Targeting Lyn Kinase in Chorea-Acanthocytosis: A Translational Treatment Approach in a Rare Disease

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Dasatinib Treatment
2.2. Evaluation of Dasatinib Treatment
2.3. Serum Neurofilament Light Chain Quantification
2.4. Immunoblot Analysis
2.5. Immunofluorescence
2.6. Osmotic Fragility of Red Blood Cells
2.7. Statistical Analysis
3. Results
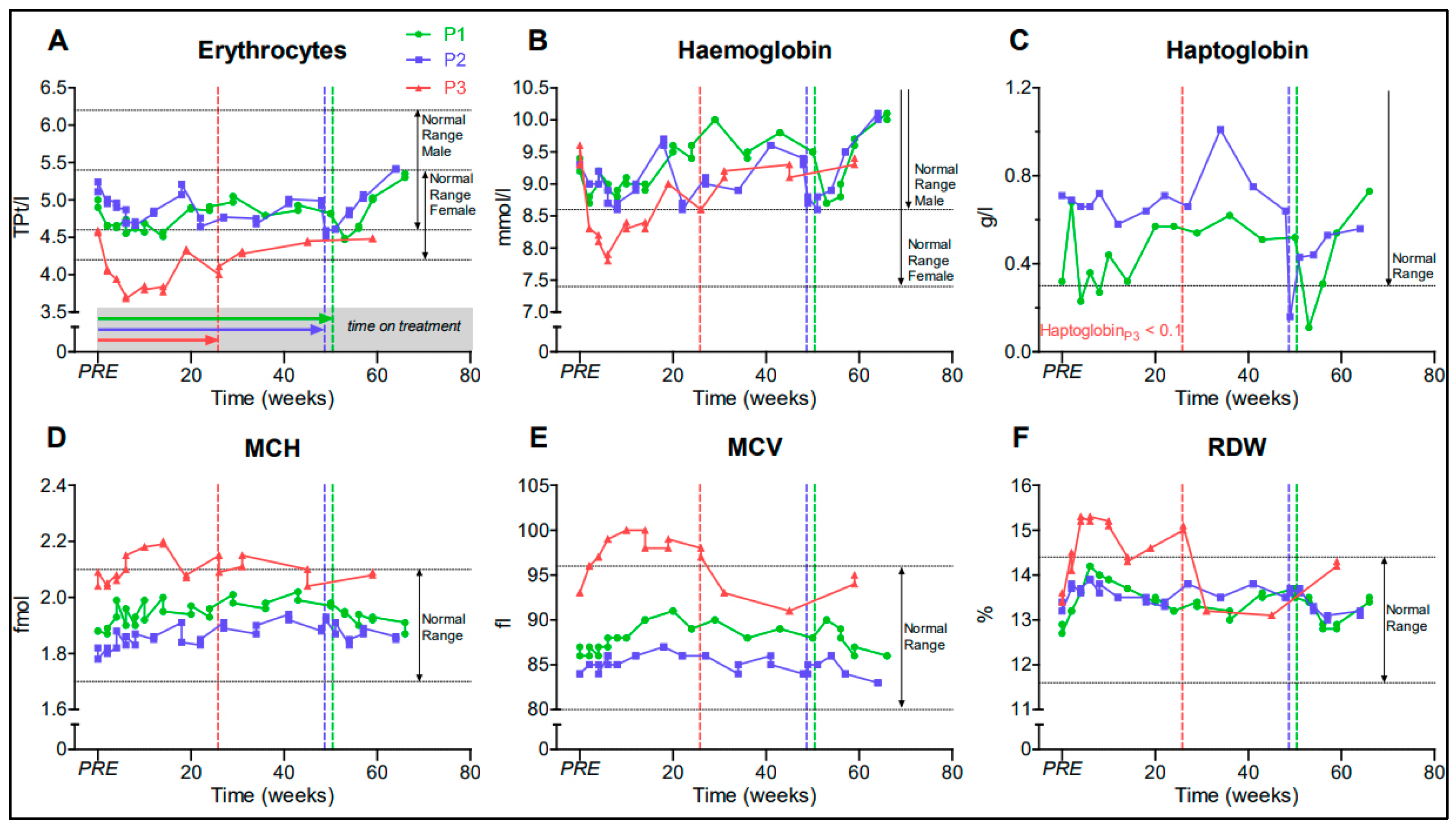
3.1. Dasatinib Treatment Was Safe
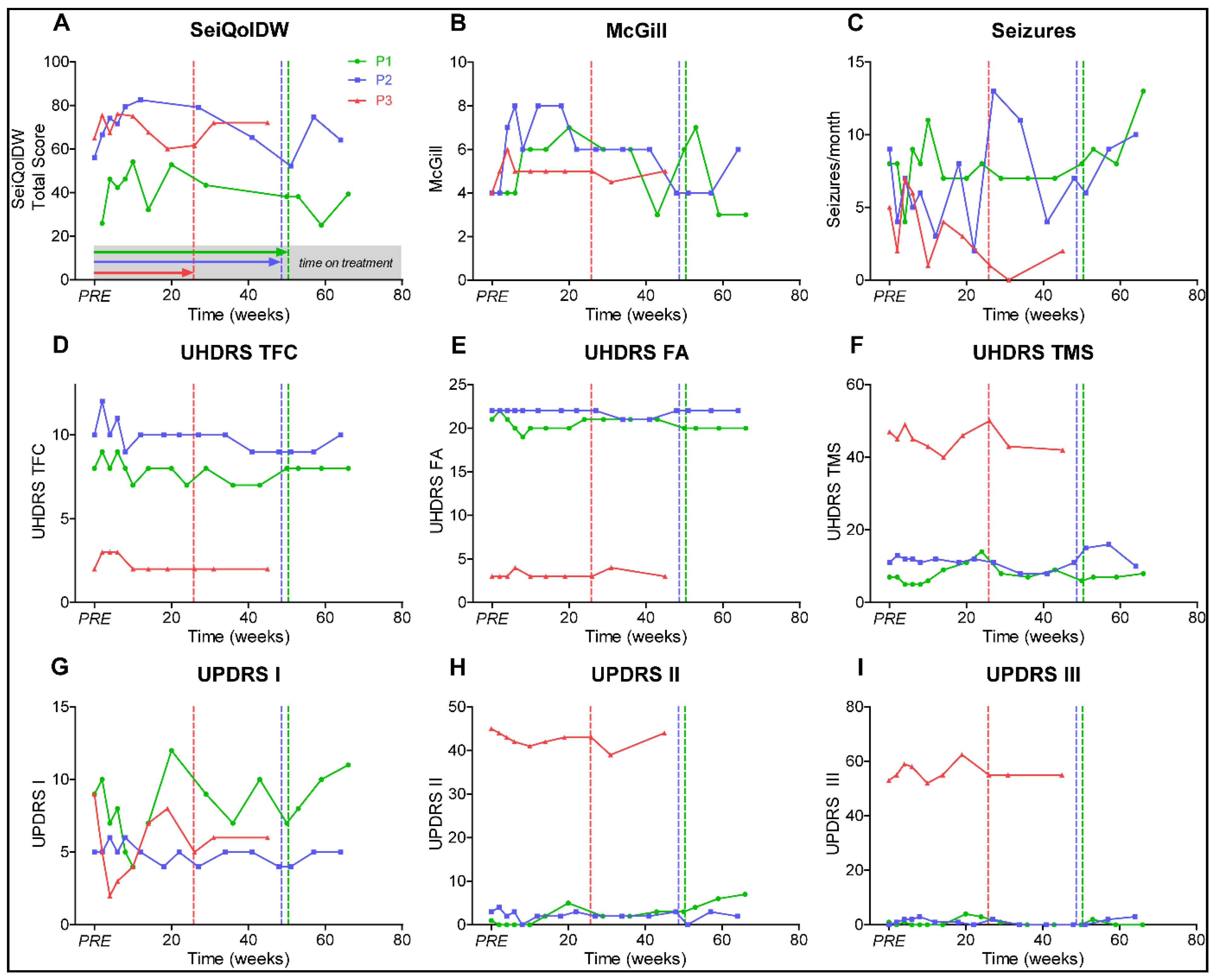
3.2. Disease Progression Remained Stable during Dasatinib Treatment in ChAc Patients
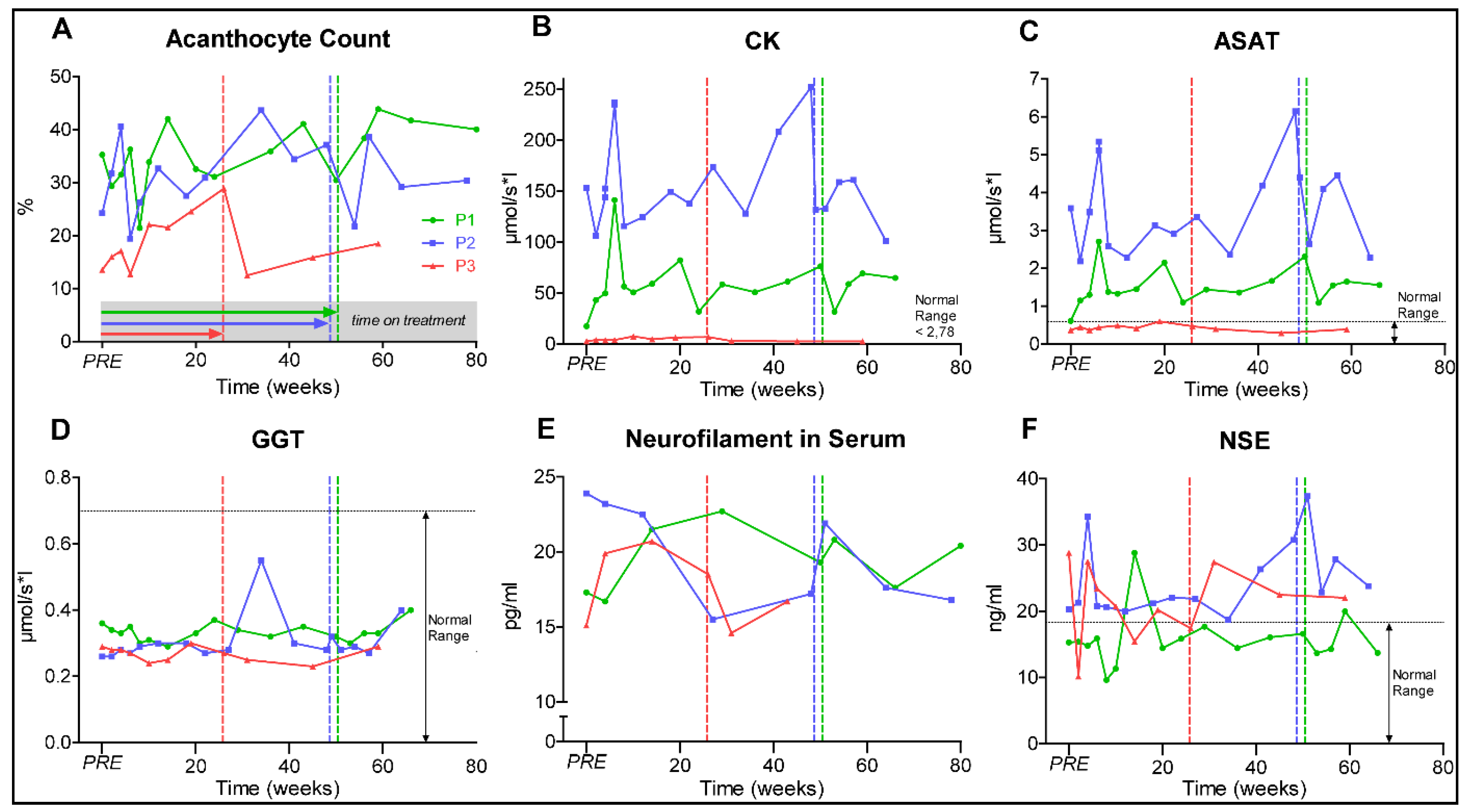
3.3. Identification of Robust Biomarkers Is Still an Unmet Need in Chorea-Acanthocytosis
3.4. Dasatinib Treatment Prevented Accumulation of Lyn and Autophagy-Related Proteins and Improved Features of ChAc RBCs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
References
- Jung, H.H.; Danek, A.; Walker, R.H. Neuroacanthocytosis syndromes. Orphanet J. Rare Dis. 2011, 6, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velayos Baeza, A.; Dobson-Stone, C.; Rampoldi, L.; Bader, B.; Walker, R.H.; Danek, A.; Monaco, A.P. Chorea-Acanthocytosis. In GeneReviews; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Stephens, K., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Walker, R.H.; Danek, A. “Neuroacanthocytosis”—Overdue for a Taxonomic Update. Tremor Other Hyperkinet. Mov. (N. Y.) 2021, 11, 1. [Google Scholar] [CrossRef]
- Peikert, K.; Danek, A.; Hermann, A. Current state of knowledge in Chorea-Acanthocytosis as core Neuroacanthocytosis syndrome. Eur. J. Med. Genet. 2018, 61, 699–705. [Google Scholar] [CrossRef]
- Danek, A.; Bader, B.; Velayos-Baeza, A.; Walker, R.H. Autosomal recessive transmission of chorea-acanthocytosis confirmed. Acta Neuropathol. 2012, 123, 905–906. [Google Scholar] [CrossRef] [Green Version]
- Dobson-Stone, C.; Danek, A.; Rampoldi, L.; Hardie, R.J.; Chalmers, R.M.; Wood, N.W.; Bohlega, S.; Dotti, M.T.; Federico, A.; Shizuka, M.; et al. Mutational spectrum of the CHAC gene in patients with chorea-acanthocytosis. Eur. J. Hum. Genet. EJHG 2002, 10, 773–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rampoldi, L.; Dobson-Stone, C.; Rubio, J.P.; Danek, A.; Chalmers, R.M.; Wood, N.W.; Verellen, C.; Ferrer, X.; Malandrini, A.; Fabrizi, G.M.; et al. A conserved sorting-associated protein is mutant in chorea-acanthocytosis. Nat. Genet. 2001, 28, 119. [Google Scholar] [CrossRef] [PubMed]
