
A Pharmacogenetic Study of CYP2C19 in Acute Coronary Syndrome Patients of Colombian Origin Reveals New Polymorphisms Potentially Related to Clopidogrel Therapy

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Sampling and Data Collection
2.2. Genotyping of the Promoter and Coding Regions of CYP2C19
2.3. Platelet Function Test
2.4. Adverse Reactions and Causality Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical and Demographic Characteristics
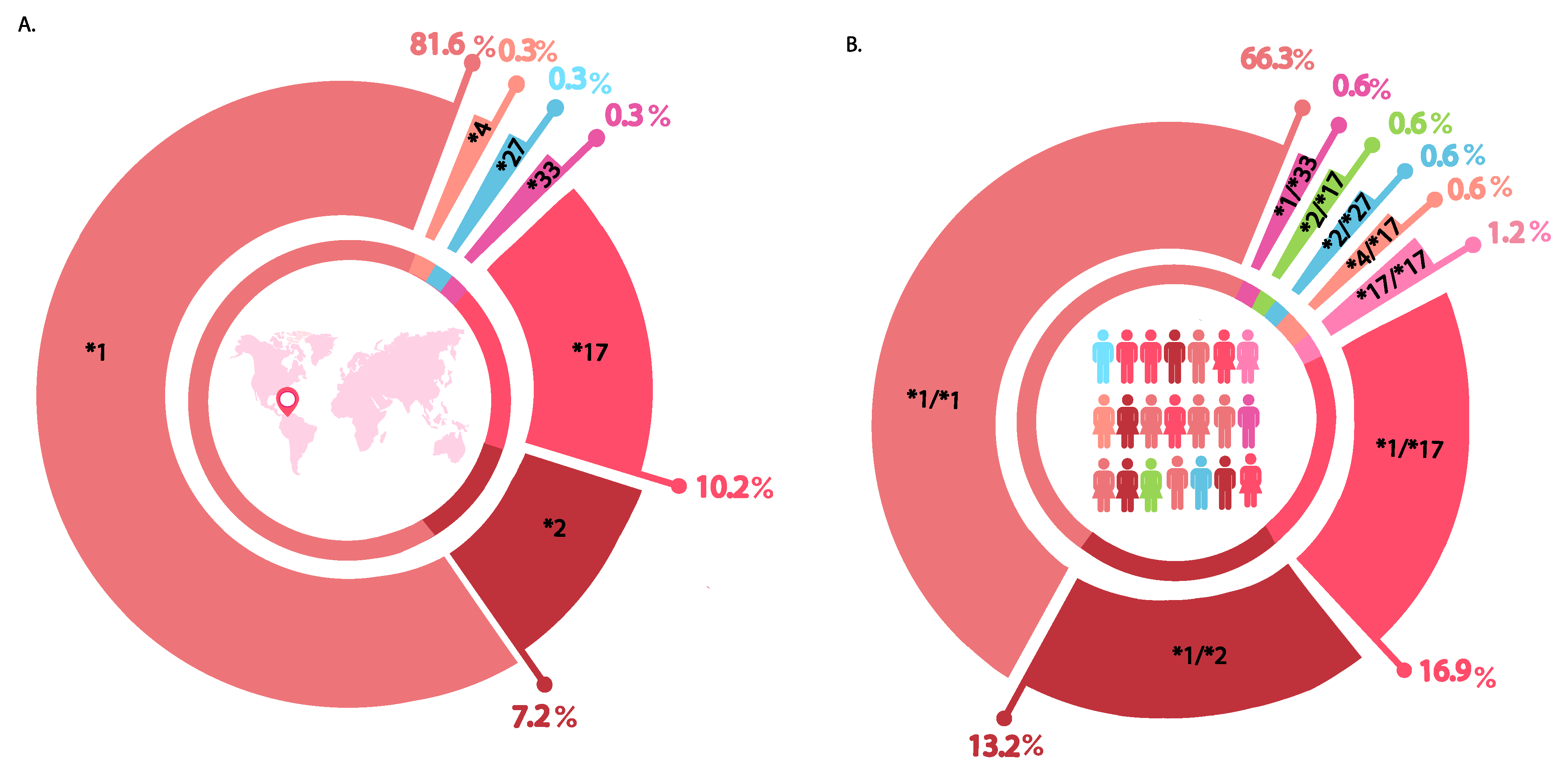
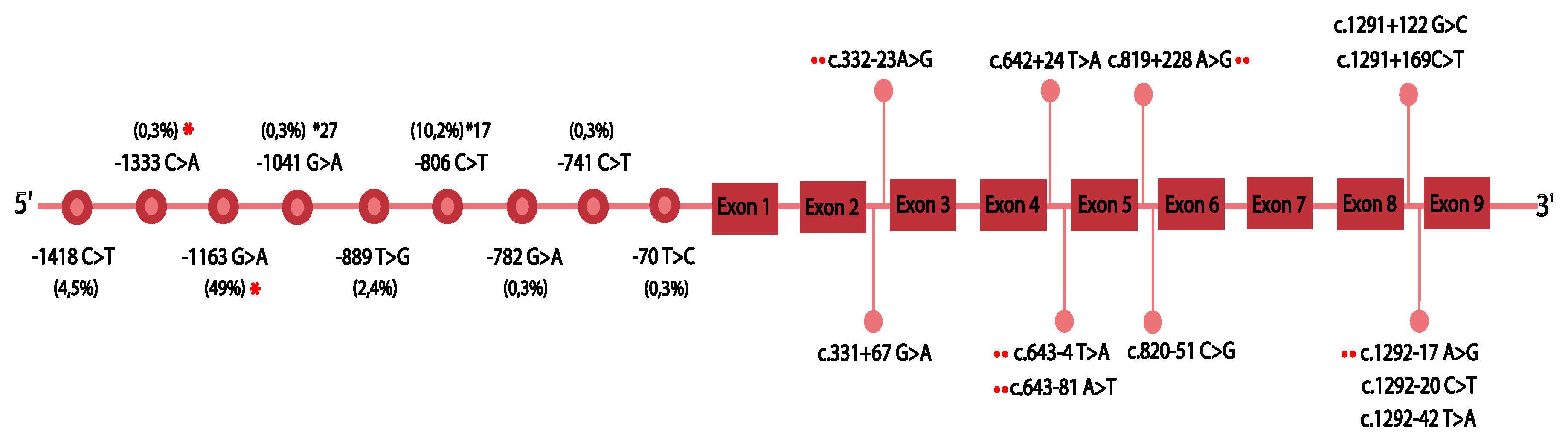
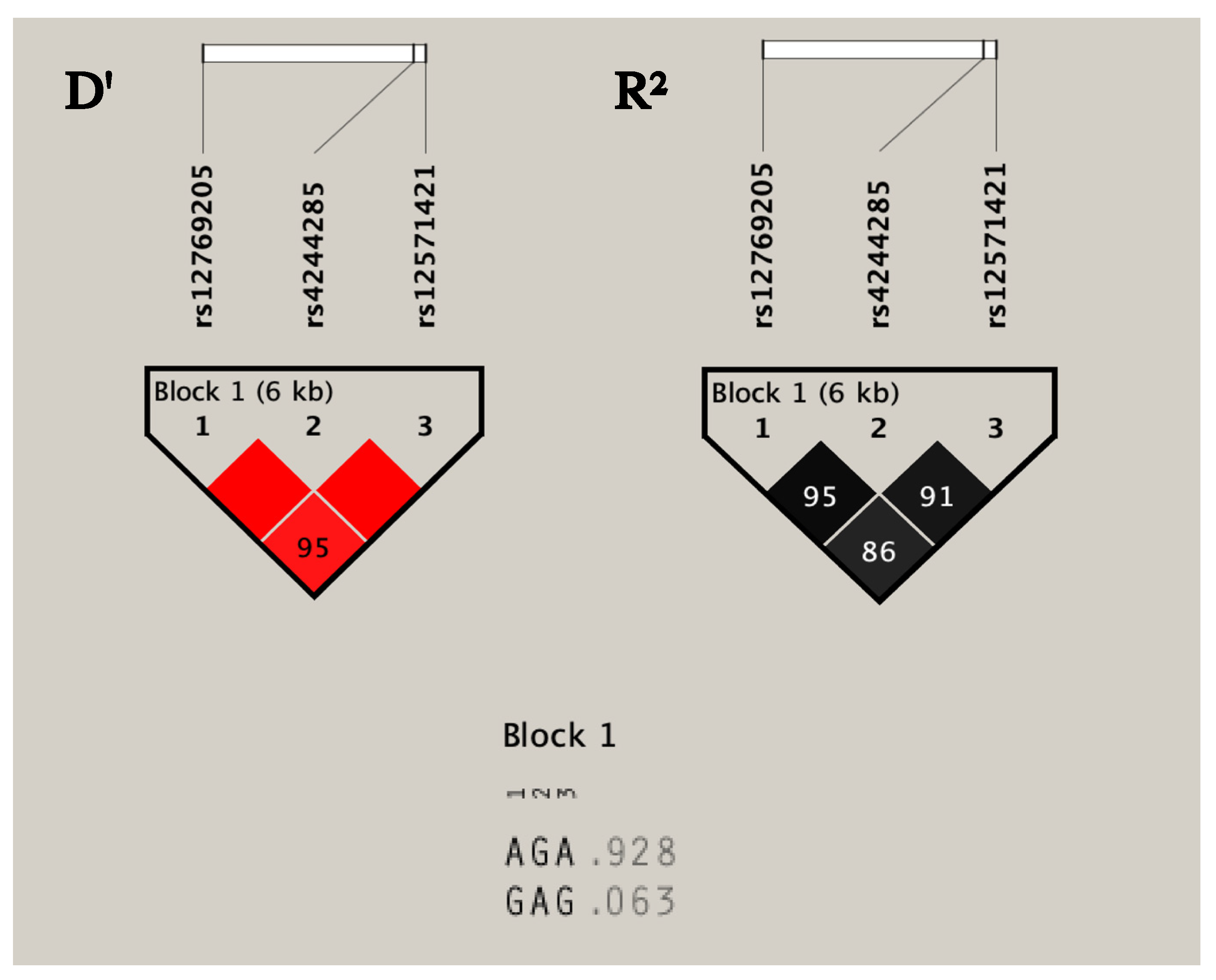
3.2. Analysis of Genetic Variants in CYP2C19
3.3. Reactivity Platelet Function and Genotype
3.4. Clinical Adverse Reactions and Causality Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peng, W.; Shi, X.; Xu, X.; Lin, Y. Both CYP2C19 and PON1 Q192R Genotypes Influence Platelet Response to Clopidogrel by Thrombelastography in Patients with Acute Coronary Syndrome. Cardiovasc. Ther. 2019, 2019, 3470145. [Google Scholar] [CrossRef]
- Pereira, N.L.; Rihal, C.S.; So, D.Y.F.; Rosenberg, Y.; Lennon, R.J.; Mathew, V.; Goodman, S.G.; Weinshilboum, R.M.; Wang, L.; Baudhuin, L.M.; et al. Clopidogrel Pharmacogenetics. Circ. Cardiovasc. Interv. 2019, 12, 1–21. [Google Scholar] [CrossRef]
- Savi, P.; Pereillo, J.M.; Uzabiaga, M.F.; Combalbert, J.; Picard, C.; Maffrand, J.P.; Pascal, M.; Herbert, J.M. Identification and biological activity of the active metabolite of clopidogrel. Thromb. Haemost. 2000, 84, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.A.; Pereira, N. Pharmacogenomic Impact of CYP2C19 Variation on Clopidogrel Therapy in Precision Cardiovascular Medicine. J. Pers. Med. 2018, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Suarez, D.F.; Botton, M.R.; Scott, S.A.; Tomey, M.I.; Garcia, M.J.; Wiley, J.; Villablanca, P.A.; Melin, K.; Lopez-Candales, A.; Renta, J.Y.; et al. Pharmacogenetic association study on clopidogrel response in Puerto Rican Hispanics with cardiovascular disease: A novel characterization of a Caribbean population. Pharmgenom. Pers. Med. 2018, 11, 95–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patti, G.; Micieli, G.; Cimminiello, C. The Role of Clopidogrel in 2020: A Reappraisal. Cardiovasc. Ther. 2020, 2020, 8703627. [Google Scholar] [CrossRef] [Green Version]
