
Different Impact of Definitions of Sarcopenia in Defining Frailty Status in a Population of Older Women with Early Breast Cancer

 , ,
, , 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sarcopenia and Frailty Definitions
2.2. Toxicities
2.3. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on February 2021).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolly, T.A.; Deal, A.M.; Nyrop, K.A.; Williams, G.R.; Pergolotti, M.; Wood, W.A.; Alston, S.M.; Gordon, B.E.; Dixon, S.A.; Moore, S.G.; et al. Geriatric Assessment-Identified Deficits in Older Cancer Patients with Normal Performance Status. Oncologist 2015, 20, 379–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paillaud, E.; Caillet, P.; Laurent, M.; Bastuji-Garin, S.; Liuu, E.; Lagrange, J.-L.; Culine, S.; Canoui-Poitrine, F. Optimal management of elderly cancer patients: Usefulness of the Comprehensive Geriatric Assessment. Clin. Interv. Aging 2014, 9, 1645–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colloca, G.; Santoro, M.; Gambassi, G. Age-related physiologic changes and perioperative management of elderly patients. Surg. Oncol. 2010, 19, 124–130. [Google Scholar] [CrossRef]
- Sedrak, M.S.; Freedman, R.A.; Cohen, H.J.; Muss, H.B.; Jatoi, A.; Klepin, H.D.; Wildes, T.M.; Le-Rademacher, J.G.; Kimmick, G.G.; Tew, W.P.; et al. Older adult participation in cancer clinical trials: A systematic review of barriers and interventions. CA Cancer J. Clin. 2021, 71, 78–92. [Google Scholar] [CrossRef]
- Singh, R.; Hellman, S.; Heimann, R. The natural history of breast carcinoma in the elderly. Cancer 2004, 100, 1807–1813. [Google Scholar] [CrossRef]
- Wildiers, H.; Kunkler, I.; Biganzoli, L.; Fracheboud, J.; Vlastos, G.; Bernard-Marty, C.; Hurria, A.; Extermann, M.; Girre, V.; Brain, E.; et al. Management of breast cancer in elderly individuals: Recommendations of the International Society of Geriatric Oncology. Lancet Oncol. 2007, 8, 1101–1115. [Google Scholar] [CrossRef]
- NICE. Early and Locally Advanced Breast Cancer: Diagnosis and Treatment. 2018. Available online: https://www.nice.org.uk/guidance/ng101 (accessed on February 2021).
- Colloca, G.; Di Capua, B.; Bellieni, A.; Fusco, D.; Ciciarello, F.; Tagliaferri, L.; Valentini, V.; Balducci, L. Biological and Functional Biomarkers of Aging: Definition, Characteristics, and How They Can Impact Everyday Cancer Treatment. Curr. Oncol. Rep. 2020, 22, 1–12. [Google Scholar] [CrossRef]
- Fusco, D.; Allocca, E.; Villani, E.R.; Franza, L.; Laudisio, A.; Colloca, G. An update in breast cancer management for elderly patients. Transl. Cancer Res. 2018, 7, S319–S328. [Google Scholar] [CrossRef]
