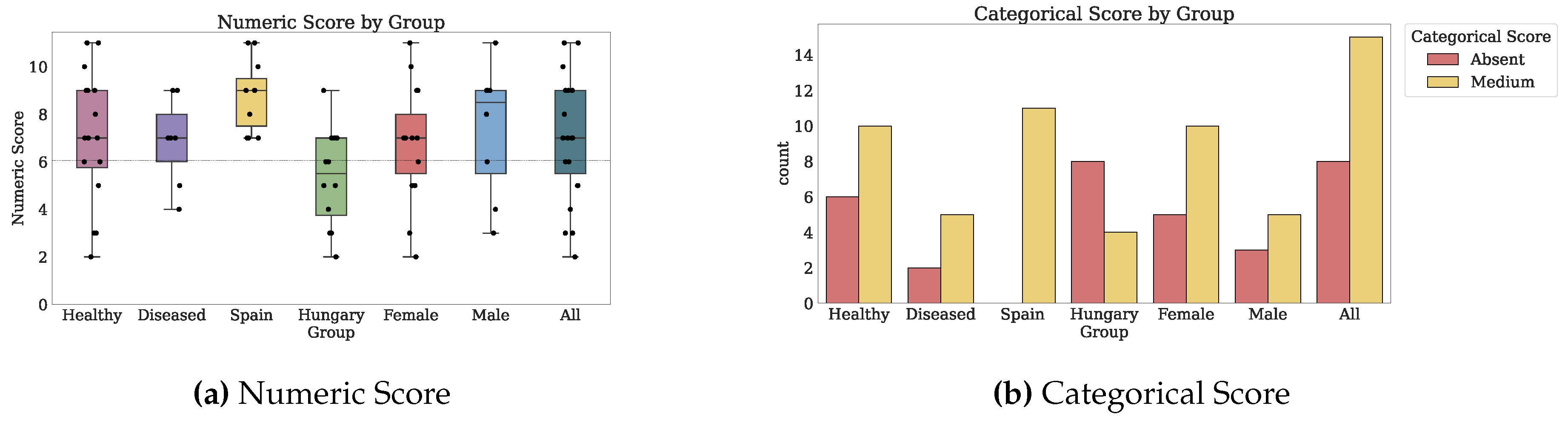
| Nutrition Mediterranean | Prevention with Mediterranean Diet (PREDIMED) [29,30] | 14 binary items: 2 items yes/no, 12 items with thresholds for ingested food quantity (Q1–Q14). Recall: indefinite | Numeric score from 0–6 for no adherence to 7–12 for medium adherence to 13–14 for high adherence. Categorical score with 3 levels: 0 absent, 1 medium, 2 high. |
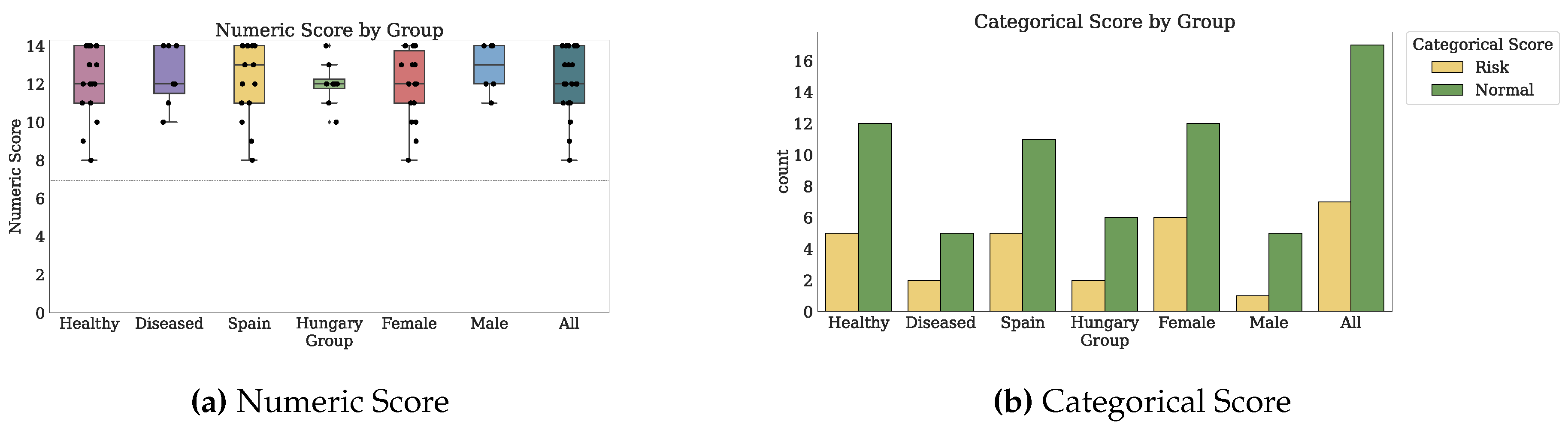
| Nutrition | Self-Reported Mini Nutritional Assessment (SelfMNA) [31] | 6 items: 5 on various levels Likert scales, 1 binary (Q1–Q6). Recall: 3 months, same day | Numeric score from 0–7 for malnourished to 8–11 for risk of malnutrition to 12–14 for normal nutrition. Categorical score with 3 levels: 0 for malnutrition, 1 for risk, and 2 for normal nutrition. |
| Memory | Memory Failures of Everyday (MFE) [32] | 28 items on a 3-level Likert scale (Q1–Q28). Recall: indefinite | Numeric score from 0 for no memory failures to 56 for potential memory failures. Categorical score separating 0 for no memory failures and 1 for potential memory failures, by comparing with deviations from the mean. |
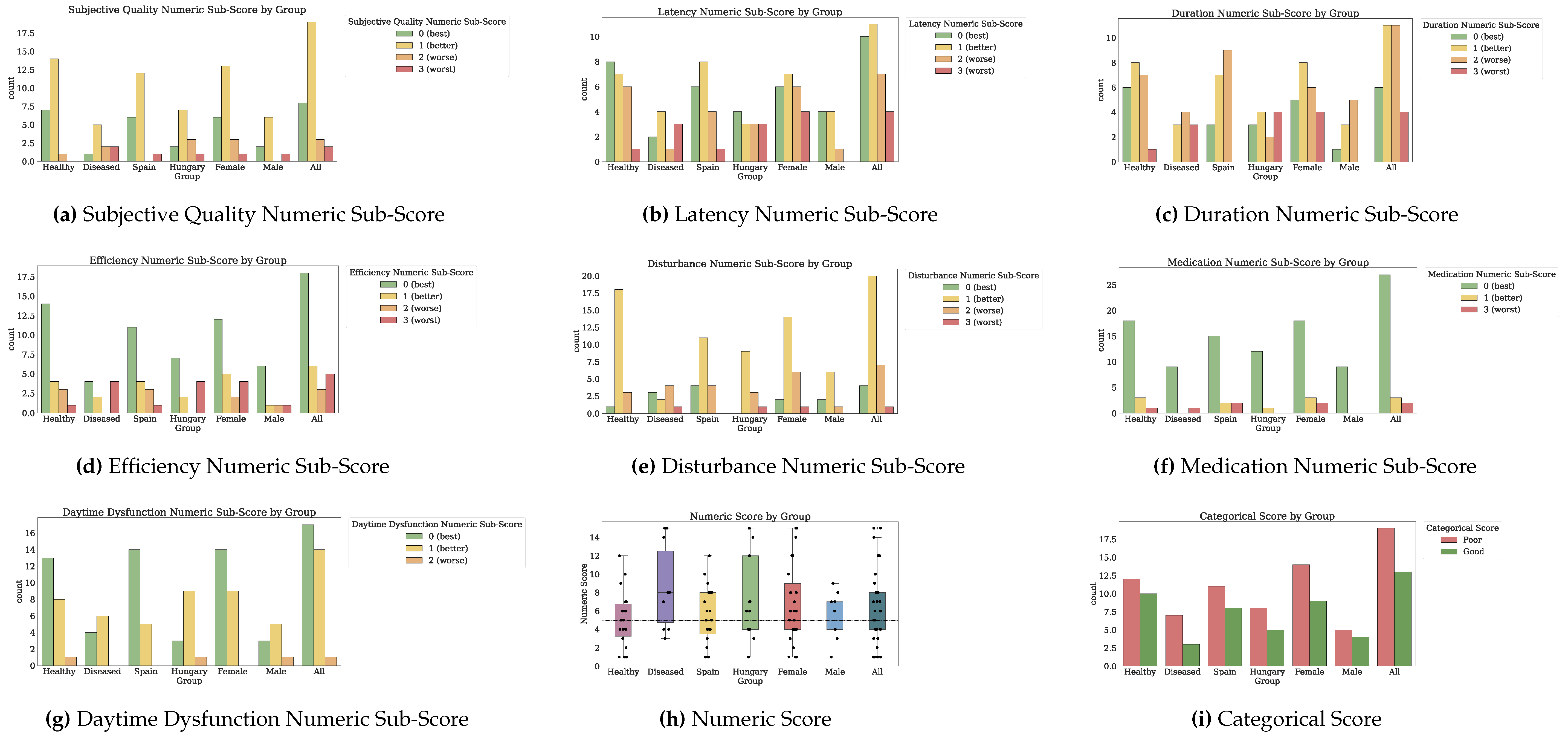
| Sleep | Pittsburgh Sleep Quality Index (PSQI) [33] | 25 items of mixed types: durations, yes/no, Likert scales (Q1, ..., Q4, Q5A, ..., Q5J, Q6, ..., Q9). Recall: 1 month | Numeric score increasing as sleep quality decreases on a 0-21 scale. Categorical score of 1 for good sleep quality (0–4) and 0 for poor sleep quality (5–21). Numeric sub-scores (0–7) for: quality, latency, duration, efficiency, disturbance, medication, and daytime dysfunction. |
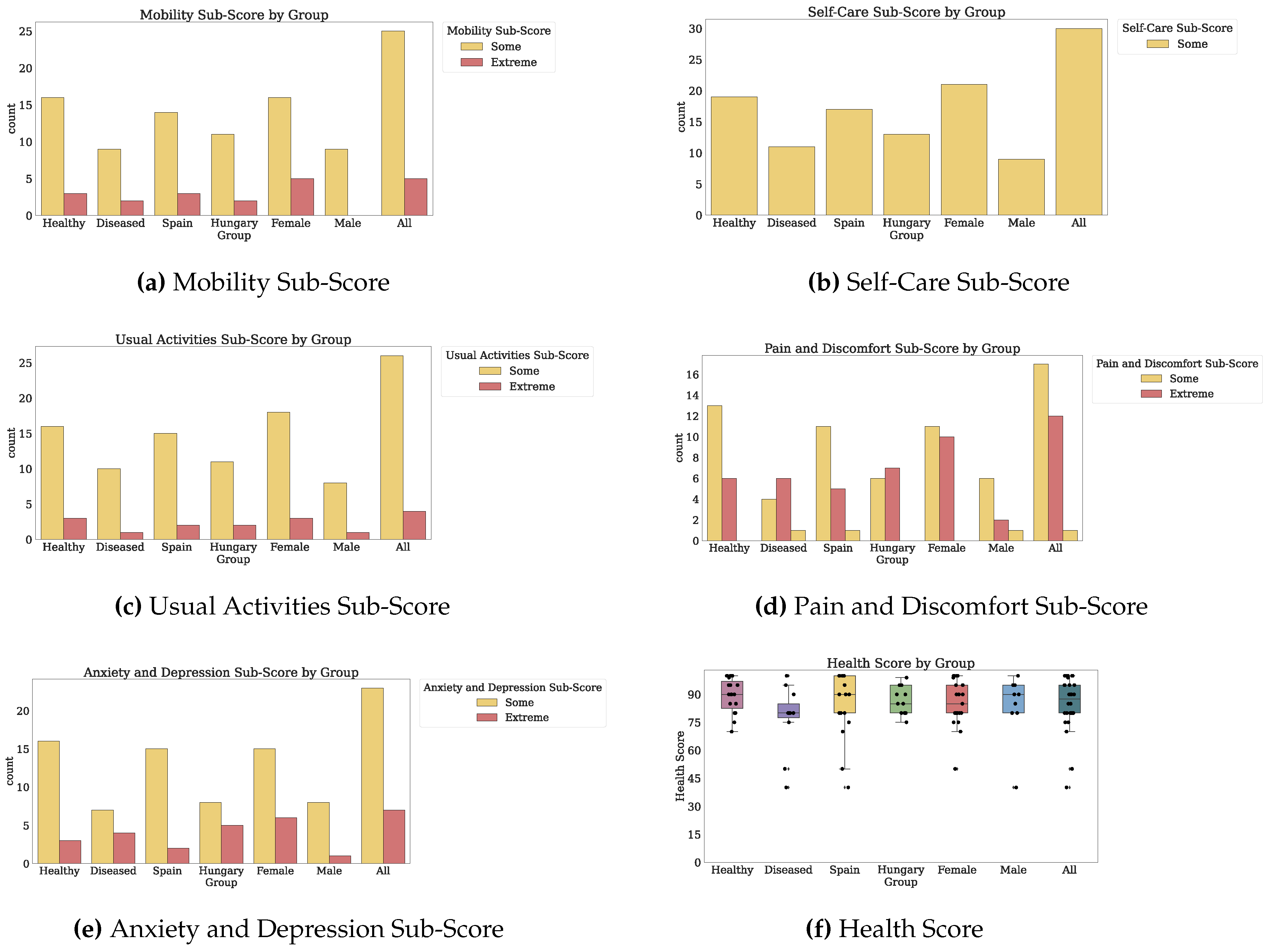
| Health-Related Quality of Life | EuroQoL health questionnaire (EQ-5D-3L) [34] | 6 items: 5 on a 3-level Likert scale (denoted by their measured outcomes), 1 on a visual analog scale (Q1–Q6). Recall: same day | Numeric scores for five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, for the Likert items, increasing from 1 to 3 as life quality decreases. Visual analog scale of health state on the day of administration (giving a health score of 0–100), where higher numbers indicate better health. |
Appendix B.1.2. Questionnaire Administration
Appendix B.1.3. Answers Scoring
Appendix B.1.4. Variables Derivation
Appendix B.2. Technology-Reported Outcomes (Fitbit)
Appendix B.2.1. Fitbit Consumer Wearable
Appendix B.2.2. Wearable Data Processing
Appendix B.2.3. Variables Derivation
Appendix B.3. Co-Calibration Using coQoL
Appendix B.3.1. Descriptive Analysis (PROs and TechROs)
Appendix B.3.2. Inferential Analysis (PROs vs. TechROs)
Appendix B.3.3. Pattern Analysis (PROs vs. TechROs)

Appendix C. Results
Appendix C.1. Descriptive Analysis (PROs and TechROs)
Appendix C.1.1. Patient-Reported Outcomes (Questionnaires)
| Physical Activity (IPAQ) | Social Support (MSPSS) | Anxiety and Depression (GADS) | Mediterranean Nutrition (PREDIMED) | Nutrition (SelfMNA) | Memory (MFE) | Sleep (PSQI) | Quality of Life (IPAQ) | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PID | Health | Country | Gender | Age | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | ||||||||
| 575 | Healthy | Hungary | Female | 65 | 5.0 | 8.0 | 5.0 | 7.0 | 3.0 | 85.0 | ||||||||||||||||||||||||||
| 569 | Healthy | Hungary | Female | 67 | 23,238.0 | 7.0 | 6.0 | 6.0 | 19.0 | 11.0 | 7.0 | 11.0 | 8.0 | 6.0 | 4.0 | 80.0 | 80.0 | 95.0 | ||||||||||||||||||
| 133 | Healthy | Hungary | Female | 71 | 19,164.0 | 19,262.9 | 6.0 | 6.0 | 6.0 | 17.0 | 13.0 | 6.0 | 14.0 | 8.0 | 7.0 | 6.0 | 4.0 | 95.0 | 95.0 | 99.0 | ||||||||||||||||
| 420 | Healthy | Hungary | Female | 71 | 576.0 | 2958.0 | 5.0 | 4.0 | 16.0 | 2.0 | 13.0 | 8.0 | 7.0 | 80.0 | 80.0 | |||||||||||||||||||||
| 215 | Healthy | Hungary | Female | 87 | 2446.0 | 5.0 | 33.0 | 3.0 | 10.0 | 8.0 | 12.0 | 80.0 | ||||||||||||||||||||||||
| 576 | Healthy | Hungary | Male | 60 | 2268.0 | 5.0 | 95.0 | |||||||||||||||||||||||||||||
| 535 | Healthy | Hungary | Male | 69 | 8712.0 | 6.0 | 3.0 | 9.0 | 12.0 | 6.0 | 1.0 | 95.0 | ||||||||||||||||||||||||
| 170 | Healthy | Hungary | Male | 70 | 8038.5 | 10,088.0 | 5.0 | 5.0 | 22.0 | 3.0 | 6.0 | 6.0 | 90.0 | 85.0 | ||||||||||||||||||||||
| 212 | Healthy | Hungary | Male | 72 | 8478.0 | 9793.5 | 5.0 | 4.0 | 5.0 | 90.0 | 90.0 | 90.0 | ||||||||||||||||||||||||
| 419 | Healthy | Hungary | Male | 95 | 2016.0 | 5.0 | 4.0 | 13.0 | 6.0 | 12.0 | 12.0 | 7.0 | 90.0 | 95.0 | ||||||||||||||||||||||
| 643 | Healthy | Spain | Female | 67 | 23,793.0 | 7.0 | 6.0 | 2.0 | 7.0 | 9.0 | 14.0 | 8.0 | 3.0 | 1.0 | 4.0 | 100.0 | 90.0 | |||||||||||||||||||
| 798 | Healthy | Spain | Female | 67 | 6.0 | 90.0 | ||||||||||||||||||||||||||||||
| 803 | Healthy | Spain | Female | 67 | 5.0 | 80.0 | ||||||||||||||||||||||||||||||
| 617 | Healthy | Spain | Female | 69 | 3186.0 | 4.0 | 4.0 | 61.0 | 7.0 | 13.0 | 19.0 | 10.0 | 100.0 | 90.0 | ||||||||||||||||||||||
| 620 | Healthy | Spain | Female | 69 | 3264.4 | 6.0 | 29.0 | 10.0 | 9.0 | 20.0 | 2.0 | 90.0 | ||||||||||||||||||||||||
| 640 | Healthy | Spain | Female | 69 | 5.0 | 26.0 | 14.0 | 10.0 | 6.0 | 70.0 | ||||||||||||||||||||||||||
| 628 | Healthy | Spain | Female | 70 | 7.0 | 3.0 | 11.0 | 5.0 | 1.0 | 100.0 | ||||||||||||||||||||||||||
| 638 | Healthy | Spain | Female | 71 | 6303.0 | 6.0 | 6.0 | 10.0 | 12.0 | 7.0 | 5.0 | 100.0 | 100.0 | |||||||||||||||||||||||
| 648 | Healthy | Spain | Female | 72 | 6.0 | 5.0 | 11.0 | 13.0 | 3.0 | 1.0 | 80.0 | |||||||||||||||||||||||||
| 649 | Healthy | Spain | Female | 72 | 14.0 | 80.0 | ||||||||||||||||||||||||||||||
| 795 | Healthy | Spain | Female | 72 | 2910.0 | 6.0 | 17.0 | 7.0 | 8.0 | 6.0 | 6.0 | 90.0 | ||||||||||||||||||||||||
| 630 | Healthy | Spain | Female | 74 | 5.0 | 31.0 | 12.0 | 18.0 | 12.0 | 75.0 | ||||||||||||||||||||||||||
| 411 | Healthy | Spain | Male | 45 | 5.0 | 80.0 | ||||||||||||||||||||||||||||||
| 790 | Healthy | Spain | Male | 66 | 10,101.0 | 6.0 | 3.0 | 11.0 | 14.0 | 7.0 | 4.0 | 100.0 | ||||||||||||||||||||||||
| 700 | Healthy | Spain | Male | 67 | 3.0 | 10.0 | 8.0 | 7.0 | 9.0 | 40.0 | ||||||||||||||||||||||||||
| 636 | Healthy | Spain | Male | 68 | 13,258.0 | 5.0 | 5.0 | 40.0 | 40.0 | |||||||||||||||||||||||||||
| 793 | Healthy | Spain | Male | 68 | 6560.0 | 5.0 | 100.0 | |||||||||||||||||||||||||||||
| 796 | Healthy | Spain | Male | 74 | 5907.0 | 4.0 | 2.0 | 9.0 | 14.0 | 0.0 | 80.0 | |||||||||||||||||||||||||
| 502 | Diseased | Hungary | Female | 63 | 80.0 | |||||||||||||||||||||||||||||||
| 169 | Diseased | Hungary | Female | 69 | 7338.0 | 21,702.0 | 5.0 | 5.0 | 5.0 | 68.0 | 51.0 | 47.0 | 7.0 | 5.0 | 7.0 | 12.0 | 12.0 | 13.0 | 15.0 | 8.0 | 15.0 | 15.0 | 14.0 | 80.0 | 75.0 | 80.0 | ||||||||||
| 132 | Diseased | Hungary | Male | 71 | 6.0 | 6.0 | 7.0 | 16.0 | 13.0 | 4.0 | 2.0 | 5.0 | 4.0 | 4.0 | 80.0 | 80.0 | 90.0 | |||||||||||||||||||
| 800 | Diseased | Spain | Female | 65 | 4.0 | 1.0 | 7.0 | 14.0 | 9.0 | 4.0 | 100.0 | |||||||||||||||||||||||||
| 641 | Diseased | Spain | Female | 71 | 18,390.0 | 5.0 | 6.0 | 51.0 | 23.0 | 9.0 | 10.0 | 15.0 | 14.0 | 8.0 | 50.0 | 80.0 | ||||||||||||||||||||
| 624 | Diseased | Spain | Female | 72 | 6.0 | 21.0 | 14.0 | 5.0 | 8.0 | 80.0 | ||||||||||||||||||||||||||
| 644 | Diseased | Spain | Male | 70 | 7.0 | 40.0 | ||||||||||||||||||||||||||||||
| 625 | Diseased | Spain | Male | 72 | 5.0 | 51.0 | 11.0 | 14.0 | 8.0 | 40.0 | ||||||||||||||||||||||||||
| 634 | Diseased | Spain | Male | 72 | 15,748.5 | 5.0 | 5.0 | 3.0 | 40.0 | 40.0 | ||||||||||||||||||||||||||
| 791 | Diseased | Spain | Male | 72 | 1953.0 | 7.0 | 100.0 | |||||||||||||||||||||||||||||
| 799 | Diseased | Spain | Male | 79 | 4.0 | 4.0 | 9.0 | 14.0 | 9.0 | 7.0 | 95.0 | |||||||||||||||||||||||||
Physical Activity (IPAQ)
| ID | Health | Wave | Country | Gender | Age | Work Domain Walking Minutes | Work Domain Moderate Minutes | Work Domain Vigorous Minutes | Work Domain Total | Active Transport Domain Walking Minutes | Active Transport Domain Cycling Minutes | Active Transport Domain Total | Domestic Home Domain Moderate Minutes | Domestic Garden Domain Moderate Minutes | Domestic Garden Domain Vigorous Minutes | Domestic Garden Domain Total | Leisure Domain Walking Minutes | Leisure Domain Moderate Minutes | Leisure Domain Vigorous Minutes | Leisure Domain Total | Work Domain Numeric Sub-Score | Leisure Domain Numeric Sub-Score | Active Transport Domain Numeric Sub-Score | Domestic Garden Domain Numeric Sub-Score | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 420 | Healthy | 1 | Hungary | Female | 71 | 0 | 0 | 0 | 0 | 90 | 0 | 90 | 60 | 0 | 0 | 60 | 30 | 0 | 0 | 30 | 0 | 99 | 297 | 180 | 576 | 0 |
| 791 | Diseased | 3 | Spain | Male | 72 | 0 | 0 | 0 | 0 | 210 | 0 | 210 | 420 | 0 | 0 | 420 | 0 | 0 | 0 | 0 | 0 | 0 | 693 | 1260 | 1953 | 0 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 0 | 0 | 0 | 0 | 90 | 0 | 90 | 70 | 105 | 150 | 325 | 80 | 0 | 0 | 80 | 0 | 264 | 297 | 1455 | 2016 | 0 |
| 576 | Healthy | 2 | Hungary | Male | 60 | 20 | 360 | 70 | 450 | 20 | 0 | 20 | 10 | 10 | 0 | 20 | 20 | 0 | 0 | 20 | 2066 | 66 | 66 | 70 | 2268 | 1 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 0 | 0 | 0 | 0 | 360 | 0 | 360 | 10 | 10 | 0 | 20 | 360 | 0 | 0 | 360 | 0 | 1188 | 1188 | 70 | 2446 | 0 |
| 795 | Healthy | 3 | Spain | Female | 72 | 0 | 0 | 0 | 0 | 140 | 0 | 140 | 420 | 0 | 0 | 420 | 360 | 0 | 0 | 360 | 0 | 1188 | 462 | 1260 | 2910 | 0 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 0 | 0 | 0 | 0 | 30 | 0 | 30 | 920 | 0 | 0 | 920 | 30 | 0 | 0 | 30 | 0 | 99 | 99 | 2760 | 2958 | 0 |
| 617 | Healthy | 2 | Spain | Female | 69 | 0 | 0 | 0 | 0 | 280 | 0 | 280 | 210 | 210 | 0 | 420 | 240 | 0 | 0 | 240 | 0 | 792 | 924 | 1470 | 3186 | 0 |
| 620 | Healthy | 2 | Spain | Female | 69 | 0 | 0 | 0 | 0 | 273 | 0 | 273 | 360 | 61 | 0 | 421 | 315 | 0 | 0 | 315 | 0 | 1039 | 900 | 1324 | 3264 | 0 |
| 796 | Healthy | 3 | Spain | Male | 74 | 0 | 0 | 0 | 0 | 210 | 0 | 210 | 210 | 210 | 150 | 570 | 630 | 210 | 0 | 840 | 0 | 2919 | 693 | 2295 | 5907 | 0 |
| 638 | Healthy | 2 | Spain | Female | 71 | 0 | 0 | 0 | 0 | 210 | 0 | 210 | 420 | 840 | 0 | 1260 | 300 | 0 | 0 | 300 | 0 | 990 | 693 | 4620 | 6303 | 0 |
| 793 | Healthy | 3 | Spain | Male | 68 | 140 | 70 | 65 | 275 | 210 | 0 | 210 | 105 | 420 | 300 | 825 | 0 | 0 | 120 | 120 | 1262 | 960 | 693 | 3645 | 6560 | 2 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 0 | 0 | 0 | 0 | 30 | 0 | 30 | 60 | 1680 | 0 | 1740 | 30 | 0 | 30 | 60 | 0 | 339 | 99 | 6900 | 7338 | 2 |
| 170 | Healthy | 2 | Hungary | Male | 70 | 540 | 350 | 210 | 1100 | 280 | 60 | 340 | 80 | 40 | 150 | 270 | 75 | 105 | 0 | 180 | 4862 | 667 | 1284 | 1225 | 8038 | 2 |
| 212 | Healthy | 1 | Hungary | Male | 72 | 0 | 0 | 0 | 0 | 360 | 360 | 720 | 180 | 180 | 0 | 360 | 300 | 240 | 240 | 780 | 0 | 3870 | 3348 | 1260 | 8478 | 0 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 180 | 0 | 0 | 180 | 630 | 0 | 630 | 0 | 360 | 0 | 360 | 630 | 630 | 0 | 1260 | 594 | 4599 | 2079 | 1440 | 8712 | 2 |
| 212 | Healthy | 2 | Hungary | Male | 72 | 0 | 0 | 0 | 0 | 375 | 720 | 1095 | 0 | 60 | 0 | 60 | 120 | 0 | 450 | 570 | 0 | 3996 | 5557 | 240 | 9793 | 0 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 210 | 420 | 300 | 930 | 350 | 200 | 550 | 140 | 140 | 300 | 580 | 100 | 0 | 0 | 100 | 4773 | 330 | 2355 | 2630 | 10,088 | 2 |
| 790 | Healthy | 3 | Spain | Male | 66 | 0 | 0 | 0 | 0 | 840 | 0 | 840 | 630 | 0 | 0 | 630 | 630 | 840 | 0 | 1470 | 0 | 5439 | 2772 | 1890 | 10,101 | 0 |
| 636 | Healthy | 2 | Spain | Male | 68 | 240 | 40 | 180 | 460 | 840 | 0 | 840 | 360 | 1440 | 60 | 1860 | 280 | 0 | 0 | 280 | 2392 | 924 | 2772 | 7170 | 13,258 | 2 |
| 634 | Diseased | 2 | Spain | Male | 72 | 840 | 840 | 105 | 1785 | 840 | 450 | 1290 | 120 | 180 | 30 | 330 | 315 | 225 | 15 | 555 | 6972 | 2059 | 5472 | 1245 | 15,748 | 2 |
| 641 | Diseased | 2 | Spain | Female | 71 | 2940 | 0 | 0 | 2940 | 280 | 0 | 280 | 840 | 840 | 0 | 1680 | 280 | 240 | 0 | 520 | 9702 | 1884 | 924 | 5880 | 18,390 | 2 |
| 133 | Healthy | 2 | Hungary | Female | 71 | 630 | 840 | 450 | 1920 | 630 | 240 | 870 | 420 | 420 | 240 | 1080 | 420 | 240 | 0 | 660 | 9039 | 2346 | 3519 | 4260 | 19,164 | 2 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 540 | 1050 | 520 | 2110 | 840 | 0 | 840 | 420 | 360 | 171 | 951 | 420 | 150 | 90 | 660 | 10,142 | 2706 | 2772 | 3642 | 19,262 | 2 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 420 | 420 | 840 | 1680 | 120 | 120 | 240 | 1260 | 1260 | 360 | 2880 | 0 | 0 | 0 | 0 | 9786 | 0 | 1116 | 10,800 | 21,702 | 2 |
| 569 | Healthy | 2 | Hungary | Female | 67 | 630 | 360 | 0 | 990 | 770 | 0 | 770 | 490 | 770 | 550 | 1810 | 910 | 550 | 550 | 2010 | 3519 | 9603 | 2541 | 7575 | 23,238 | 2 |
| 643 | Healthy | 2 | Spain | Female | 67 | 0 | 0 | 0 | 0 | 840 | 0 | 840 | 1470 | 1470 | 0 | 2940 | 1470 | 1470 | 0 | 2940 | 0 | 10,731 | 2772 | 10,290 | 23,793 | 0 |
| Median: Healthy | 0.0 | 0.0 | 0.0 | 0.0 | 315.0 | 0.0 | 350.0 | 210.0 | 160.0 | 0.0 | 495.5 | 300.0 | 0.0 | 0.0 | 337.5 | 0.0 | 1113.5 | 1236.0 | 1680.0 | 7299.0 | 0.0 | |||||
| Median: Diseased | 420.0 | 0.0 | 0.0 | 1680.0 | 210.0 | 0.0 | 240.0 | 420.0 | 840.0 | 0.0 | 1680.0 | 30.0 | 0.0 | 0.0 | 60.0 | 6972.0 | 339.0 | 924.0 | 5880.0 | 15,748.0 | 2.0 | |||||
| Median: Spain | 0.0 | 0.0 | 0.0 | 0.0 | 276.5 | 0.0 | 276.5 | 390.0 | 210.0 | 0.0 | 600.0 | 307.5 | 0.0 | 0.0 | 337.5 | 0.0 | 1113.5 | 912.0 | 2092.5 | 6431.5 | 0.0 | |||||
| Median: Hungary | 20.0 | 0.0 | 0.0 | 180.0 | 350.0 | 0.0 | 360.0 | 80.0 | 140.0 | 0.0 | 360.0 | 100.0 | 0.0 | 0.0 | 180.0 | 594.0 | 667.0 | 1284.0 | 1455.0 | 8478.0 | 2.0 | |||||
| Median: Female | 0.0 | 0.0 | 0.0 | 0.0 | 276.5 | 0.0 | 276.5 | 420.0 | 390.0 | 0.0 | 1015.5 | 307.5 | 0.0 | 0.0 | 337.5 | 0.0 | 1113.5 | 924.0 | 3951.0 | 6820.5 | 0.0 | |||||
| Median: Male | 20.0 | 0.0 | 0.0 | 180.0 | 350.0 | 0.0 | 550.0 | 120.0 | 140.0 | 30.0 | 360.0 | 120.0 | 0.0 | 0.0 | 280.0 | 594.0 | 960.0 | 2079.0 | 1440.0 | 8478.0 | 1.0 | |||||
| Median: All | 0.0 | 0.0 | 0.0 | 0.0 | 280.0 | 0.0 | 280.0 | 210.0 | 180.0 | 0.0 | 570.0 | 280.0 | 0.0 | 0.0 | 315.0 | 0.0 | 1039.0 | 1116.0 | 1890.0 | 8038.0 | 0.0 | |||||
| Mean: Healthy | 142.2 | 158.6 | 81.5 | 382.5 | 394.0 | 71.8 | 465.8 | 317.5 | 323.0 | 94.1 | 734.6 | 350.9 | 201.5 | 65.9 | 618.4 | 1756.7 | 2491.5 | 1731.0 | 2762.3 | 8741.7 | 0.7 | |||||
| Mean: Diseased | 840.0 | 252.0 | 189.0 | 1281.0 | 296.0 | 114.0 | 410.0 | 540.0 | 792.0 | 78.0 | 1410.0 | 125.0 | 93.0 | 9.0 | 227.0 | 5292.0 | 856.4 | 1660.8 | 5217.0 | 13,026.2 | 1.6 | |||||
| Mean: Spain | 346.6 | 79.1 | 29.1 | 455.0 | 431.0 | 37.5 | 468.5 | 463.7 | 472.5 | 45.0 | 981.3 | 401.6 | 248.7 | 11.2 | 661.6 | 1694.0 | 2410.4 | 1647.5 | 3529.0 | 9281.0 | 0.6 | |||||
| Mean: Hungary | 211.3 | 253.3 | 159.3 | 624.0 | 331.6 | 113.3 | 445.0 | 274.6 | 359.6 | 128.0 | 762.4 | 235.0 | 127.6 | 90.6 | 453.3 | 2985.4 | 2011.4 | 1774.4 | 2967.1 | 9738.4 | 1.1 | |||||
| Mean: Female | 368.5 | 190.7 | 129.2 | 688.5 | 349.5 | 25.7 | 375.2 | 525.7 | 565.7 | 94.3 | 1185.8 | 368.9 | 189.2 | 47.8 | 606.0 | 3013.4 | 2357.4 | 1307.5 | 4359.3 | 11,037.8 | 0.8 | |||||
| Mean: Male | 166.9 | 160.0 | 71.5 | 398.4 | 404.2 | 137.6 | 541.9 | 178.8 | 241.9 | 87.6 | 508.4 | 244.6 | 173.0 | 63.4 | 481.1 | 1763.1 | 2007.1 | 2160.0 | 1986.5 | 7916.9 | 1.0 | |||||
| Mean: All | 271.4 | 175.9 | 101.4 | 548.8 | 375.8 | 79.6 | 455.4 | 358.7 | 409.8 | 91.1 | 859.7 | 309.0 | 181.4 | 55.3 | 545.9 | 2411.4 | 2188.7 | 1718.0 | 3216.8 | 9535.1 | 0.9 | |||||
| SD: Healthy | 222.1 | 287.5 | 151.0 | 621.4 | 279.3 | 169.9 | 329.1 | 340.9 | 426.9 | 142.3 | 698.2 | 339.5 | 360.8 | 149.1 | 712.8 | 2918.6 | 2874.2 | 1384.6 | 2603.3 | 6816.5 | 0.9 | |||||
| SD: Diseased | 1095.2 | 336.0 | 328.0 | 1135.5 | 284.7 | 174.3 | 448.2 | 453.7 | 634.2 | 141.4 | 947.5 | 141.7 | 114.0 | 12.0 | 254.7 | 4437.9 | 920.5 | 1936.0 | 3629.7 | 7299.5 | 0.8 | |||||
| SD: Spain | 815.6 | 230.3 | 55.8 | 895.9 | 291.5 | 124.3 | 362.0 | 363.3 | 521.7 | 87.8 | 773.2 | 370.9 | 435.5 | 33.0 | 780.1 | 3103.9 | 2846.0 | 1445.5 | 2806.5 | 6752.6 | 0.9 | |||||
| SD: Hungary | 253.0 | 324.5 | 249.8 | 748.7 | 267.8 | 195.0 | 348.6 | 362.0 | 487.6 | 164.9 | 799.1 | 259.3 | 200.6 | 172.8 | 549.7 | 3742.2 | 2564.1 | 1543.9 | 3086.5 | 7370.5 | 0.9 | |||||
| SD: Female | 756.0 | 338.5 | 259.7 | 998.0 | 285.3 | 66.9 | 302.6 | 427.4 | 563.6 | 167.8 | 902.9 | 380.1 | 387.2 | 141.2 | 810.3 | 4307.0 | 3290.5 | 1077.2 | 3401.1 | 8806.6 | 0.9 | |||||
| SD: Male | 246.3 | 249.2 | 96.1 | 534.8 | 277.5 | 223.1 | 385.3 | 179.7 | 368.3 | 108.1 | 444.1 | 234.8 | 259.6 | 130.7 | 466.3 | 2262.5 | 1849.5 | 1749.5 | 1745.9 | 4038.2 | 0.9 | |||||
| SD: All | 579.4 | 299.3 | 200.6 | 821.7 | 282.9 | 171.5 | 354.8 | 374.6 | 506.1 | 142.2 | 795.1 | 324.5 | 332.0 | 136.5 | 670.1 | 3531.8 | 2700.3 | 1502.3 | 2978.4 | 7106.2 | 0.9 | |||||

Social Support (MSPSS)
| ID | Health | Wave | Country | Gender | Age | Q1: Special Person: Around When in Need | Q2: Special Person: Share Joys and Sorrows | Q3: Family: Tries to Help | Q4: Family: Gives Emotional Help and Support | Q5: Special Person: Real Source of Comfort | Q6: Friends: Try to Help | Q7: Friends: counted on when things go wrong | Q8: Family: Talk About Problems | Q9: Friends: Share My Joys and Sorrows | Q10: Special Person: Cares about Feelings | Q11: Family: Willing to Help Make Decisions | Q12: Friends: talk about problems | Significant Other Numeric Sub-Score | Family Numeric Sub-Score | Friends Numeric Sub-Score | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 700 | Healthy | 2 | Spain | Male | 67 | 5 | 5 | 4 | 2 | 2 | 3 | 4 | 2 | 6 | 4 | 4 | 5 | 4 | 3 | 4 | 3 | 1 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 6 | 6 | 5 | 5 | 5 | 4 | 4 | 5 | 4 | 5 | 4 | 5 | 5 | 4 | 4 | 4 | 1 |
| 212 | Healthy | 2 | Hungary | Male | 72 | 3 | 5 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 4 | 5 | 5 | 4 | 1 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 5 | 6 | 5 | 6 | 6 | 4 | 4 | 5 | 1 | 6 | 6 | 1 | 5 | 5 | 2 | 4 | 1 |
| 800 | Diseased | 3 | Spain | Female | 65 | 5 | 6 | 5 | 4 | 5 | 4 | 5 | 4 | 5 | 6 | 4 | 5 | 5 | 4 | 4 | 4 | 1 |
| 617 | Healthy | 1 | Spain | Female | 69 | 5 | 2 | 5 | 4 | 4 | 5 | 5 | 3 | 4 | 5 | 3 | 5 | 4 | 3 | 4 | 4 | 1 |
| 617 | Healthy | 2 | Spain | Female | 69 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 5 | 4 | 5 | 5 | 4 | 4 | 4 | 4 | 1 |
| 796 | Healthy | 3 | Spain | Male | 74 | 4 | 4 | 4 | 4 | 4 | 6 | 6 | 4 | 6 | 4 | 4 | 6 | 4 | 4 | 6 | 4 | 1 |
