
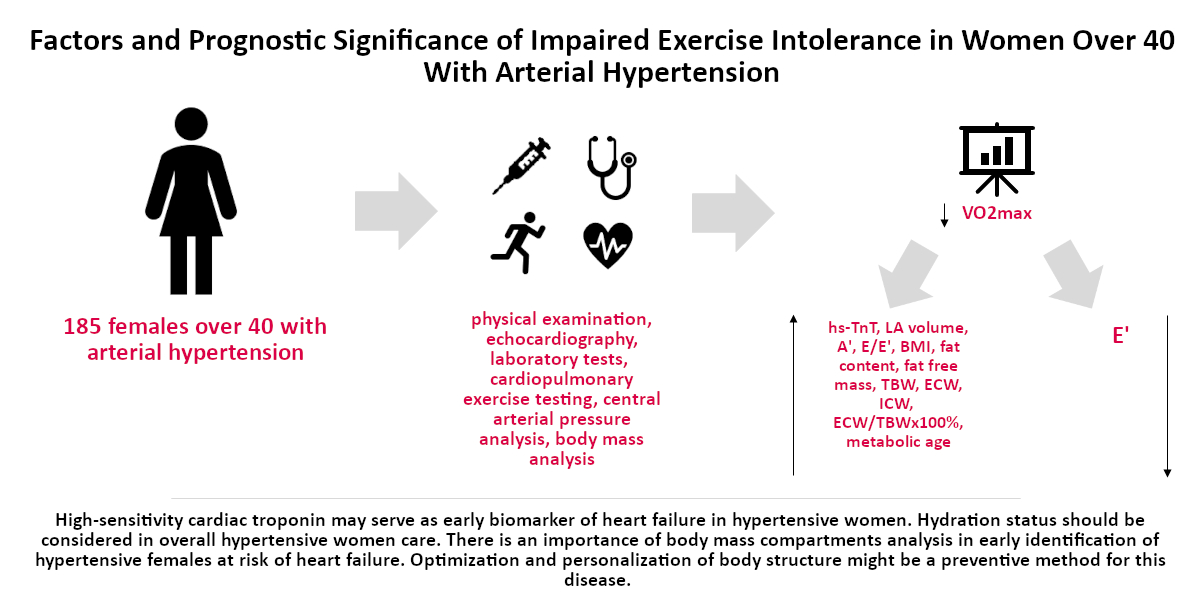
Factors and Prognostic Significance of Impaired Exercise Tolerance in Women over 40 with Arterial Hypertension

 ,
,  ,
, 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Basic Characteristics
- (a)
- uncontrolled hypertension;
- (b)
- diagnosis of heart failure or typical symptomatic heart failure;
- (b)
- left ventricular ejection fraction (LVEF) < 50%;
- (c)
- documented: hyperandrogenism, hyperestrogenism, insulin resistance, premature ovarian failure, polycystic ovary syndrome;
- (d)
- past myocardial infarction;
- (e)
- diagnosis of cardiomyopathy (hypertrophic, dilated, restrictive, peripartum, arrhythmogenic);
- (f)
- lysosomal storage disorders;
- (g)
- stroke, transient ischemic attack, intracerebral hemorrhage in medical history;
- (h)
- severe hyper- and hypothyroidism;
- (i)
- pregnancy and lactation;
- (j)
- chronic kidney disease (stage IV and V according to the National Kidney Foundation) and dialysis treatment;
- (k)
- documented neoplastic process;
- (l)
- the patient’s inability to cooperate and/or provide informed consent to participate in the research;
- (m)
- alcohol and drug abuse;
- (n)
- active autoimmune disease;
- (o)
- treatment using immunosuppressants, cytostatic drugs, glucocorticosteroids, or antiretroviral drugs;
- (p)
- a history of bone marrow transplant or other organ transplant, treatment with blood products within the last 6 months;
- (q)
- active systemic infection;
- (r)
- Hepatitis B virus (HBV), hepatitis C virus (HCV) or human immunodeficiency virus (HIV) carrier or positive for hepatitis B surface antigen (HBsAg) or antibodies to HCV;
- (s)
- surgery or serious injury within the last month;
- (t)
- patients who did not express their informed consent to participate in the study.
