
Determinants of Longitudinal Change of Lung Function in Different Gender in a Large Taiwanese Population Follow-Up Study Categories: Original Investigation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
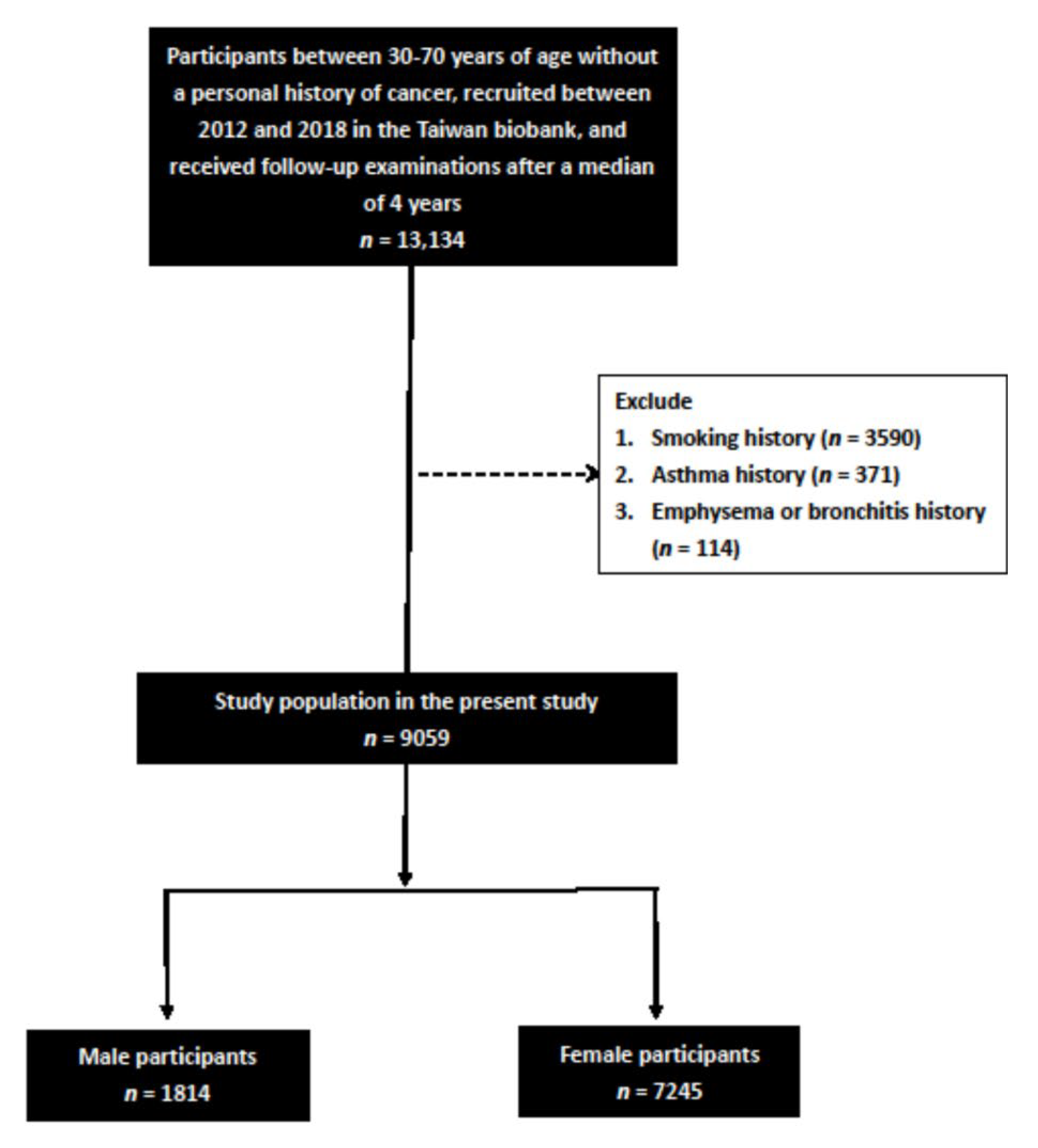
2.2. TWB
2.3. Laboratory, Medical Demographic Data
2.4. Spirometry Measurements
2.5. Statistical Analysis
3. Results
3.1. Comparisons of the Clinical Characteristics between the Male and Female Participants
3.2. Determinants of ΔFEV1/FVC Using Multivariable Linear Regression Analysis
3.3. Determinants of ΔFEV1/FVC in the Male and Female Participants Using Multivariable Linear Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jakovljevic, M.; Jakab, M.; Gerdtham, U.; McDaid, D.; Ogura, S.; Varavikova, E.; Merrick, J.; Adany, R.; Okunade, A.; Getzen, T.E. Comparative financing analysis and political economy of noncommunicable diseases. J. Med. Econ. 2019, 22, 722–727. [Google Scholar] [CrossRef]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Timofeyev, Y.; Ekkert, N.V.; Fedorova, J.V.; Skvirskaya, G.; Bolevich, S.; Reshetnikov, V.A. The impact of health expenditures on public health in BRICS nations. J. Sport Health Sci. 2019, 8, 516–519. [Google Scholar] [CrossRef]
- Hamlin, C.R.; Kohn, R.R. Determination of human chronological age by study of a collagen sample. Exp. Gerontol. 1972, 7, 377–379. [Google Scholar] [CrossRef]
- John, R.; Thomas, J. Chemical compositions of elastins isolated from aortas and pulmonary tissues of humans of different ages. Biochem. J. 1972, 127, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Mittman, C.; Edelman, N.H.; Norris, A.H.; Shock, N.W. Relationship between chest wall and pulmonary compliance and age. J. Appl. Physiol. 1965, 20, 1211–1216. [Google Scholar] [CrossRef]
- Sharma, G.; Goodwin, J. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 2006, 1, 253. [Google Scholar] [CrossRef]
- Villar, T.; Dow, L. Lung function and aging: The development and decline of lung function in health and disease. Rev. Clin. Gerontol. 1992, 2, 279–297. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 5 September 2021).
- Hsieh, M.-J.; Huang, S.-Y.; Yang, T.-M.; Tao, C.-W.; Cheng, S.-L.; Lee, C.-H.; Kuo, P.-H.; Wu, Y.-K.; Chen, N.-H.; Hsu, W.-H. The impact of 2011 and 2017 Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) guidelines on allocation and pharmacological management of patients with COPD in Taiwan: Taiwan Obstructive Lung Disease (TOLD) study. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2949. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.L.; Harrison, S.L.; Goldstein, R.S.; Brooks, D. Pain and its clinical associations in individuals with COPD: A systematic review. Chest 2015, 147, 1246–1258. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.-s.; DeGuzman, B.; Kramer, T.; Group, M.S. Reversal of COPD-associated weight loss using the anabolic agent oxandrolone. Chest 2002, 122, 421–428. [Google Scholar] [CrossRef] [Green Version]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef]
