
Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings


Abstract
:1. Introduction
1.1. Co-Occurring Conditions Can Interfere with Daily Function
1.2. Treatment Approaches to Modulate Physiological Drivers of Symptoms
1.3. An Alternative Treatment Approach to Modulate the Physiological Drivers of Anxiety and Sleep Disruption
1.4. TEN May Be an Excellent Treatment for Anxiety and Sleep in ASD
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. TEN Treatment
2.4. Outcome Measures
2.4.1. Anxiety Measures
2.4.2. Sleep Measures
2.4.3. Cognitive Battery
2.4.4. Autonomic Assessments
2.4.5. Measurement of Adverse Events
2.5. Statistical Analysis
3. Results
3.1. Adverse Effects
3.2. Anxiety
3.3. Sleep
3.4. Anxiety-Provoking Task Performance
3.5. Salivary Biomarkers
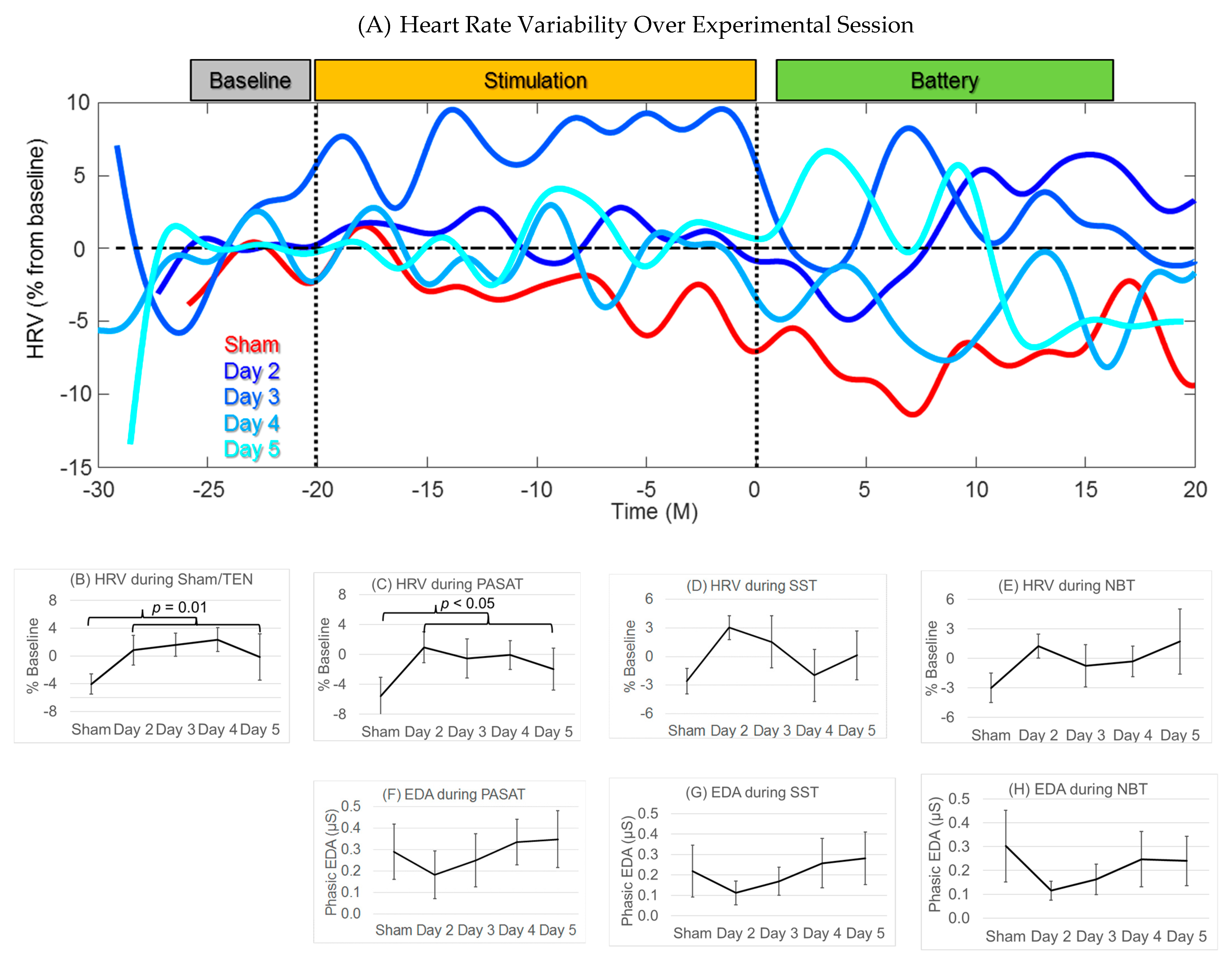
3.6. Heart Rate Variability
3.7. Electrodermal Activity
3.8. Effect of Intelligence
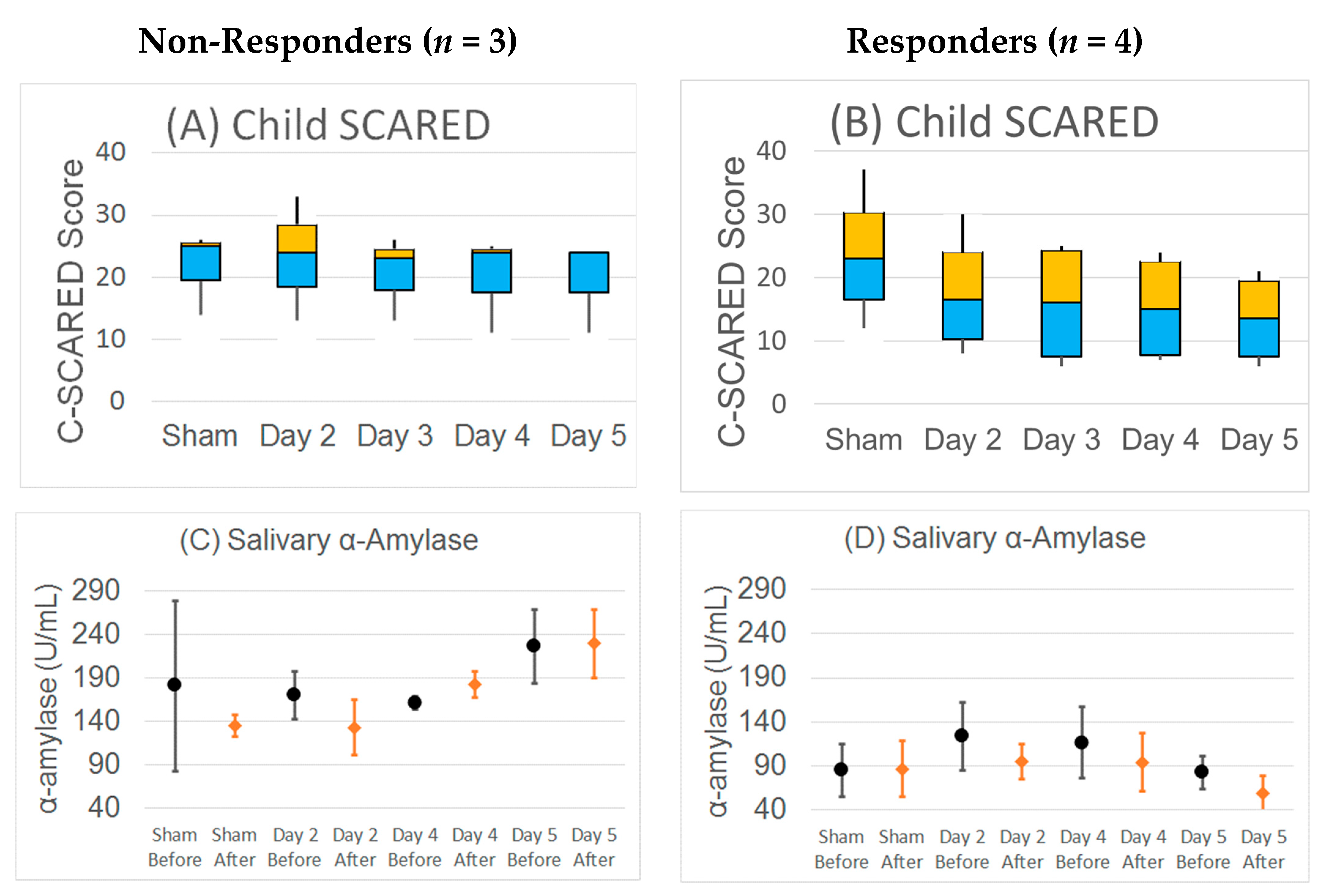
3.9. Responder Analysis
4. Discussion
4.1. TEN Improved Rating of Anxiety in ASD
4.2. Possible Effect of TEN on Sleep in ASD
4.3. TEN Improved Performance on Anxiety-Provoking Tasks
4.4. Cortisol Response to Social Paradigms as a Bio-Marker for Stress in ASD
4.5. α-Amylase Response to Social Paradigms as a Bio-Marker for Stress in ASD
4.6. TEN Improved Heart Rate Variability in ASD
4.7. Dynamic Changes in Autonomic Nervous System Measures with TEN
4.8. Further Refinement of TEN Protocol
4.9. Limitations
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rossignol, D.A.; Frye, R.E. A review of research trends in physiological abnormalities in autism spectrum disorders: Immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Mol. Psychiatry 2012, 17, 389–401. [Google Scholar] [CrossRef] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. Morbidity and Mortality Weekly Report. Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council On Children With Disabilities, S.O.D.; Behavioral, P. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Fein, D.; Barton, M.; Eigsti, I.M.; Kelley, E.; Naigles, L.; Schultz, R.T.; Stevens, M.; Helt, M.; Orinstein, A.; Rosenthal, M.; et al. Optimal outcome in individuals with a history of autism. J. Child Psychol. Psychiatry Allied Discip. 2013, 54, 195–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fountain, C.; Winter, A.S.; Bearman, P.S. Six developmental trajectories characterize children with autism. Pediatrics 2012, 129, e1112–e1120. [Google Scholar] [CrossRef] [Green Version]
- Magiati, I.; Tay, X.W.; Howlin, P. Cognitive, language, social and behavioural outcomes in adults with autism spectrum disorders: A systematic review of longitudinal follow-up studies in adulthood. Clin. Psychol Rev. 2014, 34, 73–86. [Google Scholar] [CrossRef]
- Rogge, N.; Janssen, J. The Economic Costs of Autism Spectrum Disorder: A Literature Review. J. Autism Dev. Disord. 2019. [Google Scholar] [CrossRef]
- Cakir, J.; Frye, R.E.; Walker, S.J. The lifetime social cost of autism: 1990–2029. Res. Autism Spectr. Disord. 2020, 72, 101502. [Google Scholar] [CrossRef]
