
Aortic Arch Calcification and Cardiomegaly Are Associated with Overall and Cardiovascular Mortality in Hemodialysis Patients

 , ,
, ,
Abstract
:1. Introduction
2. Study Patients and Methods
2.1. Study Patients and Design
2.2. Evaluation of AoAC and CTR by Chest X-ray
2.3. Collection of Demographic, Medical and Laboratory Data
2.4. Definitions of Overall and Cardiovascular Mortality
2.5. Reproducibility
2.6. Statistical Analysis
3. Results
3.1. Comparisons of the Clinical Characteristics among the Study Groups
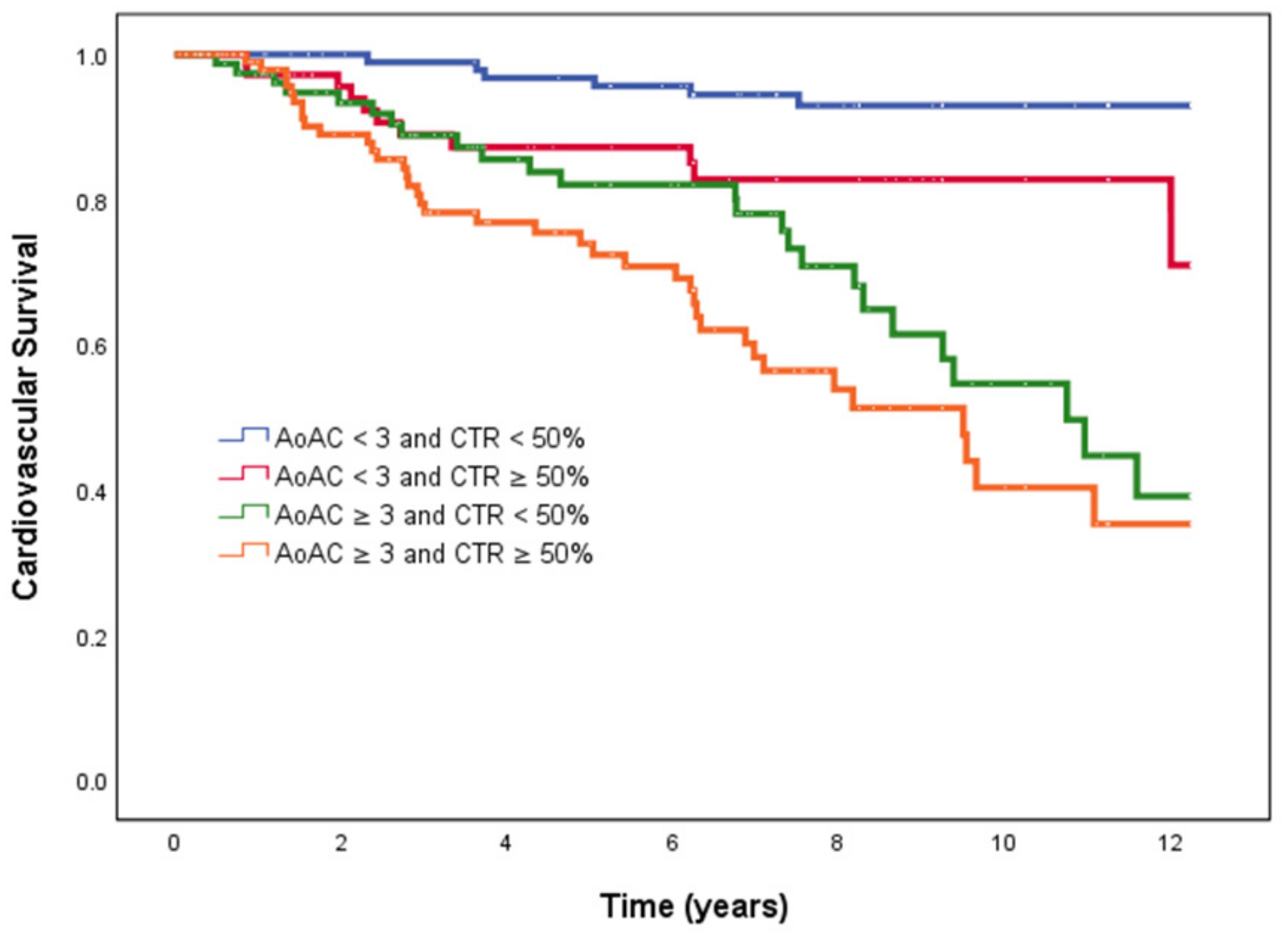
3.2. Risk of Overall Mortality
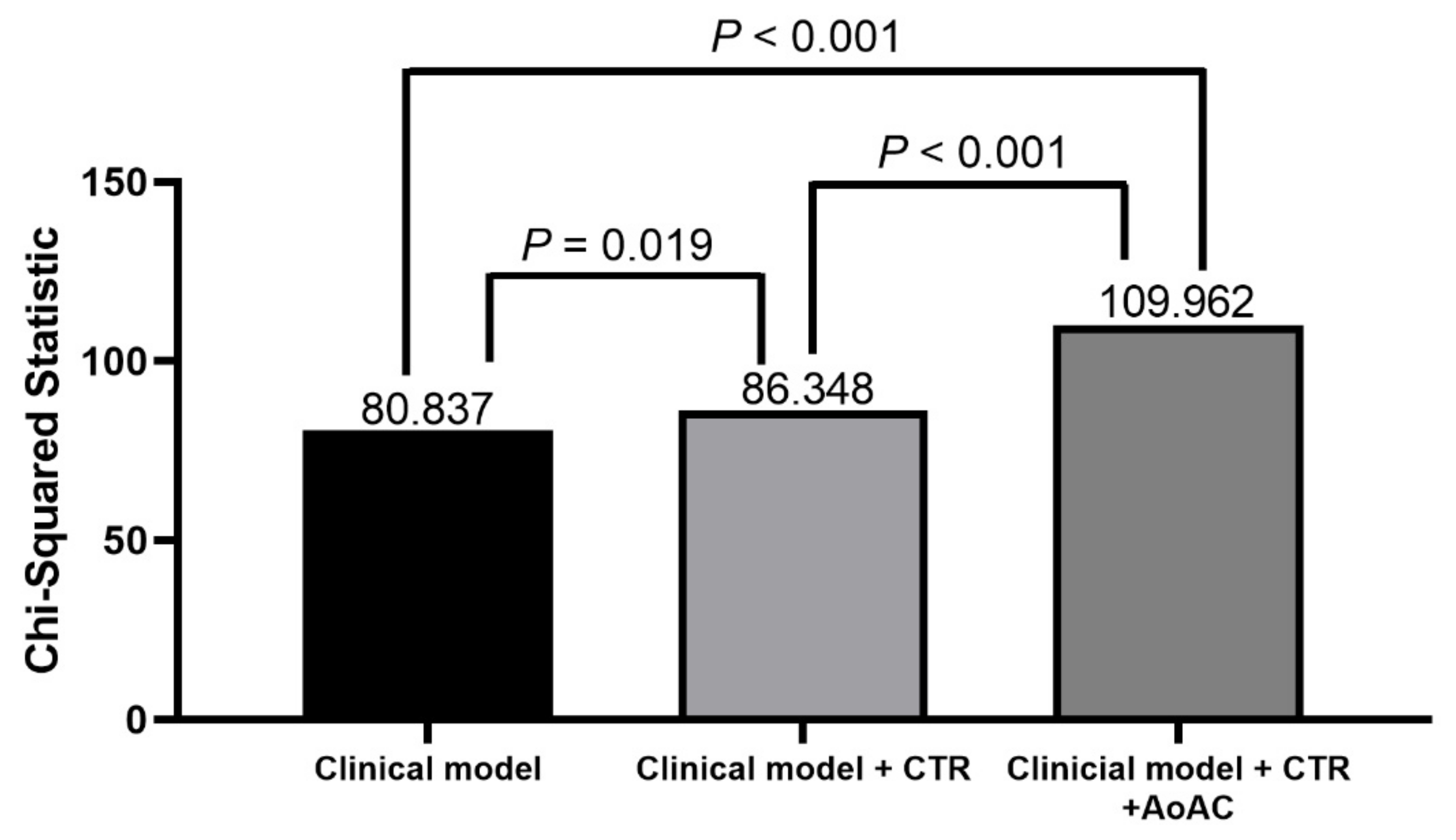
3.3. Incremental Values of CTR and AoAC in Relation to Overall Mortality
3.4. Risk of Cardiovascular Mortality
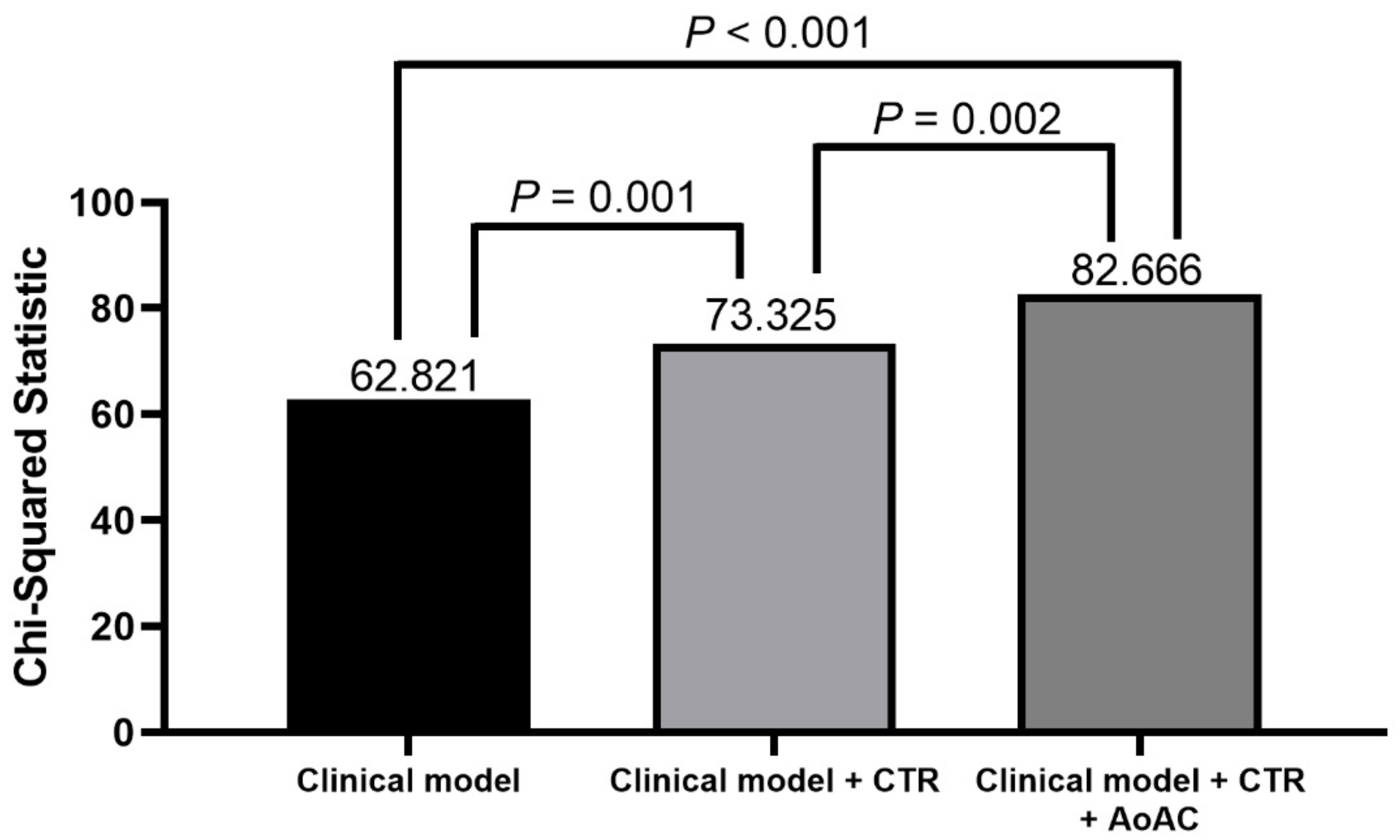
3.5. Incremental Values of CTR and AoAC in Relation to Cardiovascular Mortality
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collins, A.J. Cardiovascular mortality in end-stage renal disease. Am. J. Med. Sci. 2003, 325, 163–167. [Google Scholar] [CrossRef]
- Foley, R.N.; Murray, A.M.; Li, S.; Herzog, C.A.; McBean, A.M.; Eggers, P.W.; Collins, A.J. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J. Am. Soc. Nephrol. 2005, 16, 489–495. [Google Scholar] [CrossRef]
- Kim, H.; Kim, K.H.; Ahn, S.V.; Kang, S.-W.; Yoo, T.-H.; Ahn, H.S.; Hann, H.J.; Lee, S.; Ryu, J.-H.; Yu, M. Risk of major cardiovascular events among incident dialysis patients: A Korean national population-based study. Int. J. Cardiol. 2015, 198, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.A.; Duval, S.; Hoke, L.; Florea, N.; Grandits, G.; Carlson, C.; Lee, J.; Cohn, J.N. Early cardiovascular structural and functional abnormalities as a guide to future morbid events. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cozzolino, M.; Galassi, A.; Pivari, F.; Ciceri, P.; Conte, F. The cardiovascular burden in end-stage renal disease. Expand. Hemodial. 2017, 191, 44–57. [Google Scholar]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Yao, Q.; Pecoits-Filho, R.; Lindholm, B.; Stenvinkel, P. Traditional and non-traditional risk factors as contributors to atherosclerotic cardiovascular disease in end-stage renal disease. Scand. J. Urol. Nephrol. 2004, 38, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Ishida, H.; Matsuda, N.; Fujiu, A.; Matsuda, A.; Ito, K.; Ando, Y.; Nitta, K. Simple evaluation of aortic arch calcification by chest radiography in hemodialysis patients. Hemodial. Int. 2009, 13, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Okazaki, M.; Tsuchiya, K.; Kawaguchi, H.; Nitta, K. Aortic arch calcification predicts cardiovascular and all-cause mortality in maintenance hemodialysis patients. Kidney Blood Press. Res. 2014, 39, 658–667. