
Moving towards Integrated and Personalized Care in Parkinson’s Disease: A Framework Proposal for Training Parkinson Nurses

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
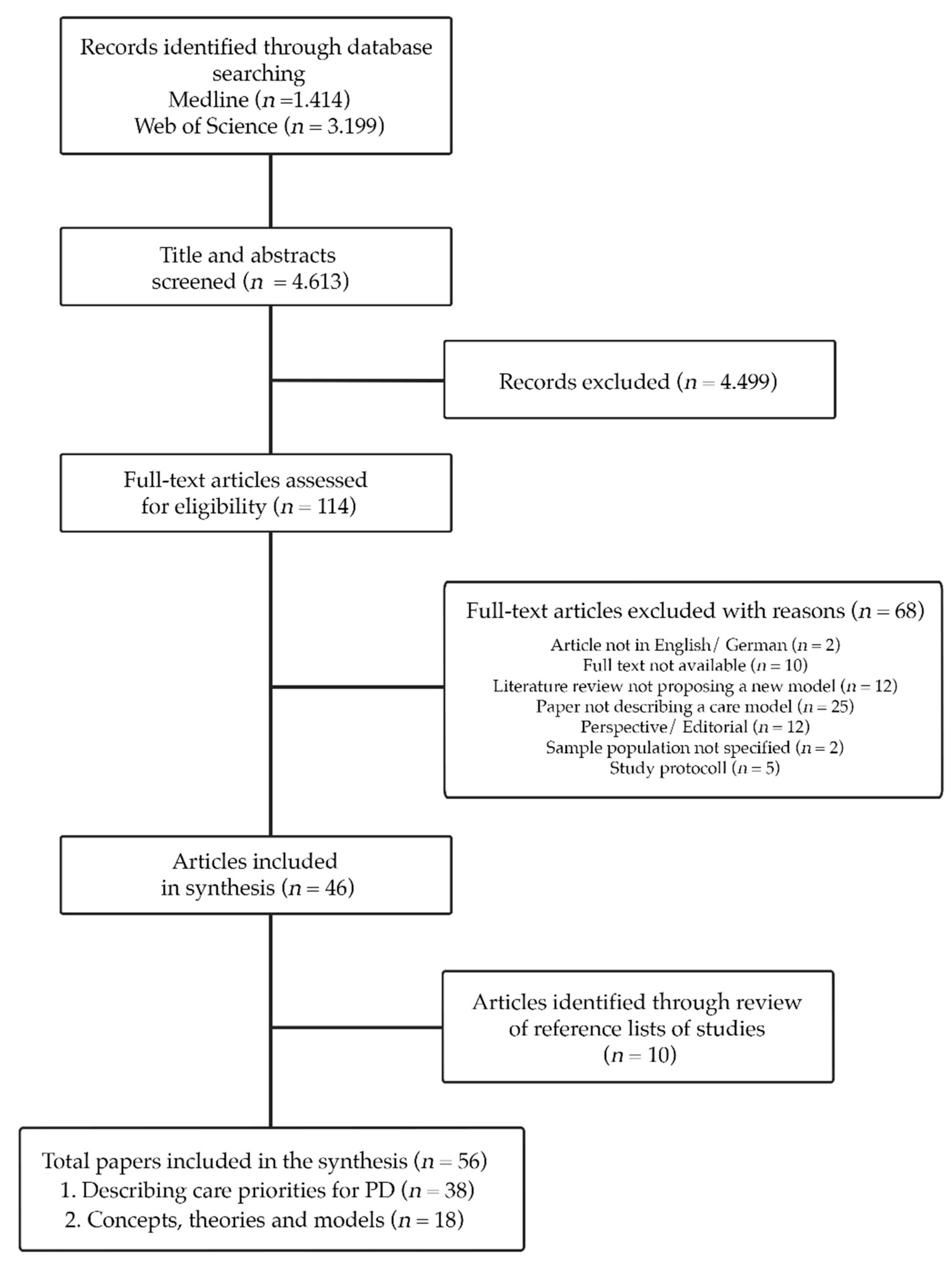
2. Materials and Methods
3. Results
Proposing a Framework for Training Parkinson Nurses to Deliver a Personalized Care Approach
- (1)
- PN ought to be competent to identify needs and preferences. Additionally, they must be able to decide their implications for the care plan.
- (2)
- PN require training in communicating with PwPs and care partner.
- (3)
- PNs, as part of the professional care team, should be able to design and implement a flexible routine network of service providers to support PwPs and their care partner in inpatient and outpatient settings.
- (4)
- The quality of care provided by PN may be influenced by specific training in the coordination of different stakeholders in the health care system and knowledge about local healthcare resources. Thus, PN should be trained to map available community resources and navigate PwPs towards them.
