
miRNA Levels as a Biomarker for Anti-VEGF Response in Patients with Diabetic Macular Edema


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcome Measurements
2.3. miRNA Profiling
2.4. mRNA Expression of Leukocyte Markers
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. miRNA Levels and Visual Acuity Outcomes
3.3. miRNA Levels and Central Area Thickness
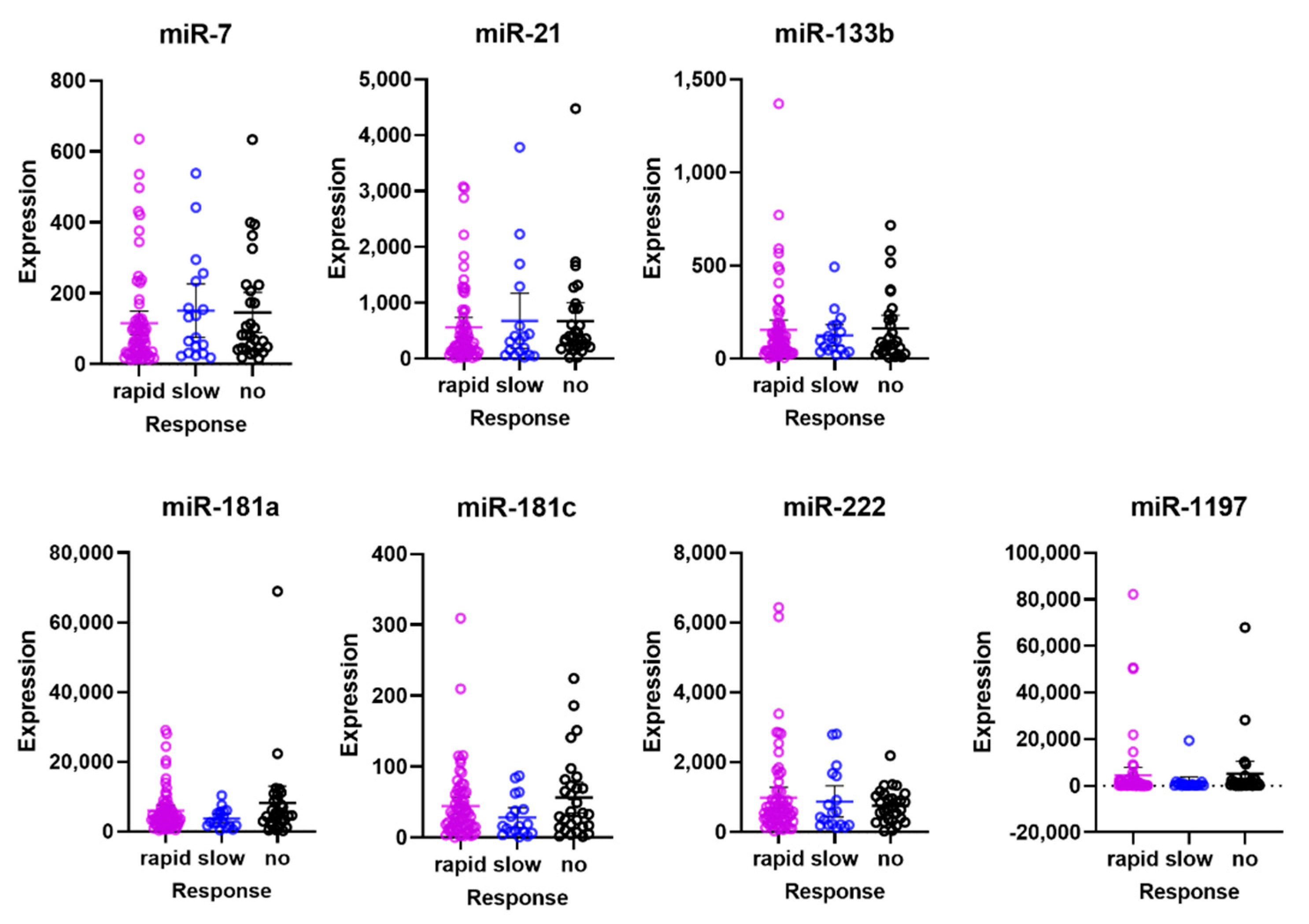
3.4. Responder Analyses
3.5. miRNA Levels and Leukocyte Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chatziralli, I. Editorial-Suboptimal response to intravitreal anti-VEGF treatment for patients with diabetic macular edema: Is there any point in switching treatment? Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5047–5050. [Google Scholar]
- Chen, Y.P.; Wu, A.L.; Chuang, C.C.; Chen, S.N. Factors influencing clinical outcomes in patients with diabetic macular edema treated with intravitreal ranibizumab: Comparison between responder and non-responder cases. Sci. Rep. 2019, 9, 10952. [Google Scholar] [CrossRef]
- Gonzalez, V.H.; Campbell, J.; Holekamp, N.M.; Kiss, S.; Loewenstein, A.; Augustin, A.J.; Ma, J.; Ho, A.C.; Patel, V.; Whitcup, S.M.; et al. Early and Long-Term Responses to Anti-Vascular Endothelial Growth Factor Therapy in Diabetic Macular Edema: Analysis of Protocol I Data. Am. J. Ophthalmol. 2016, 172, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witmer, A. Vascular endothelial growth factors and angiogenesis in eye disease. Prog. Retin. Eye Res. 2003, 22, 1–29. [Google Scholar] [CrossRef]
- Mastropasqua, R.; Toto, L.; Cipollone, F.; Santovito, D.; Carpineto, P.; Mastropasqua, L. Role of microRNAs in the modulation of diabetic retinopathy. Prog. Retin. Eye Res. 2014, 43, 92–107. [Google Scholar] [CrossRef]
- Gong, Q.; Su, G. Roles of miRNAs and long noncoding RNAs in the progression of diabetic retinopathy. Biosci. Rep. 2017, 37, BSR20171157. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.N.; Li, X.; Wu, N.; Tong, M.M.; Chen, S.; Zhu, S.S.; Qian, W.; Chen, X.L. Serum microRNA-221 as a biomarker for diabetic retinopathy in patients associated with type 2 diabetes. Int. J. Ophthalmol. 2018, 11, 1889–1894. [Google Scholar] [PubMed]
- Qing, S.; Yuan, S.; Yun, C.; Hui, H.; Mao, P.; Wen, F.; Ding, Y.; Liu, Q. Serum miRNA biomarkers serve as a fingerprint for proliferative diabetic retinopathy. Cell Physiol. Biochem. 2014, 34, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, J.; Steel, D.H.W.; Schlingemann, R.O.; Koss, M.J.; Hammes, H.P.; Krenning, G.; Klaassen, I. microRNA Expression Profile in the Vitreous of Proliferative Diabetic Retinopathy Patients and Differences from Patients Treated with Anti-VEGF Therapy. Transl. Vis. Sci. Technol. 2020, 9, 16. [Google Scholar] [CrossRef]