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, H.; Iijima, K.; Hashimoto, M.; Son, B.-K.; Ota, H.; Ogawa, S.; Eto, M.; Akishita, M.; Ouchi, Y. Validity and usefulness of aortic arch calcification in chest X-ray. J. Atheroscler. Thromb. 2009, 16, 256–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iribarren, C.; Sidney, S.; Sternfeld, B.; Browner, W.S. Calcification of the aortic arch: Risk factors and association with coronary heart disease, stroke, and peripheral vascular disease. JAMA 2000, 283, 2810–2815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iijima, K.; Hashimoto, H.; Hashimoto, M.; Son, B.-K.; Ota, H.; Ogawa, S.; Eto, M.; Akishita, M.; Ouchi, Y. Aortic arch calcification detectable on chest X-ray is a strong independent predictor of cardiovascular events beyond traditional risk factors. Atherosclerosis 2010, 210, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Ogawa, T.; Ishida, H.; Ando, Y.; Nitta, K. Aortic arch calcification evaluated on chest X-ray is a strong independent predictor of cardiovascular events in chronic hemodialysis patients. Heart Vessel. 2012, 27, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.-C.P.; Lee, M.-Y.; Huang, J.-C.; Tsai, Y.-C.; Chen, J.-H.; Chen, S.-C.; Chang, J.-M.; Chen, H.-C. Association of brachial-ankle pulse wave velocity and cardiomegaly with aortic arch calcification in patients on hemodialysis. Medicine 2016, 95, e3643. [Google Scholar]
- Salusky, I.B.; Goodman, W.G. Cardiovascular calcification in end-stage renal disease. Nephrol. Dial. Transplant. 2002, 17, 336–339. [Google Scholar] [CrossRef] [Green Version]
- Giamouzis, G.; Sui, X.; Love, T.E.; Butler, J.; Young, J.B.; Ahmed, A. A propensity-matched study of the association of cardiothoracic ratio with morbidity and mortality in chronic heart failure. Am. J. Cardiol. 2008, 101, 343–347. [Google Scholar] [CrossRef] [Green Version]
- Loomba, R.S.; Shah, P.H.; Nijhawan, K.; Aggarwal, S.; Arora, R. Cardiothoracic ratio for prediction of left ventricular dilation: A systematic review and pooled analysis. Future Cardiol. 2015, 11, 171–175. [Google Scholar] [CrossRef]
- Chen, K.-H.; Lin-Tan, D.-T.; Huang, W.-H.; Hung, C.-C.; Chang, C.-T.; Huang, J.-Y.; Lin, J.-L. Cardiothoracic ratio, malnutrition, inflammation, and two-year mortality in non-diabetic patients on maintenance hemodialysis. Kidney Blood Press. Res. 2008, 31, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Yotsueda, R.; Taniguchi, M.; Tanaka, S.; Eriguchi, M.; Fujisaki, K.; Torisu, K.; Masutani, K.; Hirakata, H.; Kitazono, T.; Tsuruya, K. Cardiothoracic ratio and all-cause mortality and cardiovascular disease events in hemodialysis patients: The Q-Cohort study. Am. J. Kidney Dis. 2017, 70, 84–92. [Google Scholar] [CrossRef]