- Yin, T.; Miyata, T. Pharmacogenomics of clopidogrel: Evidence and perspectives. Thromb. Res. 2011, 128, 307–316. [Google Scholar] [CrossRef]
- Amin, A.M.; Sheau Chin, L.; Azri Mohamed Noor, D. The Personalization of Clopidogrel Antiplatelet Therapy: The Role of Integrative Pharmacogenetics and Pharmacometabolomics. Cardiol. Res. Pract. 2017, 2017, 8062796. [Google Scholar] [CrossRef]
- Shuldiner, A.R.; O’Connell, J.R.; Bliden, K.P.; Gandhi, A.; Ryan, K.; Horenstein, R.B.; Damcott, C.M.; Pakyz, R.; Tantry, U.S.; Gibson, Q.; et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA 2009, 302, 849–857. [Google Scholar] [CrossRef]
- Singla, A.; Antonino, M.J.; Bliden, K.P.; Tantry, U.S.; Gurbel, P.A. The relation between platelet reactivity and glycemic control in diabetic patients with cardiovascular disease on maintenance aspirin and clopidogrel therapy. Am. Heart J. 2009, 158, 784.e1–784.e6. [Google Scholar] [CrossRef]
- Lewis, J.P.; Shuldiner, A.R. Clopidogrel pharmacogenetics: Beyond candidate genes and genome-wide association studies. Clin. Pharmacol. Ther. 2017, 101, 323–325. [Google Scholar] [CrossRef]
- Xu, J.; Wang, A.; Wangqin, R.; Mo, J.; Chen, Z.; Dai, L.; Meng, X.; Zhao, X.; Wang, Y.; Li, H.; et al. Efficacy of clopidogrel for stroke depends on CYP2C19 genotype and risk profile. Randomized Control. Trial 2019, 86, 419–426. [Google Scholar] [CrossRef]
- Su, Q.; Li, J.; Tang, Z.; Yang, S.; Xing, G.; Liu, T.; Peng, H. Association of CYP2C19 Polymorphism with Clopidogrel Resistance in Patients with Acute Coronary Syndrome in China. Med. Sci. Monit. 2019, 25, 7138–7148. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. CYP2C19*2 polymorphism and clopidogrel resistance. Arch. Cardiol. Mex. 2020, 90, 544–548. [Google Scholar] [PubMed]
- Scott, S.A.; Sangkuhl, K.; Stein, C.M.; Hulot, J.S.; Mega, J.L.; Roden, D.M.; Klein, T.E.; Sabatine, M.S.; Johnson, J.A.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin. Pharmacol. Ther. 2013, 94, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewski, A.; Filipska, K. The Phenomenon of Clopidogrel High On-Treatment Platelet Reactivity in Ischemic Stroke Subjects: A Comprehensive Review. Int. J. Mol. Sci. 2020, 21, 6408. [Google Scholar] [CrossRef] [PubMed]