- Extermann, M.; Aapro, M.; Bernabei, R.; Cohen, H.J.; Droz, J.-P.; Lichtman, S.; Mor, V.; Monfardini, S.; Repetto, L.; Sørbye, L.; et al. Use of comprehensive geriatric assessment in older cancer patients. Crit. Rev. Oncol. 2005, 55, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Colloca, G.; Corsonello, A.; Marzetti, E.; Balducci, L.; Landi, F.; Extermann, M.; Scambia, G.; Cesari, M.; Carreca, I.; Monfardini, S.; et al. Treating Cancer in Older and Oldest Old Patients. Curr. Pharm. Des. 2015, 21, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Bringhen, S.; Mateos, M.-V.; LaRocca, A.; Facon, T.; Kumar, S.; Offidani, M.; McCarthy, P.; Evangelista, A.; Lonial, S.; et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: An International Myeloma Working Group report. Blood 2015, 125, 2068–2074. [Google Scholar] [CrossRef]
- Corre, R.; Greillier, L.; Le Caër, H.; Audigier-Valette, C.; Baize, N.; Bérard, H.; Falchero, L.; Monnet, I.; Dansin, E.; Vergnenègre, A.; et al. Use of a Comprehensive Geriatric Assessment for the Management of Elderly Patients with Advanced Non–Small-Cell Lung Cancer: The Phase III Randomized ESOGIA-GFPC-GECP 08-02 Study. J. Clin. Oncol. 2016, 34, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Goede, V.; Bahlo, J.; Chataline, V.; Eichhorst, B.; Dürig, J.; Stilgenbauer, S.; Kolb, G.; Honecker, F.; Wedding, U.; Hallek, M. Evaluation of geriatric assessment in patients with chronic lymphocytic leukemia: Results of the CLL9 trial of the German CLL study group. Leuk. Lymphoma 2015, 57, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Kroep, J.R.; Van Werkhoven, E.; Polee, M.; Van Groeningen, C.J.; Beeker, A.; Erdkamp, F.; Weijl, N.; Van Bochove, A.; Erjavec, Z.; Kapiteijn, E.; et al. Randomised study of tegafur–uracil plus leucovorin versus capecitabine as first-line therapy in elderly patients with advanced colorectal cancer—TLC study. J. Geriatr. Oncol. 2015, 6, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildes, T.M.; O’Donovan, A.; Colloca, G.F.; Cheung, K.-L. Tumour boards in geriatric oncology. Age Ageing 2018, 47, 168–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcovich, S.; Colloca, G.; Sollena, P.; Andrea, B.; Balducci, L.; Cho, W.C.; Bernabei, R.; Peris, K. Skin Cancer Epidemics in the Elderly as An Emerging Issue in Geriatric Oncology. Aging Dis. 2017, 8, 643–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colloca, G.; Lattanzio, F.; Balducci, L.; Onder, G.; Ronconi, G.; Landi, F.; Morlans, G.; Bernabei, R. Treating Cancer and No-Cancer Pain in Older and Oldest Old Patients. Curr. Pharm. Des. 2015, 21, 1706–1714. [Google Scholar] [CrossRef]
