
Dementia Risk among Coronavirus Disease Survivors: A Nationwide Cohort Study in South Korea

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Concerns
2.2. Data Source (NHIS-COVID-19 DB)
2.3. Management of COVID-19 Patients in South Korea
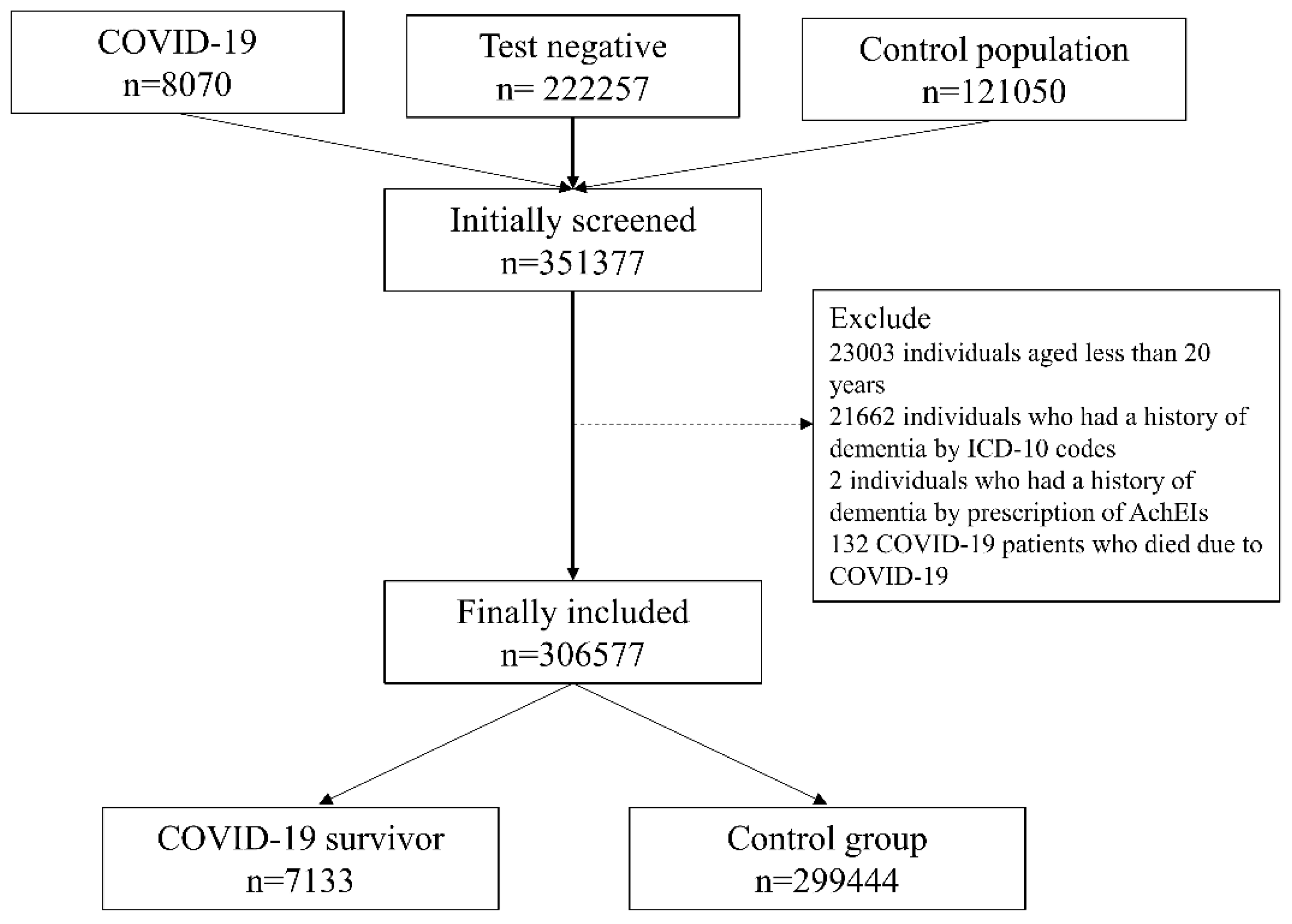
2.4. COVID-19 Survivors and the Control Group (Adults Who Did Not Contract COVID-19)
2.5. Endpoint: Development of Dementia
2.6. Measurement of Confounders
2.7. Statistical Methodology
3. Results
3.1. Main Analyses
3.2. Sensitivity Analysis after Excluding Test-Negative Individuals
3.3. Specific Type of Dementia
3.4. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.-D.; Schuchat, A.J.T.L. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Coronavirus COVID. Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). 2020. Available online: https://www.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6 (accessed on 30 March 2021).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernan, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Jacobs, L.G.; Gourna Paleoudis, E.; Lesky-Di Bari, D.; Nyirenda, T.; Friedman, T.; Gupta, A.; Rasouli, L.; Zetkulic, M.; Balani, B.; Ogedegbe, C.; et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS ONE 2020, 15, e0243882. [Google Scholar] [CrossRef] [PubMed]
- Valent, A.; Dudoignon, E.; Ressaire, Q.; Depret, F.; Plaud, B. Three-month quality of life in survivors of ARDS due to COVID-19: A preliminary report from a French academic centre. Anaesth. Crit. Care Pain Med. 2020, 39, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Wolters, F.J.; Ikram, M.A. Epidemiology of Dementia: The Burden on Society, the Challenges for Research. Methods Mol. Biol. 2018, 1750, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Natoli, S.; Oliveira, V.; Calabresi, P.; Maia, L.F.; Pisani, A. Does SARS-Cov-2 invade the brain? Translational lessons from animal models. Eur. J. Neurol. 2020, 27, 1764–1773. [Google Scholar] [CrossRef]
- Siddiqui, R.; Mungroo, M.R.; Khan, N.A. SARS-CoV-2 invasion of the central nervous: A brief review. Hosp. Pract. 2021, 49, 157–163. [Google Scholar] [CrossRef]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Butler, M.; Pollak, T.A.; Rooney, A.G.; Michael, B.D.; Nicholson, T.R. Neuropsychiatric complications of covid-19. BMJ 2020, 371, m3871. [Google Scholar] [CrossRef]
- Wang, Q.; Davis, P.B.; Gurney, M.E.; Xu, R. COVID-19 and dementia: Analyses of risk, disparity, and outcomes from electronic health records in the US. Alzheimers Dement. 2021, 17, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.M.; Kim, J.H.; Park, J.S.; Chang, M.C.; Park, D. Neurological diseases as mortality predictive factors for patients with COVID-19: A retrospective cohort study. Neurol. Sci. 2020, 41, 2317–2324. [Google Scholar] [CrossRef] [PubMed]
