
Contrast-Enhanced Ultrasonography in the Diagnosis and Treatment Modulation of Breast Cancer



Abstract
: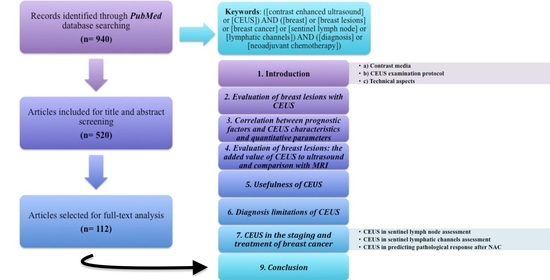
1. Introduction
2. Evaluation of Breast Lesions with CEUS
3. Correlation between Prognostic Factors and CEUS Characteristics and Quantitative Parameters
4. Evaluation of Breast Lesions: The Added Value of CEUS to Ultrasound and Comparison with MRI
- Score 1 = BIRADS 3: no enhancement, clear delimitation of the lesion from the adjacent parenchyma;
- Score 2 = BIRADS 4A: synchronous and iso-enhancement with the adjacent parenchyma, without clear delimitation;
- Score 3 = BIRADS 4B: early, homogeneous/heterogeneous enhancement, regular shape (round/oval), sharp margins, size equal to/smaller than at gray-scale ultrasound;
- Score 4 = BIRADS 4C: early heterogeneous enhancement, lesion size larger than at gray-scale ultrasound, irregular shape, ± perfusion defects, ± crab-claw-like enhancement;
- Score 5 = BIRADS 5: early, heterogeneous and typical crab-claw-like enhancement, irregular margins, lesion size larger than at gray-scale ultrasound, ± perfusion defects.
5. Usefulness of CEUS
6. Diagnosis Limitations of CEUS
7. CEUS in the Staging and Treatment of Breast Cancer
7.1. CEUS in Sentinel Lymph Node Assessment
- type I—homogeneous enhancement.
- type II—heterogeneous uptake (regional or diffuse), with hypoperfusion or unperfused areas.
7.2. CEUS in Sentinel Lymphatic Channels Assessment
- superficial sentinel lymphatic channels (SSLCs)—which start from the subareolar lymphatic plexus and pass into the subcutaneous adipose tissue.
- penetrating sentinel lymphatic channels (PSLCs)—which also originate from the subareolar lymphatic plexus and pass into the breast glandular parenchyma.
- deep sentinel lymphatic channels (DSLCs)—which start from the breast parenchyma and pass through the breast parenchyma or into the retro mammary cellular space [56].
7.3. CEUS in Predicting Pathological Response After NAC
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Du, J.; Wang, L.; Wan, C.-F.; Hua, J.; Fang, H.; Chen, J.; Li, F.H. Differentiating benign from malignant solid breast lesions: Combined utility of conventional ultrasound and contrast-enhanced ultrasound in comparison with magnetic resonance imaging. Eur. J. Radiol. 2012, 81, 3890–3899. [Google Scholar] [CrossRef] [PubMed]
- Nykänen, A.; Arponen, O.; Sutela, A.; Vanninen, R.; Sudah, M. Is there a role for contrast-enhanced ultrasound in the detection and biopsy of MRI only visible breast lesions? Radiol. Oncol. 2017, 51, 386–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, T.; Hirakata, T.; Yanagita, Y.; Iijima, M.; Horikoshi, H.; Takeuchi, K.; Saitoh, Y. The detection of pCR after PST by con-trast-enhanced ultrasonography for breast cancer. Breast Cancer 2013, 20, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Dong, L.; Jiang, Q.; Guan, X.; Wu, H.; Luo, B. Incorporating Contrast-Enhanced Ultrasound into the BI-RADS Scoring System Improves Accuracy in Breast Tumor Diagnosis: A Preliminary Study in China. Ultrasound Med. Biol. 2016, 42, 2630–2638. [Google Scholar] [CrossRef]
- Sever, A.R.; Mills, P.; Weeks, J.; Jones, S.E.; Fish, D.; Jones, P.A.; Fish, D.; Jones, P.A.; Mali, W. Preoperative needle biopsy of sentinel lymph nodes using in-tradermal microbubbles and contrast-enhanced ultrasound in patients with breast cancer. Am. J. Roentgenol. 2012, 199, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Michailidou, A.; Trenz, H.-J.; de Wilde, P. Annex I: The Internet and European Integration; Verlag Barbara Budrich: Leverkusen, Germany, 2019; pp. 167–172. [Google Scholar]