- Brown, C.C.; Tilford, J.M.; Payakachat, N.; Williams, D.K.; Kuhlthau, K.A.; Pyne, J.M.; Hoefman, R.J.; Brouwer, W.B.F. Measuring Health Spillover Effects in Caregivers of Children with Autism Spectrum Disorder: A Comparison of the EQ-5D-3L and SF-6D. Pharmacoeconomics 2019, 37, 609–620. [Google Scholar] [CrossRef] [Green Version]
- Hartley, S.L.; Papp, L.M.; Bolt, D. Spillover of Marital Interactions and Parenting Stress in Families of Children With Autism Spectrum Disorder. J. Clin. Child Adolesc. Psychol. Off. J. Soc. Clin. Child. Adolesc. Psychol. Am. Psychol. Assoc. Div. 2018, 47, S88–S99. [Google Scholar] [CrossRef] [PubMed]
- Tilford, J.M.; Payakachat, N.; Kuhlthau, K.A.; Pyne, J.M.; Kovacs, E.; Bellando, J.; Williams, D.K.; Brouwer, W.B.; Frye, R.E. Treatment for Sleep Problems in Children with Autism and Caregiver Spillover Effects. J. Autism Dev. Disord. 2015, 45, 3613–3623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, K.; Rydzewska, E.; Fleming, M.; Cooper, S.A. Prevalence of mental health conditions, sensory impairments and physical disability in people with co-occurring intellectual disabilities and autism compared with other people: A cross-sectional total population study in Scotland. BMJ Open 2020, 10, e035280. [Google Scholar] [CrossRef] [PubMed]
- Viscidi, E.W.; Triche, E.W.; Pescosolido, M.F.; McLean, R.L.; Joseph, R.M.; Spence, S.J.; Morrow, E.M. Clinical characteristics of children with autism spectrum disorder and co-occurring epilepsy. PLoS ONE 2013, 8, e67797. [Google Scholar] [CrossRef] [Green Version]
- Holingue, C.; Newill, C.; Lee, L.C.; Pasricha, P.J.; Daniele Fallin, M. Gastrointestinal symptoms in autism spectrum disorder: A review of the literature on ascertainment and prevalence. Autism Res. Off. J. Int. Soc. Autism Res. 2018, 11, 24–36. [Google Scholar] [CrossRef]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef]
- Grondhuis, S.N.; Aman, M.G. Assessment of anxiety in children and adolescents with autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 1345–1365. [Google Scholar] [CrossRef]
- van Steensel, F.J.A.; Heeman, E.J. Anxiety Levels in Children with Autism Spectrum Disorder: A Meta-Analysis. J. Child. Fam Stud. 2017, 26, 1753–1767. [Google Scholar] [CrossRef] [Green Version]
- Baker, E.K.; Richdale, A.L.; Hazi, A. Employment status is related to sleep problems in adults with autism spectrum disorder and no comorbid intellectual impairment. Autism Int. J. Res. Pract. 2019, 23, 531–536. [Google Scholar] [CrossRef]
- Deliens, G.; Peigneux, P. Sleep-behaviour relationship in children with autism spectrum disorder: Methodological pitfalls and insights from cognition and sensory processing. Dev. Med. Child Neurol. 2019, 61, 1368–1376. [Google Scholar] [CrossRef] [Green Version]
- Kuusikko, S.; Pollock-Wurman, R.; Jussila, K.; Carter, A.S.; Mattila, M.L.; Ebeling, H.; Pauls, D.L.; Moilanen, I. Social anxiety in high-functioning children and adolescents with Autism and Asperger syndrome. J. Autism Dev. Disord. 2008, 38, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, Y.-S.; Koh, Y.-J.; Song, J.; Leventhal, B.L. A contrast of comorbid condition and adaptive function between children with Autism Spectrum Disorder from clinical and non-clinical populations. Res. Autism Spectr. Disord. 2014, 8, 1471–1481. [Google Scholar] [CrossRef]