- Li, L.C.; Lee, Y.T.; Lee, Y.W.; Chou, C.A.; Lee, C.T. Aortic arch calcification predicts the renal function progression in patients with stage 3 to 5 chronic kidney disease. Biomed. Res. Int. 2015, 2015, 131263. [Google Scholar] [CrossRef]
- Chen, S.-C.; Teh, M.; Huang, J.-C.; Wu, P.-Y.; Chen, C.-Y.; Tsai, Y.-C.; Chiu, Y.-W.; Chang, J.-M.; Chen, H.-C. Increased aortic arch calcification and cardiomegaly is associated with rapid renal progression and increased cardiovascular mortality in chronic kidney disease. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Daugirdas, J.T.; Depner, T.A.; Gotch, F.A.; Greene, T.; Keshaviah, P.; Levin, N.W.; Schulman, G. Comparison of methods to predict equilibrated Kt/V in the HEMO Pilot Study. Kidney Int. 1997, 52, 1395–1405. [Google Scholar] [PubMed] [Green Version]
- Sanchis, P.; Ho, C.Y.; Liu, Y.; Beltran, L.E.; Ahmad, S.; Jacob, A.P.; Furmanik, M.; Laycock, J.; Long, D.A.; Shroff, R. Arterial “inflammaging” drives vascular calcification in children on dialysis. Kidney Int. 2019, 95, 958–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, M.A.; Kalra, P.A.; Hunter, J.; Menoyo, J.; Stankus, N. The prevalence of vascular calcification in patients with end-stage renal disease on hemodialysis: A cross-sectional observational study. Ther. Adv. Chronic Dis. 2015, 6, 84–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellasi, A.; Raggi, P. Vascular Calcification in Patients with Kidney Disease: Techniques and Technologies to Assess Vascular Calcification. Semin. Dial. 2007, 20, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Raggi, P.; O'Neill, W.C. Imaging for Vascular Calcification. Semin. Dial. 2017, 30, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Niu, Q.; Zhao, H.; Wu, B.; Tsai, S.; Wu, J.; Zhang, M.; Lu, L.; Qiao, J.; Men, C.; Zuo, L. Study on the prevalence of vascular calcification in different types of arteries and influencing factors in maintenance peritoneal Dialysis patients. Blood Purif. 2019, 47, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.-S.; Shih, M.-C.P.; Wu, P.-Y.; Huang, J.-C.; Chen, S.-C.; Chiu, Y.-W.; Chang, J.-M.; Chen, H.-C. Progression of Aortic Arch Calcification Is Associated with Overall and Cardiovascular Mortality in Hemodialysis. Dis. Markers 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-T.; Huang, C.-C.; Hsu, C.-Y.; Chiou, T.T.