
Plateletworks® as a Point-of-Care Test for ASA Non-Sensitivity


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Patient Selection
2.3. Baseline Measurements
2.4. Specimen Collection
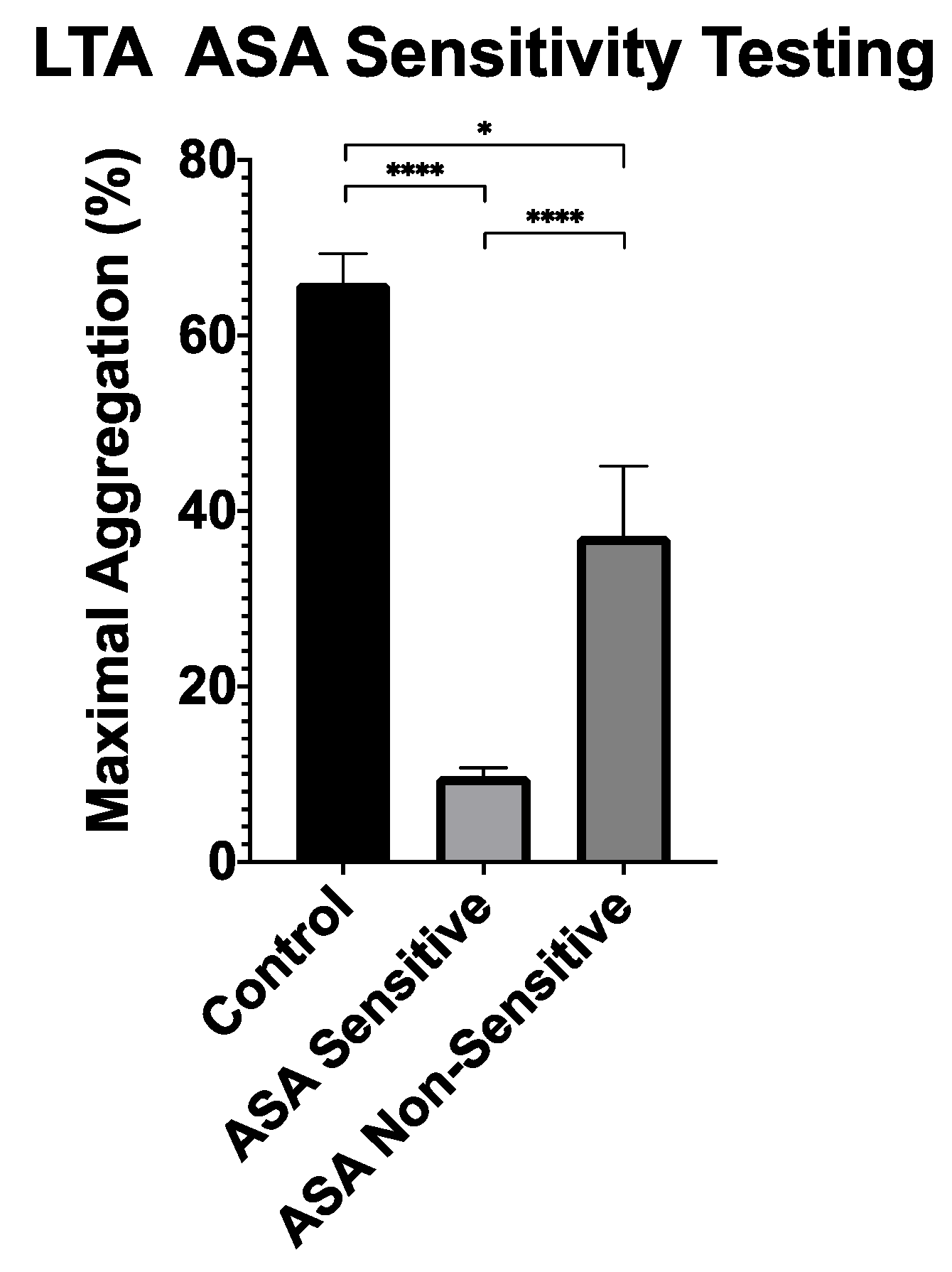
2.5. Gold Standard Light Transmission Aggregometry-Aspirin Sensitivity Testing
2.6. Plateletworks® Testing
2.7. Statistical Analysis
2.8. Optimal Cut-Off Point Selection for Predicting ASA Non-Sensitivity