| 799 | Diseased | 3 | Spain | Male | 79 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 1 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 5 | 6 | 7 | 7 | 3 | 5 | 5 | 6 | 6 | 5 | 3 | 5 | 4 | 5 | 5 | 5 | 1 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 6 | 7 | 5 | 3 | 6 | 7 | 7 | 3 | 7 | 6 | 5 | 7 | 6 | 4 | 7 | 5 | 1 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 5 | 5 | 6 | 5 | 5 | 6 | 7 | 5 | 7 | 6 | 6 | 7 | 5 | 5 | 6 | 5 | 1 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 6 | 7 | 5 | 5 | 4 | 7 | 7 | 3 | 7 | 6 | 4 | 7 | 5 | 4 | 7 | 5 | 1 |
| 420 | Healthy | 1 | Hungary | Female | 71 | 6 | 6 | 6 | 5 | 6 | 1 | 5 | 5 | 5 | 6 | 4 | 5 | 6 | 5 | 4 | 5 | 1 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 6 | 6 | 6 | 6 | 5 | 5 | 5 | 5 | 5 | 6 | 6 | 5 | 5 | 5 | 5 | 5 | 1 |
| 576 | Healthy | 2 | Hungary | Male | 60 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 1 |
| 170 | Healthy | 2 | Hungary | Male | 70 | 5 | 5 | 6 | 5 | 5 | 6 | 6 | 5 | 7 | 5 | 7 | 7 | 5 | 5 | 6 | 5 | 1 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 5 | 5 | 6 | 4 | 6 | 6 | 6 | 5 | 6 | 5 | 5 | 6 | 5 | 5 | 6 | 5 | 1 |
| 212 | Healthy | 1 | Hungary | Male | 72 | 6 | 6 | 5 | 6 | 5 | 5 | 5 | 6 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 5 | 1 |
| 212 | Healthy | 3 | Hungary | Male | 72 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 1 |
| 419 | Healthy | 1 | Hungary | Male | 95 | 6 | 6 | 5 | 5 | 6 | 5 | 5 | 5 | 5 | 6 | 5 | 5 | 6 | 5 | 5 | 5 | 1 |
| 640 | Healthy | 1 | Spain | Female | 69 | 1 | 6 | 5 | 5 | 6 | 5 | 6 | 6 | 6 | 6 | 6 | 6 | 4 | 5 | 5 | 5 | 1 |
| 641 | Diseased | 1 | Spain | Female | 71 | 3 | 6 | 6 | 5 | 6 | 6 | 6 | 5 | 6 | 3 | 6 | 6 | 4 | 5 | 6 | 5 | 1 |
| 630 | Healthy | 1 | Spain | Female | 74 | 4 | 6 | 5 | 3 | 5 | 6 | 6 | 6 | 6 | 6 | 4 | 6 | 5 | 4 | 6 | 5 | 1 |
| 411 | Healthy | 1 | Spain | Male | 45 | 1 | 7 | 6 | 6 | 6 | 5 | 6 | 6 | 6 | 7 | 6 | 7 | 5 | 6 | 6 | 5 | 1 |
| 636 | Healthy | 1 | Spain | Male | 68 | 7 | 5 | 6 | 6 | 7 | 5 | 5 | 6 | 5 | 7 | 5 | 5 | 6 | 5 | 5 | 5 | 1 |
| 636 | Healthy | 2 | Spain | Male | 68 | 5 | 7 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 5 | 1 |
| 793 | Healthy | 3 | Spain | Male | 68 | 6 | 6 | 6 | 6 | 6 | 5 | 5 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 5 | 5 | 1 |
| 625 | Diseased | 1 | Spain | Male | 72 | 7 | 7 | 7 | 7 | 7 | 5 | 2 | 7 | 3 | 7 | 7 | 5 | 7 | 7 | 3 | 5 | 1 |
| 634 | Diseased | 1 | Spain | Male | 72 | 3 | 6 | 6 | 6 | 5 | 5 | 5 | 6 | 5 | 6 | 7 | 5 | 5 | 6 | 5 | 5 | 1 |
| 634 | Diseased | 2 | Spain | Male | 72 | 6 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 1 |
| 569 | Healthy | 2 | Hungary | Female | 67 | 6 | 7 | 7 | 7 | 7 | 5 | 5 | 7 | 5 | 7 | 7 | 5 | 6 | 7 | 5 | 6 | 2 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 7 | 6 | 6 | 7 | 6 | 6 | 6 | 2 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 7 | 6 | 7 | 7 | 6 | 6 | 6 | 2 |
| 133 | Healthy | 2 | Hungary | Female | 71 | 7 | 7 | 7 | 6 | 7 | 6 | 7 | 7 | 6 | 7 | 7 | 7 | 7 | 6 | 6 | 6 | 2 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 6 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 7 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 6 | 7 | 6 | 6 | 7 | 6 | 6 | 2 |
| 132 | Diseased | 1 | Hungary | Male | 71 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 6 | 5 | 7 | 6 | 5 | 7 | 6 | 5 | 6 | 2 |
| 132 | Diseased | 2 | Hungary | Male | 71 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 6 | 5 | 7 | 7 | 5 | 7 | 6 | 5 | 6 | 2 |
| 643 | Healthy | 2 | Spain | Female | 67 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 798 | Healthy | 3 | Spain | Female | 67 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 620 | Healthy | 2 | Spain | Female | 69 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 638 | Healthy | 1 | Spain | Female | 71 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 638 | Healthy | 2 | Spain | Female | 71 | 6 | 6 | 7 | 6 | 6 | 5 | 5 | 7 | 6 | 7 | 6 | 6 | 6 | 6 | 5 | 6 | 2 |
| 641 | Diseased | 2 | Spain | Female | 71 | 5 | 6 | 7 | 7 | 6 | 6 | 6 | 6 | 6 | 4 | 7 | 6 | 5 | 6 | 6 | 6 | 2 |
| 624 | Diseased | 1 | Spain | Female | 72 | 7 | 6 | 7 | 7 | 7 | 6 | 7 | 7 | 7 | 7 | 7 | 7 | 6 | 7 | 6 | 6 | 2 |
| 648 | Healthy | 1 | Spain | Female | 72 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 2 |
| 795 | Healthy | 3 | Spain | Female | 72 | 6 | 6 | 7 | 7 | 6 | 7 | 7 | 7 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 6 | 2 |
| 790 | Healthy | 3 | Spain | Male | 66 | 7 | 6 | 7 | 7 | 7 | 6 | 6 | 7 | 6 | 5 | 7 | 6 | 6 | 7 | 6 | 6 | 2 |
| 569 | Healthy | 1 | Hungary | Female | 67 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| 643 | Healthy | 1 | Spain | Female | 67 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| 628 | Healthy | 1 | Spain | Female | 70 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| 644 | Diseased | 1 | Spain | Male | 70 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| 791 | Diseased | 3 | Spain | Male | 72 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 2 |
| Median: Healthy | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 6.0 | 5.0 | 1.0 | |||||
| Median: Diseased | 6.0 | 6.5 | 6.5 | 6.5 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.5 | 6.0 | 5.5 | 6.0 | 6.0 | 5.0 | 1.0 | |||||
| Median: Spain | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 1.0 | |||||
| Median: Hungary | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 6.0 | 6.0 | 6.0 | 5.0 | 6.0 | 5.0 | 5.0 | 5.0 | 1.0 | |||||
| Median: Female | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 2.0 | |||||
| Median: Male | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 5.0 | 6.0 | 5.0 | 6.0 | 6.0 | 5.0 | 5.0 | 5.0 | 5.0 | 5.0 | 1.0 | |||||
| Median: All | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 6.0 | 5.0 | 1.0 | |||||
| Mean: Healthy | 5.5 | 5.9 | 5.9 | 5.7 | 5.7 | 5.3 | 5.5 | 5.7 | 5.6 | 5.9 | 5.5 | 5.6 | 5.5 | 5.4 | 5.3 | 5.3 | 1.4 | |||||
| Mean: Diseased | 5.7 | 6.2 | 6.1 | 5.8 | 5.9 | 5.8 | 5.8 | 5.5 | 5.8 | 5.9 | 6.0 | 5.9 | 5.7 | 5.6 | 5.6 | 5.5 | 1.4 | |||||
| Mean: Spain | 5.3 | 5.8 | 5.9 | 5.6 | 5.7 | 5.5 | 5.6 | 5.7 | 5.7 | 5.8 | 5.7 | 5.8 | 5.4 | 5.5 | 5.4 | 5.3 | 1.4 | |||||
| Mean: Hungary | 5.9 | 6.2 | 6.0 | 5.8 | 5.8 | 5.4 | 5.7 | 5.6 | 5.5 | 6.0 | 5.6 | 5.6 | 5.7 | 5.4 | 5.4 | 5.3 | 1.4 | |||||
| Mean: Female | 5.7 | 6.1 | 6.1 | 5.8 | 5.8 | 5.6 | 5.9 | 5.8 | 5.9 | 6.0 | 5.6 | 6.0 | 5.6 | 5.5 | 5.6 | 5.5 | 1.5 | |||||
| Mean: Male | 5.4 | 5.8 | 5.8 | 5.7 | 5.7 | 5.3 | 5.3 | 5.5 | 5.3 | 5.8 | 5.7 | 5.4 | 5.5 | 5.5 | 5.2 | 5.1 | 1.2 | |||||
| Mean: All | 5.6 | 6.0 | 6.0 | 5.7 | 5.8 | 5.5 | 5.6 | 5.6 | 5.6 | 5.9 | 5.7 | 5.7 | 5.5 | 5.5 | 5.4 | 5.3 | 1.4 | |||||
| SD: Healthy | 1.4 | 1.0 | 0.9 | 1.2 | 1.1 | 1.1 | 0.8 | 1.1 | 1.0 | 0.9 | 1.1 | 1.0 | 0.9 | 1.0 | 0.9 | 0.9 | 0.4 | |||||
| SD: Diseased | 1.3 | 0.9 | 0.9 | 1.3 | 1.0 | 0.9 | 1.3 | 1.3 | 1.2 | 1.2 | 1.1 | 1.0 | 1.0 | 1.1 | 1.2 | 0.9 | 0.4 | |||||
| SD: Spain | 1.6 | 1.1 | 1.0 | 1.3 | 1.2 | 0.9 | 1.1 | 1.3 | 0.9 | 1.1 | 1.1 | 0.7 | 1.0 | 1.2 | 1.0 | 1.0 | 0.4 | |||||
| SD: Hungary | 0.9 | 0.8 | 0.8 | 1.1 | 1.1 | 1.2 | 0.9 | 1.1 | 1.2 | 0.7 | 1.1 | 1.2 | 0.9 | 0.8 | 1.0 | 0.7 | 0.4 | |||||
| SD: Female | 1.3 | 1.0 | 0.8 | 1.2 | 1.0 | 1.2 | 0.8 | 1.3 | 0.8 | 1.0 | 1.2 | 0.7 | 0.9 | 1.1 | 0.9 | 0.8 | 0.4 | |||||
| SD: Male | 1.5 | 0.9 | 1.0 | 1.2 | 1.2 | 0.9 | 1.0 | 1.1 | 1.2 | 1.0 | 1.0 | 1.2 | 1.0 | 1.0 | 1.1 | 0.9 | 0.4 | |||||
| SD: All | 1.4 | 1.0 | 0.9 | 1.2 | 1.1 | 1.1 | 1.0 | 1.2 | 1.1 | 1.0 | 1.1 | 1.0 | 1.0 | 1.0 | 1.0 | 0.9 | 0.4 | |||||

Anxiety and Depression (GADS)
| ID | Health | Wave | Country | Gender | Age | Q1A: Keyed-up or on Edge | Q2A: Worrying a Lot | Q3A: Irritable | Q4A: Difficulty Relaxing | Q5A: Sleeping Poorly | Q6A: Headaches or Neck Aches | Q7A: Trembling [...] Urine | Q8A: Worried about Your Health | Q9A: Difficulty Falling Asleep | Q1D: Lacking Energy | Q2D: Lost Interest in Things | Q3D: Lost Confidence in Yourself | Q4D: Hopeless | Q5D: Difficulty Concentrating | Q6D: Lost Weight Due to Poor Appetite | Q7D: Waking Early | Q8D: Slowed Down | Q9D: Worse in the Mornings | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 800 | Diseased | 3 | Spain | Female | 65 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 643 | Healthy | 1 | Spain | Female | 67 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 0 |
| 796 | Healthy | 3 | Spain | Male | 74 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 0 |
| 628 | Healthy | 1 | Spain | Female | 70 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 3 | 0 |
| 790 | Healthy | 3 | Spain | Male | 66 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 0 |
| 799 | Diseased | 3 | Spain | Male | 79 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 |
| 648 | Healthy | 1 | Spain | Female | 72 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 5 | 0 |
| 643 | Healthy | 2 | Spain | Female | 67 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 7 | 0 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 8 | 0 |
| 638 | Healthy | 1 | Spain | Female | 71 | 0 | 1 | 2 | 2 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 10 | 1 |
| 700 | Healthy | 2 | Spain | Male | 67 | 2 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 10 | 1 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 11 | 1 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 1 | 1 | 1 | 0 | 2 | 2 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 13 | 1 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 2 | 1 | 13 | 1 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 0 | 0 | 1 | 0 | 0 | 4 | 4 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 13 | 1 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 1 | 1 | 0 | 0 | 1 | 3 | 0 | 0 | 1 | 0 | 1 | 2 | 0 | 1 | 1 | 0 | 4 | 0 | 16 | 1 |
| 132 | Diseased | 1 | Hungary | Male | 71 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 16 | 1 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 0 | 1 | 1 | 2 | 0 | 0 | 1 | 1 | 2 | 2 | 0 | 17 | 1 |
| 795 | Healthy | 3 | Spain | Female | 72 | 1 | 1 | 0 | 1 | 2 | 0 | 0 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 4 | 1 | 1 | 0 | 17 | 1 |
| 569 | Healthy | 1 | Hungary | Female | 67 | 1 | 1 | 0 | 2 | 4 | 2 | 1 | 0 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 19 | 1 |
| 624 | Diseased | 1 | Spain | Female | 72 | 1 | 4 | 3 | 0 | 2 | 0 | 0 | 0 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 4 | 3 | 0 | 21 | 1 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 3 | 2 | 0 | 22 | 2 |
| 641 | Diseased | 2 | Spain | Female | 71 | 2 | 4 | 3 | 2 | 1 | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 1 | 0 | 4 | 1 | 1 | 23 | 2 |
| 640 | Healthy | 1 | Spain | Female | 69 | 1 | 1 | 1 | 1 | 1 | 4 | 2 | 3 | 2 | 3 | 0 | 0 | 0 | 4 | 0 | 1 | 2 | 0 | 26 | 2 |
| 620 | Healthy | 2 | Spain | Female | 69 | 2 | 2 | 2 | 1 | 3 | 4 | 0 | 2 | 2 | 1 | 2 | 0 | 0 | 1 | 0 | 3 | 4 | 0 | 29 | 2 |
| 630 | Healthy | 1 | Spain | Female | 74 | 4 | 3 | 2 | 2 | 2 | 2 | 0 | 3 | 1 | 3 | 0 | 0 | 0 | 1 | 2 | 4 | 2 | 0 | 31 | 2 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 1 | 2 | 1 | 2 | 4 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 3 | 2 | 33 | 2 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 4 | 1 | 4 | 3 | 4 | 0 | 1 | 1 | 4 | 4 | 4 | 5 | 1 | 1 | 1 | 4 | 4 | 1 | 47 | 3 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 4 | 3 | 3 | 3 | 5 | 0 | 1 | 4 | 5 | 2 | 4 | 3 | 1 | 1 | 1 | 4 | 4 | 3 | 51 | 3 |
| 641 | Diseased | 1 | Spain | Female | 71 | 4 | 4 | 4 | 4 | 4 | 2 | 4 | 4 | 1 | 3 | 3 | 1 | 1 | 1 | 2 | 3 | 2 | 4 | 51 | 3 |
| 625 | Diseased | 1 | Spain | Male | 72 | 4 | 4 | 0 | 0 | 4 | 1 | 3 | 4 | 4 | 2 | 4 | 1 | 2 | 2 | 4 | 5 | 4 | 3 | 51 | 3 |
| 617 | Healthy | 2 | Spain | Female | 69 | 3 | 3 | 4 | 4 | 4 | 4 | 4 | 3 | 4 | 5 | 4 | 4 | 5 | 2 | 0 | 4 | 3 | 1 | 61 | 4 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 4 | 1 | 4 | 4 | 5 | 4 | 3 | 3 | 5 | 4 | 4 | 5 | 4 | 3 | 2 | 5 | 5 | 3 | 68 | 4 |
| Median: Healthy | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 1.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 13.0 | 1.0 | |||||
| Median: Diseased | 2.0 | 1.0 | 3.0 | 1.0 | 2.0 | 1.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 1.0 | 0.0 | 1.0 | 1.0 | 4.0 | 2.0 | 1.0 | 23.0 | 2.0 | |||||
| Median: Spain | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 10.0 | 1.0 | |||||
| Median: Hungary | 1.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 16.0 | 1.0 | |||||
| Median: Female | 1.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 0.0 | 0.5 | 1.0 | 1.0 | 1.0 | 0.0 | 0.0 | 1.0 | 0.0 | 1.5 | 1.5 | 0.0 | 18.0 | 1.0 | |||||
| Median: Male | 1.0 | 0.5 | 0.5 | 0.0 | 0.5 | 1.0 | 0.5 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 11.5 | 1.0 | |||||
| Median: All | 1.0 | 1.0 | 1.0 | 0.5 | 1.0 | 1.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.5 | 0.0 | 16.0 | 1.0 | |||||
| Mean: Healthy | 1.0 | 1.0 | 0.9 | 0.8 | 1.3 | 1.4 | 0.7 | 0.6 | 1.0 | 1.0 | 0.8 | 0.4 | 0.3 | 0.5 | 0.5 | 1.3 | 1.2 | 0.2 | 15.6 | 1.0 | |||||
| Mean: Diseased | 2.2 | 2.0 | 2.0 | 1.5 | 2.4 | 1.0 | 1.2 | 1.6 | 2.0 | 2.1 | 1.9 | 1.5 | 0.8 | 0.9 | 1.0 | 2.8 | 2.4 | 1.5 | 31.4 | 1.9 | |||||
| Mean: Spain | 1.4 | 1.6 | 1.2 | 0.9 | 1.3 | 1.1 | 0.7 | 1.1 | 1.1 | 1.4 | 0.8 | 0.3 | 0.4 | 0.6 | 0.6 | 1.8 | 1.2 | 0.4 | 18.7 | 1.1 | |||||
| Mean: Hungary | 1.4 | 0.9 | 1.3 | 1.2 | 2.2 | 1.6 | 1.0 | 0.8 | 1.7 | 1.2 | 1.5 | 1.4 | 0.5 | 0.7 | 0.6 | 1.6 | 2.1 | 0.9 | 23.3 | 1.4 | |||||
| Mean: Female | 1.6 | 1.5 | 1.5 | 1.3 | 2.0 | 1.5 | 0.8 | 1.1 | 1.6 | 1.5 | 1.2 | 0.9 | 0.5 | 0.7 | 0.7 | 2.0 | 1.8 | 0.7 | 23.7 | 1.4 | |||||
| Mean: Male | 1.0 | 0.9 | 0.5 | 0.3 | 1.0 | 0.9 | 1.0 | 0.7 | 0.7 | 0.9 | 1.0 | 0.5 | 0.3 | 0.4 | 0.6 | 1.3 | 1.2 | 0.5 | 13.7 | 0.9 | |||||
| Mean: All | 1.4 | 1.3 | 1.2 | 1.0 | 1.7 | 1.3 | 0.9 | 1.0 | 1.3 | 1.3 | 1.1 | 0.8 | 0.4 | 0.6 | 0.6 | 1.7 | 1.6 | 0.6 | 20.7 | 1.2 | |||||
| SD: Healthy | 0.9 | 0.9 | 0.9 | 1.0 | 1.3 | 1.4 | 1.1 | 1.0 | 1.2 | 1.2 | 1.0 | 1.0 | 1.0 | 0.9 | 0.9 | 1.2 | 1.2 | 0.5 | 13.4 | 0.9 | |||||
| SD: Diseased | 1.6 | 1.6 | 1.7 | 1.6 | 1.8 | 1.2 | 1.3 | 1.6 | 2.0 | 1.1 | 1.7 | 1.8 | 1.1 | 0.8 | 1.2 | 1.8 | 1.6 | 1.3 | 21.6 | 1.3 | |||||
| SD: Spain | 1.4 | 1.4 | 1.3 | 1.2 | 1.4 | 1.4 | 1.3 | 1.4 | 1.2 | 1.4 | 1.3 | 0.9 | 1.1 | 1.0 | 1.2 | 1.6 | 1.3 | 1.0 | 18.1 | 1.2 | |||||
| SD: Hungary | 1.3 | 0.8 | 1.2 | 1.3 | 1.6 | 1.2 | 1.1 | 1.1 | 1.8 | 1.2 | 1.3 | 1.6 | 1.0 | 0.7 | 0.5 | 1.5 | 1.5 | 0.9 | 17.7 | 1.0 | |||||
| SD: Female | 1.4 | 1.2 | 1.4 | 1.4 | 1.6 | 1.4 | 1.2 | 1.3 | 1.5 | 1.4 | 1.4 | 1.6 | 1.2 | 0.9 | 0.9 | 1.6 | 1.5 | 1.1 | 18.8 | 1.2 | |||||
| SD: Male | 1.1 | 1.2 | 0.5 | 0.4 | 1.2 | 1.1 | 1.3 | 1.1 | 1.2 | 0.9 | 1.1 | 0.6 | 0.6 | 0.6 | 1.2 | 1.4 | 1.3 | 0.9 | 13.9 | 0.9 | |||||
| SD: All | 1.3 | 1.3 | 1.3 | 1.3 | 1.6 | 1.3 | 1.2 | 1.3 | 1.5 | 1.3 | 1.4 | 1.4 | 1.1 | 0.9 | 1.0 | 1.6 | 1.5 | 1.0 | 18.1 | 1.1 | |||||

Mediterranean Nutrition (PREDIMED)

| ID | Health | Wave | Country | Gender | Age | Q1: Olive Oil Main Culinary Fat | Q2: Olive Oil Use | Q3: Vegetables Use | Q4: Fruits Use | Q5: Red Meat, Hamburger, or Meat Use | Q6: Butter, Margarine, or Cream Use | Q7: Sweet/Carbonated Beverage Use | Q8: Wine Use | Q9: Legumes Use | Q10: Fish or Shellfish Use | Q11: Commercial Sweets or Pastries | Q12: Nuts Use | Q13: Preference to Small Animal Meat | Q14: Sofrito Use | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 420 | Healthy | 2 | Hungary | Female | 71 | 0 | 1.0 | 1.0 | 2.0 | 1.0 | 2.0 | 0.0 | 0.0 | 1.0 | 0.0 | 2.0 | 0.0 | 1.0 | 1.0 | 2 | 0 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 0 | 0.0 | 1.0 | 2.0 | 1.0 | 2.0 | 0.0 | 0.0 | 1.0 | 0.0 | 2.0 | 3.0 | 0.0 | 2.0 | 3 | 0 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 0 | 1.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 5.0 | 1.0 | 1.0 | 5.0 | 3.0 | 1.0 | 3.0 | 3 | 0 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 0 | 0.0 | 2.1 | 1.1 | 1.0 | 2.0 | 0.0 | 1.0 | 2.1 | 1.0 | 2.0 | 1.2 | 1.0 | 2.0 | 4 | 0 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 0 | 0.0 | 2.0 | 1.0 | 2.0 | 1.0 | 0.0 | 3.0 | 1.0 | 1.0 | 4.0 | 3.0 | 1.0 | 4.0 | 5 | 0 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 0 | 0.0 | 1.0 | 2.0 | 0.3 | 1.0 | 0.0 | 2.0 | 0.5 | 0.5 | 1.0 | 0.3 | 1.0 | 4.0 | 5 | 0 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 1 | 4.0 | 2.0 | 2.0 | 1.0 | 4.0 | 0.0 | 1.0 | 1.0 | 0.0 | 2.0 | 2.0 | 1.0 | 2.0 | 6 | 0 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 1 | 1.0 | 2.0 | 2.0 | 1.0 | 2.0 | 0.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 1.0 | 2.0 | 6 | 0 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 1 | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 0.0 | 1.0 | 2.0 | 3.0 | 2.0 | 6.0 | 1.0 | 6.0 | 7 | 1 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 1 | 3.0 | 2.0 | 1.0 | 0.2 | 1.0 | 0.0 | 5.0 | 2.0 | 0.2 | 0.0 | 0.0 | 1.0 | 5.0 | 7 | 1 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 1 | 1.0 | 2.0 | 1.0 | 0.3 | 1.0 | 0.0 | 7.0 | 0.5 | 0.2 | 0.0 | 0.5 | 1.0 | 1.0 | 7 | 1 |
| 800 | Diseased | 3 | Spain | Female | 65 | 1 | 1.0 | 1.0 | 3.0 | 0.0 | 0.0 | 0.0 | 3.0 | 1.0 | 2.0 | 4.0 | 7.0 | 1.0 | 0.0 | 7 | 1 |
| 617 | Healthy | 2 | Spain | Female | 69 | 1 | 2.0 | 2.0 | 2.0 | 0.8 | 0.0 | 0.0 | 0.0 | 1.0 | 2.4 | 2.0 | 5.0 | 0.0 | 2.0 | 7 | 1 |
| 795 | Healthy | 3 | Spain | Female | 72 | 1 | 4.0 | 1.0 | 2.0 | 0.5 | 0.0 | 0.0 | 1.0 | 1.0 | 2.0 | 0.0 | 0.7 | 1.0 | 0.0 | 7 | 1 |
| 700 | Healthy | 2 | Spain | Male | 67 | 1 | 2.0 | 1.0 | 2.0 | 0.0 | 0.0 | 0.0 | 6.0 | 4.0 | 2.0 | 0.0 | 2.0 | 1.0 | 3.0 | 8 | 1 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 1 | 2.0 | 2.0 | 5.3 | 0.1 | 0.0 | 0.0 | 3.0 | 2.0 | 1.0 | 3.0 | 3.0 | 1.0 | 3.0 | 9 | 1 |
| 643 | Healthy | 2 | Spain | Female | 67 | 1 | 2.0 | 2.0 | 4.0 | 0.5 | 0.0 | 0.0 | 7.0 | 2.0 | 2.0 | 0.0 | 1.0 | 1.0 | 1.0 | 9 | 1 |
| 641 | Diseased | 2 | Spain | Female | 71 | 1 | 3.0 | 2.0 | 2.0 | 0.0 | 0.0 | 0.0 | 2.0 | 1.0 | 7.0 | 7.0 | 4.0 | 1.0 | 7.0 | 9 | 1 |
| 796 | Healthy | 3 | Spain | Male | 74 | 1 | 3.0 | 2.0 | 3.0 | 0.0 | 0.0 | 0.0 | 1.0 | 2.0 | 2.0 | 0.0 | 2.0 | 1.0 | 3.0 | 9 | 1 |
| 799 | Diseased | 3 | Spain | Male | 79 | 1 | 1.0 | 1.0 | 3.0 | 0.0 | 0.0 | 0.0 | 3.0 | 2.0 | 2.0 | 0.0 | 4.0 | 1.0 | 2.0 | 9 | 1 |
| 620 | Healthy | 2 | Spain | Female | 69 | 1 | 2.0 | 2.0 | 4.0 | 1.0 | 0.0 | 0.0 | 1.0 | 2.0 | 3.0 | 0.0 | 4.0 | 1.0 | 2.0 | 10 | 1 |
| 648 | Healthy | 1 | Spain | Female | 72 | 1 | 2.0 | 2.0 | 3.0 | 0.8 | 0.0 | 0.0 | 2.0 | 6.0 | 3.0 | 7.0 | 5.0 | 1.0 | 5.0 | 11 | 1 |
| 790 | Healthy | 3 | Spain | Male | 66 | 1 | 10.0 | 3.0 | 4.0 | 1.0 | 0.0 | 0.0 | 0.0 | 5.0 | 1.0 | 0.0 | 7.0 | 1.0 | 4.0 | 11 | 1 |