- (5)
- In order to advise and assist PwPs properly, an understanding of the disease and its complexity is indispensable, making it an essential part of a PN training. Considering the Knowledge Translation Framework, we propose that a PN training should include aspects of motivational interviewing in order to facilitate knowledge use [89].
- (6)
- Education on telemedicine should be incorporated whenever possible and applicable.
- (7)
- Based on these requirements, we propose that PN should be trained in three central aspects in order to deliver a personalized care approach: i. understanding PD, ii. health coaching and iii. delivering comprehensive care. These aspects form the framework of the PN training displayed in Table 4.
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gustavsson, A.; Svensson, M.; Jacobi, F.; Allgulander, C.; Alonso, J.; Beghi, E.; Dodel, R.; Ekman, M.; Faravelli, C.; Fratiglioni, L.; et al. Cost of disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 718–779. [Google Scholar] [CrossRef] [Green Version]
- Dorsey, E.R.; Constantinescu, R.; Thompson, J.P.; Biglan, K.M.; Holloway, R.G.; Kieburtz, K.; Marshall, F.J.; Ravina, B.M.; Schifitto, G.; Siderowf, A.; et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007, 68, 384–386. [Google Scholar] [CrossRef]
- Radder, D.L.M.; de Vries, N.M.; Riksen, N.P.; Diamond, S.J.; Gross, D.; Gold, D.R.; Heesakkers, J.; Henderson, E.; Hommel, A.L.A.J.; Lennaerts, H.H.; et al. Multidisciplinary care for people with Parkinson’s disease: The new kids on the block! Expert Rev. Neurother. 2019, 19, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Rajan, R.; Brennan, L.; Bloem, B.R.; Dahodwala, N.; Gardner, J.; Goldman, J.G.; Grimes, D.A.; Iansek, R.; Kovács, N.; McGinley, J.; et al. Integrated Care in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Mov. Disord. 2020, 35, 1509–1531. [Google Scholar] [CrossRef]
- Van der Marck, M.A.; Munneke, M.; Mulleners, W.; Hoogerwaard, E.M.; Borm, G.F.; Overeem, S.; Bloem, B.R. Integrated multidisciplinary care in Parkinson’s disease: A non-randomised, controlled trial (IMPACT). Lancet Neurol. 2013, 12, 947–956. [Google Scholar] [CrossRef]
- MacMahon, D.G. Parkinson’s disease nurse specialists: An important role in disease management. Neurology 1999, 52.7 (Suppl. 3), S21–S25. [Google Scholar]
- Prell, T.; Siebecker, F.; Lorrain, M.; Tönges, L.; Warnecke, T.; Klucken, J.; Wellach, I.; Buhmann, C.; Wolz, M.; Lorenzl, S.; et al. Specialized Staff for the Care of People with Parkinson’s Disease in Germany: An Overview. J. Clin. Med. 2020, 9, 2581. [Google Scholar] [CrossRef] [PubMed]
- Parkinson’s, U.K. A Competency Frame-Work for Nurses Working in Parkinson’s Disease Management, 3rd ed.; Parkinson’s U.K.: London, UK, 2016. [Google Scholar]
- Morgan, E.; Moran, M. The Parkinson’s disease nurse specialist. In Parkinson’s Disease in the Older Patient, 2nd ed.; Palyfer, J., Hindle, J.V., Lees, A., Eds.; CRC Press: London, UK, 2008; pp. 314–323. ISBN 9781315365428. [Google Scholar]
- Mai, T. Stand und Entwicklung der Rolle als Parkinson Nurse in Deutschland—Eine Online-Befragung. Pflege 2018, 31, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Schober, M.; Lehwaldt, D.; Rogers, M.; Steinke, M.; Turale, S.; Pulcini, J.; Roussel, J.; Stewart, D. Guidelines on Advanced Practice Nursing; International Council of Nurses: Geneva, Switzerland, 2020; ISBN 9789295099715. [Google Scholar]
- Bryant-Lukosius, D.; Spichiger, E.; Martin, J.; Stoll, H.; Kellerhals, S.D.; Fliedner, M.; Roussel, J.; de Geest, S. Framework for evaluating the impact of advanced practice nursing roles. J. Nurs. Scholarsh. 2016, 48, 201–209. [Google Scholar] [CrossRef] [PubMed]
- DiCenso, A.; Martin-Misener, R.; Bryant-Lukosius, D.; Bourgeault, I.; Kilpatrick, K.; Donald, F.; Kaasalainen, S.; Harbman, P.; Carter, N.; Kioke, S.; et al. Advanced practice nursing in Canada: Overview of a decision support synthesis. Nurs. Leadersh. 2010, 23, 15–34. [Google Scholar] [CrossRef]
- Carter, F.D.; Harbman, P.; Kilpatrick, K.; Martin-Misener, R.; Sherifali, D.; Tranmer, J.; Valaitis, R. Report on Advanced Practice Nursing (APN) in Canada. In Proceedings of the Global Summit, Ottawa, ON, Canada, 28–29 July 2014; Available online: https://fhs.mcmaster.ca/ccapnr/documents/CanadianReportGlobalAPNSummit2014June12FINAL.pdf (accessed on 14 May 2021).