-Y.; Ng, H.-Y.; Wu, C.-H.; Kuo, W.-H.; Lee, Y.-T. Calcification of the aortic arch predicts cardiovascular and all-cause mortality in chronic hemodialysis patients. Cardiorenal Med. 2014, 4, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitta, K.; Ogawa, T. Aortic arch calcification and clinical outcome in patients with end-stage renal disease. Tohoku J. Exp. Med. 2011, 223, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Kakani, E.; Elyamny, M.; Ayach, T.; El-Husseini, A. Pathogenesis and Management of Vascular Calcification in CKD and Dialysis Patients. Semin. Dial. 2019, 32, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Paloian, N.J.; Giachelli, C.M. A current understanding of vascular calcification in CKD. Am. J. Physiol. Ren. Physiol. 2014, 307, F891–F900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitta, K.; Hanafusa, N.; Okazaki, M.; Komatsu, M.; Kawaguchi, H.; Tsuchiya, K. Association between risk factors including bone-derived biomarkers and aortic arch calcification in maintenance hemodialysis patients. Kidney Blood Press. Res. 2018, 43, 1554–1562. [Google Scholar] [CrossRef] [PubMed]
- Byon, C.H.; Chen, Y. Molecular mechanisms of vascular calcification in chronic kidney disease: The link between bone and the vasculature. Curr. Osteoporos. Rep. 2015, 13, 206–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, S.; Giachelli, C.M. Vascular calcification in CKD-MBD: Roles for phosphate, FGF23, and Klotho. Bone 2017, 100, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Brandenburg, V.M.; Schuh, A.; Kramann, R. Valvular calcification in chronic kidney disease. Adv. Chronic Kidney Dis. 2019, 26, 464–471. [Google Scholar] [CrossRef]
- Monfared, A.B.; Farajollah, S.A.; Sabour, F.; Farzanegan, R.; Taghdisi, S. Comparison of radiological findings of chest x-ray with echocardiography in determination of the heart size. Iran. Red. Crescent Med. J. 2015, 17, e18242. [Google Scholar]
- Rayner, B.L.; Goodman, H.; Opie, L.H. The chest radiograph: A useful investigation in the evaluation of hypertensive patients. Am. J. Hypertens. 2004, 17, 507–510. [Google Scholar] [CrossRef] [Green Version]
- Aoki, J.; Ikari, Y.; Nakajima, H.; Mori, M.; Sugimoto, T.; Hatori, M.; Tanimoto, S.; Amiya, E.; Hara, K. Clinical and pathologic characteristics of dilated cardiomyopathy in hemodialysis patients. Kidney Int. 2005, 67, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizawa, S.; Uto, K.; Nishikawa, T.; Hagiwara, N.; Oda, H. Histological features of endomyocardial biopsies in patients undergoing hemodialysis: Comparison with dilated cardiomyopathy and hypertensive heart disease. Cardiovasc. Pathol. 