2.2. Echocardiography
2.3. Laboratory Tests
2.4. Spiroergometry
2.5. SphygmoCor
2.6. Body Mass Analysis
2.7. Statistical Analysis
3. Results
3.1. Evaluation of Basic Characteristics
3.2. Evaluation of Echocardiographic and Hemodynamic Parameters
3.3. Evaluation of Cardiocirculatory, Pulmonary and Metabolic Response to Exercise in CPET
3.4. Evaluation of Body Mass Analysis
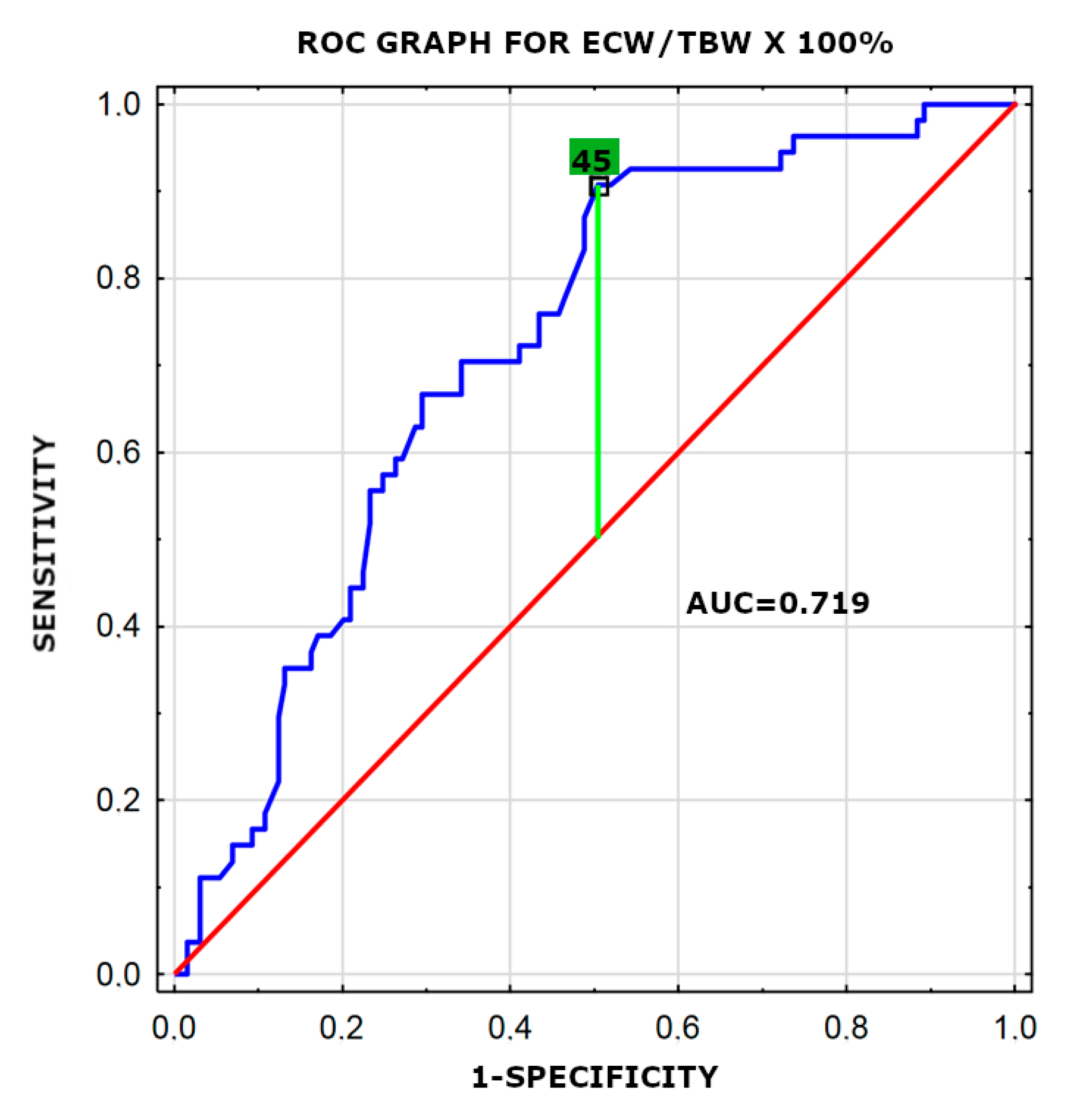
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Bielecka-Dabrowa, A.; Aronow, W.S.; Rysz, J.; Banach, M. The rise and fall of hypertension: Lessons learned from Eastern Europe. Curr. Cardiovasc. Risk Rep. 2011, 5, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Okoth, K.; Chandan, J.S.; Marshall, T.; Thangaratinam, S.; Thomas, G.N.; Nirantharakumar, K.; Adderley, N.J. Association between the reproductive health of young women and cardiovascular disease in later life: Umbrella review. BMJ 2020, 7, m3502. [Google Scholar] [CrossRef]
- Savarese, G.; D’Amario, D. Sex differences in heart failure. Adv. Exp. Med. Biol. 2018, 1065, 529–544. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.R.; Lambrinoudaki, I.; Lumsden, M.; Mishra, G.D.; Pal, L.; Rees, M.; Santoro, N.; Simoncini, T. Menopause. Nat. Rev. Dis. Primers 2015, 1, 15004. [Google Scholar] [CrossRef]
- Messerli, F.H.; Rimoldi, S.F.; Bangalore, S. The transition from hypertension to heart failure: Contemporary update. JACC Heart Fail. 2017, 5, 543–551. [Google Scholar] [CrossRef]
- Herdy, A.H.; Ritt, L.E.; Stein, R.; Araújo, C.G.; Milani, M.; Meneghelo, R.S.; Ferraz, A.S.; Hossri, C.; Almeida, A.E.; Fernandes-Silva, M.M.; et al. Cardiopulmonary exercise test: Background, applicability and interpretation. Arq. Bras. Cardiol. 2016, 107, 467–481. [Google Scholar] [CrossRef]
- Saric, M.; Armour, A.C.; Arnaout, M.S.; Thomas, G.N.; Nirantharakumar, K. Guidelines for the use of echocardiography in the evaluation of a cardiac source of embolism. J. Am. Soc. Echocardiogr. 2016, 29, 1–42. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Riegler, L.; Rucco, M.A.; Cocchia, R.; Scarafile, R.; Salerno, G.; Martone, F.; Vriz, O.; Caso, P.; Calabrò, R.; et al. Left atrial volume index in healthy subjects: Clinical and echocardiographic correlates. Echocardiography 2013, 30, 1001–1007. [Google Scholar] [CrossRef]