- Bryant-Lukosius, D.; Carter, N.; Kilpatrick, K.; Martin-Misener, R.; Donald, F.; Kaasalainen, S.; Harbman, P.; Bourgeault, I.; DiCenso, A. The clinical nurse specialist role in Canada. Nurs. Leadersh. 2010, 23, 140–166. [Google Scholar] [CrossRef]
- Canadian Nurses Association. Advanced Practice Nursing. A Pan-Canadian Framework; Canadian Nurses Association: Ottawa, ON, Canada, 2019. [Google Scholar]
- Lennaerts, H.; Groot, M.; Rood, B.; Gilissen, K.; Tulp, H.; van Wensen, E.; Munneke, M.; van Laar, T.; Bloem, B.R. A Guideline for Parkinson’s Disease Nurse Specialists, with Recommendations for Clinical Practice. J. Parkinsons. Dis. 2017, 7, 749–754. [Google Scholar] [CrossRef]
- Fawcett, S.E.; Waller, M.A.; Miller, J.W.; Schwieterman, M.A.; Hazen, B.T.; Overstreet, R.E. A Trail Guide to Publishing Success: Tips on Writing Influential Conceptual, Qualitative, and Survey Research. J. Bus Logist. 2014, 35, 1–16. [Google Scholar] [CrossRef]
- Jaakkola, E. Designing conceptual articles: Four approaches. AMS Rev 2020, 10, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Lynham, S.A. The General Method of Theory-Building Research in Applied Disciplines. Adv. Dev. Hum. Resour. 2002, 4, 221–241. [Google Scholar] [CrossRef] [Green Version]
- Khalil, H.; Peters, M.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Parker, D. An Evidence-Based Approach to Scoping Reviews. Worldviews Evid. Based Nurs. 2016, 13, 118–123. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Bloem, B.R.; Rompen, L.; De Vries, N.M.; Klink, A.; Munneke, M.; Jeurissen, P. ParkinsonNet: A Low-Cost Health Care Innovation with A Systems Approach from The Netherlands. Health Aff. 2017, 36, 1987–1996. [Google Scholar] [CrossRef]
- Nijkrake, M.J.; Keus, S.H.J.; Overeem, S.; Oostendorp, R.A.B.; Vlieland, T.P.V.; Mulleners, W.; Hoogerwaard, E.M.; Bloem, B.R.; Munneke, M. The ParkinsonNet concept: Development, implementation and initial experience. Mov. Disord. 2010, 25, 823–829. [Google Scholar] [CrossRef]
- Tosserams, A.; de Vries, N.M.; Bloem, B.R.; Nonnekes, J. Multidisciplinary Care to Optimize Functional Mobility in Parkinson Disease. Clin. Geriatr. Med. 2020, 36, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Van der Eijk, M.; Bloem, B.R.; Nijhuis, F.A.P.; Koetsenruijter, J.; Vrijhoef, H.J.M.; Munneke, M.; Wensing, M.; Faber, M.J. Multidisciplinary Collaboration in Professional Networks for PD A Mixed-Method Analysis. J. Parkinsons. Dis. 2015, 5, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Larson, D.N.; Schneider, R.B.; Simuni, T. A New Era: The Growth of Video-Based Visits for Remote Management of Persons with Parkinson’s Disease. J. Parkinsons. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Okun, M.S.; Bloem, B.R. Care, Convenience, Comfort, Confidentiality, and Contagion: The 5 C’s that Will Shape the Future of Telemedicine. J. Parkinsons. Dis. 2020, 10, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Aye, Y.M.; Liew, S.; Neo, S.X.; Li, W.; Ng, H.-L.; Chua, S.-T.; Zhou, W.-T.; Au, W.-L.; Tan, E.-K.; Tay, K.-Y.; et al. Patient-Centric Care for Parkinson’s Disease: From Hospital to the Community. Front. Neurol. 2020, 11, 502. [Google Scholar] [CrossRef]
- Cohen, E.V.; Hagestuen, R.; González-Ramos, G.; Cohen, H.W.; Bassich, C.; Book, E.; Bradley, K.P.; Carter, J.H.; Di Minno, M.; Gardner, J.; et al. Interprofessional education increases knowledge, promotes team building, and changes practice in the care of Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22, 21–27. [Google Scholar] [CrossRef]
- Eggers, C.; Dano, R.; Schill, J.; Fink, G.R.; Timmermann, L.; Voltz, R.; Golla, H.; Lorenzl, S. Access to End-of Life Parkinson’s Disease Patients Through Patient-Centered Integrated Healthcare. Front. Neurol. 2018, 9, 627. [Google Scholar] [CrossRef] [Green Version]
- Fleisher, J.E.; Klostermann, E.C.; Hess, S.P.; Lee, J.; Myrick, E.; Chodosh, J. Interdisciplinary palliative care for people with advanced Parkinson’s disease: A view from the home. Ann. Palliat. Med. 2020, 9, S80–S89. [Google Scholar] [CrossRef]