2020, 49, 107256. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.-M.; Wang, M.; Woo, J.; Lam, C.W.-K.; Lui, S.-F.; Li, P.K.-T.; Sanderson, J.E. Inflammation, residual kidney function, and cardiac hypertrophy are interrelated and combine adversely to enhance mortality and cardiovascular death risk of peritoneal dialysis patients. J. Am. Soc. Nephrol. 2004, 15, 2186–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, H.S.; Cho, J.S.; Hong, Y.A.; Chang, Y.K.; Kim, S.Y.; Shin, S.J.; Yoon, H.E. Vascular calcification and left ventricular hypertrophy in hemodialysis patients: Interrelationship and clinical impacts. Int. J. Med. Sci. 2018, 15, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitta, K.; Akiba, T.; Uchida, K.; Otsubo, S.; Otsubo, Y.; Takei, T.; Ogawa, T.; Yumura, W.; Kabaya, T.; Nihei, H. Left ventricular hypertrophy is associated with arterial stiffness and vascular calcification in hemodialysis patients. Hypertens. Res. 2004, 27, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Lullo, L.; Gorini, A.; Russo, D.; Santoboni, A.; Ronco, C. Left ventricular hypertrophy in chronic kidney disease patients: From pathophysiology to treatment. Cardiorenal Med. 2015, 5, 254–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, C.; Hu, J.-X.; Dong, Y.-F.; Zhan, R.; Li, P.; Su, H.; Peng, Q.; Wu, T.; Huang, X.; Sun, W.-H. Association of endothelial and mild renal dysfunction with the severity of left ventricular hypertrophy in hypertensive patients. Am. J. Hypertens. 2016, 29, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Trinh, E.; Chan, C.T. Intensive home hemodialysis results in regression of left ventricular hypertrophy and better clinical outcomes. Am. J. Nephrol. 2016, 44, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.-C.; Hsu, C.-Y.; Chen, C.-L. The strategy to prevent and regress the vascular calcification in dialysis patients. Biomed. Res. Int. 2017, 2017, 9035193. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Suzuki, M.; Hanafusa, N.; Tsuchiya, K.; Nitta, K. Denosumab recovers aortic arch calcification during long-term hemodialysis. Kidney Int. Rep. 2020, 6, 605–612. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | AoAC < 3 and CTR < 50% (n = 107) | AoAC < 3 and CTR ≥ 50% (n = 75) | AoAC ≥ 3 and CTR < 50% (n = 81) | AoAC ≥ 3 and CTR ≥ 50% (n = 102) | p |
|---|---|---|---|---|---|
| AoAC | 0.32 ± 0.71 | 0.55 ± 0.86 | 6.69 ± 2.95 *,† | 7.03 ± 2.94 *,† | <0.001 |
| CTR (%) | 44.7 ± 3.2 | 55.1 ± 6.3 * | 46.0 ± 2.5 † | 55.5 ± 4.4 *,# | <0.001 |
| Age (year) | 50.1 ± 11.5 | 5.68 ± 11.2 * | 63.2 ± 9.6 *,† | 64.5 ± 10.4 *,† | <0.001 |
