Author Contributions
Conceptualization, M.O.; data curation, T.H., Y.T., T.O., A.U., S.W. and K.N.; formal analysis, T.H. and M.O.; funding acquisition, Y.T.; methodology, M.O.; project administration; M.O.; validation, K.N., S.M. and M.O.; Writing original draft, T.H., K.N. and M.O.; writing review and editing, M.O. All authors have read and agreed to the published version of the manuscript.
Figure 1.
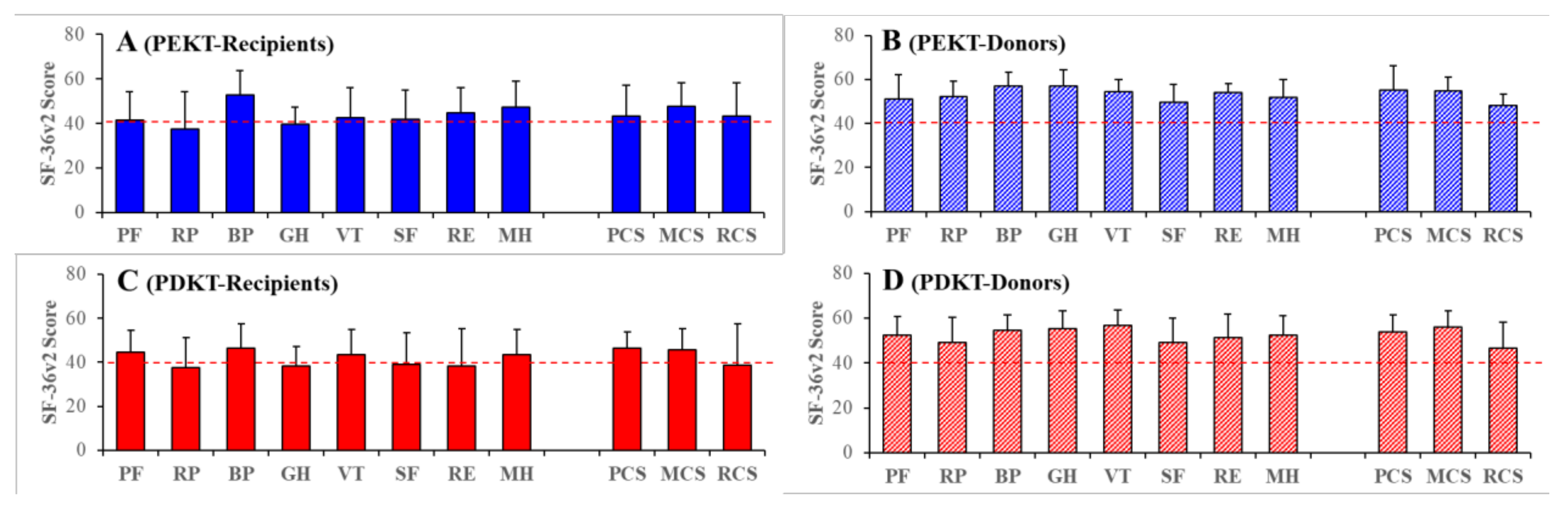
Short Form-36 Health Survey version 2 (SF-36v2) scores (quality of life: QOL) of recipients (A,C) and donors (B,D) in preemptive kidney transplantation (PEKT: A,B) and post-dialysis kidney transplantation (PDKT: C,D). Ordinates indicate the mean ± SD of the scores of SF-36v2. Red lines indicate the lowest SF-36v2 scores among the healthy general Japanese population. SF-36v2 is composed of eight subscales—“physical functioning” (PF), “role physical” (RP), “bodily pain” (BP), “general health” (GH), “vitality” (VT), “social functioning” (SF), “role emotional” (RE) and “mental health” (MH)—and three QOL components: Physical (PCS), mental (MCS), and role social (RCS) components.
Figure 1.
Short Form-36 Health Survey version 2 (SF-36v2) scores (quality of life: QOL) of recipients (A,C) and donors (B,D) in preemptive kidney transplantation (PEKT: A,B) and post-dialysis kidney transplantation (PDKT: C,D). Ordinates indicate the mean ± SD of the scores of SF-36v2. Red lines indicate the lowest SF-36v2 scores among the healthy general Japanese population. SF-36v2 is composed of eight subscales—“physical functioning” (PF), “role physical” (RP), “bodily pain” (BP), “general health” (GH), “vitality” (VT), “social functioning” (SF), “role emotional” (RE) and “mental health” (MH)—and three QOL components: Physical (PCS), mental (MCS), and role social (RCS) components.