- Myles, B.S.; Barnhill, G.P.; Hagiwara, T.; Griswold, D.E.; Simpson, R.L. A Synthesis of Studies on the Intellectual, Academic, Social/ Emotional and Sensory Characteristics of Children and Youth with Asperger Syndrome. Educ. Train. Ment. Retard. Dev. Disabil. 2001, 36, 304–311. [Google Scholar]
- Ader, R.; Cohen, N.; Felten, D. Psychoneuroimmunology: Interactions between the nervous system and the immune system. Lancet 1995, 345, 99–103. [Google Scholar] [CrossRef]
- Padgett, D.A.; Glaser, R. How stress influences the immune response. Trends Immunol. 2003, 24, 444–448. [Google Scholar] [CrossRef]
- Brotman, D.J.; Golden, S.H.; Wittstein, I.S. The cardiovascular toll of stress. Lancet 2007, 370, 1089–1100. [Google Scholar] [CrossRef]
- Hodge, D.; Carollo, T.M.; Lewin, M.; Hoffman, C.D.; Sweeney, D.P. Sleep patterns in children with and without autism spectrum disorders: Developmental comparisons. Res. Dev. Disabil. 2014, 35, 1631–1638. [Google Scholar] [CrossRef]
- Dewrang, P.; Sandberg, A.D. Parental retrospective assessment of development and behavior in Asperger syndrome during the first 2 years of life. Res. Autism Spectr. Disord. 2010, 4, 461–473. [Google Scholar] [CrossRef]
- Barnevik Olsson, M.; Carlsson, L.H.; Westerlund, J.; Gillberg, C.; Fernell, E. Autism before diagnosis: Crying, feeding and sleeping problems in the first two years of life. Acta Paediatr. 2013, 102, 635–639. [Google Scholar] [CrossRef]
- Deliens, G.; Leproult, R.; Schmitz, R.; Destrebecqz, A.; Peigneux, P. Sleep Disturbances in Autism Spectrum Disorders. Rev. J. Autism Dev. Disord. 2015, 2, 343–356. [Google Scholar] [CrossRef] [Green Version]
- Rossignol, D.A.; Frye, R.E. Psychotropic Medications for Sleep Disorders in Autism Spectrum Disorders. In Handbook of Autism and Pervasive Developmental Disorders; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2021. [Google Scholar]
- Williams, K.; Brignell, A.; Randall, M.; Silove, N.; Hazell, P. Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2013, 8, Cd004677. [Google Scholar] [CrossRef] [PubMed]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Scully, D.; Kremer, J.; Meade, M.M.; Graham, R.; Dudgeon, K. Physical exercise and psychological well being: A critical review. Br. J. Sports Med. 1998, 32, 111–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams Buckley, A.; Hirtz, D.; Oskoui, M.; Armstrong, M.J.; Batra, A.; Bridgemohan, C.; Coury, D.; Dawson, G.; Donley, D.; Findling, R.L.; et al. Practice guideline: Treatment for insomnia and disrupted sleep behavior in children and adolescents with autism spectrum disorder: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2020, 94, 392–404. [Google Scholar] [CrossRef] [Green Version]
- Panju, S.; Brian, J.; Dupuis, A.; Anagnostou, E.; Kushki, A. Atypical sympathetic arousal in children with autism spectrum disorder and its association with anxiety symptomatology. Mol. Autism 2015, 6, 64. [Google Scholar] [CrossRef] [Green Version]