- Chou, H.Y.; Liang, D.J.; Wang, S.Y.; Hsu, S.J.; Hu, J.T.; Yang, S.S.; Wang, H.-K.; Lee, T.-Y.; Tiu, C.-M. Safety of perfluorobutane (Sonazoid) in characterizing focal liver lesions. J. Med. Ultrasound. 2019, 27, 81–85. [Google Scholar] [CrossRef]
- Luo, J.; Chen, J.-D.; Chen, Q.; Yue, L.-X.; Zhou, G.; Lan, C.; Li, Y.; Wu, C.-H.; Lu, J.-Q. Contrast-enhanced ultrasound improved performance of breast im-aging reporting and data system evaluation of critical breast lesions. World J. Radiol. 2016, 8, 610. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.-L.; Bao, W.; Zhu, S.-G.; Wang, L.-H.; Sun, M.-H.; Men, Y.-M.; Xue, J.; Wang, L. Contrast-Enhanced Ultrasound Characteristics of Breast Cancer: Correlation with Prognostic Factors. Ultrasound Med. Biol. 2014, 40, 11–17. [Google Scholar] [CrossRef]
- Xiao, X.; Ou, B.; Yang, H.; Wu, H.; Luo, B. Breast Contrast-Enhanced Ultrasound: Is a Scoring System Feasible?—A Preliminary Study in China. PLoS ONE 2014, 9, e105517. [Google Scholar] [CrossRef]
- Wang, Z.; Zhou, Q.; Liu, J.; Tang, S.; Liang, X.; Zhou, Z.; He, Y.; Peng, H.; Xiao, Y. Tumor size of breast invasive ductal cancer measured with con-trast-enhanced ultrasound predicts regional lymph node metastasis and N stage. Int. J. Clin. Exp. Pathol. 2014, 7, 6985–6991. [Google Scholar]
- Zhao, L.-X.; Liu, H.; Wei, Q.; Xu, G.; Wu, J.; Xu, H.; Wu, R.; Pu, H. Contrast-Enhanced Ultrasonography Features of Breast Malignancies with Different Sizes: Correlation with Prognostic Factors. BioMed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nakata, N.; Ohta, T.; Nishioka, M.; Takeyama, H.; Toriumi, Y.; Kato, K.; Nogi, H.; Kamio, M.; Fukuda, K. Optimization of region of interest drawing for quan-titative analysis: Differentiation between benign and malignant breast lesions on contrast-enhanced sonography. J. Ultrasound Med. 2015, 34, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Vraka, I.; Panourgias, E.; Sifakis, E.; Koureas, A.; Galanis, P.; Dellaportas, D.; Gouliamos, A.; Antoniou, A. Correlation between contrast-enhanced ultrasound characteristics (qualitative and quantitative) and pathological prognostic factors in breast cancer. In Vivo 2018, 32, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Omoto, K.; Matsunaga, H.; Take, N.; Hozumi, Y.; Takehara, M.; Omoto, Y.; Shiozawa, M.; Mizunuma, H.; Harashima, H.; Taniguchi, N.; et al. Sentinel Node Detection Method Using Con-trast-Enhanced Ultrasonography with Sonazoid in Breast Cancer: Preliminary Clinical Study. Ultrasound Med. Biol. 2009, 35, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Esfehani, M.H.; Yazdankhah-Kenari, A.; Omranipour, R. Validation of Contrast Enhanced Ultrasound Technique to Wire Lo-calization of Sentinel Lymph Node in Patients with Early Breast Cancer. Indian J. Surg. Oncol. 2015, 6, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Gong, H.; Ling, L.; Du, L.; Su, T.; Wang, S.; Wang, J. Diagnostic performance of contrast-enhanced ultrasound and enhanced magnetic resonance for breast nodules. J. Biomed. Res. 2018, 32, 198–207. [Google Scholar] [CrossRef]
- Wang, Y.-M.; Fan, W.; Zhang, K.; Zhang, L.; Tan, Z.; Ma, R. Comparison of transducers with different frequencies in breast contrast-enhanced ultrasound (CEUS) using SonoVue as contrast agent. Br. J. Radiol. 2016, 89, 20151050. [Google Scholar] [CrossRef] [Green Version]