- Cheng, Y.-J.; Chen, Z.-G.; Li, Z.-Y.; Mei, W.-Y.; Bi, W.-T.; Luo, D.-L. Longitudinal change in lung function and subsequent risks of cardiovascular events: Evidence from four prospective cohort studies. BMC Med. 2021, 19, 153. [Google Scholar] [CrossRef]
- Cavaillès, A.; Brinchault-Rabin, G.; Dixmier, A.; Goupil, F.; Gut-Gobert, C.; Marchand-Adam, S.; Meurice, J.C.; Morel, H.; Person-Tacnet, C.; Leroyer, C.; et al. Comorbidities of COPD. Eur. Respir. Rev. 2013, 22, 454–475. [Google Scholar] [CrossRef]
- Bolton, C.; Evans, M.; Ionescu, A.; Edwards, S.; Morris, R.; Dunseath, G.; Luzio, S.; Owens, D.; Shale, D. Insulin resistance and inflammation—a further systemic complication of COPD. COPD J. Chronic Obstr. Pulm. Dis. 2007, 4, 121–126. [Google Scholar] [CrossRef]
- Rabe, K.F.; Hurd, S.; Anzueto, A.; Barnes, P.J.; Buist, S.A.; Calverley, P.; Fukuchi, Y.; Jenkins, C.; Rodriguez-Roisin, R.; Van Weel, C. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2007, 176, 532–555. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Davis, K.J. Lung function decline and outcomes in an elderly population. Thorax 2006, 61, 472–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Padilla, R.; Fernandez-Plata, R.; Montes de Oca, M.; Lopez-Varela, M.V.; Jardim, J.R.; Muiño, A.; Valdivia, G.; Menezes, A.M.B.; PLATINO Group. Lung function decline in subjects with and without COPD in a population-based cohort in Latin-America. PLoS ONE 2017, 12, e0177032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.T.; Guppy, M.; Straus, S.E.; Bell, K.J.L.; Glasziou, P. Rate of normal lung function decline in ageing adults: A systematic review of prospective cohort studies. BMJ Open 2019, 9, e028150. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-H.; Park, S.; Shin, Y.-H.; Kim, M.-Y.; Lee, Y.-J. Sex differences in the relationship between metabolic syndrome and pulmonary function: The 2007 Korean National Health and Nutrition Examination Survey. Endocr. J. 2011, 58, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Yang, J.H.; Chiang, C.W.K.; Hsiung, C.N.; Wu, P.E.; Chang, L.C.; Chu, H.W.; Chang, J.; Song, I.W.; Yang, S.L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet. 2016, 25, 5321–5331. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.T.; Hung, T.H.; Yeh, C.K. Taiwan Regulation of Biobanks. J. Law Med. Ethics 2015, 43, 816–826. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enright, P.L.; Kronmal, R.A.; Manolio, T.A.; Schenker, M.B.; Hyatt, R.E. Respiratory muscle strength in the elderly. Correlates and reference values. Cardiovascular Health Study Research Group. Am. J. Respir. Crit. Care Med. 1994, 149, 430–438. [Google Scholar] [CrossRef]