| Median: Healthy | 1.0 | 2.0 | 2.0 | 2.0 | 1.0 | 0.0 | 0.0 | 1.0 | 1.5 | 1.5 | 2.0 | 3.0 | 1.0 | 2.5 | 7.0 | 1.0 | |||||
| Median: Diseased | 1.0 | 1.0 | 2.0 | 2.0 | 0.2 | 1.0 | 0.0 | 3.0 | 1.0 | 1.0 | 1.0 | 1.2 | 1.0 | 2.0 | 7.0 | 1.0 | |||||
| Median: Spain | 1.0 | 2.0 | 2.0 | 3.0 | 0.5 | 0.0 | 0.0 | 2.0 | 2.0 | 2.0 | 0.0 | 4.0 | 1.0 | 2.0 | 9.0 | 1.0 | |||||
| Median: Hungary | 0.5 | 1.0 | 2.0 | 2.0 | 1.0 | 2.0 | 0.0 | 1.5 | 1.0 | 0.3 | 2.0 | 1.6 | 1.0 | 2.5 | 5.5 | 0.0 | |||||
| Median: Female | 1.0 | 2.0 | 2.0 | 2.0 | 0.8 | 1.0 | 0.0 | 2.0 | 1.0 | 2.0 | 2.0 | 3.0 | 1.0 | 2.0 | 7.0 | 1.0 | |||||
| Median: Male | 1.0 | 1.5 | 2.0 | 2.5 | 0.5 | 0.0 | 0.0 | 2.0 | 2.0 | 1.0 | 0.0 | 2.5 | 1.0 | 3.0 | 8.5 | 1.0 | |||||
| Median: All | 1.0 | 2.0 | 2.0 | 2.0 | 0.8 | 0.0 | 0.0 | 2.0 | 1.0 | 1.0 | 2.0 | 3.0 | 1.0 | 2.0 | 7.0 | 1.0 | |||||
| Mean: Healthy | 0.7 | 2.3 | 1.8 | 2.5 | 0.8 | 0.9 | 0.0 | 2.0 | 2.0 | 1.4 | 1.8 | 2.9 | 0.8 | 2.6 | 7.0 | 0.6 | |||||
| Mean: Diseased | 0.7 | 1.2 | 1.5 | 1.8 | 0.2 | 0.7 | 0.0 | 3.2 | 1.3 | 1.8 | 2.0 | 2.4 | 1.0 | 3.0 | 6.8 | 0.7 | |||||
| Mean: Spain | 1.0 | 2.9 | 1.7 | 2.9 | 0.4 | 0.0 | 0.0 | 2.3 | 2.4 | 2.5 | 1.8 | 3.7 | 0.9 | 2.6 | 8.8 | 1.0 | |||||
| Mean: Hungary | 0.5 | 1.2 | 1.7 | 1.8 | 0.9 | 1.6 | 0.0 | 2.4 | 1.2 | 0.6 | 1.9 | 1.8 | 0.9 | 2.9 | 5.3 | 0.3 | |||||
| Mean: Female | 0.7 | 1.8 | 1.7 | 2.2 | 0.7 | 0.9 | 0.0 | 2.3 | 1.5 | 1.7 | 2.2 | 2.7 | 0.8 | 2.8 | 6.8 | 0.6 | |||||
| Mean: Male | 0.7 | 2.5 | 1.7 | 2.6 | 0.5 | 0.7 | 0.1 | 2.5 | 2.3 | 1.2 | 1.2 | 2.7 | 1.0 | 2.7 | 7.3 | 0.6 | |||||
| Mean: All | 0.7 | 2.0 | 1.7 | 2.3 | 0.6 | 0.8 | 0.0 | 2.3 | 1.8 | 1.5 | 1.8 | 2.7 | 0.9 | 2.7 | 7.0 | 0.6 | |||||
| SD: Healthy | 0.4 | 2.2 | 0.6 | 1.1 | 0.5 | 1.1 | 0.2 | 2.1 | 1.5 | 1.0 | 2.0 | 2.0 | 0.3 | 1.4 | 2.7 | 0.4 | |||||
| SD: Diseased | 0.4 | 1.1 | 0.5 | 0.8 | 0.3 | 0.6 | 0.0 | 1.9 | 0.6 | 2.2 | 2.4 | 2.4 | 0.0 | 2.2 | 1.7 | 0.4 | |||||
| SD: Spain | 0.0 | 2.3 | 0.6 | 0.7 | 0.4 | 0.0 | 0.0 | 2.1 | 1.6 | 1.4 | 2.7 | 2.0 | 0.2 | 2.0 | 1.4 | 0.0 | |||||
| SD: Hungary | 0.5 | 1.2 | 0.5 | 1.1 | 0.5 | 0.9 | 0.2 | 2.1 | 0.5 | 0.8 | 1.4 | 1.7 | 0.2 | 1.4 | 1.9 | 0.4 | |||||
| SD: Female | 0.4 | 1.2 | 0.5 | 0.9 | 0.5 | 1.1 | 0.0 | 2.2 | 1.2 | 1.8 | 2.2 | 2.2 | 0.3 | 2.1 | 2.3 | 0.4 | |||||
| SD: Male | 0.4 | 2.9 | 0.6 | 1.3 | 0.4 | 0.9 | 0.3 | 2.0 | 1.3 | 0.6 | 1.7 | 1.9 | 0.0 | 0.6 | 2.5 | 0.4 | |||||
| SD: All | 0.4 | 2.0 | 0.6 | 1.1 | 0.5 | 1.0 | 0.2 | 2.1 | 1.3 | 1.5 | 2.1 | 2.1 | 0.2 | 1.7 | 2.4 | 0.4 | |||||
Nutrition (SelfMNA)
| ID | Health | Wave | Country | Gender | Age | Q1: Food Intake Declined | Q2: Weight Lost | Q3: Described Current Mobility | Q4: Stressed or Severely Ill | Q5: Dementia and/or Severe Sadness | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 795 | Healthy | 3 | Spain | Female | 72 | 1 | 0 | 2 | 2 | 2 | 8 | 1 |
| 620 | Healthy | 2 | Spain | Female | 69 | 1 | 0 | 2 | 2 | 2 | 9 | 1 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 2 | 3 | 1 | 0 | 1 | 10 | 1 |
| 641 | Diseased | 1 | Spain | Female | 71 | 2 | 3 | 2 | 0 | 2 | 10 | 1 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 2 | 0 | 2 | 2 | 2 | 11 | 1 |
| 628 | Healthy | 1 | Spain | Female | 70 | 1 | 3 | 2 | 2 | 2 | 11 | 1 |
| 625 | Diseased | 1 | Spain | Male | 72 | 1 | 2 | 2 | 2 | 2 | 11 | 1 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 2 | 3 | 2 | 0 | 2 | 12 | 2 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 2 | 3 | 2 | 0 | 2 | 12 | 2 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 1 | 2 | 2 | 2 | 2 | 12 | 2 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 2 | 1 | 2 | 2 | 2 | 12 | 2 |
| 638 | Healthy | 1 | Spain | Female | 71 | 2 | 3 | 2 | 2 | 2 | 12 | 2 |
| 630 | Healthy | 1 | Spain | Female | 74 | 1 | 2 | 2 | 2 | 2 | 12 | 2 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 1 | 3 | 2 | 2 | 2 | 13 | 2 |
| 617 | Healthy | 2 | Spain | Female | 69 | 1 | 3 | 2 | 2 | 2 | 13 | 2 |
| 648 | Healthy | 1 | Spain | Female | 72 | 1 | 3 | 2 | 2 | 2 | 13 | 2 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 800 | Diseased | 3 | Spain | Female | 65 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 643 | Healthy | 1 | Spain | Female | 67 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 640 | Healthy | 1 | Spain | Female | 69 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 624 | Diseased | 1 | Spain | Female | 72 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 790 | Healthy | 3 | Spain | Male | 66 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 796 | Healthy | 3 | Spain | Male | 74 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| 799 | Diseased | 3 | Spain | Male | 79 | 2 | 3 | 2 | 2 | 2 | 14 | 2 |
| Median: Healthy | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 12.0 | 2.0 | |||||
| Median: Diseased | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 12.0 | 2.0 | |||||
| Median: Spain | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 13.0 | 2.0 | |||||
| Median: Hungary | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 12.0 | 2.0 | |||||
| Median: Female | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 12.0 | 2.0 | |||||
| Median: Male | 2.0 | 2.5 | 2.0 | 2.0 | 2.0 | 13.0 | 2.0 | |||||
| Median: All | 2.0 | 3.0 | 2.0 | 2.0 | 2.0 | 12.0 | 2.0 | |||||
| Mean: Healthy | 1.5 | 2.2 | 1.9 | 1.8 | 1.9 | 12.1 | 1.7 | |||||
| Mean: Diseased | 1.8 | 2.8 | 2.0 | 1.1 | 2.0 | 12.4 | 1.7 | |||||
| Mean: Spain | 1.5 | 2.5 | 2.0 | 1.8 | 2.0 | 12.3 | 1.6 | |||||
| Mean: Hungary | 1.7 | 2.2 | 1.8 | 1.2 | 1.8 | 12.0 | 1.7 | |||||
| Mean: Female | 1.6 | 2.4 | 1.9 | 1.5 | 1.9 | 12.0 | 1.6 | |||||
| Mean: Male | 1.6 | 2.3 | 2.0 | 2.0 | 2.0 | 12.8 | 1.8 | |||||
| Mean: All | 1.6 | 2.4 | 1.9 | 1.6 | 1.9 | 12.2 | 1.7 | |||||
| SD: Healthy | 0.4 | 1.1 | 0.2 | 0.4 | 0.2 | 1.7 | 0.4 | |||||
| SD: Diseased | 0.3 | 0.3 | 0.0 | 0.9 | 0.0 | 1.4 | 0.4 | |||||
| SD: Spain | 0.4 | 1.0 | 0.0 | 0.4 | 0.0 | 1.9 | 0.4 | |||||
| SD: Hungary | 0.4 | 1.0 | 0.3 | 0.9 | 0.3 | 1.1 | 0.4 | |||||
| SD: Female | 0.4 | 1.1 | 0.2 | 0.8 | 0.2 | 1.7 | 0.4 | |||||
| SD: Male | 0.4 | 0.7 | 0.0 | 0.0 | 0.0 | 1.2 | 0.3 | |||||
| SD: All | 0.4 | 1.0 | 0.1 | 0.7 | 0.1 | 1.7 | 0.4 | |||||

Memory (MFE)
| ID | Health | Wave | Country | Gender | Age | Q1: Forgetting Objects put | Q2: Failing to Recognise Places | Q3: Finding a Television Story Difficult | Q4: Not Remembering a Change in Daily Routine | Q5: Checking Whether Something Was Done | Q6: Forgetting Time of Events | Q7: Completely Forgetting to Take Things | Q8: Being Reminded about Things | Q9: Reading Anew Already Read Something | Q10: Letting Ramble about Unimportant Things | Q11: Failing to Recognise Close Relatives or Friends | Q12: Having Difficulty Picking up a New Skill | Q13: Finding Word Is “on the tip of the Tongue” | Q14: Forgetting Forgetting to do Planned Things | Q15: Forgetting important details of done things | Q16: Forgetting the Topic of an Ongoing Conversation | Q17: Failing to follow a Story in a Newspaper | Q18: Forgetting to tEll Somebody Something Important | Q19: Forgetting Important Details about Oneself | Q20: Getting Told Details Mixed up and Confused | Q21: Telling Someone a Story or Joke Repeatedly | Q22: Forgetting Details of Things You Do Regularly | Q23: Finding Famous Faces Unfamiliar | Q24: Forgetting Where Things Are Normally Kept | Q25: Getting Lost Where You Have OFTEN been before | Q26: Getting Lost Where You Have Been RARELY before | Q27: Doing Some Routine Thing Twice by Mistake | Q28: Repeating to sOmeone What You Have just Told Them | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 796 | Healthy | 3 | Spain | Male | 74 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 132 | Diseased | 1 | Hungary | Male | 71 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 2 | 0 |
| 643 | Healthy | 2 | Spain | Female | 67 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 3 | 0 |
| 648 | Healthy | 1 | Spain | Female | 72 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 4 | 0 |
| 132 | Diseased | 2 | Hungary | Male | 71 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 5 | 0 |
| 628 | Healthy | 1 | Spain | Female | 70 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 5 | 0 |
| 624 | Diseased | 1 | Spain | Female | 72 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 5 | 0 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0 |
| 535 | Healthy | 3 | Hungary | Male | 69 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 6 | 0 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0 |
| 795 | Healthy | 3 | Spain | Female | 72 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 6 | 0 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 7 | 0 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 7 | 0 |
| 638 | Healthy | 1 | Spain | Female | 71 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 7 | 0 |
| 790 | Healthy | 3 | Spain | Male | 66 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 7 | 0 |
| 700 | Healthy | 2 | Spain | Male | 67 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 7 | 0 |
| 569 | Healthy | 1 | Hungary | Female | 67 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 8 | 0 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 8 | 0 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 8 | 0 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 8 | 0 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 8 | 0 |
| 643 | Healthy | 1 | Spain | Female | 67 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 8 | 0 |
| 800 | Diseased | 3 | Spain | Female | 65 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 9 | 0 |
| 799 | Diseased | 3 | Spain | Male | 79 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 9 | 0 |
| 640 | Healthy | 1 | Spain | Female | 69 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 10 | 0 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 2 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 12 | 0 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 2 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 13 | 1 |
| 641 | Diseased | 2 | Spain | Female | 71 | 0 | 0 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 14 | 1 |
| 649 | Healthy | 1 | Spain | Female | 72 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | 14 | 1 |
| 625 | Diseased | 1 | Spain | Male | 72 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 14 | 1 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 2 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 15 | 1 |
| 641 | Diseased | 1 | Spain | Female | 71 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 15 | 1 |
| 630 | Healthy | 1 | Spain | Female | 74 | 1 | 1 | 0 | 0 | 1 | 1 | 2 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 2 | 1 | 0 | 0 | 1 | 1 | 18 | 1 |
| 617 | Healthy | 2 | Spain | Female | 69 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 2 | 0 | 0 | 1 | 1 | 19 | 1 |
| 620 | Healthy | 2 | Spain | Female | 69 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 20 | 1 |
| Median: Healthy | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.5 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 7.0 | 0.0 | |||||
| Median: Diseased | 0.5 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.5 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.5 | 0.0 | 0.5 | 0.0 | 0.0 | 9.0 | 0.0 | |||||
| Median: Spain | 1.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 0.5 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.5 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 8.5 | 0.0 | |||||
| Median: Hungary | 0.5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 7.5 | 0.0 | |||||
| Median: Female | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 8.0 | 0.0 | |||||
| Median: Male | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 6.0 | 0.0 | |||||
| Median: All | 1.0 | 0.0 | 0.0 | 0.0 | 0.5 | 0.5 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 8.0 | 0.0 | |||||
| Mean: Healthy | 0.7 | 0.0 | 0.1 | 0.1 | 0.4 | 0.4 | 0.4 | 0.5 | 0.1 | 0.2 | 0.0 | 0.5 | 0.8 | 0.2 | 0.1 | 0.1 | 0.0 | 0.3 | 0.0 | 0.2 | 0.4 | 0.2 | 0.4 | 0.5 | 0.0 | 0.2 | 0.2 | 0.2 | 8.4 | 0.1 | |||||
| Mean: Diseased | 0.6 | 0.0 | 0.2 | 0.1 | 0.5 | 0.6 | 0.5 | 0.6 | 0.3 | 0.0 | 0.0 | 0.1 | 0.9 | 0.5 | 0.4 | 0.3 | 0.0 | 0.5 | 0.0 | 0.0 | 0.3 | 0.1 | 0.1 | 0.5 | 0.2 | 0.5 | 0.2 | 0.0 | 9.4 | 0.4 | |||||
| Mean: Spain | 0.7 | 0.0 | 0.2 | 0.1 | 0.6 | 0.6 | 0.6 | 0.5 | 0.3 | 0.1 | 0.0 | 0.4 | 1.0 | 0.3 | 0.2 | 0.0 | 0.1 | 0.4 | 0.0 | 0.1 | 0.5 | 0.2 | 0.5 | 0.6 | 0.0 | 0.3 | 0.4 | 0.3 | 9.6 | 0.3 | |||||
| Mean: Hungary | 0.7 | 0.0 | 0.1 | 0.1 | 0.3 | 0.3 | 0.3 | 0.7 | 0.1 | 0.2 | 0.0 | 0.3 | 0.6 | 0.4 | 0.2 | 0.3 | 0.0 | 0.3 | 0.0 | 0.2 | 0.3 | 0.1 | 0.1 | 0.4 | 0.1 | 0.3 | 0.0 | 0.1 | 7.6 | 0.1 | |||||
| Mean: Female | 0.8 | 0.0 | 0.2 | 0.1 | 0.4 | 0.5 | 0.5 | 0.6 | 0.3 | 0.2 | 0.0 | 0.4 | 1.0 | 0.4 | 0.2 | 0.2 | 0.1 | 0.4 | 0.0 | 0.2 | 0.4 | 0.2 | 0.3 | 0.6 | 0.0 | 0.2 | 0.2 | 0.2 | 9.7 | 0.3 | |||||
| Mean: Male | 0.5 | 0.0 | 0.0 | 0.1 | 0.5 | 0.4 | 0.3 | 0.4 | 0.0 | 0.0 | 0.0 | 0.1 | 0.5 | 0.3 | 0.1 | 0.0 | 0.0 | 0.2 | 0.0 | 0.0 | 0.3 | 0.0 | 0.3 | 0.2 | 0.2 | 0.3 | 0.1 | 0.1 | 6.5 | 0.0 | |||||
| Mean: All | 0.7 | 0.0 | 0.1 | 0.1 | 0.5 | 0.5 | 0.4 | 0.6 | 0.2 | 0.1 | 0.0 | 0.3 | 0.8 | 0.3 | 0.2 | 0.1 | 0.0 | 0.4 | 0.0 | 0.1 | 0.4 | 0.1 | 0.3 | 0.5 | 0.0 | 0.3 | 0.2 | 0.2 | 8.7 | 0.2 | |||||
| SD: Healthy | 0.5 | 0.2 | 0.3 | 0.3 | 0.4 | 0.4 | 0.5 | 0.4 | 0.3 | 0.4 | 0.0 | 0.5 | 0.4 | 0.4 | 0.3 | 0.3 | 0.2 | 0.4 | 0.0 | 0.4 | 0.4 | 0.4 | 0.6 | 0.5 | 0.0 | 0.4 | 0.4 | 0.4 | 4.8 | 0.3 | |||||
| SD: Diseased | 0.7 | 0.0 | 0.5 | 0.3 | 0.4 | 0.4 | 0.5 | 0.4 | 0.4 | 0.2 | 0.2 | 0.3 | 0.6 | 0.4 | 0.4 | 0.4 | 0.2 | 0.4 | 0.0 | 0.2 | 0.4 | 0.3 | 0.3 | 0.5 | 0.4 | 0.5 | 0.4 | 0.2 | 4.4 | 0.4 | |||||
| SD: Spain | 0.4 | 0.2 | 0.5 | 0.3 | 0.4 | 0.4 | 0.5 | 0.5 | 0.4 | 0.3 | 0.0 | 0.4 | 0.3 | 0.4 | 0.4 | 0.2 | 0.3 | 0.4 | 0.0 | 0.3 | 0.5 | 0.4 | 0.6 | 0.5 | 0.0 | 0.4 | 0.4 | 0.4 | 5.5 | 0.4 | |||||
| SD: Hungary | 0.8 | 0.2 | 0.3 | 0.3 | 0.4 | 0.4 | 0.4 | 0.4 | 0.3 | 0.4 | 0.2 | 0.4 | 0.5 | 0.4 | 0.4 | 0.4 | 0.0 | 0.4 | 0.0 | 0.4 | 0.4 | 0.3 | 0.3 | 0.4 | 0.3 | 0.4 | 0.0 | 0.3 | 3.1 | 0.3 | |||||
| SD: Female | 0.6 | 0.1 | 0.5 | 0.3 | 0.4 | 0.4 | 0.5 | 0.4 | 0.4 | 0.4 | 0.1 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.3 | 0.4 | 0.0 | 0.4 | 0.4 | 0.4 | 0.6 | 0.5 | 0.0 | 0.4 | 0.4 | 0.4 | 4.7 | 0.4 | |||||
| SD: Male | 0.6 | 0.2 | 0.0 | 0.3 | 0.4 | 0.4 | 0.4 | 0.4 | 0.0 | 0.2 | 0.0 | 0.3 | 0.4 | 0.4 | 0.3 | 0.2 | 0.0 | 0.4 | 0.0 | 0.2 | 0.4 | 0.2 | 0.4 | 0.4 | 0.4 | 0.4 | 0.3 | 0.3 | 3.8 | 0.2 | |||||
| SD: All | 0.6 | 0.2 | 0.4 | 0.3 | 0.5 | 0.5 | 0.5 | 0.4 | 0.4 | 0.3 | 0.1 | 0.4 | 0.5 | 0.4 | 0.4 | 0.3 | 0.2 | 0.4 | 0.0 | 0.3 | 0.4 | 0.3 | 0.5 | 0.5 | 0.2 | 0.4 | 0.4 | 0.4 | 4.7 | 0.4 | |||||

Sleep (PSQI)
| ID | Health | Wave | Country | Gender | Age | Q1: Time gone to bed at night | Q2: Duration taken to fall asleep | Q3: Time gotten up in the morning | Q4: Duration of actual sleep | Q5A: Trouble sleeping: cannot get to sleep | Q5B: Trouble sleeping: wake up in the middle of the night | Q5C: Trouble sleeping: use the bathroom | Q5D: Trouble sleeping: cannot breathe comfortably | Q5E: Trouble sleeping: cough or snore loudly | Q5F: Trouble sleeping: too cold | Q5G: Trouble sleeping: too hot | Q5H: Trouble sleeping: bad dreams | Q5I: Trouble sleeping: pain | Q5J: Trouble sleeping for other reason(s) | Q6: Frequency of medicine to help you sleep | Q7: Trouble staying awake while driving, eating, or socializing | Q8: Problem with keeping up enthusiasm to get things done | Q9: Sleep quality overall | Subjective Quality Numeric Sub-Score | Latency Numeric Sub-Score | Duration Numeric Sub-Score | Efficiency Numeric Sub-Score | Disturbance Numeric Sub-Score | Medication Numeric Sub-Score | Daytime Dysfunction Numeric Sub-Score | Efficiency Numeric Sub-Score | Numeric Score | Categorical Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 535 | Healthy | 3 | Hungary | Male | 69 | 1410.0 | 10.0 | 510.0 | 480.0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0.9 | 1 | 1 |
| 643 | Healthy | 1 | Spain | Female | 67 | 1410.0 | 5.0 | 420.0 | 420.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0.9 | 1 | 1 |
| 628 | Healthy | 1 | Spain | Female | 70 | 1440.0 | 10.0 | 510.0 | 480.0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0.9 | 1 | 1 |
| 648 | Healthy | 1 | Spain | Female | 72 | 1500.0 | 10.0 | 540.0 | 480.0 | 0 | 1 | 2 | 0 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1.0 | 1 | 1 |
| 620 | Healthy | 2 | Spain | Female | 69 | 1435.0 | 0.0 | 480.0 | 480.0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1.0 | 2 | 1 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 1395.0 | 5.0 | 420.0 | 420.0 | 0 | 1 | 3 | 0 | 0 | 0 | 0 | 3 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0.9 | 3 | 1 |
| 634 | Diseased | 1 | Spain | Male | 72 | 1439.0 | 15.0 | 420.0 | 420.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1.0 | 3 | 1 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 1385.0 | 10.0 | 405.0 | 420.0 | 2 | 2 | 3 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0.9 | 4 | 1 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 1315.0 | 30.0 | 375.0 | 480.0 | 2 | 0 | 1 | 0 | 2 | 0 | 0 | 1 | 2 | 0 | 0 | 0 | 0 | 1 | 1 | 2 | 0 | 0 | 1 | 0 | 0 | 1.0 | 4 | 1 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 1330.0 | 10.0 | 370.0 | 420.0 | 0 | 2 | 0 | 0 | 0 | 0 | 1 | 1 | 2 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0.9 | 4 | 1 |
| 800 | Diseased | 3 | Spain | Female | 65 | 1440.0 | 15.0 | 420.0 | 360.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0.9 | 4 | 1 |
| 643 | Healthy | 2 | Spain | Female | 67 | 1380.0 | 1.0 | 435.0 | 420.0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0.8 | 4 | 1 |
| 790 | Healthy | 3 | Spain | Male | 66 | 1440.0 | 2.0 | 420.0 | 420.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1.0 | 4 | 1 |
| 803 | Healthy | 3 | Spain | Female | 67 | 1500.0 | 15.0 | 390.0 | 360.0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 2 | 0 | 1 | 0 | 1 | 1.0 | 5 | 0 |
| 638 | Healthy | 1 | Spain | Female | 71 | 1470.0 | 24.0 | 480.0 | 420.0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0.9 | 5 | 0 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 1375.0 | 30.0 | 353.0 | 420.0 | 2 | 1 | 2 | 0 | 2 | 0 | 2 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 2 | 1 | 0 | 1 | 0 | 1 | 1.0 | 6 | 0 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 1380.0 | 5.0 | 360.0 | 360.0 | 1 | 2 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 1 | 0.9 | 6 | 0 |
