
Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
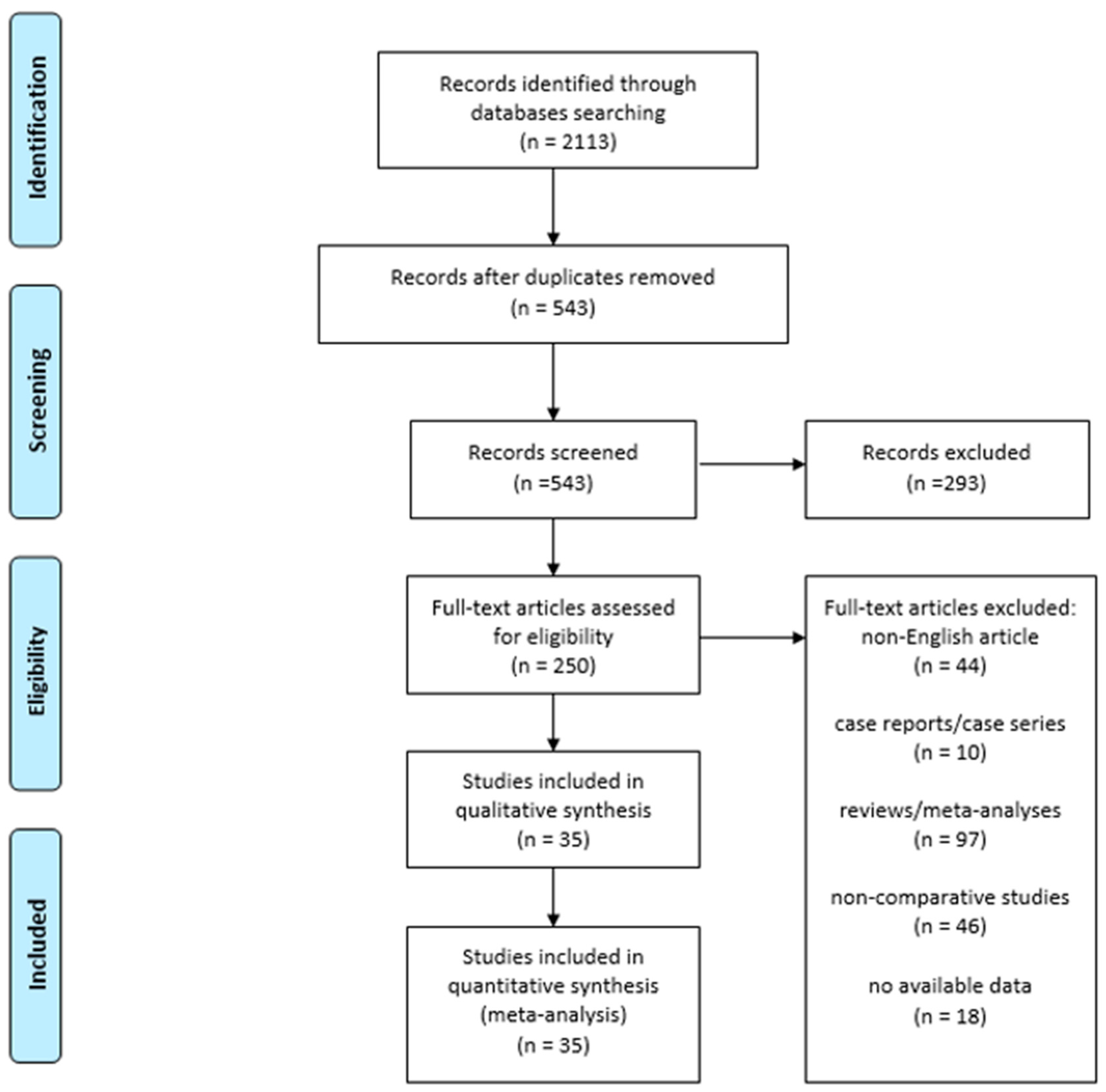
2.1. Literature Search and Study Selection
2.2. Data Extraction and Risk of Bias Assessment
2.3. Statistical Analysis
3. Results
Study Selection
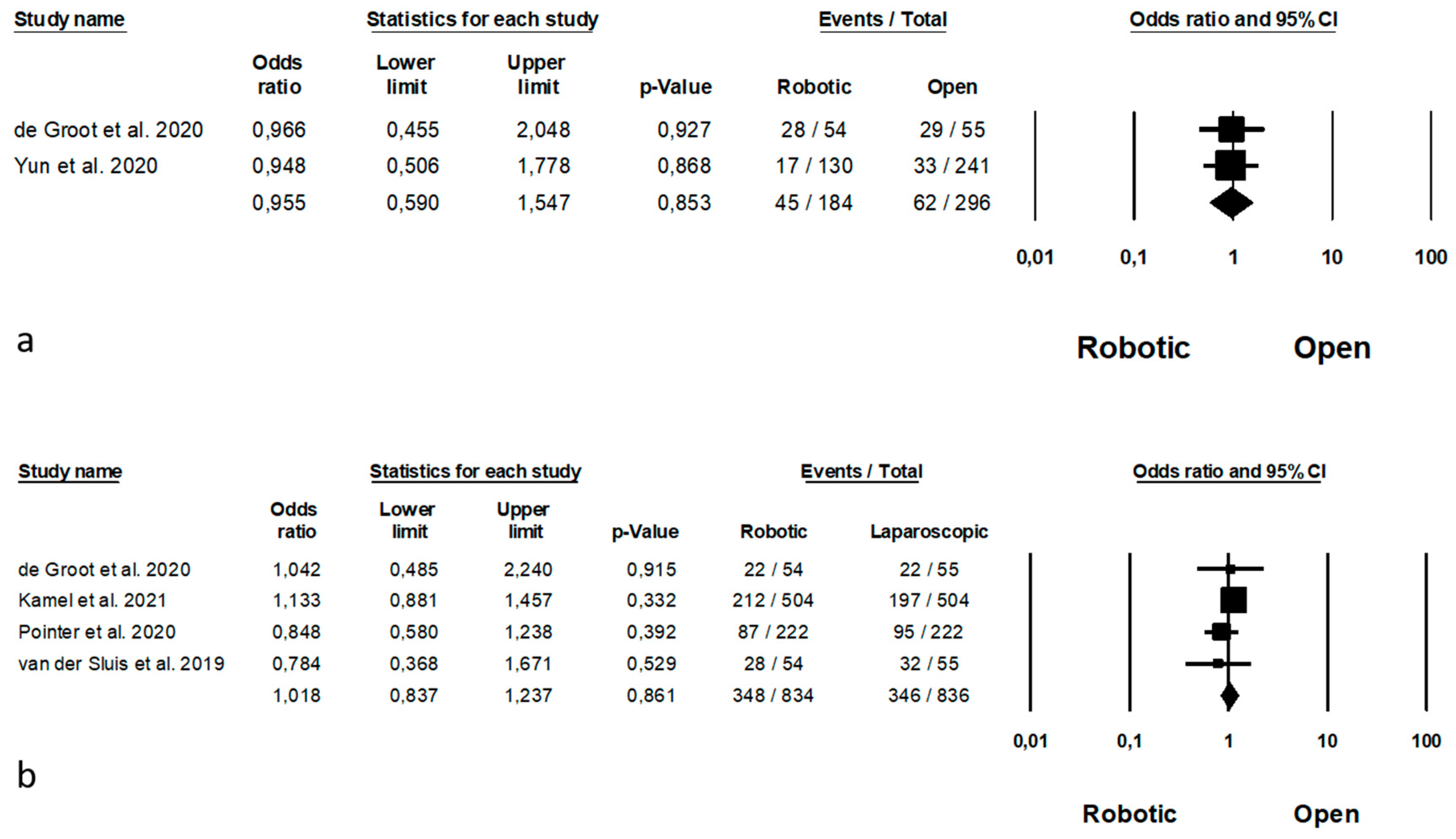
4. Robotic Versus Laparoscopic Esophagectomy
4.1. Study Characteristics
4.2. Risk of Bias Assessment
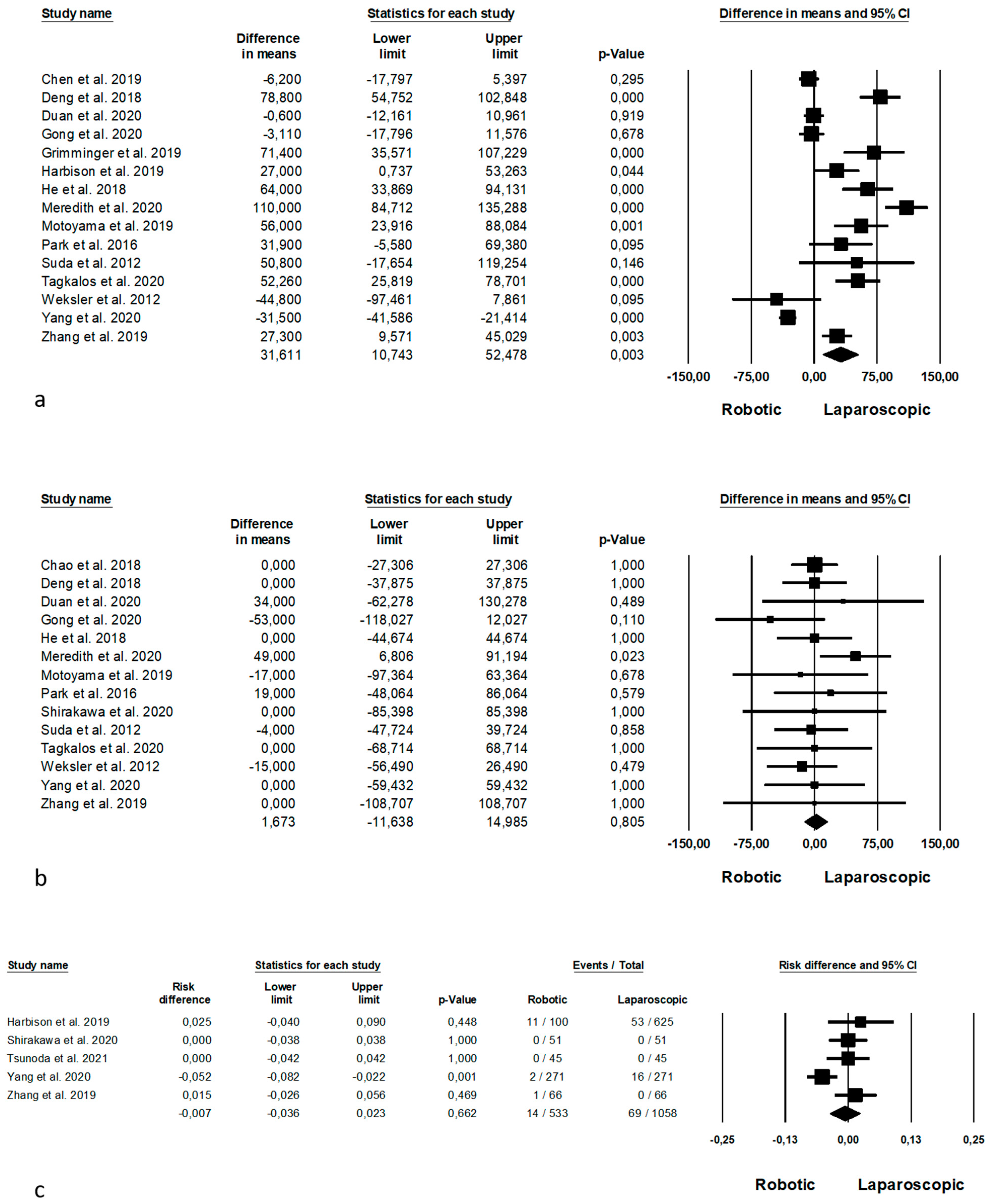
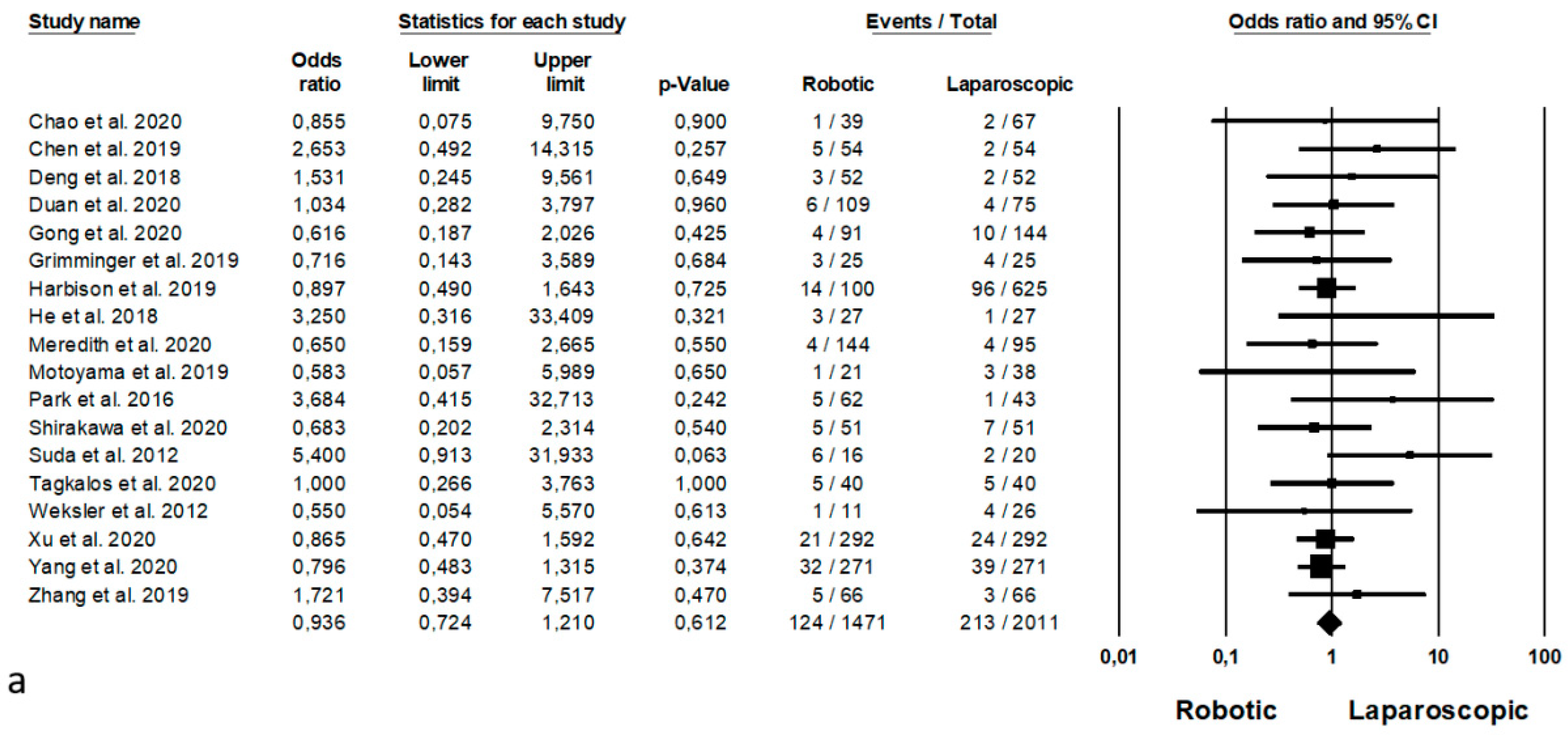
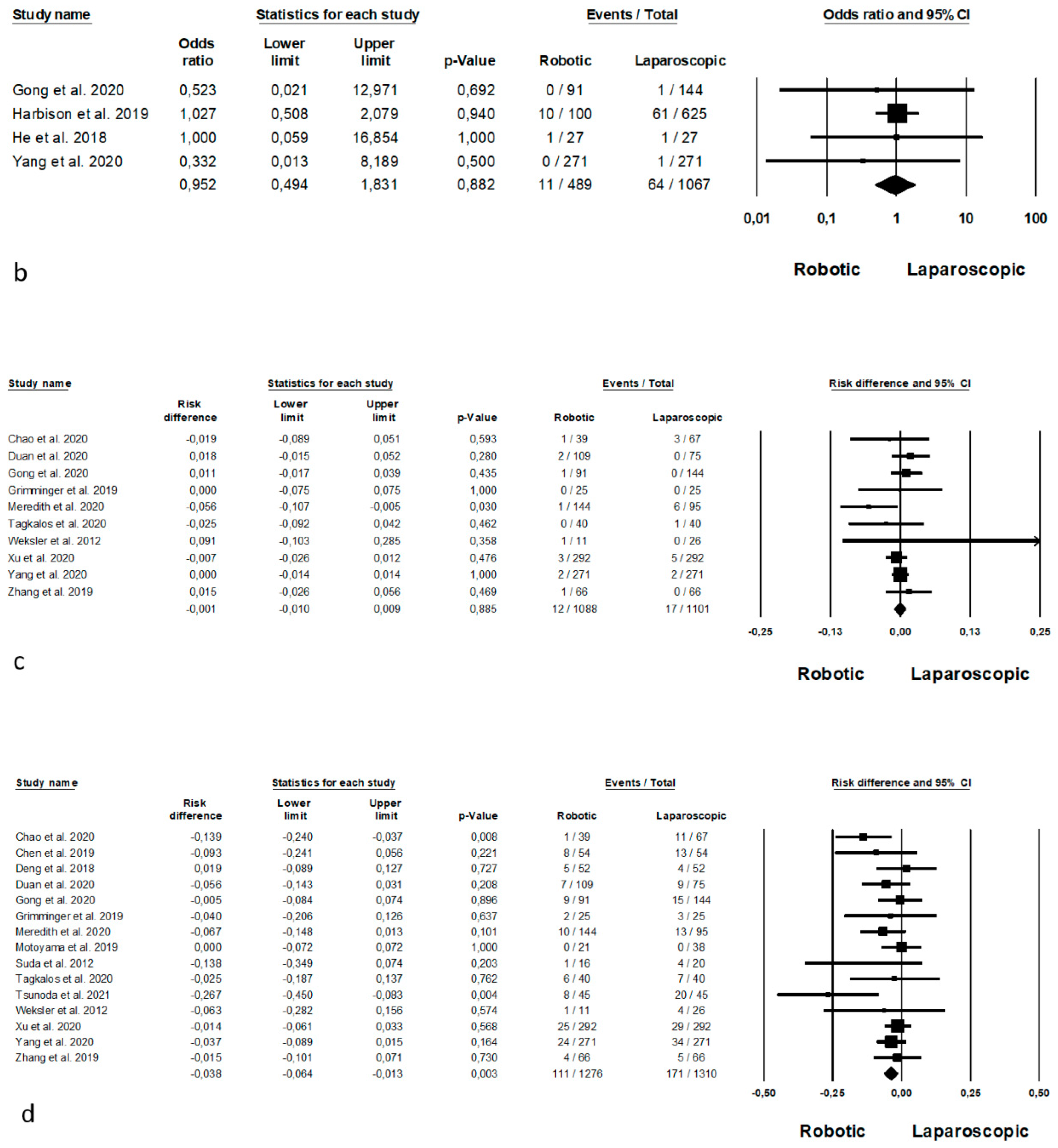
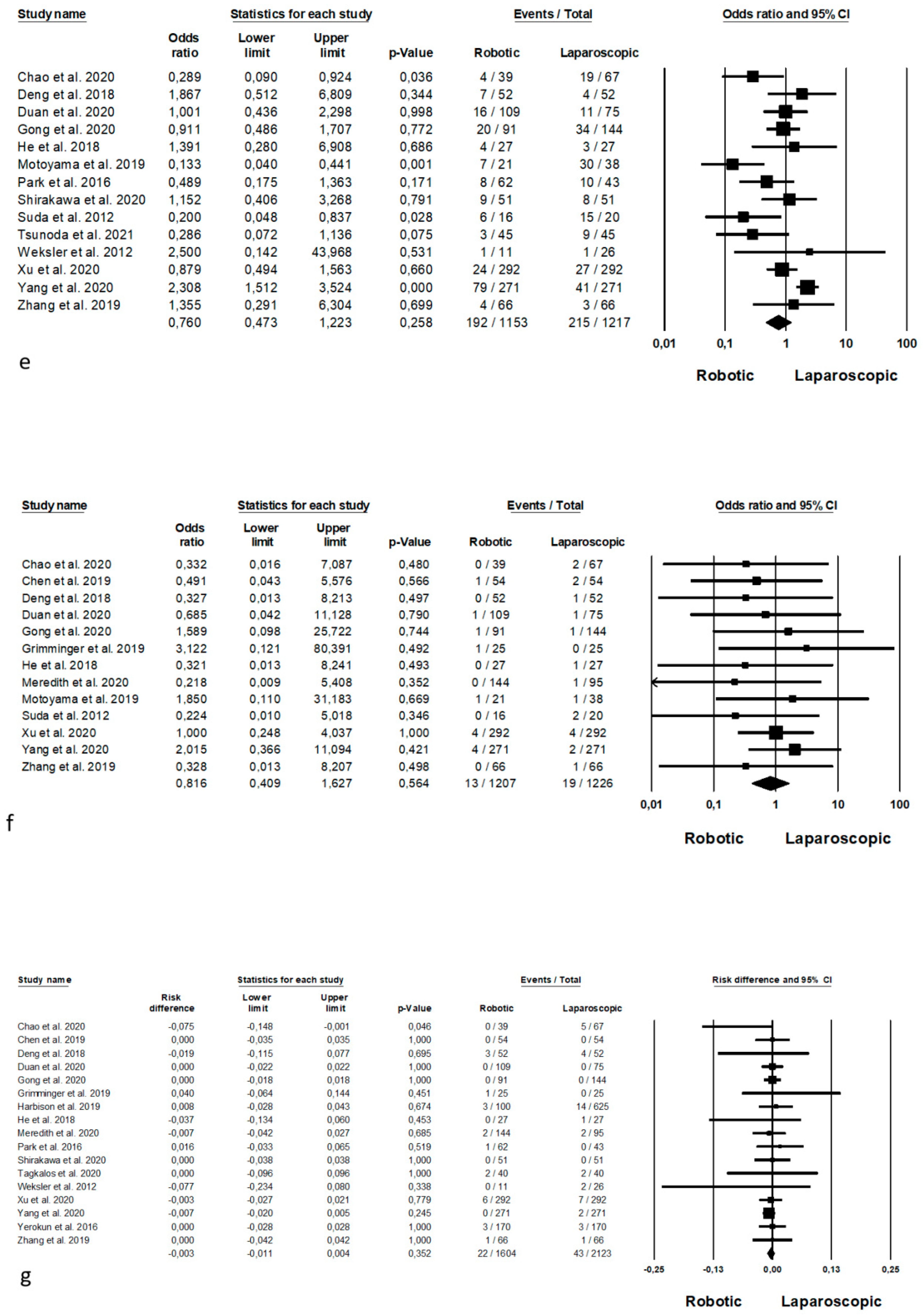
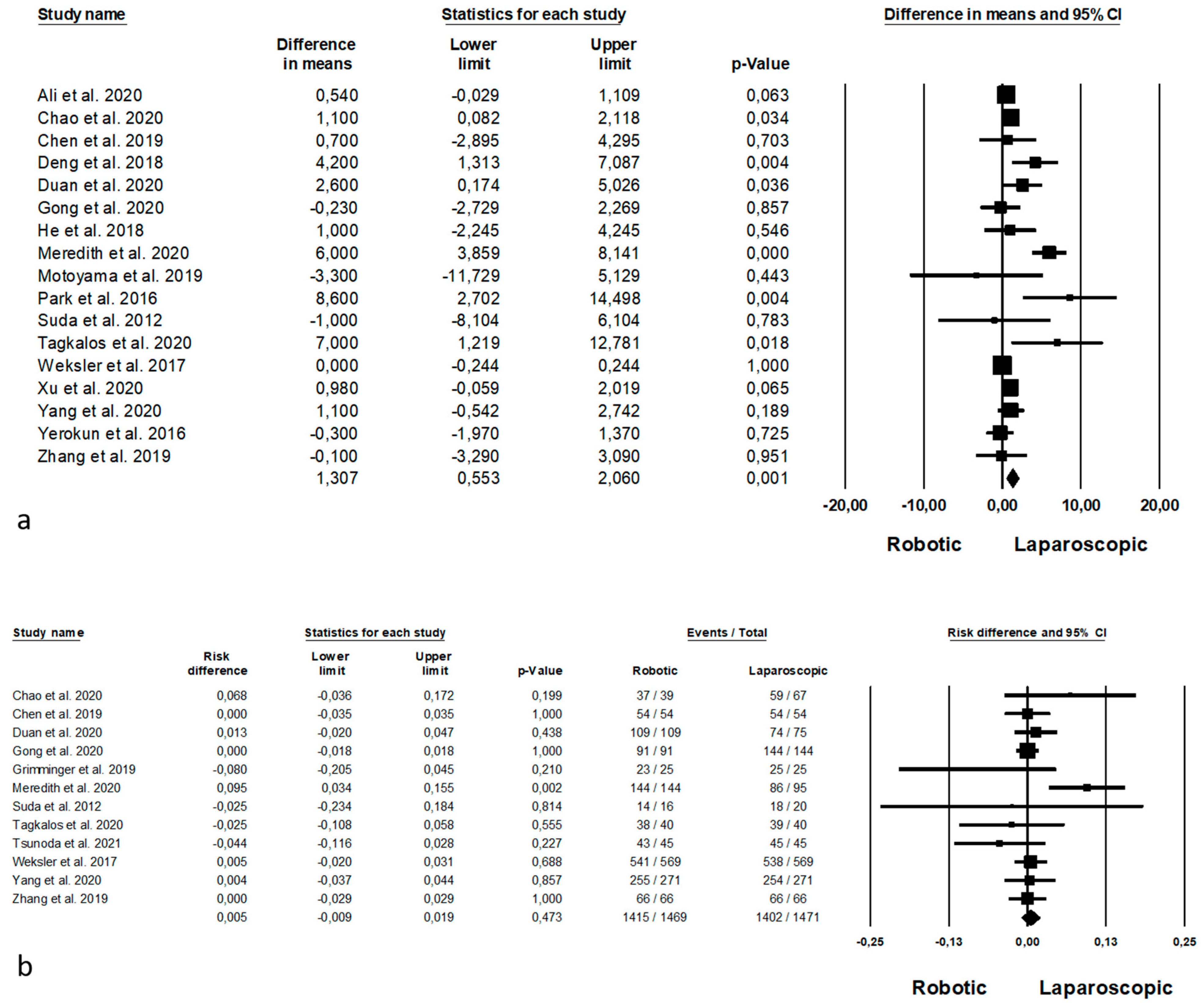
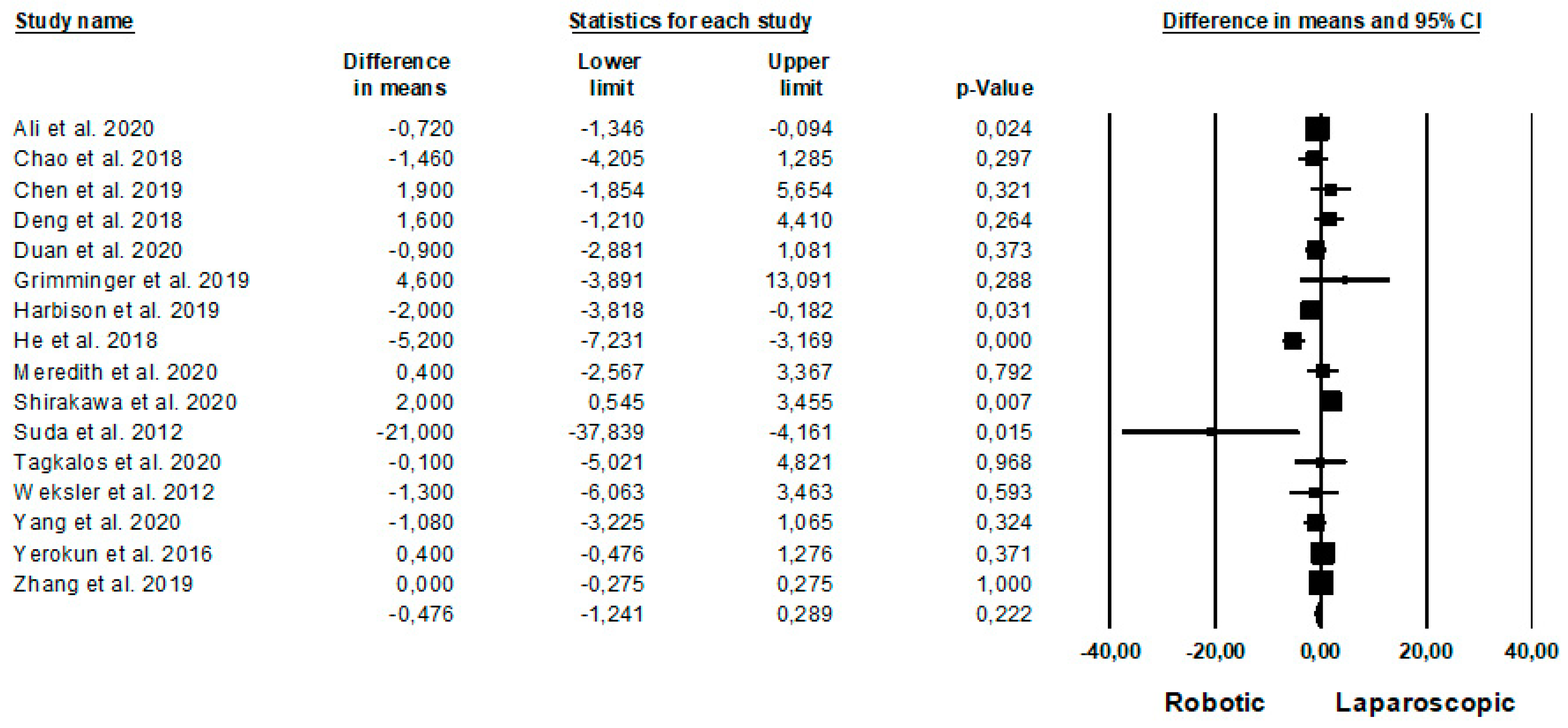
4.3. Short Term-Outcomes
5. Long-Term Outcomes
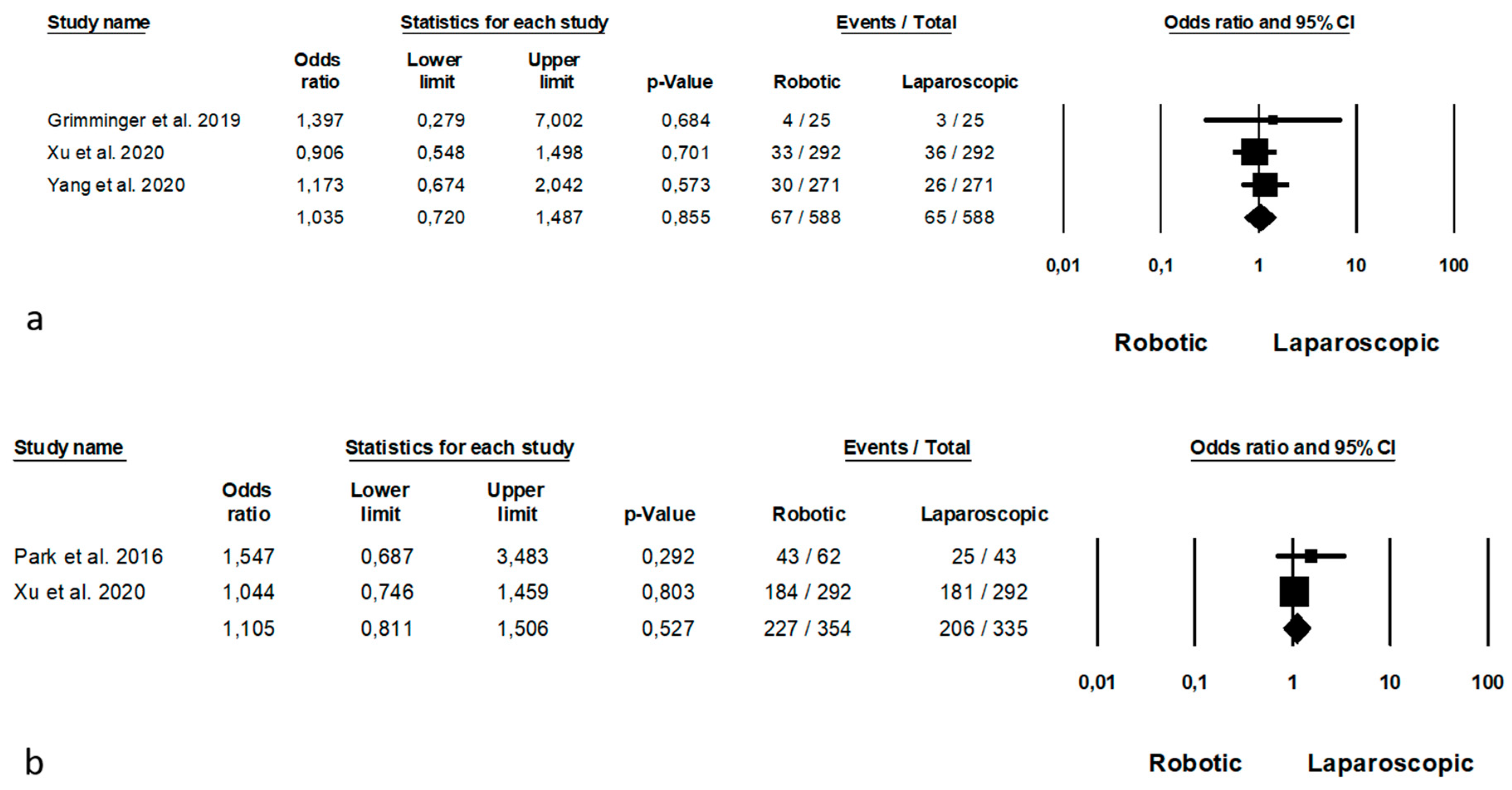
6. Subgroup Analysis
6.1. Fully Robotic vs. Fully Laparoscopic Procedures
6.2. McKeown Esophagectomy
6.3. Ivor-Lewis Esophagectomy
6.4. Publication Bias
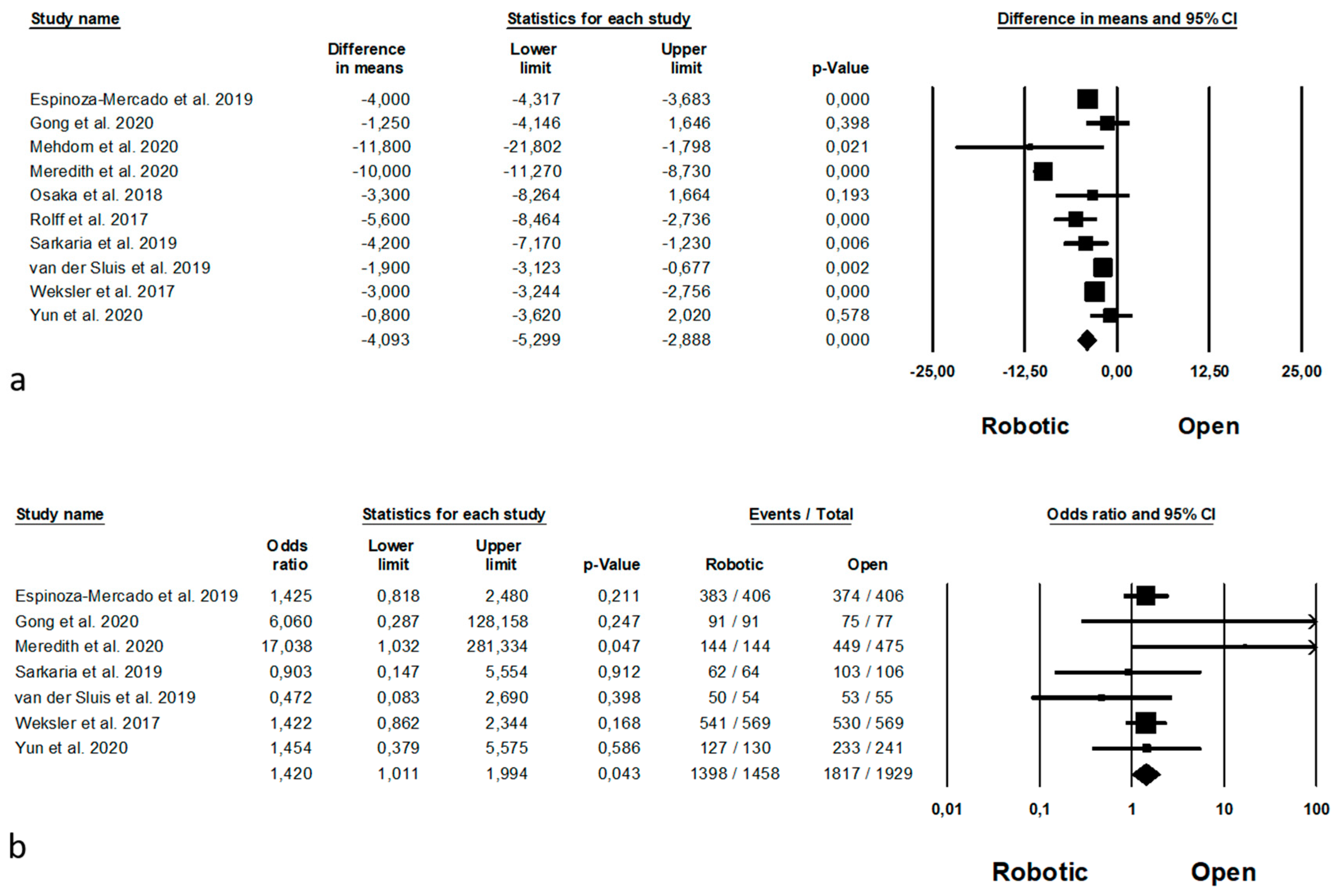
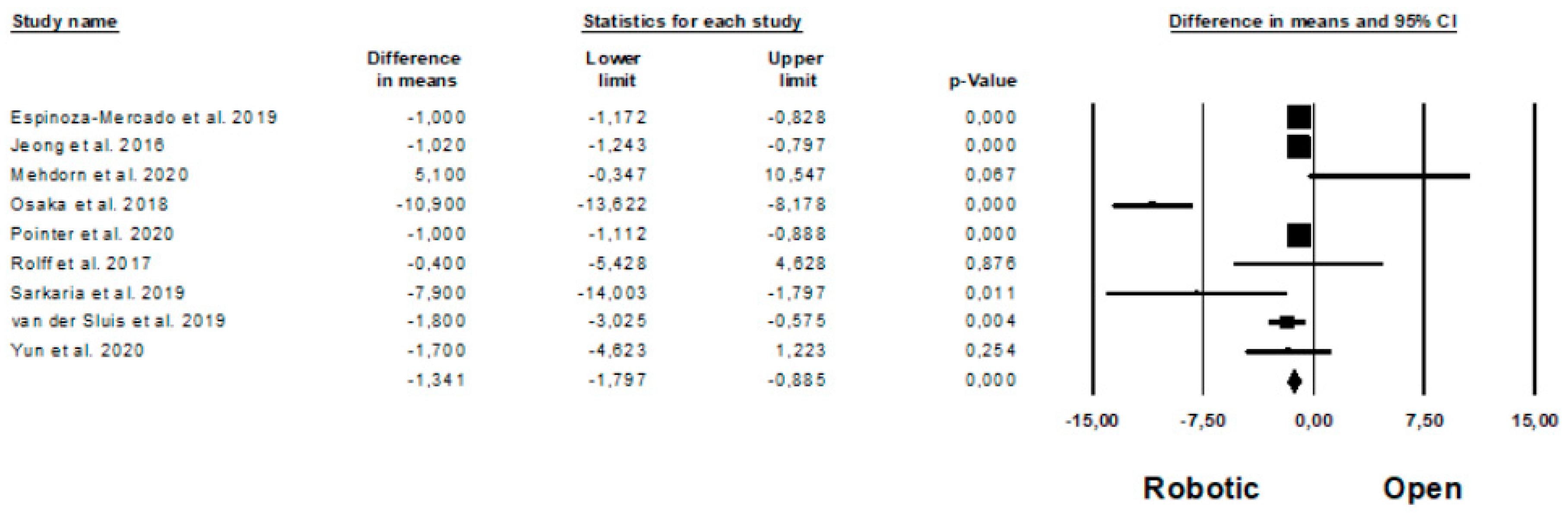
7. Robotic Versus Open Esophagectomy
7.1. Study Characteristics
7.2. Risk of Bias Assessment
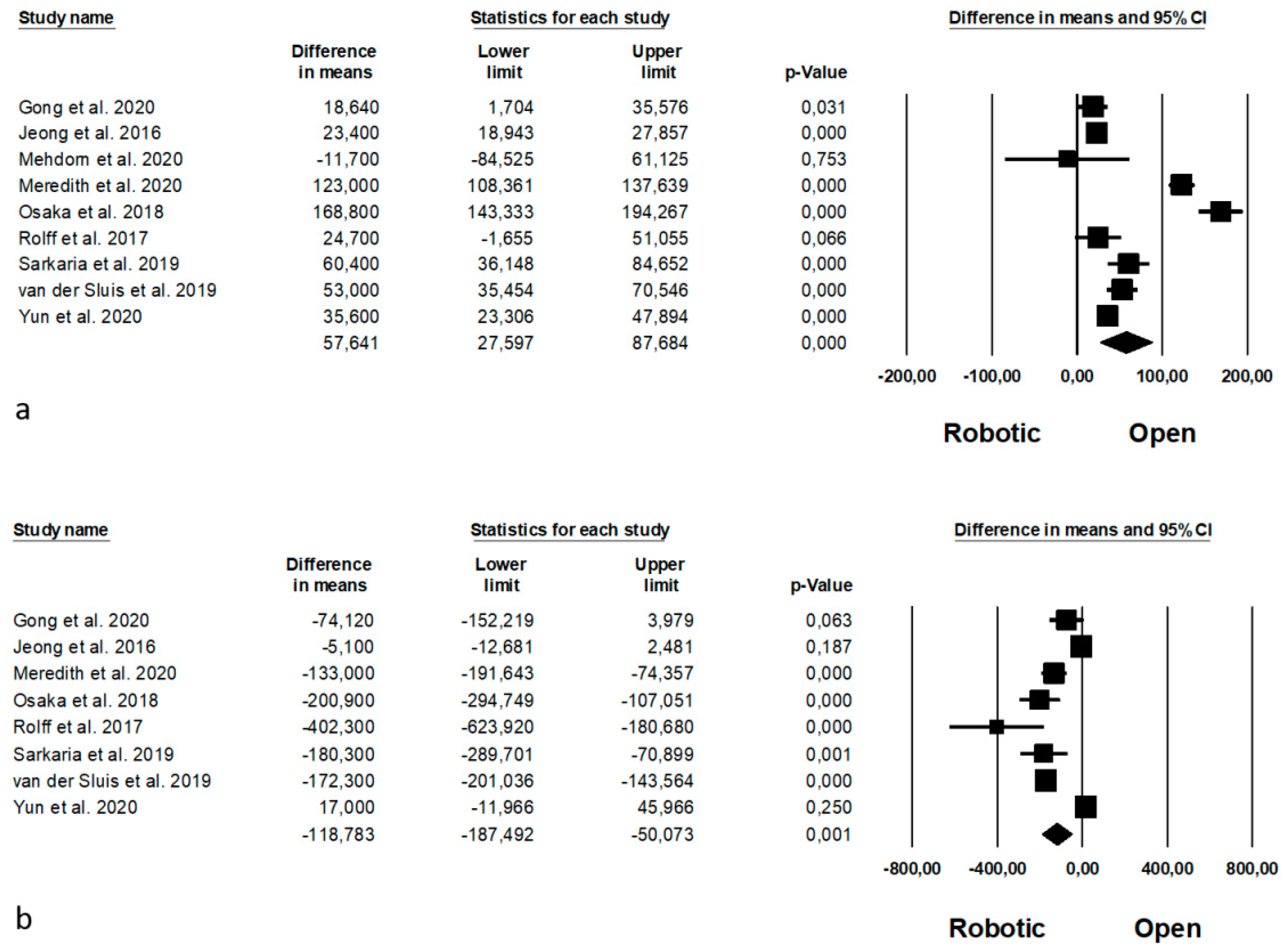
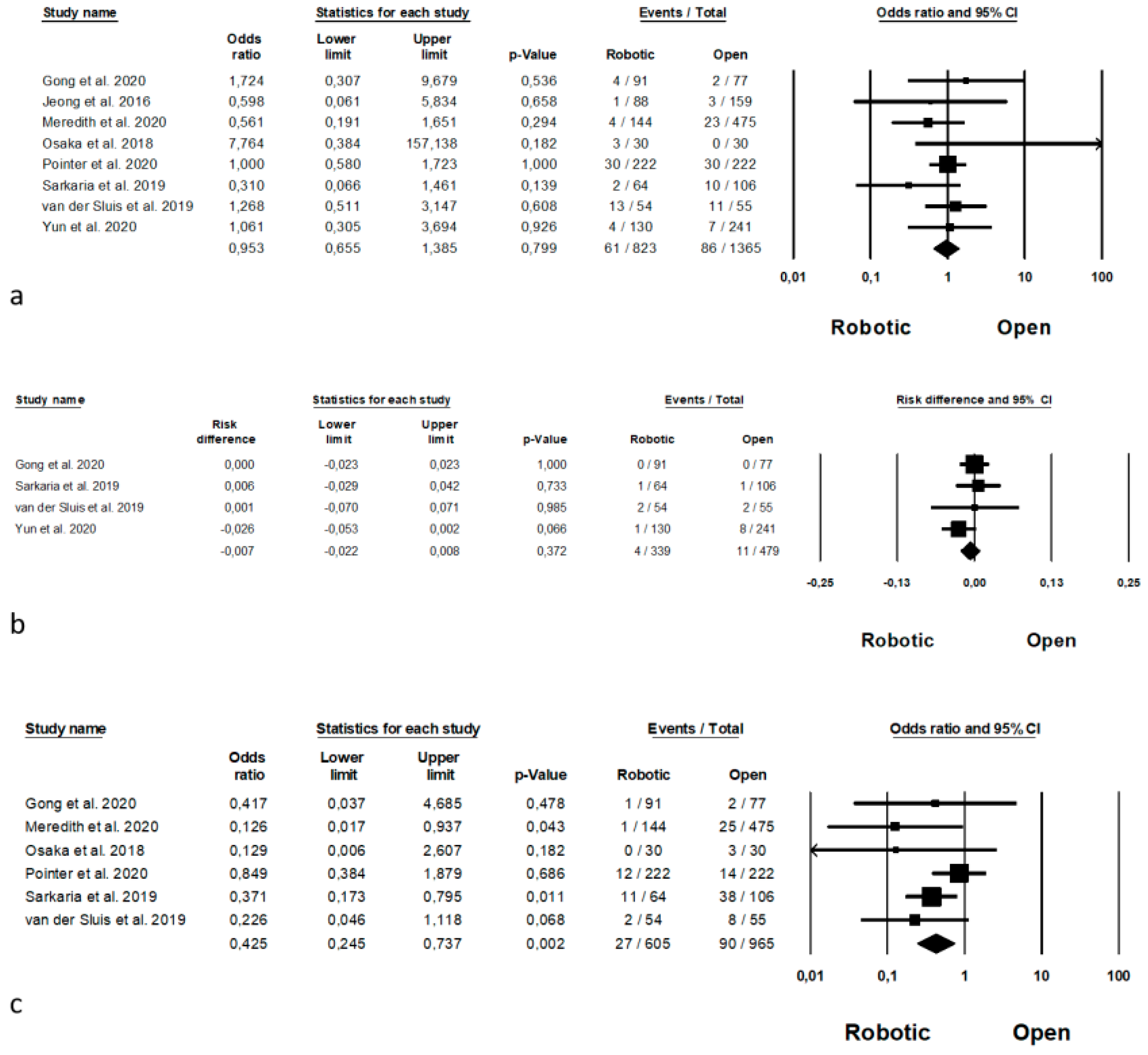
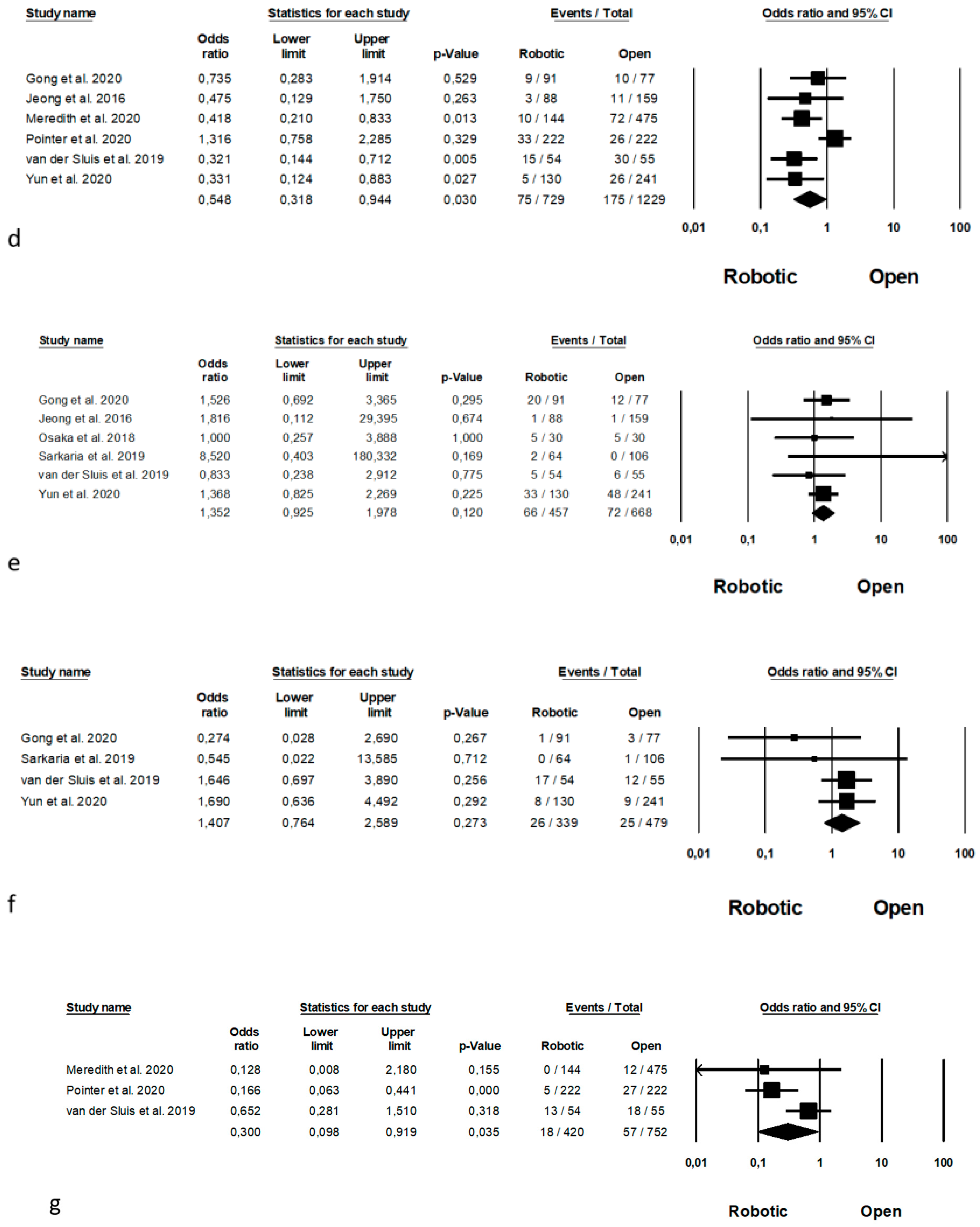
7.3. Short-Term Outcomes
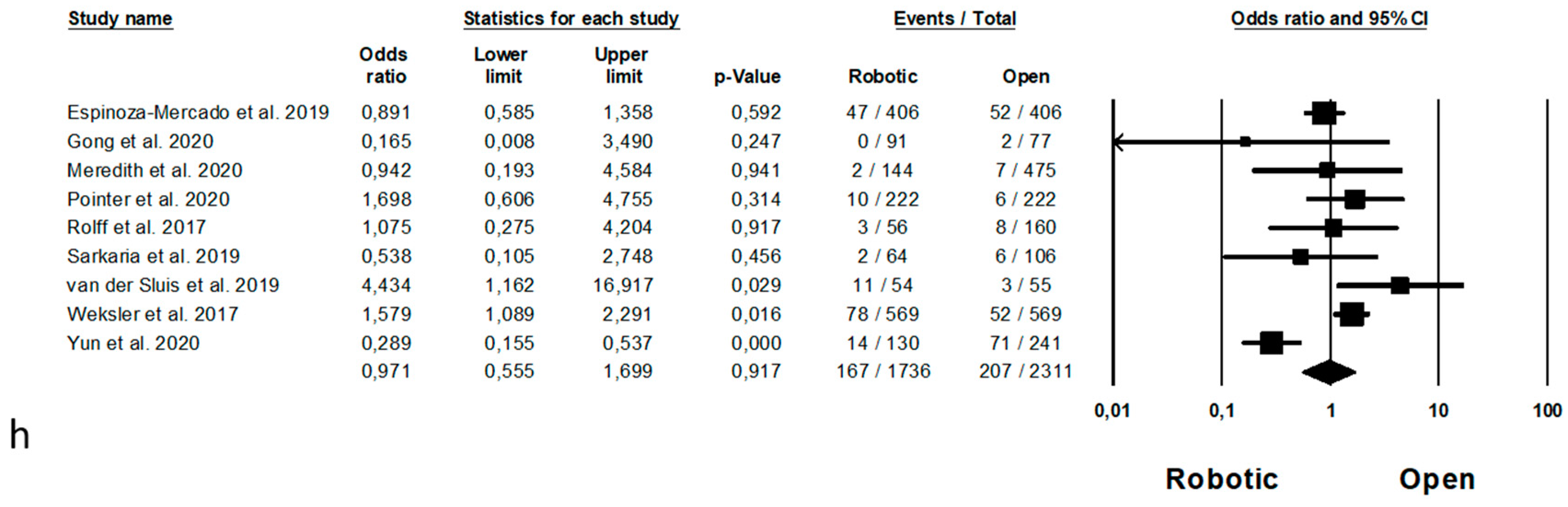
8. Long-Term Outcomes
9. Subgroup Analysis
9.1. Fully Robotic vs. Open Procedures
9.2. McKeown Esophagectomy
9.3. Ivor-Lewis Esophagectomy
9.4. Publication Bias
10. Discussion
11. Conclusions
- robotic surgery could be considered absolutely safe, being the results about postoperative complications comparable to open and laparoscopic surgery;
- robotic surgery could be considered superior to open approach, being guaranteed less postoperative complications and superior oncologic results;
- robotic approach appeared to be slightly superor to laparoscopic surgery, providing less postoperative pneumonia and higher number of harvested nodes;
- being by our results safety and effectiveness of robotic surgery to treat esophageal cancer, future perspective is the call to perform randomized clinical trial to confirm the advantages of robotic surgery. Definitive conclusions cannot be drawn, due to limitations of the current literature.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.F.; Yang, Y.H.; Lai, C.H.; Chen, P.C.; Chen, W.C. Outcome of patients with esophageal cancer: A nationwide analysis. Ann. Surg. Oncol. 2013. [Google Scholar] [CrossRef]
- Lewis, I. The surgical treatment of carcinoma of the oesophagus with special reference to a new operation for growths of the middle third. Br. J. Surg. 1946. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zuo, Z.; Chen, H.; Qiu, B.; Du, M.; Gao, Y. The comparison of thoracoscopic-laparoscopic esophagectomy and open esophagectomy: A meta-analysis. Indian J. Cancer 2017. [Google Scholar] [CrossRef]
- Guo, W.; Ma, X.; Yang, S.; Zhu, X.; Qin, W.; Xiang, J.; Lerut, T.; Li, H. Combined thoracoscopic-laparoscopic esophagectomy versus open esophagectomy: A meta-analysis of outcomes. Surg. Endosc. 2016. [Google Scholar] [CrossRef]
