
Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment




Abstract
:1. Introduction
2. Materials and Methods
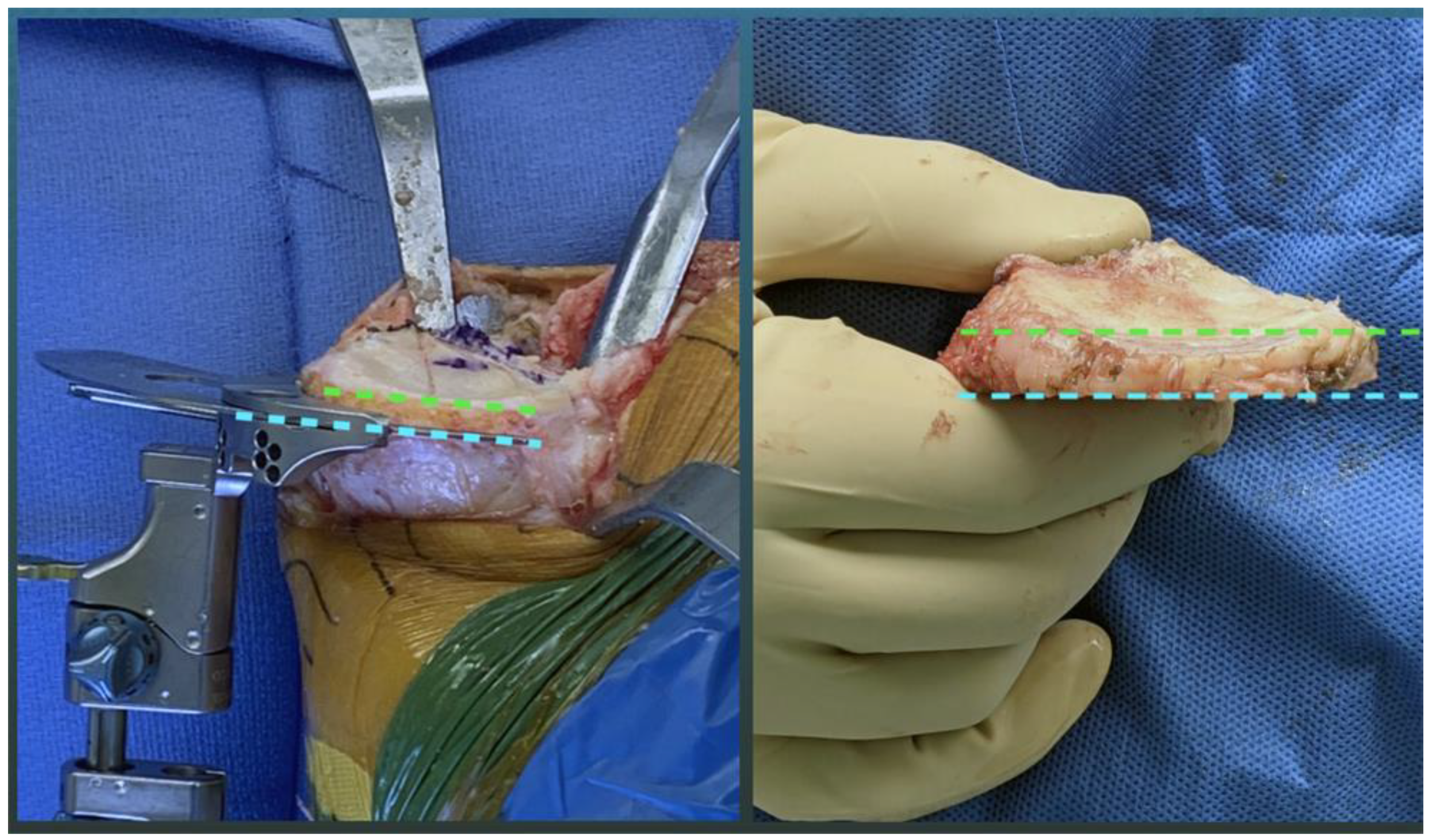
2.1. Overview of Unrestricted Calipered KA Technique and Accuracy Analysis of Component Placement
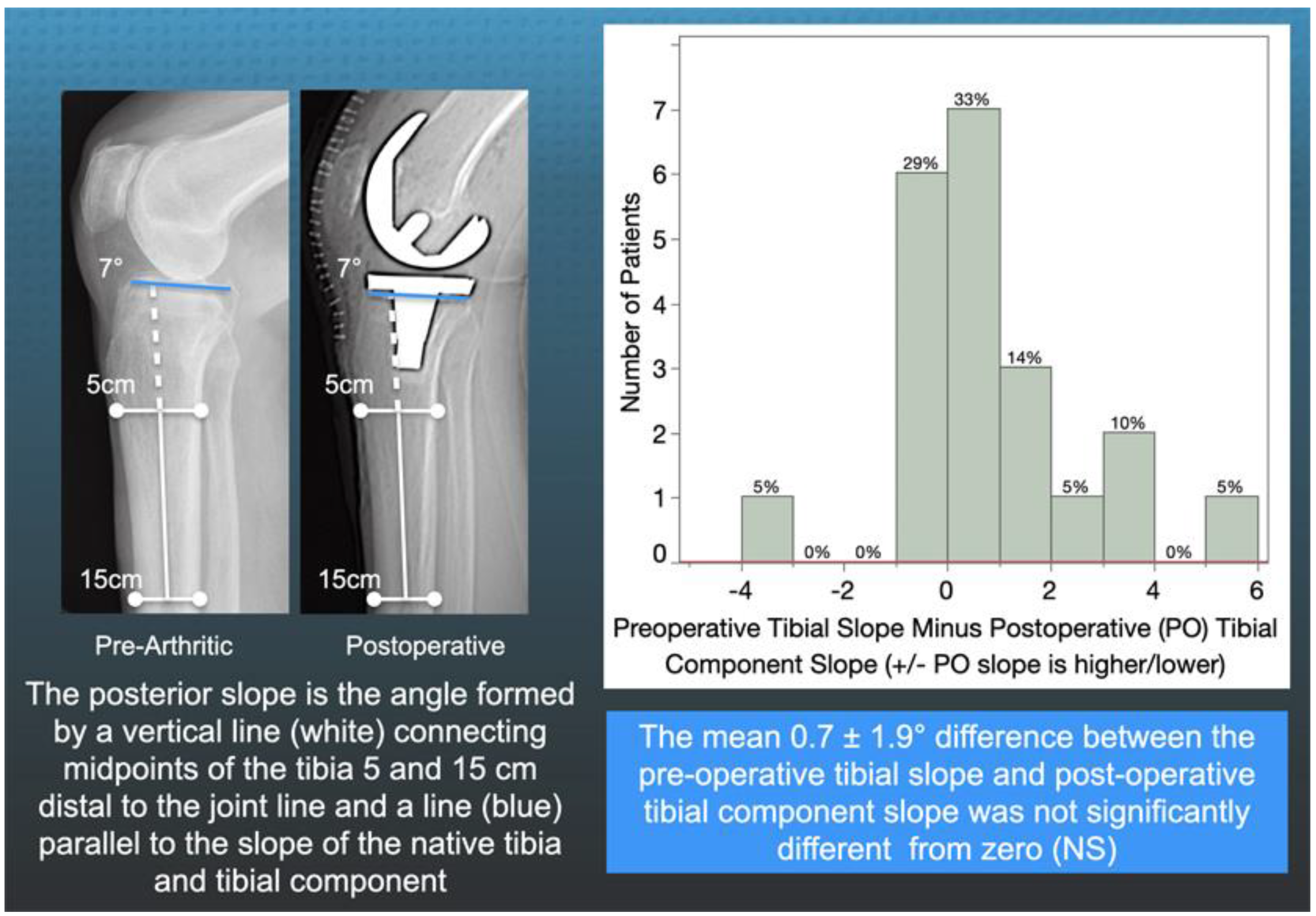
2.2. Method for Radiographically Measuring the Preoperative Tibial Slope and Postoperative Tibial Component Slope
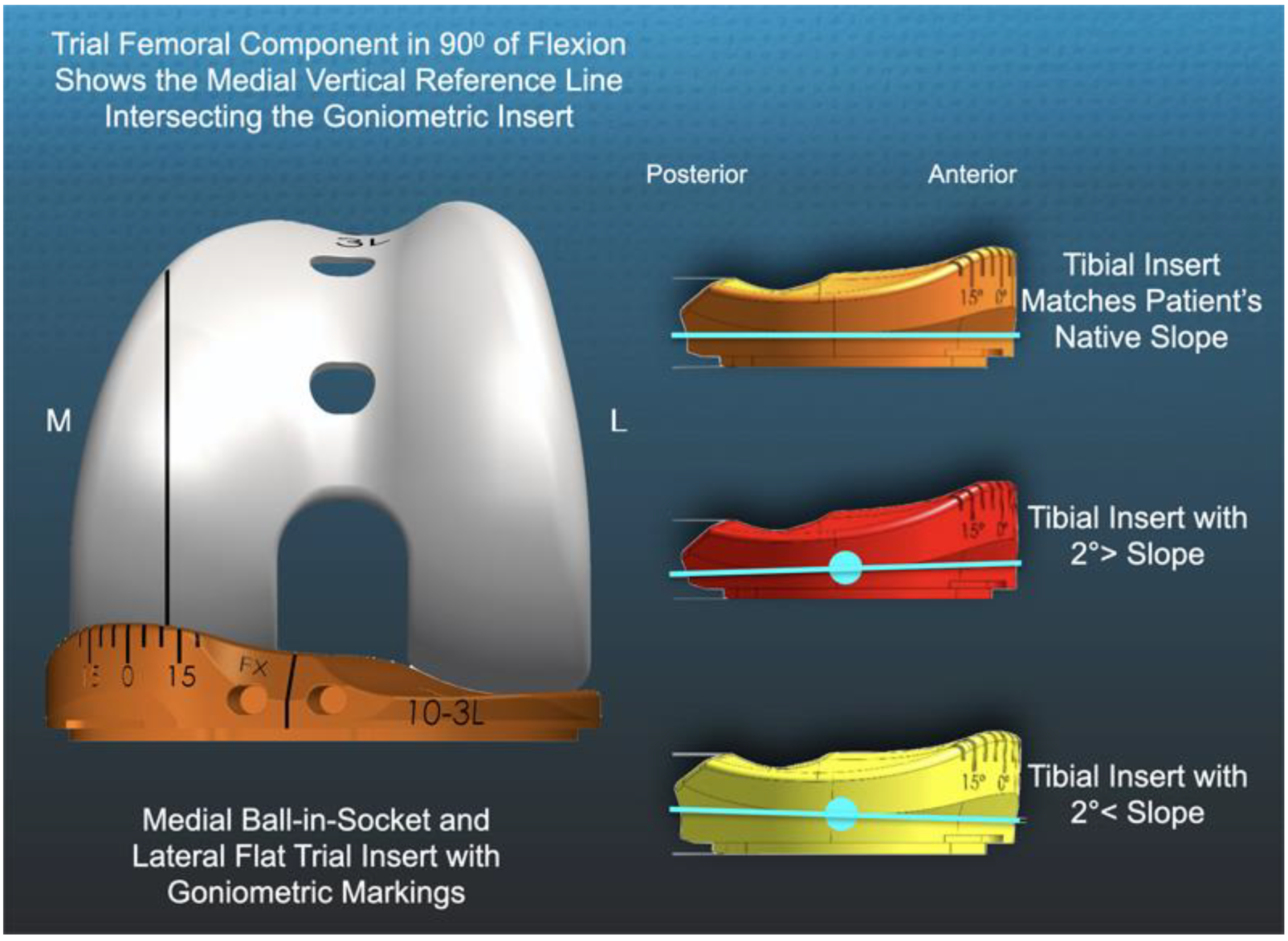
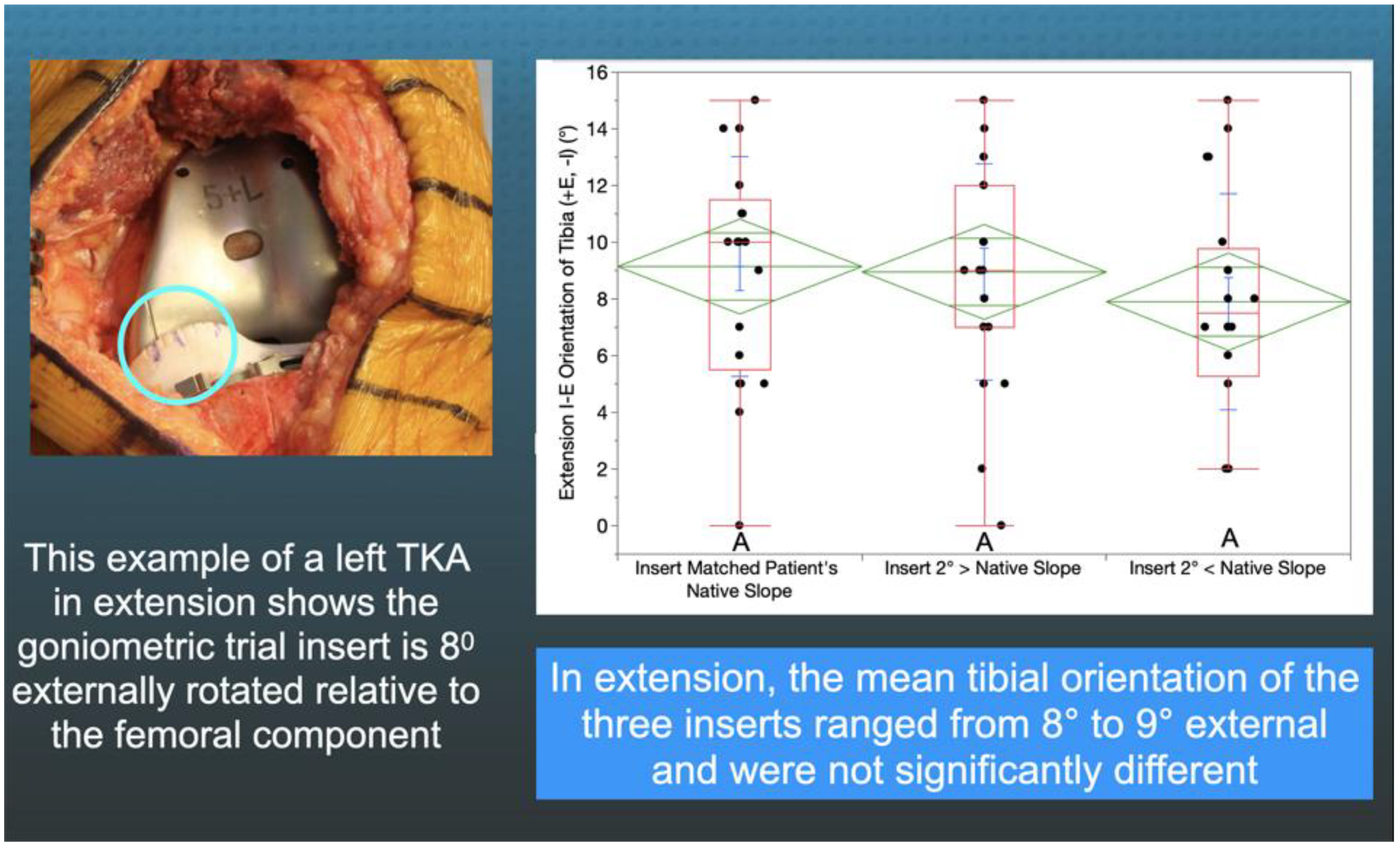
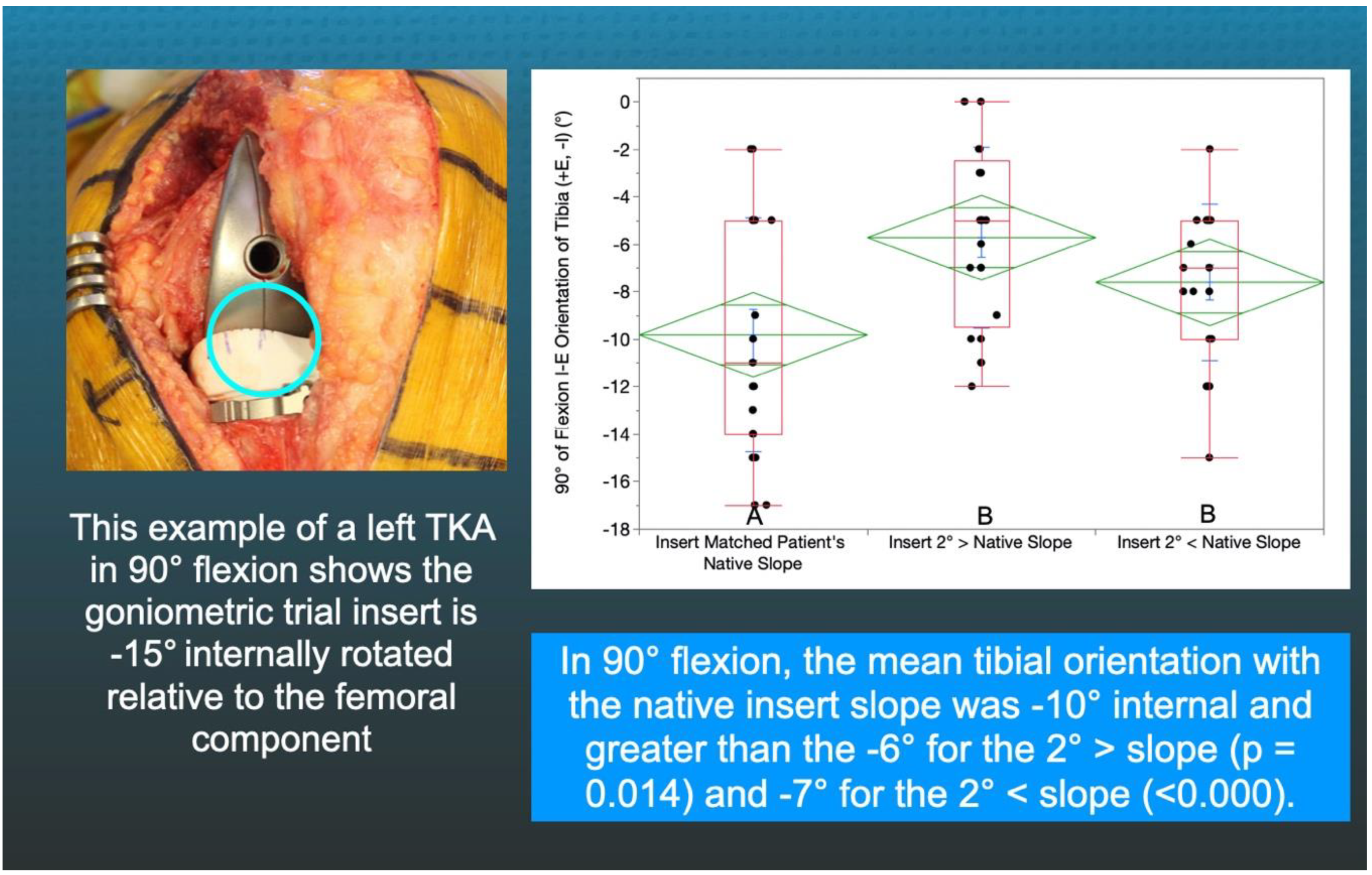
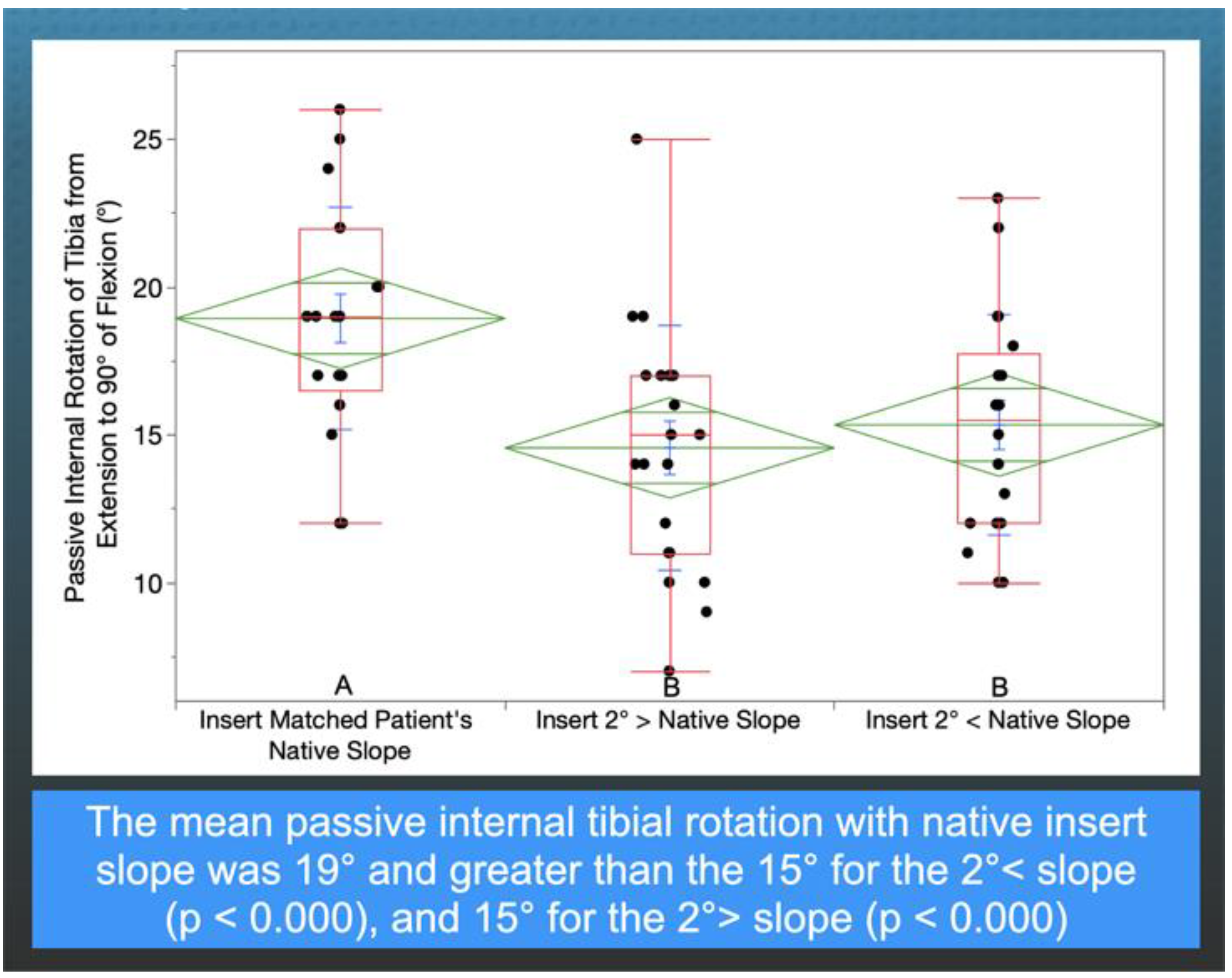
2.3. Method of Measuring the Orientation of the Tibia with Trial Goniometric Insert
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Peters, C.L.; Jimenez, C.; Erickson, J.; Anderson, M.B.; Pelt, C.E. Lessons learned from selective soft-tissue release for gap balancing in primary total knee arthroplasty: An analysis of 1216 consecutive total knee arthroplasties: AAOS exhibit selection. J. Bone Jt. Surg. Am. 2013, 95, e152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heesterbeek, P.J.; Wymenga, A.B. PCL balancing, an example of the need to couple detailed biomechanical parameters with clinical functional outcome. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1301–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellemans, J.; Robijns, F.; Duerinckx, J.; Banks, S.; Vandenneucker, H. The influence of tibial slope on maximal flexion after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. What mechanisms are associated with tibial component failure after kinematically-aligned total knee arthroplasty? Int. Orthop. 