| 640 | Healthy | 1 | Spain | Female | 69 | 1440.0 | 20.0 | 480.0 | 420.0 | 2 | 2 | 2 | 0 | 2 | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 2 | 1 | 0 | 2 | 0 | 0 | 0.9 | 6 | 0 |
| 795 | Healthy | 3 | Spain | Female | 72 | 1500.0 | 10.0 | 510.0 | 360.0 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 0 | 0.8 | 6 | 0 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 1350.0 | 20.0 | 510.0 | 480.0 | 2 | 2 | 3 | 1 | 2 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 2 | 0 | 1 | 2 | 0 | 1 | 0.8 | 7 | 0 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 1320.0 | 3.0 | 330.0 | 360.0 | 0 | 2 | 3 | 0 | 0 | 0 | 0 | 0 | 2 | 2 | 0 | 2 | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 2 | 0.8 | 7 | 0 |
| 799 | Diseased | 3 | Spain | Male | 79 | 1440.0 | 30.0 | 600.0 | 360.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 1 | 2 | 3 | 0 | 0 | 1 | 0.6 | 7 | 0 |
| 641 | Diseased | 2 | Spain | Female | 71 | 1380.0 | 5.0 | 394.0 | 360.0 | 0 | 1 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 3 | 0 | 0 | 1 | 1 | 0 | 2 | 1 | 1 | 3 | 0 | 0.8 | 8 | 0 |
| 624 | Diseased | 1 | Spain | Female | 72 | 1410.0 | 30.0 | 465.0 | 420.0 | 2 | 3 | 3 | 0 | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 2 | 0 | 1 | 0.8 | 8 | 0 |
| 625 | Diseased | 1 | Spain | Male | 72 | 1380.0 | 15.0 | 360.0 | 360.0 | 0 | 3 | 1 | 0 | 3 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 3 | 3 | 1 | 2 | 0 | 2 | 0 | 0 | 0.9 | 8 | 0 |
| 700 | Healthy | 2 | Spain | Male | 67 | 1410.0 | 15.0 | 480.0 | 360.0 | 2 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 2 | 2 | 2 | 1 | 0 | 1 | 0.7 | 9 | 0 |
| 617 | Healthy | 2 | Spain | Female | 69 | 1416.0 | 30.0 | 517.0 | 360.0 | 3 | 3 | 2 | 1 | 1 | 1 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 0 | 0.7 | 10 | 0 |
| 215 | Healthy | 1 | Hungary | Female | 87 | 1380.0 | 30.0 | 420.0 | 250.0 | 1 | 1 | 3 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 2 | 2 | 1 | 3 | 3 | 1 | 1 | 1 | 0.5 | 12 | 0 |
| 630 | Healthy | 1 | Spain | Female | 74 | 1380.0 | 60.0 | 390.0 | 300.0 | 3 | 2 | 2 | 0 | 0 | 0 | 3 | 0 | 0 | 2 | 3 | 0 | 0 | 1 | 1 | 3 | 2 | 2 | 1 | 3 | 0 | 0.7 | 12 | 0 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 1380.0 | 100.0 | 210.0 | 150.0 | 3 | 3 | 1 | 0 | 3 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 1 | 2 | 2 | 3 | 3 | 3 | 2 | 0 | 1 | 0.6 | 14 | 0 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 1404.0 | 60.0 | 245.0 | 150.0 | 3 | 3 | 1 | 0 | 3 | 0 | 2 | 2 | 3 | 3 | 0 | 0 | 1 | 3 | 3 | 3 | 3 | 3 | 2 | 0 | 1 | 0.5 | 15 | 0 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 1320.0 | 120.0 | 300.0 | 161.0 | 3 | 3 | 1 | 1 | 3 | 3 | 1 | 2 | 3 | 3 | 0 | 0 | 1 | 2 | 2 | 3 | 3 | 3 | 3 | 0 | 1 | 0.4 | 15 | 0 |
| Median: Healthy | 1410.0 | 10.0 | 427.5 | 420.0 | 1.0 | 1.0 | 2.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.8 | 5.0 | 0.0 | |||||
| Median: Diseased | 1392.0 | 22.5 | 382.0 | 360.0 | 0.0 | 2.5 | 1.0 | 0.0 | 1.0 | 0.0 | 0.5 | 0.0 | 1.5 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 1.5 | 0.0 | 1.0 | 0.8 | 8.0 | 0.0 | |||||
| Median: Spain | 1439.0 | 15.0 | 465.0 | 420.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.8 | 5.0 | 0.0 | |||||
| Median: Hungary | 1380.0 | 20.0 | 370.0 | 420.0 | 2.0 | 2.0 | 2.0 | 0.0 | 2.0 | 0.0 | 1.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 1.0 | 0.8 | 6.0 | 0.0 | |||||
| Median: Female | 1404.0 | 20.0 | 420.0 | 420.0 | 2.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.8 | 6.0 | 0.0 | |||||
| Median: Male | 1410.0 | 10.0 | 420.0 | 360.0 | 0.0 | 2.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 1.0 | 1.0 | 1.0 | 2.0 | 0.0 | 1.0 | 0.0 | 1.0 | 0.8 | 6.0 | 0.0 | |||||
| Median: All | 1407.0 | 15.0 | 420.0 | 420.0 | 1.0 | 1.0 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0.0 | 1.0 | 0.0 | 0.0 | 0.8 | 6.0 | 0.0 | |||||
| Mean: Healthy | 1410.5 | 15.6 | 442.5 | 406.8 | 1.0 | 1.2 | 1.4 | 0.1 | 0.5 | 0.0 | 0.6 | 0.5 | 0.5 | 0.3 | 0.2 | 0.3 | 0.2 | 0.7 | 0.7 | 1.0 | 1.1 | 0.5 | 1.0 | 0.2 | 0.4 | 0.8 | 5.2 | 0.4 | |||||
| Mean: Diseased | 1392.3 | 40.0 | 378.4 | 316.1 | 1.1 | 1.8 | 0.9 | 0.1 | 1.4 | 0.4 | 0.7 | 0.7 | 1.4 | 0.6 | 0.3 | 0.4 | 0.4 | 1.5 | 1.5 | 1.5 | 2.0 | 1.4 | 1.3 | 0.3 | 0.6 | 0.7 | 8.6 | 0.3 | |||||
| Mean: Spain | 1432.1 | 16.4 | 458.4 | 397.8 | 0.8 | 1.2 | 0.9 | 0.0 | 0.4 | 0.0 | 0.5 | 0.2 | 0.5 | 0.2 | 0.4 | 0.3 | 0.0 | 0.7 | 0.7 | 1.0 | 1.3 | 0.6 | 1.0 | 0.4 | 0.2 | 0.8 | 5.4 | 0.4 | |||||
| Mean: Hungary | 1364.9 | 33.3 | 369.8 | 350.0 | 1.4 | 1.7 | 1.7 | 0.2 | 1.3 | 0.3 | 0.7 | 1.2 | 1.1 | 0.6 | 0.0 | 0.3 | 0.6 | 1.2 | 1.2 | 1.3 | 1.5 | 1.0 | 1.3 | 0.0 | 0.8 | 0.7 | 7.5 | 0.3 | |||||
| Mean: Female | 1408.9 | 27.8 | 420.3 | 372.6 | 1.3 | 1.4 | 1.3 | 0.1 | 1.0 | 0.2 | 0.8 | 0.7 | 0.8 | 0.3 | 0.3 | 0.1 | 0.3 | 0.9 | 0.9 | 1.3 | 1.3 | 0.9 | 1.2 | 0.3 | 0.3 | 0.8 | 6.6 | 0.3 | |||||
| Mean: Male | 1394.3 | 11.6 | 427.7 | 393.3 | 0.3 | 1.4 | 1.0 | 0.0 | 0.3 | 0.0 | 0.2 | 0.2 | 0.7 | 0.4 | 0.0 | 0.8 | 0.3 | 1.0 | 1.0 | 0.6 | 1.4 | 0.6 | 0.8 | 0.0 | 0.7 | 0.8 | 5.4 | 0.4 | |||||
| Mean: All | 1404.8 | 23.2 | 422.4 | 378.4 | 1.0 | 1.4 | 1.2 | 0.1 | 0.8 | 0.1 | 0.6 | 0.6 | 0.8 | 0.4 | 0.2 | 0.3 | 0.3 | 0.9 | 0.9 | 1.1 | 1.4 | 0.8 | 1.1 | 0.2 | 0.5 | 0.8 | 6.3 | 0.4 | |||||
| SD: Healthy | 51.1 | 13.8 | 60.2 | 61.3 | 1.0 | 0.9 | 1.2 | 0.3 | 0.8 | 0.2 | 0.9 | 0.8 | 0.7 | 0.6 | 0.6 | 0.5 | 0.4 | 0.5 | 0.5 | 0.9 | 0.8 | 0.8 | 0.4 | 0.6 | 0.5 | 0.1 | 3.2 | 0.4 | |||||
| SD: Diseased | 40.9 | 38.2 | 106.3 | 109.2 | 1.3 | 1.3 | 0.9 | 0.3 | 1.4 | 0.9 | 0.7 | 0.9 | 1.2 | 1.2 | 0.9 | 0.6 | 0.4 | 0.9 | 0.9 | 1.1 | 0.7 | 1.3 | 1.0 | 0.9 | 0.4 | 0.1 | 4.3 | 0.4 | |||||
| SD: Spain | 38.5 | 13.8 | 59.3 | 48.5 | 1.0 | 1.1 | 1.0 | 0.2 | 0.8 | 0.2 | 0.9 | 0.5 | 0.8 | 0.5 | 0.9 | 0.5 | 0.2 | 0.6 | 0.6 | 0.8 | 0.7 | 0.9 | 0.6 | 0.9 | 0.4 | 0.1 | 3.1 | 0.4 | |||||
| SD: Hungary | 32.3 | 36.2 | 84.8 | 122.8 | 1.1 | 0.8 | 1.1 | 0.4 | 1.2 | 0.8 | 0.7 | 0.8 | 1.0 | 1.1 | 0.2 | 0.6 | 0.4 | 0.7 | 0.7 | 1.1 | 1.1 | 1.3 | 0.6 | 0.2 | 0.5 | 0.1 | 4.6 | 0.4 | |||||
| SD: Female | 50.4 | 29.9 | 83.2 | 102.2 | 1.1 | 1.0 | 1.1 | 0.3 | 1.1 | 0.6 | 1.0 | 0.9 | 0.9 | 0.9 | 0.8 | 0.3 | 0.4 | 0.7 | 0.7 | 1.0 | 1.0 | 1.1 | 0.6 | 0.8 | 0.4 | 0.1 | 4.3 | 0.4 | |||||
| SD: Male | 43.1 | 8.0 | 82.5 | 41.0 | 0.6 | 1.1 | 1.2 | 0.0 | 0.9 | 0.0 | 0.4 | 0.4 | 1.1 | 0.6 | 0.0 | 0.7 | 0.4 | 0.8 | 0.8 | 0.6 | 0.6 | 1.0 | 0.5 | 0.0 | 0.6 | 0.1 | 2.4 | 0.4 | |||||
| SD: All | 48.9 | 26.7 | 83.1 | 89.8 | 1.1 | 1.0 | 1.1 | 0.3 | 1.1 | 0.5 | 0.9 | 0.8 | 1.0 | 0.8 | 0.7 | 0.5 | 0.4 | 0.7 | 0.7 | 1.0 | 0.9 | 1.1 | 0.6 | 0.7 | 0.5 | 0.1 | 3.9 | 0.4 | |||||

Health-Related Quality of Life (EQ-5D-3L)

| ID | Health | Wave | Country | Gender | Age | Q1: Mobility | Q2: Self-Care | Q3: Usual Activities | Q4: Pain/Discomfort | Q5: Anxiety/Depression | Health Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 625 | Diseased | 1 | Spain | Male | 72 | 1 | 1 | 1 | 3 | 1 | 40 |
| 641 | Diseased | 1 | Spain | Female | 71 | 1 | 1 | 1 | 2 | 2 | 50 |
| 640 | Healthy | 1 | Spain | Female | 69 | 1 | 1 | 1 | 2 | 1 | 70 |
| 169 | Diseased | 2 | Hungary | Female | 69 | 1 | 1 | 2 | 2 | 2 | 75 |
| 630 | Healthy | 1 | Spain | Female | 74 | 2 | 1 | 2 | 1 | 2 | 75 |
| 169 | Diseased | 1 | Hungary | Female | 69 | 2 | 1 | 1 | 2 | 2 | 80 |
| 169 | Diseased | 3 | Hungary | Female | 69 | 1 | 1 | 1 | 1 | 2 | 80 |
| 420 | Healthy | 2 | Hungary | Female | 71 | 2 | 1 | 1 | 2 | 2 | 80 |
| 132 | Diseased | 1 | Hungary | Male | 71 | 1 | 1 | 1 | 1 | 1 | 80 |
| 641 | Diseased | 2 | Spain | Female | 71 | 1 | 1 | 1 | 2 | 1 | 80 |
| 624 | Diseased | 1 | Spain | Female | 72 | 2 | 1 | 1 | 2 | 1 | 80 |
| 648 | Healthy | 1 | Spain | Female | 72 | 2 | 1 | 2 | 2 | 1 | 80 |
| 796 | Healthy | 3 | Spain | Male | 74 | 1 | 1 | 1 | 1 | 1 | 80 |
| 575 | Healthy | 2 | Hungary | Female | 65 | 1 | 1 | 1 | 2 | 1 | 85 |
| 170 | Healthy | 3 | Hungary | Male | 70 | 1 | 1 | 1 | 2 | 2 | 85 |
| 132 | Diseased | 3 | Hungary | Male | 71 | 1 | 1 | 1 | 2 | 1 | 90 |
| 212 | Healthy | 1 | Hungary | Male | 72 | 1 | 1 | 2 | 1 | 1 | 90 |
| 643 | Healthy | 2 | Spain | Female | 67 | 1 | 1 | 1 | 1 | 1 | 90 |
| 617 | Healthy | 2 | Spain | Female | 69 | 1 | 1 | 1 | 1 | 1 | 90 |
| 795 | Healthy | 3 | Spain | Female | 72 | 1 | 1 | 1 | 1 | 1 | 90 |
| 569 | Healthy | 3 | Hungary | Female | 67 | 1 | 1 | 1 | 2 | 1 | 95 |
| 133 | Healthy | 1 | Hungary | Female | 71 | 1 | 1 | 1 | 1 | 1 | 95 |
| 419 | Healthy | 2 | Hungary | Male | 95 | 1 | 1 | 1 | 1 | 1 | 95 |
| 799 | Diseased | 3 | Spain | Male | 79 | 1 | 1 | 1 | 1 | 1 | 95 |
| 133 | Healthy | 3 | Hungary | Female | 71 | 1 | 1 | 1 | 1 | 1 | 99 |
| 800 | Diseased | 3 | Spain | Female | 65 | 1 | 1 | 1 | 1 | 1 | 100 |
| 643 | Healthy | 1 | Spain | Female | 67 | 1 | 1 | 1 | 1 | 1 | 100 |
| 628 | Healthy | 1 | Spain | Female | 70 | 1 | 1 | 1 | 1 | 1 | 100 |
| 638 | Healthy | 1 | Spain | Female | 71 | 1 | 1 | 1 | 1 | 1 | 100 |
| 790 | Healthy | 3 | Spain | Male | 66 | 1 | 1 | 1 | 1 | 1 | 100 |
| Median: Healthy | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 90.0 | |||||
| Median: Diseased | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 80.0 | |||||
| Median: Spain | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 90.0 | |||||
| Median: Hungary | 1.0 | 1.0 | 1.0 | 2.0 | 1.0 | 85.0 | |||||
| Median: Female | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 85.0 | |||||
| Median: Male | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 90.0 | |||||
| Median: All | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 87.5 | |||||
| Mean: Healthy | 1.1 | 1.0 | 1.1 | 1.3 | 1.1 | 89.4 | |||||
| Mean: Diseased | 1.1 | 1.0 | 1.0 | 1.7 | 1.3 | 77.2 | |||||
| Mean: Spain | 1.1 | 1.0 | 1.1 | 1.4 | 1.1 | 83.5 | |||||
| Mean: Hungary | 1.1 | 1.0 | 1.1 | 1.5 | 1.3 | 86.8 | |||||
| Mean: Female | 1.2 | 1.0 | 1.1 | 1.4 | 1.2 | 85.4 | |||||
| Mean: Male | 1.0 | 1.0 | 1.1 | 1.4 | 1.1 | 83.8 | |||||
| Mean: All | 1.1 | 1.0 | 1.1 | 1.4 | 1.2 | 84.9 | |||||
| SD: Healthy | 0.3 | 0.0 | 0.3 | 0.4 | 0.3 | 8.9 | |||||
| SD: Diseased | 0.3 | 0.0 | 0.2 | 0.6 | 0.4 | 16.9 | |||||
| SD: Spain | 0.3 | 0.0 | 0.3 | 0.5 | 0.3 | 17.0 | |||||
| SD: Hungary | 0.3 | 0.0 | 0.3 | 0.4 | 0.4 | 7.3 | |||||
| SD: Female | 0.4 | 0.0 | 0.3 | 0.4 | 0.4 | 12.2 | |||||
| SD: Male | 0.0 | 0.0 | 0.3 | 0.6 | 0.3 | 16.7 | |||||
| SD: All | 0.3 | 0.0 | 0.3 | 0.5 | 0.4 | 13.8 | |||||
Appendix C.1.2. Technology-Reported Outcomes (Fitbit)





| PID | Health | Country | Gender | Age | Monitored Days | Energy | Steps | Heart Rate | Sedentary | Sedentary+Light | Light | Light+Fair | Fair | Fair+Very | Very | Active | Sleep | Valid Days |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 502 | Diseased | Hungary | Female | 63 | 231 | 231 | 80 | 73 | 50 | 22 | 49 | 15 | 15 | 9 | 9 | 9 | 8 | 0 |
| 649 | Healthy | Spain | Female | 72 | 135 | 135 | 125 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 630 | Healthy | Spain | Female | 74 | 23 | 23 | 13 | 7 | 7 | 7 | 7 | 4 | 4 | 4 | 4 | 4 | 7 | 1 |
| 799 | Diseased | Spain | Male | 79 | 34 | 34 | 20 | 15 | 16 | 13 | 15 | 6 | 6 | 6 | 6 | 6 | 13 | 5 |
| 648 | Healthy | Spain | Female | 72 | 35 | 35 | 24 | 21 | 22 | 19 | 22 | 14 | 14 | 12 | 12 | 12 | 18 | 11 |
| 791 | Diseased | Spain | Male | 72 | 74 | 74 | 67 | 64 | 56 | 54 | 56 | 12 | 12 | 12 | 12 | 12 | 54 | 11 |
| 800 | Diseased | Spain | Female | 65 | 43 | 43 | 33 | 22 | 22 | 20 | 22 | 17 | 17 | 17 | 17 | 17 | 19 | 12 |
| 798 | Healthy | Spain | Female | 67 | 47 | 47 | 39 | 35 | 36 | 35 | 36 | 31 | 31 | 31 | 31 | 31 | 34 | 20 |
| 796 | Healthy | Spain | Male | 74 | 77 | 77 | 63 | 46 | 49 | 48 | 49 | 48 | 48 | 48 | 48 | 48 | 25 | 20 |
| 575 | Healthy | Hungary | Female | 65 | 69 | 69 | 61 | 59 | 60 | 58 | 60 | 41 | 41 | 41 | 41 | 41 | 59 | 23 |
| 795 | Healthy | Spain | Female | 72 | 274 | 274 | 261 | 40 | 38 | 38 | 38 | 32 | 32 | 31 | 31 | 31 | 35 | 26 |
| 790 | Healthy | Spain | Male | 66 | 79 | 79 | 70 | 67 | 67 | 65 | 67 | 63 | 63 | 63 | 63 | 63 | 30 | 28 |
| 624 | Diseased | Spain | Female | 72 | 153 | 153 | 143 | 138 | 139 | 130 | 139 | 50 | 50 | 47 | 47 | 47 | 131 | 30 |
| 420 | Healthy | Hungary | Female | 71 | 552 | 552 | 446 | 344 | 420 | 233 | 417 | 138 | 138 | 113 | 114 | 113 | 173 | 34 |
| 644 | Diseased | Spain | Male | 70 | 169 | 169 | 142 | 90 | 61 | 58 | 61 | 53 | 53 | 53 | 53 | 53 | 54 | 37 |
| 576 | Healthy | Hungary | Male | 60 | 439 | 439 | 430 | 430 | 430 | 420 | 430 | 119 | 119 | 94 | 95 | 94 | 429 | 49 |
| 634 | Diseased | Spain | Male | 72 | 237 | 237 | 230 | 75 | 60 | 57 | 60 | 55 | 55 | 55 | 55 | 55 | 56 | 50 |
| 793 | Healthy | Spain | Male | 68 | 119 | 119 | 107 | 52 | 52 | 52 | 52 | 52 | 52 | 52 | 52 | 52 | 51 | 51 |
| 641 | Diseased | Spain | Female | 71 | 167 | 167 | 156 | 118 | 134 | 132 | 134 | 122 | 122 | 120 | 121 | 120 | 129 | 63 |
| 643 | Healthy | Spain | Female | 67 | 217 | 217 | 201 | 186 | 186 | 186 | 186 | 171 | 171 | 159 | 159 | 159 | 185 | 90 |
| 638 | Healthy | Spain | Female | 71 | 211 | 211 | 208 | 208 | 208 | 207 | 208 | 147 | 147 | 129 | 130 | 129 | 206 | 127 |
| 212 | Healthy | Hungary | Male | 72 | 733 | 733 | 698 | 580 | 538 | 465 | 538 | 244 | 244 | 230 | 233 | 230 | 439 | 136 |
| 170 | Healthy | Hungary | Male | 70 | 785 | 785 | 777 | 551 | 369 | 353 | 363 | 303 | 303 | 298 | 299 | 298 | 347 | 140 |
| 169 | Diseased | Hungary | Female | 69 | 794 | 794 | 778 | 561 | 398 | 360 | 398 | 312 | 312 | 302 | 303 | 302 | 293 | 141 |
| 625 | Diseased | Spain | Male | 72 | 288 | 288 | 276 | 254 | 254 | 250 | 254 | 221 | 221 | 217 | 217 | 217 | 250 | 141 |
| 628 | Healthy | Spain | Female | 70 | 303 | 303 | 290 | 286 | 289 | 288 | 289 | 278 | 278 | 273 | 273 | 273 | 276 | 146 |
| 617 | Healthy | Spain | Female | 69 | 402 | 402 | 395 | 391 | 392 | 392 | 392 | 355 | 355 | 342 | 344 | 342 | 392 | 170 |
| 569 | Healthy | Hungary | Female | 67 | 501 | 501 | 498 | 483 | 479 | 475 | 479 | 417 | 417 | 415 | 415 | 415 | 476 | 215 |
| 133 | Healthy | Hungary | Female | 71 | 632 | 632 | 623 | 622 | 623 | 622 | 623 | 521 | 521 | 486 | 487 | 486 | 621 | 242 |
| 419 | Healthy | Hungary | Male | 95 | 599 | 599 | 594 | 561 | 567 | 563 | 566 | 502 | 502 | 493 | 494 | 493 | 553 | 245 |
| 640 | Healthy | Spain | Female | 69 | 385 | 385 | 380 | 376 | 377 | 375 | 377 | 346 | 346 | 344 | 345 | 344 | 371 | 295 |
| 132 | Diseased | Hungary | Male | 71 | 639 | 639 | 623 | 618 | 622 | 619 | 622 | 613 | 613 | 613 | 613 | 613 | 617 | 301 |
| Median: Healthy | 274.0 | 274.0 | 261.0 | 208.0 | 208.0 | 207.0 | 208.0 | 138.0 | 138.0 | 113.0 | 114.0 | 113.0 | 185.0 | 51.0 | ||||
| Median: Diseased | 169.0 | 169.0 | 143.0 | 90.0 | 61.0 | 58.0 | 61.0 | 53.0 | 53.0 | 53.0 | 53.0 | 53.0 | 56.0 | 37.0 | ||||
| Median: Spain | 153.0 | 153.0 | 142.0 | 67.0 | 60.0 | 57.0 | 60.0 | 52.0 | 52.0 | 52.0 | 52.0 | 52.0 | 54.0 | 30.0 | ||||
| Median: Hungary | 599.0 | 599.0 | 594.0 | 551.0 | 430.0 | 420.0 | 430.0 | 303.0 | 303.0 | 298.0 | 299.0 | 298.0 | 429.0 | 140.0 | ||||
| Median: Female | 217.0 | 217.0 | 201.0 | 138.0 | 139.0 | 132.0 | 139.0 | 122.0 | 122.0 | 113.0 | 114.0 | 113.0 | 131.0 | 34.0 | ||||
| Median: Male | 237.0 | 237.0 | 230.0 | 90.0 | 67.0 | 65.0 | 67.0 | 63.0 | 63.0 | 63.0 | 63.0 | 63.0 | 56.0 | 50.0 | ||||
| Median: All | 224.0 | 224.0 | 204.5 | 128.0 | 136.5 | 131.0 | 136.5 | 91.0 | 91.0 | 78.5 | 79.0 | 78.5 | 130.0 | 49.5 | ||||
| Mean: Healthy | 315.0 | 315.0 | 300.1 | 254.5 | 248.0 | 233.3 | 247.5 | 182.1 | 182.1 | 174.1 | 174.7 | 174.1 | 225.0 | 98.5 | ||||
| Mean: Diseased | 257.1 | 257.1 | 231.6 | 184.3 | 164.7 | 155.9 | 164.5 | 134.1 | 134.1 | 131.9 | 132.0 | 131.9 | 147.6 | 71.9 | ||||
| Mean: Spain | 165.3 | 165.3 | 154.4 | 118.6 | 117.3 | 115.5 | 117.3 | 98.9 | 98.9 | 95.9 | 96.1 | 95.9 | 111.2 | 63.5 | ||||
| Mean: Hungary | 543.0 | 543.0 | 509.8 | 443.8 | 414.1 | 380.9 | 413.1 | 293.1 | 293.1 | 281.2 | 282.0 | 281.2 | 365.0 | 138.7 | ||||
| Mean: Female | 272.3 | 272.3 | 250.2 | 208.9 | 204.2 | 189.4 | 204.0 | 158.4 | 158.4 | 151.3 | 151.7 | 151.3 | 180.6 | 86.6 | ||||
| Mean: Male | 328.6 | 328.6 | 315.1 | 261.7 | 241.6 | 232.0 | 241.0 | 176.2 | 176.2 | 171.8 | 172.3 | 171.8 | 224.4 | 93.3 | ||||
| Mean: All | 295.1 | 295.1 | 276.5 | 230.4 | 219.4 | 206.7 | 219.0 | 165.6 | 165.6 | 159.6 | 160.0 | 159.6 | 198.4 | 89.3 | ||||
| SD: Healthy | 238.7 | 238.7 | 234.0 | 216.8 | 207.8 | 198.5 | 207.5 | 164.9 | 164.9 | 160.6 | 161.0 | 160.6 | 199.4 | 89.8 | ||||
| SD: Diseased | 231.9 | 231.9 | 235.4 | 200.9 | 181.4 | 179.0 | 181.6 | 177.8 | 177.8 | 177.2 | 177.3 | 177.2 | 173.8 | 86.6 | ||||
| SD: Spain | 113.4 | 113.4 | 114.1 | 116.9 | 118.2 | 118.2 | 118.2 | 109.5 | 109.5 | 106.7 | 107.1 | 106.7 | 118.9 | 72.5 | ||||
| SD: Hungary | 215.8 | 215.8 | 235.1 | 194.6 | 188.3 | 195.7 | 188.6 | 193.3 | 193.3 | 193.8 | 193.8 | 193.8 | 202.2 | 98.0 | ||||
| SD: Female | 215.0 | 215.0 | 212.8 | 195.0 | 186.9 | 179.3 | 186.8 | 158.9 | 158.9 | 153.8 | 154.2 | 153.8 | 176.5 | 89.2 | ||||
| SD: Male | 264.5 | 264.5 | 263.1 | 235.7 | 222.7 | 214.5 | 222.4 | 186.7 | 186.7 | 185.5 | 185.7 | 185.5 | 215.6 | 90.0 | ||||
| SD: All | 238.0 | 238.0 | 236.7 | 214.1 | 203.0 | 195.5 | 202.8 | 171.0 | 171.0 | 167.7 | 168.0 | 167.7 | 194.5 | 89.6 | ||||

| PID | Health | Country | Gender | Age | Energy (kcal.) | Steps (count) | Heart Rate (bpm) | Sedentary (min.) | Sedentary+Light (min.) | Light (min.) | Light+Fair (min.) | Fair (min.) | Fair+Very (min.) | Very (min.) | Active (min.) | Sleep (h:min.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 575 | Healthy | Hungary | Female | 65 | 1733.0 | 8835.0 | 64.0 | 750.0 | 1005.5 | 252.0 | 266.0 | 7.0 | 29.0 | 23.0 | 289.0 | 6:48 |
| 569 | Healthy | Hungary | Female | 67 | 1753.0 | 10,038.5 | 56.0 | 689.0 | 931.0 | 235.0 | 264.0 | 17.0 | 46.0 | 26.0 | 295.0 | 7:42 |
| 420 | Healthy | Hungary | Female | 71 | 1349.0 | 3462.0 | 66.0 | 1286.0 | 945.0 | 120.0 | 181.5 | 10.0 | 19.0 | 6.0 | 184.0 | 9:00 |
| 133 | Healthy | Hungary | Female | 71 | 2163.0 | 9856.0 | 64.0 | 628.0 | 894.0 | 257.0 | 286.0 | 26.0 | 53.0 | 24.0 | 316.0 | 8:18 |
| 576 | Healthy | Hungary | Male | 60 | 2516.0 | 2624.5 | 63.0 | 829.0 | 996.5 | 171.0 | 194.0 | 8.0 | 12.0 | 3.0 | 197.0 | 7:18 |
| 170 | Healthy | Hungary | Male | 70 | 2585.0 | 13,882.0 | 53.0 | 620.0 | 929.0 | 309.0 | 333.0 | 15.0 | 51.5 | 31.0 | 375.0 | 7:42 |
| 212 | Healthy | Hungary | Male | 72 | 2046.0 | 3445.0 | 56.0 | 1152.5 | 1203.0 | 92.0 | 120.5 | 8.0 | 22.0 | 11.0 | 133.5 | 4:18 |
| 419 | Healthy | Hungary | Male | 95 | 2490.0 | 5239.0 | 52.0 | 704.0 | 885.0 | 168.0 | 206.0 | 26.0 | 68.0 | 37.5 | 250.0 | 8:12 |