- Triebner, K.; Accordini, S.; Calciano, L.; Johannessen, A.; Benediktsdóttir, B.; Bifulco, E.; Demoly, P.; Dharmage, S.C.; Franklin, K.A.; Garcia-Aymerich, J. Exogenous female sex steroids may reduce lung ageing after menopause: A 20-year follow-up study of a general population sample (ECRHS). Maturitas 2019, 120, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Straub, R.H. The complex role of estrogens in inflammation. Endocr. Rev. 2007, 28, 521–574. [Google Scholar] [CrossRef] [Green Version]
- Bartholomew, H.C.; Knuiman, M.W. Longitudinal analysis of the effect of smoking cessation on cardiovascular risk factors in a community sample: The Busselton Study. Eur. J. Cardiovasc. Prev. Rehabil. 1998, 5, 263–271. [Google Scholar] [CrossRef]
- Triebner, K.; Matulonga, B.; Johannessen, A.; Suske, S.; Benediktsdóttir, B.; Demoly, P.; Dharmage, S.C.; Franklin, K.A.; Garcia-Aymerich, J.; Gullon Blanco, J.A. Menopause is associated with accelerated lung function decline. Am. J. Respir. Crit. Care Med. 2017, 195, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Hur, K.Y.; Choi, Y.H.; Kim, S.W.; Chung, J.H.; Kim, H.K.; Lee, M.-K.; Min, Y.-K.; Kim, K.-W.; Kim, J.H. The relationship between lung function and metabolic syndrome in obese and non-obese Korean adult males. Korean Diabetes J. 2010, 34, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Gol, R.M.; Rafraf, M. Association between abdominal obesity and pulmonary function in apparently healthy adults: A systematic review. Obes. Res. Clin. Pract. 2021, 15, 415–424. [Google Scholar]
- Hegewald, M.J. Impact of obesity on pulmonary function: Current understanding and knowledge gaps. Curr. Opin. Pulm. Med. 2021, 27, 132–140. [Google Scholar] [CrossRef] [PubMed]
- van Huisstede, A.; Cabezas, M.C.; Birnie, E.; van de Geijn, G.-J.M.; Rudolphus, A.; Mannaerts, G.; Njo, T.L.; Hiemstra, P.S.; Braunstahl, G.-J. Systemic inflammation and lung function impairment in morbidly obese subjects with the metabolic syndrome. J. Obes. 2013, 2013, 131349. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Vollmer, W.M.; Buist, A.S.; Tsai, R.; Cen, R.; Wu, X.; Chen, P.; Lai, Y.; Guo, C.; Mai, J. Relationship between lung function and blood pressure in Chinese men and women of Beijing and Guangzhou. Int. J. Epidemiol. 1998, 27, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Heo, B.M.; Ryu, K.H. Prediction of prehypertenison and hypertension based on anthropometry, blood parameters, and spirometry. Int. J. Environ. Res. Public Health 2018, 15, 2571. [Google Scholar] [CrossRef] [Green Version]