- Wang, K.; Zhong, J.; Liu, Q.; Lin, P.; Fu, J. A Propensity Score-matched Analysis of Thoraco-laparoscopic versus Open McKeown’s Esophagectomy. Ann. Thorac. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nuytens, F.; Dabakuyo-Yonli, T.S.; Meunier, B.; Gagnière, J.; Collet, D.; D’Journo, X.B.; Brigand, C.; Perniceni, T.; Carrère, N.; Mabrut, J.Y.; et al. Five-Year Survival Outcomes of Hybrid Minimally Invasive Esophagectomy in Esophageal Cancer: Results of the MIRO Randomized Clinical Trial. JAMA Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mariette, C.; Markar, S.; Dabakuyo-Yonli, T.S.; Meunier, B.; Pezet, D.; Collet, D.; D’Journo, X.B.; Brigand, C.; Perniceni, T.; Carrere, N.; et al. Health-related quality of life following hybrid minimally invasive versus open esophagectomy for patients with esophageal cancer, analysis of a multicenter, open-label, randomized phase III controlled trial: The MIRO trial. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Yoshida, N.; Yamamoto, H.; Baba, H.; Miyata, H.; Watanabe, M.; Toh, Y.; Matsubara, H.; Kakeji, Y.; Seto, Y. Can Minimally Invasive Esophagectomy Replace Open Esophagectomy for Esophageal Cancer? Latest Analysis of 24,233 Esophagectomies from the Japanese National Clinical Database. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Maas, K.W.; Cuesta, M.A.; Van Berge Henegouwen, M.I.; Roig, J.; Bonavina, L.; Rosman, C.; Gisbertz, S.S.; Biere, S.S.A.Y.; Van Der Peet, D.L. Quality of Life and Late Complications After Minimally Invasive Compared to Open Esophagectomy: Results of a Randomized Trial. World J. Surg. 2015. [Google Scholar] [CrossRef] [Green Version]
- van der Sluis, P.C.; van der Horst, S.; May, A.M.; Schippers, C.; Brosens, L.A.A.; Joore, H.C.A.; Kroese, C.C.; Haj Mohammad, N.; Mook, S.; Vleggaar, F.P.; et al. Robot-assisted Minimally Invasive Thoracolaparoscopic Esophagectomy Versus Open Transthoracic Esophagectomy for Resectable Esophageal Cancer: A Randomized Controlled Trial. Ann. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Egberts, J.H.; Stein, H.; Aselmann, H.; Jan-Hendrik, A.; Becker, T. Fully robotic da Vinci Ivor-Lewis esophagectomy in four-arm technique-problems and solutions. Dis. Esophagus 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milone, M.; Manigrasso, M.; Velotti, N.; Torino, S.; Vozza, A.; Sarnelli, G.; Aprea, G.; Maione, F.; Gennarelli, N.; Musella, M.; et al. Completeness of total mesorectum excision of laparoscopic versus robotic surgery: A review with a meta-analysis. Int. J. Colorectal Dis. 2019, 34, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Andolfi, E.; Biancafarina, A.; Rocca, A.; Amato, M.; Milone, M.; Scricciolo, M.; Frezza, B.; Miranda, E.; De Prizio, M.; et al. Robot-assisted surgery in elderly and very elderly population: Our experience in oncologic and general surgery with literature review. Aging Clin. Exp. Res. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, A.S.; Garofalo, J.; Koirala, P.; Vu, M.L.T.; Chuang, L. Robotic Surgery in Gynecology. Surg. Clin. N. Am. 2020, 82, 96–109. [Google Scholar] [CrossRef]