| 643 | Healthy | Spain | Female | 67 | 1795.0 | 9281.0 | 57.0 | 603.0 | 935.5 | 322.0 | 362.0 | 32.0 | 49.0 | 15.0 | 384.0 | 7:42 |
| 798 | Healthy | Spain | Female | 67 | 1817.0 | 9911.0 | 76.0 | 691.0 | 971.0 | 263.5 | 309.0 | 23.0 | 75.0 | 42.0 | 351.0 | 6:42 |
| 640 | Healthy | Spain | Female | 69 | 1708.0 | 8892.5 | 59.5 | 705.0 | 934.0 | 225.0 | 248.0 | 18.0 | 38.0 | 20.0 | 273.0 | 7:48 |
| 617 | Healthy | Spain | Female | 69 | 1639.0 | 8545.0 | 70.0 | 691.0 | 873.5 | 180.0 | 207.0 | 22.0 | 56.0 | 33.0 | 239.0 | 8:18 |
| 628 | Healthy | Spain | Female | 70 | 1833.0 | 8876.0 | 57.0 | 583.0 | 821.0 | 235.0 | 310.5 | 70.0 | 126.0 | 40.0 | 362.0 | 8:18 |
| 638 | Healthy | Spain | Female | 71 | 1896.0 | 7907.5 | 67.0 | 728.5 | 976.0 | 248.0 | 274.0 | 21.0 | 47.0 | 18.0 | 284.0 | 7:06 |
| 648 | Healthy | Spain | Female | 72 | 1425.0 | 6235.0 | 66.0 | 778.0 | 992.0 | 226.5 | 244.5 | 13.0 | 24.5 | 8.0 | 251.5 | 7:18 |
| 649 | Healthy | Spain | Female | 72 | 1854.0 | 7520.0 | ||||||||||
| 795 | Healthy | Spain | Female | 72 | 1396.0 | 5664.0 | 58.0 | 764.0 | 1039.0 | 265.5 | 300.0 | 26.0 | 48.0 | 17.0 | 316.0 | 6:18 |
| 630 | Healthy | Spain | Female | 74 | 1320.0 | 6577.0 | 57.0 | 825.0 | 1008.0 | 147.0 | 163.5 | 6.5 | 17.5 | 9.5 | 171.0 | 6:54 |
| 790 | Healthy | Spain | Male | 66 | 2686.0 | 14123.5 | 60.0 | 1106.0 | 1298.0 | 205.0 | 233.0 | 23.0 | 79.0 | 52.0 | 304.0 | 3:30 |
| 793 | Healthy | Spain | Male | 68 | 2536.0 | 8879.0 | 64.0 | 791.5 | 1086.5 | 291.0 | 328.0 | 35.5 | 59.0 | 25.0 | 367.0 | 4:48 |
| 796 | Healthy | Spain | Male | 74 | 2347.0 | 13989.0 | 61.0 | 1113.0 | 1292.5 | 175.0 | 210.5 | 29.0 | 97.0 | 71.5 | 288.5 | 8:06 |
| 502 | Diseased | Hungary | Female | 63 | 1230.0 | 2171.0 | 75.0 | 1327.5 | 1424.5 | 96.0 | 155.0 | 11.0 | 14.0 | 3.0 | 166.0 | 1:36 |
| 169 | Diseased | Hungary | Female | 69 | 2000.5 | 7659.0 | 54.0 | 836.5 | 994.0 | 199.0 | 248.0 | 24.0 | 56.0 | 22.0 | 284.5 | 7:06 |
| 132 | Diseased | Hungary | Male | 71 | 3036.0 | 11136.0 | 51.0 | 605.5 | 807.0 | 193.0 | 231.0 | 32.0 | 127.0 | 96.0 | 335.0 | 8:24 |
| 800 | Diseased | Spain | Female | 65 | 1643.0 | 9030.0 | 77.5 | 739.0 | 989.5 | 244.0 | 284.0 | 21.0 | 43.0 | 19.0 | 308.0 | 7:00 |
| 641 | Diseased | Spain | Female | 71 | 1676.0 | 10216.0 | 65.0 | 718.0 | 965.5 | 223.5 | 274.0 | 33.0 | 69.0 | 31.0 | 308.0 | 7:06 |
| 624 | Diseased | Spain | Female | 72 | 1979.0 | 5292.0 | 63.0 | 730.0 | 970.0 | 257.0 | 279.5 | 13.0 | 21.0 | 7.0 | 287.0 | 7:42 |
| 644 | Diseased | Spain | Male | 70 | 2566.0 | 7903.5 | 61.0 | 781.0 | 952.0 | 177.0 | 197.0 | 11.0 | 40.0 | 27.0 | 231.0 | 7:30 |
| 625 | Diseased | Spain | Male | 72 | 2197.0 | 10394.5 | 53.0 | 589.0 | 876.0 | 291.0 | 320.0 | 20.0 | 45.0 | 22.0 | 351.0 | 8:30 |
| 634 | Diseased | Spain | Male | 72 | 3121.0 | 12832.5 | 61.0 | 794.5 | 1060.0 | 232.5 | 310.0 | 54.0 | 141.0 | 77.0 | 393.0 | 4:24 |
| 791 | Diseased | Spain | Male | 72 | 2397.5 | 4012.0 | 62.0 | 789.0 | 986.0 | 185.0 | 199.0 | 7.5 | 12.5 | 5.0 | 204.5 | 7:36 |
| 799 | Diseased | Spain | Male | 79 | 1682.0 | 4268.0 | 49.0 | 878.0 | 960.0 | 140.0 | 187.5 | 7.5 | 13.0 | 7.0 | 193.0 | 8:00 |
| Median: Healthy | 1833.0 | 8835.0 | 60.5 | 739.2 | 973.5 | 230.7 | 256.0 | 21.5 | 48.5 | 23.5 | 288.7 | 7:30 | ||||
| Median: Diseased | 2000.5 | 7903.5 | 61.0 | 781.0 | 970.0 | 199.0 | 248.0 | 20.0 | 43.0 | 22.0 | 287.0 | 7:24 | ||||
| Median: Spain | 1833.0 | 8876.0 | 61.0 | 751.5 | 973.5 | 229.5 | 274.0 | 21.5 | 47.5 | 21.0 | 296.2 | 7:24 | ||||
| Median: Hungary | 2046.0 | 7659.0 | 56.0 | 750.0 | 945.0 | 193.0 | 231.0 | 15.0 | 46.0 | 23.0 | 284.5 | 7:36 | ||||
| Median: Female | 1733.0 | 8545.0 | 64.0 | 729.2 | 970.5 | 235.0 | 270.0 | 21.0 | 46.5 | 19.5 | 288.0 | 7:12 | ||||
| Median: Male | 2516.0 | 8879.0 | 60.0 | 791.5 | 986.0 | 185.0 | 210.5 | 20.0 | 51.5 | 27.0 | 288.5 | 7:30 | ||||
| Median: All | 1875.0 | 8690.0 | 61.0 | 750.0 | 971.0 | 225.0 | 248.0 | 21.0 | 47.0 | 22.0 | 288.5 | 7:24 | ||||
| Mean: Healthy | 1947.0 | 8275.3 | 61.3 | 801.8 | 1000.8 | 219.3 | 252.0 | 21.8 | 50.8 | 25.6 | 281.5 | 7:06 | ||||
| Mean: Diseased | 2138.9 | 7719.5 | 61.0 | 798.9 | 998.5 | 203.4 | 244.0 | 21.2 | 52.8 | 28.7 | 278.2 | 6:48 | ||||
| Mean: Spain | 1976.8 | 8588.0 | 62.2 | 769.8 | 999.3 | 226.6 | 262.0 | 24.3 | 55.0 | 27.3 | 293.3 | 7:00 | ||||
| Mean: Hungary | 2081.9 | 7122.5 | 59.4 | 857.0 | 1001.3 | 190.1 | 225.9 | 16.7 | 45.2 | 25.6 | 256.8 | 6:54 | ||||
| Mean: Female | 1695.2 | 7682.5 | 64.0 | 781.8 | 981.6 | 222.0 | 258.6 | 21.8 | 46.1 | 20.1 | 281.6 | 7:06 | ||||
| Mean: Male | 2477.3 | 8671.4 | 57.3 | 827.1 | 1025.5 | 202.2 | 236.1 | 21.2 | 59.0 | 35.7 | 278.6 | 6:42 | ||||
| Mean: All | 2012.9 | 8084.2 | 61.2 | 800.8 | 1000.0 | 213.7 | 249.2 | 21.6 | 51.5 | 26.7 | 280.3 | 7:00 | ||||
| SD: Healthy | 423.2 | 3171.9 | 5.8 | 195.5 | 126.4 | 59.8 | 61.2 | 13.8 | 27.7 | 16.5 | 69.1 | 1:24 | ||||
| SD: Diseased | 569.0 | 3237.4 | 8.7 | 186.8 | 148.5 | 52.3 | 51.7 | 13.4 | 42.2 | 28.9 | 68.1 | 1:54 | ||||
| SD: Spain | 462.0 | 2735.1 | 6.7 | 135.3 | 115.4 | 47.6 | 53.6 | 15.2 | 34.1 | 19.9 | 62.4 | 1:18 | ||||
| SD: Hungary | 524.4 | 3768.4 | 7.1 | 257.4 | 164.0 | 66.6 | 58.9 | 8.4 | 31.6 | 24.8 | 73.3 | 2:00 | ||||
| SD: Female | 246.3 | 2204.8 | 6.9 | 196.6 | 119.0 | 54.1 | 52.0 | 13.9 | 25.8 | 11.0 | 59.4 | 1:30 | ||||
| SD: Male | 363.2 | 4196.1 | 4.9 | 183.5 | 150.1 | 60.7 | 63.4 | 13.4 | 40.8 | 28.7 | 79.8 | 1:42 | ||||
| SD: All | 486.9 | 3205.5 | 7.0 | 192.5 | 134.7 | 57.8 | 58.2 | 13.7 | 33.6 | 21.8 | 68.8 | 1:36 | ||||

Energy Expenditure (Raw Family)
Steps (Raw Family)
Heart Rate (Raw Family)
Sedentary Duration (Processed Family)
Light Intensity Physical Activity Duration (Processed Family)
Fair Intensity Physical Activity Duration (Processed Family)
Vigorous Intensity Physical Activity Duration (Processed Family)
Sleep Duration (Processed Family)
Appendix C.2. Inferential Analysis (PROs vs. TechROs)
| PRO | Work walking activity | Work Moderate Activity | Work Vigorous Activity | Work Total Activity | Transport Walking Activity | Transport Bicycle Activity | Transport Total Activity | Domestic Moderate Activity | Garden Moderate Activity | Garden Vigorous Activity | Domestic+Garden Total Activity | Leisure Walking Activity | Leisure Moderate Activity | Leisure Vigorous Activity | Leisure Total Activity | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | ||||||||||||||||||||||||||||||||||||||||||||||
| Steps | |||||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | |||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | |||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | |||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | |||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||
| Active | |||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 1 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | |||||||||||||||||||
| Processed | Total | 2 | 2 | 2 | 5 | 2 | 3 | 5 | 1 | 2 | 2 | 1 | 5 | 1 | 1 | 4 | 2 | 4 | 4 | 4 | 2 | 4 | 6 | 1 | 2 | 6 | 3 | 4 | 1 | 3 | 4 | 3 | 3 | 3 | 4 | 1 | 6 | 2 | 4 | 4 | |||||||
| CLR PA | Total | 1 | 2 | 3 | 1 | 2 | 1 | 1 | 3 | 3 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 3 | 2 | 4 | 1 | 1 | 3 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | ||||||||||||||
| CLR PA+S | Total | 3 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | 3 | 1 | 2 | 2 | 2 | 1 | 2 | 3 | 2 | 3 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | |||||||||||||
| All Families | Total | 5 | 7 | 8 | 3 | 6 | 10 | 6 | 9 | 11 | 4 | 8 | 8 | 4 | 9 | 6 | 4 | 7 | 5 | 6 | 2 | 8 | 11 | 6 | 7 | 10 | 4 | 3 | 7 | 12 | 8 | 7 | 5 | 4 | 4 | 5 | 7 | 7 | 5 | 1 | 1 | 12 | 5 | 4 | 9 | ||
| PRO | Q1: Special person: around when in need | Q2: Special person: share joys and sorrows | Q3: Family: tries to help | Q4: Family: gives emotional help and support | Q5: Special person: real source of comfort | Q6: Friends: try to help | Q7: Friends: counted on when things go wrong | Q8: Family: talk about problems | Q9: Friends: share my joys and sorrows | Q10: Special person: cares about feelings | Q11: Family: willing to help make decisions | Q12: Friends: talk about problems | Significant other numeric sub-score | Family numeric sub-score | Friends numeric sub-score | Categorical score | Numeric score | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Steps | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Active | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||||||||||||||||||||||
| Processed | Total | 2 | 5 | 4 | 2 | 6 | 5 | 3 | 6 | 2 | 2 | 4 | 2 | 4 | 6 | 2 | 4 | 7 | 3 | 3 | 6 | 3 | 4 | 5 | 2 | 6 | 2 | 2 | 7 | 3 | 5 | 6 | 1 | 2 | 7 | 2 | 2 | 7 | 4 | 4 | 7 | 3 | 6 | 2 | 4 | 7 | 1 | 4 | 7 | 4 | |||
| CLR PA | Total | 1 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 2 | 2 | 1 | 1 | 3 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 2 | ||||||||||||||||
| CLR PA+S | Total | 1 | 3 | 1 | 2 | 3 | 2 | 4 | 1 | 1 | 1 | 2 | 2 | 1 | 4 | 3 | 3 | 3 | 4 | 1 | 4 | 1 | 3 | 4 | 2 | 2 | 2 | 2 | 3 | 3 | 1 | 1 | 3 | 1 | 3 | 1 | 1 | 2 | 2 | 1 | 3 | 1 | |||||||||||
| All Families | Total | 4 | 9 | 5 | 5 | 10 | 6 | 7 | 14 | 3 | 3 | 6 | 2 | 7 | 9 | 3 | 5 | 14 | 4 | 9 | 11 | 5 | 10 | 10 | 1 | 5 | 13 | 5 | 6 | 12 | 5 | 10 | 10 | 2 | 6 | 13 | 3 | 3 | 10 | 6 | 6 | 11 | 1 | 8 | 12 | 4 | 7 | 11 | 4 | 8 | 13 | 5 | |
| PRO | Q1A: Keyed-up or on edge | Q2A: Worrying a lot? | Q3A: Irritable? | Q4A: Difficulty relaxing? | Q5A: Sleeping poorly? | Q6A: Headaches or neck aches? | Q7A: Trembling [...] urine? | Q8A: Worried about your health? | Q9A: Difficulty falling asleep? | Q1D: Lacking energy? | Q2D: Lost interest in things? | Q3D: Lost confidence in yourself? | Q4D: Hopeless? | Q5D: Difficulty concentrating? | Q6D: Lost weight due to poor appetite? | Q7D: Waking early? | Q8D: Slowed down? | Q9D: Worse in the mornings? | Numeric score | Categorical score | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Steps | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Active | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | |||||||||||||||||||||||||||||||||||||||
| Processed | Total | 6 | 1 | 4 | 2 | 2 | 3 | 2 | 1 | 2 | 1 | 4 | 1 | 5 | 1 | 4 | 2 | 2 | 3 | 3 | 3 | 4 | 1 | 3 | 6 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 5 | 2 | 1 | 2 | 4 | 4 | 1 | 3 | 1 | 1 | 2 | 2 | 2 | |||||||||||||||||
| CLR PA | Total | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 1 | 4 | 1 | 1 | 4 | 1 | 1 | 3 | 2 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 3 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 1 | |||||||||||||||||||||||
| CLR PA+S | Total | 2 | 1 | 1 | 1 | 1 | 2 | 3 | 2 | 1 | 2 | 1 | 4 | 3 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 1 | 4 | 2 | 1 | 3 | 2 | 2 | 3 | 2 | 1 | 3 | 3 | 4 | 2 | 2 | 2 | 1 | 3 | 4 | 4 | 4 | 4 | 3 | 2 | ||||||||||||||
| All Families | Total | 3 | 1 | 2 | 1 | 2 | 11 | 4 | 7 | 6 | 4 | 8 | 4 | 6 | 6 | 3 | 2 | 7 | 4 | 7 | 4 | 10 | 4 | 4 | 8 | 7 | 7 | 10 | 8 | 3 | 5 | 12 | 3 | 5 | 5 | 2 | 5 | 4 | 5 | 4 | 4 | 1 | 12 | 7 | 3 | 2 | 1 | 3 | 7 | 8 | 3 | 6 | 8 | 2 | 6 | 8 | 1 | 5 | 5 | 1 | ||
| PRO | Q2: Olive oil use | Q3: Vegetables use | Q4: Fruits use | Q5: Red meat, hamburger, or meat use | Q6: Butter, margarine, or cream use | Q7: Sweet/carbonated beverage use | Q8: Wine use | Q9: Legumes use | Q10: Fish or shellfish use | Q11: Commercial sweets or pastries | Q12: Nuts use | Q14: Sofrito use | Numeric score | Categorical score | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | |||||||||||||||||||||||||||||||||||||||||||
| Steps | ||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | ||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | |||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | ||||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | ||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | ||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||
| Active | ||||||||||||||||||||||||||||||||||||||||||||
| Sleep | ||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | |||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | |||||||||||||||||||||||||||||||||||||||||||
| Light | ||||||||||||||||||||||||||||||||||||||||||||
| Fair | ||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | ||||||||||||||||||||||||||||||||||||||||||||
| Sleep | ||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | |||||||||||||||||||||||||||||||
| Processed | Total | 1 | 1 | 2 | 2 | 3 | 1 | 3 | 1 | 2 | 3 | 2 | 3 | 1 | 2 | 2 | 1 | 3 | 2 | 4 | 2 | |||||||||||||||||||||||
| CLR PA | Total | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 4 | 1 | 3 | 2 | ||||||||||||||||||||||
| CLR PA+S | Total | 1 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 1 | 4 | 1 | 3 | 2 | 1 | 5 | 3 | 1 | 1 | 1 | 2 | ||||||||||||||||||
| All Families | Total | 2 | 4 | 3 | 4 | 5 | 7 | 4 | 5 | 1 | 4 | 2 | 2 | 4 | 5 | 4 | 3 | 2 | 1 | 5 | 2 | 6 | 1 | 7 | 3 | 7 | 5 | 9 | 4 | 10 | 6 | 1 | ||||||||||||
| PRO | Q1: Food Intake Declined | Q2: Weight Lost | Q4: Stressed or Severely Ill | Q5: Dementia and/or Severe Sadness | Numeric Score | Categorical Score | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | |||||||||||||||||||
| Steps | ||||||||||||||||||||
| Heart rate | ||||||||||||||||||||
| Processed | Sedentary | |||||||||||||||||||
| Sedentary+light | ||||||||||||||||||||
| Light | ||||||||||||||||||||
| Light+fair | ||||||||||||||||||||
| Fair | ||||||||||||||||||||
| Fair+vigorous | ||||||||||||||||||||
| Vigorous | ||||||||||||||||||||
| Active | ||||||||||||||||||||
| Sleep | ||||||||||||||||||||
| CLR PA | Sedentary | |||||||||||||||||||
| Light | ||||||||||||||||||||
| Fair | ||||||||||||||||||||
| Vigorous | ||||||||||||||||||||
| CLR PA+S | Sedentary | |||||||||||||||||||
| Light | ||||||||||||||||||||
| Fair | ||||||||||||||||||||
| Vigorous | ||||||||||||||||||||
| Sleep | ||||||||||||||||||||
| Raw | Total | 1 | 1 | |||||||||||||||||
| Processed | Total | 2 | 3 | 3 | 2 | 1 | ||||||||||||||
| CLR PA | Total | 1 | 1 | 2 | 2 | 2 | ||||||||||||||
| CLR PA+S | Total | 2 | 2 | 1 | 1 | 2 | 2 | |||||||||||||
| All Families | Total | 6 | 7 | 4 | 3 | 6 | 5 | |||||||||||||
| PRO | Q1: Forgetting objects put | Q2: Failing to recognise places | Q3: Finding a television story difficult | Q4: Not remembering a change in daily routine | Q5: Checking whether something was done | Q6: Forgetting the time of events | Q7: Completely forgetting to take things | Q8: Being reminded about things | Q9: Reading anew something already read | Q10: Letting ramble about unimportant things | Q11: Failing to recognise close relatives or friends | Q12: Having difficulty picking up a new skill | Q13: Finding word is “on the tip of the tongue” | Q14: Forgetting to do planned things | Q15: Forgetting important details of done things | Q16: Forgetting the topic of an ongoing conversation | Q17: Failing to follow a story in a newspaper | Q18: Forgetting to tell somebody something important | Q20: Getting told details mixed up and confused | Q21: Telling someone a story or joke repeatedly | Q22: Forgetting details of things you do regularly | Q23: Finding famous faces unfamiliar | Q24: Forgetting where things are normally kept | Q25: Getting lost where you have OFTEN been before | Q26: Getting lost where you have been RARELY before | Q27: Doing some routine thing twice by mistake | Q28: Repeating to someone what you have just told them | Numeric score | Categorical score | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Steps | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Active | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Total | 3 | 6 | 1 | 1 | 1 | 1 | 2 | 4 | 1 | 3 | 2 | 2 | 4 | 7 | 5 | 3 | 5 | 1 | 1 | 4 | 1 | 2 | 2 | 4 | 6 | 6 | 1 | 4 | 7 | 5 | 6 | 2 | 3 | 7 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 5 | 4 | 1 | 1 | 1 | 4 | 2 | 3 | 1 | 1 | 2 | 2 | 1 | 3 | 2 | 7 | 3 | 1 | 1 | 3 | 6 | 6 | 3 | 5 | 5 | ||||||||||||||||||||||
| CLR PA | Total | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 3 | 3 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 1 | 2 | 1 | 3 | 1 | 1 | 3 | 2 | 2 | 3 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 3 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 3 | 2 | 2 | 1 | ||||||||||||||||||||||||||||||
| CLR PA+S | Total | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 3 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 3 | 3 | 4 | 3 | 2 | 2 | 3 | 3 | 1 | 4 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 3 | 2 | 1 | 1 | 3 | 3 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | ||||||||||||||||||||||||||||||||
| All Families | Total | 1 | 5 | 11 | 1 | 1 | 1 | 1 | 3 | 4 | 6 | 4 | 7 | 5 | 6 | 9 | 14 | 8 | 2 | 8 | 9 | 3 | 3 | 8 | 2 | 2 | 6 | 9 | 11 | 12 | 3 | 7 | 13 | 10 | 12 | 2 | 7 | 13 | 2 | 3 | 3 | 2 | 2 | 2 | 1 | 4 | 5 | 8 | 2 | 6 | 5 | 8 | 5 | 6 | 6 | 5 | 5 | 5 | 4 | 3 | 7 | 1 | 3 | 12 | 6 | 1 | 5 | 5 | 6 | 1 | 3 | 6 | 11 | 11 | 6 | 10 | 8 | ||||||||||||
| PRO | Q1: time gone to bed at night | Q2: duration taken to fall asleep | Q3: time gotten up in the morning | Q4: duration of actual sleep | Q5A: trouble sleeping: cannot get to sleep | Q5B: trouble sleeping: wake up in the middle of the night | Q5C: trouble sleeping: use the bathroom | Q5D: trouble sleeping: cannot breathe comfortably | Q5E: trouble sleeping: cough or snore loudly | Q5F: trouble sleeping: too cold | Q5G: trouble sleeping: too hot | Q5H: trouble sleeping: bad dreams | Q5I: trouble sleeping: pain | Q5J: trouble sleeping for other reason(s) | Q6: Frequency of medicine to help you sleep | Q7: Trouble staying awake while driving, eating, or socializing | Q8: Problem with keeping up enthusiasm to get things done | Q9: sleep quality overall | Q11: Duration stayed in bed | Numeric score | Categorical score | Quality numeric sub-score | Latency numeric sub-score | Duration numeric sub-score | Efficiency numeric sub-score | Disturbance numeric sub-score | Medication numeric sub-score | Daily dysfunction numeric sub-score | Efficiency numeric sub-score | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Steps | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart rate | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sedentary+light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light+fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair+vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Active | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Raw | Total | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 2 | |||||||||||||||||||||||||||||||||||||||||||||||||