2017, 41, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.D.; Chmell, M.J. Balancing the posterior cruciate ligament during cruciate-retaining fixed and mobile-bearing total knee arthroplasty: Description of the pull-out lift-off and slide-back tests. J. Arthroplast. 2008, 23, 605–608. [Google Scholar] [CrossRef]
- Hofmann, A.A.; Bachus, K.N.; Wyatt, R.W. Effect of the tibial cut on subsidence following total knee arthroplasty. Clin. Orthop. Relat. Res. 1991, 63–69. [Google Scholar] [CrossRef]
- Ahmad, R.; Patel, A.; Mandalia, V.; Toms, A. Posterior Tibial Slope: Effect on, and Interaction with, Knee Kinematics. JBJS Rev. 2016, 4, e3. [Google Scholar] [CrossRef]
- Calek, A.K.; Hochreiter, B.; Hess, S.; Amsler, F.; Leclerq, V.; Hirschmann, M.T.; Behrend, H. High inter- and intraindividual differences in medial and lateral posterior tibial slope are not reproduced accurately by conventional TKA alignment techniques. Knee Surg. Sports Traumatol. Arthrosc. 2021. [Google Scholar] [CrossRef]
- Meier, M.; Janssen, D.; Koeck, F.X.; Thienpont, E.; Beckmann, J.; Best, R. Variations in medial and lateral slope and medial proximal tibial angle. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 939–946. [Google Scholar] [CrossRef]
- Nunley, R.M.; Nam, D.; Johnson, S.R.; Barnes, C.L. Extreme variability in posterior slope of the proximal tibia: Measurements on 2395 CT scans of patients undergoing UKA? J. Arthroplast. 2014, 29, 1677–1680. [Google Scholar] [CrossRef] [Green Version]