- Kushki, A.; Drumm, E.; Pla Mobarak, M.; Tanel, N.; Dupuis, A.; Chau, T.; Anagnostou, E. Investigating the autonomic nervous system response to anxiety in children with autism spectrum disorders. PLoS ONE 2013, 8, e59730. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, B.J.; Marler, S.; Altstein, L.L.; Lee, E.B.; Akers, J.; Sohl, K.; McLaughlin, A.; Hartnett, K.; Kille, B.; Mazurek, M.; et al. Psychophysiological Associations with Gastrointestinal Symptomatology in Autism Spectrum Disorder. Autism Res. Off. J. Int. Soc. Autism Res. 2017, 10, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Daluwatte, C.; Miles, J.H.; Sun, J.; Yao, G. Association between pupillary light reflex and sensory behaviors in children with autism spectrum disorders. Res. Dev. Disabil. 2015, 37, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Tyler, W.J.; Boasso, A.M.; Mortimore, H.M.; Silva, R.S.; Charlesworth, J.D.; Marlin, M.A.; Aebersold, K.; Aven, L.; Wetmore, D.Z.; Pal, S.K. Transdermal neuromodulation of noradrenergic activity suppresses psychophysiological and biochemical stress responses in humans. Sci. Rep. 2015, 5, 13865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, I.A.; Schrader, L.M.; Degiorgio, C.M.; Miller, P.R.; Maremont, E.R.; Leuchter, A.F. Trigeminal nerve stimulation in major depressive disorder: Acute outcomes in an open pilot study. Epilepsy Behav. 2013, 28, 221–226. [Google Scholar] [CrossRef]
- Couto, L.B.; Moroni, C.R.; dos Reis Ferreira, C.M.; Elias-Filho, D.H.; Parada, C.A.; Pela, I.R.; Coimbra, N.C. Descriptive and functional neuroanatomy of locus coeruleus-noradrenaline-containing neurons involvement in bradykinin-induced antinociception on principal sensory trigeminal nucleus. J. Chem. Neuroanat. 2006, 32, 28–45. [Google Scholar] [CrossRef] [PubMed]
- Aston-Jones, G.; Shipley, M.T.; Chouvet, G.; Ennis, M.; van Bockstaele, E.; Pieribone, V.; Shiekhattar, R.; Akaoka, H.; Drolet, G.; Astier, B.; et al. Afferent regulation of locus coeruleus neurons: Anatomy, physiology and pharmacology. Prog. Brain Res. 1991, 88, 47–75. [Google Scholar] [CrossRef] [PubMed]
- Berridge, C.W.; Waterhouse, B.D. The locus coeruleus-noradrenergic system: Modulation of behavioral state and state-dependent cognitive processes. Brain Res. Brain Res. Rev. 2003, 42, 33–84. [Google Scholar] [CrossRef]
- McGough, J.J.; Sturm, A.; Cowen, J.; Tung, K.; Salgari, G.C.; Leuchter, A.F.; Cook, I.A.; Sugar, C.A.; Loo, S.K. Double-Blind, Sham-Controlled, Pilot Study of Trigeminal Nerve Stimulation for Attention-Deficit/Hyperactivity Disorder. J. Am. Acad. Child. Adolesc. Psychiatry 2019, 58, 403–411 e403. [Google Scholar] [CrossRef]
- Blech, B.; Starling, A.J. Noninvasive Neuromodulation in Migraine. Curr. Pain Headache Rep. 2020, 24, 78. [Google Scholar] [CrossRef]
- Trevizol, A.P.; Shiozawa, P.; Albuquerque Sato, I.; da Silva, M.E.; de Barros Calfat, E.L.; Alberto, R.L.; Cook, I.A.; Cordeiro, Q. Trigeminal Nerve Stimulation (TNS) for Post-traumatic Stress Disorder: A Case Study. Brain Stimul. 2015, 8, 676–678. [Google Scholar] [CrossRef] [Green Version]