- Luciani, A.; Biganzoli, L.; Colloca, G.; Falci, C.; Castagneto, B.; Floriani, I.; Battisti, N.; Dottorini, L.; Ferrari, D.; Fiduccia, P.; et al. Estimating the risk of chemotherapy toxicity in older patients with cancer: The role of the Vulnerable Elders Survey-13 (VES-13). J. Geriatr. Oncol. 2015, 6, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Dale, W.; Mohile, S.G.; Eldadah, B.A.; Trimble, E.L.; Schilsky, R.L.; Cohen, H.J.; Muss, H.B.; Schmader, K.E.; Ferrell, B.; Extermann, M.; et al. Biological, Clinical, and Psychosocial Correlates at the Interface of Cancer and Aging Research. J. Natl. Cancer Inst. 2012, 104, 581–589. [Google Scholar] [CrossRef] [Green Version]
- Extermann, M.; Overcash, J.; Lyman, G.H.; Parr, J.; Balducci, L. Comorbidity and functional status are independent in older cancer patients. J. Clin. Oncol. 1998, 16, 1582–1587. [Google Scholar] [CrossRef]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting Chemotherapy Toxicity in Older Adults with Cancer: A Prospective Multicenter Study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colloca, G.; Tagliaferri, L.; Di Capua, B.; Gambacorta, M.A.; Lanzotti, V.; Bellieni, A.; Monfardini, S.; Balducci, L.; Bernabei, R.; Cho, W.C.; et al. Management of The Elderly Cancer Patients Complexity: The Radiation Oncology Potential. Aging Dis. 2020, 11, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Repetto, L.; Fratino, L.; Audisio, R.A.; Venturino, A.; Gianni, W.; Vercelli, M.; Parodi, S.; Lago, D.D.; Gioia, F.; Monfardini, S.; et al. Comprehensive Geriatric Assessment Adds Information to Eastern Cooperative Oncology Group Performance Status in Elderly Cancer Patients: An Italian Group for Geriatric Oncology Study. J. Clin. Oncol. 2002, 20, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low Relative Skeletal Muscle Mass (Sarcopenia) in Older Persons Is Associated with Functional Impairment and Physical Disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [Green Version]
- Colloca, G.; Di Capua, B.; Bellieni, A.; Cesari, M.; Marzetti, E.; Valentini, V.; Calvani, R. Muscoloskeletal aging, sarcopenia and cancer. J. Geriatr. Oncol. 2019, 10, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Pahor, M.; Manini, T.; Cesari, M. Sarcopenia: Clinical evaluation, biological markers and other evaluation tools. J. Nutr. Health Aging 2009, 13, 724–728. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the Biological Substrate of Physical Frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Feliciano, E.M.C.; Kroenke, C.H.; Meyerhardt, J.A.; Prado, C.M.; Bradshaw, P.T.; Dannenberg, A.J.; Kwan, M.L.; Xiao, J.; Quesenberry, C.; Weltzien, E.K.; et al. Metabolic Dysfunction, Obesity, and Survival Among Patients with Early-Stage Colorectal Cancer. J. Clin. Oncol. 