| Male gender (%) | 65.4 | 34.7 * | 64.2 † | 39.2 *,# | <0.001 |
| Smoking (ever) (%) | 35.8 | 22.7 | 37.5 | 26.7 | 0.109 |
| Diabetes mellitus (%) | 41.1 | 46.7 | 54.3 | 55.9 | 0.130 |
| Hypertension (%) | 78.5 | 70.7 | 77.8 | 82.3 | 0.325 |
| Coronary artery disease (%) | 6.5 | 16.0 | 19.8 | 41.2 *,†,# | <0.001 |
| Cerebrovascular disease (%) | 0 | 10.7 | 14.8 * | 11.8 * | 0.001 |
| Laboratory parameters | |||||
| Fasting glucose (mg/dL) | 110.5 ± 44.6 | 137.7 ± 107.1 | 132.4 ± 8.02 | 137.2 ± 69.1 | 0.033 |
| Triglyceride (mg/dL) | 125 (85–187) | 131 (89.5–181.5) | 132 (84.5–201.5) | 155.5 (89.75–197) | 0.673 |
| Total cholesterol (mg/dL) | 177.6 ± 44.0 | 186.6 ± 46.2 | 179.5 ± 62.7 | 178.4 ± 42.6 | 0.635 |
| Hemoglobin (g/dL) | 10.2 ± 1.1 | 9.8 ± 1.3 | 10.3 ± 1.1 † | 10.1 ± 1.3 | 0.025 |
| Total calcium (mg/dL) | 9.3 ± 0.8 | 9.3 ± 0.8 | 9.5 ± 1.0 | 9.5 ± 0.9 | 0.209 |
| Phosphorous (mg/dL) | 4.8 ± 1.2 | 5.0 ± 1.5 | 4.8 ± 1.3 | 4.8 ± 1.3 | 0.644 |
| Calcium-phosphorous product (mg2/dL2) | 44.6 ± 12.3 | 46.6 ± 14.0 | 45.6 ± 13.8 | 45.5 ± 12.0 | 0.806 |
| Kt/V (Daugirdas) | 1.49 ± 0.26 | 1.60 ± 0.29 | 1.53 ± 0.25 | 1.56 ± 0.30 | 0.084 |
| Medications | |||||
| ACEI and/or ARB use (%) | 19.4 | 18.8 | 16.2 | 23.9 | 0.652 |
| Statins use (%) | 31.6 | 23.4 | 24.3 | 39.1 | 0.105 |
| Antiplatelet agent use (%) | 4.1 | 14.1 | 21.6 * | 32.6 *,† | <0.001 |
| Outcome | |||||
| Follow-up period (years) | 8.2 (6.2–12.2) | 6.2 (2.3–9.2) * | 6.8 (2.6–8.3) * | 4.6 (2.4–7.6) * | <0.001 |
| Overall mortality (%) | 13.1 | 21.3 | 65.4 *,† | 66.7 *,† | <0.001 |
| Cardiovascular mortality (%) | 5.6 | 14.7 | 30.9 * | 37.3 *,† | <0.001 |
| Parameter | Univariable | Multivariable (Model 1) | Multivariable (Model 2) | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Study group | ||||||
| AoAC < 3 and CTR < 50% | Reference | Reference | — | — | ||
| AoAC < 3 and CTR ≥ 50% | 2.249 (1.096–4.615) | 0.027 | 1.739 (0.765–3.950) | 0.187 | — | — |
| AoAC ≥ 3 and CTR < 50% | 7.482 (4.138–13.529) | <0.001 | 4.576 (2.314–9.051) | <0.001 | — | — |
| AoAC ≥ 3 and CTR ≥ 50% | 9.338 (5.214–16.725) | <0.001 | 5.912 (2.968–11.776) | <0.001 | — | — |
| AoAC (per 1 score) | 1.165 (1.125–1.206) | <0.001 | — | — | 1.106 (1.054–1.160) | <0.001 |
| CTR (per 1%) | 1.049 (1.027–1.071) | <0.001 | — | — | 1.042 (1.010–1.076) | 0.011 |
| Age (per 1 year) | 1.062 (1.047–1.078) | <0.001 | 1.031 (1.012–1.051) | 0.002 | 1.033 (1.013–1.054) | 0.001 |
| Gender (male vs. female) | 1.157 (0.840–1.592) | 0.372 | 1.021 (0.626–1.666) | 0.933 | 1.148 (0.702–1.876) | 0.583 |