Figure 2.
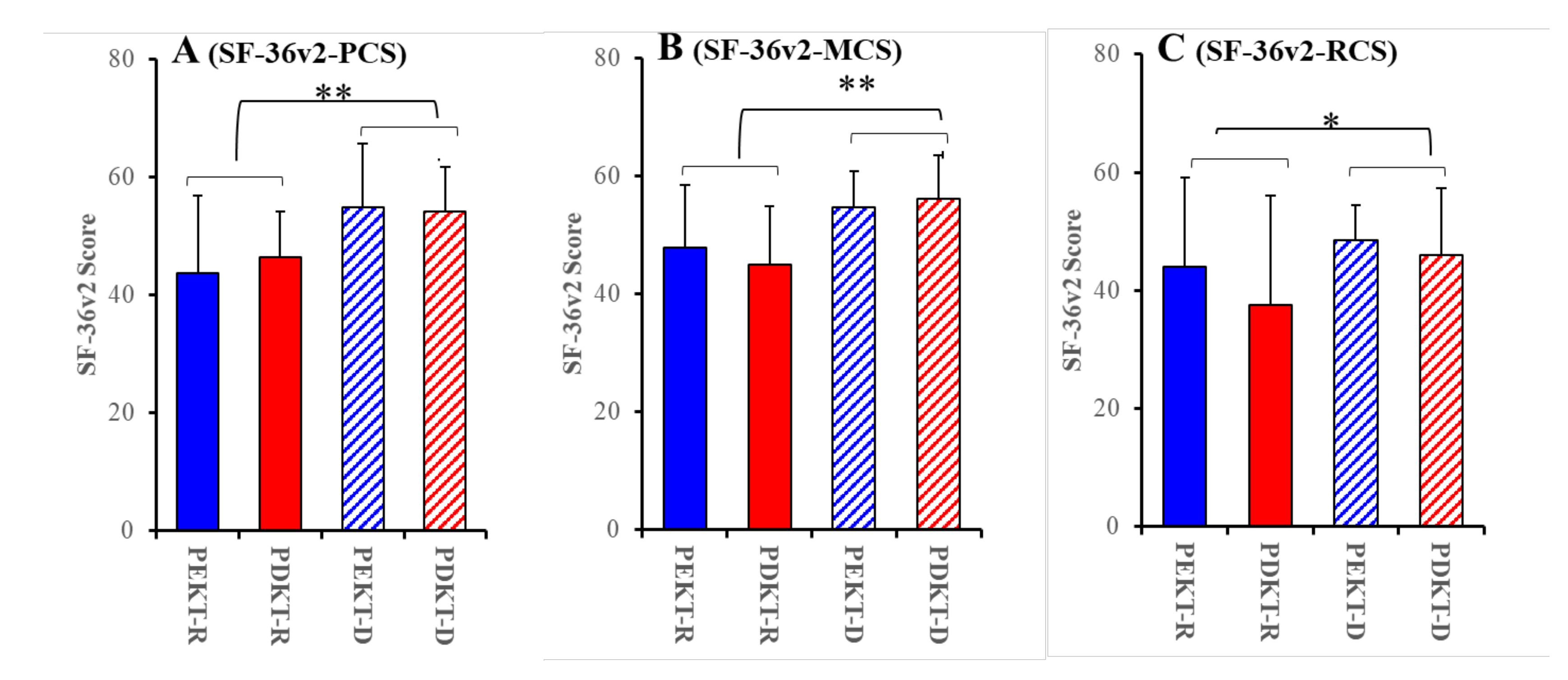
Comparisons of SF-36v2-PCS (A), SF-36v2-MCS (B), and SF-36v2-RSC (C) among PEKT recipients (PEKT-R), PDKT recipients (PDKT-R), PEKT donors (PEKT-D), and PDKT donors (PDKT-D) during kidney transplant decision-making. Ordinates indicate the mean ± SD for the scores of the SF-36v2 components. * p < 0.05, ** p < 0.01, relative to the SF-36v2 component scores of donors using a two-way analysis of variance (ANOVA) with Scheffe’s post-hoc test. Analyses between PEKT and PDKT were impossible since the F-values of the two-way ANOVA for the transplantation factor (PEKT vs. PDKT) and interaction factors (transplantation with relationship) were not violated (p > 0.05).