- Jiang, L.; Cao, H.; Deng, T.; Yang, M.; Meng, T.; Yang, H.; Luo, X. Serum exosomal miR-377-3p inhibits retinal pigment epithelium proliferation and offers a biomarker for diabetic macular edema. J. Int. Med. Res. 2021, 49, 3000605211002975. [Google Scholar] [CrossRef] [PubMed]
- Grieco, G.E.; Sebastiani, G.; Eandi, C.M.; Neri, G.; Nigi, L.; Brusco, N.; D’Aurizio, R.; Posarelli, M.; Bacci, T.; De Benedetto, E.; et al. MicroRNA Expression in the Aqueous Humor of Patients with Diabetic Macular Edema. Int. J. Mol. Sci. 2020, 21, 7328. [Google Scholar] [CrossRef]
- Cho, H.; Hwang, M.; Hong, E.H.; Yu, H.; Park, H.H.; Koh, S.H.; Shin, Y.U. Micro-RNAs in the aqueous humour of patients with diabetic macular oedema. Clin. Exp. Ophthalmol. 2020, 48, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Castro-Villegas, C.; Pérez-Sánchez, C.; Escudero, A.; Filipescu, I.; Verdu, M.; Ruiz-Limón, P.; Aguirre, M.A.; Jiménez-Gomez, Y.; Font, P.; Rodriguez-Ariza, A.; et al. Circulating miRNAs as potential biomarkers of therapy effectiveness in rheumatoid arthritis patients treated with anti-TNFα. Arthritis Res. Ther. 2015, 17, 49. [Google Scholar] [CrossRef] [Green Version]
- Citron, F.; Segatto, I.; Musco, L.; Pellarin, I.; Rampioni Vinciguerra, G.L.; Franchin, G.; Fanetti, G.; Miccichè, F.; Giacomarra, V.; Lupato, V.; et al. miR-9 modulates and predicts the response to radiotherapy and EGFR inhibition in HNSCC. EMBO Mol. Med. 2021, 13, e12872. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yao, Y.; Yuan, F.; Xie, B. Overexpression of miR-181a-5p inhibits retinal neovascularization through endocan and the ERK1/2 signaling pathway. J. Cell Physiol. 2020, 235, 9323–9335. [Google Scholar] [CrossRef]
- Dentelli, P.; Rosso, A.; Orso, F.; Olgasi, C.; Taverna, D.; Brizzi, M.F. microRNA-222 controls neovascularization by regulating signal transducer and activator of transcription 5A expression. Arter. Thromb. Vasc. Biol. 2010, 30, 1562–1568. [Google Scholar] [CrossRef] [Green Version]
- Robinson, P.M.; Chuang, T.D.; Sriram, S.; Pi, L.; Luo, X.P.; Petersen, B.E.; Schultz, G.S. MicroRNA signature in wound healing following excimer laser ablation: Role of miR-133b on TGFβ1, CTGF, SMA, and COL1A1 expression levels in rabbit corneal fibroblasts. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6944–6951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babae, N.; Bourajjaj, M.; Liu, Y.; Van Beijnum, J.R.; Cerisoli, F.; Scaria, P.V.; Verheul, M.; Van Berkel, M.P.; Pieters, E.H.; Van Haastert, R.J.; et al. Systemic miRNA-7 delivery inhibits tumor angiogenesis and growth in murine xenograft glioblastoma. Oncotarget 2014, 5, 6687–6700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vader, M.J.C.; Schauwvlieghe, A.M.E.; Verbraak, F.D.; Dijkman, G.; Hooymans, J.M.M.; Los, L.I.; Zwinderman, A.H.; Peto, T.; Hoyng, C.B.; van Leeuwen, R.; et al. Comparing the Efficacy of Bevacizumab and Ranibizumab in Patients with Diabetic Macular Edema (BRDME): The BRDME Study, a Randomized Trial. Ophthalmol. Retin. 2020, 4, 777–788. [Google Scholar] [CrossRef]