| Processed | Total | 4 | 2 | 1 | 1 | 1 | 1 | 5 | 5 | 4 | 1 | 1 | 2 | 1 | 2 | 4 | 4 | 2 | 3 | 1 | 2 | 2 | 1 | 2 | 3 | 2 | 1 | 1 | 2 | 5 | 5 | 4 | 1 | 2 | 3 | 5 | 2 | 2 | 2 | 6 | 2 | 1 | 5 | 3 | 5 | 2 | 1 | 1 | 1 | 3 | 3 | 1 | 1 | 2 | 4 | 3 | 4 | 3 | 2 | ||||||||||||||||||||||||||||||
| CLR PA | Total | 1 | 1 | 2 | 1 | 1 | 1 | 3 | 3 | 2 | 1 | 1 | 1 | 1 | 2 | 1 | 4 | 3 | 3 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 4 | 3 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 3 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 1 | 3 | 2 | 2 | 2 | 2 | 2 | 1 | 3 | 3 | 1 | 3 | 2 | |||||||||||||||||||||||||||||||
| CLR PA+S | Total | 1 | 2 | 5 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 3 | 3 | 4 | 3 | 2 | 3 | 1 | 2 | 1 | 2 | 3 | 2 | 4 | 1 | 2 | 1 | 3 | 1 | 1 | 1 | 1 | 2 | 2 | 3 | 1 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | ||||||||||||||||||||||||||||||||||||||||||
| All Families | Total | 6 | 4 | 2 | 7 | 6 | 4 | 4 | 5 | 2 | 11 | 11 | 6 | 4 | 5 | 4 | 4 | 5 | 2 | 7 | 10 | 4 | 3 | 7 | 7 | 2 | 4 | 1 | 3 | 5 | 1 | 7 | 3 | 4 | 6 | 4 | 2 | 1 | 5 | 1 | 1 | 14 | 10 | 5 | 5 | 7 | 1 | 5 | 8 | 5 | 4 | 8 | 2 | 5 | 8 | 4 | 3 | 6 | 1 | 5 | 8 | 5 | 4 | 7 | 3 | 8 | 8 | 1 | 4 | 5 | 1 | 2 | 3 | 2 | 1 | 1 | 10 | 9 | 7 | 8 | 5 | ||||||||
| PRO | Q1: Mobility | Q2: Self-Care | Q3: Usual Activities | Q4: Pain/Discomfort | Q5: Anxiety/Depression | Health Score | Mobility Numeric Score | Self-Care Numeric Score | Usual aCtivities Numeric Score | Pain/Discomfort Numeric Score | Anxiety/Depression Numeric Score | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family | TechRO | Health | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased | Both | Healthy | Diseased |
| Raw | Energy | ||||||||||||||||||||||||||||||||||
| Steps | |||||||||||||||||||||||||||||||||||
| Heart rate | |||||||||||||||||||||||||||||||||||
| Processed | Sedentary | ||||||||||||||||||||||||||||||||||
| Sedentary+light | |||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||
| Light+fair | |||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||
| Fair+vigorous | |||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||
| Active | |||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||
| CLR PA | Sedentary | ||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||
| CLR PA+S | Sedentary | ||||||||||||||||||||||||||||||||||
| Light | |||||||||||||||||||||||||||||||||||
| Fair | |||||||||||||||||||||||||||||||||||
| Vigorous | |||||||||||||||||||||||||||||||||||
| Sleep | |||||||||||||||||||||||||||||||||||
| Raw | Total | 1 | 1 | 2 | 1 | 1 | 1 | 2 | |||||||||||||||||||||||||||
| Processed | Total | 1 | 2 | 4 | 2 | 3 | 2 | 3 | 4 | 1 | 1 | 2 | 4 | 2 | 3 | 2 | 3 | ||||||||||||||||||
| CLR PA | Total | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 1 | |||||||||||||||||||||||||
| CLR PA+S | Total | 3 | 1 | 3 | 2 | 3 | 1 | ||||||||||||||||||||||||||||
| All Families | Total | 1 | 1 | 6 | 7 | 3 | 3 | 3 | 5 | 8 | 5 | 2 | 1 | 1 | 6 | 7 | 3 | 3 | 3 | 5 | |||||||||||||||
References
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- WHO Regional Office for Europe. Noncommunicable Diseases; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Anderson, G. Responding to the Growing Cost and Prevalence of People with Multiple Chronic Conditions. Ph.D. Thesis, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA, 2011. [Google Scholar]
- United States Office of the Assistant Secretary for Health. Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention; United States Public Health Service: Washington, DC, USA, 1979.
- United Nations Department of Economic and Social Affairs. World Population Prospects 2019: Highlights; United Nations Department for Economic and Social Affairs: New York, NY, USA, 2019.
- Mayo, N.E.; Figueiredo, S.; Ahmed, S.; Bartlett, S.J. Montréal Accord on Patient-Reported Outcomes (PROs) use series–Paper 2: Terminology proposed to measure what matters in health. J. Clin. Epidemiol. 2017, 89, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.; Smith, F.; Duffy, A.; Hilton, S. The vagaries of self-reports of physical activity: A problem revisited and addressed in a study of exercise promotion in the over 65 s in general practice. Fam. Pract. 1999, 16, 152–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, K.N.; Catt, M.; Collerton, J.; Davies, K.; von Zglinicki, T.; Kirkwood, T.B.; Jagger, C. Assessment of sleep and circadian rhythm disorders in the very old: the Newcastle 85+ Cohort Study. Age Ageing 2014, 43, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Berg, J.F.; Van Rooij, F.J.; Vos, H.; Tulen, J.H.; Hofman, A.; Miedema, H.M.; Neven, A.K.; Tiemeier, H. Disagreement between subjective and actigraphic measures of sleep duration in a population-based study of elderly persons. J. Sleep Res. 2008, 17, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Wac, K. From quantified self to quality of life. In Digital Health; Springer: Berlin/Heidelberg, Germany, 2018; pp. 83–108. [Google Scholar]
- Sylvia, L.G.; Bernstein, E.E.; Hubbard, J.L.; Keating, L.; Anderson, E.J. Practical guide to measuring physical activity. J. Acad. Nutr. Diet. 2014, 114, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, T.; Rowlands, A.V.; Olds, T.; Maher, C. The validity of consumer-level, activity monitors in healthy adults worn in free-living conditions: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 42. [Google Scholar] [CrossRef] [Green Version]
- International Data Corporation. IDC Forecasts Sustained Double-Digit Growth for Wearable Devices Led by Steady Adoption of Smartwatches; International Data Corporation: San Mateo, CA, USA, 2019. [Google Scholar]
- Dominick, G.M.; Winfree, K.N.; Pohlig, R.T.; Papas, M.A. Physical activity assessment between consumer-and research-grade accelerometers: A comparative study in free-living conditions. JMIR mHealth uHealth 2016, 4, e110. [Google Scholar] [CrossRef]
- McMahon, S.K.; Lewis, B.; Oakes, M.; Guan, W.; Wyman, J.F.; Rothman, A.J. Older adults’ experiences using a commercially available monitor to self-track their physical activity. JMIR mHealth uHealth 2016, 4, e35. [Google Scholar] [CrossRef]
- Martinez, G.J.; Mattingly, S.M.; Mirjafari, S.; Nepal, S.K.; Campbell, A.T.; Dey, A.K.; Striegel, A.D. On the Quality of Real-world Wearable Data in a Longitudinal Study of Information Workers. In Proceedings of the 2020 IEEE International Conference on Pervasive Computing and Communications Workshops (PerCom Workshops), Austin, TX, USA, 23–27 March 2020; pp. 1–6. [Google Scholar]
- Adam Noah, J.; Spierer, D.K.; Gu, J.; Bronner, S. Comparison of steps and energy expenditure assessment in adults of Fitbit Tracker and Ultra to the Actical and indirect calorimetry. J. Med Eng. Technol. 2013, 37, 456–462. [Google Scholar] [CrossRef]
- Imboden, M.T.; Nelson, M.B.; Kaminsky, L.A.; Montoye, A.H. Comparison of four Fitbit and Jawbone activity monitors with a research-grade ActiGraph accelerometer for estimating physical activity and energy expenditure. Br. J. Sport. Med. 2018, 52, 844–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Camp, C. Accuracy of Predicted Energy Expenditure from a Fitbit Inspire HR Activity Monitor during Short-and Long-Duration Exercise. Master’s Thesis, Eastern Michigan University, Ypsilanti, MI, USA, 2020. [Google Scholar]
- CoME Consortium. Caregiver & ME (CoME): Application for Healthier Self-Management of Seniors. 2017. Available online: http://come-aal.eu/ (accessed on 1 August 2020).
- De Vet, H.; Terwee, C.; Mokkink, L.; Knol, D. Concepts, theories and models, and types of measurements. In Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011; pp. 7–29. [Google Scholar]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Sindi, S.; Kåreholt, I.; Johansson, L.; Skoog, J.; Sjöberg, L.; Wang, H.X.; Johansson, B.; Fratiglioni, L.; Soininen, H.; Solomon, A.; et al. Sleep disturbances and dementia risk: A multicenter study. Alzheimer’s Dement. 2018, 14, 1235–1242. [Google Scholar] [CrossRef]
- Chen, J.C.; Espeland, M.A.; Brunner, R.L.; Lovato, L.C.; Wallace, R.B.; Leng, X.; Phillips, L.S.; Robinson, J.G.; Kotchen, J.M.; Johnson, K.C.; et al. Sleep duration, cognitive decline, and dementia risk in older women. Alzheimer’s Dement. 2016, 12, 21–33. [Google Scholar] [CrossRef]
- Benedict, C.; Byberg, L.; Cedernaes, J.; Hogenkamp, P.S.; Giedratis, V.; Kilander, L.; Lind, L.; Lannfelt, L.; Schiöth, H.B. Self-reported sleep disturbance is associated with Alzheimer’s disease risk in men. Alzheimer’s Dementia 2015, 11, 1090–1097. [Google Scholar] [CrossRef]
- The IPAQ Group. International Physical Activity Questionnaire. 2002. Available online: https://sites.google.com/site/theipaq/ (accessed on 1 August 2020).
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D.; Bridges, K.; Duncan-Jones, P.; Grayson, D. Detecting anxiety and depression in general medical settings. Br. Med. J. 1988, 297, 897–899. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Nestlé Nutrition Institute. Mini Nutritional Assessment (Self MNA®) for Adults 65 Years of Age and Older. 2012. Available online: https://www.mna-elderly.com/ (accessed on 1 August 2020).
- Sunderland, A.; Watts, K.; Baddeley, A.D.; Harris, J.E. Subjective memory assessment and test performance in elderly adults. J. Gerontol. 1986, 41, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-3L. 2020. Available online: https://euroqol.org/eq-5d-instruments/eq-5d-3l-about/ (accessed on 1 August 2020).
- Fitbit, Inc. Fitbit Official Website. 2020. Available online: https://www.fitbit.com/dk/home (accessed on 29 October 2020).
- Garriguet, D.; Tremblay, S.; Colley, R.C. Comparison of physical activity adult questionnaire results with accelerometer data. Health Rep. 2015, 26, 11. [Google Scholar] [PubMed]
- Brewer, W.; Swanson, B.T.; Ortiz, A. Validity of Fitbit’s active minutes as compared with a research-grade accelerometer and self-reported measures. BMJ Open Sport Exerc. Med. 2017, 3, e000254. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Frechette, L.; Miller, D.; Miller, E.; Friel, C.; Van Arsdale, A.; Lin, J.; Shankar, V.; Kuo, D.Y.; Nevadunsky, N.S. Acceptability and feasibility of a Fitbit physical activity monitor for endometrial cancer survivors. Gynecol. Oncol. 2018, 149, 470–475. [Google Scholar] [CrossRef]
- Meyer, J.; von Holdt, K.; Beck, E.; Brandes, M.; Pischke, C.; Voelcker-Rehage, C. Toy or tool? Activity trackers for the assessment of physical activity in the wild. In Proceedings of the 2019 IEEE International Conference on Healthcare Informatics (ICHI), Xi’an, China, 10–13 June 2019; pp. 1–9. [Google Scholar]
- Santomas, K. Passive Monitoring of Physical Activity Using a Fitbit Charge 3 in Individuals at Risk for Depression; Technical Report; University of Massachussetts Lowell: Lowell, MA, USA, 2020. [Google Scholar]
- Troxel, W.M.; Buysse, D.J.; Monk, T.H.; Begley, A.; Hall, M. Does social support differentially affect sleep in older adults with versus without insomnia? J. Psychosom. Res. 2010, 69, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Carlson, J.A.; Sallis, J.F.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Kerr, J.; Cain, K.L.; King, A.C. Interactions between psychosocial and built environment factors in explaining older adults’ physical activity. Prev. Med. 2012, 54, 68–73. [Google Scholar] [CrossRef] [Green Version]
- McMurdo, M.E.; Argo, I.; Crombie, I.K.; Feng, Z.; Sniehotta, F.F.; Vadiveloo, T.; Witham, M.D.; Donnan, P.T. Social, environmental and psychological factors associated with objective physical activity levels in the over 65 s. PLoS ONE 2012, 7, e31878. [Google Scholar] [CrossRef] [Green Version]
- Ho, E.C.; Hawkley, L.; Dale, W.; Waite, L.; Huisingh-Scheetz, M. Social capital predicts accelerometry-measured physical activity among older adults in the US: A cross-sectional study in the National Social Life, Health, and Aging Project. BMC Public Health 2018, 18, 804. [Google Scholar] [CrossRef] [PubMed]
- Arigo, D.; Pasko, K.; Mogle, J.A. Daily relations between social perceptions and physical activity among college women. Psychol. Sport Exerc. 2019, 47, 101528. [Google Scholar] [CrossRef]
- Doryab, A.; Villalba, D.K.; Chikersal, P.; Dutcher, J.M.; Tumminia, M.; Liu, X.; Cohen, S.; Creswell, K.; Mankoff, J.; Creswell, J.D.; et al. Identifying Behavioral Phenotypes of Loneliness and Social Isolation with Passive Sensing: Statistical Analysis, Data Mining and Machine Learning of Smartphone and Fitbit Data. JMIR mHealth uHealth 2019, 7, e13209. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.J.; Remick, R.A.; Davis, J.C.; Vazirian, S.; Khan, K.M. Exercise as medicine—the use of group medical visits to promote physical activity and treat chronic moderate depression: A preliminary 14-week pre–post study. BMJ Open Sport Exerc. Med. 2015, 1, e000036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helgadóttir, B.; Forsell, Y.; Ekblom, Ö. Physical activity patterns of people affected by depressive and anxiety disorders as measured by accelerometers: A cross-sectional study. PLoS ONE 2015, 10, e0115894. [Google Scholar] [CrossRef]
- Liau, A.K.; Neihart, M.; Teo, C.T.; Goh, L.S.; Chew, P. A Quasi-experimental study of a fitbit-based self-regulation intervention to improve physical activity, well-being, and mental health. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Vidal Bustamante, C.M.; Rodman, A.M.; Dennison, M.J.; Flournoy, J.C.; Mair, P.; McLaughlin, K.A. Within-person fluctuations in stressful life events, sleep, and anxiety and depression symptoms during adolescence: A multiwave prospective study. J. Child Psychol. Psychiatry 2020, 61, 1116–1125. [Google Scholar] [CrossRef] [PubMed]
- Falck, R.S.; Landry, G.J.; Best, J.R.; Davis, J.C.; Chiu, B.K.; Liu-Ambrose, T. Cross-sectional relationships of physical activity and sedentary behavior with cognitive function in older adults with probable mild cognitive impairment. Phys. Ther. 2017, 97, 975–984. [Google Scholar] [CrossRef]
- Giannakos, M.N.; Sharma, K.; Papavlasopoulou, S.; Pappas, I.O.; Kostakos, V. Fitbit for learning: Towards capturing the learning experience using wearable sensing. Int. J. Hum. Comput. Stud. 2020, 136, 102384. [Google Scholar] [CrossRef]
- McLaren, B.; Andrews, S.C.; Glikmann-Johnston, Y.; Mercieca, E.C.; Murray, N.W.; Loy, C.; Bellgrove, M.A.; Stout, J.C. Feasibility and initial validation of ‘HD-Mobile’, a smartphone application for remote self-administration of performance-based cognitive measures in Huntington’s disease. J. Neurol. 2020, 1432–1459. [Google Scholar] [CrossRef]
- Sano, A.; Phillips, A.J.; Amy, Z.Y.; McHill, A.W.; Taylor, S.; Jaques, N.; Czeisler, C.A.; Klerman, E.B.; Picard, R.W. Recognizing academic performance, sleep quality, stress level, and mental health using personality traits, wearable sensors and mobile phones. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–6. [Google Scholar]
- Peach, H.D.; Gaultney, J.F.; Ruggiero, A.R. Direct and indirect associations of sleep knowledge and attitudes with objective and subjective sleep duration and quality via sleep hygiene. J. Prim. Prev. 2018, 39, 555–570. [Google Scholar] [CrossRef]
- Thota, D. Evaluating the Relationship Between Fitbit Sleep Data and Self-Reported Mood, Sleep, and Environmental Contextual Factors in Healthy Adults: Pilot Observational Cohort Study. JMIR Form. Res. 2020, 4, e18086. [Google Scholar] [CrossRef]
- Lohne-Seiler, H.; Hansen, B.H.; Kolle, E.; Anderssen, S.A. Accelerometer-determined physical activity and self-reported health in a population of older adults (65–85 years): A cross-sectional study. BMC Public Health 2014, 14, 284. [Google Scholar] [CrossRef] [Green Version]
- Mobbs, R.J.; Phan, K.; Maharaj, M.; Rao, P.J. Physical activity measured with accelerometer and self-rated disability in lumbar spine surgery: A prospective study. Glob. Spine J. 2016, 6, 459–464. [Google Scholar] [CrossRef] [Green Version]
- Gresham, G.; Hendifar, A.E.; Spiegel, B.; Neeman, E.; Tuli, R.; Rimel, B.; Figlin, R.A.; Meinert, C.L.; Piantadosi, S.; Shinde, A.M. Wearable activity monitors to assess performance status and predict clinical outcomes in advanced cancer patients. NPJ Digit. Med. 2018, 1, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, S.; Kanai, M.; Shinoda, T.; Morita, H.; Shimada, S.; Izawa, K.P. Relation between health utility score and physical activity in community-dwelling ambulatory patients with stroke: A preliminary cross-sectional study. Top. Stroke Rehabil. 2018, 25, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Twiggs, J.; Salmon, L.; Kolos, E.; Bogue, E.; Miles, B.; Roe, J. Measurement of physical activity in the pre-and early post-operative period after total knee arthroplasty for Osteoarthritis using a Fitbit Flex device. Med. Eng. Phys. 2018, 51, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Laghouila, S.; Manea, V.; Estrada, V.; Wac, K. Digital Health Tools for Chronic Illness and Dementia Risk Assessment in Older Adults. In Annals of Behavioral Medicine; Oxford Univ Press Inc.: Oxford, UK, 2018; Volume 52, p. S291. [Google Scholar]
- Fitbit, Inc. Fitbit Developer API—Daily Activity Summary; Fitbit, Inc.: San Francisco, CA, USA, 2019. [Google Scholar]
- Rosenberger, M.E.; Fulton, J.E.; Buman, M.P.; Troiano, R.P.; Grandner, M.A.; Buchner, D.M.; Haskell, W.L. The 24-H Activity Cycle: A New Paradigm for Physical Activity. Med. Sci. Sport. Exerc. 2019, 51, 454–464. [Google Scholar] [CrossRef]
- Aitchison, J. The statistical analysis of compositional data. J. R. Stat. Soc. Ser. B Methodol. 1982, 44, 139–160. [Google Scholar] [CrossRef]
- Fitbit, Inc. Fitbit User Forums: Lightly Active vs. Active vs. Very Active; Fitbit, Inc.: San Francisco, CA, USA, 2019. [Google Scholar]
- Fitbit, Inc. Fitbit User Forums: How Activity Categories Are Determined; Fitbit, Inc.: San Francisco, CA, USA, 2019. [Google Scholar]
- Fitbit, Inc. What are Active Minutes? Fitbit, Inc.: San Francisco, CA, USA, 2019. [Google Scholar]
- Smith, G.L.; Banting, L.; Eime, R.; O’Sullivan, G.; Van Uffelen, J.G. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef]
- Spearman, C. The Proof and Measurement of Association between Two Things; Appleton-Century-Crofts: New York, NY, USA, 1961. [Google Scholar]
- The SciPy community. SciPy 1.5.0 Release Notes. 2020. Available online: https://docs.scipy.org/doc/scipy/reference/release.1.5.0.html (accessed on 1 August 2020).