- Amioka, A.; Masumoto, N.; Gouda, N.; Kajitani, K.; Shigematsu, H.; Emi, A.; Kadoya, T.; Okada, M. Ability of contrast-enhanced ultrasonography to determine clinical responses of breast cancer to neoadjuvant chemotherapy. Jpn. J. Clin. Oncol. 2016, 46, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Saracco, A.; Szabó, B.K.; Tánczos, E.; Bergh, J.; Hatschek, T. Contrast-enhanced ultrasound (CEUS) in assessing early response among patients with invasive breast cancer undergoing neoadjuvant chemotherapy. Acta Radiol. 2017, 58, 394–402. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kim, S.H.; Kang, B.J.; Kim, Y.J. Contrast-Enhanced Ultrasound for Early Prediction of Response of Breast Cancer to Neo-adjuvant Chemotherapy. Ultraschall Med. 2019, 40, 194–204. [Google Scholar]
- Wan, C.; Du, J.; Fang, H.; Li, F.; Wang, L. Evaluation of breast lesions by contrast enhanced ultrasound: Qualitative and quantitative analysis. Eur. J. Radiol. 2012, 81, e444–e450. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Ito, T.; Takada, E.; Omoto, K.; Hirai, T.; Moriyasu, F. Efficacy of Sonazoid (perflubutane) for contrast-enhanced ul-trasound in the differentiation of focal breast lesions: Phase 3 multicenter clinical trial. Am. J. Roentgenol. 2014, 202, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Drudi, F.M.; Cantisani, V.; Gnecchi, M.; Malpassini, F.; Di Leo, N.; De Felice, C. Contrast-Enhanced Ultrasound Examination of the Breast: A Literature Review. Ultraschall Med. Eur. J. Ultrasound 2012, 33, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- La Forgia, D.; Fanizzi, A.; Campobasso, F.; Bellotti, R.; Didonna, V.; Lorusso, V.; Moschetta, M.; Massafra, R.; Tamborra, P.; Tangaro, S.; et al. Radiomic analysis in contrast-enhanced spectral mammog-raphy for predicting breast cancer histology outcome. Diagnostics 2020, 10, 708. [Google Scholar] [CrossRef]
- Ji, C.-L.; Li, X.-L.; He, Y.-P.; Li, D.-D.; Gu, X.-G.; Xu, H.-X. Quantitative parameters of contrast-enhanced ultrasound in breast invasive ductal carcinoma: The correlation with pathological prognostic factors. Clin. Hemorheol. Microcirc. 2017, 66, 333–345. [Google Scholar] [CrossRef]
- Kutomi, G.; Mizuguchi, T.; Satomi, F.; Maeda, H.; Shima, H.; Kimura, Y.; Hirata, K. Current status of the prognostic molecular biomarkers in breast cancer: A systematic review. Oncol. Lett. 2017, 13, 1491–1498. [Google Scholar] [CrossRef] [Green Version]
- Thangarajah, F.; Enninga, I.; Malter, W.; Hamacher, S.; Markiefka, B.; Richters, L.; Krämer, S.; Mallmann, P.; Kirn, V. A Retrospective Analysis of Ki-67 Index and its Prognostic Significance in over 800 Primary Breast Cancer Cases. Anticancer. Res. 2017, 37, 1957–1964. [Google Scholar] [CrossRef]
- Zhao, Y.-X.; Liu, S.; Hu, Y.-B.; Ge, Y.-Y.; Lv, D.-M. Diagnostic and prognostic values of contrast-enhanced ultrasound in breast cancer: A retrospective study. OncoTargets Ther. 2017, 10, 1123–1129. [Google Scholar] [CrossRef] [Green Version]
- Bassullu, N.; Turkmen, I.; Dayangac, M.; Korkmaz, P.Y.; Yasar, R.; Akyildiz, M.; Yaprak, O.; Tokat, Y.; Yuzer, Y.; Dogusoy, G.B. The Predictive and Prognostic Significance of c-erb-B2, EGFR, PTEN, mTOR, PI3K, p27, and ERCC1 Expression in Hepatocellular Carcinoma. Zahedan J. Res. Med. Sci. 2012, 12, e7492. [Google Scholar] [CrossRef] [Green Version]