- Tang, A.B.; Lamaina, M.; Childers, C.P.; Mak, S.S.; Ruan, Q.; Begashaw, M.M.; Bergman, J.; Booth, M.S.; Shekelle, P.G.; Wilson, M.; et al. Perioperative and Long-Term Outcomes of Robot-Assisted Partial Nephrectomy: A Systematic Review. Am. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kernstine, K.H.; DeArmond, D.T.; Karimi, M.; Van Natta, T.L.; Campos, J.C.; Yoder, M.R.; Everett, J.E. The robotic, 2-stage, 3-field esophagolymphadenectomy. J. Thorac. Cardiovasc. Surg. 2004. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’connell, D.; Petersen, J.; Welch, V.; Losos, M.; Tugwell, P.; The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Department of Epidemiology and Community Medicine, University of Ottawa: ottawa, ON, Canada, 2012. Available online: www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 May 2021).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011. [Google Scholar] [CrossRef] [Green Version]
- Messori, A.; Maratea, D.; Fadda, V.; Trippoli, S. Using risk difference as opposed to odds-ratio in meta-analysis. Int. J. Cardiol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Luo, D.; Weng, H.; Zeng, X.T.; Lin, L.; Chu, H.; Tong, T. Optimally estimating the sample standard deviation from the five-number summary. Res. Synth. Methods 2020. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, T.A.; Barbui, C.; Cipriani, A.; Brambilla, P.; Watanabe, N. Imputing missing standard deviations in meta-analyses can provide accurate results. J. Clin. Epidemiol. 2006. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Sharp, S.J. Explaining heterogeneity in meta-analysis: A comparison of methods. Stat. Med. 1999, 18, 2693–2708. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.M.; Bachman, K.C.; Worrell, S.G.; Gray, K.E.; Perry, Y.; Linden, P.A.; Towe, C.W. Robotic minimally invasive esophagectomy provides superior surgical resection. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Grimminger, P.P.; Tagkalos, E.; Hadzijusufovic, E.; Corvinus, F.; Babic, B.; Lang, H. Change from Hybrid to Fully Minimally Invasive and Robotic Esophagectomy is Possible without Compromises. Thorac. Cardiovasc. Surg. 2019. [Google Scholar] [CrossRef]
- Harbison, G.J.; Vossler, J.D.; Yim, N.H.; Murayama, K.M. Outcomes of robotic versus non-robotic minimally-invasive esophagectomy for esophageal cancer: An American College of Surgeons NSQIP database analysis. Am. J. Surg. 2019. [Google Scholar] [CrossRef]
- He, H.; Wu, Q.; Wang, Z.; Zhang, Y.; Chen, N.; Fu, J.; Zhang, G. Short-term outcomes of robot-assisted minimally invasive esophagectomy for esophageal cancer: A propensity score matched analysis. J. Cardiothorac. Surg. 2018. [Google Scholar] [CrossRef]
- Jeong, D.M.; Kim, J.A.; Ahn, H.J.; Yang, M.; Heo, B.Y.; Lee, S.H. Decreased Incidence of Postoperative Delirium in Robot-assisted Thoracoscopic Esophagectomy Compared with Open Transthoracic Esophagectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Kamel, M.K.; Sholi, A.N.; Rahouma, M.; Harrison, S.W.; Lee, B.; Stiles, B.M.; Altorki, N.K.; Port, J.L. National trends and perioperative outcomes of robotic oesophagectomy following induction chemoradiation therapy: A National Cancer Database propensity-matched analysis. Eur. J. Cardio-Thoracic Surg. 2021. [Google Scholar] [CrossRef]