- Barroso, A.T.; Martín, E.M.; Romero, L.M.R.; Ruiz, F.O. Factors affecting lung function: A review of the literature. Arch. De Bronconeumol. 2018, 54, 327–332. [Google Scholar] [CrossRef]
- Koo, H.K.; Kim, D.K.; Chung, H.S.; Lee, C.H. Association between metabolic syndrome and rate of lung function decline: A longitudinal analysis. Int. J. Tuberc. Lung Dis. 2013, 17, 1507–1514. [Google Scholar] [CrossRef]
- Zureik, M.; Benetos, A.; Neukirch, C.; Courbon, D.; Bean, K.; Thomas, F.; Ducimetiere, P. Reduced pulmonary function is associated with central arterial stiffness in men. Am. J. Respir. Crit. Care Med. 2001, 164, 2181–2185. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kim, H.Y.; Ahn, H.S.; Sohn, T.S.; Song, J.Y.; Lee, Y.B.; Lee, D.H.; Lee, J.I.; Lee, T.K.; Jeong, S.C.; et al. Glomerular filtration rate affects interpretation of pulmonary function test in a Korean general population: Results from the Korea National Health and Nutrition Examination Survey 2010 to 2012. Korean J. Intern. Med. 2016, 31, 1101–1109. [Google Scholar] [CrossRef]
- Gibbons, C.H.; Freeman, R. Orthostatic dyspnea: A neglected symptom of orthostatic hypotension. Clin. Auton. Res. 2005, 15, 40–44. [Google Scholar] [CrossRef]
- Navaneethan, S.D.; Mandayam, S.; Arrigain, S.; Rahman, M.; Winkelmayer, W.C.; Schold, J.D. Obstructive and Restrictive Lung Function Measures and CKD: National Health and Nutrition Examination Survey (NHANES) 2007-2012. Am. J. Kidney Dis. 2016, 68, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, D.H.; Shim, J.Y.; Lee, H.R.; Moon, B.S.; Park, B.J.; Lee, Y.J. Relationship between non-alcoholic fatty liver disease and pulmonary function. Intern. Med. J. 2012, 42, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Bellentani, S.; Scaglioni, F.; Marino, M.; Bedogni, G. Epidemiology of non-alcoholic fatty liver disease. Dig. Dis. 2010, 28, 155–161. [Google Scholar] [CrossRef]
- Rascu, A.; Arghir, O.C.; Naghi, E.; Otelea, M.R. Serum aminotransferases and the severity of asthma. Rev. Chim. 2018, 69, 1200–1202. [Google Scholar] [CrossRef]
- Lum, G. Low activities of aspartate and alanine aminotransferase: Their significance in alcoholic liver disease. Lab. Med. 1995, 26, 273–276. [Google Scholar] [CrossRef]
- Lim, H.I.; Jun, S.J.; Lee, S.W. Glomerular hyperfiltration may be a novel risk factor of restrictive spirometry pattern: Analysis of the Korea National Health and Nutrition Examination Survey (KNHANES) 2009-2015. PLoS ONE 2019, 14, e0223050. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Male (n = 1814) | Female (n = 7245) | p |