- Trevizol, A.P.; Shiozawa, P.; Sato, I.A.; Calfat, E.L.; Alberto, R.L.; Cook, I.A.; Medeiros, H.H.; Cordeiro, Q. Trigeminal Nerve Stimulation (TNS) for Generalized Anxiety Disorder: A Case Study. Brain Stimul. 2015, 8, 659–660. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Jia, M.X.; Zhang, J.S.; Xu, X.J.; Shou, X.J.; Zhang, X.T.; Li, L.; Li, N.; Han, S.P.; Han, J.S. Transcutaneous electrical acupoint stimulation in children with autism and its impact on plasma levels of arginine-vasopressin and oxytocin: A prospective single-blinded controlled study. Res. Dev. Disabil. 2012, 33, 1136–1146. [Google Scholar] [CrossRef]
- Zhang, J.S.; Zhang, X.T.; Zou, L.P.; Zhang, R.; Han, S.P.; Han, J.S. [A Preliminary Study on Effect of Transcutaneous Electrical Acupoint Stimulation for Children with Autism]. Zhen Ci Yan Jiu 2017, 42, 249–253. [Google Scholar]
- Wang, X.; Ding, R.; Song, Y.; Wang, J.; Zhang, C.; Han, S.; Han, J.; Zhang, R. Transcutaneous Electrical Acupoint Stimulation in Early Life Changes Synaptic Plasticity and Improves Symptoms in a Valproic Acid-Induced Rat Model of Autism. Neural Plast. 2020, 2020, 8832694. [Google Scholar] [CrossRef]
- Jin, Y.; Kong, J. Transcutaneous Vagus Nerve Stimulation: A Promising Method for Treatment of Autism Spectrum Disorders. Front. Neurosci. 2016, 10, 609. [Google Scholar] [CrossRef] [Green Version]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [Green Version]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child. Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Blakeley-Smith, A.; Reaven, J.; Ridge, K.; Hepburn, S. Parent–child agreement of anxiety symptoms in youth with autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 707–716. [Google Scholar] [CrossRef]
- Stern, J.A.; Gadgil, M.S.; Blakeley-Smith, A.; Reaven, J.A.; Hepburn, S.L. Psychometric Properties of the SCARED in Youth with Autism Spectrum Disorder. Res. Autism Spectr. Disord. 2014, 8, 1225–1234. [Google Scholar] [CrossRef] [Green Version]
- Behrens, B.; Swetlitz, C.; Pine, D.S.; Pagliaccio, D. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Informant Discrepancy, Measurement Invariance, and Test-Retest Reliability. Child. Psychiatry Hum. Dev. 2019, 50, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Scahill, L.; Lecavalier, L.; Schultz, R.T.; Evans, A.N.; Maddox, B.; Pritchett, J.; Herrington, J.; Gillespie, S.; Miller, J.; Amoss, R.T.; et al. Development of the Parent-Rated Anxiety Scale for Youth With Autism Spectrum Disorder. J. Am. Acad. Child. Adolesc. Psychiatry 2019, 58, 887–896.e882. [Google Scholar] [CrossRef]
- Moore, M.; Evans, V.; Hanvey, G.; Johnson, C. Assessment of Sleep in Children with Autism Spectrum Disorder. Children 2017, 4, 72. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. A comprehensive review of the Paced Auditory Serial Addition Test (PASAT). Arch. Clin. Neuropsychol. 2006, 21, 53–76. [Google Scholar] [CrossRef] [Green Version]