3. Results
3.1. ASA Non-Sensitivity Cut-Off Point Discovery
3.1.1. Patient Characteristics
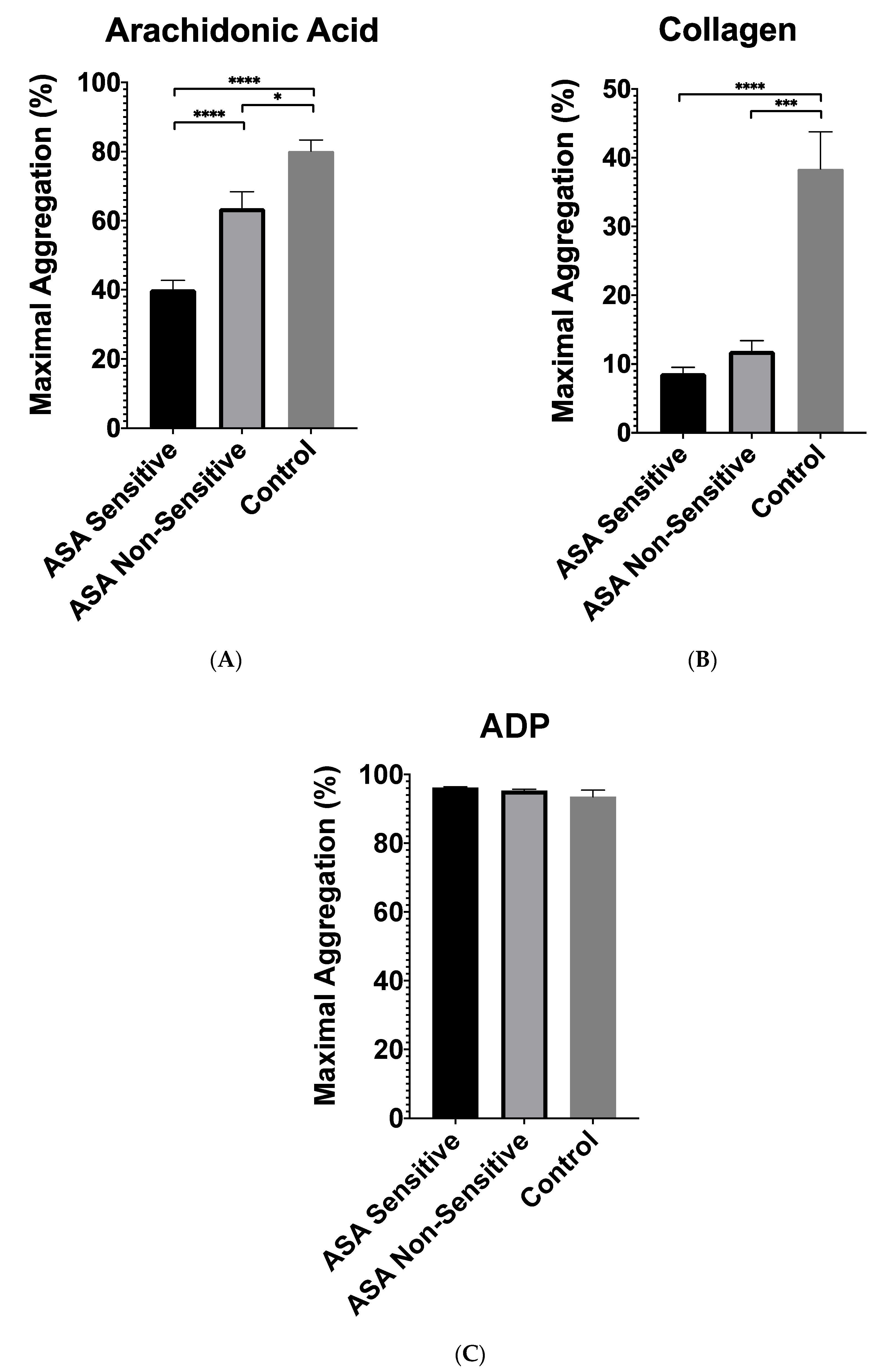
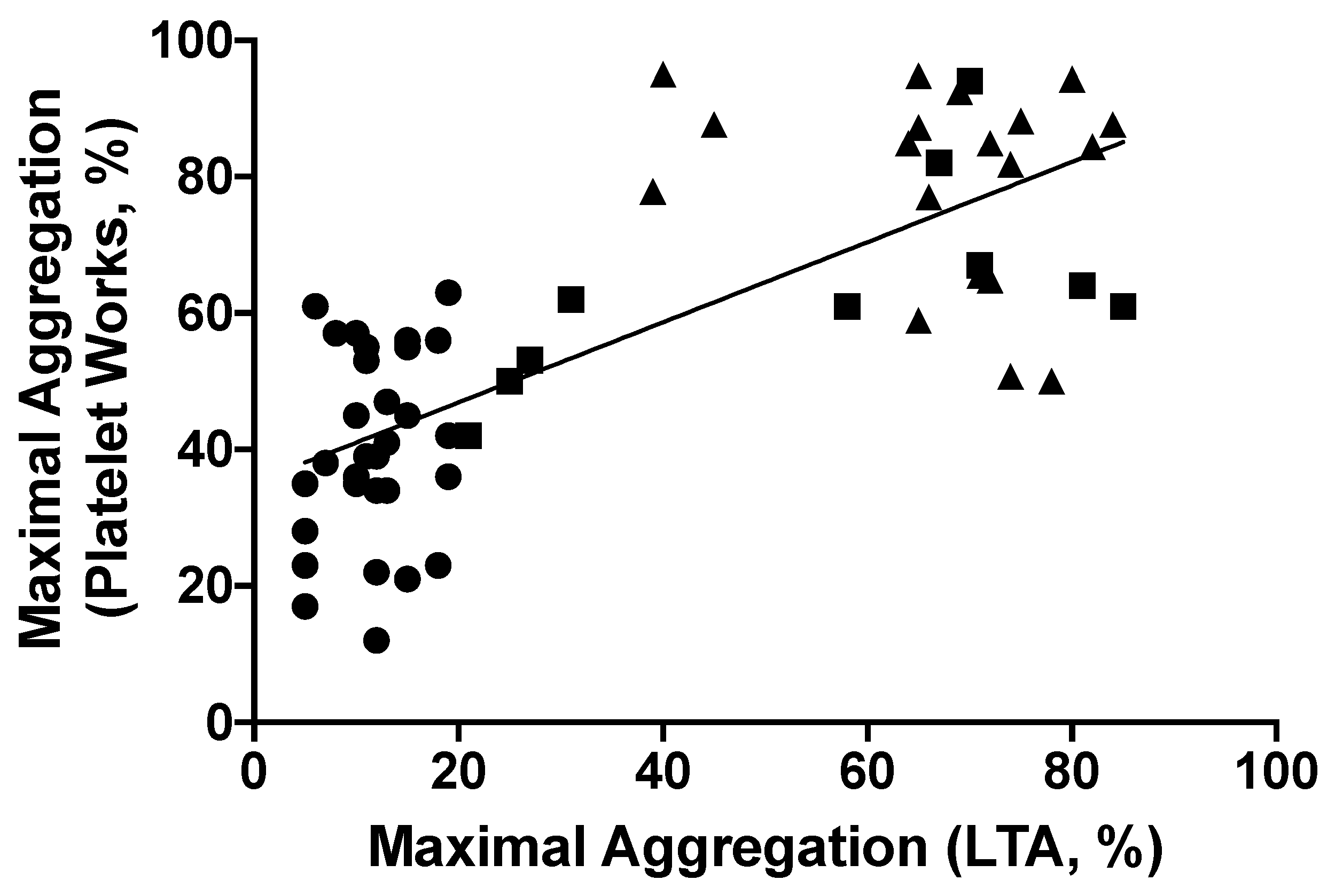
3.1.2. Plateletworks® Analysis
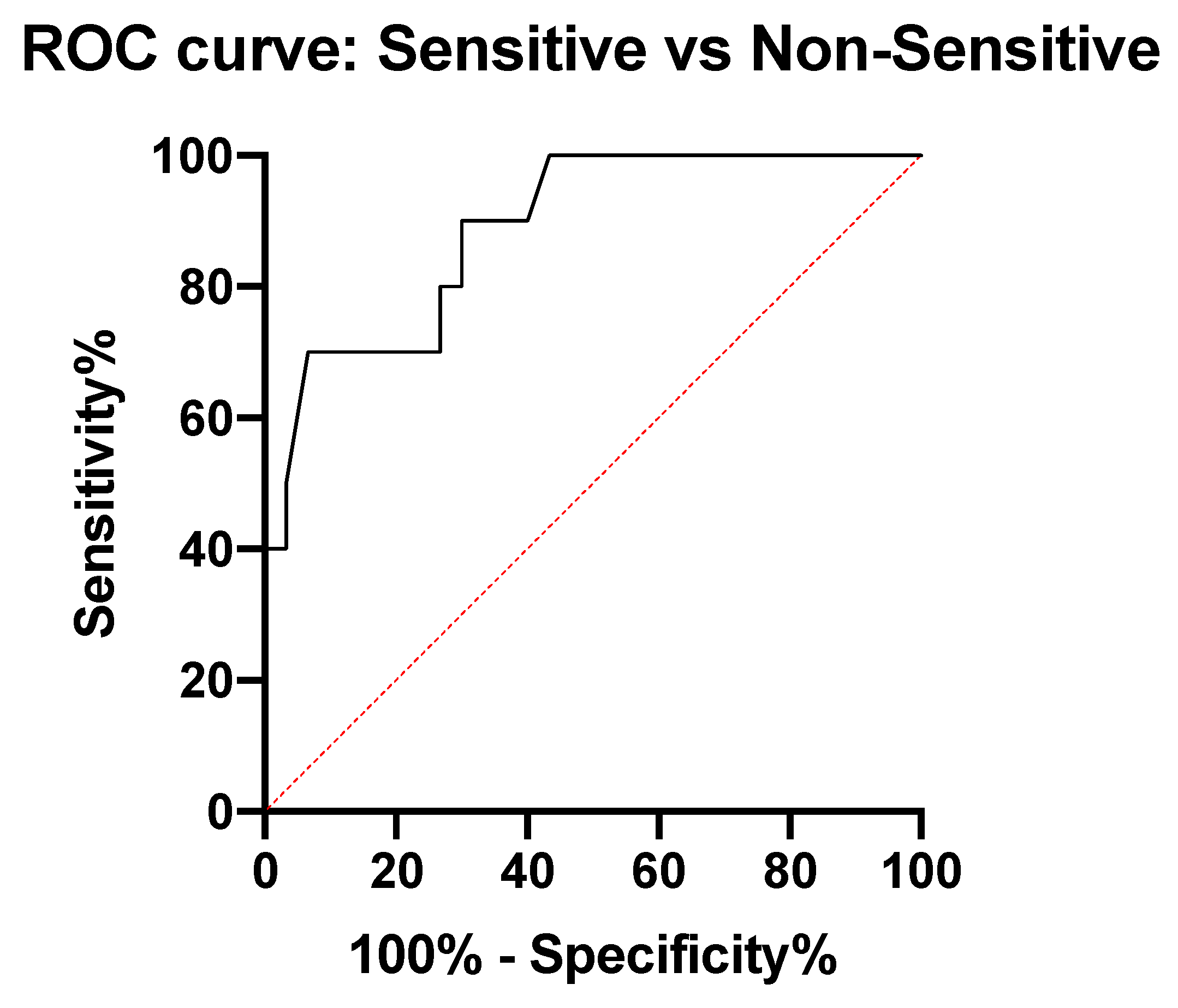
3.1.3. Cut-Off Point Discovery
3.2. ASA Non-Sensitivity Cut-Off Point Validation
3.2.1. Patient Characteristics
3.2.2. Cut-Off Point Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ittaman, S.V.; VanWormer, J.J.; Rezkalla, S.H. The Role of Aspirin in the Prevention of Cardiovascular Disease. Clin. Med. Res. 2014, 12, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Ricotta, J.J.; Aburahma, A.; Ascher, E.; Eskandari, M.; Faries, P.; Lal, B.K. Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary. J. Vasc. Surg. 2011, 54, 832–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Available online: https://pubmed.ncbi.nlm.nih.gov/30879355/ (accessed on 30 March 2021).
- Society for Vascular Surgery Practice Guidelines for Atherosclerotic Occlusive Disease of the Lower Extremities: Management of Asymptomatic Disease and Claudication. Available online: https://pubmed.ncbi.nlm.nih.gov/25638515/ (accessed on 30 March 2021).