- Fründt, O.; Mainka, T.; Schönwald, B.; Müller, B.; Dicusar, P.; Gerloff, C.; Buhmann, C. The Hamburg Parkinson day-clinic: A new treatment concept at the border of in- and outpatient care. J. Neural. Transm. 2018, 125, 1461–1472. [Google Scholar] [CrossRef]
- Giladi, N.; Manor, Y.; Hilel, A.; Gurevich, T. Interdisciplinary teamwork for the treatment of people with Parkinson’s disease and their families. Curr. Neurol. Neurosci. Rep. 2014, 14, 493. [Google Scholar] [CrossRef]
- Grimes, D.; Fitzpatrick, M.; Gordon, J.; Miyasaki, J.; Fon, E.A.; Schlossmacher, M.; Suchowersky, O.; Rajput, A.; Lafontaine, A.L.; Mestre, T.; et al. Canadian guideline for Parkinson disease. CMAJ 2019, 191, E989–E1004. [Google Scholar] [CrossRef] [Green Version]
- Hack, N.; Akbar, U.; Monari, E.H.; Eilers, A.; Thompson-Avila, A.; Hwynn, N.H.; Sriram, A.; Haq, I.; Hardwick, A.; Malaty, I.A.; et al. Person-Centered Care in the Home Setting for Parkinson’s Disease: Operation House Call Quality of Care Pilot Study. Parkinsons. Dis. 2015, 2015, 639494. [Google Scholar] [CrossRef]
- Iansek, R. Interdisciplinary rehabilitation in Parkinson’s disease. Adv. Neurol. 1999, 80, 555–559. [Google Scholar] [PubMed]
- Jones, B.; Hopkins, G.; Wherry, S.-A.; Lueck, C.J.; Das, C.P.; Dugdale, P. Evaluation of a Regional Australian Nurse-Led Parkinson’s Service Using the Context, Input, Process, and Product Evaluation Model. Clin. Nurse Spec. 2016, 30, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Kessler, D.; Hatch, S.; Alexander, L.; Grimes, D.; Côté, D.; Liddy, C.; Mestre, T. The Integrated Parkinson’s disease Care Network (IPCN): Qualitative evaluation of a new approach to care for Parkinson’s disease. Patient Educ. Couns. 2021, 104, 136–142. [Google Scholar] [CrossRef]
- Keus, S.H.J.; Nijkrake, M.J.; Borm, G.F.; Kwakkel, G.; Roos, R.A.C.; Berendse, H.W.; Adang, E.M.; Overeem, S.; Bloem, B.R.; Munneke, M. The ParkinsonNet trial: Design and baseline characteristics. Mov. Disord. 2010, 25, 830–837. [Google Scholar] [CrossRef]
- Loewenbrück, K.F.; Stein, D.B.; Amelung, V.E.; Bitterlich, R.; Brumme, M.; Falkenburger, B.; Fehre, A.; Feige, T.; Frank, A.; Gißke, C.; et al. Parkinson Network Eastern Saxony (PANOS): Reaching Consensus for a Regional Intersectoral Integrated Care Concept for Patients with Parkinson’s Disease in the Region of Eastern Saxony, Germany. J. Clin. Med. 2020, 9, 2906. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Laurini, A.; Rocca, B.; Foti, C. In-patient multidisciplinary rehabilitation for Parkinson’s disease: A randomized controlled trial. Mov. Disord. 2015, 30, 1050–1058. [Google Scholar] [CrossRef]
- Radder, D.L.M.; Nonnekes, J.; van Nimwegen, M.; Eggers, C.; Abbruzzese, G.; Alves, G.; Browner, N.; Chaudhuri, K.R.; Ebersbach, G.; Ferreira, J.J.; et al. Recommendations for the Organization of Multidisciplinary Clinical Care Teams in Parkinson’s Disease. J. Parkinsons. Dis. 2020, 10, 1087–1098. [Google Scholar] [CrossRef]
- Rompen, L.; De Vries, N.M.; Munneke, M.; Neff, C.; Sachs, T.; Cedrone, S.; Cheves, J.; Bloem, B.R. Introduction of Network-Based Healthcare at Kaiser Permanente. J. Parkinsons. Dis. 2020, 10, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Shrubsole, K. Implementation of an integrated multidisciplinary Movement Disorders Clinic: Applying a knowledge translation framework to improve multidisciplinary care. Disabil. Rehabil. 2019, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Anderson, W.S.; Brandt, J.; Mari, Z.; Pontone, G.M. Neuropsychiatric Complications of Parkinson Disease Treatments: Importance of Multidisciplinary Care. Am. J. Geriatr. Psychiatry 2016, 24, 1171–1180. [Google Scholar] [CrossRef] [Green Version]
- Tönges, L.; Ehret, R.; Lorrain, M.; Riederer, P.; Müngersdorf, M. Epidemiology of Parkinson’s Disease and Current Concepts of Outpatient Care in Germany. Fortschr. Neurol. Psychiatr. 2017, 85, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Van der Marck, M.A.; Bloem, B.R. How to organize multispecialty care for patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2014, 20, S167–S173. [Google Scholar] [CrossRef]