- Parsons, T.D.; Courtney, C.G. An initial validation of the Virtual Reality Paced Auditory Serial Addition Test in a college sample. J. Neurosci. Methods 2014, 222, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.K.; Lange, G.; DeLuca, J.; Korn, L.R.; Natelson, B. The effects of fatigue on neuropsychological performance in patients with chronic fatigue syndrome, multiple sclerosis, and depression. Appl. Neuropsychol. 1997, 4, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.; Harris, L.; Pollick, F.; Melville, C. A meta-analysis of working memory in individuals with autism spectrum disorders. PLoS ONE 2019, 14, e0216198. [Google Scholar] [CrossRef] [Green Version]
- Peirce, J.; Gray, J.R.; Simpson, S.; MacAskill, M.; Höchenberger, R.; Sogo, H.; Kastman, E.; Lindeløv, J.K. PsychoPy2: Experiments in behavior made easy. Behav. Res. Methods 2019, 51, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Speer, K.E.; Semple, S.; Naumovski, N.; McKune, A.J. Measuring Heart Rate Variability Using Commercially Available Devices in Healthy Children: A Validity and Reliability Study. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 390–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, J.A.; Quintana, D.S.; Abbott, M.J.; Kemp, A.H. Anxiety Disorders are Associated with Reduced Heart Rate Variability: A Meta-Analysis. Front. Psychiatry 2014, 5, 80. [Google Scholar] [CrossRef] [Green Version]
- Benedek, M.; Kaernbach, C. A continuous measure of phasic electrodermal activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [Green Version]
- Caporino, N.E.; Sakolsky, D.; Brodman, D.M.; McGuire, J.F.; Piacentini, J.; Peris, T.S.; Ginsburg, G.S.; Walkup, J.T.; Iyengar, S.; Kendall, P.C.; et al. Establishing Clinical Cutoffs for Response and Remission on the Screen for Child Anxiety Related Emotional Disorders (SCARED). J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 696–702. [Google Scholar] [CrossRef]
- Schiltz, H.K.; Magnus, B.E. Differential Item Functioning Based on Autism Features, IQ, and Age on the Screen for Child Anxiety Related Disorders (SCARED) Among Youth on the Autism Spectrum. Autism Res. Off. J. Int. Soc. Autism Res. 2021, 14, 1220–1236. [Google Scholar] [CrossRef]
- Qiu, J.; Kong, X.; Li, J.; Yang, J.; Huang, Y.; Huang, M.; Sun, B.; Su, J.; Chen, H.; Wan, G.; et al. Transcranial Direct Current Stimulation (tDCS) over the Left Dorsal Lateral Prefrontal Cortex in Children with Autism Spectrum Disorder (ASD). Neural Plast. 2021, 2021, 6627507. [Google Scholar] [CrossRef]
- Keogh, S.; Bridle, C.; Siriwardena, N.A.; Nadkarni, A.; Laparidou, D.; Durrant, S.J.; Kargas, N.; Law, G.R.; Curtis, F. Effectiveness of non-pharmacological interventions for insomnia in children with Autism Spectrum Disorder: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0221428. [Google Scholar] [CrossRef]
- Giannotti, F.; Cortesi, F.; Cerquiglini, A.; Bernabei, P. An open-label study of controlled-release melatonin in treatment of sleep disorders in children with autism. J. Autism Dev. Disord. 2006, 36, 741–752. [Google Scholar] [CrossRef]
- Pardo, G.; Coates, S.; Okuda, D.T. Outcome measures assisting treatment optimization in multiple sclerosis. J. Neurol. 2021. Available online: https://link.springer.com/article/10.1007/s00415-021-10674-8 (accessed on 31 August 2021). [CrossRef]