|---|---|---|---|
| Age (year) | 50.6 ± 11.6 | 51.1 ± 9.9 | 0.067 |
| DM (%) | 5.5 | 4.0 | 0.004 |
| Hypertension (%) | 15.2 | 10.3 | <0.001 |
| Regular exercise habits (%) | 51.9 | 48.8 | 0.019 |
| Menopause (%) | 44.3 | ||
| SBP (mmHg) | 121.5 ± 16.1 | 114.6 ± 17.8 | <0.001 |
| DBP (mmHg) | 76.6 ± 10.2 | 69.8 ± 10.3 | <0.001 |
| BMI (kg/m2) | 24.8 ± 3.2 | 23.4 ± 3.4 | <0.001 |
| Laboratory parameters | |||
| Fasting glucose (mg/dL) | 98.1 ± 19.0 | 93.9 ± 17.0 | <0.001 |
| Hemoglobin (g/dL) | 15.0 ± 1.1 | 13.0 ± 1.3 | <0.001 |
| Triglyceride (mg/dL) | 121.2 ± 88.5 | 102.2 ± 67.7 | <0.001 |
| Total cholesterol (mg/dL) | 191.0 ± 34.4 | 197.5 ± 35.3 | <0.001 |
| AST (U/L) | 25.9 ± 10.6 | 23.7 ± 10.4 | <0.001 |
| ALT (U/L) | 27.5 ± 17.8 | 20.9 ± 15.9 | <0.001 |
| eGFR (mL/min/1.73 m2) | 98.8 ± 19.7 | 114.0 ± 25.6 | <0.001 |
| Uric acid (mg/dL) | 6.4 ± 1.3 | 4.9 ± 1.1 | <0.001 |
| Lung function | |||
| FVC (L, baseline) | 3.6 ± 0.7 | 2.4 ± 0.5 | <0.001 |
| FVC (L, follow-up) | 3.3 ± 0.7 | 2.2 ± 0.5 | <0.001 |
| FEV1 (L, baseline) | 2.6 ± 0.8 | 1.8 ± 0.6 | <0.001 |
| FEV1 (L, follow-up) | 2.9 ± 0.7 | 2.0 ± 0.5 | <0.001 |
| FEV1/FVC (%, baseline) | 73.7 ± 18.4 | 72.5 ± 18.4 | 0.017 |
| FEV1/FVC (%, follow-up) | 86.9 ± 10.2 | 87.5 ± 10.7 | 0.037 |
| Characteristics | Multivariable | |
|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | |
| Age (per 1 year) | −0.055 (−0.108, −0.002) | 0.041 |
| Male (vs. female) | −1.602 (−2.966, −0.239) | 0.021 |
| DM | 0.029 (−2.330, 2.387) | 0.981 |
| Hypertension | −0.566 (−2.025, 0.893) | 0.447 |
| Regular exercise habits | −0.530 (−1.421, 0.361) | 0.243 |
| SBP (per 1 mmHg) | 0.071 (0.029, 0.112) | 0.001 |
| DBP (per 1 mmHg) | 0.084 (0.019, 0.148) | 0.011 |
| BMI (per 1 kg/m2) | −0.175 (−0.317, −0.034) | 0.015 |
| Laboratory parameters | ||
| Fasting glucose (per 1 mg/dL) | −0.002 (−0.030, 0.027) | 0.910 |
| Hemoglobin (per 1 g/dL) | −0.025 (−0.386, 0.337) | 0.894 |
| Triglyceride (per 1 mg/dL) | −0.002 (−0.009, 0.004) | 0.442 |
| Total cholesterol (per 1 mg/dL) | 0.012 (−0.001, 0.025) | 0.077 |
| AST (per 1 U/L) | 0.314 (0.257, 0.390) | <0.001 |
| ALT (per 1 U/L) | −0.196 (−0.246, −0.146) | <0.001 |
| eGFR (per 1 mL/min/1.73 m2) | 0.039 (0.020, 0.057) | <0.001 |
| Uric acid (per 1 mg/dL) | 0.274 (−0.142, 0.690) | 0.196 |
| Characteristics | Male (n = 1814) | Female (n = 7245) | |||
|---|---|---|---|---|---|
| Multivariable | Multivariable | ||||
| Unstandardized Coefficient β (95% CI) | P | Unstandardized Coefficient β (95% CI) | P | Interaction p | |
| Age (per 1 year) | −0.089 (−0.192, 0.014) | 0.090 | −0.032 (−0.119, 0.055) | 0.472 | 0.138 |
| DM | 3.844 (−1.030, 8.718) | 0.122 | −0.955 (−3.660, 1.749) | 0.489 | 0.281 |