Figure 2.
Comparisons of SF-36v2-PCS (A), SF-36v2-MCS (B), and SF-36v2-RSC (C) among PEKT recipients (PEKT-R), PDKT recipients (PDKT-R), PEKT donors (PEKT-D), and PDKT donors (PDKT-D) during kidney transplant decision-making. Ordinates indicate the mean ± SD for the scores of the SF-36v2 components. * p < 0.05, ** p < 0.01, relative to the SF-36v2 component scores of donors using a two-way analysis of variance (ANOVA) with Scheffe’s post-hoc test. Analyses between PEKT and PDKT were impossible since the F-values of the two-way ANOVA for the transplantation factor (PEKT vs. PDKT) and interaction factors (transplantation with relationship) were not violated (p > 0.05).
Figure 3.
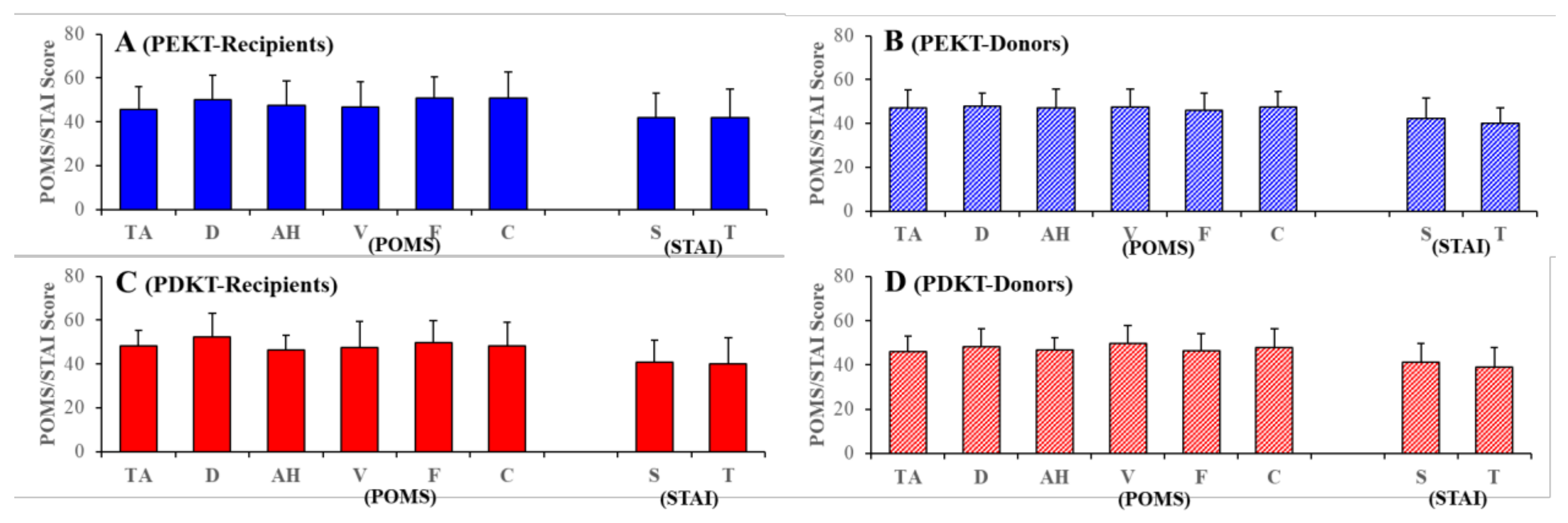
Scores for the Profile of Mood States (POMS) and State–Trait Anxiety Inventory (STAI) for the recipients (A,C) and donors (B,D) of PEKT (A,B) and PDKT (C,D). Ordinates indicate the mean ± SD of the scores of POMS and STAI. POMS is composed of 6 subscales: “tension/anxiety” (TA), “depression” (D), “anger/hostility” (AH), “vigour” (V), “fatigue” (F) and “confusion” (C). STAI is composed of two subscales: “state anxiety” (S) and “trait anxiety” (T).