- Ueno, S.-I.; Maruki, Y.; Nakamura, M.; Tomemori, Y.; Kamae, K.; Tanabe, H.; Yamashita, Y.; Matsuda, S.; Kaneko, S.; Sano, A. The gene encoding a newly discovered protein, chorein, is mutated in chorea-acanthocytosis. Nat. Genet. 2001, 28, 121. [Google Scholar] [CrossRef]
- Walker, R.H. Management of Neuroacanthocytosis Syndromes. Tremor Other Hyperkinet. Mov. (N. Y.) 2015, 5, 346. [Google Scholar] [CrossRef]
- Rampoldi, L.; Danek, A.; Monaco, A.P. Clinical features and molecular bases of neuroacanthocytosis. J. Mol. Med. (Berl. Ger.) 2002, 80, 475–491. [Google Scholar] [CrossRef]
- Estevez-Fraga, C.; Lopez-Sendon Moreno, J.L.; Martinez-Castrillo, J.C. Phenomenology and disease progression of chorea-acanthocytosis patients in Spain. Parkinsonism Relat. Disord. 2018, 49, 17–21. [Google Scholar] [CrossRef]
- Hermann, A.; Walker, R.H. Diagnosis and treatment of chorea syndromes. Curr. Neurol. Neurosci. Rep. 2015, 15, 514. [Google Scholar] [CrossRef] [PubMed]
- Peikert, K.; Akgün, K.; Beste, C.; Ziemssen, T.; Buhmann, C.; Danek, A.; Hermann, A. Neurofilament light chain in serum is significantly increased in chorea-acanthocytosis. Parkinsonism Relat. Disord. 2020, 80, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Heinsen, H.; Grinberg, L.T.; Alho, E.; Amaro, E., Jr.; Pasqualucci, C.A.; Rub, U.; den Dunnen, W.; Arzberger, T.; Schmitz, C.; et al. Subcortical neurodegeneration in chorea: Similarities and differences between chorea-acanthocytosis and Huntington’s disease. Parkinsonism Relat. Disord. 2018, 49, 54–59. [Google Scholar] [CrossRef]
- Liu, J.; Heinsen, H.; Grinberg, L.T.; Alho, E.; Amaro, E., Jr.; Pasqualucci, C.A.; Rub, U.; Seidel, K.; den Dunnen, W.; Arzberger, T.; et al. Pathoarchitectonics of the cerebral cortex in chorea-acanthocytosis and HD. Neuropathol. Appl. Neurobiol. 