- Heneka, M.T.; Golenbock, D.; Latz, E.; Morgan, D.; Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimers Res. Ther. 2020, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Mendez, R.; Balanza-Martinez, V.; Luperdi, S.C.; Estrada, I.; Latorre, A.; Gonzalez-Jimenez, P.; Feced, L.; Bouzas, L.; Yepez, K.; Ferrando, A.; et al. Short-term neuropsychiatric outcomes and quality of life in COVID-19 survivors. J. Intern. Med. 2021, 290, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Nannoni, S.; de Groot, R.; Bell, S.; Markus, H.S. Stroke in COVID-19: A systematic review and meta-analysis. Int. J. Stroke 2021, 16, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Kuzma, E.; Lourida, I.; Moore, S.F.; Levine, D.A.; Ukoumunne, O.C.; Llewellyn, D.J. Stroke and dementia risk: A systematic review and meta-analysis. Alzheimers Dement. 2018, 14, 1416–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Parsons, V.L. Stratified sampling. Wiley StatsRef Stat. Ref. Online 2014, 1–11. [Google Scholar] [CrossRef]
- Dighe, A.; Cattarino, L.; Cuomo-Dannenburg, G.; Skarp, J.; Imai, N.; Bhatia, S.; Gaythorpe, K.A.M.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med. 2020, 18, 321. [Google Scholar] [CrossRef]
- Shapiro, E.G.; Klein, K.A. Dementia in childhood: Issues in neuropsychological assessment with application to the natural history and treatment of degenerative storage diseases. In Advances in Child Neuropsychology; Springer: New York, NY, USA, 1994; pp. 119–171. [Google Scholar]
- McGleenon, B.M.; Dynan, K.B.; Passmore, A.P. Acetylcholinesterase inhibitors in Alzheimer’s disease. Br. J. Clin. Pharmacol. 1999, 48, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Rafferty, L.A.; Cawkill, P.E.; Stevelink, S.A.M.; Greenberg, K.; Greenberg, N. Dementia, post-traumatic stress disorder and major depressive disorder: A review of the mental health risk factors for dementia in the military veteran population. Psychol. Med. 2018, 48, 1400–1409. [Google Scholar] [CrossRef]
- Kanji, J.N.; Zelyas, N.; MacDonald, C.; Pabbaraju, K.; Khan, M.N.; Prasad, A.; Hu, J.; Diggle, M.; Berenger, B.M.; Tipples, G. False negative rate of COVID-19 PCR testing: A discordant testing analysis. Virol. J. 2021, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Peters, R.; Booth, A.; Rockwood, K.; Peters, J.; D’Este, C.; Anstey, K.J. Combining modifiable risk factors and risk of dementia: A systematic review and meta-analysis. BMJ Open 2019, 9, e022846. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.M.; Chopra, T.; Korzeniewski, S.J.; Levy, P. COVID-19 as a risk factor for Alzheimer’s disease and related dementia: A perspective from Detroit, MI. Psychiatry Res. 2020, 294, 113557. [Google Scholar] [CrossRef] [PubMed]