- Giani, A.; Cigada, M.; Choudhry, N.; Deiro, A.P.; Oldani, M.; Pellegrini, M.; Invernizzi, A.; Duca, P.; Miller, J.W.; Staurenghi, G. Reproducibility of retinal thickness measurements on normal and pathologic eyes by different optical coherence tomography instruments. Am. J. Ophthalmol. 2010, 150, 815–824. [Google Scholar] [CrossRef]
- Ruijter, J.M.; Ramakers, C.; Hoogaars, W.M.; Karlen, Y.; Bakker, O.; van den Hoff, M.J.; Moorman, A.F. Amplification efficiency: Linking baseline and bias in the analysis of quantitative PCR data. Nucleic Acids Res. 2009, 37, e45. [Google Scholar] [CrossRef] [Green Version]
- Klaassen, I.; Hughes, J.M.; Vogels, I.M.; Schalkwijk, C.G.; Van Noorden, C.J.; Schlingemann, R.O. Altered expression of genes related to blood-retina barrier disruption in streptozotocin-induced diabetes. Exp. Eye Res. 2009, 89, 4–15. [Google Scholar] [CrossRef] [PubMed]
- del Toro, R.; Prahst, C.; Mathivet, T.; Siegfried, G.; Kaminker, J.S.; Larrivee, B.; Breant, C.; Duarte, A.; Takakura, N.; Fukamizu, A.; et al. Identification and functional analysis of endothelial tip cell-enriched genes. Blood 2010, 116, 4025–4033. [Google Scholar] [CrossRef] [Green Version]
- Rocha, S.F.; Schiller, M.; Jing, D.; Li, H.; Butz, S.; Vestweber, D.; Biljes, D.; Drexler, H.C.; Nieminen-Kelhä, M.; Vajkoczy, P.; et al. Esm1 modulates endothelial tip cell behavior and vascular permeability by enhancing VEGF bioavailability. Circ. Res. 2014, 115, 581–590. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Tahiri, H.; Cai, C.; Gu, M.; Gagnon, C.; Hardy, P. microRNA-181a inhibits ocular neovascularization by interfering with vascular endothelial growth factor expression. Cardiovasc. Ther. 2018, 36, e12329. [Google Scholar] [CrossRef] [PubMed]
- Kamal, N.N.M.; Shahidan, W.N.S. Non-Exosomal and Exosomal Circulatory MicroRNAs: Which Are More Valid as Biomarkers? Front. Pharmacol. 2019, 10, 1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| miRNA | miR7 | miR21 | miR133b | miR181a | miR181c | miR222 | miR1197 | |
|---|---|---|---|---|---|---|---|---|
| Baseline BCVA | Beta | 0.132 | 0.152 | −0.047 | 0.102 | 0.080 | 0.154 | 0.078 |
| SE | 1.868 | 1.486 | 1.782 | 1.904 | 1.345 | 1.911 | 0.990 | |
| p-value | 0.128 | 0.078 | 0.586 | 0.240 | 0.354 | 0.074 | 0.371 | |
| ∆BCVA 3 months | Beta | −0.135 | −0.088 | 0.068 | 0.020 | 0.046 | −0.041 | −0.040 |
| SE | 1.299 | 1.042 | 1.238 | 1.331 | 0.938 | 1.344 | 0.690 | |
| p-value | 0.118 | 0.310 | 0.430 | 0.821 | 0.579 | 0.635 | 0.642 | |