Figure 3.
Scores for the Profile of Mood States (POMS) and State–Trait Anxiety Inventory (STAI) for the recipients (A,C) and donors (B,D) of PEKT (A,B) and PDKT (C,D). Ordinates indicate the mean ± SD of the scores of POMS and STAI. POMS is composed of 6 subscales: “tension/anxiety” (TA), “depression” (D), “anger/hostility” (AH), “vigour” (V), “fatigue” (F) and “confusion” (C). STAI is composed of two subscales: “state anxiety” (S) and “trait anxiety” (T).
Figure 4.
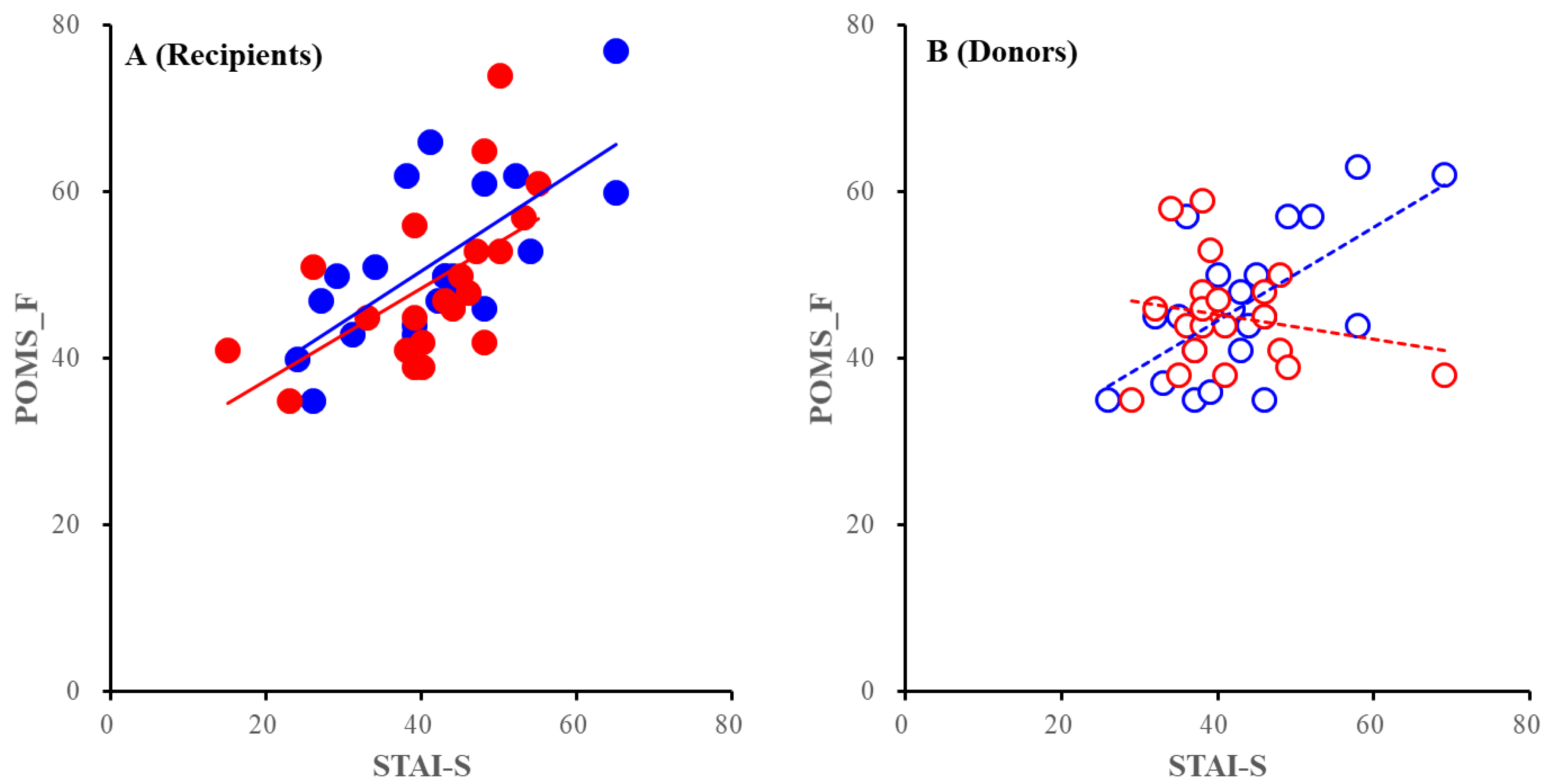
Correlation between the POMS-TA and STAI-T of recipients (A) and donors (B). Blue and red circles indicate PEKT, and PDKT, respectively. Closed and opened circles indicate recipients and donors, respectively. Full and dotted lines indicate the regressions of recipients and donors, respectively. Ordinates and abscissas indicate the mean ± SD of the POMS-TA, and STAI-T scores, respectively.