- Daskalov, I.R.; Petrovsky, P.D.; Demirevska, L.D. Mitral annular systolic velocity as a marker of preclinical systolic dysfunction among patients with arterial hypertension. Cardiovasc. Ultrasound. 2012, 28, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Datta, D.; Normandin, E.; ZuWallack, R. Cardiopulmonary exercise testing in the assessment of exertional dyspnea. Ann. Thorac. Med. 2015, 10, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Bjørke, A.C.H.; Raastad, T.; Berntsen, S. Criteria for the determination of maximal oxygen uptake in patients newly diagnosed with cancer: Baseline data from the randomized controlled trial of physical training and cancer (Phys-Can). PLoS ONE 2020, 11, e0234507. [Google Scholar] [CrossRef]
- Martin, J.S.; Borges, A.R.; Christy, J.B. Considerations for SphygmoCor radial artery pulse wave analysis: Side selection and peripheral arterial blood pressure calibration. Hypertens. Res. 2015, 38, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Milan, A.; Zocaro, G.; Leone, D.; Tosello, F.; Buraioli, I.; Schiavone, D.; Veglio, F. Current assessment of pulse wave velocity: Comprehensive review of validation studies. J. Hypertens. 2019, 37, 1547–1557. [Google Scholar] [CrossRef]
- Jaafar, Z.A.; Kreidieh, D.; Itani, L.; Tannir, H.; El Masri, D.; El Ghoch, M. Cross-validation of prediction equations for estimating the body fat percentage in adults with obesity. Clin. Nutr. ESPEN 2021, 41, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Rucco, M.A.; Cocchia, R. Extracellular water to total body water ratio in viral liver diseases: A study using bioimpedance analysis. Nutrients 2018, 10, 1072. [Google Scholar] [CrossRef] [Green Version]
- Israel, A.; Kivity, S.; Sidi, Y.; Segev, S.; Berkovitch, A.; Klempfner, R.; Lavi, B.; Goldenberg, I.; Maor, E. Use of exercise capacity to improve SCORE risk prediction model in asymptomatic adults. Eur. Heart J. 2016, 1, 2300–2306. [Google Scholar] [CrossRef] [Green Version]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation 2016, 134, 653–699. [Google Scholar] [CrossRef]