| Smoking (ever vs. never) | 1.528 (1.089–2.143) | 0.014 | 1.622 (0.957–2.750) | 0.072 | 1.713 (1.016–2.888) | 0.043 |
| Diabetes mellitus | 2.370 (1.702–3.302) | <0.001 | 1.566 (1.059–2.315) | 0.025 | 1.660 (1.124–2.451) | 0.011 |
| Hypertension | 1.095 (0.749–1.599) | 0.640 | — | — | — | — |
| Coronary artery disease | 1.893 (1.326–2.702) | <0.001 | 1.364 (0.895–2.077) | 0.148 | 1.484 (0.976–2.257) | 0.065 |
| Cerebrovascular disease | 2.380 (1.462–3.874) | <0.001 | 1.352 (0.763–2.399) | 0.302 | 1.352 (0.767–2.383) | 0.297 |
| Laboratory parameters | ||||||
| Fasting glucose (per 1 mg/dL) | 1.003 (1.002–1.005) | <0.001 | 1.002 (0.999–1.004) | 0.170 | 1.002 (1.000–1.004) | 0.077 |
| Triglyceride (log per 1 mg/dL) | 1.088 (0.610–1.939) | 0.775 | — | — | — | — |
| Total cholesterol (per 1 mg/dL) | 0.997 (0.993–1.001) | 0.997 | — | — | — | — |
| Hemoglobin (per 1 g/dL) | 1.040 (0.911–1.188) | 0.562 | — | — | — | — |
| Total calcium (per 1 mg/dL) | 0.916 (0.757–1.107) | 0.363 | — | — | — | — |
| Phosphorous (per 1 mg/dL) | 0.977 (0.862–1.108) | 0.715 | — | — | — | — |
| Calcium—phosphorous product (per 1 mg2/dL2) | 0.996 (0.983–1.009) | 0.511 | — | — | — | — |
| Kt/V (Daugirdas) (per 1) | 0.892 (0.489–1.6260 | 0.709 | — | — | — | — |
| Medications | — | — | — | — | ||
| ACEI and/or ARB use | 1.238 (0.820–1.870) | 0.309 | — | — | — | — |
| Statins use | 0.930 (0.640–1.351) | 0.702 | — | — | — | — |
| Antiplatelet agent use | 2.407 (1.627–3.560) | <0.001 | 0.924 (0.586–1.457) | 0.734 | 0.956 (0.604–1.512) | 0.846 |
| Parameter | Univariable | Multivariable (Model 1) | Multivariable (Model 2) | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Study group | ||||||
| AoAC < 3 and CTR < 50% | Reference | Reference | — | — | ||
| AoAC < 3 and CTR ≥ 50% | 3.640 (1.343–9.865) | 0.011 | 3.806 (1.264–11.460) | 0.017 | — | — |
| AoAC ≥ 3 and CTR < 50% | 8.081 (3.302–19.777) | <0.001 | 4.993 (1.783–13.981) | 0.002 | — | — |
| AoAC ≥ 3 and CTR ≥ 50% | 11.970 (5.011–28.592) | <0.001 | 8.614 (3.112–23.845) | <0.001 | — | — |
| AoAC (per 1 score) | 1.160 (1.106–1.217) | <0.001 | — | — | 1.108 (1.035–1.187) | 0.003 |
| CTR (per 1%) | 1.057 (1.029–1.085) | <0.001 | — | — | 1.077 (1.039–1.116) | <0.001 |
| Age (per 1 year) | 1.061 (1.039–1.082) | <0.001 | 1.024 (0.997–1.051) | 0.086 | 1.023 (0.995–1.052) | 0.111 |
| Gender (male vs. female) | 1.191 (0.767–1.848) | 0.436 | 0.728 (0.347–1.526) | 0.401 | 0.861 (0.416–1.781) | 0.686 |
| Smoking (ever vs. never) | 1.856 (1.178–2.923) | 0.008 | 2.760 (1.289–5.908) | 0.009 | 2.915 (1.380–6.157) | 0.005 |
| Diabetes mellitus | 3.196 (1.989–5.135) | <0.001 | 2.013 (1.170–3.464) | 0.011 | 2.041 (1.193–3.493) | 0.009 |