- Bachert, C.; Чучалин, А.; Eisebitt, R.; Netayzhenko, V.Z.; Voelker, M. Aspirin Compared with Acetaminophen in the Treatment of Feverand OtherSymptoms of Upper Respiratory Tract Infection in Adults: A Multicenter, Randomized, Double-Blind, Double-Dummy, Placebo-Controlled, Parallel-Group, Single-Dose, 6-Hour Dose-Ranging Study. Clin. Ther. 2005, 27, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Group BMJP. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002, 324, 71–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, K.A. Aspirin Resistance. Neurohospitalist 2011, 1, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Clavijo, L.C.; Al-Asady, N.; Dhillon, A.; Matthews, R.V.; Caro, J.; Tun, H.; Rowe, V.; Shavelle, D.M. Prevalence of high on-treatment (aspirin and clopidogrel) platelet reactivity in patients with critical limb ischemia. Cardiovasc. Revascularization Med. 2018, 19, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Guirgis, M.; Thompson, P.; Jansen, S. Review of aspirin and clopidogrel resistance in peripheral arterial disease. J. Vasc. Surg. 2017, 66, 1576–1586. [Google Scholar] [CrossRef]
- Pasala, T.; Hoo, J.S.; Lockhart, M.K.; Waheed, R.; Sengodan, P.; Alexander, J.; Gandhi, S. Aspirin Resistance Predicts Adverse Cardiovascular Events in Patients with Symptomatic Peripheral Artery Disease. Tex. Heart Inst. J. 2016, 43, 482–487. [Google Scholar] [CrossRef]
- Khan, H.; Gallant, R.C.; Zamzam, A.; Jain, S.; Afxentiou, S.; Syed, M.; Kroezen, Z.; Shanmuganathan, M.; Britz-McKibbin, P.; Rand, M.L.; et al. Personalization of Aspirin Therapy Ex Vivo in Patients with Atherosclerosis Using Light Transmission Aggregometry. Diagnostics 2020, 10, 871. [Google Scholar] [CrossRef]
- Khan, H.; Gallant, R.; Jain, S.; Al-Omran, M.; De Mestral, C.; Greco, E.; Wheatcroft, M.; Alazonni, A.; Abdin, R.; Rand, M.; et al. Ticagrelor as an Alternative Antiplatelet Therapy in Cardiac Patients Non-Sensitive to Aspirin. Medicina 2020, 56, 519. [Google Scholar] [CrossRef]
- Campbell, J.; Ridgway, H.; Carville, D. Plateletworks®. Mol. Diagn. Ther. 2008, 12, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Karkouti, K.; Callum, J.; Wijeysundera, D.; Rao, V.; Crowther, M.; Grocott, H.P.; Pinto, R.; Scales, D.C.; Achen, B.; Brar, S.; et al. Point-of-Care Hemostatic Testing in Cardiac Surgery. Circulation 2016, 134, 1152–1162. [Google Scholar] [CrossRef] [PubMed]
- van Werkum, J.W.; Kleibeuker, M.; Postma, S.; Bouman, H.J.; Elsenberg, E.H.; Berg, J.M.T.; Hackeng, C.M. A comparison between the Plateletworks™-assay and light transmittance aggregometry for monitoring the inhibitory effects of clopidogrel. Int. J. Cardiol. 2010, 140, 123–126. [Google Scholar] [CrossRef]
- White, M.M.; Krishnan, R.; Kueter, T.J.; Jacoski, M.V.; Jennings, L.K. The Use of the Point of Care Helena ICHOR/Plateletworks® and the Accumetrics Ultegra® RPFA for Assessment of Platelet Function with GPIIb-IIIa Antagonists. J. Thromb. Thrombolysis 2004, 18, 163–169. [Google Scholar] [CrossRef]
- Syed, M.H.; Zamzam, A.; Khan, H.; Singh, K.; Forbes, T.L.; Rotstein, O.; Abdin, R.; Eikelboom, J.; Qadura, M. Fatty acid binding protein 3 is associated with peripheral arterial disease. JVS Vasc. Sci. 2020, 1, 168–175. [Google Scholar] [CrossRef]
- Xu, X.R.; Wang, Y.; Adili, R.; Ju, L.; Spring, C.M.; Jin, J.W.; Yang, H.; Neves, M.A.; Chen, P.; Yang, Y.; et al. Apolipoprotein A-IV binds αIIbβ3 integrin and inhibits thrombosis. Nat. Commun. 2018, 9, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Gum, P.A.; Kottke-Marchant, K.; Poggio, E.D.; Gurm, H.; Welsh, P.A.; Brooks, L.; Sapp, S.K.; Topol, E.J. Profile and prevalence of aspirin resistance in patients with cardiovascular disease. Am. J. Cardiol. 2001, 88, 230–235. [Google Scholar] [CrossRef]