- Hulens, M.; Vansant, G.; Lysens, R.; Claessens, A.L.; Muls, E. Exercise capacity in lean versus obese women. Scand. J. Med. Sci. Sports 2001, 11, 305–309. [Google Scholar] [CrossRef]
- Babb, T.G.; Korzick, D.; Meador, M.; Hodgson, J.L.; Buskirk, E.R. Ventilatory response of moderately obese women to submaximal exercise. Int. J. Obes. 1991, 15, 59–65. [Google Scholar] [PubMed]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef]
- Shah, K.S.; Maisel, A.S.; Fonarow, G.C. Troponin in heart failure. Heart Fail. Clin. 2018, 14, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Ebong, I.A.; Wilson, M.D.; Bertoni, A.G.; Appiah, D.; Polonsky, T.; Michos, E.D.; Ballantyne, C.; Chang, P. High-sensitivity cardiac troponin T and the risk of heart failure in postmenopausal women of the ARIC Study. Menopause 2021, 4. [Google Scholar] [CrossRef]
- Waki, M.; Kral, J.G.; Mazariegos, M.; Wang, J.; Pierson, R.N., Jr.; Heymsfield, S.B. Relative expansion of extracellular fluid in obese vs. nonobese women. Am. J. Physiol. 1991, 261, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Zuo, M.L.; Yue, W.S.; Yip, T.; Ng, F.; Lam, K.F.; Yiu, K.H.; Lui, S.L.; Tse, H.F.; Siu, C.W.; Lo, W.K. Prevalence of and associations with reduced exercise capacity in peritoneal dialysis patients. Am. J. Kidney Dis. 2013, 62, 939–946. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Group in the Lowest Percentile of VO2max (<17 mL/kg/min) n = 54 | Group in Higher Percentiles of VO2max n = 131 | p |
|---|---|---|---|
| Age | 51.28 (±8.13) | 54.94 (±7.54) | 0.005 |
| Height (cm) | (160–167), 164 * | (160–167), 163 * | 0.28 |
| Body mass (kg) | (71.8–93.5), 81.45 * | (62.1–80.2), 68.8 * | <0.0001 |
| BMI (kg/m2) | (26.80–34.76), 30.34 * | (22.93–29.71), 25.85 * | <0.0001 |
| Glucose (mg/dL) | (87–99), 93 * | (87–97), 92 * | 0.54 |
| HDL cholesterol (mg/dL) | (36–56), 47 * | (42–61.5), 51 * | <0.05 |
| LDL cholesterol (mg/dL) | 113.51 (±31.23) | 118.58 (±36.05) | 0.42 |
| Triglycerides (mg/dL) | (80–183), 124 * | (82–153), 114 * | 0.42 |
| Hemoglobin (g/dL) | (12.5–13.9), 13.45 * | (12.5–14.2), 13.5 * | 0.64 |
| GFR (mL/min/1.73 m3) | (75.8–96.1), 85.25 * | (76.5–100.3), 86.1 * | 0.6 |
| ALT (U/L) | (14–27), 20 * | (14–27), 19 * | 0.98 |
| AST (U/L) | (20–26), 23 * | (19–26), 22 * | 0.46 |