- Vaughan, C.P.; Prizer, L.P.; Vandenberg, A.E.; Goldstein, F.C.; Trotti, L.M.; Hermida, A.P.; Factor, S.A. A Comprehensive Approach to Care in Parkinson’s Disease Adds Quality to the Current Gold Standard. Mov. Disord. Clin. Pract. 2017, 4, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Vickers, L.F.; O’Neill, C.M. An interdisciplinary home healthcare program for patients with Parkinson’s disease. Rehabil. Nurs. 1998, 23, 286–289. [Google Scholar] [CrossRef]
- Albanese, A.; Di Fonzo, A.; Fetoni, V.; Franzini, A.; Gennuso, M.; Molini, G.; Pacchetti, C.; Priori, A.; Riboldazzi, G.; Volonté, M.A.; et al. Design and Operation of the Lombardy Parkinson’s Disease Network. Front. Neurol. 2020, 11, 573. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.I.; Cheng, E.M.; Barry, F.; Siebens, H.C.; Lee, M.L.; Ganz, D.A.; Mittman, B.S.; Connor, M.K.; Edwards, L.K.; McGowan, M.G.; et al. Randomized trial of care management to improve Parkinson disease care quality. Neurology 2019, 92, e1831–e1842. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, J.; Barbosa, W.; Sweeney, M.M.; Oyler, S.E.; Lemen, A.C.; Fazl, A.; Ko, M.; Meisel, T.; Friede, N.; Dacpano, G.; et al. Interdisciplinary Home Visits for Individuals with Advanced Parkinson’s Disease and Related Disorders. J. Am. Geriatr. Soc. 2018, 66, 1226–1232. [Google Scholar] [CrossRef]
- Marr, J.A.; Reid, B. Implementing managed care and case management: The neuroscience experience. J. Neurosci. Nurs. 1992, 24, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Pretzer-Aboff, I.; Prettyman, A. Implementation of an Integrative Holistic Healthcare Model for People Living with Parkinson’s Disease. Gerontologist 2015, 55 (Suppl. 1), S146–S153. [Google Scholar] [CrossRef] [Green Version]
- Mestre, T.A.; Kessler, D.; Côté, D.; Liddy, C.; Thavorn, K.; Taljaard, M.; Grimes, D. Pilot Evaluation of a Pragmatic Network for Integrated Care and Self-Management in Parkinson’s Disease. Mov. Disord. 2021, 36, 398–406. [Google Scholar] [CrossRef]
- Achey, M.A.; Beck, C.A.; Beran, D.B.; Boyd, C.M.; Schmidt, P.N.; Willis, A.W.; Riggare, S.S.; Simone, R.B.; Biglan, K.M.; Dorsey, E.R. Virtual house calls for Parkinson disease (Connect.Parkinson): Study protocol for a randomized, controlled trial. Trials 2014, 15, 465. [Google Scholar] [CrossRef] [Green Version]
- Dorsey, E.R.; Achey, M.A.; Beck, C.A.; Beran, D.B.; Biglan, K.M.; Boyd, C.M.; Schmidt, P.N.; Simone, R.; Willis, A.W.; Galifianakis, N.B.; et al. National Randomized Controlled Trial of Virtual House Calls for People with Parkinson’s Disease: Interest and Barriers. Telemed. J. E Health 2016, 22, 590–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorm, L.R.; Walter, S.R.; Lujic, S.; Byles, J.E.; Kendig, H.L. Home and community care services: A major opportunity for preventive health care. BMC Geriatr. 2010, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Hellqvist, C.; Dizdar, N.; Hagell, P.; Berterö, C.; Sund-Levander, M. Improving self-management for persons with Parkinson’s disease through education focusing on management of daily life: Patients’ and relatives’ experience of the Swedish National Parkinson School. J. Clin. Nurs. 2018, 27, 3719–3728. [Google Scholar] [CrossRef]
- Hellqvist, C. Promoting Self-Care in Nursing Encounters with Persons Affected by Long-Term Conditions-A Proposed Model to Guide Clinical Care. Int. J. Environ. Res. Public Health 2021, 18, 2223. [Google Scholar] [CrossRef]
- Schröder, S.; Martus, P.; Odin, P.; Schaefer, M. Impact of community pharmaceutical care on patient health and quality of drug treatment in Parkinson’s disease. Int. J. Clin. Pharm. 2012, 34, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Coulter, A.; Cleary, P.D. Patients’ experiences with hospital care in five countries. Health Aff. 2001, 20, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl Hammarlund, C.; Westergren, A.; Åström, I.; Edberg, A.-K.; Hagell, P. The Impact of Living with Parkinson’s Disease: Balancing within a Web of Needs and Demands. Parkinsons. Dis. 2018, 2018, 4598651. [Google Scholar] [CrossRef] [PubMed]
- Minkman, M.M.N. Developing integrated care. Towards a development model for integrated care. Int. J. Integr. Care 2012, 12, e197. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Evans, D.B. Health Systems Performance Assessment: Debates, Methods and Empiricism; World Health Organization: Geneva, Switzerland, 2003; ISBN 9789241562454. [Google Scholar]