- Iwashyna, T.J.; Ely, E.W.; Smith, D.M.; Langa, K.M. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 2010, 304, 1787–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amruta, N.; Chastain, W.H.; Paz, M.; Solch, R.J.; Murray-Brown, I.C.; Befeler, J.B.; Gressett, T.E.; Longo, M.T.; Engler-Chiurazzi, E.B.; Bix, G. SARS-CoV-2 mediated neuroinflammation and the impact of COVID-19 in neurological disorders. Cytokine Growth Factor Rev. 2021, 1–15. [Google Scholar] [CrossRef]
- Zhou, Z.; Kang, H.; Li, S.; Zhao, X. Understanding the neurotropic characteristics of SARS-CoV-2: From neurological manifestations of COVID-19 to potential neurotropic mechanisms. J. Neurol. 2020, 267, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Siu, K.L.; Yuen, K.S.; Castano-Rodriguez, C.; Ye, Z.W.; Yeung, M.L.; Fung, S.Y.; Yuan, S.; Chan, C.P.; Yuen, K.Y.; Enjuanes, L.; et al. Severe acute respiratory syndrome coronavirus ORF3a protein activates the NLRP3 inflammasome by promoting TRAF3-dependent ubiquitination of ASC. FASEB J. 2019, 33, 8865–8877. [Google Scholar] [CrossRef]
- Tejera, D.; Mercan, D.; Sanchez-Caro, J.M.; Hanan, M.; Greenberg, D.; Soreq, H.; Latz, E.; Golenbock, D.; Heneka, M.T. Systemic inflammation impairs microglial Abeta clearance through NLRP3 inflammasome. EMBO J. 2019, 38, e101064. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.; Atluri, V.; Kaushik, A.; Yndart, A.; Nair, M. Alzheimer’s disease: Pathogenesis, diagnostics, and therapeutics. Int. J. Nanomed. 2019, 14, 5541–5554. [Google Scholar] [CrossRef] [Green Version]
- Heneka, M.T.; Kummer, M.P.; Stutz, A.; Delekate, A.; Schwartz, S.; Vieira-Saecker, A.; Griep, A.; Axt, D.; Remus, A.; Tzeng, T.C.; et al. NLRP3 is activated in Alzheimer’s disease and contributes to pathology in APP/PS1 mice. Nature 2013, 493, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Sasannejad, C.; Ely, E.W.; Lahiri, S. Long-term cognitive impairment after acute respiratory distress syndrome: A review of clinical impact and pathophysiological mechanisms. Crit. Care 2019, 23, 352. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-Term Respiratory and Neurological Sequelae of COVID-19. Med. Sci. Monit. 2020, 26, e928996. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Anstey, K.J.; Ee, N.; Eramudugolla, R.; Jagger, C.; Peters, R. A Systematic Review of Meta-Analyses that Evaluate Risk Factors for Dementia to Evaluate the Quantity, Quality, and Global Representativeness of Evidence. J. Alzheimers Dis. 2019, 70, S165–S186. [Google Scholar] [CrossRef] [Green Version]
- Lu, Z.K.; Li, M.; Yuan, J.; Wu, J. The role of cerebrovascular disease and the association between diabetes mellitus and dementia among aged medicare beneficiaries. Int. J. Geriatr. Psychiatry 2016, 31, 92–98. [Google Scholar] [CrossRef]