| ∆BCVA 6 months | Beta | −0.062 | 0.004 | 0.167 | 0.108 | 0.081 | 0.060 | 0.008 |
| SE | 1.437 | 1.149 | 1.343 | 1.453 | 1.027 | 1.475 | 0.758 | |
| p-value | 0.473 | 0.962 | 0.053 | 0.214 | 0.353 | 0.490 | 0.922 |
| miRNA | miR7 | miR21 | miR133b | miR181a | miR181c | miR222 | miR1197 | ||
|---|---|---|---|---|---|---|---|---|---|
| Baseline CAT | Univariable | Beta | −0.194 | −0.154 | −0.151 | −0.298 | −0.157 | −0.217 | −0.171 |
| SE | 19.132 | 15.373 | 18.244 | 18.906 | 13.792 | 19.538 | 10.119 | ||
| p-value | 0.024 | 0.074 | 0.080 | 0.000 | 0.070 | 0.011 | 0.048 | ||
| Multivariable | Beta | −0.083 | 0.013 | −0.002 | −0.348 | 0.070 | 0.097 | −0.106 | |
| SE | 30.418 | 27.553 | 22.193 | 33.824 | 18.543 | 43.481 | 10.780 | ||
| p-value | 0.540 | 0.932 | 0.986 | 0.020 | 0.546 | 0.608 | 0.246 | ||
| ∆CAT 3 months | Univariable | Beta | 0.138 | 0.058 | 0.001 | 0.054 | −0.028 | 0.025 | 0.104 |
| SE | 21.117 | 16.982 | 20.178 | 21.619 | 15.260 | 21.876 | 11.167 | ||
| p-value | 0.111 | 0.506 | 0.993 | 0.535 | 0.747 | 0.774 | 0.228 | ||
| Multivariable | Beta | 0.273 | 0.034 | −0.074 | 0.168 | −0.129 | −0.259 | 0.113 | |
| SE | 34.108 | 30.896 | 24.886 | 37.928 | 20.793 | 48.757 | 12.088 | ||
| p-value | 0.051 | 0.827 | 0.493 | 0.270 | 0.278 | 0.182 | 0.226 | ||
| ∆CAT 6 months | Univariable | Beta | 0.120 | 0.053 | 0.010 | 0.137 | 0.018 | 0.066 | 0.144 |
| SE | 21.871 | 17.553 | 20.850 | 22.160 | 15.773 | 22.563 | 11.482 | ||
| p-value | 0.164 | 0.541 | 0.913 | 0.112 | 0.839 | 0.446 | 0.096 | ||
| Multivariable | Beta | 0.191 | −0.009 | −0.091 | 0.286 | −0.122 | −0.218 | 0.142 | |
| SE | 35.111 | 31.804 | 25.617 | 39.043 | 21.404 | 50.190 | 12.444 | ||
| p-value | 0.169 | 0.957 | 0.394 | 0.061 | 0.302 | 0.259 | 0.128 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vader, M.J.C.; Habani, Y.I.; Schlingemann, R.O.; Klaassen, I. miRNA Levels as a Biomarker for Anti-VEGF Response in Patients with Diabetic Macular Edema. J. Pers. Med. 2021, 11, 1297. https://doi.org/10.3390/jpm11121297
Vader MJC, Habani YI, Schlingemann RO, Klaassen I. miRNA Levels as a Biomarker for Anti-VEGF Response in Patients with Diabetic Macular Edema. Journal of Personalized Medicine. 2021; 11(12):1297. https://doi.org/10.3390/jpm11121297
Chicago/Turabian StyleVader, Maartje J. C., Yasmin I. Habani, Reinier O. Schlingemann, and Ingeborg Klaassen. 2021. "miRNA Levels as a Biomarker for Anti-VEGF Response in Patients with Diabetic Macular Edema" Journal of Personalized Medicine 11, no. 12: 1297. https://doi.org/10.3390/jpm11121297
APA StyleVader, M. J. C., Habani, Y. I., Schlingemann, R. O., & Klaassen, I. (2021). miRNA Levels as a Biomarker for Anti-VEGF Response in Patients with Diabetic Macular Edema. Journal of Personalized Medicine, 11(12), 1297. https://doi.org/10.3390/jpm11121297