- Hartweg, D. Dorothea Orem: Self-Care Deficit Theory: Notes on Nursing Theories Volume 4; SAGE Publications: Thousand Oaks, CA, USA, 1991; ISBN 0803942990. [Google Scholar]
- Van der Eijk, M.; Faber, M.J.; Al Shamma, S.; Munneke, M.; Bloem, B.R. Moving towards patient-centered healthcare for patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2011, 17, 360–364. [Google Scholar] [CrossRef]
- Fereshtehnejad, S.-M.; Lökk, J. Active aging for individuals with Parkinson’s disease: Definitions, literature review, and models. Parkinsons. Dis. 2014, 2014, 739718. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Davis, C.L.; Funnell, M.M.; Beck, A. Implementing Practical Interventions to Support Chronic Illness Self-Management. JT Comm. J. Qual. Saf. 2003, 29, 563–574. [Google Scholar] [CrossRef]
- Freeman, G.K.; Olesen, F.; Hjortdahl, P. Continuity of care: An essential element of modern general practice? Fam. Pract. 2003, 20, 623–627. [Google Scholar] [CrossRef] [Green Version]
- Fabbri, M.; Caldas, A.C.; Ramos, J.B.; Sanchez-Ferro, Á.; Antonini, A.; Růžička, E.; Lynch, T.; Rascol, O.; Grimes, D.; Eggers, C.; et al. Moving towards home-based community-centred integrated care in Parkinson’s disease. Parkinsonism Relat. Disord. 2020, 78, 21–26. [Google Scholar] [CrossRef]
- Goodwin, N. Understanding Integrated Care. Int. J. Integr. Care 2016, 16, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenison, E.; Smink, A.; Redwood, S.; Darweesh, S.; Cottle, H.; van Halteren, A.; van den Haak, P.; Hamlin, R.; Ypinga, J.; Bloem, B.R.; et al. Proactive and Integrated Management and Empowerment in Parkinson’s Disease: Designing a New Model of Care. Parkinsons. Dis. 2020, 2020. [Google Scholar] [CrossRef]
- Valentijn, P.P.; Schepman, S.M.; Opheij, W.; Bruijnzeels, M.A. Understanding integrated care: A comprehensive conceptual framework based on the integrative functions of primary care. Int. J. Integr. Care 2013, 13, e010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving chronic illness care: Translating evidence into action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Halteren, A.D.; Munneke, M.; Smit, E.; Thomas, S.; Bloem, B.R.; Darweesh, S.K.L. Personalized Care Management for Persons with Parkinson’s Disease. J. Parkinsons. Dis. 2020, 10, S11–S20. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, C.S.; Leff, B.; Garrigues, S.K.; Perissinotto, C.; Sheehan, O.C.; Harrison, K.L. A Quality of Care Framework for Home-Based Medical Care. J. Am. Med. Dir. Assoc. 2018, 19, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef]
- Titova, N.; Chaudhuri, K.R. Personalized medicine in Parkinson’s disease: Time to be precise. Mov. Disord. 2017, 32, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishna, A.; Alexander, S.A. Understanding Parkinson Disease: A Complex and Multifaceted Illness. J. Neurosci. Nurs. 2015, 47, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.J.; Godinho, C.; Santos, A.T.; Domingos, J.; Abreu, D.; Lobo, R.; Gonçalves, N.; Barra, M.; Larsen, F.; Fagerbakke, Ø.; et al. Quantitative home-based assessment of Parkinson’s symptoms: The SENSE-PARK feasibility and usability study. BMC Neurol. 2015, 15, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, D.; Liddy, C. Self-management support programs for persons with Parkinson’s disease: An integrative review. Patient Educ. Couns. 2017, 100, 1787–1795. [Google Scholar] [CrossRef]
- Kessler, D.; Hauteclocque, J.; Grimes, D.; Mestre, T.; Côtéd, D.; Liddy, C. Development of the Integrated Parkinson’s Care Network (IPCN): Using co-design to plan collaborative care for people with Parkinson’s disease. Qual. Life Res. 2019, 28, 1355–1364. [Google Scholar] [CrossRef]
- Lawn, S.; Schoo, A. Supporting self-management of chronic health conditions: Common approaches. Patient Educ. Couns. 2010, 80, 205–211. [Google Scholar] [CrossRef]