- Park, S.Y.; Choi, G.; Lee, H.; Kim, N.Y.; Lee, S.Y.; Kim, K.; Shin, S.; Jang, E.; Moon, Y.; Oh, K.; et al. Early Intervention Reduces the Spread of COVID-19 in Long-Term Care Facilities in the Republic of Korea. Osong Public Health Res. Perspect. 2020, 11, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Zhou, R.; Zhong, T.; Li, R.; Tan, J.; Zhou, H. Association of smoking and alcohol drinking with dementia risk among elderly men in China. Curr. Alzheimer Res. 2014, 11, 899–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | COVID-19 Survivor n = 7133 | Control Group n = 299,444 | p-Value | |
|---|---|---|---|---|
| Sex: male | 2813 (39.4) | 134,007 (44.8) | <0.001 | |
| Age | <0.001 | |||
| 20–29 | 2057 (28.8) | 68,314 (22.8) | ||
| 30–39 | 829 (11.6) | 50,378 (16.8) | ||
| 40–49 | 1030 (14.4) | 46,706 (15.6) | ||
| 50–59 | 1523 (21.4) | 51,882 (17.3) | ||
| 60–69 | 1103 (15.5) | 41,702 (13.9) | ||
| 70–79 | 467 (6.5) | 25,380 (8.5) | ||
| ≥80 | 124 (1.7) | 15,082 (5.0) | ||
| Residence in 2020 | <0.001 | |||
| Seoul | 500 (7.0) | 49,906 (16.7) | ||
| Gyeonggido | 407 (5.7) | 53,104 (17.7) | ||
| Daegu | 4673 (65.5) | 92,507 (30.9) | ||
| Gyeongsangbukdo | 790 (11.1) | 24,119 (8.1) | ||
| Other area | 763 (10.7) | 79,808 (26.7) | ||
| Annual income level in 2020 | <0.001 | |||
| Q1 (lowest) | 2204 (30.9) | 67,301 (22.5) | ||
| Q2 | 1390 (19.35) | 60,106 (20.1) | ||
| Q3 | 1467 (20.6) | 73,800 (24.6) | ||
| Q4 | 1960 (27.5) | 93,035 (31.1) | ||
| Unknown | 112 (1.6) | 5202 (1.7) | ||
| Charlson comorbidity index | 2.3 (2.3) | 3.0 (3.0) | <0.001 | |
| Myocardial infarction | 158 (2.2) | 9114 (3.0) | <0.001 | |
| Congestive heart failure | 324 (4.5) | 26,841 (9.0) | <0.001 | |
| Peripheral vascular disease | 1050 (14.7) | 53,536 (17.9) | <0.001 | |
| Cerebrovascular disease | 599 (8.4) | 34,785 (11.6) | <0.001 | |
| Chronic pulmonary disease | 3565 (50.0) | 170,197 (56.8) | <0.001 | |
| Rheumatic disease | 657 (9.2) | 31,154 (10.4) | 0.001 | |
| Peptic ulcer disease | 2848 (39.9) | 137,331 (45.9) | <0.001 | |
| Mild liver disease | 2960 (41.5) | 134,913 (45.1) | <0.001 | |
| DM without chronic complication | 1522 (21.3) | 79,194 (26.4) | <0.001 | |
| DM with chronic complication | 429 (6.0) | 25,168 (8.4) | <0.001 | |
| Hemiplegia or paraplegia | 67 (0.9) | 3572 (1.2) | 0.051 | |
| Renal disease | 131 (1.8) | 12,355 (4.1) | <0.001 | |
| Any malignancy | 510 (7.1) | 42,191 (14.1) | <0.001 | |
| Moderate or severe liver disease | 24 (0.3) | 2576 (0.9) | <0.001 | |
| Metastatic solid tumour | 58 (0.8) | 8228 (2.7) | <0.001 | |
| AIDS/HIV | 7 (0.1) | 551 (0.2) | 0.093 | |
| Intracranial Injury | 4 (0.1) | 437 (0.1) | 0.069 | |
| Thyroid disorder | 2310 (32.4) | 108,355 (36.2) | <0.001 | |
| Underlying psychiatric illness | ||||
| Anxiety disorder | 1461 (20.5) | 72,405 (24.2) | <0.001 | |
| Substance abuse | 96 (1.3) | 5091 (1.7) | 0.022 | |
| Depression | 971 (13.6) | 49,016 (16.4) | <0.001 | |
| PTSD | 11 (0.2) | 520 (0.2) | 0.696 | |
| Hospital admission in 2020 | 797 (11.2) | 38,745 (12.9) | <0.001 | |