- Freeman, M.A.; Pinskerova, V. The movement of the knee studied by magnetic resonance imaging. Clin. Orthop. Relat. Res. 2003, 410, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Gill, T.J.; DeFrate, L.E.; Zayontz, S.; Glatt, V.; Zarins, B. Biomechanical consequences of PCL deficiency in the knee under simulated muscle loads—An in vitro experimental study. J. Orthop. Res. 2002, 20, 887–892. [Google Scholar] [CrossRef]
- Li, G.; Papannagari, R.; Li, M.; Bingham, J.; Nha, K.W.; Allred, D.; Gill, T. Effect of posterior cruciate ligament deficiency on in vivo translation and rotation of the knee during weightbearing flexion. Am. J. Sports Med. 2008, 36, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Fukubayashi, T.; Torzilli, P.A.; Sherman, M.F.; Warren, R.F. An in vitro biomechanical evaluation of anterior-posterior motion of the knee. Tibial displacement, rotation, and torque. J. Bone Jt. Surg. Am. 1982, 64, 258–264. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. Deviations in femoral joint lines using calipered kinematically aligned TKA from virtually planned joint lines are small and do not affect clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3118–3127. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Singh, A.K.; Howell, S.M.; Hull, M.L. Does Calipered Kinematically Aligned TKA Restore Native Left to Right Symmetry of the Lower Limb and Improve Function? J. Arthroplast. 2018, 33, 398–406. [Google Scholar] [CrossRef]