2018, 45, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Yang, H. VPS13: A lipid transfer protein making contacts at multiple cellular locations. J. Cell Biol. 2018, 217, 3322–3324. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Leonzino, M.; Hancock-Cerutti, W.; Horenkamp, F.A.; Li, P.; Lees, J.A.; Wheeler, H.; Reinisch, K.M.; De Camilli, P. VPS13A and VPS13C are lipid transport proteins differentially localized at ER contact sites. J. Cell Biol. 2018, 217, 3625–3639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeshaw, W.M.; van der Zwaag, M.; Pinto, F.; Lahaye, L.L.; Faber, A.I.; Gomez-Sanchez, R.; Dolga, A.M.; Poland, C.; Monaco, A.P.; van IJzendoorn1, S.C.; et al. Human VPS13A is associated with multiple organelles and influences mitochondrial morphology and lipid droplet motility. eLife 2019, 8, e43561. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Neiman, A.M. XK is a partner for VPS13A: A molecular link between Chorea-Acanthocytosis and McLeod Syndrome. Mol. Biol. Cell 2020, 31, 2425–2436. [Google Scholar] [CrossRef]
- Dziurdzik, S.K.; Conibear, E. The Vps13 Family of Lipid Transporters and Its Role at Membrane Contact Sites. Int. J. Mol. Sci. 2021, 22, 2905. [Google Scholar] [CrossRef]
- Lang, F.; Pelzl, L.; Schols, L.; Hermann, A.; Foller, M.; Schaffer, T.E.; Stournaras, C. Neurons, Erythrocytes and Beyond—The Diverse Functions of Chorein. Neuro-Signals 2017, 25, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Lupo, F.; Tibaldi, E.; Matte, A.; Sharma, A.K.; Brunati, A.M.; Alper, S.L.; Zancanaro, C.; Benati, D.; Siciliano, A.; Bertoldi, M.; et al. A new molecular link between defective autophagy and erythroid abnormalities in chorea-acanthocytosis. Blood 2016, 128, 2976–2987. [Google Scholar] [CrossRef] [Green Version]
- Munoz-Braceras, S.; Calvo, R.; Escalante, R. TipC and the chorea-acanthocytosis protein VPS13A regulate autophagy in Dictyostelium and human HeLa cells. Autophagy 2015, 11, 918–927. [Google Scholar] [CrossRef] [Green Version]