- Mehdorn, A.-S.; Möller, T.; Franke, F.; Richter, F.; Kersebaum, J.-N.; Becker, T.; Egberts, J.-H. Long-Term, Health-Related Quality of Life after Open and Robot-Assisted Ivor-Lewis Procedures—A Propensity Score-Matched Study. J. Clin. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meredith, K.L.; Maramara, T.; Blinn, P.; Lee, D.; Huston, J.; Shridhar, R. Comparative Perioperative Outcomes by Esophagectomy Surgical Technique. J. Gastrointest. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meredith, K.; Blinn, P.; Maramara, T.; Takahashi, C.; Huston, J.; Shridhar, R. Comparative outcomes of minimally invasive and robotic-assisted esophagectomy. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Motoyama, S.; Sato, Y.; Wakita, A.; Kawakita, Y.; Nagaki, Y.; Imai, K.; Minamiya, Y. Extensive lymph node dissection around the left laryngeal nerve achieved with robot-assisted thoracoscopic esophagectomy. Anticancer Res. 2019. [Google Scholar] [CrossRef]
- Osaka, Y.; Tachibana, S.; Ota, Y.; Suda, T.; Makuuti, Y.; Watanabe, T.; Iwasaki, K.; Katsumata, K.; Tsuchida, A. Usefulness of robot-assisted thoracoscopic esophagectomy. Gen. Thorac. Cardiovasc. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.K.; Hsieh, M.J.; Liu, Y.H.; Liu, H.P. Lymph Node Evaluation in Robot-Assisted Versus Video-Assisted Thoracoscopic Esophagectomy for Esophageal Squamous Cell Carcinoma: A Propensity-Matched Analysis. World J. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Hwang, Y.; Lee, H.J.; Park, I.K.; Kim, Y.T.; Kang, C.H. Comparison of robot-assisted esophagectomy and thoracoscopic esophagectomy in esophageal squamous cell carcinoma. J. Thorac. Dis. 2016. [Google Scholar] [CrossRef] [Green Version]
- Pointer, D.T.; Saeed, S.; Naffouje, S.A.; Mehta, R.; Hoffe, S.E.; Dineen, S.P.; Fleming, J.B.; Fontaine, J.P.; Pimiento, J.M. Outcomes of 350 Robotic-assisted Esophagectomies at a High-volume Cancer Center. Ann. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rolff, H.C.; Ambrus, R.B.; Belmouhand, M.; Achiam, M.P.; Wegmann, M.; Siemsen, M.; Kofoed, S.C.; Svendsen, L.B. Robot-Assisted Hybrid Esophagectomy Is Associated with a Shorter Length of Stay Compared to Conventional Transthoracic Esophagectomy: A Retrospective Study. Minim. Invasive Surg. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkaria, I.S.; Rizk, N.P.; Goldman, D.A.; Sima, C.; Tan, K.S.; Bains, M.S.; Adusumilli, P.S.; Molena, D.; Bott, M.; Atkinson, T.; et al. Early Quality of Life Outcomes After Robotic-Assisted Minimally Invasive and Open Esophagectomy. Ann. Thorac. Surg. 2019. [Google Scholar] [CrossRef]
- Shirakawa, Y.; Noma, K.; Kunitomo, T.; Hashimoto, M.; Maeda, N.; Tanabe, S.; Sakurama, K.; Fujiwara, T. Initial introduction of robot-assisted, minimally invasive esophagectomy using the microanatomy-based concept in the upper mediastinum. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Suda, K.; Ishida, Y.; Kawamura, Y.; Inaba, K.; Kanaya, S.; Teramukai, S.; Satoh, S.; Uyama, I. Robot-assisted thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve for esophageal squamous cell carcinoma in the prone position: Technical report and short-term outcomes. World J. Surg. 2012. [Google Scholar] [CrossRef] [PubMed]