- Dennis, D.A.; Mahfouz, M.R.; Komistek, R.D.; Hoff, W. In vivo determination of normal and anterior cruciate ligament-deficient knee kinematics. J. Biomech. 2005, 38, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Schutz, P.; Taylor, W.R.; Postolka, B.; Fucentese, S.F.; Koch, P.P.; Freeman, M.A.R.; Pinskerova, V.; List, R. Kinematic Evaluation of the GMK Sphere Implant During Gait Activities: A Dynamic Videofluoroscopy Study. J. Orthop. Res. 2019, 37, 2337–2347. [Google Scholar] [CrossRef] [Green Version]
- Gray, H.A.; Guan, S.; Young, T.J.; Dowsey, M.M.; Choong, P.F.; Pandy, M.G. Comparison of posterior-stabilized, cruciate-retaining, and medial-stabilized knee implant motion during gait. J. Orthop. Res. 2020, 38, 1753–1768. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Zamora, T.; Shelton, T.; Howell, S.M.; Hull, M. A Best-Fit of an Anatomic Tibial Baseplate Closely Parallels the Flexion-Extension Plane and Covers a High Percentage of the Proximal Tibia. J. Knee Surg. 2020. [Google Scholar] [CrossRef]
- Howell, S.M.; Shelton, T.J.; Gill, M.; Hull, M.L. A cruciate-retaining implant can treat both knees of most windswept deformities when performed with calipered kinematically aligned TKA. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 437–445. [Google Scholar] [CrossRef]
- Nam, D.; Lin, K.M.; Howell, S.M.; Hull, M.L. Femoral bone and cartilage wear is predictable at 0 degrees and 90 degrees in the osteoarthritic knee treated with total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2975–2981. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. Does Malrotation of the Tibial and Femoral Components Compromise Function in Kinematically Aligned Total Knee Arthroplasty? Orthop. Clin. N. Am. 2016, 47, 41–50. [Google Scholar] [CrossRef]