2016, 34, 3664–3671. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of Sarcopenia among the Elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaap, L.A.; Van Schoor, N.M.; Lips, P.; Visser, M. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1199–1204. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Fusco, D.; Ferrini, A.; Pasqualetti, G.; Giannotti, C.; Cesari, M.; Laudisio, A.; Ballestrero, A.; Scabini, S.; Odetti, P.R.; Colloca, G.F.; et al. Comprehensive geriatric assessment in older adults with cancer: Recommendations by the Italian Society of Geriatrics and Gerontology (SIGG). Eur. J. Clin. Investig. 2021, 51, e13347. [Google Scholar] [CrossRef]
- Sorensen, J.B.; Klee, M.R.; Palshof, T.; Hansen, H.H. Performance status assessment in cancer patients. An inter-observer variability study. Br. J. Cancer 1993, 67, 773–775. [Google Scholar] [CrossRef] [Green Version]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, A.E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Cockrell, J.R.; Folstein, M.F. Mini-Mental State Examination (MMSE). Psychopharmacol. Bull. 1988, 24, 689–692. [Google Scholar] [PubMed]
- Guigoz, P.Y.; Vellas, M.B.; Garry, P.P.J. Assessing the Nutritional Status of the Elderly: The Mini Nutritional Assessment as Part of the Geriatric Evaluation. Nutr. Rev. 2009, 54, S59–S65. [Google Scholar] [CrossRef] [PubMed]
- Conradsson, M.; Rosendahl, E.; Littbrand, H.; Gustafson, Y.; Olofsson, B.; Lövheim, H. Usefulness of the Geriatric Depression Scale 15-item version among very old people with and without cognitive impairment. Aging Ment. Health 2013, 17, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; Di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [Green Version]
- Bischoff, H.A.; Stähelin, H.B.; Monsch, A.U.; Iversen, M.D.; Weyh, A.; von Dechend, M.; Akos, R.; Conzelmann, M.; Dick, W.; Theiler, R. Identifying a cut-off point for normal mobility: A comparison of the timed ’up and go’ test in community-dwelling and institutionalised elderly women. Age Ageing 2003, 32, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.; Jagger, C.; et al. Grip Strength across the Life Course: Normative Data from Twelve British Studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Kritchevsky, S.B.; Newman, A.B.; Simonsick, E.M.; Harris, T.B.; Penninx, B.W.; Pt, J.S.B.; Tylavsky, F.A.; Satterfield, S.; Bauer, D.C.; et al. Added Value of Physical Performance Measures in Predicting Adverse Health-Related Events: Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2009, 57, 251–259. [Google Scholar] [CrossRef]