- Pereira, N.L.; Geske, J.B.; Mayr, M.; Shah, S.H.; Rihal, C.S. Pharmacogenetics of Clopidogrel: An Unresolved Issue. Circ. Cardiovasc. Genet. 2016, 9, 185–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mărginean, A.; Bănescu, C.; Moldovan, V.; Scridon, A.; Mărginean, M.; Bălaşa, R.; Maier, S.; Ţăruşi, M.; Dobreanu, M. The Impact of CYP2C19 Loss-of-Function Polymorphisms, Clinical, and Demographic Variables on Platelet Response to Clopidogrel Evaluated Using Impedance Aggregometry. Clin. Appl. Thromb. Hemost. 2017, 23, 255–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paré, G.; Mehta, S.R.; Yusuf, S.; Anand, S.S.; Connolly, S.J.; Hirsh, J.; Simonsen, K.; Bhatt, D.L.; Fox, K.A.; Eikelboom, J.W. Effects of CYP2C19 genotype on outcomes of clopidogrel treatment. N. Engl. J. Med. 2010, 363, 1704–1714. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Choi, J.L.; Guo, L.Z.; Goh, R.Y.; Kim, B.R.; Woo, K.S.; Kim, M.H.; Han, J.Y. Correlation between the CYP2C19 phenotype status and the results of three different platelet function tests in cardiovascular disease patients receiving antiplatelet therapy: An emphasis on newly introduced platelet function analyzer-200 P2Y test. Ann. Lab. Med. 2016, 36, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Klein, M.D.; Williams, A.K.; Lee, C.R.; Stouffer, G.A. Clinical Utility of CYP2C19 Genotyping to Guide Antiplatelet Therapy in Patients With an Acute Coronary Syndrome or Undergoing Percutaneous Coronary Intervention. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Rath, C.L.; Jørgensen, N.R.; Wienecke, T. Clopidogrel responder status is uninfluenced by CYP2C19*2 in Danish patients with stroke. PLoS ONE. 2020, 15, e0236260. [Google Scholar] [CrossRef]
- Rodrigues-Soares, F.; Peñas-Lledó, E.M.; Tarazona-Santos, E.; Sosa-Macías, M.; Terán, E.; López-López, M.; Rodeiro, I.; Moya, G.E.; Calzadilla, L.R.; Ramírez-Roa, R.; et al. Genomic Ancestry, CYP2D6, CYP2C9, and CYP2C19 Among Latin Americans. Clin. Pharmacol. Ther. 2020, 107, 257–268. [Google Scholar] [CrossRef]
- Dorji, P.W.; Tshering, G.; Na-Bangchang, K. CYP2C9, CYP2C19, CYP2D6 and CYP3A5 polymorphisms in South-East and East Asian populations: A systematic review. J. Clin. Pharm. Ther. 2019, 44, 508–524. [Google Scholar] [CrossRef] [Green Version]