- Howell, S.M.; Gill, M.; Shelton, T.J.; Nedopil, A.J. Reoperations are few and confined to the most valgus phenotypes 4 years after unrestricted calipered kinematically aligned TKA. Knee Surg. Sports Traumatol. Arthrosc. 2021. [Google Scholar] [CrossRef]
- Roth, J.D.; Howell, S.M.; Hull, M.L. Kinematically aligned total knee arthroplasty limits high tibial forces, differences in tibial forces between compartments, and abnormal tibial contact kinematics during passive flexion. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1589–1601. [Google Scholar] [CrossRef]
- Johnson, J.M.; Mahfouz, M.R.; Midillioglu, M.R.; Nedopil, A.J.; Howell, S.M. Three-dimensional analysis of the tibial resection plane relative to the arthritic tibial plateau in total knee arthroplasty. J. Exp. Orthop. 2017, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelton, T.J.; Howell, S.M.; Hull, M.L. Is There a Force Target That Predicts Early Patient-reported Outcomes After Kinematically Aligned TKA? Clin. Orthop. Relat. Res. 2019, 477, 1200–1207. [Google Scholar] [CrossRef]
- Shelton, T.J.; Nedopil, A.J.; Howell, S.M.; Hull, M.L. Do varus or valgus outliers have higher forces in the medial or lateral compartments than those which are in-range after a kinematically aligned total knee arthroplasty? limb and joint line alignment after kinematically aligned total knee arthroplasty. Bone Jt. J. 2017, 99-B, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.D.; Howell, S.M.; Hull, M.L. Analysis of differences in laxities and neutral positions from native after kinematically aligned TKA using cruciate retaining implants. J. Orthop. Res. 2019, 37, 358–369. [Google Scholar] [CrossRef] [Green Version]