- Balducci, L.; Beghe, C. The application of the principles of geriatrics to the management of the older person with cancer. Crit. Rev. Oncol. 2000, 35, 147–154. [Google Scholar] [CrossRef]
- Balducci, L.; Colloca, G.; Cesari, M.; Gambassi, G. Assessment and treatment of elderly patients with cancer. Surg. Oncol. 2010, 19, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Dubianski, R.; Wildes, T.M.; Wildiers, H. SIOG guidelines-essential for good clinical practice in geriatric oncology. J. Geriatr. Oncol. 2019, 10, 196–198. [Google Scholar] [CrossRef]
- McGregor, R.A.; Cameron-Smith, D.; Poppitt, S.D. It is not just muscle mass: A review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev. Healthspan 2014, 3, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, D.R. Loss of skeletal muscle mass in aging: Examining the relationship of starvation, sarcopenia and cachexia. Clin. Nutr. 2007, 26, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J.A.; Schmitz, K.H.; Berger, N.A. Sarcopenia in aging, obesity, and cancer. Transl. Cancer Res. 2020, 9, 5760–5771. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Damanti, S.; Colloca, G.F.; Ferrini, A.; Consonni, D.; Cesari, M. Sarcopenia (and sarcopenic obesity) in older patients with gynecological malignancies. J. Geriatr. Oncol. 2020. [Google Scholar] [CrossRef]
- Prado, C.M.; Baracos, V.E.; McCargar, L.J.; Reiman, T.; Mourtzakis, M.; Tonkin, K.; Mackey, J.R.; Koski, S.; Pituskin, E.; Sawyer, M.B. Sarcopenia as a Determinant of Chemotherapy Toxicity and Time to Tumor Progression in Metastatic Breast Cancer Patients Receiving Capecitabine Treatment. Clin. Cancer Res. 2009, 15, 2920–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villaseñor, A.; Ballard-Barbash, R.; Baumgartner, K.B.; Baumgartner, R.N.; Bernstein, L.; McTiernan, A.; Neuhouser, M.L. Prevalence and prognostic effect of sarcopenia in breast cancer survivors: The HEAL Study. J. Cancer Surviv. 2012, 6, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Vledder, M.G.; Levolger, S.; Ayez, N.; Verhoef, C.; Tran, T.C.K.; Ijzermans, J.N.M. Body composition and outcome in patients undergoing resection of colorectal liver metastases19. BJS 2012, 99, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Kazemi-Bajestani, S.M.R.; Mazurak, V.C.; Baracos, V. Computed tomography-defined muscle and fat wasting are associated with cancer clinical outcomes. Semin. Cell Dev. Biol. 2016, 54, 2–10. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Lee, Y.; Chung, Y.-S.; Lee, D.-J.; Joo, N.-S.; Hong, D.; Song, G.E.; Kim, H.-J.; Choi, Y.J.; Kim, K.