- Rodeiro, I.; Remírez-Figueredo, D.; García-Mesa, M.; Dorado, P.; LLerena, A.; CEIBA. Pharmacogenetics in Latin American populations: Regulatory aspects, application to herbal medicine, cardiovascular and psychiatric disorders. Drug Metabol. Drug Interact. 2012, 27, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Gurbel, P.A.; Tantry, U.S. Do platelet function testing and genotyping improve outcome in patients treated with antithrombotic agents? Circulation 2012, 125, 1276–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, D.R., Jr.; Dehmer, G.J.; Kaul, S.; Leifer, D.; O’Gara, P.T.; Stein, C.M. ACCF/AHA clopidogrel clinical alert: Approaches to the FDA “boxed warning”: A report of the American College of Cardiology Foundation Task Force on clinical expert consensus documents and the American Heart Association endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2010, 56, 321–341. [Google Scholar] [PubMed] [Green Version]
- Wallentin, L.; James, S.; Storey, R.F.; Armstrong, M.; Barratt, B.J.; Horrow, J.; Husted, S.; Katus, H.; Steg, P.G.; Shah, S.H.; et al. Effect of CYP2C19 and ABCB1 single nucleotide polymorphisms on outcomes of treatment with ticagrelor versus clopidogrel for acute coronary syndromes: A genetic substudy of the PLATO trial. Lancet 2010, 376, 1320–1328. [Google Scholar] [CrossRef]
- Notarangelo, F.M.; Maglietta, G.; Bevilacqua, P.; Cereda, M.; Merlini, P.A.; Villani, G.Q.; Moruzzi, P.; Patrizi, G.; Malagoli Tagliazucchi, G.; Crocamo, A.; et al. Pharmacogenomic Approach to Selecting Antiplatelet Therapy in Patients With Acute Coronary Syndromes: The PHARMCLO Trial. J. Am. Coll. Cardiol. 2018, 71, 1869–1877. [Google Scholar] [CrossRef]
- Li, Y.; Tang, H.L.; Hu, Y.F.; Xie, H.G. The gain-of-function variant allele CYP2C19*17: A double-edged sword between thrombosis and bleeding in clopidogrel-treated patients. J. Thromb. Haemost. 2012, 10, 199–206. [Google Scholar] [CrossRef]
- Mega, J.L.; Close, S.L.; Wiviott, S.D.; Shen, L.; Hockett, R.D.; Brandt, J.T.; Walker, J.R.; Antman, E.M.; Macias, W.; Braunwald, E.; et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N. Engl. J. Med. 2009, 360, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Helsby, N.A.; Burns, K.E. Molecular mechanisms of genetic variation and transcriptional regulation of CYP2C19. Front. Genet. 2012, 3, 206. [Google Scholar] [CrossRef] [Green Version]