- Tennigkeit, J.; Feige, T.; Haak, M.; Hellqvist, C.; Seven, Ü.S.; Kalbe, E.; Schwarz, J.; Warnecke, T.; Tönges, L.; Eggers, C.; et al. Structured Care and Self-Management Education for Persons with Parkinson’s Disease: Why the First Does Not Go without the Second-Systematic Review, Experiences and Implementation Concepts from Sweden and Germany. J. Clin. Med. 2020, 9, 2787. [Google Scholar] [CrossRef]
- Chenoweth, L.; Gallagher, R.; Sheriff, J.N.; Donoghue, J.; Stein-Parbury, J. Factors supporting self-management in Parkinson’s disease: Implications for nursing practice. Int. J. Older People Nurs. 2008, 3, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Rollnick, S.; Miller, W.R. What is Motivational Interviewing? Behav. Cogn. Psychother. 1995, 23, 325–334. [Google Scholar] [CrossRef]
- Achey, M.; Aldred, J.L.; Aljehani, N.; Bloem, B.R.; Biglan, K.M.; Chan, P.; Cubo, E.; Dorsey, E.R.; Goetz, C.G.; Guttman, M.; et al. The past, present, and future of telemedicine for Parkinson’s disease. Mov. Disord. 2014, 29, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Bhidayasiri, R.; Martinez-Martin, P. Clinical Assessments in Parkinson’s Disease: Scales and Monitoring. Int. Rev. Neurobiol. 2017, 132, 129–182. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Henderson, E.J.; Dorsey, E.R.; Okun, M.S.; Okubadejo, N.; Chan, P.; Andrejack, J.; Darweesh, S.K.L.; Munneke, M. Integrated and patient-centred management of Parkinson’s disease: A network model for reshaping chronic neurological care. Lancet Neurol. 2020, 19, 623–634. [Google Scholar] [CrossRef]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s disease. Lancet 2021. [Google Scholar] [CrossRef]
- Beck, C.A.; Beran, D.B.; Biglan, K.M.; Boyd, C.M.; Dorsey, E.R.; Schmidt, P.N.; Simone, R.; Willis, A.W.; Galifianakis, N.B.; Katz, M.; et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology 2017, 89, 1152–1161. [Google Scholar] [CrossRef]
- Bianchi, M.; Bagnasco, A.; Bressan, V.; Barisone, M.; Timmins, F.; Rossi, S.; Pellegrini, R.; Aleo, G.; Sasso, L. A review of the role of nurse leadership in promoting and sustaining evidence-based practice. J. Nurs. Manag. 2018, 26, 918–932. [Google Scholar] [CrossRef]
- Reynolds, H.; Wilson-Barnett, J.; Richardson, G. Evaluation of the role of the Parkinson’s disease nurse specialist. Int. J. Nurs. Stud. 2000, 37, 337–349. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Browne, P.; Chan, P.; Cubo, E.; Guttman, M.; Hassan, A.; Hatcher-Martin, J.; Mari, Z.; Moukheiber, E.; Okubadejo, N.U.; et al. The Promise of Telemedicine for Movement Disorders: An Interdisciplinary Approach. Curr. Neurol. Neurosci. Rep. 2018, 18, 26. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Venkataraman, V.; Grana, M.J.; Bull, M.T.; George, B.P.; Boyd, C.M.; Beck, C.A.; Rajan, B.; Seidmann, A.; Biglan, K.M. Randomized controlled clinical trial of “virtual house calls” for Parkinson disease. JAMA Neurol. 2013, 70, 565–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chirra, M.; Marsili, L.; Wattley, L.; Sokol, L.L.; Keeling, E.; Maule, S.; Sobrero, G.; Artusi, C.A.; Romagnolo, A.; Zibetti, M.; et al. Telemedicine in Neurological Disorders: Opportunities and Challenges. Telemed. J. E Health 2019, 25, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Monje, M.H.G.; Foffani, G.; Obeso, J.; Sánchez-Ferro, Á. New Sensor and Wearable Technologies to Aid in the Diagnosis and Treatment Monitoring of Parkinson’s Disease. Annu. Rev. Biomed. Eng. 2019, 21, 111–143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country | Role | Formal Education | Reference |
|---|---|---|---|
| United Kingdom | Being responsible for overall management within primary or secondary care teams Resource of Information and advice for PwPs Catalyst for improving public awareness | Provided via national universities Prerequisite:
| [8,9] |
| Germany | Providing information and advice to patients and care givers on medication, symptoms and treatment options | Provided via German Parkinson Society (DPG), German Parkinson Association, (dPV), Parkinson Competence Network (KNP), Association of Parkinson Nurses and Assistants (VPNA) Prerequisite:
| [7,10] |
| United States 1 | Role of APN (generally)
| Advanced Practice Nurse (APN) → post-graduate education in nursing Two Types of APN roles have been recognized in the United States.