| hs-CRP (mg/L) | (0.5–0.76), 0.5 * | (0.5–0.56), 0.5 * | 0.1 |
| hs-cTnT (pg/mL) | (3.4–5.9), 4.5 * | (3–4.7), 3.4 * | 0.001 |
| NT-proBNP (pg/mL) | (37–140), 71 * | (40–97), 64 * | 0.32 |
| Parameter | Group in the Lowest Percentile of VO2max (<17 mL/kg/min) n = 54 | Group in Higher Percentiles of VO2max n = 131 | p |
|---|---|---|---|
| EF (%) | (61–65), 64 * | (61–67), 64 * | 0.7 |
| LA volume (mL) | (55–71.5), 62.5 * | (45.5–65.5), 52 * | 0.0003 |
| LAVi (mL/m2) | (28.35–38.9), 34.03 * | (27.24–35.84), 30.12 * | 0.07 |
| E′ (cm/s) | (8–10.5), 8.5 * | (8.5–12), 10 * | 0.001 |
| A′ (cm/s) | (10–12.5), 11 * | (9–12), 10 * | 0.02 |
| E/E′ (cm/s) | (7.2–10), 8.2 * | (6.56–8.7), 7.68 * | 0.04 |
| TAPSE (mm) | (22–26), 23 * | (21–27), 23 * | 0.96 |
| PWV (m/s) | (6.9–8.8), 7.65 * | (6.8–8.5), 7.4 * | 0.36 |
| Aortic SP (mmHg) | (112–130), 119 * | (109–129), 118 * | 0.36 |
| Aortic PP (mmHg) | (41–80), 68.5 * | (41–80), 63 * | 0.64 |
| AP (mmHg) | (9–17), 13 * | (10–15), 12 * | 0.5 |
| Alx (%) | (23–42), 31.5 * | (27–37), 32 * | 0.91 |
| Alx@HR75 (%) | (22–36), 27.5 * | (23–35), 32 * | 0.74 |
| Parameter | Group in the Lowest Percentile of VO2max (<17 mL/kg/min) n = 54 | Group in Higher Percentiles of VO2max n = 131 | p |
|---|---|---|---|
| Exercise time (min) | 9.05 (±2.07) | 7.28 (±1.93) | <0.0001 |
| HR max | 150.06 (±16.05) | 127.17 (±19.89) | <0.0001 |
| Peripheral SBP max (mmHg) | (160–190), 180 * | (160–190), 170 * | 0.88 |
| Peripheral DBP max (mmHg) | (80–90), 80 * | (80–90), 80 * | 0.44 |
| FEV1 (L) | (2.19–2.87), 2.63 * | (2.48–2.98), 2.71 * | 0.01 |
| FVC (L) | (2.48–3.34), 3.15 * | (2.97–3.75), 3.34 * | 0.001 |
| FVC% | (95–115), 105 * | (101.5–123.5), 111 * | 0.001 |
| FEV1/FVC | (79–88), 85 * | (78–87), 83 * | 0.13 |
| FEV1/FVC% | (100–113), 108 * | (98–109), 105 * | 0.02 |
| FEF 25–75 | (1.65–3.13), 2.43 * | (1.88–3.19), 2.59 * | 0.13 |
| RER | (1.01–1.12), 1.07 * | (1.09–1.18), 1.14 * | <0.0001 |
| VO2max (mL/min/kg) | (14–16), 15 * | (18–23), 21 * | <0.0001 |
| VO2AT (mL/min/kg) | (9–11), 10 * | (12–15), 13 * | <0.0001 |
| Peak VO2max (L/min) | (1.09–1.4), 1.24 * | (1.29–1.64), 1.45 * | <0.0001 |
| VE/VCO2 slope | 27.98 (±3.71) | 29.35 (±4.55) | 0.04 |