-M. Prevalence of Sarcopenia and Sarcopenic Obesity in the Korean Population Based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N. Body Composition in Healthy Aging. Ann. N. Y. Acad. Sci. 2006, 904, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Aleixo, G.F.P.; Williams, G.R.; Nyrop, K.A.; Muss, H.B.; Shachar, S.S. Muscle composition and outcomes in patients with breast cancer: Meta-analysis and systematic review. Breast Cancer Res. Treat. 2019, 177, 569–579. [Google Scholar] [CrossRef]
- Desmedt, C.; Fornili, M.; Clatot, F.; Demicheli, R.; De Bortoli, D.; Di Leo, A.; Viale, G.; De Azambuja, E.; Crown, J.; Francis, P.A.; et al. Differential Benefit of Adjuvant Docetaxel-Based Chemotherapy in Patients with Early Breast Cancer According to Baseline Body Mass Index. J. Clin. Oncol. 2020, 38, 2883–2891. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.M.; Groessl, E.J.; et al. Effect of Structured Physical Activity on Prevention of Major Mobility Disability in Older Adults. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
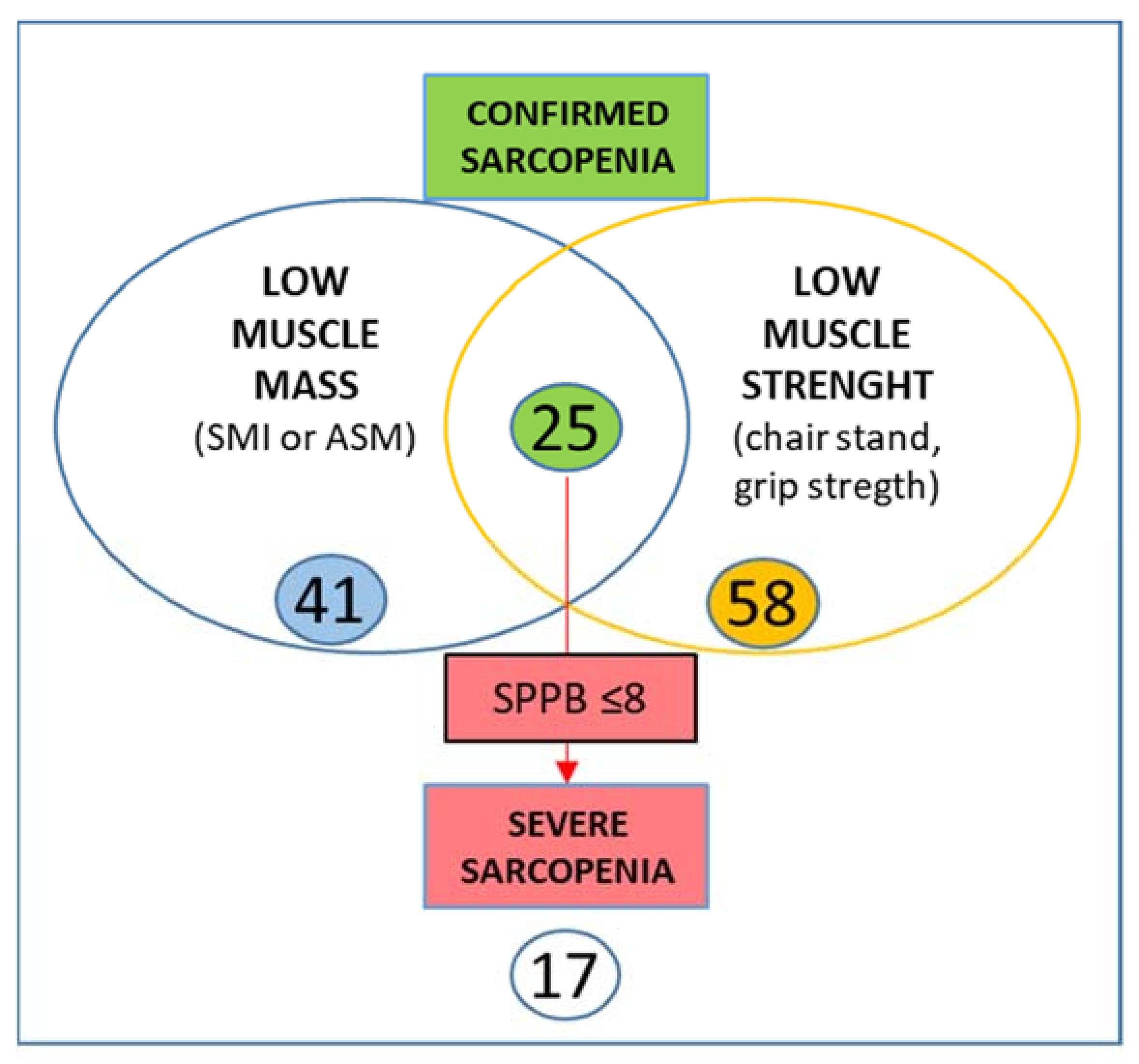
| Criteria: | Suggested Measures and Cut-offs (for Women) |
|---|---|
| (1) Low muscle strength | Grip strength, <16 kg Chair standing, >15 s for five rises |
| (2) Low muscle quantity or quality | ASM (appendicular skeletal muscle mass), <15 kg SMI (Skeletal Muscle Index): ASM/height2, <5.5 kg/m2 |
| (3) Low physical performance | Gait speed, ≤0.8 m/s Short Physical Performance Battery (SPPB), ≤8 points score Timed Up-and-Go Test, ≥20 s 400 m walk test, noncompletion or ≥6 min for completion |
| Definitions: Probable sarcopenia is identified by Criterion 1. Confirmed sarcopenia: both Criterion 1 and Criterion 2 are satisfied. Severe sarcopenia: if Criteria 1, 2 and 3 are all met. | |
| N. of Patients | % | |
|---|---|---|
| Histotype | 96 | 100 |
| Invasive Ductal Carcinoma | 72 | 75 |
| Invasive Lobular Carcinoma | 14 | 14.6 |
| other | 10 | 9.6 |
| STAGE | ||
| 0 | 1 | 1 |
| I | 45 | 46.9 |
| II | 37 | 38.5 |
| IIIa | 10 | 10.4 |
| IIIb | 3 | 3.1 |
| ECOG Performance status | ||
| 0–1 | 86 | 89.6 |
| ≥2 | 9 | 9.4 |
| Breast Surgery | ||
| Conservative | 82 | 85.4 |
| Mastectomy | 14 | 14.58 |
| Axillary Surgery | ||
| None | 17 | 17.7 |
| Sentinel Lymph Node | 38 | 39.6 |
| Lymph Node Sampling | 21 | 21.9 |
| Lymphadenectomy | 13 | 13.5 |
| Adjuvant Treatments | ||
| Chemotherapy | 19 | 19.8 |
| Radiotherapy | 62 | 64.6 |
| Hormone therapy | 82 | 85.4 |
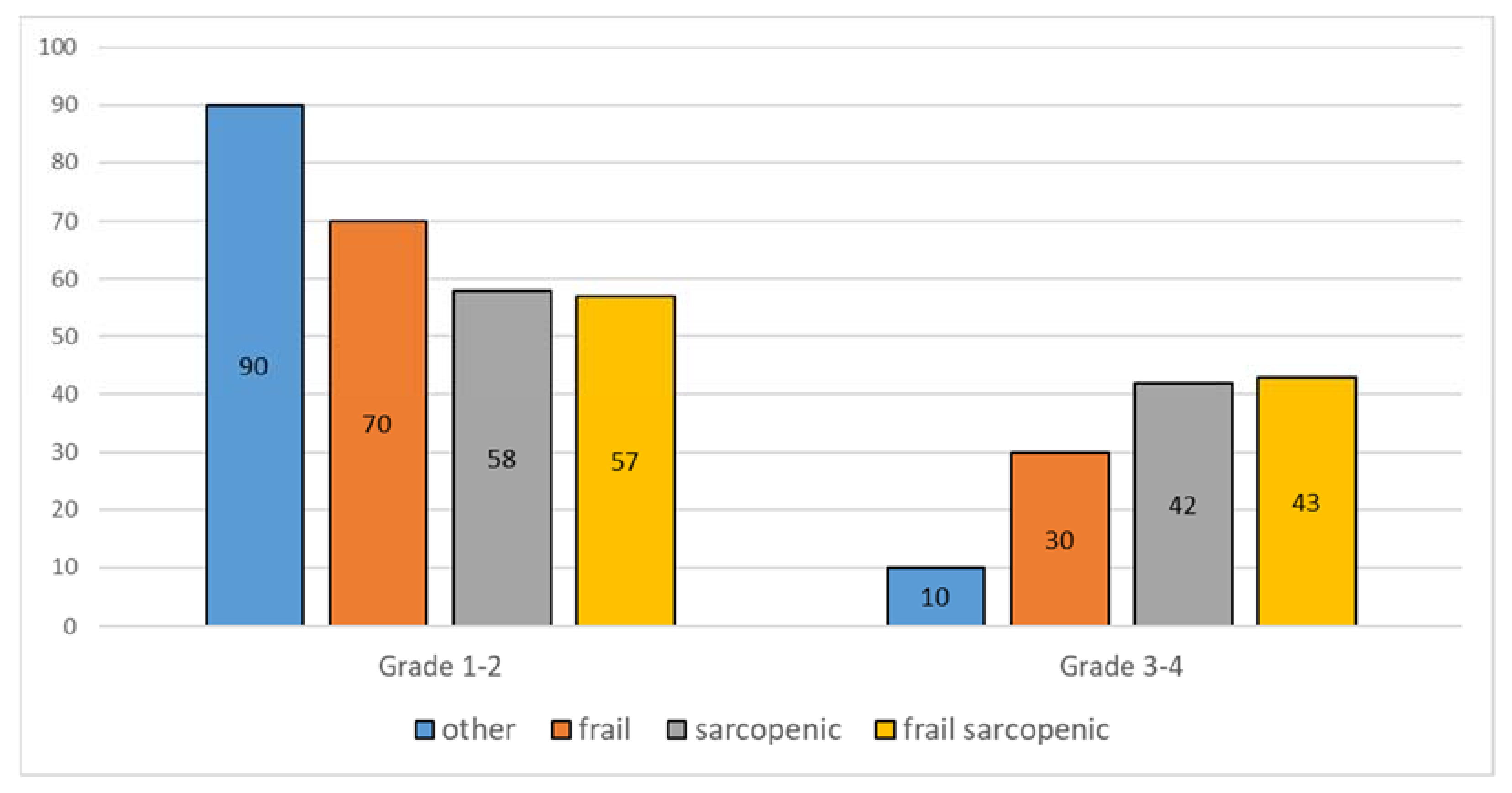
| Toxicities | 52 | 100 |
| Grade 1–2 | 42 | 81 |
| Grade 3–4 | 10 | 19 |
| Parameters | Nonfrail Patients | Frail Patients | ||||||
|---|---|---|---|---|---|---|---|---|
