
Gender Differences in Patients with Metastatic Pancreatic Cancer Who Received FOLFIRINOX

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
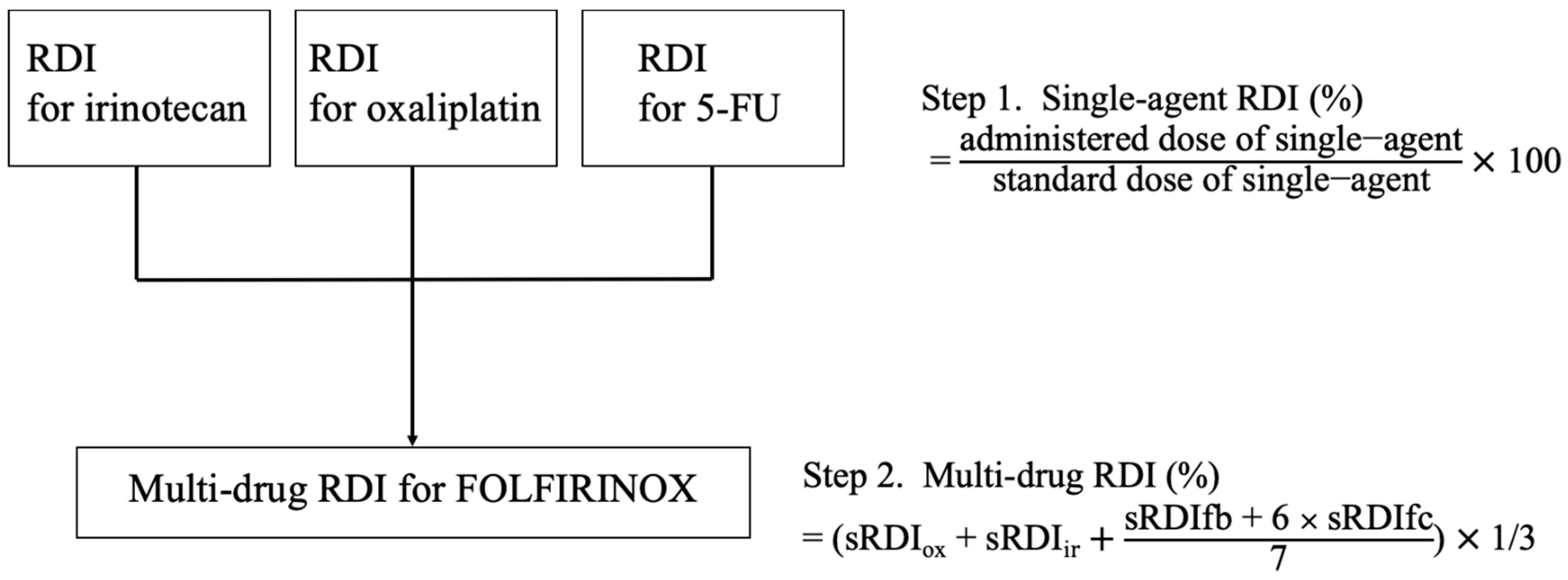
2.2. Calculation of the Modified Dose of FOLFIRINOX
2.3. Study Objectives
2.4. Statistical analysis
3. Results
3.1. Baseline Patient and Tumor Characteristics
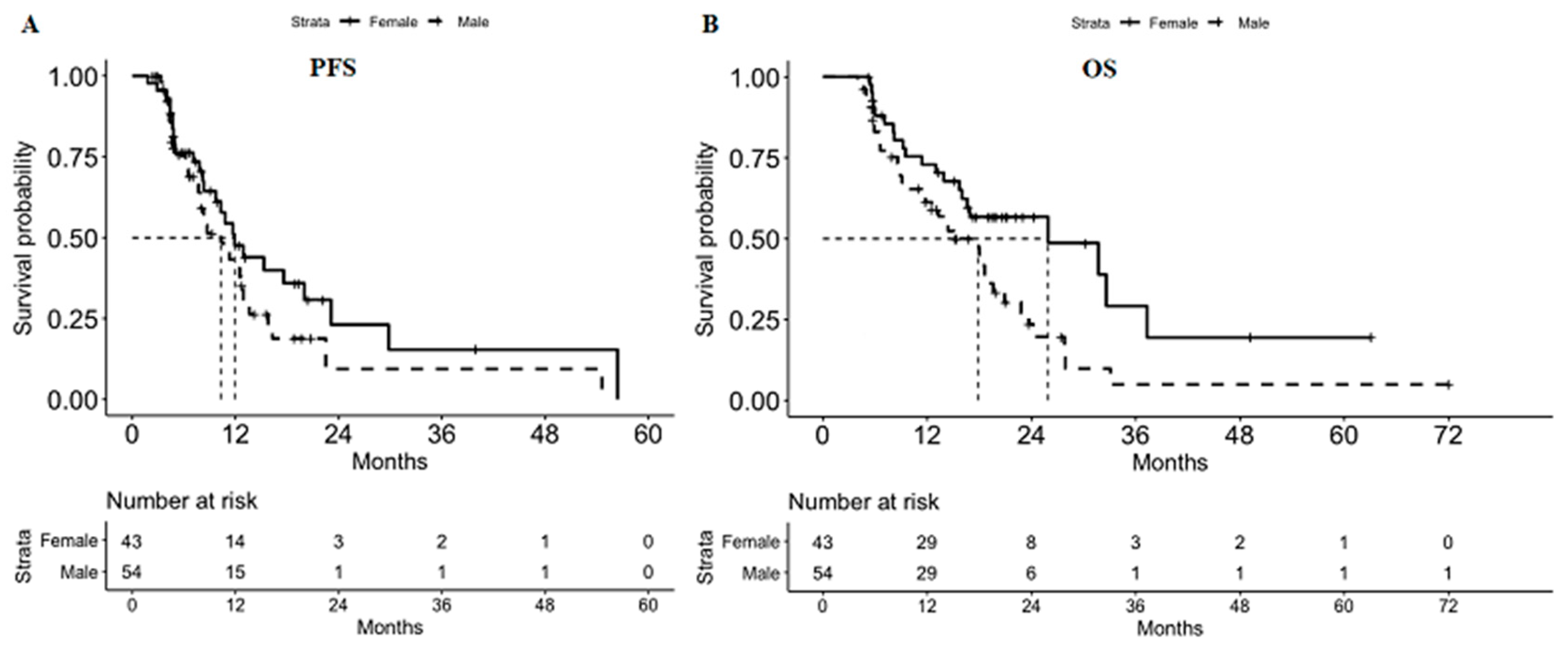
3.2. PFS and OS
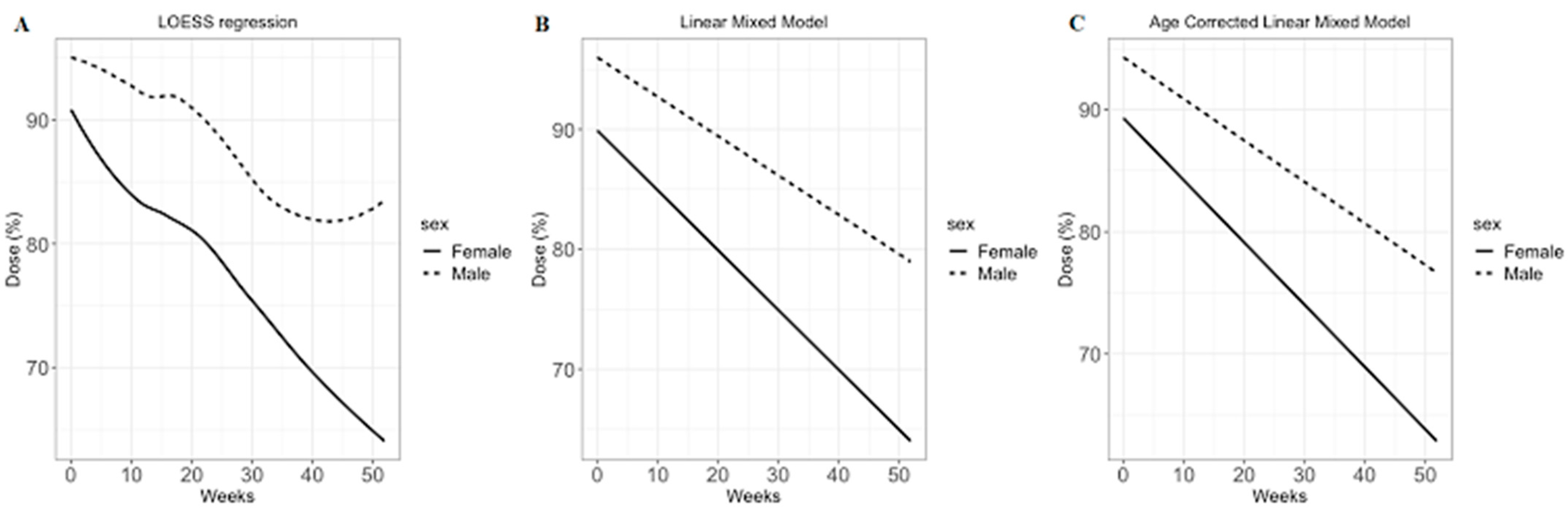
3.3. FOLFIRINOX Dose Modification Pattern
3.4. Treatment-Related Adverse Events and the Number of Visits to the Emergency Department
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic adenocarcinoma. N. Engl. J. Med. 2014, 371, 2140–2141. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A.; Schwarz, L.; Borbath, I.; Henry, A.; Van Laethem, J.L.; Malka, D.; Ducreux, M.; Conroy, T. An update on treatment options for pancreatic adenocarcinoma. Ther. Adv. Med. Oncol. 2019, 11, 1758835919875568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.I.; Lim, H.; Moon, A. Sex Differences in Cancer: Epidemiology, Genetics and Therapy. Biomol. Ther. (Seoul) 2018, 26, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Milano, G.; Etienne, M.C.; Cassuto-Viguier, E.; Thyss, A.; Santini, J.; Frenay, M.; Renee, N.; Schneider, M.; Demard, F. Influence of sex and age on fluorouracil clearance. J. Clin. Oncol. 1992, 10, 1171–1175. [Google Scholar] [CrossRef] [PubMed]
- Sloan, J.A.; Goldberg, R.M.; Sargent, D.J.; Vargas-Chanes, D.; Nair, S.; Cha, S.S.; Novotny, P.J.; Poon, M.A.; O’Connell, M.J.; Loprinzi, C.L. Women experience greater toxicity with fluorouracil-based chemotherapy for colorectal cancer. J. Clin. Oncol. 