Prerequisite:
| [11,12] |
| Canada 1 | Role of APN (generally)
| Two types of APN roles have been recognized in Canada.
NP → Registered nurses; completed NP education program; Bachelor- or Master’s degree CNP → Master or Doctoral degree in nursing Topics covered during education for APNs:
| [13,14,15,16] |
| Care Priority | Citation (Frequency) | Reference |
|---|---|---|
| Multidisciplinary care | 24 | [19,24,25,26,27,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] |
| Patient-centeredness | 17 | [24,25,26,27,32,36,39,40,41,42,43,44,45,47,48,52,53,54,55,56] |
| Integrated care | 16 | [3,24,25,26,27,31,32,36,38,40,42,44,45,46,48,51,52,56,57] |
| Home-based care | 13 | [36,37,40,41,42,44,51,53,56,57,58,59,60] |
| Self-management | 11 | [24,25,26,27,36,39,40,44,45,55,57,61,62] |
| Community-centered care | 9 | [24,25,26,27,30,41,45,52,53,59,60,63] |
| Patient-/care partner education | 7 | [36,39,40,42,44,51,55] |
| Telemedicine | 7 | [30,42,44,56,57,58,59] |
| Professional education | 1 | [55] |
| Care Priority | Citation (Frequency) | Reference |
|---|---|---|
| Patient-centeredness | 9 | [64,65,66,67,68,69,70,71,72] |
| Integrated care | 8 | [66,68,69,73,74,75,76,77] |
| Multidisciplinary care | 6 | [64,66,68,74,76,78] |
| Community-centered care | 6 | [67,68,69,71,77,78] |
| Home-based care | 5 | [28,29,65,68,73,79] |
| Personalized care | 4 | [70,75,78,80] |
| Self-management | 4 | [65,70,73,77] |
| Patient-/care partner education | 2 | [75,80] |
| Telemedicine | 1 | [28,29] |
| Professional education | 1 | [65] |
| Module | Topic | Components | Goals |
|---|---|---|---|
| 1 | Understanding Parkinson’s disease |
| Acquire fundamental knowledge about PD and management principles of motor and non-motor symptoms |
| 2 | Being a health coach |
| Acquire skills and knowledge to assess patient-outcomes and identify personal care requirements |
| 3 | Aspects of care delivery for people living with Parkinson’s disease and care partner |
| Acquire knowledge about available local care resources and methods to motivate patients and care partners to use them |
| 4 | Telemedicine |
| Acquire knowledge about the technology |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Munster, M.; Stümpel, J.; Thieken, F.; Pedrosa, D.J.; Antonini, A.; Côté, D.; Fabbri, M.; Ferreira, J.J.; Růžička, E.; Grimes, D.; et al. Moving towards Integrated and Personalized Care in Parkinson’s Disease: A Framework Proposal for Training Parkinson Nurses. J. Pers. Med. 2021, 11, 623. https://doi.org/10.3390/jpm11070623
van Munster M, Stümpel J, Thieken F, Pedrosa DJ, Antonini A, Côté D, Fabbri M, Ferreira JJ, Růžička E, Grimes D, et al. Moving towards Integrated and Personalized Care in Parkinson’s Disease: A Framework Proposal for Training Parkinson Nurses. Journal of Personalized Medicine. 2021; 11(7):623. https://doi.org/10.3390/jpm11070623
Chicago/Turabian Stylevan Munster, Marlena, Johanne Stümpel, Franziska Thieken, David J. Pedrosa, Angelo Antonini, Diane Côté, Margherita Fabbri, Joaquim J. Ferreira, Evžen Růžička, David Grimes, and et al. 2021. "Moving towards Integrated and Personalized Care in Parkinson’s Disease: A Framework Proposal for Training Parkinson Nurses" Journal of Personalized Medicine 11, no. 7: 623. https://doi.org/10.3390/jpm11070623
APA Stylevan Munster, M., Stümpel, J., Thieken, F., Pedrosa, D. J., Antonini, A., Côté, D., Fabbri, M., Ferreira, J. J., Růžička, E., Grimes, D., & Mestre, T. A. (2021). Moving towards Integrated and Personalized Care in Parkinson’s Disease: A Framework Proposal for Training Parkinson Nurses. Journal of Personalized Medicine, 11(7), 623. https://doi.org/10.3390/jpm11070623