| Supplemental Oxygen therapy | 758 (10.6) | 37,036 (12.4) | <0.001 | |
| Mechanical ventilator support | 72 (1.0) | 5359 (1.8) | <0.001 | |
| ICU admission in 2020 | 162 (2.3) | 11,814 (3.9) | <0.001 | |
| Development of dementia | 49 (0.7) | 3497 (1.2) | <0.001 | |
| Alzheimer’s dementia | 36 (0.5) | 2632 (0.9) | 0.001 | |
| Vascular dementia | 5 (0.1) | 321 (0.1) | 0.342 | |
| Other dementia | 17 (0.2) | 969 (0.3) | 0.209 | |
| Variable | Cox Regression Analysis | p-Value | |
|---|---|---|---|
| HR (95% CI) | |||
| Unadjusted (univariable analysis) | |||
| COVID-19 survivors (vs. Control group) | 0.59 (0.44, 0.78) | <0.001 | |
| Covariates-adjusted model 1 (multivariable analysis) | |||
| COVID-19 survivors (vs. Control group) | 1.39 (1.05, 1.85) | 0.023 | |
| Covariates-adjusted model 2 (multivariable analysis) | |||
| Control group (n = 299,444) | 1 | ||
| COVID-19 survivors without hospitalization (n = 6336) | 1.28 (0.89, 1.84) | 0.185 | |
| COVID-19 survivors with hospitalization (n = 797) | 1.62 (1.03, 2.54) | 0.038 | |
| Covariates-adjusted model 3 (multivariable analysis) | |||
| Control group (n = 299,444) | 1 | ||
| COVID-19 survivors without oxygen therapy (n = 6375) | 1.31 (0.92, 1.87) | 0.139 | |
| COVID-19 survivors with oxygen therapy (n = 758) | 1.56 (1.02, 2.48) | 0.042 | |
| Covariates-adjusted model 4 (multivariable analysis) | |||
| Duration of isolation due to COVID-19, day | 1.01 (1.00, 1.02) | 0.011 | |
| Variable | Cox Regressuib Analysis | p-Value | |
|---|---|---|---|
| HR (95% CI) | |||
| Covariates-adjusted model 1 (multivariable analysis) | |||
| Control group | 1 | ||
| COVID-19 survivors | 3.30 (2.43, 4.47) | <0.001 | |
| Covariates-adjusted model 2 (multivariable analysis) | |||
| Control group (n = 299,444) | 1 | ||
| COVID-19 survivors without hospitalization (n = 6336) | 3.09 (2.11, 4.52) | <0.001 | |
| COVID-19 survivors with hospitalization (n = 797) | 3.68 (2.31, 5.88) | <0.001 | |
| Covariates-adjusted model 3 (multivariable analysis) | |||
| Control group (n = 299,444) | 1 | ||
| COVID-19 survivors without oxygen therapy (n = 6375) | 3.17 (2.18, 4.62) | <0.001 | |
| COVID-19 survivors with oxygen therapy (n = 758) | 3.53 (2.19, 5.71) | <0.001 | |
| Covariates-adjusted model 4 (multivariable analysis) | |||
| Duration of isolation due to COVID-19, day | 1.03 (1.02, 1.03) | <0.001 | |
| Variable | Multivariable Model | p-Value | |
|---|---|---|---|
| HR (95% CI) | |||
| Alzheimer’s dementia | |||
| COVID-19 survivors (vs. control group) | 1.32 (1.05, 1.86) | 0.028 | |
| Vascular dementia | |||
| COVID-19 survivors (vs. control group) | 1.51 (0.62, 3.70) | 0.364 | |
| Other dementia | |||
| COVID-19 survivors (vs. control group) | 2.04 (1.25, 3.32) | 0.004 | |
| Variable | Dementia Event (%) | Multivariable Model | p-Value | |
|---|---|---|---|---|