- Corbett, B.A.; Muscatello, R.A.; Kim, A.; Patel, K.; Vandekar, S. Developmental effects in physiological stress in early adolescents with and without autism spectrum disorder. Psychoneuroendocrinology 2021, 125, 105115. [Google Scholar] [CrossRef]
- Levine, T.P.; Sheinkopf, S.J.; Pescosolido, M.; Rodino, A.; Elia, G.; Lester, B. Physiologic Arousal to Social Stress in Children with Autism Spectrum Disorders: A Pilot Study. Res. Autism Spectr. Disord. 2012, 6, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.L.; Corbett, B.A. A review of rhythm and responsiveness of cortisol in individuals with autism spectrum disorders. Psychoneuroendocrinology 2014, 49, 207–228. [Google Scholar] [CrossRef] [Green Version]
- Hollocks, M.J.; Pickles, A.; Howlin, P.; Simonoff, E. Dual Cognitive and Biological Correlates of Anxiety in Autism Spectrum Disorders. J. Autism Dev. Disord. 2016, 46, 3295–3307. [Google Scholar] [CrossRef] [Green Version]
- Corbett, B.A.; Mendoza, S.; Abdullah, M.; Wegelin, J.A.; Levine, S. Cortisol circadian rhythms and response to stress in children with autism. Psychoneuroendocrinology 2006, 31, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Corbett, B.A.; Mendoza, S.; Wegelin, J.A.; Carmean, V.; Levine, S. Variable cortisol circadian rhythms in children with autism and anticipatory stress. J. Psychiatry Neurosci. 2008, 33, 227–234. [Google Scholar] [PubMed]
- Corbett, B.A.; Schupp, C.W.; Levine, S.; Mendoza, S. Comparing cortisol, stress, and sensory sensitivity in children with autism. Autism Res. Off. J. Int. Soc. Autism Res. 2009, 2, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiper, M.W.M.; Verhoeven, E.W.M.; Geurts, H.M. Heart rate variability predicts inhibitory control in adults with autism spectrum disorders. Biol. Psychol. 2017, 128, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Thapa, R.; Alvares, G.A.; Zaidi, T.A.; Thomas, E.E.; Hickie, I.B.; Park, S.H.; Guastella, A.J. Reduced heart rate variability in adults with autism spectrum disorder. Autism Res. Off. J. Int. Soc. Autism Res. 2019, 12, 922–930. [Google Scholar] [CrossRef]
- Dijkhuis, R.R.; Ziermans, T.; van Rijn, S.; Staal, W.; Swaab, H. Emotional Arousal During Social Stress in Young Adults With Autism: Insights From Heart Rate, Heart Rate Variability and Self-Report. J. Autism Dev. Disord. 2019, 49, 2524–2535. [Google Scholar] [CrossRef] [Green Version]
- Cai, R.Y.; Richdale, A.L.; Dissanayake, C.; Uljarevic, M. Resting heart rate variability, emotion regulation, psychological wellbeing and autism symptomatology in adults with and without autism. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2019, 137, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bujnakova, I.; Ondrejka, I.; Mestanik, M.; Visnovcova, Z.; Mestanikova, A.; Hrtanek, I.; Fleskova, D.; Calkovska, A.; Tonhajzerova, I. Autism spectrum disorder is associated with autonomic underarousal. Physiol. Res. 2016, 65, S673–S682. [Google Scholar] [CrossRef]