| Hypertension | 1.123 (0.664–1.900) | 0.666 | — | — | — | — |
| Coronary artery disease | 2.344 (1.198–4.586) | 0.013 | 1.954 (1.116–3.423) | 0.019 | 2.202 (1.262–3.842) | 0.005 |
| Cerebrovascular disease | 2.394 (1.502–3.818) | <0.001 | 1.033 (0.473–2.256) | 0.935 | 1.084 (0.497–2.363) | 0.839 |
| Laboratory parameters | ||||||
| Fasting glucose (per 1 mg/dL) | 1.004 (1.001–1.006) | 0.001 | 1.002 (0.999–1.005) | 0.270 | 1.003 (1.000–1.006) | 0.075 |
| Triglyceride (log per 1 mg/dL) | 0.934 (0.420–2.076) | 0.866 | — | — | — | — |
| Total cholesterol (per 1 mg/dL) | 0.994 (0.989–1.000) | 0.038 | 0.995 (0.989–1.001) | 0.124 | 0.993 (0.986–1.000) | 0.044 |
| Hemoglobin (per 1 g/dL) | 1.138 (0.950–1.363) | 0.161 | — | — | — | — |
| Total calcium (per 1 mg/dL) | 0.925 (0.712–1.200) | 0.925 | — | — | — | — |
| Phosphorous (per 1 mg/dL) | 0.943 (0.791–1.125) | 0.517 | — | — | — | — |
| Calcium-phosphorous product (per 1 mg2/dL2) | 0.991 (0.973–1.009) | 0.341 | — | — | — | — |
| Kt/V (Daugirdas) (per 1) | 0.482 (0.204–1.135) | 0.095 | — | — | — | — |
| Medications | — | — | — | — | ||
| ACEI and/or ARB use | 1.127 (0.639–1.988) | 0.679 | — | — | — | — |
| Statins use | 0.884 (0.533–1.466) | 0.633 | — | — | — | — |
| Antiplatelet agent use | 3.046 (1.848–5.020) | < 0.001 | 0.994 (0.555–1.781) | 0.984 | 0.954 (0.529–1.722) | 0.877 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ou, S.-H.; Liu, Y.-H.; Chung, T.-L.; Huang, J.-C.; Wu, P.-Y.; Su, H.-M.; Chen, S.-C. Aortic Arch Calcification and Cardiomegaly Are Associated with Overall and Cardiovascular Mortality in Hemodialysis Patients. J. Pers. Med. 2021, 11, 657. https://doi.org/10.3390/jpm11070657
Ou S-H, Liu Y-H, Chung T-L, Huang J-C, Wu P-Y, Su H-M, Chen S-C. Aortic Arch Calcification and Cardiomegaly Are Associated with Overall and Cardiovascular Mortality in Hemodialysis Patients. Journal of Personalized Medicine. 2021; 11(7):657. https://doi.org/10.3390/jpm11070657
Chicago/Turabian StyleOu, Shih-Hsiang, Yi-Hsueh Liu, Tung-Ling Chung, Jiun-Chi Huang, Pei-Yu Wu, Ho-Ming Su, and Szu-Chia Chen. 2021. "Aortic Arch Calcification and Cardiomegaly Are Associated with Overall and Cardiovascular Mortality in Hemodialysis Patients" Journal of Personalized Medicine 11, no. 7: 657. https://doi.org/10.3390/jpm11070657
APA StyleOu, S. -H., Liu, Y. -H., Chung, T. -L., Huang, J. -C., Wu, P. -Y., Su, H. -M., & Chen, S. -C. (2021). Aortic Arch Calcification and Cardiomegaly Are Associated with Overall and Cardiovascular Mortality in Hemodialysis Patients. Journal of Personalized Medicine, 11(7), 657. https://doi.org/10.3390/jpm11070657