- Fisher, D.R.; Baltzer, P.; Malich, A.; Wurdinger, S.; Freesmeyer, M.G.; Marx, C.; Kaiser, W.A. Is the “blomming sign” a promising additonal tool to determine malignancy in MR mammography? Eur. Radiol. 2004, 14, 394–401. [Google Scholar] [CrossRef]
- Colpaert, C.; Vermeulen, P.; Van Marck, E.; Dirix, L.Y. The Presence of a Fibrotic Focus Is an Independent Predictor of Early Metastasis in Lymph Node-Negative Breast Cancer Patients. Am. J. Surg. Pathol. 2001, 25, 1557–1558. [Google Scholar] [CrossRef]
- Wan, C.F.; Du, J.; Fang, H.; Li, F.H.; Zhu, J.S.; Liu, Q. Enhancement patterns and parameters of breast cancers at contrast-enhanced us: Correlation with prognostic factors. Radiology. 2012, 262, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, Y.; Zhu, Y.; Fu, L.; Liu, P. Association between enhancement patterns and parameters of contrast-enhanced ultrasound and microvessel distribution in breast cancer. Oncol. Lett. 2018, 15, 5643–5649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Hu, M.; Chen, Z.; Li, C.; Zhang, X.; Song, Y.; Xiang, F. Meta-Analysis: Contrast-Enhanced Ultrasound Versus Conventional Ultrasound for Differentiation of Benign and Malignant Breast Lesions. Ultrasound Med. Biol. 2018, 44, 919–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Wu, Y.; Chen, M.; Gu, X.-G. Application of contrast-enhanced ultrasound in the diagnosis of small breast lesions. Clin. Hemorheol. Microcirc. 2018, 70, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Spick, C.; Baltzer, P.A.T. Diagnostic utility of second-look US for breast lesions identified at MR imaging: Systematic review and meta-analysis. Radiology 2014, 273, 401–409. [Google Scholar] [CrossRef]
- Gao, Y.; Bagadiya, N.R.; Jardon, M.L.; Heller, S.L.; Melsaether, A.N.; Toth, H.B.; Moy, L. Outcomes of Preoperative MRI-Guided Needle Localization of Nonpalpable Mammographically Occult Breast Lesions. Am. J. Roentgenol. 2016, 207, 1–9. [Google Scholar] [CrossRef]
- Chen, Y.; Tang, L.; Du, Z.; Zhong, Z.; Luo, J.; Yang, L.; Shen, R.; Cheng, Y.; Zhang, Z.; Han, E.; et al. Factors influencing the performance of a diagnostic model including contrast-enhanced ultrasound in 1023 breast lesions: Comparison with histopathology. Ann. Transl. Med. 2019, 7, 647. [Google Scholar] [CrossRef]
- Zhang, W.; Li, J.M.; He, W.; Pan, M.X.; Jin, Z.Q.; Liang, T.; Zhang, H. Ultrasound-guided percunateous microwave ablation for benign breast lesions: Evaluated by contrast-enhanced ultrasound combined with magnetic resonance imaging. J. Thorac. Dis. 2017, 9, 4767–4773. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Yang, K.; Cao, Y.; Zhou, X.; Xu, J.; Liu, J.; Wang, Q.; Wang, Z.; Wang, D. Comparison of the synergistic effect of lipid nanobubbles and SonoVue microbubbles for high intensity focused ultrasound thermal ablation of tumors. Peer J. 2016, 4, e1716. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Xu, P.; Wang, Y.; Grant, E.G. Contrast-enhanced ultrasonographic findings of different histopathologic types of breast cancer. Acta Radiol. 2011, 52, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Fanizzi, A.; Basile, T.M.; Lasurdo, L.; Bellotti, R.; Bottigli, U.; Campobasso, F.; Didonna, V.; Fausto, A.; Massafra, R.; Tagliafico, A.; et al. Ensemble discrete wavelet transform and gray-level co-occurrence matrix for microcalcification cluster classification in digital mammography. Appl. Sci. 2019, 9, 5388. [Google Scholar] [CrossRef]