- Harder, R.; Malow, B.A.; Goodpaster, R.L.; Iqbal, F.; Halbower, A.; Goldman, S.E.; Fawkes, D.B.; Wang, L.; Shi, Y.; Baudenbacher, F.; et al. Heart rate variability during sleep in children with autism spectrum disorder. Clin. Auton. Res. Off. J. Clin. Auton. Res. Soc. 2016, 26, 423–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Hensley, M.K.; Tasman, A.; Sears, L.; Casanova, M.F.; Sokhadze, E.M. Heart Rate Variability and Skin Conductance During Repetitive TMS Course in Children with Autism. Appl. Psychophysiol. Biofeedback 2016, 41, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Vidyashree, H.M.; Maheshkumar, K.; Sundareswaran, L.; Sakthivel, G.; Partheeban, P.K.; Rajan, R. Effect of Yoga Intervention on Short-Term Heart Rate Variability in Children with Autism Spectrum Disorder. Int. J. Yoga 2019, 12, 73–77. [Google Scholar] [CrossRef]
- Casanova, M.F.; Hensley, M.K.; Sokhadze, E.M.; El-Baz, A.S.; Wang, Y.; Li, X.; Sears, L. Effects of weekly low-frequency rTMS on autonomic measures in children with autism spectrum disorder. Front. Hum. Neurosci. 2014, 8, 851. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study ID | Age (Years) | Gender | KBIT-2 Score | SCARED—Child | SCARED—Parent | PRAS | Total CSHQ | Sleep Anxiety |
| TEN-01 | 12 | Female | 103 | 14 | 25 | 43 | 46 | 4 |
| TEN-03 | 13 | Male | 83 | 12 | 25 | 38 | 63 | 6 |
| TEN-05 | 10 | Male | 116 | 25 | 46 | 48 | 64 | 8 |
| TEN-06 | 21 | Male | 109 | 26 | 33 | 32 | 54 | 5 |
| TEN-07 | 20 | Male | 104 | 28 | 29 | 42 | 59 | 6 |
| TEN-08 | 10 | Male | 96 | 18 | 36 | 38 | 52 | 5 |
| TEN-09 | 13 | Female | 109 | 37 | 50 | 45 | 53 | 4 |
| Study ID | Frequency (Hz) | Duty Cycle | Pulse Width (ms) | Daily Threshold (Milliamps) | ||||
|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | ||||
| TENS-01 | 300 | 50% | 350 | 2.5 | 2.0 | 3.5 | 3.0 | 3.0 |
| TENS-03 | 300 | 50% | 350 | 4.5 | 4.0 | 5.5 | 6.5 | 5.5 |
| TENS-05 | 300 | 50% | 350 | 2.5 | 2.0 | 2.0 | 2.5 | 2.5 |
| TENS-06 | 300 | 50% | 350 | 2.5 | 3.5 | 3.5 | 2.5 | 4.5 |
| TENS-07 | 300 | 50% | 350 | 0.5 | 3.0 | 1.5 | 1.0 | 1.5 |
| TENS-08 | 300 | 50% | 350 | 3.5 | 13.5 | 13.5 | 12.5 | 8.5 |
| TENS-09 | 300 | 50% | 350 | 2.0 | 3.0 | 1.0 | 1.0 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foldes, S.T.; Jensen, A.R.; Jacobson, A.; Vassall, S.; Foldes, E.; Guthery, A.; Brown, D.; Levine, T.; Tyler, W.J.; Frye, R.E. Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings. J. Pers. Med. 2021, 11, 1307. https://doi.org/10.3390/jpm11121307
Foldes ST, Jensen AR, Jacobson A, Vassall S, Foldes E, Guthery A, Brown D, Levine T, Tyler WJ, Frye RE. Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings. Journal of Personalized Medicine. 2021; 11(12):1307. https://doi.org/10.3390/jpm11121307
Chicago/Turabian StyleFoldes, Stephen T., Amanda R. Jensen, Austin Jacobson, Sarah Vassall, Emily Foldes, Ann Guthery, Danni Brown, Todd Levine, William James Tyler, and Richard E. Frye. 2021. "Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings" Journal of Personalized Medicine 11, no. 12: 1307. https://doi.org/10.3390/jpm11121307
APA StyleFoldes, S. T., Jensen, A. R., Jacobson, A., Vassall, S., Foldes, E., Guthery, A., Brown, D., Levine, T., Tyler, W. J., & Frye, R. E. (2021). Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings. Journal of Personalized Medicine, 11(12), 1307. https://doi.org/10.3390/jpm11121307