- Pelzl, L.; Elsir, B.; Sahu, I.; Bissinger, R.; Singh, Y.; Sukkar, B.; Honisch, S.; Schoels, L.; Jemaa, M.; Lang, E.; et al. Lithium Sensitivity of Store Operated Ca2+ Entry and Survival of Fibroblasts Isolated from Chorea-Acanthocytosis Patients. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2017, 42, 2066–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foller, M.; Hermann, A.; Gu, S.; Alesutan, I.; Qadri, S.M.; Borst, O.; Schmidt, E.M.; Schiele, F.; vom Hagen, J.M.; Saft, C.; et al. Chorein-sensitive polymerization of cortical actin and suicidal cell death in chorea-acanthocytosis. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2012, 26, 1526–1534. [Google Scholar] [CrossRef]
- Hosseinzadeh, Z.; Hauser, S.; Singh, Y.; Pelzl, L.; Schuster, S.; Sharma, Y.; Höflinger, P.; Zacharopoulou, N.; Stournaras, C.; Rathbun, D.L.; et al. Decreased Na+/K+ ATPase Expression and Depolarized Cell Membrane in Neurons Differentiated from Chorea-Acanthocytosis Patients. Sci. Rep. 2020, 10, 8391. [Google Scholar] [CrossRef] [PubMed]
- De Franceschi, L.; Tomelleri, C.; Matte, A.; Brunati, A.M.; Bovee-Geurts, P.H.; Bertoldi, M.; Lasonder, E.; Tibaldi, E.; Danek, A.; Walker, R.H.; et al. Erythrocyte membrane changes of chorea-acanthocytosis are the result of altered Lyn kinase activity. Blood 2011, 118, 5652–5663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz-Braceras, S.; Tornero-Ecija, A.R.; Vincent, O.; Escalante, R. VPS13A is closely associated with mitochondria and is required for efficient lysosomal degradation. Dis. Models Mech. 2019, 12. [Google Scholar] [CrossRef] [Green Version]
- Stanslowsky, N.; Reinhardt, P.; Glass, H.; Kalmbach, N.; Naujock, M.; Hensel, N.; Lubben, V.; Pal, A.; Venneri, A.; Lupo, F.; et al. Neuronal Dysfunction in iPSC-Derived Medium Spiny Neurons from Chorea-Acanthocytosis Patients Is Reversed by Src Kinase Inhibition and F-Actin Stabilization. J. Neurosci. Off. J. Soc. Neurosci. 2016, 36, 12027–12043. [Google Scholar] [CrossRef] [Green Version]
- Roskoski, R., Jr. Src protein-tyrosine kinase structure, mechanism, and small molecule inhibitors. Pharmacol. Res. 2015, 94, 9–25. [Google Scholar] [CrossRef]