- Tagkalos, E.; Goense, L.; Hoppe-Lotichius, M.; Ruurda, J.P.; Babic, B.; Hadzijusufovic, E.; Kneist, W.; Van Der Sluis, P.C.; Lang, H.; Van Hillegersberg, R.; et al. Robot-assisted minimally invasive esophagectomy (RAMIE) compared to conventional minimally invasive esophagectomy (MIE) for esophageal cancer: A propensity-matched analysis. Dis. Esophagus 2020. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, S.; Obama, K.; Hisamori, S.; Nishigori, T.; Okamura, R.; Maekawa, H.; Sakai, Y. Lower Incidence of Postoperative Pulmonary Complications Following Robot-Assisted Minimally Invasive Esophagectomy for Esophageal Cancer: Propensity Score-Matched Comparison to Conventional Minimally Invasive Esophagectomy. Ann. Surg. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Weksler, B.; Sharma, P.; Moudgill, N.; Chojnacki, K.A.; Rosato, E.L. Robot-assisted minimally invasive esophagectomy is equivalent to thoracoscopic minimally invasive esophagectomy. Dis. Esophagus 2012. [Google Scholar] [CrossRef]
- Weksler, B.; Sullivan, J.L. Survival after Esophagectomy: A Propensity-Matched Study of Different Surgical Approaches. Ann. Thorac. Surg. 2017. [Google Scholar] [CrossRef] [Green Version]
- Chao, Y.K.; Wen, Y.W.; Chuang, W.Y.; Cerfolio, R.J. Transition from video-assisted thoracoscopic to robotic esophagectomy: A single surgeon’s experience. Dis. Esophagus 2020. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, X.-K.; Cong, Z.-Z.; Zhou, H.; Wu, W.-J.; Qiang, Y.; Yi, J.; Shen, Y. Long-term outcomes of robotic-assisted versus thoraco-laparoscopic McKeown esophagectomy for esophageal cancer: A propensity score-matched study. Dis. Esophagus 2020. [Google Scholar] [CrossRef] [PubMed]
- Yerokun, B.A.; Sun, Z.; Jeffrey Yang, C.F.; Gulack, B.C.; Speicher, P.J.; Adam, M.A.; D’Amico, T.A.; Onaitis, M.W.; Harpole, D.H.; Berry, M.F.; et al. Minimally Invasive Versus Open Esophagectomy for Esophageal Cancer: A Population-Based Analysis. Ann. Thorac. Surg. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Han, Y.; Gan, Q.; Xiang, J.; Jin, R.; Chen, K.; Che, J.; Hang, J.; Li, H. Early Outcomes of Robot-Assisted Versus Thoracoscopic-Assisted Ivor Lewis Esophagectomy for Esophageal Cancer: A Propensity Score-Matched Study. Ann. Surg. Oncol. 2019. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, X.; Li, B.; Hua, R.; Yang, Y.; He, Y.; Ye, B.; Guo, X.; Sun, Y.; Li, Z. Short- And mid-term outcomes of robotic versus thoraco-laparoscopic McKeown esophagectomy for squamous cell esophageal cancer: A propensity score-matched study. Dis. Esophagus 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Liu, Q.; Zhang, X.; Yang, H.; Tan, Z.; Lin, Y.; Fu, J. Comparisons of short-term outcomes between robot-assisted and thoraco-laparoscopic esophagectomy with extended two-field lymph node dissection for resectable thoracic esophageal squamous cell carcinoma. J. Thorac. Dis. 2019. [Google Scholar] [CrossRef]
- Deng, H.Y.; Luo, J.; Li, S.X.; Li, G.; Alai, G.; Wang, Y.; Liu, L.X.; Lin, Y.D. Does robot-assisted minimally invasive esophagectomy really have the advantage of lymphadenectomy over video-assisted minimally invasive esophagectomy in treating esophageal squamous cell carcinoma? A propensity score-matched analysis based on short-term. Dis. Esophagus 2019. [Google Scholar] [CrossRef]