| HR (95% CI) | ||||
| Male (n = 136,820) | ||||
| Control group | 1687 (1.3) | 1 | ||
| COVID-19 survivors | 19 (0.7) | 1.23 (0.78, 1.94) | 0.376 | |
| Female (n = 169,757) | ||||
| Control group | 1809 (1.1) | 1 | ||
| COVID-19 survivors | 30 (0.7) | 1.56 (1.08, 2.25) | 0.017 | |
| Age: 20–59 (n = 222,719) | ||||
| Control group | 248 (0.1) | 1 | ||
| COVID-19 survivors | 6 (0.1) | 1.72 (0.76, 3.92) | 0.197 | |
| Age: ≥ 60 (n = 83,858) | ||||
| Control group | 3248 (4.0) | 1 | ||
| COVID-19 survivors | 43 (2.5) | 1.38 (1.02, 1.87) | 0.039 | |
| CCI: 0–2 (n = 173,189) | ||||
| Control group | 541 (0.3) | 1 | ||
| COVID-19 survivors | 11 (0.2) | 1.38 (0.76, 2.54) | 0.293 | |
| CCI: ≥ 3 (n = 133,388) | ||||
| Control group | 2955 (2.3) | 1 | ||
| COVID-19 survivors | 38 (1.5) | 1.42 (1.00, 1.91) | 0.048 | |
| Underlying anxiety disorder (n = 73,866) | ||||
| Control group | 1701 (2.3) | 1 | ||
| COVID-19 survivors | 19 (1.3) | 1.10 (0.70, 1.73) | 0.690 | |
| Underlying depression group (n = 49,987) | ||||
| Control group | 1264 (2.6) | 1 | ||
| COVID-19 survivors | 19 (2.0) | 1.48 (0.94, 2.35) | 0.094 | |
| Underlying PTSD group (n = 531) | ||||
| Control group | 5 (1.0) | 1 | ||
| COVID-19 survivors | 0 (0.0) | 0.00 (0.00) | 0.824 | |
| Underlying substance abuse (n = 5187) | ||||
| Control group | 113 (2.2) | 1 | ||
| COVID-19 survivors | 3 (3.1) | 1.77 (0.52, 5.97) | 0.358 | |
| Underlying diabetes group (n = 84,807) | ||||
| Control group | 2319 (2.8) | 1 | ||
| COVID-19 survivors | 31 (1.9) | 1.52 (1.06, 2.18/) | 0.022 | |
| Underlying CVD group (n = 35,385) | ||||
| Control group | 1468 (4.2) | 1 | ||
| COVID-19 survivors | 21 (3.5) | 1.64 (1.06, 2.54) | 0.024 | |
| After excluding 8 patients in the control group, who were diagnosed as COVID-19 from 4 June 2020 to 1 December 2020 | ||||
| Control group | 3496 (1.2) | 1 | ||
| COVID-19 survivors | 49 (0.7) | 1.39 (1.04, 1.85) | 0.024 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-Y.; Song, I.-A.; Oh, T.-K. Dementia Risk among Coronavirus Disease Survivors: A Nationwide Cohort Study in South Korea. J. Pers. Med. 2021, 11, 1015. https://doi.org/10.3390/jpm11101015
Park H-Y, Song I-A, Oh T-K. Dementia Risk among Coronavirus Disease Survivors: A Nationwide Cohort Study in South Korea. Journal of Personalized Medicine. 2021; 11(10):1015. https://doi.org/10.3390/jpm11101015
Chicago/Turabian StylePark, Hye-Yoon, In-Ae Song, and Tak-Kyu Oh. 2021. "Dementia Risk among Coronavirus Disease Survivors: A Nationwide Cohort Study in South Korea" Journal of Personalized Medicine 11, no. 10: 1015. https://doi.org/10.3390/jpm11101015
APA StylePark, H. -Y., Song, I. -A., & Oh, T. -K. (2021). Dementia Risk among Coronavirus Disease Survivors: A Nationwide Cohort Study in South Korea. Journal of Personalized Medicine, 11(10), 1015. https://doi.org/10.3390/jpm11101015