- Porkka, K.; Koskenvesa, P.; Lundan, T.; Rimpilainen, J.; Mustjoki, S.; Smykla, R.; Wild, R.; Luo, R.; Arnan, M.; Brethon, B.; et al. Dasatinib crosses the blood-brain barrier and is an efficient therapy for central nervous system Philadelphia chromosome-positive leukemia. Blood 2008, 112, 1005–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khairoalsindi, O.A.; Abuzinadah, A.R. Maximizing the Survival of Amyotrophic Lateral Sclerosis Patients: Current Perspectives. Neurol. Res. Int. 2018, 2018, 6534150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trias, E.; Ibarburu, S.; Barreto-Nunez, R.; Babdor, J.; Maciel, T.T.; Guillo, M.; Gros, L.; Dubreuil, P.; Diaz-Amarilla, P.; Cassina, P.; et al. Post-paralysis tyrosine kinase inhibition with masitinib abrogates neuroinflammation and slows disease progression in inherited amyotrophic lateral sclerosis. J. Neuroinflamm. 2016, 13, 177. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.S.; Hebron, M.L.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, J.N.; Anjum, M.; Pagan, F.; Torres-Yaghi, Y.; Shi, W.; et al. Nilotinib Effects on Safety, Tolerability, and Biomarkers in Alzheimer’s Disease. Ann. Neurol. 2020, 88, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Pagan, F.L.; Hebron, M.L.; Wilmarth, B.; Torres-Yaghi, Y.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, N.J.; Anjum, M.; Arellano, J.; et al. Nilotinib Effects on Safety, Tolerability, and Potential Biomarkers in Parkinson Disease: A Phase 2 Randomized Clinical Trial. JAMA Neurol. 2020, 77, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Simuni, T.; Fiske, B.; Merchant, K.; Coffey, C.S.; Klingner, E.; Caspell-Garcia, C.; Lafontant, D.E.; Matthews, H.; Wyse, R.K.; Brundin, P.; et al. Efficacy of Nilotinib in Patients With Moderately Advanced Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2020, 78, 312–320. [Google Scholar] [CrossRef]
- Dobson-Stone, C.; Velayos-Baeza, A.; Filippone, L.A.; Westbury, S.; Storch, A.; Erdmann, T.; Wroe, S.J.; Leenders, K.L.; Lang, A.E.; Dotti, M.T.; et al. Chorein detection for the diagnosis of chorea-acanthocytosis. Ann. Neurol. 2004, 56, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Kuhle, J.; Plattner, K.; Bestwick, J.P.; Lindberg, R.L.; Ramagopalan, S.V.; Norgren, N.; Nissim, A.; Malaspina, A.; Leppert, D.; Giovannoni, G.; et al. A comparative study of CSF neurofilament light and heavy chain protein in MS. Mult. Scler. J. 2013, 19, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Keshavan, A.; Heslegrave, A.; Zetterberg, H.; Schott, J.M. Stability of blood-based biomarkers of Alzheimer’s disease over multiple freeze-thaw cycles. Alzheimer’s Dement. (Amst.) 2018, 10, 448–451. [Google Scholar] [CrossRef]