- Drögemöller, B.I.; Wright, G.E.; Niehaus, D.J.; Koen, L.; Malan, S.; Da Silva, D.M.; Hillermann-Rebello, R.; La Grange, A.M.; Venter, M.; Warnich, L. Characterization of the genetic profile of CYP2C19 in two South African populations. Pharmacogenomics 2010, 11, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Arefayene, M.; Skaar, T.C.; Zhao, X.; Rae, J.M.; Tanus-Santos, J.E.; Brinkmann, U.; Brehm, I.; Salat, U.; Nguyen, A.; Desta, Z.; et al. Sequence diversity and functional characterization of the 5′-regulatory region of human CYP2C19. Pharmacogenetics 2003, 13, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Fukushima-Uesaka, H.; Saito, Y.; Maekawa, K.; Ozawa, S.; Hasegawa, R.; Kajio, H.; Kuzuya, N.; Yasuda, K.; Kawamoto, M.; Kamatani, N.; et al. Genetic variations and haplotypes of CYP2C19 in a Japanese population. Drug Metab. Pharmacokinet. 2005, 20, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Satyanarayana, C.R.; Devendran, A.; Jayaraman, M.; Mannu, J.; Mathur, P.P.; Gopal, S.D.; Rajagopal, K.; Chandrasekaran, A. Influence of the genetic polymorphisms in the 5′ flanking and exonic regions of CYP2C19 on proguanil oxidation. Drug Metab. Pharmacokinet. 2009, 24, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, A.S.; Prasad, B.; Shirasaka, Y.; Fohner, A.; Finkelstein, D.; Fan, Y.; Wang, S.; Wu, G.; Aklillu, E.; Sim, S.C.; et al. The CYP2C19 Intron 2 Branch Point SNP is the Ancestral Polymorphism Contributing to the Poor Metabolizer Phenotype in Livers with CYP2C19*35 and CYP2C19*2 Alleles. Drug Metab. Dispos. 2015, 43, 1226–1235. [Google Scholar] [CrossRef] [Green Version]
- Královicová, J.; Lei, H.; Vorechovský, I. Phenotypic consequences of branch point substitutions. Hum. Mutat. 2006, 27, 803–813. [Google Scholar] [CrossRef]
- Morales-Rosado, J.A.; Goel, K.; Zhang, L.; Åkerblom, A.; Baheti, S.; Black, J.L.; Eriksson, N.; Wallentin, L.; James, S.; Storey, R.F.; et al. Next-Generation Sequencing of CYP2C19 in Stent Thrombosis: Implications for Clopidogrel Pharmacogenomics. Cardiovasc. Drugs Ther. 2020. [Google Scholar] [CrossRef]