Figure 4.
Correlation between the POMS-TA and STAI-T of recipients (A) and donors (B). Blue and red circles indicate PEKT, and PDKT, respectively. Closed and opened circles indicate recipients and donors, respectively. Full and dotted lines indicate the regressions of recipients and donors, respectively. Ordinates and abscissas indicate the mean ± SD of the POMS-TA, and STAI-T scores, respectively.
Figure 5.
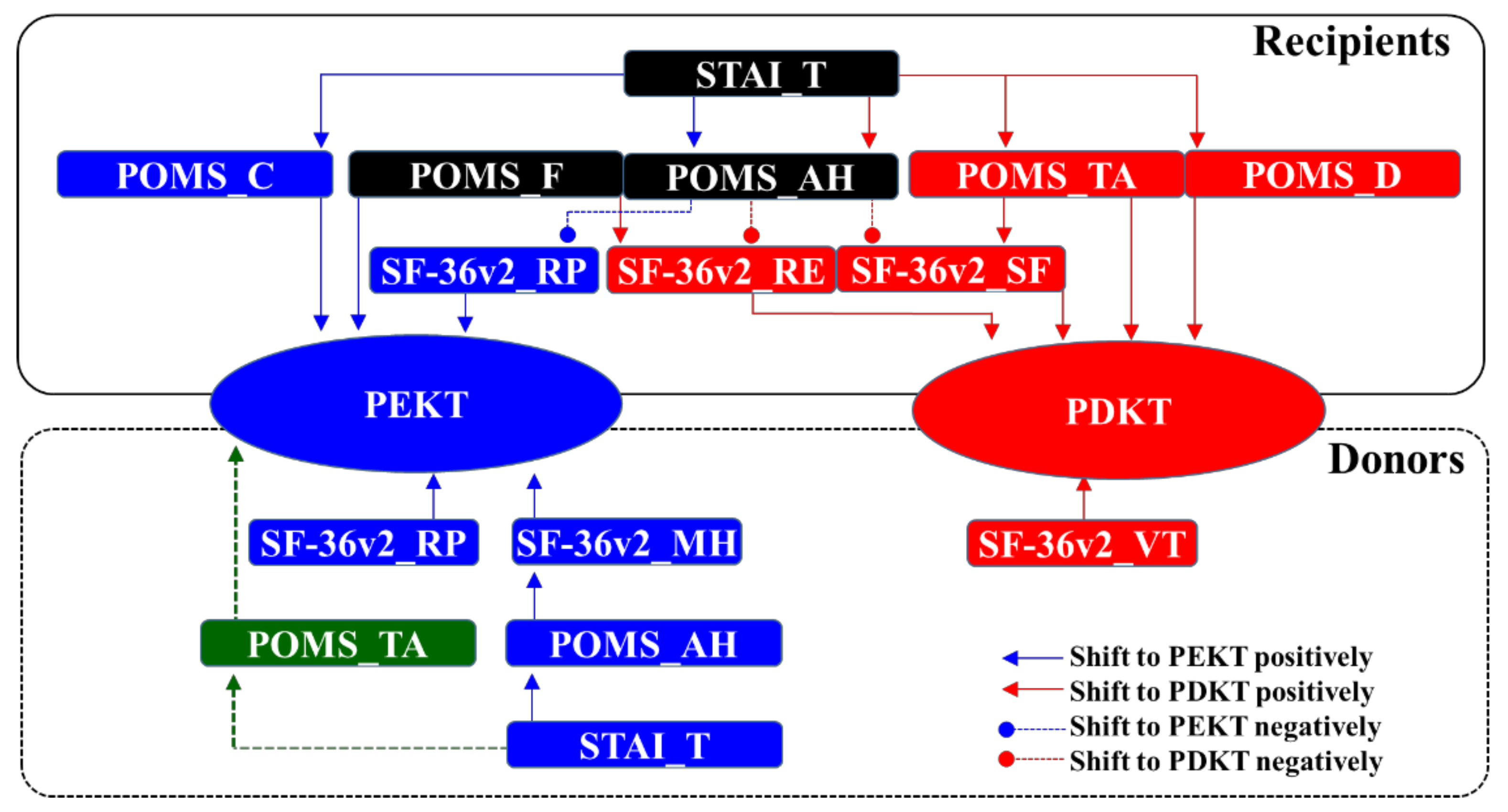
Proposed cascades of decision-making processes for PEKT and PDKT.