| N | N | Mean | Std. Dev. | N | Mean | Std. Dev. | p < 0.05 | |
| AGE | 96 | 61 | 75.6 | 3.88 | 35 | 79 | 4.994 | 0.000 |
| CCI | 96 | 61 | 6.11 | 1.462 | 35 | 7.71 | 2.163 | 0.01 |
| FRIED criteria | 96 | 61 | 1.13 | 1.049 | 35 | 2.88 | 1.066 | 0.000 |
| ADL | 96 | 61 | 5.72 | 0.488 | 35 | 5 | 0.97 | 0.000 |
| IADL | 96 | 61 | 7.64 | 0.895 | 35 | 5.4 | 2.316 | 0.000 |
| MMSE | 96 | 61 | 27.88 | 2.345 | 35 | 25.09 | 3.76 | 0.001 |
| MNA | 93 | 60 | 25.87 | 2.262 | 33 | 23.12 | 3.517 | 0.001 |
| GDS | 85 | 58 | 3.47 | 2.617 | 27 | 6.19 | 3.903 | 0.000 |
| SPPB | 96 | 61 | 9.38 | 1.823 | 35 | 4.66 | 2.3 | 0.000 |
| TUGT | 75 | 49 | 10.29 | 2.227 | 26 | 16.76 | 6.018 | 0.000 |
| SPEEDs | 90 | 58 | 4.27 | 1.099 | 32 | 7.32 | 3.532 | 0.000 |
| HANDGRIP | 66 | 40 | 17.51 | 4.695 | 26 | 11.77 | 5.279 | 0.002 |
| BMI | 96 | 61 | 28.18 | 4.598 | 35 | 28.71 | 5.723 | 0.01 |
| POLYPHARMACY Mean number of drugs | 96 | 61 | 4.79 | 2.583 | 35 | 6.34 | 2.449 | 0.001 |
| SMI | 96 | 61 | 6.46 | 0.73 | 35 | 6.51 | 1.134 | 0.959 |
| ASM | 96 | 61 | 15.7 | 2.1 | 35 | 15.7 | 3 | 0.988 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellieni, A.; Fusco, D.; Sanchez, A.M.; Franceschini, G.; Di Capua, B.; Allocca, E.; Di Stasio, E.; Marazzi, F.; Tagliaferri, L.; Masetti, R.; et al. Different Impact of Definitions of Sarcopenia in Defining Frailty Status in a Population of Older Women with Early Breast Cancer. J. Pers. Med. 2021, 11, 243. https://doi.org/10.3390/jpm11040243
Bellieni A, Fusco D, Sanchez AM, Franceschini G, Di Capua B, Allocca E, Di Stasio E, Marazzi F, Tagliaferri L, Masetti R, et al. Different Impact of Definitions of Sarcopenia in Defining Frailty Status in a Population of Older Women with Early Breast Cancer. Journal of Personalized Medicine. 2021; 11(4):243. https://doi.org/10.3390/jpm11040243
Chicago/Turabian StyleBellieni, Andrea, Domenico Fusco, Alejandro Martin Sanchez, Gianluca Franceschini, Beatrice Di Capua, Elena Allocca, Enrico Di Stasio, Fabio Marazzi, Luca Tagliaferri, Riccardo Masetti, and et al. 2021. "Different Impact of Definitions of Sarcopenia in Defining Frailty Status in a Population of Older Women with Early Breast Cancer" Journal of Personalized Medicine 11, no. 4: 243. https://doi.org/10.3390/jpm11040243
APA StyleBellieni, A., Fusco, D., Sanchez, A. M., Franceschini, G., Di Capua, B., Allocca, E., Di Stasio, E., Marazzi, F., Tagliaferri, L., Masetti, R., Bernabei, R., & Colloca, G. F. (2021). Different Impact of Definitions of Sarcopenia in Defining Frailty Status in a Population of Older Women with Early Breast Cancer. Journal of Personalized Medicine, 11(4), 243. https://doi.org/10.3390/jpm11040243