- Duan, X.; Yue, J.; Chen, C.; Gong, L.; Ma, Z.; Shang, X.; Yu, Z.; Jiang, H. Lymph node dissection around left recurrent laryngeal nerve: Robot-assisted vs. video-assisted McKeown esophagectomy for esophageal squamous cell carcinoma. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Gong, L.; Jiang, H.; Yue, J.; Duan, X.; Tang, P.; Ren, P.; Zhao, X.; Liu, X.; Zhang, X.; Yu, Z. Comparison of the short-term outcomes of robot-assisted minimally invasive, video-assisted minimally invasive, and open esophagectomy. J. Thorac. Dis. 2020. [Google Scholar] [CrossRef]
- Espinoza-Mercado, F.; Imai, T.A.; Borgella, J.D.; Sarkissian, A.; Serna-Gallegos, D.; Alban, R.F.; Soukiasian, H.J. Does the Approach Matter? Comparing Survival in Robotic, Minimally Invasive, and Open Esophagectomies. Ann. Thorac. Surg. 2019. [Google Scholar] [CrossRef]
- Yun, J.K.; Chong, B.K.; Kim, H.J.; Lee, I.S.; Gong, C.S.; Kim, B.S.; Lee, G.D.; Choi, S.; Kim, H.R.; Kim, D.K.; et al. Comparative outcomes of robot-assisted minimally invasive versus open esophagectomy in patients with esophageal squamous cell carcinoma: A propensity score-weighted analysis. Dis. Esophagus 2021. [Google Scholar] [CrossRef] [PubMed]
- de Groot, E.M.; van der Horst, S.; Feike Kingma, B.; Goense, L.; van der Sluis, P.C.; Ruurda, J.P.; van Hillegersberg, R. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open esophagectomy: Long-term follow-up of a randomized clinical trial. Dis. Esophagus 2020. [Google Scholar] [CrossRef]
- Gisbertz, S.S.; Hagens, E.R.C.; Ruurda, J.P.; Schneider, P.M.; Tan, L.J.; Domrachev, S.A.; Hoeppner, J.; van Berge Henegouwen, M.I. The evolution of surgical approach for esophageal cancer. Ann. N. Y. Acad. Sci. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lv, L.; Hu, W.; Ren, Y.; Wei, X. Minimally invasive esophagectomy versus open esophagectomy for esophageal cancer: A meta-analysis. OncoTargets Ther. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariette, C.; Piessen, G.; Triboulet, J.P. Therapeutic strategies in oesophageal carcinoma: Role of surgery and other modalities. Lancet Oncol. 2007, 8, 545–553. [Google Scholar] [CrossRef]
- Biere, S.S.A.Y.; Van Berge Henegouwen, M.I.; Maas, K.W.; Bonavina, L.; Rosman, C.; Garcia, J.R.; Gisbertz, S.S.; Klinkenbijl, J.H.G.; Hollmann, M.W.; De Lange, E.S.M.; et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: A multicentre, open-label, randomised controlled trial. Lancet 2012. [Google Scholar] [CrossRef]
- Jin, D.; Yao, L.; Yu, J.; Liu, R.; Guo, T.; Yang, K.; Gou, Y. Robotic-assisted minimally invasive esophagectomy versus the conventional minimally invasive one: A meta-analysis and systematic review. Int. J. Med. Robot. Comput. Assist. Surg. 2019, 15, e1988. [Google Scholar] [CrossRef]
- Siaw-Acheampong, K.; Kamarajah, S.K.; Gujjuri, R.; Bundred, J.R.; Singh, P.; Griffiths, E.A. Minimally invasive techniques for transthoracic oesophagectomy for oesophageal cancer: Systematic review and network meta-analysis. BJS Open 2020, 4, 787–803. [Google Scholar] [CrossRef]
- Zheng, C.; Li, X.K.; Zhang, C.; Zhou, H.; Ji, S.G.; Zhong, J.H.; Xu, Y.; Cong, Z.Z.; Wang, G.M.; Wu, W.J.; et al. Comparison of short-term clinical outcomes between robot-assisted minimally invasive esophagectomy and video-assisted minimally invasive esophagectomy: A systematic review and meta-analysis. J. Thorac. Dis. 2021. [Google Scholar] [CrossRef]