- Beste, C.; Stock, A.K.; Zink, N.; Ocklenburg, S.; Akgun, K.; Ziemssen, T. How minimal variations in neuronal cytoskeletal integrity modulate cognitive control. NeuroImage 2019, 185, 129–139. [Google Scholar] [CrossRef]
- Akgün, K.; Kretschmann, N.; Haase, R.; Proschmann, U.; Kitzler, H.H.; Reichmann, H.; Ziemssen, T. Profiling individual clinical responses by high-frequency serum neurofilament assessment in MS. Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matte, A.; De Falco, L.; Federti, E.; Cozzi, A.; Iolascon, A.; Levi, S.; Mohandas, N.; Zamo, A.; Bruno, M.; Lebouef, C.; et al. Peroxiredoxin-2: A Novel Regulator of Iron Homeostasis in Ineffective Erythropoiesis. Antioxid. Redox Signal. 2018, 28, 1–14. [Google Scholar] [CrossRef]
- Beneduce, E.; Matte, A.; De Falco, L.; Mbiandjeu, S.; Chiabrando, D.; Tolosano, E.; Federti, E.; Petrillo, S.; Mohandas, N.; Siciliano, A.; et al. Fyn kinase is a novel modulator of erythropoietin signaling and stress erythropoiesis. Am. J. Hematol. 2019, 94, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honisch, S.; Gu, S.; Vom Hagen, J.M.; Alkahtani, S.; Al Kahtane, A.A.; Tsapara, A.; Hermann, A.; Storch, A.; Schols, L.; Lang, F.; et al. Chorein Sensitive Arrangement of Cytoskeletal Architecture. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2015, 37, 399–408. [Google Scholar] [CrossRef]
- Olivieri, O.; De Franceschi, L.; Bordin, L.; Manfredi, M.; Miraglia del Giudice, E.; Perrotta, S.; De Vivo, M.; Guarini, P.; Corrocher, R. Increased membrane protein phosphorylation and anion transport activity in chorea-acanthocytosis. Haematologica 1997, 82, 648–653. [Google Scholar]
- De Franceschi, L.; Fumagalli, L.; Olivieri, O.; Corrocher, R.; Lowell, C.A.; Berton, G. Deficiency of Src family kinases Fgr and Hck results in activation of erythrocyte K/Cl cotransport. J. Clin. Investig. 1997, 99, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Steegmann, J.L.; Baccarani, M.; Breccia, M.; Casado, L.F.; Garcia-Gutierrez, V.; Hochhaus, A.; Kim, D.W.; Kim, T.D.; Khoury, H.J.; Le Coutre, P.; et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia 2016, 30, 1648–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P1 | P2 | P3 | |