- Roth, J.D.; Howell, S.M.; Hull, M.L. Native Knee Laxities at 0 degrees, 45 degrees, and 90 degrees of Flexion and Their Relationship to the Goal of the Gap-Balancing Alignment Method of Total Knee Arthroplasty. J. Bone Jt. Surg. Am. 2015, 97, 1678–1684. [Google Scholar] [CrossRef] [PubMed]
- Dean, R.S.; DePhillipo, N.N.; Chahla, J.; Larson, C.M.; LaPrade, R.F. Posterior Tibial Slope Measurements Using the Anatomic Axis Are Significantly Increased Compared With Those That Use the Mechanical Axis. Arthroscopy 2021, 37, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Hozan, C.T.; Cavalu, S.; Cinta Pinzaru, S.; Mohan, A.G.; Beteg, F.; Murvai, G. Rapid Screening of Retrieved Knee Prosthesis Components by Confocal Raman Micro-Spectroscopy. Appl. Sci. 2020, 10, 5343. [Google Scholar] [CrossRef]
- Li, G.; Papannagari, R.; Nha, K.W.; Defrate, L.E.; Gill, T.J.; Rubash, H.E. The coupled motion of the femur and patella during in vivo weightbearing knee flexion. J. Biomech. Eng. 2007, 129, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.C.; Yip, K.M.; Liu, T.K. Posterior slope angle of the medial tibial plateau. J. Formos. Med. Assoc. 1994, 93, 509–512. [Google Scholar]
- Freeman, M.A.; Pinskerova, V. The movement of the normal tibio-femoral joint. J. Biomech. 2005, 38, 197–208. [Google Scholar] [CrossRef]