- Li, X.K.; Xu, Y.; Zhou, H.; Cong, Z.Z.; Wu, W.J.; Qiang, Y.; Shen, Y. Does robot-assisted minimally invasive oesophagectomy have superiority over thoraco-laparoscopic minimally invasive oesophagectomy in lymph node dissection? Dis. esophagus Off. J. Int. Soc. Dis. Esophagus 2021. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | N. of Enrolled Patients | Mean Age | Mean BMI | ASA Score (%) | Tumor Stage (%) | Tumor Localization (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RAMIE | MIE | I | II | III | IV | 0 | I | II | III | IV | ||||||||
| Ali et al., 2020 | retro | 1543 | 5118 | 63.71 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Chao et al., 2018 | retro | 34 | 34 | 55.12 | NR | NR | NR | NR | NR | 0.00 | 47.10 | 0.00 | 52.90 | 0.00 | 29.40 | 50.00 | 20.60 | 0.00 |
| Chao et al., 2020 | retro | 39 | 67 | 55.60 | 22.34 | NR | NR | NR | NR | 0.00 | 0.00 | 7.55 | 92.45 | 0.00 | 22.65 | 48.08 | 29.27 | 0.00 |
| Chen et al., 2019 | retro | 54 | 54 | 61.80 | 22.85 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Deng et al., 2018 | prosp | 52 | 52 | 60.95 | NR | NR | NR | NR | NR | 0.00 | 12.50 | 45.15 | 37.50 | 0.00 | 16.35 | 60.60 | 22.10 | 0.95 |
| Duan et al., 2020 | retro | 109 | 75 | 60.45 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Gong et al., 2020 | retro | 91 | 144 | NR | NR | NR | NR | NR | NR | 0.00 | 18.59 | 33.33 | 20.83 | 2.57 | 3.53 | 33.01 | 38.78 | 0.00 |
| Grimminger et al., 2019 | prosp | 25 | 25 | 62.05 | 25.55 | NR | NR | NR | NR | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 14.00 | 89.00 | 0.00 |
| Harbison et al., 2019 | retro | 100 | 625 | 64.00 | 27.63 | 17.38 | 0.00 | 77.66 | 4.97 | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| He et al., 2018 | retro | 27 | 27 | 61.30 | 21.70 | NR | NR | NR | NR | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 7.40 | 61.10 | 31.45 | 0.00 |
| Meredith et al., 2020 | prosp | 144 | 95 | 50.97 | 21.84 | 0.35 | 35.94 | 42.15 | 0.67 | 0.00 | 15.70 | 25.11 | 35.37 | 2.22 | NR | NR | NR | NR |
| Motoyama et al., 2019 | retro | 21 | 38 | 64.10 | NR | NR | NR | NR | NR | 0.00 | 38.80 | 15.14 | 45.71 | 0.00 | 25.78 | 38.80 | 35.42 | 0.00 |
| Park et al., 2016 | retro | 62 | 43 | 65.08 | 23.42 | 30.50 | 65.72 | 3.84 | 0.00 | 0.00 | 58.08 | 25.79 | 15.24 | 0.94 | 14.29 | 22.85 | 62.86 | 0.00 |
| Shirakawa et al., 2020 | retro | 51 | 51 | 68.00 | 21.95 | 21.60 | 64.70 | 13.70 | NR | NR | NR | NR | NR | NR | 18.60 | 46.10 | 25.50 | 3.90 |
| Suda et al., 2012 | prosp | 16 | 20 | 65.39 | 20.78 | NR | NR | NR | NR | 2.78 | 33.33 | 11.11 | 50.00 | 2.78 | 11.11 | 52.78 | 36.11 | 0.00 |
| Tagkalos et al., 2020 | prosp | 40 | 40 | 62.50 | 26.00 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Tsunoda et al., 2021 | retro | 45 | 45 | NR | NR | 9.00 | 89.00 | 2.00 | 0.00 | 0.00 | 51.00 | 19.00 | 23.00 | 7.00 | 14.50 | 28.00 | 57.50 | 0.00 |
| Weksler et al., 2012 | retro | 11 | 26 | 62.64 | 27.66 | NR | NR | NR | NR | 27.02 | 32.39 | 16.23 | 24.35 | 0.00 | NR | NR | NR | NR |
| Weksler et al., 2017 | retro | 569 | 569 | 41.90 | NR | NR | NR | NR | NR | 4.70 | 22.73 | 19.33 | 17.53 | 2.40 | NR | NR | NR | NR |
| Xu et al., 2020 | retro | 292 | 292 | 64.63 | 23.09 | 17.50 | 76.05 | 6.50 | 0.00 | 0.00 | 38.90 | 20.90 | 39.05 | 1.15 | 7.50 | 73.30 | 19.20 | 0.00 |