|---|---|---|---|
| Sex | male | male | female |
| Age at beginning of treatment (Y) | 27 | 32 | 49 |
| Age at onset (Y) | |||
| -- symptoms | -- 14 | -- 23 | -- 21 |
| -- diagnosis | -- 18 | -- 23 | -- 39 |
| Current clinical presentation |
|
|
|
| Laboratory findings |
|
|
|
| Time on dasatinib treatment (weeks) | 50.4 | 48.7 | 25.8 |
| Comedication |
|
|
|
| Main clinical observations during dasatinib treatment |
|
|
|
| Adverse reactions or events |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peikert, K.; Glaß, H.; Federti, E.; Matte, A.; Pelzl, L.; Akgün, K.; Ziemssen, T.; Ordemann, R.; Lang, F.; Patients, T.N.f.T.R.f.N.; et al. Targeting Lyn Kinase in Chorea-Acanthocytosis: A Translational Treatment Approach in a Rare Disease. J. Pers. Med. 2021, 11, 392. https://doi.org/10.3390/jpm11050392
Peikert K, Glaß H, Federti E, Matte A, Pelzl L, Akgün K, Ziemssen T, Ordemann R, Lang F, Patients TNfTRfN, et al. Targeting Lyn Kinase in Chorea-Acanthocytosis: A Translational Treatment Approach in a Rare Disease. Journal of Personalized Medicine. 2021; 11(5):392. https://doi.org/10.3390/jpm11050392
Chicago/Turabian StylePeikert, Kevin, Hannes Glaß, Enrica Federti, Alessandro Matte, Lisann Pelzl, Katja Akgün, Tjalf Ziemssen, Rainer Ordemann, Florian Lang, The Network for Translational Research for Neuroacanthocytosis Patients, and et al. 2021. "Targeting Lyn Kinase in Chorea-Acanthocytosis: A Translational Treatment Approach in a Rare Disease" Journal of Personalized Medicine 11, no. 5: 392. https://doi.org/10.3390/jpm11050392
APA StylePeikert, K., Glaß, H., Federti, E., Matte, A., Pelzl, L., Akgün, K., Ziemssen, T., Ordemann, R., Lang, F., Patients, T. N. f. T. R. f. N., De Franceschi, L., & Hermann, A. (2021). Targeting Lyn Kinase in Chorea-Acanthocytosis: A Translational Treatment Approach in a Rare Disease. Journal of Personalized Medicine, 11(5), 392. https://doi.org/10.3390/jpm11050392