- Pinskerova, V.; Samuelson, K.M.; Stammers, J.; Maruthainar, K.; Sosna, A.; Freeman, M.A. The knee in full flexion: An anatomical study. J. Bone Jt. Surg. Br. 2009, 91, 830–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirschmann, M.T.; Moser, L.B.; Amsler, F.; Behrend, H.; Leclerq, V.; Hess, S. Functional knee phenotypes: A novel classification for phenotyping the coronal lower limb alignment based on the native alignment in young non-osteoarthritic patients. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Riley, J.; Roth, J.D.; Howell, S.M.; Hull, M.L. Increases in tibial force imbalance but not changes in tibiofemoral laxities are caused by varus-valgus malalignment of the femoral component in kinematically aligned TKA. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3238–3248. [Google Scholar] [CrossRef]
- Riley, J.; Roth, J.D.; Howell, S.M.; Hull, M.L. Internal-external malalignment of the femoral component in kinematically aligned total knee arthroplasty increases tibial force imbalance but does not change laxities of the tibiofemoral joint. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1618–1628. [Google Scholar] [CrossRef]
- Roth, J.D.; Howell, S.M.; Hull, M.L. Measuring Tibial Forces is More Useful than Varus-Valgus Laxities for Identifying and Correcting Overstuffing in Kinematically Aligned Total Knee Arthroplasty. J. Orthop. Res. 2020. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative Demographics and Clinical and Radiographic Characteristics | Included Patients N = 21 | Not-Included Patients N = 15 | Significance |
|---|---|---|---|
| DEMOGRAPHICS | |||