| Yang et al., 2020 | retro | 271 | 271 | 63.45 | 23.20 | 1.50 | 89.50 | 9.05 | 0.00 | 0.00 | 28.20 | 33.75 | 26.95 | 11.05 | 12.70 | 62.75 | 24.55 | 0.00 |
| Yerokun et al., 2016 | retro | 170 | 170 | 62.95 | NR | NR | NR | NR | NR | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 2.95 | 51.15 | 45.90 | 0.00 |
| Zhang et al., 2019 | retro | 66 | 66 | 62.15 | 23.00 | 42.45 | 52.25 | 5.30 | 0.00 | 6.10 | 27.25 | 43.20 | 23.45 | 0.00 | 0.00 | 21.95 | 28.05 | 0.00 |
| Study | Study Design | N. of Enrolled Patients | Mean Age | Mean BMI | ASA Score (%) | Tumor Stage (%) | Tumor Localization (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RAMIE | OPEN | I | II | III | IV | 0 | I | II | III | IV | ||||||||
| Espinoza-Mercado et al., 2019 | retro | 406 | 406 | 64 | NR | NR | NR | NR | NR | 14.65 | 25.75 | 37.8 | 21.3 | 0 | NR | NR | NR | NR |
| Gong et al., 2020 | retro | 91 | 77 | NR | NR | NR | NR | NR | NR | 2.974 | 33.33 | 39.88 | 21.42 | 2.38 | 26.18 | 37.50 | 31.54 | 0.91 |
| Jeong et al., 2016 | retro | 88 | 159 | NR | 22.66 | NR | NR | NR | NR | 41.19838 | 42.53 | 13.12 | 2.78 | 0.35 | NR | NR | NR | NR |
| Mehdorn et al., 2020 | prosp | 11 | 11 | 63.8 | 27.4 | 0 | 31.85 | 68.15 | 0 | 13.65 | 9.1 | 36.4 | 27.3 | 4.55 | NR | NR | NR | NR |
| Meredith et al., 2020 | prosp | 144 | 475 | 64.46 | 28 | 0.38 | 49.62 | 49.20 | 0.70 | 9.66 | 34.78 | 41.24 | 12.27 | 44.43 | NR | NR | NR | NR |
| Osaka et al., 2018 | retro | 30 | 30 | 62.5 | NR | NR | NR | NR | NR | 26.65 | 45 | 18.3 | 10 | 0 | 26.65 | 48.35 | 26.35 | 0 |
| Pointer et al., 2020 | retro | 222 | 222 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Rolff et al., 2017 | retro | 56 | 160 | 64.65 | 26.51 | 27.03 | 50 | 23.22 | 0.51 | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Sarkaria et al., 2019 | prosp | 64 | 106 | 61.89 | 29.12 | 0 | 14.16 | 79.38 | 6.48 | 22.48 | 32.52 | 24.83 | 8.24 | 0 | 0 | 1.18 | 63.54 | 41.54 |
| Weksler et al., 2017 | retro | 569 | 569 | 63 | NR | NR | NR | NR | NR | 20.4 | 32.15 | 27.7 | 14.35 | 35.55 | NR | NR | NR | NR |
| Yun et al., 2020 | prosp | 130 | 241 | 62.92 | 23.21 | NR | NR | NR | NR | 20.74 | 19.16 | 20.51 | 3.78 | 0 | 43.62 | 31.80 | 5.92 | 4.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manigrasso, M.; Vertaldi, S.; Marello, A.; Antoniou, S.A.; Francis, N.K.; De Palma, G.D.; Milone, M. Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes. J. Pers. Med. 2021, 11, 640. https://doi.org/10.3390/jpm11070640
Manigrasso M, Vertaldi S, Marello A, Antoniou SA, Francis NK, De Palma GD, Milone M. Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes. Journal of Personalized Medicine. 2021; 11(7):640. https://doi.org/10.3390/jpm11070640
Chicago/Turabian StyleManigrasso, Michele, Sara Vertaldi, Alessandra Marello, Stavros Athanasios Antoniou, Nader Kamal Francis, Giovanni Domenico De Palma, and Marco Milone. 2021. "Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes" Journal of Personalized Medicine 11, no. 7: 640. https://doi.org/10.3390/jpm11070640
APA StyleManigrasso, M., Vertaldi, S., Marello, A., Antoniou, S. A., Francis, N. K., De Palma, G. D., & Milone, M. (2021). Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes. Journal of Personalized Medicine, 11(7), 640. https://doi.org/10.3390/jpm11070640