| Parameter | Group in the Lowest Percentile of VO2max (<17 mL/kg/min) n = 54 | Group in Higher Percentiles of VO2max n = 131 | p |
|---|---|---|---|
| Fat (%) | (35.8–40.8), 38.3 * | (29.45–38.1), 33.75 * | <0.0001 |
| Fat (kg) | (27.3–37.7), 30.4 * | (17.75–29.5), 23.8 * | <0.0001 |
| FFM (kg) | (50.8–56.8), 53.8 * | (42.1–47.2), 44.8 * | <0.0001 |
| TBW (kg) | (32.1–39.5), 36.25 * | (30.5–35.7), 32.4 * | 0.0002 |
| TBW (%) | (42–45.3), 43.7 * | (43.9–50.3), 47.1 * | <0.0001 |
| ECW (kg) | (14.8–18.3), 16.7 * | (13.6–16.2), 14.4 * | <0.0001 |
| ICW (kg) | (17.5–21), 19.3 * | (16.5–19.5), 18 * | 0.005 |
| ECW/TBW × 100% | (45.45–47.28), 46.5 * | (43.75–46.28), 45 * | <0.0001 |
| Metabolic age | (54–67), 61 * | (40–59), 47 * | <0.0001 |
| Variable | OR | 95% CI for OR | p | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| ECW/TBW × 100% | 4.45 | 1.77 | 11.21 | 0.002 |
| BMI | 7.11 | 2.01 | 25.11 | 0.002 |
| hs-cTnT | 2.69 | 1.23 | 5.91 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bielecka-Dabrowa, A.; Gryglewska, K.; Sakowicz, A.; von Haehling, S.; Janikowski, K.; Maciejewski, M.; Banach, M. Factors and Prognostic Significance of Impaired Exercise Tolerance in Women over 40 with Arterial Hypertension. J. Pers. Med. 2021, 11, 759. https://doi.org/10.3390/jpm11080759
Bielecka-Dabrowa A, Gryglewska K, Sakowicz A, von Haehling S, Janikowski K, Maciejewski M, Banach M. Factors and Prognostic Significance of Impaired Exercise Tolerance in Women over 40 with Arterial Hypertension. Journal of Personalized Medicine. 2021; 11(8):759. https://doi.org/10.3390/jpm11080759
Chicago/Turabian StyleBielecka-Dabrowa, Agata, Katarzyna Gryglewska, Agata Sakowicz, Stephan von Haehling, Kamil Janikowski, Marek Maciejewski, and Maciej Banach. 2021. "Factors and Prognostic Significance of Impaired Exercise Tolerance in Women over 40 with Arterial Hypertension" Journal of Personalized Medicine 11, no. 8: 759. https://doi.org/10.3390/jpm11080759
APA StyleBielecka-Dabrowa, A., Gryglewska, K., Sakowicz, A., von Haehling, S., Janikowski, K., Maciejewski, M., & Banach, M. (2021). Factors and Prognostic Significance of Impaired Exercise Tolerance in Women over 40 with Arterial Hypertension. Journal of Personalized Medicine, 11(8), 759. https://doi.org/10.3390/jpm11080759