- Losurdo, L.; Fanizzi, A.; Basile, T.M.A.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Lorusso, V.; Massafra, R.; Tamborra, P.; et al. Radiomics Analysis on Contrast-Enhanced Spectral Mammography Images for Breast Cancer Diagnosis: A Pilot Study. Entropy 2019, 21, 1110. [Google Scholar] [CrossRef] [Green Version]
- Nielsen Moody, A.; Bull, J.; Culpan, A.M.; Munyombwe, T.; Sharma, N.; Whitaker, M.; Wolstenhulme, S. Preoperative sentinel lymph node identification, biopsy and localisation using contrast enhanced ultrasound (CEUS) in patients with breast cancer: A systematic review and meta-analysis. Clin. Radiol. 2017, 72, 959–971. [Google Scholar] [CrossRef]
- Pesek, S.; Ashikaga, T.; Krag, L.E.; Krag, D. The false-negative rate of sentinel node biopsy in patients with breast cancer: A me-ta-analysis. World J. Surg. 2012, 36, 2239–2251. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhou, W.; Li, C.; Gong, H.; Li, C.; Yang, N.; Nianzhao, Y.; Chen, L.; Xia, T.; Liu, X.; et al. Variation of sentinel lymphatic channels (SLCs) and sentinel lymph nodes (SLNs) assessed by contrast-enhanced ultrasound (CEUS) in breast cancer patients. World J. Surg. Oncol. 2017, 15, 1–7. [Google Scholar] [CrossRef]
- Ahmed, M.; Purushotham, A.D.; Douek, M. Novel techniques for sentinel lymph node biopsy in breast cancer: A systematic review. Lancet Oncol. 2014, 15, e351–e362. [Google Scholar] [CrossRef]
- Zhong, J.; Sun, D.-S.; Wei, W.; Liu, X.; Liu, J.; Wu, X.; Zhang, Y.; Luo, H.; Li, Y. Contrast-Enhanced Ultrasound-Guided Fine-Needle Aspiration for Sentinel Lymph Node Biopsy in Early-Stage Breast Cancer. Ultrasound Med. Biol. 2018, 44, 1371–1378. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, J.; Zhu, Q.-L.; Jiang, Y.; Sun, Q.; Zhou, Y.; Wang, M.-Q.; Meng, Z.-L.; Mao, X. The value of contrast-enhanced ultrasound for sentinel lymph node identification and characterisation in pre-operative breast cancer patients: A prospective study. Eur. Radiol. 2018, 28, 1654–1661. [Google Scholar] [CrossRef]
- Xie, F.; Zhang, D.; Cheng, L.; Yu, L.; Yang, L.; Tong, F.; Liu, H.; Wang, S.; Wang, S. Intradermal microbubbles and contrast-enhanced ultrasound (CEUS) is a feasible approach for sentinel lymph node identification in early-stage breast cancer. World J. Surg. Oncol. 2015, 13, 319. [Google Scholar] [CrossRef]
- Agliata, G.; Valeri, G.; Argalia, G.; Tarabelli, E.; Giuseppetti, G.M. Role of Contrast-Enhanced Sonography in the Evaluation of Axillary Lymph Nodes in Breast Carcinoma: A Monocentric Study. J. Ultrasound Med. 2017, 36, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; Von Minckwitz, G.; Nekljudova, V.; et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Breslin, T.M.; Cohen, L.; Sahin, A.; Fleming, J.B.; Kuerer, H.M.; Newman, L.A.; Delpassand, E.S.; House, R.; Ames, F.C.; Feig, B.W.; et al. Sentinel Lymph Node Biopsy Is Accurate After Neoadjuvant Chemotherapy for Breast Cancer. J. Clin. Oncol. 2000, 18, 3480–3486. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, X.-M.; Kang, S.; Li, X.; Geng, J. Contrast-enhanced ultrasonography in qualitative diagnosis of sentinel lymph node metastasis in breast cancer: A meta-analysis. J. Cancer Res. Ther. 2015, 11, 697. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, W.; Zhao, Y.; Xia, T.; Zha, X.; Ding, Q.; Liu, X.; Zhao, Y.; Ling, L.; Chen, L.; et al. A Novel Finding of Sentinel Lymphatic Channels in Early Stage Breast Cancer Patients: Which May Influence Detection Rate and False-Negative Rate of Sentinel Lymph Node Biopsy. PLoS ONE 2012, 7, e51226. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Cheng, X.; Li, J.; Jiang, J.; Jiang, Z.; Li, H.; Li, T.; Zhang, Z.; Tan, B.; Lu, M. Preliminary study of real-time three-dimensional contrast-enhanced ultrasound of sentinel lymph nodes in breast cancer. Eur. Radiol. 2019, 30, 1426–1435. [Google Scholar] [CrossRef]