- Wanner, M.; Probst-Hensch, N.; Kriemler, S.; Meier, F.; Autenrieth, C.; Martin, B.W. Validation of the long international physical activity questionnaire: influence of age and language region. Prev. Med. Rep. 2016, 3, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Kent de Grey, R.G.; Uchino, B.N.; Trettevik, R.; Cronan, S.; Hogan, J.N. Social support and sleep: A meta-analysis. Health Psychol. 2018, 37, 787. [Google Scholar] [CrossRef]
- Monroe, C.M.; Thompson, D.L.; Bassett, D.R., Jr.; Fitzhugh, E.C.; Raynor, H.A. Usability of mobile phones in physical activity–related research: A systematic review. Am. J. Health Educ. 2015, 46, 196–206. [Google Scholar] [CrossRef]
- Feng, Y.; Chang, C.K.; Chang, H. An adl recognition system on smart phone. In International Conference on Smart Homes and Health Telematics; Springer: Cham, Switzerland, 2016; pp. 148–158. [Google Scholar]
- Feng, Y.; Chang, C.K.; Ming, H. Recognizing activities of daily living to improve well-being. IT Prof. 2017, 19, 31–37. [Google Scholar] [CrossRef]
- Simon, E.B.; Walker, M.P. Sleep loss causes social withdrawal and loneliness. Nat. Commun. 2018, 9, 1–9. [Google Scholar] [CrossRef]
- Wu, J.; Feng, Y.; Sun, P. Sensor fusion for recognition of activities of daily living. Sensors 2018, 18, 4029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebden, L.; Cook, A.; Van Der Ploeg, H.P.; Allman-Farinelli, M. Development of smartphone applications for nutrition and physical activity behavior change. JMIR Res. Protoc. 2012, 1, e9. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R. Escala de Goldberg. 1993. Available online: http://www.sld.cu/galerias/pdf/sitios/rehabilitacion/goldberg-depresion.pdf (accessed on 1 August 2020).
- EuroQol Research Foundation. Available EQ-5D Versions. 2020. Available online: https://euroqol.org/eq-5d-instruments/all-eq-5d-versions/ (accessed on 1 August 2020).
- Carrasco, P.M.; Peña, M.M.; Sueiro, M.J. The memory failures of everyday questionnaire (MFE): Internal consistency and reliability. Span. J. Psychol. 2012, 15, 768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nestlé Nutrition Institute. Mini Nutritional Assessment (Self MNA®) Para Adultos a Partir de 65 Años. 2012. Available online: https://www.mna-elderly.com/forms/Self-MNA_Spanish.pdf (accessed on 1 August 2020).
- Centro de Investigacion Biomedica en Red. Estudio Predimed. 2020. Available online: http://www.predimed.es/uploads/8/0/5/1/8051451/p14_medas.pdf (accessed on 1 August 2020).
- The IPAQ Group. Cuestionario Internacional de Actividad Fisica. 2002. Available online: https://sites.google.com/site/theipaq/questionnaire_links/IPAQ_Spanish%28USA%29_self-admin_long.pdf (accessed on 1 August 2020).
- Universitat de Barcelona. Indice de calidad de sueño de Pittsburgh. 1998. Available online: http://www.ub.edu/psicobiologia/Pmemlleng/images/Index%20de%20Pittsburgh.pdf (accessed on 1 August 2020).
- American Academy of Pediatrics. Multidimensional Scale of Perceived Social Support (Spanish). 2010. Available online: http://www.heardalliance.org/wp-content/uploads/2011/04/Multidimensional-Scale-of-Perceived-Social-Support-Spanish.pdf (accessed on 1 August 2020).
- Orsolya, P.Z.; Zoltán, K.M.; Szilvia, J. A Multidimenzionális észlelt társas támogatás kérdőív magyar nyelvű validálása. Mentálhigiéné Pszichoszomatika 2017, 18, 230–262. [Google Scholar] [CrossRef]
- The IPAQ Group. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ). 2005. Available online: https://docs.google.com/viewer?a=v&pid=sites&srcid=ZGVmYXVsdGRvbWFpbnx0aGVpcGFxfGd4OjE0NDgxMDk3NDU1YWRlZTM (accessed on 1 August 2020).
- Rasch, G. Probabilistic Models for Some Intelligence and Attainment Tests; ERIC: Washington, DC, USA, 1993.
- Inkin. Wearables: The Comprehensive List of Wearables on the Market. 2020. Available online: https://www.inkin.com/wearables/ (accessed on 29 October 2020).
- United States Food and Drug Administration. FDA Selects Participants for New Digital Health Software Precertification Pilot Program; United States Food and Drug Administration: Silver Spring, MD, USA, 2017.
- Kooiman, T.J.; Dontje, M.L.; Sprenger, S.R.; Krijnen, W.P.; van der Schans, C.P.; de Groot, M. Reliability and validity of ten consumer activity trackers. BMC Sports Sci. Med. Rehabil. 2015, 7, 24. [Google Scholar] [CrossRef] [Green Version]
- Keill, A. Validity of wearable fitness trackers on sleep measure. Med. Sci. Sports Exerc. 2016, 48, 10. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Byun, W.; Keill, A.; Dinkel, D.; Seo, Y. Comparison of Wearable Trackers’ Ability to Estimate Sleep. Int. J. Environ. Res. Public Health 2018, 15, 1265. [Google Scholar] [CrossRef] [Green Version]
- Tedesco, S.; Sica, M.; Ancillao, A.; Timmons, S.; Barton, J.; O’Flynn, B. Validity Evaluation of the Fitbit Charge2 and the Garmin vivosmart HR+ in Free-Living Environments in an Older Adult Cohort. JMIR mHealth uHealth 2019, 7, e13084. [Google Scholar] [CrossRef]
- Paul, S.S.; Tiedemann, A.; Hassett, L.M.; Ramsay, E.; Kirkham, C.; Chagpar, S.; Sherrington, C. Validity of the Fitbit activity tracker for measuring steps in community-dwelling older adults. BMJ Open Sport Exerc. Med. 2015, 1, e000013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooke, J. SUS-A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Steinert, A.; Haesner, M.; Steinhagen-Thiessen, E. Activity-tracking devices for older adults: Comparison and preferences. Univers. Access Inf. Soc. 2018, 17, 411–419. [Google Scholar] [CrossRef]
- Cooper, C.; Gross, A.; Brinkman, C.; Pope, R.; Allen, K.; Hastings, S.; Bogen, B.E.; Goode, A. The impact of wearable motion sensing technology on physical activity in older adults. Exp. Gerontol. 2018, 112, 9–19. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]









| Outcome | PRO: Name | TechRO: Name, Position on Body | Study: Population, Sample, Duration | Co-Calibration: Method | Results | Reference |
|---|---|---|---|---|---|---|
| Physical Activity | International Physical Activity Questionnaire (IPAQ); Physical Activity for Adults Questionnaire (PAAQ) | Actical (research-grade accelerometer), right hip | Individuals, , age range 18–79, mean age 47, 7 days, in the wild | Spearman correlation | PAAQ and IPAQ agreed for moderate and vigorous activity ( = 0.44, = 0.2, respectively). | Garriguet et al. (2015) [36] |
| Physical Activity | International Physical Activity Questionnaire (IPAQ) | Fitbit (consumer wearable), non-dominant arm; ActiGraph GT3X+ (research-grade accelerometer), right waist | Students, , mean age 28.10 ± 9.12, 7 days | Paired t-test, Bland Altman | No significant correlations were found between the IPAQ and the two devices. | Brewer et al. (2017) [37] |
| Physical Activity | Godin Leisure-Time Exercise Questionnaire (GLTEQ) | Fitbit Alta (consumer wearable), wrist | Endometrial cancer survivors, , mean age 62 ± 9, 30 days | U statistic | No significant correlations were found between the GLTEQ and steps. | Rossi et al. (2018) [38] |
| Physical Activity | International Physical Activity Questionnaire (IPAQ) | Fitbit Zip (consumer wearable), wrist; ActiGraph GTX3 (research-grade accelerometer) | Seniors, , age range 62–77, mean age 70.1 ± 3.3), 7 days (ActiGraph, Fitbit), 70 days (study) | Descriptive | IPAQ good for duration of activities but not intensity. | Meyer et al. (2019) [39] |
| Physical Activity | International Physical Activity Questionnaire (IPAQ), Patient Health Questionnaire (PHQ) | Fitbit Charge 3 (consumer wearable), wrist | Individuals with depression, , age range 18–95, mean age 45, 8 weeks | Descriptive | IPAQ score associated with Fitbit steps. | Santomas et al. (2020) [40] |
| Social Support | Pittsburgh Sleep Quality Index (PSQI), Pittsburgh Sleep Diary (PghSD), Interpersonal Support Evaluation List (ISEL), Hamilton Rating Scale for Depression (HRSD), Comorbidity Questionnaire, and others | Actiwatch 64 (accelerometer), wrist | Individuals with and without chronic insomnia, (79 with insomnia), min. age 60, 7 days | Analysis of covariance (ANCOVA), ordinal logistic regression | Social support associated with lower wakefulness after sleep onset for all participants, and shorter sleep latency for those with insomnia. | Troxel et al. (2010) [41] |
| Social Support | Social Support Scale for Exercise Behaviour and others | ActiGraph (accelerometer) | Seniors, , mean age 74.4 ± 6.3, 7 days | Mixed effects regression | Socially supportive environment related to 30 min. to 1 h. of physical activity in participants with positive psycho-social attributes and up to 30 min. for those with less positive psycho-social attributes. | Carlson et al. (2012) [42] |
| Social support | Hospital Anxiety and Depression Score (HADS), Short Form Health Survey (SF-36) | RT3 (accelerometer), waist | Seniors, , mean age 79 ± 8, 7 days | Multiple regression | Number of people nearby to turn to associated with higher physical activity ( = 0.32). | McMurdo et al. (2012) [43] |
| Social support | Custom questionnaire to estimate social networks and social engagement, Center for Epidemiological Studies Depression (CES-D), Montreal Cognitive Assessment (MoCA), and others | Actiwatch Spectrum (accelerometer), non-dominant wrist | Seniors, , mean age 71.9 ± 7.2, 3 days | Multivariate linear regression | Larger social networks (), higher network proportion of friends (), more frequent visiting with neighbors (p < 0.01), and more frequent attendance at organized group meetings () associated with higher physical activity intensity levels. | Ho et al. (2018) [44] |
| Social support | Iowa-Netherlands Comparison Orientation Measure, Rochester Social Comparison Record, and others | Fitbit Flex (consumer wearable), wrist | College women, , mean age 20 ± 1.07, 7 days | Multilevel regression | Increase in negative social interactions (especially with friends) were consistently associated with decreases in daily physical activity with high variability. | Arigo et al. (2019) [45] |
| Social support | University of California Los Angeles Loneliness Questionnaire | Fitbit Flex 2 (consumer wearable), wrist | First-year college students, , 16 weeks (one semester) | Data mining (Apriori), machine learning classification (gradient boosting, logistic regression) | Binary level of loneliness can be detected with 80.2% accuracy. More physical activity and less sedentary behaviour associated with less loneliness. | Doryab et al. (2019) [46] |
| Anxiety and Depression | Patient Health Questionnaire (PHQ-9), Generalised Anxiety Disorder 7-Item Scale (GAD-7), International Physical Activity Questionnaire (IPAQ), Social Support, and others | SenseWear (accelerometer), arm | Individuals with chronic major depressive disorder or a bipolar 2 disorder, , age range 42–72, mean age 54.5 ± 8.7, 7 days (wear), 14 weeks (study) | Wilcoxon signed rank difference test | Physical activity results in an improvement in anxiety and depression in patients with chronic depression (median depression score decreased 38%, p < 0.05). | Adams et al., 2015 [47] |
| Anxiety and Depression | Patient Health Questionnaire (PHQ-9), Mini International Neuropsychiatric Interview (MINI), Montgomery-ÅDepression Rating Scale (MADRS) | ActiGraph GT3X+ (accelerometer) | Anxiety and depression patients, , age range 18–65, mean age 41.8 ± 11.6, 7 days | Analysis of variance (ANOVA), analysis of covariance (ANCOVA), paired t-tests | No significant results; depressed participants tended to be less active at light intensity ( = , p < 0.01). | Helgadóttir et al. (2015) [48] |
| Anxiety and Depression | Depression Anxiety Stress Scale (DASS) | Fitbit (consumer wearable), wrist | University students and staff, , mean age 22 ± 3, 3 weeks | Analysis of variance (ANOVA) | An increase in steps correlated with a decrease in depression for female participants. | Liau et al. (2018) [49] |
| Anxiety and Depression | University of California Los Angeles Life Stress Interview (LSI), Generalized Anxiety Disorder 7-Item Scale (GAD-7), Patient Health Questionnaire (PHQ-9) | Fitbit Charge 2 (consumer wearable), wrist | Female adolescents, N = 30, mean age 16.4 ± 0.8, 1 year, mean wear 7 months | Pearson correlation, Bayesian multilevel models | Within-person fluctuations in stressful life events were associated with variability in sleep duration (r = 0.48, p < 0.05). Within-person increases in sleep duration variability correlated with greater depression symptoms ( = 0.38, p < 0.05) while sleep regularity correlated with lesser depression (, p < 0.05). | Vidal Bustamante et al. (2020) [50] |
| Memory | Montreal Cognitive Assessment (MoCA), Alzheimer Disease Assessment Scale-Cognitive-Plus (ADAS-Cog Plus) | MotionWatch 8 (accelerometer), wrist | N = 151, min. age 55, mean age 71.1 ± 7.2, 5 days | Paired t-test, analysis of covariance (ANCOVA), multiple linear regression | Participants with probable mild cognitive impairment were less active and more sedentary, better ADAS-Cog Plus performance correlates with more physical activity and less sedentary behavior. | Falck et al. (2017) [51] |
| Memory | Self-reported learning experience (satisfaction, usefulness, and performance) | Empatica E4 (accelerometer), non-dominant wrist | College students, , age range 21–53, mean age 24 ± 5.9, 35 min | Machine learning (random forest, support vector machine with 3 separate kernels) | Students’ perceived learning can be predicted accurately from the physiological data (89% accuracy). | Giannakos et al. (2020) [52] |
| Memory | Enroll-HD cognitive battery | Fitbit (consumer wearable) | Individuals with Huntington’s disease, (20 healthy controls), 3 uses across 8 days | Correlation tests | Medium to strong correlations between motor symptoms and cognitive tasks (r = –0.54). | McLaren et al. (2020) [53] |
| Sleep | Pittsburgh Sleep Quality Index (PSQI), Perceived Stress Scale (PSS), Short Form Health Survey (SF-12) | Q-sensor (accelerometer), dominant hand | Undergraduate students, , mean age 20.1 ± 1.5, 30 days | Machine learning (classification, support vector machine with 2 separate kernels) | Skin conductance, skin temperature, and acceleration classified poor/good sleep with 80–90% accuracy. | Sano et al. (2015) [54] |
| Sleep | Pittsburgh Sleep Quality Index (PSQI), Charlotte Attitudes Towards Sleep Scale (CATS), Sleep Hygiene Practice Scale (SHPS), and others | Fitbit Flex (consumer wearable), wrist | College students, , age range 18–38, mean age 20.3 ± 2.5, 7 days | Path model, Spearman correlation | Correlations between sleep duration from PSQI and Fitbit ( = 0.33, p < 0.01). | Peach et al. (2018) [55] |
| Sleep | Pittsburgh Sleep Quality Index (PSQI) | Fitbit Flex 2 (consumer wearable), wrist | Military individuals, , 2 weeks | Wilcoxon signed rank difference test, Spearman rank correlation test | Moderate correlation between PSQI and Fitbit sleep durations ( = 0.643, p = 0.005). Top contextual factors disrupting sleep were pain, noises, and worrying. | Thota et al. (2020) [56] |
| Quality of Life | Self-reported health scale (5 levels) | ActiGraph GT1M (accelerometer) | Seniors, , age range 65–85, mean age 71.6 ± 5.6, 7 days | Analysis of variance (ANOVA) | 51% higher physical activity level was registered in those with very good health compared to those with poor and very poor health. | Lohne-Seiler et al. (2014) [57] |
| Quality of Life | Short Form Health Survey (SF-12), Oswestry Disability Index (ODI) | Fitbit Zip (consumer wearable) | Lumbar spine surgery patients, , mean age 42.6 ± 10.3, 7 days (pre-operatory wear), 6 months (post-operatory wear) | Paired t-test, Pearson correlation | No significant correlation between the improvement in steps () or distance traveled per day (). | Mobbs et al. (2015) [58] |
| Quality of Life | Eastern Cooperative Oncology Group Performance Status (ECOG-PS), Karnofsky Performance Status (KPS), Patient-Reported Outcomes Measurement Information System (NIH PROMIS) | Fitbit Charge HR (consumer wearable), wrist | Advanced cancer patients, , age range 34–81, median age 62, 2 weeks | Spearman correlation, Kaplan-Meier curves, multivariate proportional hazards | Correlations were observed between average daily steps and ECOG-PS (, p < 0.05) and KPS ( = 0.69). Correlations were also observed between distance and ECOG-PS () and KPS (). | Gresham et al. (2018) [59] |
| Quality of Life | EuroQoL with 5 Dimensions and 3 Levels (EQ-5D-3L) | Fitbit One (consumer wearable), belt | Stroke patients, , mean age 69.5, 7 days | Correlation tests | Quality of Life health score correlates with the number of steps (r = 0.46, p < 0.03). | Sasaki et al. (2018) [60] |
| Quality of Life | Short Form Health Survey (SF-12), Knee Injury and Osteoarthritis Outcome Score (KOOS) | Fitbit Flex (consumer wearable), non-dominant wrist | Knee arthroplasty patients, , mean age 67 ± 13, 7 days for 3 times points (2 weeks before surgery, day after surgery, and 2 weeks after surgery) | Multiple linear regression, Spearman rank correlation | Significant correlations of SF-12 (physical component summary) and post-operative step count ( = 0.521, p < 0.05). | Twiggs et al. (2018) [61] |
| Outcome | Scale | Item Variables | Score Variables | Total |
|---|---|---|---|---|
| Physical Activity | International Physical Activity Questionnaire (IPAQ) [26] | 15: 11 for the combinations of domains and intensities, 4 for the domain totals | 8: 4 for the domain numeric scores, 3 for the intensity numeric scores, and 1 for the overall numeric score | 23 |
| Social Support | Multi-Dimensional Scale Perceived Social Support (MSPSS) [27] | 12 for the items | 5: 3 for the numeric sub-scores and 2 for the numeric and categorical scores | 17 |
| Anxiety and Depression | Goldberg depression and anxiety scale (GADS) [28] | 18 for the items | 2 for the numeric and categorical scores | 20 |
| Nutrition Mediterranean | Prevention with Mediterranean Diet (PREDIMED) [29,30] | 14 for the items | 2 for the numeric and categorical scores | 16 |
| Nutrition | Self-Reported Mini Nutritional Assessment (SelfMNA) [31] | 5 for the items | 2 for the numeric and categorical scores | 7 |
| Memory | Memory Failures of Everyday (MFE) [32] | 28 for the items | 2 for the numeric and categorical scores | 30 |
| Sleep | Pittsburgh Sleep Quality Index (PSQI) [33] | 18 for the items | 10: 8 for the sub-scores and 2 for the numeric and categorical scores | 28 |
| Health-Related Quality of Life | EuroQoL health questionnaire (EQ-5D-3L) [34] | 6 for the items | 0 (the scores coincide with the items) | 6 |
| Amount | Family | Outcome | Variable | Unit |
|---|---|---|---|---|
| Absolute | Raw | Energy | Median count over 7 days | kcal. |
| Median count over 14 days | ||||
| Median count over 21 days | ||||
| Median count over 28 days | ||||
| Median count over 60 days | ||||
| Median count over 90 days | ||||
| Median count over 120 days | ||||
| Steps | Median count over [...] days | count | ||
| Heart rate | Median beats over [...] days | bpm. | ||
| Processed | Sedentary | Median duration over [...] days | min. | |
| Sedentary+Light | Median duration over [...] days | |||
| Light | Median duration over [...] days | |||
| Light+Fair | Median duration over [...] days | |||
| Fair | Median duration over [...] days | |||
| Fair+Vigorous | Median duration over [...] days | |||
| Vigorous | Median duration over [...] days | |||
| Active | Median duration over [...] days | |||
| Sleep | Median duration over [...] days | |||
| Relative | CLR PA | Sedentary | Geometric mean over [...] days | - |
| Light | Geometric mean over [...] days | |||
| Fair | Geometric mean over [...] days | |||
| Vigorous | Geometric mean over [...] days | |||
| CLR PA+S | Sedentary | Geometric mean over [...] days | ||
| Light | Geometric mean over [...] days | |||
| Fair | Geometric mean over [...] days | |||
| Vigorous | Geometric mean over [...] days | |||
| Sleep | Geometric mean over [...] days |
| Variables | Mean (SD) or n [%] | Variables | Mean (SD) or n [%] | ||
|---|---|---|---|---|---|
| Spain | Hungary | Spain | Hungary | ||
| Count | 26 [66.7%] | 13 [33.3%] | Health status | ||
| Age | 69.2 (±5.7) | 71.5 (±9.1) | Healthy | 18 [46.2%] | 10 [25.6%] |
| Gender | Diseased | 8 [20.5%] | 3 [7.7%] | ||
| Women | 15 [38.5%] | 7 [17.9%] | Smoking | ||
| Men | 11 [28.2%] | 6 [15.4%] | Yes | 5 [12.8%] | 1 [2.6%] |
| Education | No | 21 [53.8%] | 12 [30.8%] | ||
| Primary | 7 [17.9%] | 0 [0.0%] | Alcohol | ||
| Secondary | 5 [12.8%] | 3 [7.7%] | Never | 10 [25.6%] | 4 [10.3%] |
| High school | 5 [12.8%] | 1 [2.6%] | Monthly | 5 [12.8%] | 5 [12.8%] |
| University | 9 [23.1%] | 9 [23.1%] | Weekly | 7 [17.9%] | 1 [2.6%] |
| Living | Few days | 1 [2.6%] | 2 [5.1%] | ||
| Alone | 11 [28.2%] | 3 [7.7%] | Daily | 3 [7.7%] | 1 [2.6%] |
| +Partner | 14 [35.9%] | 10 [25.6%] | Systolic blood pressure | 146.2 (±63.2) | 124.7 (±15.0) |
| +Children | 1 [2.6%] | 0 [0.0%] | Body mass index | 25.5 (±4.64) | 28.5 (±4.1) |
| Wave 1 | Wave 2 | Wave 3 | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PID | Health | Country | Gender | Age | Physical Activity (IPAQ) | Social Support (MSPSS) | Anxiety and Depression (GADS) | Mediterranean Nutrition (PREDIMED) | Nutrition (SelfMNA) | Memory (MFW) | Sleep (PSQI) | Quality of Life (EQ-5D-3L) | Physical Activity (IPAQ) | Social Support (MSPSS) | Anxiety and Depression (GADS) | Mediterranean Nutrition (PREDIMED) | Nutrition (SelfMNA) | Memory (MFW) | Sleep (PSQI) | Quality of Life (EQ-5D-3L) | Physical Activity (IPAQ) | Social Support (MSPSS) | Anxiety and Depression (GADS) | Mediterranean Nutrition (PREDIMED) | Nutrition (SelfMNA) | Memory (MFE) | Sleep (PSQI) | Quality of Life (EQ-5D-3L) | ||||
| 575 | Healthy | Hungary | Female | 65 | • | • | • | • | • | • | ||||||||||||||||||||||
| 569 | Healthy | Hungary | Female | 67 | • | • | • | • | • | • | • | • | • | • | • | • | • | • | ||||||||||||||
| 133 | Healthy | Hungary | Female | 71 | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | ||||||||||||
| 420 | Healthy | Hungary | Female | 71 | • | • | • | • | • | • | • | • | • | • | • | |||||||||||||||||
| 215 | Healthy | Hungary | Female | 87 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 576 | Healthy | Hungary | Male | 60 | • | • | • | |||||||||||||||||||||||||
| 535 | Healthy | Hungary | Male | 69 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 170 | Healthy | Hungary | Male | 70 | • | • | • | • | • | • | • | • | • | • | ||||||||||||||||||
| 212 | Healthy | Hungary | Male | 72 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 419 | Healthy | Hungary | Male | 95 | • | • | • | • | • | • | • | • | • | • | ||||||||||||||||||
| 643 | Healthy | Spain | Female | 67 | • | • | • | • | • | • | • | • | • | • | • | • | • | |||||||||||||||
| 798 | Healthy | Spain | Female | 67 | • | • | ||||||||||||||||||||||||||
| 803 | Healthy | Spain | Female | 67 | • | • | ||||||||||||||||||||||||||