2002, 20, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Hohla, F.; Hopfinger, G.; Romeder, F.; Rinnerthaler, G.; Bezan, A.; Stattner, S.; Hauser-Kronberger, C.; Ulmer, H.; Greil, R. Female gender may predict response to FOLFIRINOX in patients with unresectable pancreatic cancer: A single institution retrospective review. Int. J. Oncol. 2014, 44, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A.; Jarlier, M.; Gourgou Bourgade, S.; Conroy, T. Response to FOLFIRINOX by gender in patients with metastatic pancreatic cancer: Results from the PRODIGE 4/ ACCORD 11 randomized trial. PLoS ONE 2017, 12, e0183288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.C.; Kim, J.W.; Ahn, S.; Kim, H.W.; Lee, J.; Kim, Y.H.; Paik, K.H.; Kim, J.; Hwang, J.H. Optimal dose reduction of FOLFIRINOX for preserving tumour response in advanced pancreatic cancer: Using cumulative relative dose intensity. Eur. J. Cancer 2017, 76, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Hryniuk, W.; Bush, H. The importance of dose intensity in chemotherapy of metastatic breast cancer. J. Clin. Oncol. 1984, 2, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.D.; Oertelt-Prigione, S.; Adjei, A.; Buclin, T.; Cristina, V.; Csajka, C.; Coukos, G.; Dafni, U.; Dotto, G.P.; Ducreux, M.; et al. Gender medicine and oncology: Report and consensus of an ESMO workshop. Ann. Oncol. 2019, 30, 1914–1924. [Google Scholar] [CrossRef] [Green Version]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of lean bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef] [PubMed]