Figure 5.
Proposed cascades of decision-making processes for PEKT and PDKT.
Table 1.
Background of subjects in this study. PEKT: Pre-emptive kidney transplantation. PDKT: post-dialysis kidney transplantation. The statistical p values were analysed using a two-way ANOVA (age), a Mann–Whitney U test (duration of chronic kidney disease), a Cochran–Armitage test (relationship and primary disease), and the Cochran–Mantel–Haenstzel method (gender and employment).
Table 1.
Background of subjects in this study. PEKT: Pre-emptive kidney transplantation. PDKT: post-dialysis kidney transplantation. The statistical p values were analysed using a two-way ANOVA (age), a Mann–Whitney U test (duration of chronic kidney disease), a Cochran–Armitage test (relationship and primary disease), and the Cochran–Mantel–Haenstzel method (gender and employment).
| | PEKT | PDKT |
|---|
| | Recipient | Donor | Recipient | Donor |
|---|
| Male/Female | 13/11 | 8/16 | 14/7 | 9/12 |
| Age | 50.4 ± 12.1 | 59.9 ± 10.4 | 52.0 ± 13.5 | 60.1 ± 12.4 |
| Employment/Unemployment | 14/10 | 17/7 | 16/5 | 18/3 |
| Duration of chronic kidney disease (years) | 15.7 ± 15.3 | | 11.4 ± 9.9 | |
| Relationship | | | | |
| spouse | 16(67%) | | 9(43%) | |
| offspring | 7(29%) | | 9(43%) | |
| sibling | 1(4%) | | 1(5%) | |
| father in law | 0 | | 1(5%) | |
| brother in law | 0 | | 1(5%) | |
| Primary disease | | | | |
| unknown chronic renal failure | 8(33%) | | 1(5%) | |
| diabetic nephropathy | 2(8%) | | 6(29%) | |
| polycystic kidney disease | 5(21%) | | 1(5%) | |
| glomerulonephritis | 3(13%) | | 1(5%) | |
| IgA nephropathy | 1(4%) | | 3(14%) | |
| lupus nephritis | 1(4%) | | 2(10%) | |
| Others | 4(16%) | | 6(29%) | |
Table 2.
Impact components of SF-36v2 on choosing between PEKT and PDKT for recipients and donors analysed using binomial logistic regulation analysis with robust standard errors. β means standard partial regression coefficient. SE: standard Error. VIF: Variance Inflation Factor. OR: Odds Ration.
Table 2.
Impact components of SF-36v2 on choosing between PEKT and PDKT for recipients and donors analysed using binomial logistic regulation analysis with robust standard errors. β means standard partial regression coefficient. SE: standard Error. VIF: Variance Inflation Factor. OR: Odds Ration.
| Nagelkerke R2 (p Value) | Components | β | SE | p Value | VIF | OR | OR (95% CI) |
|---|
| 0.078 (0.872) | Recipients | SF-36v2_PCS | 0.025 | 0.029 | 0.933 | 1.117 | 1.025 | 0.968 | 1.085 |
| | | SF-36v2_MCS | −0.013 | 0.035 | 0.393 | 1.165 | 0.987 | 0.922 | 1.057 |
| | | SF-36v2_RCS | −0.003 | 0.020 | 0.715 | 1.225 | 0.997 | 0.959 | 1.037 |
| | Donors | SF-36v2_PCS | −0.022 | 0.038 | 0.881 | 1.105 | 0.978 | 0.908 | 1.053 |
| | | SF-36v2_MCS | 0.038 | 0.053 | 0.550 | 1.229 | 1.038 | 0.936 | 1.152 |
| | | SF-36v2_RCS | −0.019 | 0.034 | 0.479 | 1.072 | 0.981 | 0.917 | 1.049 |
Table 3.