| 617 | Healthy | Spain | Female | 69 | • | • | • | • | • | • | • | • | • | • | ||||||||||||||||||
| 620 | Healthy | Spain | Female | 69 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 640 | Healthy | Spain | Female | 69 | • | • | • | • | • | • | ||||||||||||||||||||||
| 628 | Healthy | Spain | Female | 70 | • | • | • | • | • | • | ||||||||||||||||||||||
| 638 | Healthy | Spain | Female | 71 | • | • | • | • | • | • | • | • | • | |||||||||||||||||||
| 648 | Healthy | Spain | Female | 72 | • | • | • | • | • | • | • | |||||||||||||||||||||
| 649 | Healthy | Spain | Female | 72 | • | • | ||||||||||||||||||||||||||
| 795 | Healthy | Spain | Female | 72 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 630 | Healthy | Spain | Female | 74 | • | • | • | • | • | • | ||||||||||||||||||||||
| 411 | Healthy | Spain | Male | 45 | • | • | ||||||||||||||||||||||||||
| 790 | Healthy | Spain | Male | 66 | • | • | • | • | • | • | • | • | ||||||||||||||||||||
| 700 | Healthy | Spain | Male | 67 | • | • | • | • | • | • | ||||||||||||||||||||||
| 636 | Healthy | Spain | Male | 68 | • | • | • | • | • | |||||||||||||||||||||||
| 793 | Healthy | Spain | Male | 68 | • | • | • | |||||||||||||||||||||||||
| 796 | Healthy | Spain | Male | 74 | • | • | • | • | • | • | • | |||||||||||||||||||||
| 502 | Diseased | Hungary | Female | 63 | • | |||||||||||||||||||||||||||
| 169 | Diseased | Hungary | Female | 69 | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | • | ||||||
| 132 | Diseased | Hungary | Male | 71 | • | • | • | • | • | • | • | • | • | • | • | • | • | |||||||||||||||
| 800 | Diseased | Spain | Female | 65 | • | • | • | • | • | • | • | |||||||||||||||||||||
| 641 | Diseased | Spain | Female | 71 | • | • | • | • | • | • | • | • | • | • | • | • | ||||||||||||||||
| 624 | Diseased | Spain | Female | 72 | • | • | • | • | • | • | ||||||||||||||||||||||
| 644 | Diseased | Spain | Male | 70 | • | • | ||||||||||||||||||||||||||
| 625 | Diseased | Spain | Male | 72 | • | • | • | • | • | • | ||||||||||||||||||||||
| 634 | Diseased | Spain | Male | 72 | • | • | • | • | • | • | ||||||||||||||||||||||
| 791 | Diseased | Spain | Male | 72 | • | • | • | |||||||||||||||||||||||||
| 799 | Diseased | Spain | Male | 79 | • | • | • | • | • | • | • | |||||||||||||||||||||
| Outcome | PRO | Health | PRO | TechRO Families | ||||
|---|---|---|---|---|---|---|---|---|
| Item/Sub-Score/Score | Raw | Processed | CLR PA | CLR PA+S | All | |||
| Physical activity | IPAQ | All | Domestic moderate activity | 4 | 2 | 2 | 8 | |
| Physical activity | IPAQ | All | Domestic+garden total activiy | 3 | 2 | 3 | 8 | |
| Physical activity | IPAQ | All | Garden moderate activity | 4 | 2 | 1 | 7 | |
| Physical activity | IPAQ | All | Leisure moderate activity | 1 | 3 | 2 | 1 | 7 |
| Physical activity | IPAQ | Healthy | Domestic moderate activity | 2 | 4 | 3 | 2 | 11 |
| Physical activity | IPAQ | Healthy | Garden moderate activity | 6 | 4 | 10 | ||
| Physical activity | IPAQ | Diseased | Garden vigorous activity | 1 | 6 | 3 | 2 | 12 |
| Physical activity | IPAQ | Diseased | Leisure vigorous activity | 2 | 6 | 2 | 2 | 12 |
| Physical activity | IPAQ | Diseased | Work vigorous activity | 1 | 5 | 3 | 2 | 11 |
| Physical activity | IPAQ | Diseased | Work moderate activity | 2 | 5 | 1 | 2 | 10 |
| Social support | MSPSS | All | Q8: family talks about problems | 4 | 3 | 3 | 10 | |
| Social support | MSPSS | All | Q11: family willing to help make decisions | 1 | 5 | 2 | 2 | 10 |
| Social support | MSPSS | Healthy | Q3: family tries to help | 1 | 6 | 3 | 4 | 14 |
| Social support | MSPSS | Healthy | Q6: friends try to help | 1 | 7 | 2 | 4 | 14 |
| Social support | MSPSS | Healthy | Q9: friends share joys and sorrows | 1 | 6 | 2 | 4 | 13 |
| Social support | MSPSS | Healthy | Q12: friends talk problems | 1 | 7 | 2 | 3 | 13 |
| Social support | MSPSS | Healthy | Q10: special person cares about feelings | 7 | 1 | 4 | 12 | |
| Social support | MSPSS | Healthy | Friends numeric sub-score | 1 | 6 | 2 | 3 | 12 |
| Social support | MSPSS | Diseased | Q2: special person shares joys and sorrows | 1 | 5 | 6 | ||
| Social support | MSPSS | Diseased | Significant other numeric sub-score | 1 | 4 | 1 | 6 | |
| Anxiety and depression | GADS | All | Q6D: lost weight due to poor appetite | 5 | 3 | 4 | 12 | |
| Anxiety and depression | GADS | All | Q8A: worried about own health | 4 | 4 | 2 | 10 | |
| Anxiety and depression | GADS | All | Q1D: lacking energy | 3 | 3 | 4 | 10 | |
| Anxiety and depression | GADS | Healthy | Q2D: lost interest in things | 6 | 3 | 3 | 12 | |
| Anxiety and depression | GADS | Diseased | Q2A: worrying a lot | 2 | 6 | 2 | 1 | 11 |
| Mediterranean nutrition | PREDIMED | All | Categorical score | 2 | 4 | 3 | 1 | 10 |
| Mediterranean nutrition | PREDIMED | All | Numeric score | 1 | 3 | 4 | 1 | 9 |
| Mediterranean nutrition | PREDIMED | All | Q12: nuts use | 2 | 2 | 1 | 2 | 7 |
| Mediterranean nutrition | PREDIMED | All | Q14: sofrito use | 2 | 5 | 7 | ||
| Mediterranean nutrition | PREDIMED | Healthy | Q4: fruit use | 1 | 3 | 2 | 1 | 7 |
| Mediterranean nutrition | PREDIMED | Healthy | Categorical score | 2 | 2 | 2 | 6 | |
| Nutrition | SelfMNA | All | Categorical score | 2 | 2 | 2 | 6 | |
| Nutrition | SelfMNA | Healthy | Categorical score | 1 | 2 | 2 | 5 | |
| Nutrition | SelfMNA | Diseased | Q2: weight lost | 1 | 3 | 1 | 2 | 7 |
| Nutrition | SelfMNA | Diseased | Q1: food intake declined | 1 | 2 | 1 | 2 | 6 |
| Memory | MFE | All | Q12: having difficulty picking up a new skill | 6 | 1 | 4 | 11 | |
| Memory | MFE | All | Q14: forgetting to do planned things | 5 | 2 | 3 | 10 | |
| Memory | MFE | All | Q6: forgetting time of events | 4 | 3 | 2 | 9 | |
| Memory | MFE | Healthy | Q6: forgetting time of events | 1 | 7 | 3 | 3 | 14 |
| Memory | MFE | Healthy | Q15: forgetting details of done things | 7 | 2 | 4 | 13 | |
| Memory | MFE | Healthy | Q12: having difficulty picking up a new skill | 6 | 3 | 3 | 12 | |
| Memory | MFE | Healthy | Q14: forgetting to do planned things | 1 | 6 | 2 | 3 | 12 |
| Memory | MFE | Diseased | Q13: having a word on the tip of the tongue | 1 | 7 | 3 | 2 | 13 |
| Memory | MFE | Diseased | Q25: getting lost in often visited place | 7 | 3 | 2 | 12 | |
| Sleep | PSQI | All | Q7: trouble staying awake driving, eating, socializing | 2 | 5 | 4 | 3 | 14 |
| Sleep | PSQI | All | Q4: duration of actual sleep | 1 | 5 | 3 | 2 | 11 |
| Sleep | PSQI | All | Daily dysfunction numeric sub-score | 1 | 4 | 3 | 2 | 10 |
| Sleep | PSQI | Healthy | Q4: duration of actual sleep | 1 | 5 | 3 | 2 | 11 |
| Sleep | PSQI | Healthy | Q5C: trouble sleeping due to using the bathroom | 4 | 4 | 2 | 10 | |
| Sleep | PSQI | Healthy | Q7: trouble staying awake driving, eating, socializing | 2 | 5 | 3 | 10 | |
| Sleep | PSQI | Healthy | Daily dysfunction numeric sub-score | 2 | 3 | 3 | 1 | 9 |
| Sleep | PSQI | Diseased | Daily dysfunction numeric sub-score | 2 | 4 | 1 | 7 | |
| Sleep | PSQI | Diseased | Q6: duration of actual sleep | 4 | 2 | 6 | ||
| Quality of Life | EQ-5D-3L | All | Q6: health state today | 4 | 1 | 3 | 8 | |
| Quality of Life | EQ-5D-3L | All | Q4: pain/discomfort | 2 | 1 | 3 | 6 | |
| Quality of Life | EQ-5D-3L | Healthy | Q4: pain/discomfort | 4 | 2 | 1 | 7 | |
| Quality of Life | EQ-5D-3L | Diseased | Q5: anxiety/depression | 2 | 3 | 5 | ||
| PRO | TechRO | Correlation/Contour | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Health | Domain | Variable | Amount | Family | Variable | Lower | Higher | |||
| All | Work | Vigorous activity | Absolute | Processed | Active | +0.8 | ||||
| All | Domestic | Moderate activity | Absolute | Processed | Light+fair | +0.7 | +0.8 | × | ||
| Healthy | Work | Moderate activity | Absolute | Processed | Fair | × | × | |||
| Healthy | Work | Total activity | Absolute | Processed | Fair | × | × | |||
| Diseased | Work | Walking activity | Relative | CLR PA | Light | × | ||||
| Diseased | Work | Moderate activity | Absolute | Processed | Fair | × | +0.8 | +0.7 | +0.7 | |
| Diseased | Work | Moderate activity | Relative | CLR PA | Sedentary | × | ||||
| Diseased | Work | Vigorous activity | Relative | CLR PA | Light | |||||
| Diseased | Garden | Vigorous activity | Relative | CLR PA | Light | |||||
| Diseased | Garden | Vigorous activity | Relative | CLR PA+S | Sedentary | |||||
| Diseased | Leisure | Walking activity | Absolute | Raw | Energy | +0.8 | ||||
| Diseased | Leisure | Walking activity | Absolute | Raw | Steps | +0.8 | ||||
| Diseased | Leisure | Vigorous activity | Absolute | Processed | Fair+Vigorous | × | +0.8 | +0.6 | ||
| Diseased | Leisure | Vigorous activity | Relative | CLR PA | Sedentary | −0.8 | × | |||
| Diseased | Leisure | Vigorous activity | Relative | CLR PA | Vigorous | × | +0.8 | |||
| Diseased | Leisure | Vigorous activity | Relative | CLR PA+S | Light | × | ||||
| Diseased | Leisure | Total activity | Absolute | Processed | Sedentary+light | × | ||||
| PRO | TechRO | Correlation/Contour | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Health | Source | Variable | Amount | Family | Variable | Lower | Higher | |||
| All | Significant other | Q2: shares joys and sorrows | Relative | CLR PA+S | Vigorous | +0.3 | +0.7 | +0.8 | ||
| All | Significant other | Q5: a real source of comfort | Relative | CLR PA+S | Vigorous | +0.4 | +0.7 | +0.8 | ||
| All | Significant other | Q10: cares about feelings | Relative | CLR PA+S | Vigorous | +0.5 | +0.7 | +0.8 | ||
| All | Family | Q3: tries to help | Relative | CLR PA+S | Fair | +0.3 | +0.8 | +0.7 | ||
| All | Family | Q8: talks about problems | Relative | CLR PA+S | Fair | +0.6 | +0.8 | +0.8 | ||
| All | Family | Q8: talks about problems | Relative | CLR PA+S | Vigorous | +0.6 | +0.8 | +0.8 | ||
| All | Family | Numeric sub-score | Relative | CLR PA+S | Fair | +0.3 | +0.8 | × | ||
| Healthy | Significant other | Q1: around when in need | Absolute | Processed | Fair | × | ||||
| Healthy | Significant other | Q2: shares joys and sorrows | Absolute | Processed | Fair | × | ||||
| Healthy | Significant other | Q5: a real source of comfort | Absolute | Processed | Fair | × | ||||
| Healthy | Significant other | Q5: a real source of comfort | Relative | CLR PA+S | Fair | +0.4 | +0.8 | +0.6 | ||
| Healthy | Significant other | Q10: cares about feelings | Absolute | Processed | Fair | × | ||||
| Healthy | Significant other | Numeric sub-score | Absolute | Processed | Fair | × | ||||
| Healthy | Family | Q3: tries to help | Absolute | Processed | Fair | × | ||||
| Healthy | Family | Q3: tries to help | Relative | CLR PA+S | Fair | +0.5 | +0.5 | +0.9 | +0.6 | |
| Healthy | Family | Q8: talks about problems | Absolute | Processed | Fair | × | ||||
| Healthy | Family | Q8: talks about problems | Relative | CLR PA+S | Fair | +0.6 | +0.5 | +0.8 | +0.6 | |
| Healthy | Family | Q11: willing to help make decisions | Relative | CLR PA | Fair | +0.4 | +0.8 | × | ||
| Healthy | Family | Numeric sub-score | Relative | CLR PA+S | Fair | +0.5 | +0.4 | +0.8 | +0.4 | |
| Healthy | Friends | Q9: share joys and sorrows | Absolute | Processed | Light | × | +0.8 | +0.7 | + 0.4 | |
| Healthy | Friends | Q12: talk about problems | Absolute | Processed | Light | × | +0.8 | +0.7 | ||
| Healthy | All | Categorical score | Absolute | Processed | Active | +0.8 | ||||
| Healthy | All | Categorical score | Relative | CLR PA | Light | × | +0.8 | × | ||
| Healthy | All | Numeric score | Absolute | Processed | Light+Fair | +0.7 | +0.8 | × | ||
| Healthy | All | Numeric score | Relative | CLR PA+S | Fair | +0.6 | +0.5 | +0.8 | +0.4 | |
| Diseased | Family | Q4: gives emotional help and support | Absolute | Processed | Sedentary | × | ||||
| Diseased | Friends | Q12: talk about problems | Absolute | Raw | Steps | +0.8 | ||||
| PRO | TechRO | Correlation/Contour | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Health | Outcome | Variable | Amount | Family | Variable | Lower | Higher | ||
| All | Anxiety | Q3A: irritable | Relative | CLR PA | Vigorous | × | +0.8 | ||
| All | Anxiety | Q5A: sleeping poorly | Relative | CLR PA+S | Light | +0.5 | +0.8 | +0.5 | +0.3 |
| All | Anxiety | Q7A: trembling | Absolute | Processed | Active | ||||
| All | Depression | Q1D: lacking energy | Relative | CLR PA+S | Vigorous | × | |||
| All | Depression | Q6D: lost weight due to poor appetite | Relative | CLR PA+S | Light | × | +0.8 | × | |
| All | Both | Numeric score | Relative | CLR PA+S | Sleep | +0.8 | |||
| Healthy | Anxiety | Q3A: irritable | Absolute | Processed | Active | ||||
| Healthy | Anxiety | Q7A: trembling | Absolute | Processed | Light+fair | ||||
| Healthy | Anxiety | Q7A: trembling | Absolute | Processed | Vigorous | × | +0.8 | ||
| Healthy | Anxiety | Q7A: trembling | Absolute | Processed | Active | ||||
| Healthy | Anxiety | Q7A: trembling | Relative | CLR PA | Light | × | × | ||
| Healthy | Anxiety | Q7A: trembling | Relative | CLR PA+S | Vigorous | × | +0.8 | ||
| Healthy | Depression | Q2D: lost interest in things | Relative | CLR PA | Light | × | × | ||
| Healthy | Depression | Q6D: lost weight due to poor appetite | Relative | CLR PA+S | Sleep | +0.8 | |||
| Healthy | Depression | Q9D: worse in the morning | Relative | CLR PA+S | Sedentary | +0.8 | × | ||
| PRO | TechRO | Correlation/Contour | |||||
|---|---|---|---|---|---|---|---|
| Health | Variable | Amount | Family | Variable | Lower | Higher | |
| All | Q12: nuts use | Absolute | Processed | Fair | × | × | |
| All | Q12: nuts use | Relative | CLR PA+S | Light | +0.6 | +0.8 | × |
| All | Numeric score | Absolute | Processed | Vigorous | |||
| All | Numeric score | Relative | CLR PA+S | Light | +0.6 | +0.8 | +0.6 |
| Healthy | Q3: vegetables use | Relative | CLR PA | Fair | × | × | |
| Healthy | Q3: vegetables use | Relative | CLR PA+S | Fair | × | ||
| Diseased | Q5: red meat, hamburger, or meat use | Absolute | Raw | Energy | +0.8 | ||
| Diseased | Q11: commercial sweets or pastries use | Absolute | Raw | Heart rate | +0.8 | ||
| PRO | TechRO | Correlation/Contour | |||||
|---|---|---|---|---|---|---|---|
| Health | Variable | Amount | Family | Variable | Lower | Higher | |
| Diseased | Q1: food intake declined | Relative | CLR PA+S | Sleep | |||
| Diseased | Q2: weight lost | Relative | CLR PA+S | Sleep | |||
| Diseased | Q4: stressed or severely ill | Absolute | Processed | Sedentary | × | ||
| PRO | TechRO | Correlation/Contour | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Health | Variable | Amount | Family | Variable | Lower | Higher | |||
| All | Q7: completely forgetting to take things | Relative | CLR PA+S | Sleep | +0.8 | ||||
| All | Q12: having difficulty picking up a new skill | Relative | CLR PA+S | Light | × | × | |||
| All | Q13: finding a word on the tip of the tongue | Relative | CLR PA+S | Sleep | +0.8 | ||||
| All | Q24: forgetting where things are normally kept | Relative | CLR PA | Fair | × | +0.8 | × | ||
| All | Q24: forgetting where things are normally kept | Relative | CLR PA+S | Fair | × | ||||
| All | Numeric score | Absolute | Processed | Active | |||||
| Healthy | Q7: completely forgetting to take things | Relative | CLR PA+S | Sleep | +0.8 | ||||
| Healthy | Q10: letting ramble about unimportant things | Absolute | Processed | Light+fair | × | × | |||
| Healthy | Q14: forgetting to do planned things | Absolute | Processed | Fair+vigorous | × | +0.8 | +0.8 | ||
| Healthy | Q14: forgetting to do planned things | Absolute | Processed | Vigorous | +0.8 | +0.8 | |||
| Healthy | Q16: forgetting the topic of an ongoing conversation | Absolute | Processed | Fair | × | ||||
| Healthy | Q24: forgetting where things are normally kept | Relative | CLR PA+S | Fair | × | × | |||
| Healthy | Numeric score | Relative | CLR PA | Fair | × | × | |||
| Diseased | Q1: forgetting objects put | Relative | CLR PA+S | Vigorous | |||||
| Diseased | Q6: forgetting the time of events | Absolute | Raw | Heart rate | +0.8 | ||||
| Diseased | Q6: forgetting the time of events | Absolute | Processed | Light | +0.7 | +0.8 | × | ||
| Diseased | Q6: forgetting the time of events | Absolute | Processed | Sleep | |||||
| Diseased | Q8: being reminded about things | Absolute | Processed | Light+fair | +0.6 | +0.8 | × | ||
| Diseased | Q9: reading anew something already read | Absolute | Processed | Sleep | |||||
| Diseased | Q13: finding a word on the tip of the tongue | Absolute | Processed | Active | |||||
| Diseased | Q13: finding a word on the tip of the tongue | Relative | CLR PA+S | Sedentary | +0.8 | +0.7 | |||
| Diseased | Q18: forgetting to tell somebody something important | Absolute | Processed | Fair | × | ||||
| Diseased | Q18: forgetting to tell somebody something important | Absolute | Processed | Fair+vigorous | |||||
| Diseased | Q18: forgetting to tell somebody something important | Absolute | Processed | Vigorous | |||||
| Diseased | Numeric score | Absolute | Processed | Active | |||||
| PRO | TechRO | Correlation/Contour | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Health | Variable | Amount | Family | Variable | Lower | Higher | |||
| All | Q5A: trouble sleeping due to not getting to sleep | Relative | CLR PA+S | Sleep | +0.8 | ||||
| All | Q5E: trouble sleeping due to coughing or snoring loudly | Relative | CLR PA | Vigorous | |||||
| All | Q5F: trouble sleeping due to feeling too cold | Relative | CLR PA+S | Light | +0.6 | +0.8 | +0.6 | ||
| All | Q7: trouble staying awake while driving, eating, socializing | Relative | CLR PA | Light | × | ||||
| All | Q7: trouble staying awake while driving, eating, socializing | Relative | CLR PA+S | Sleep | |||||
| All | Latency numeric sub-score | Relative | CLR PA+S | Sleep | +0.8 | ||||
| All | Efficiency numeric sub-score | Relative | CLR PA | Fair | × | +0.8 | × | ||
| All | Daily dysfunction numeric sub-score | Absolute | Processed | Vigorous | +0.5 | +0.5 | +0.8 | ||
| All | Daily dysfunction numeric sub-score | Relative | CLR PA | Light | × | ||||
| All | Daily dysfunction numeric sub-score | Relative | CLR PA+S | Sleep | |||||
| Healthy | Q2: duration taken to fall asleep | Relative | CLR PA+S | Sleep | +0.8 | ||||
| Healthy | Q3: time gotten up in the morning | Absolute | Raw | Energy | |||||
| Healthy | Q5A: trouble sleeping due to not getting to sleep | Relative | CLR PA+S | Sleep | +0.8 | ||||
| Healthy | Q5B: trouble sleeping due to waking up in the middle of the night | Relative | CLR PA+S | Vigorous | × | +0.8 | |||
| Healthy | Q5C: trouble sleeping due to using the bathroom | Absolute | Processed | Light+Fair | × | ||||
| Healthy | Q5C: trouble sleeping due to using the bathroom | Relative | CLR PA | Light | × | ||||
| Healthy | Q5E: trouble sleeping due to coughing or snoring loudly | Relative | CLR PA+S | Light | × | × | |||
| Healthy | Q11: duration stayed in bed | Relative | CLR PA+S | Sleep | +0.8 | ||||
| Healthy | Numeric score | Absolute | Processed | Fair+vigorous | × | +0.8 | +0.6 | ||
| Healthy | Latency numeric sub-score | Relative | CLR PA+S | Sleep | +0.8 | ||||
| Healthy | Efficiency numeric sub-score | Relative | CLR PA | Fair | × | +0.8 | × | ||
| Diseased | Q1: time gone to bed at night | Absolute | Processed | Sleep | |||||
| Diseased | Q4: duration of actual sleep | Absolute | Processed | Fair | × | +0.8 | +0.8 | +0.9 | |
| Diseased | Q4: duration of actual sleep | Absolute | Processed | Fair+vigorous | +0.8 | +0.8 | +0.9 | ||
| Diseased | Q4: duration of actual sleep | Absolute | Processed | Vigorous | +0.8 | +0.8 | +0.9 | ||
| Diseased | Q5B: trouble sleeping due to waking up in the middle of the night | Absolute | Raw | Energy | |||||
| Diseased | Q5C: trouble sleeping due to using the bathroom | Absolute | Raw | Energy | |||||
| PRO | TechRO | Correlation/Contour | ||||||
|---|---|---|---|---|---|---|---|---|
| Health | Domain | Variable | Amount | Family | Variable | Lower | Higher | |
| Diseased | Anxiety/depression | Q5: anxiety/depression | Absolute | Processed | Sedentary | +0.8 | × | |
| 7 | 14 | 21 | 28 | 60 | 90 | 120 | |
|---|---|---|---|---|---|---|---|
| 0 | |||||||
| 7 | |||||||
| 14 | |||||||
| 21 | |||||||
| 28 | |||||||
| 60 | |||||||
| 90 | |||||||
| 120 |
| Participant ID | Wave | Q3 (PRO) | Fair (TechRO) |
|---|---|---|---|
| 617 | 2 | 4 | |
| 419 | 1 | 5 | |
| 419 | 2 | 5 | |
| 643 | 2 | 6 | |
| 793 | 3 | 6 | +1.05 |
| 170 | 3 | 6 | +1.49 |
| 569 | 1 | 7 | +2.10 |
| 133 | 2 | 7 | +1.73 |
| 569 | 2 | 7 | +2.09 |
| 133 | 3 | 7 | +1.69 |
| 569 | 3 | 7 | +1.88 |
| ID | Health | Wave | Country | Gender | Age | Physical Activity (IPAQ): Numeric Score | Social Support (MSPSS): Numeric Score | Depression and Anxiety (GADS): Numeric Score | Nutrition Mediterranean (PREDIMED): Numeric Score | Nutrition (SelfMNA): Numeric Score | Memory (MFE): Numeric Score | Sleep (PSQI): Numeric Score | Quality of Life (EQ-5D-3L): Health Score | TechRO: Energy (Kcal.) | TechRO: Steps (count) | TechRO: Heart Rate (bpm.) | TechRO: Sedentary (min.) | TechRO: Sedentary+Light (min.) | TechRO: Light (min.) | TechRO: Light+Fair (min.) | Fair (min.) | TechRO: Fair+Vigorous (min.) | TechRO: Vigorous (min.) | TechRO: Active (min.) | TechRO: Sleep (h:min.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 169 | Diseased | 1 | Hungary | Female | 69 | 5 | 68 | 7 | 12 | 13 | 15 | 80 | 2044.0 | 8035.0 | 52.5 | 842.0 | 999.0 | 192.5 | 253.0 | 23.0 | 51.0 | 19.0 | 300.0 | 7:06 | |
| 169 | Diseased | 2 | Hungary | Female | 69 | 7338 | 5 | 51 | 5 | 15 | 15 | 75 | 1889.0 | 6076.0 | 56.0 | 843.0 | 994.0 | 207.0 | 245.0 | 21.0 | 51.5 | 22.5 | 273.5 | 7:08 | |
| 169 | Diseased | 3 | Hungary | Female | 69 | 21,702 | 5 | 47 | 7 | 12 | 8 | 14 | 80 | 1979.0 | 8172.0 | 55.0 | 798.0 | 975.0 | 204.0 | 248.0 | 40.0 | 70.0 | 33.0 | 294.0 | 7:03 |
| Median | 14,520.0 | 5.0 | 51.0 | 7.0 | 12.0 | 13.0 | 15.0 | 80.0 | 1979.0 | 8035.0 | 55.0 | 842.0 | 994.0 | 204.0 | 248.0 | 23.0 | 51.5 | 22.5 | 294.0 | 7:06 | |||||
| Mean | 14,520.0 | 5.0 | 55.3 | 6.3 | 12.0 | 12.0 | 14.7 | 78.3 | 1970.7 | 7427.7 | 54.5 | 827.7 | 989.3 | 201.2 | 248.7 | 28.0 | 57.5 | 24.8 | 289.2 | 7:05 | |||||
| SD | 10,156.9 | 0 | 11.2 | 1.2 | 0.0 | 3.6 | 0.6 | 2.9 | 77.8 | 1172.6 | 1.8 | 25.7 | 12.7 | 7.7 | 4.0 | 10.4 | 10.8 | 7.3 | 13.9 | 0:03 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manea, V.; Wac, K. Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method. J. Pers. Med. 2020, 10, 203. https://doi.org/10.3390/jpm10040203
Manea V, Wac K. Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method. Journal of Personalized Medicine. 2020; 10(4):203. https://doi.org/10.3390/jpm10040203
Chicago/Turabian StyleManea, Vlad, and Katarzyna Wac. 2020. "Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method" Journal of Personalized Medicine 10, no. 4: 203. https://doi.org/10.3390/jpm10040203
APA StyleManea, V., & Wac, K. (2020). Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method. Journal of Personalized Medicine, 10(4), 203. https://doi.org/10.3390/jpm10040203