- Marinovich, M.L.; Macaskill, P.; Irwig, L.; Sardanelli, F.; Mamounas, E.P.; Von Minckwitz, G.; Guarneri, V.; Partridge, S.C.; Wright, F.C.; Choi, J.H.; et al. Agreement between MRI and pathologic breast tumor size after neoadjuvant chemotherapy, and comparison with alternative tests: Individual patient data meta-analysis. BMC Cancer 2015, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Chu, W.; Jin, W.; Liu, D.; Wang, J.; Geng, C.; Chen, L.; Huang, X. Diffusion-weighted imaging in identifying breast cancer pathological response to neoadjuvant chemotherapy: A meta-analysis. Oncotarget 2017, 9, 7088–7100. [Google Scholar] [CrossRef] [Green Version]
- Galli, G.; Bregni, G.; Cavalieri, S.; Porcu, L.; Baili, P.; Hade, A.; Di Salvo, F.; Sant, M.; Agresti, R.; Gennaro, M.; et al. Neoadjuvant Chemotherapy Exerts Selection Pressure Towards Luminal Phenotype Breast Cancer. Breast Care 2017, 12, 391–394. [Google Scholar] [CrossRef]
- Kaufmann, M.; Von Minckwitz, G.; Mamounas, E.P.; Cameron, D.; Carey, L.A.; Cristofanilli, M.; Denkert, C.; Eiermann, W.; Gnant, M.; Harris, J.R.; et al. Recommendations from an International Consensus Conference on the Current Status and Future of Neoadjuvant Systemic Therapy in Primary Breast Cancer. Ann. Surg. Oncol. 2011, 19, 1508–1516. [Google Scholar] [CrossRef]
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef]
- Jia, K.; Li, L.; Wu, X.J.; Hao, M.J.; Xue, H.Y. Contrast-enhanced ultrasound for evaluating the pathologic response of breast cancer to neoadjuvant chemotherapy: A meta-analysis. Medicine 2019, 98, 142–158. [Google Scholar] [CrossRef] [PubMed]
- Wan, C.-F.; Liu, X.-S.; Wang, L.; Zhang, J.; Lu, J.-S.; Li, F. Quantitative contrast-enhanced ultrasound evaluation of pathological complete response in patients with locally advanced breast cancer receiving neoadjuvant chemotherapy. Eur. J. Radiol. 2018, 103, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Xue, J.; Zhao, B. Potential Application Value of Contrast-Enhanced Ultrasound In Neoadjuvant Chemotherapy of Breast Cancer. Ultrasound Med. Biol. 2012, 38, 2065–2071. [Google Scholar] [CrossRef]
- Lee, S.C.; Grant, E.; Sheth, P.; Garcia, A.A.; Desai, B.; Ji, L.; Groshen, S.; Hwang, D.; Yamashita, M.; Hovanessian-Larsen, L. Ultrasound Compared with Magnetic Resonance Imaging in As-sessing the Tumor Response After Neoadjuvant Chemotherapy for Breast Cancer. J. Ultrasound Med. 2017, 36, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Jiang, T.; Huang, M.; Wang, J.; Chu, Y.; Zhong, L.; Zheng, S. Evaluation of the response of breast cancer patients to neoadjuvant chemotherapy by combined contrast-enhanced ultrasonography and ultrasound elastography. Exp. Ther. Med. 2019, 17, 3655–3663. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breast Lesions at CEUS | |
|---|---|
| Qualitative Characteristics | Quantitative Parameters |