- Shukla, A.; Huang, W.; Depaz, I.M.; Gillam, E.M. Membrane integration of recombinant human P450 forms. Xenobiotica 2009, 39, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Ahn, K.; Szczesna-Skorupa, E.; Kemper, B. The amino-terminal 29 amino acids of cytochrome P450 2C1 are sufficient for retention in the endoplasmic reticulum. J. Biol. Chem. 1993, 268, 18726–18733. [Google Scholar] [CrossRef]
- Xu, R.A.; Gu, E.M.; Liu, T.H.; Ou-Yang, Q.G.; Hu, G.X.; Cai, J.P. The effects of cytochrome P450 2C19 polymorphism on the metabolism of voriconazole in vitro. Infect. Drug Resist. 2018, 11, 2129–2135. [Google Scholar] [CrossRef] [Green Version]
- Hasemann, C.A.; Kurumbail, R.G.; Boddupalli, S.S.; Peterson, J.A.; Deisenhofer, J. Structure and function of cytochromes P450: A comparative analysis of three crystal structures. Structure 1995, 3, 41–62. [Google Scholar] [CrossRef]
- Wang, H.; An, N.; Wang, H.; Gao, Y.; Liu, D.; Bian, T.; Zhu, J.; Chen, C. Evaluation of the effects of 20 nonsynonymous single nucleotide polymorphisms of CYP2C19 on S-mephenytoin 4′-hydroxylation and omeprazole 5′-hydroxylation. Drug Metab. Dispos. 2011, 39, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Koessler, J.; Kobsar, A.L.; Rajkovic, M.S.; Schafer, A.; Flierl, U.; Pfoertsch, S.; Bauersachs, J.; Steigerwald, U.; Rechner, A.R.; Walter, U. The new INNOVANCE® PFA P2Y cartridge is sensitive to the detection of the P2Y12 receptor inhibition. Platelets 2011, 22, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Harmsze, A.; van Werkum, J.W.; Bouman, H.J.; Ruven, H.J.; Breet, N.J.; Ten Berg, J.M.; Hackeng, C.M.; Tjoeng, M.M.; Klungel, O.H.; de Boer, A.; et al. Besides CYP2C19*2, the variant allele CYP2C9*3 is associated with higher on-clopidogrel platelet reactivity in patients on dual antiplatelet therapy undergoing elective coronary stent implantation. Pharm. Genom. 2010, 20, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.H.; Li, S.; An, G.D.; Woo, K.S.; Kim, K.H.; Kim, J.M.; Kim, M.H.; Han, J.Y. Platelet Function Analyzer-200 P2Y Results Are Predictive of the Risk of Major Adverse Cardiac Events in Korean Patients Receiving Clopidogrel Therapy Following Acute Coronary Syndrome. Ann. Lab. Med. 2018, 38, 413–419. [Google Scholar] [CrossRef]