Significant impact factors of SF-36v2 on choosing between PEKT and PDKT. * p < 0.05, ** p < 0.01 based on binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant impact factor on choosing PEKT or PDKT for recipients and donors.
Table 3.
Significant impact factors of SF-36v2 on choosing between PEKT and PDKT. * p < 0.05, ** p < 0.01 based on binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant impact factor on choosing PEKT or PDKT for recipients and donors.
| Nagelkerke R2 (p Value) | Factors | β | SE | p Value | VIF | OR | OR (95% CI) |
|---|
| 0.763 (0.005 **) | Recipients | SF3-6v2_PF | 0.145 | 0.081 | 0.072 | 2.044 | 1.157 | 0.987 | 1.355 |
| | | SF-36v2_RP | 0.332 | 0.148 | 0.025 * | 3.638 | 1.394 | 1.043 | 1.863 |
| | | SF-36v2_BP | −0.252 | 0.084 | 0.003 ** | 2.419 | 0.777 | 0.659 | 0.916 |
| | | SF-36v2_GH | 0.115 | 0.069 | 0.096 | 2.277 | 1.122 | 0.980 | 1.284 |
| | | SF-36v2_VT | −0.023 | 0.099 | 0.815 | 3.519 | 0.977 | 0.805 | 1.186 |
| | | SF-36v2_SF | −0.094 | 0.055 | 0.090 | 3.859 | 0.911 | 0.817 | 1.015 |
| | | SF-36v2_RE | −0.178 | 0.100 | 0.076 | 3.163 | 0.837 | 0.688 | 1.019 |
| | | SF-36v2_MH | −0.069 | 0.116 | 0.555 | 3.625 | 0.934 | 0.743 | 1.173 |
| | Donors | SF-36v2_PF | −0.044 | 0.078 | 0.577 | 2.273 | 0.957 | 0.821 | 1.116 |
| | | SF-36v2_RP | 0.088 | 0.093 | 0.344 | 2.277 | 1.092 | 0.910 | 1.312 |
| | | SF-36v2_BP | −0.210 | 0.100 | 0.035 * | 1.856 | 0.811 | 0.667 | 0.986 |
| | | SF3-6v2_GH | 0.006 | 0.087 | 0.942 | 1.638 | 1.006 | 0.848 | 1.194 |
| | | SF-36v2_VT | 0.373 | 0.168 | 0.026 * | 2.706 | 1.452 | 1.045 | 2.018 |
| | | SF-36v2_SF | 0.033 | 0.125 | 0.790 | 2.422 | 1.034 | 0.809 | 1.322 |
| | | SF-36v2_RE | −0.340 | 0.222 | 0.125 | 2.225 | 0.712 | 0.461 | 1.099 |
| | | SF-36v2_MH | 0.003 | 0.126 | 0.979 | 4.943 | 1.003 | 0.784 | 1.283 |
Table 4.
Significant impact factors of POMS on choosing between PEKT and PDKT. * p < 0.05 according to binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05: significant impact factor on choosing between PEKT and PDKT for recipients and donors.
Table 4.
Significant impact factors of POMS on choosing between PEKT and PDKT. * p < 0.05 according to binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05: significant impact factor on choosing between PEKT and PDKT for recipients and donors.