- Mueller, F.; Buchel, B.; Koberle, D.; Schurch, S.; Pfister, B.; Krahenbuhl, S.; Froehlich, T.K.; Largiader, C.R.; Joerger, M. Gender-specific elimination of continuous-infusional 5-fluorouracil in patients with gastrointestinal malignancies: Results from a prospective population pharmacokinetic study. Cancer Chemother. Pharmacol. 2013, 71, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.K.; Buckner, J.C.; Galanis, E.; Jaeckle, K.A.; Ames, M.M.; Reid, J.M. Quantification of the impact of enzyme-inducing antiepileptic drugs on irinotecan pharmacokinetics and SN-38 exposure. J. Clin. Pharmacol. 2015, 55, 1303–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, C.E.; Gupta, E.; Reid, J.M.; Atherton, P.J.; Sloan, J.A.; Pitot, H.C.; Ratain, M.J.; Kastrissios, H. Population pharmacokinetic model for irinotecan and two of its metabolites, SN-38 and SN-38 glucuronide. Clin. Pharmacol. Ther. 2002, 72, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Infante, J.R.; Keedy, V.L.; Jones, S.F.; Chan, E.; Bendell, J.C.; Lee, W.; Zamboni, B.A.; Ikeda, S.; Kodaira, H.; et al. Population pharmacokinetics of PEGylated liposomal CPT-11 (IHL-305) in patients with advanced solid tumors. Eur. J. Clin. Pharmacol. 2013, 69, 2073–2081. [Google Scholar] [CrossRef] [PubMed]
- Cristina, V.; Mahachie, J.; Mauer, M.; Buclin, T.; Van Cutsem, E.; Roth, A.; Wagner, A.D. Association of Patient Sex With Chemotherapy-Related Toxic Effects: A Retrospective Analysis of the PETACC-3 Trial Conducted by the EORTC Gastrointestinal Group. JAMA Oncol. 2018, 4, 1003–1006. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Men (N = 54) | Women (N = 43) | Total (N = 97) | p | |
|---|---|---|---|---|
| Age, years | 0.005 | |||
| Median | 58.8 | 64.9 | 61.1 | |
| Range | 55.0–64.2 | 58.7–69.9 | 55.9–68.7 | |
| Tumor location, no. (%) | 0.211 | |||
| Head | 19 (35.8) | 21 (48.8) | 40 (41.7) | |
| Body | 7 (13.2) | 6 (14) | 13 (13.5) | |
| Tail | 26 (49.1) | 13 (30.2) | 39 (40.6) | |