- Roule, V.; Ardouin, P.; Repessé, Y.; Le Querrec, A.; Blanchart, K.; Lemaitre, A.; Sabatier, R.; Borel-Derlon, A.; Beygui, F. Point of Care Tests VerifyNow P2Y12 and INNOVANCE PFA P2Y Compared to Light Transmittance Aggregometry After Fibrinolysis. Clin. Appl. Thromb. Hemost. 2018, 24, 1109–1116. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Mehta, S.R.; Tanguay, J.F.; Eikelboom, J.W.; Jolly, S.S.; Joyner, C.D.; Granger, C.B.; Faxon, D.P.; Rupprecht, H.J.; Budaj, A.; Avezum, A.; et al. Double-dose versus standard-dose clopidogrel and high-dose versus low-dose aspirin in individuals undergoing percutaneous coronary intervention for acute coronary syndromes (CURRENT-OASIS 7): A randomised factorial trial. Lancet 2010, 376, 1233–1243. [Google Scholar] [CrossRef]
- Nijjer, S.S.; Davies, J.E.; Francis, D.P. Quantitative comparison of clopidogrel 600 mg, prasugrel and ticagrelor, against clopidogrel 300 mg on major adverse cardiovascular events and bleeding in coronary stenting: Synthesis of CURRENT-OASIS-7, TRITON-TIMI-38 and PLATO. Int. J. Cardiol. 2012, 158, 181–185. [Google Scholar] [CrossRef]
- Mehta, S.R.; Bassand, J.P.; Chrolavicius, S.; Diaz, R.; Eikelboom, J.W.; Fox, K.A.; Granger, C.B.; Jolly, S.; Joyner, C.D.; Rupprecht, H.J.; et al. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes. N. Engl. J. Med. 2010, 363, 930–942. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | (n) | % |
|---|---|---|
| Sex | 166 | 100 |
| Female | 60 | 36.1 |
| Male | 106 | 63.8 |
| Age (years) | ||
| 30–50 | 11 | 6.6 |
| 50–70 | 88 | 53 |
| >70 | 67 | 40.3 |
| Type of ACS | ||
| UA | 25 | 15 |
| STEMI | 105 | 63.2 |
| NSTEMI | 36 | 21.6 |
| Previous ACS medical history * | 54 | 32.5 |
| Type of intervention current event | ||
| Medical † | 44 | 26.5 |
| PCI | 86 | 51.8 |
| CABG | 36 | 21.6 |
| Stent placement current event | 73 | 43.9 |
| Type 2 Diabetes Mellitus | ||
| Body Mass Index | 46 | 27.7 |
| Underweight | 2 | 1.2 |
| Normal | 58 | 34.9 |
| Overweight | 64 | 38.5 |
| Obese | 42 | 25.3 |
| Genetic Variants Genotypes | All | HPR | Non-HPR | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | p-Value | |
| CYP2C19 Loss function alleles | ||||
| Wild type | 143 (86) | 46 (27.7) | 97 (58.4) | 0.21 |
| Carrier | 23 (14) | 11 (6.6) | 12 (7.2) | |
| CYP2C19 Gain function alleles | ||||
| Wild type | 134 (80.7) | 45 (27.1) | 89 (53.6) | 0.83 |
| Carrier | 32 (19.2) | 12 (7.2) | 20 (12) |
| Therapeutic failures | 3 |
| Acute myocardial infarction | 2 |
| Ischemic stroke and death | 1 |