| enhancement degree compared with the surrounding breast tissue (hypo-, iso-, hyperenhancement) | Peak (%): the maximum intensity of the enhancing curve during the bolus given by the formula [(post-contrast signal−pre-contrast signal)/pre-contrast signal] × 100% |
| internal homogeneity (homogeneous/inhomogeneous) | TTP (time to peak) (s): the time from the appearance of the first microbubbles in the lesion to its maximum peak intensity |
| presence/absence of perfusion defects | MTT (mean transit time) (s): the time interval from the appearance of the first microbubbles in the lesion to the time when the peak intensity fells to half. |
| uptake pattern (centripetal/centrifugal) | RBV (regional blood volume) (mL): the area under time-intensity curve, reflecting total volume of contrast medium (or blood) traversing the region of interest |
| lesion margins (well/ill-defined >50% of circumference) | RBF (regional blood flow) (mL/sec): the relative blood flow in the selected lesion’s area, calculated as RBV/MTT |
| presence/absence of perilesional enhancement | |
| Peak (%) | TTP (s) | MTT (s) | RBV (mL) | RBF (mL/s) | |
|---|---|---|---|---|---|
| Benign | 23.18 ± 12.4 | 34.79 ± 11.60 | 47.54 ± 13.94 | 1277.25 ± 14.98 | 26.17 ± 14.98 |
| Malign | 29.22 ± 6.78 | 25.92 ± 11.09 | 47.45 ± 15.16 | 1806.80 ± 48.40 | 37.02 ± 9.74 |
| Cut-off points | 24.25 | 26.71 | - | 1310.80 | 29.65 |
| ER | Ki-67 | Her2 | ||||
|---|---|---|---|---|---|---|
| Negative | Positive | Negative | Positive | Negative | Positive | |
| Peak (%) * | 52.6 ± 18.6 | 56.3 ± 24.1 | 57.9 ± 23.3 | 52.1 ± 21.9 | 53.1 ± 24.4 | 57.3 ± 21.2 |
| TTP (s) * | 14.1 ± 4.5 | 15.8 ± 8.0 | 15.7 ± 5.9 | 15.0 ± 8.7 | 16.6 ± 8.7 | 14.2 ± 5.3 |
| MTT (s) ** | 24.6 (9.2) | 21.1 (12.6) | 18.7 (49.6) | 23.1 (17.4) | 20.8 (36.6) | 18.1 (49.6) |
| RBV (mL) ** | 1436.8 (737.7) | 1316.3 (1099.2) | 932.3 (3770.4) | 2120.5 (1680.9) | 908.3 (3046.7) | 956.9 (3770.4) |
| RBF (mL/s) * | 56.4 ± 16.6 | 60.0 ± 25.5 | 61.1 ± 24.3 | 56.5 ± 23.8 | 56.6 ± 25.9 | 61.4 ± 22.5 |
| Tumor Histological Grade | Quantitative Parameters | |
|---|---|---|
| Rise Time (The Time from 10% Maximum Intensity to 90%) | TTP | |
| I or II | 9.3 s ± 3.9 s | 11.6s ± 6.1 s |
| III | 11.4 s ± 5.4 s | 14.7s ± 7.7 s |
| Pooled Values | CEUS Versus the US | CEUS + US Versus US | ||
|---|---|---|---|---|
| CEUS | US | CEUS + US | US | |
| Sensitivity | 0.93 (95%CI:0.91–0.95) | 0.87 (95%CI:0.85–0.90) | 0.94 (95%CI:0.92–0.96) | 0.87 (95%CI:0.84–0.90) |
| Specificity | 0.86 (95%CI:0.84–0.88) | 0.72 (95%CI:0.69–0.75) | 0.86 (95%CI:0.82–0.89) | 0.80 (95%CI:0.76–0.84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boca, I.; Dudea, S.M.; Ciurea, A.I. Contrast-Enhanced Ultrasonography in the Diagnosis and Treatment Modulation of Breast Cancer. J. Pers. Med. 2021, 11, 81. https://doi.org/10.3390/jpm11020081
Boca I, Dudea SM, Ciurea AI. Contrast-Enhanced Ultrasonography in the Diagnosis and Treatment Modulation of Breast Cancer. Journal of Personalized Medicine. 2021; 11(2):81. https://doi.org/10.3390/jpm11020081
Chicago/Turabian StyleBoca (Bene), Ioana, Sorin M. Dudea, and Anca I. Ciurea. 2021. "Contrast-Enhanced Ultrasonography in the Diagnosis and Treatment Modulation of Breast Cancer" Journal of Personalized Medicine 11, no. 2: 81. https://doi.org/10.3390/jpm11020081
APA StyleBoca, I., Dudea, S. M., & Ciurea, A. I. (2021). Contrast-Enhanced Ultrasonography in the Diagnosis and Treatment Modulation of Breast Cancer. Journal of Personalized Medicine, 11(2), 81. https://doi.org/10.3390/jpm11020081