| Age (years) | 70 (±7.9) | 68 (±8.8) | n.s. |
| Sex (male) | 8 (38%) | 7 (47%) | n.s. |
| Body Mass Index (kg/m2) | 29.2 (±5.3) | 30.2 (±4.4) | n.s. |
| PREOPERATIVE MOTION, DEFORMITY, ACL CONDITION, AND KELLGREN-LAWRENCE SCORE | |||
| Extension (degrees) | 7 (±5) | 7 (±8) | n.s. |
| Flexion (degrees) | 112 (±6.4) | 110 (±8.7) | n.s. |
| Varus (+)/Valgus (−) Deformity (degrees) | −12.2 (±3.1) | −10.8 (±3.1) | n.s. |
| Kellgren- Lawrence Score | 3.6 (±0.6) | 3.4 (±0.5) | n.s. |
| PREOPERATIVE FUNCTION | |||
| Oxford Score (48 is best, 0 is worst) | 21 (±8.4) | 16 (±6.5) | n.s. |
| Knee Society Score | 38 (±11.7) | 38 (±16.4) | n.s. |
| Knee Function Score | 55 (±21.5) | 46 (±16.1) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedopil, A.J.; Delman, C.; Howell, S.M.; Hull, M.L. Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment. J. Pers. Med. 2021, 11, 516. https://doi.org/10.3390/jpm11060516
Nedopil AJ, Delman C, Howell SM, Hull ML. Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment. Journal of Personalized Medicine. 2021; 11(6):516. https://doi.org/10.3390/jpm11060516
Chicago/Turabian StyleNedopil, Alexander J., Connor Delman, Stephen M. Howell, and Maury L. Hull. 2021. "Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment" Journal of Personalized Medicine 11, no. 6: 516. https://doi.org/10.3390/jpm11060516
APA StyleNedopil, A. J., Delman, C., Howell, S. M., & Hull, M. L. (2021). Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment. Journal of Personalized Medicine, 11(6), 516. https://doi.org/10.3390/jpm11060516