| Bleedings (all minor) | 19 |
| Ecchymosis | 7 |
| Epistaxis | 4 |
| Gingivorrhagia | 2 |
| Hematemesis | 1 |
| Petechiae | 1 |
| Rectorrhagia | 1 |
| Spontaneous bruising | 2 |
| Uterine hemorrhage | 1 |
| Causality (ADR excluding FT cases) | |
| Probable | 8 |
| Possible | 11 |
| Unclassifiable | (fatal cases) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angulo-Aguado, M.; Panche, K.; Tamayo-Agudelo, C.A.; Ruiz-Torres, D.-A.; Sambracos-Parrado, S.; Niño-Orrego, M.J.; Páez, N.; Piñeros-Hernandez, L.B.; Castillo-León, L.-F.; Pardo-Oviedo, J.M.; et al. A Pharmacogenetic Study of CYP2C19 in Acute Coronary Syndrome Patients of Colombian Origin Reveals New Polymorphisms Potentially Related to Clopidogrel Therapy. J. Pers. Med. 2021, 11, 400. https://doi.org/10.3390/jpm11050400
Angulo-Aguado M, Panche K, Tamayo-Agudelo CA, Ruiz-Torres D-A, Sambracos-Parrado S, Niño-Orrego MJ, Páez N, Piñeros-Hernandez LB, Castillo-León L-F, Pardo-Oviedo JM, et al. A Pharmacogenetic Study of CYP2C19 in Acute Coronary Syndrome Patients of Colombian Origin Reveals New Polymorphisms Potentially Related to Clopidogrel Therapy. Journal of Personalized Medicine. 2021; 11(5):400. https://doi.org/10.3390/jpm11050400
Chicago/Turabian StyleAngulo-Aguado, Mariana, Karen Panche, Caroll Andrea Tamayo-Agudelo, Daniel-Armando Ruiz-Torres, Santiago Sambracos-Parrado, Maria Jose Niño-Orrego, Nathaly Páez, Laura B Piñeros-Hernandez, Luisa-Fernanda Castillo-León, Juan Mauricio Pardo-Oviedo, and et al. 2021. "A Pharmacogenetic Study of CYP2C19 in Acute Coronary Syndrome Patients of Colombian Origin Reveals New Polymorphisms Potentially Related to Clopidogrel Therapy" Journal of Personalized Medicine 11, no. 5: 400. https://doi.org/10.3390/jpm11050400
APA StyleAngulo-Aguado, M., Panche, K., Tamayo-Agudelo, C. A., Ruiz-Torres, D. -A., Sambracos-Parrado, S., Niño-Orrego, M. J., Páez, N., Piñeros-Hernandez, L. B., Castillo-León, L. -F., Pardo-Oviedo, J. M., Abaunza, K. P., Laissue, P., Contreras, N., Calderón-Ospina, C. A., & Fonseca-Mendoza, D. J. (2021). A Pharmacogenetic Study of CYP2C19 in Acute Coronary Syndrome Patients of Colombian Origin Reveals New Polymorphisms Potentially Related to Clopidogrel Therapy. Journal of Personalized Medicine, 11(5), 400. https://doi.org/10.3390/jpm11050400