| Hypertension | −0.543 (−3.369, 2.284) | 0.706 | −0.439 (−2.148, 1.271) | 0.615 | 0.733 |
| Regular exercise habits | 0.023 (−1.939, 1.984) | 0.982 | −0.695 (−1.696, 0.307) | 0.174 | 0.919 |
| Menopause | − | − | −0.052 (−1.621, 1.516) | 0.948 | − |
| SBP (per 1 mmHg) | 0.080 (−0.012, 0.172) | 0.090 | 0.067 (0.020, 0.114) | 0.005 | 0.767 |
| DBP (per 1 mmHg) | 0.101 (−0.035, 0.238) | 0.146 | 0.081 (0.008, 0.154) | 0.031 | 0.916 |
| BMI (per 1 kg/m2) | −0.252 (−0.580, 0.076) | 0.132 | −0.151 (−0.310, 0.007) | 0.061 | 0.716 |
| Laboratory parameters | |||||
| Fasting glucose (per 1 mg/dL) | −0.033 (0.092, 0.026) | 0.270 | 0.007 (−0.025, 0.039) | 0.682 | 0.516 |
| Hemoglobin (per 1 g/dL) | −0.322 (−1.236, 0.592) | 0.490 | 0.009 (−0.394, 0.412) | 0.966 | 0.404 |
| Triglyceride (per 1 mg/dL) | −0.002 (−0.013, 0.009) | 0.729 | −0.003 (−0.010, 0.005) | 0.515 | 0.894 |
| Total cholesterol (per 1 mg/dL) | 0.014 (−0.015, 0.042) | 0.337 | 0.010 (−0.005, 0.025) | 0.182 | 0.626 |
| AST (per 1 U/L) | 0.226 (0.078, 0.373) | 0.003 | 0.345 (0.255, 0.435) | <0.001 | 0.770 |
| ALT (per 1 U/L) | −0.131 (−0.225, −0.037) | 0.006 | −0.222 (−0.282, −0.162) | <0.001 | 0.958 |
| eGFR (per 1 mL/min/1.73 m2) | 0.080 (0.028, 0.133) | 0.003 | 0.033 (0.013, 0.053) | 0.001 | 0.150 |
| Uric acid (per 1 mg/dL) | 0.708 (−0.078, 1.495) | 0.078 | 0.113 (−0.383, 0.610) | 0.655 | 0.341 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-H.; Chen, S.-C.; Geng, J.-H.; Wu, D.-W.; Huang, J.-C.; Wu, P.-Y. Determinants of Longitudinal Change of Lung Function in Different Gender in a Large Taiwanese Population Follow-Up Study Categories: Original Investigation. J. Pers. Med. 2021, 11, 1033. https://doi.org/10.3390/jpm11101033
Chang C-H, Chen S-C, Geng J-H, Wu D-W, Huang J-C, Wu P-Y. Determinants of Longitudinal Change of Lung Function in Different Gender in a Large Taiwanese Population Follow-Up Study Categories: Original Investigation. Journal of Personalized Medicine. 2021; 11(10):1033. https://doi.org/10.3390/jpm11101033
Chicago/Turabian StyleChang, Chia-Heng, Szu-Chia Chen, Jiun-Hung Geng, Da-Wei Wu, Jiun-Chi Huang, and Pei-Yu Wu. 2021. "Determinants of Longitudinal Change of Lung Function in Different Gender in a Large Taiwanese Population Follow-Up Study Categories: Original Investigation" Journal of Personalized Medicine 11, no. 10: 1033. https://doi.org/10.3390/jpm11101033
APA StyleChang, C. -H., Chen, S. -C., Geng, J. -H., Wu, D. -W., Huang, J. -C., & Wu, P. -Y. (2021). Determinants of Longitudinal Change of Lung Function in Different Gender in a Large Taiwanese Population Follow-Up Study Categories: Original Investigation. Journal of Personalized Medicine, 11(10), 1033. https://doi.org/10.3390/jpm11101033