| Nagelkerke R2 (p Value) | Factor | β | SE | p Value | VIF | OR | OR (95% CI) |
|---|
| 0.679 (0.005 *) | Recipients | POMS_TA | 0.396 | 0.194 | 0.041 * | 5.667 | 1.485 | 1.015 | 2.173 |
| | | POMS_D | 0.573 | 0.236 | 0.015 * | 7.651 | 1.774 | 1.117 | 2.817 |
| | | POMS_AH | −0.194 | 0.132 | 0.141 | 5.063 | 0.824 | 0.636 | 1.066 |
| | | POMS_V | −0.036 | 0.080 | 0.655 | 2.167 | 0.965 | 0.824 | 1.129 |
| | | POMS_F | −0.512 | 0.238 | 0.032 * | 3.978 | 0.600 | 0.376 | 0.956 |
| | | POMS_C | −0.336 | 0.141 | 0.017 * | 5.500 | 0.714 | 0.542 | 0.942 |
| | Donors | POMS_TA | −0.397 | 0.210 | 0.059 | 4.380 | 0.672 | 0.445 | 1.015 |
| | | POMS_D | 0.013 | 0.161 | 0.936 | 3.305 | 1.013 | 0.739 | 1.388 |
| | | POMS_AH | −0.027 | 0.127 | 0.834 | 2.618 | 0.974 | 0.759 | 1.249 |
| | | POMS_V | 0.078 | 0.089 | 0.382 | 1.487 | 1.081 | 0.907 | 1.288 |
| | | POMS_F | −0.036 | 0.130 | 0.785 | 1.800 | 0.965 | 0.748 | 1.246 |
| | | POMS_C | 0.508 | 0.243 | 0.037 * | 3.115 | 1.662 | 1.032 | 2.678 |
Table 5.
Impact factor of STAI on choosing between PEKT and PDKT detected according to binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant impact factor on choosing between PEKT and PDKT for recipients and donors.
Table 5.
Impact factor of STAI on choosing between PEKT and PDKT detected according to binomial logistic regulation analysis with robust standard errors. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant impact factor on choosing between PEKT and PDKT for recipients and donors.
| Nagelkerke R2 (p Value) | Factor | β | SE | p Value | VIF | OR | OR (95% CI) |
|---|
| 0.067 (0.713) | Recipients | STAI_S | −0.022 | 0.059 | 0.706 | 3.861 | 0.978 | 0.872 | 1.097 |
| | | STAI_T | −0.001 | 0.049 | 0.977 | 3.835 | 0.999 | 0.907 | 1.099 |
| | Donors | STAI_S | −0.012 | 0.040 | 0.768 | 1.376 | 0.988 | 0.914 | 1.069 |
| | | STAI_T | −0.057 | 0.053 | 0.283 | 1.395 | 0.945 | 0.852 | 1.048 |
Table 6.
Significant impact factors of POMS on choosing between PEKT and PDKT. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant effects of POMS scores on the direct impact factors for choosing between PEKT and PDKT among recipients and donors according to stepwise multiple regression analysis with robust standard errors.
Table 6.
Significant impact factors of POMS on choosing between PEKT and PDKT. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant effects of POMS scores on the direct impact factors for choosing between PEKT and PDKT among recipients and donors according to stepwise multiple regression analysis with robust standard errors.
| Model | Adjusted R2 | F Value | p Value | Factor | β | p Value |
|---|
| Recipient | SF-36v2_RP | 0.288 | 6.015 | 0.001 ** | POMS_AH | 0.653 | 0.011 * |
| Donor | SF-36v2_BP | 0.092 | 2.485 | 0.043 * | POMS_V | −0.257 | 0.049 * |
| | | | | | POMS_C | −0.430 | 0.005 ** |
Table 7.
Significant impact factors of STAI on choosing between PEKT and PDKT. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant effects of STAI scores on the direct/secondary impact factors for choosing between PEKT and PDKT among recipients and donors according to stepwise multiple regression analysis with robust standard errors.
Table 7.
Significant impact factors of STAI on choosing between PEKT and PDKT. Multicollinearity was suspected if the VIF value was greater than 10. * p < 0.05, ** p < 0.01: significant effects of STAI scores on the direct/secondary impact factors for choosing between PEKT and PDKT among recipients and donors according to stepwise multiple regression analysis with robust standard errors.
| Model | Adjusted R2 | F Value | p Value | Factor | β | p Value |
|---|
| Recipient | POMS_TA | 0.443 | 14.062 | 0.001 ** | STAI_T | 0.516 | 0.018 * |
| | POMS_D | 0.546 | 14.849 | 0.001 ** | STAI_T | 0.852 | 0.001 ** |
| | POMS_AH | 0.397 | 17.744 | 0.001 ** | STAI_T | 0.633 | 0.001 ** |
| | POMS_C | 0.439 | 18.830 | 0.001 ** | STAI_T | 0.822 | 0.001 ** |
| Donor | POMS_C | 0.174 | 4.067 | 0.025 * | STAI_T | 0.478 | 0.025 * |


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}