| Multiple | 1 (1.9) | 3 (7) | 4 (4.2) | |
| Metastatic site, no. (%) | 0.704 | |||
| Liver | 30 (37.0) | 23 (36.5) | 53 (36.8) | |
| Peritoneum | 19 (23.5) | 10 (15.9) | 29 (20.1) | |
| Lung | 7 (8.6) | 9 (14.3) | 16 (11.1) | |
| Lymph node | 22 (27.2) | 19 (30.2) | 41 (28.5) | |
| Bone | 3 (3.7) | 2 (3.2) | 5 (3.5) | |
| BMI (kg/m2) | 0.248 | |||
| Median | 22.7 | 24.1 | 23.1 | |
| Range | 20.5–24.9 | 20.8–26 | 20.7–25.7 | |
| BSA (m2) | <0.001 | |||
| Median | 1.7 | 1.6 | 1.6 | |
| Range | 1.6–1.8 | 1.5–1.6 | 1.5–1.8 | |
| CA 19-9 (U/mL) | 0.413 | |||
| Median | 900.0 | 620.0 | 760.0 | |
| Range | 192.6–3800.0 | 64.0–2100.0 | 118.0–2100.0 | |
| ECOG PS score (%) | 0.326 | |||
| 0 | 21 (38.9) | 21 (48.8) | 42 (43.3) | |
| 1 | 33 (61.1) | 22 (51.2) | 55 (56.7) | |
| Use of G-CSF | 0.647 | |||
| Yes | 46 (85.2) | 38 (88.4) | 84 (86.6) | |
| No | 8 (14.8) | 5 (11.6) | 13 (13.4) | |
| Surgery (%) | 0.793 | |||
| Yes | 2 (3.7) | 3 (7.0) | 5 (5.2) | |
| No | 52 (96.3) | 40 (93.0) | 92 (94.8) | |
| Second-line chemotherapy, no. (%) | 0.733 * | |||
| Gemcitabine | 4 (7.4) | 3 (7.0) | 7 (7.2) | |
| Gemcitabine plus erlotinib | 8 (14.8) | 4 (9.3) | 12 (12.4) | |
| Gemcitabine plus cisplatin | 4 (7.4) | 2 (4.7) | 6 (6.2) | |
| Gemcitabine plus nab-paclitaxel | 8 (14.8) | 7 (16.3) | 15 (15.5) | |
| TS-1 | 3 (5.6) | 7 (16.3) | 10 (10.3) | |
| None | 27 (50.0) | 20 (46.5) | 47 (48.5) |
| Men (N = 54) | Women (N = 43) | Total (N = 97) | p | |
|---|---|---|---|---|
| Hematologic | ||||
| Neutropenia | 17 (31.5) | 20 (46.5) | 37 (38.1) | 0.192 |
| Febrile neutropenia | 6 (11.1) | 9 (20.9) | 15 (15.5) | 0.296 |
| Anemia | 0 (0.0) | 1 (2.3) | 1 (1.0) | 0.909 |
| Thrombocytopenia | 1 (1.9) | 4 (9.3) | 5 (5.2) | 0.235 |
| Non-hematologic | ||||
| Anorexia | 1 (1.9) | 1 (2.3) | 2 (2.1) | >0.99 |
| Nausea | 12 (22.2) | 8 (18.6) | 20 (20.6) | 0.853 |
| Vomiting | 6 (11.1) | 3 (7.0) | 9 (9.3) | 0.730 |
| Diarrhea | 4 (7.4) | 2 (4.7) | 6 (6.2) | 0.892 |
| Fatigue | 0 (0.0) | 2 (4.7) | 2 (2.1) | 0.378 |
| Sensory neuropathy | 7 (13.0) | 3 (7.0) | 10 (10.3) | 0.531 |
| Men (N = 54) | Women (N = 43) | Total (N = 97) | p | |
|---|---|---|---|---|
| 0.239 | ||||
| 0 | 36 (66.7) | 25 (58.1) | 61 (62.9) | |
| 1~2 | 17 (31.5) | 14 (32.6) | 31 (32.0) | |
| More than 3 | 1 (1.9) | 4 (9.3) | 5 (5.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Ji, E.; Jung, K.; Jung, I.H.; Park, J.; Lee, J.-C.; Kim, J.W.; Hwang, J.-H.; Kim, J. Gender Differences in Patients with Metastatic Pancreatic Cancer Who Received FOLFIRINOX. J. Pers. Med. 2021, 11, 83. https://doi.org/10.3390/jpm11020083
Kim J, Ji E, Jung K, Jung IH, Park J, Lee J-C, Kim JW, Hwang J-H, Kim J. Gender Differences in Patients with Metastatic Pancreatic Cancer Who Received FOLFIRINOX. Journal of Personalized Medicine. 2021; 11(2):83. https://doi.org/10.3390/jpm11020083
Chicago/Turabian StyleKim, Jinkook, Eunjeong Ji, Kwangrok Jung, In Ho Jung, Jaewoo Park, Jong-Chan Lee, Jin Won Kim, Jin-Hyeok Hwang, and Jaihwan Kim. 2021. "Gender Differences in Patients with Metastatic Pancreatic Cancer Who Received FOLFIRINOX" Journal of Personalized Medicine 11, no. 2: 83. https://doi.org/10.3390/jpm11020083
APA StyleKim, J., Ji, E., Jung, K., Jung, I. H., Park, J., Lee, J. -C., Kim, J. W., Hwang, J. -H., & Kim, J. (2021). Gender Differences in Patients with Metastatic Pancreatic Cancer Who Received FOLFIRINOX. Journal of Personalized Medicine, 11(2), 83. https://doi.org/10.3390/jpm11020083