- Lordkipanidze, M.; Pharand, C.; Schampaert, E.; Turgeon, J.; Palisaitis, D.A.; Diodati, J.G. A comparison of six major platelet function tests to determine the prevalence of aspirin resistance in patients with stable coronary artery disease. Eur. Heart J. 2007, 28, 1702–1708. [Google Scholar] [CrossRef] [Green Version]
- Maree, A.; Curtin, R.; Dooley, M.; Conroy, R.; Crean, P.; Cox, D.; Fitzgerald, D.J. Platelet Response to Low-Dose Enteric-Coated Aspirin in Patients with Stable Cardiovascular Disease. J. Am. Coll. Cardiol. 2005, 46, 1258–1263. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, S.B.; Grove, E.; Nielsen, H.L.; Mortensen, J.; Kristensen, S.D.; Hvas, A.-M. Evaluation of aspirin response by Multiplate® whole blood aggregometry and light transmission aggregometry. Platelets 2009, 20, 415–420. [Google Scholar] [CrossRef]
- Tantry, U.S.; Bliden, K.P.; Gurbel, P.A. Overestimation of Platelet Aspirin Resistance Detection by Thrombelastograph Platelet Mapping and Validation by Conventional Aggregometry Using Arachidonic Acid Stimulation. J. Am. Coll. Cardiol. 2005, 46, 1705–1709. [Google Scholar] [CrossRef] [Green Version]
- Mukaka, M.M. A guide to appropriate use of Correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Westphal, E.S.; Rainka, M.; Amsler, M.; Aladeen, T.; Wisniewski, C.; Bates, V.; Gengo, F.M. Prospective Determination of Aspirin Sensitivity in Patients Resistant to Low Dose Aspirin: A Proof of Concept Study. J. Clin. Pharmacol. 2018, 58, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Krasopoulos, G.; Brister, S.J.; Beattie, W.S.; Buchanan, M.R. Aspirin “resistance” and risk of cardiovascular morbidity: Systematic review and meta-analysis. BMJ 2008, 336, 195–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frontroth, J.P. Light Transmission Aggregometry. Adv. Struct. Saf. Stud. 2013, 992, 227–240. [Google Scholar] [CrossRef]
- Hvas, A.-M.; Favaloro, E.J. Platelet Function Analyzed by Light Transmission Aggregometry. Methods Mol. Biol. 2017, 1646, 321–331. [Google Scholar] [CrossRef]
- Sun, P.; McMillan-Ward, E.; Mian, R.; Israels, S.J. Comparison of light transmission aggregometry and multiple electrode aggregometry for the evaluation of patients with mucocutaneous bleeding. Int. J. Lab. Hematol. 2019, 41, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Van Werkum, J.W.; Harmsze, A.M.; Elsenberg, E.H.A.M.; Bouman, H.J.; Berg, J.M.T.; Hackeng, C.M. The use of the VerifyNowsystem to monitor antiplatelet therapy: A review of the current evidence. Platelets 2008, 19, 479–488. [Google Scholar] [CrossRef]
- Chung, Y.H.; Lee, K.A.; Cho, M.; Shin, S.; Lee, B.K. Performance comparison of platelet function analyzers in cardiology patients: VerifyNow and Anysis-200 aspirin assays. Clin. Hemorheol. Microcirc. 2020, 76, 33–42. [Google Scholar] [CrossRef]
- Nielsen, H.L.; Kristensen, S.D.; Thygesen, S.S.; Mortensen, J.; Pedersen, S.B.; Grove, E.L.; Hvas, A.-M. Aspirin response evaluated by the VerifyNow™ Aspirin System and Light Transmission Aggregometry. Thromb. Res. 2008, 123, 267–273. [Google Scholar] [CrossRef]
- Nielsen, H.L.; Kristensen, S.D.; Hvas, A.-M. Is the New Point-of-Care Test VerifyNow® Aspirin Able to Identify Aspirin Resistance Using the Recommended Cut-Off? Blood 2007, 110, 3896. [Google Scholar] [CrossRef]
- Pharand, C.; Lordkipanidzé, M.; Sia, Y.K.; Merhi, Y.; Diodati, J.G.; Blais, N. Response to aspirin in healthy individuals. Cross-comparison of light transmission aggregometry, VerifyNow system, platelet count drop, thromboelastography (TEG) and urinary 11-dehydrothromboxane B(2). Thromb. Haemost. 2009, 102, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Koltai, K.; Kesmarky, G.; Feher, G.; Tibold, A.; Toth, K. Platelet Aggregometry Testing: Molecular Mechanisms, Techniques and Clinical Implications. Int. J. Mol. Sci. 2017, 18, 1803. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discovery Phase | ||
|---|---|---|
| Control Cohort (n = 20) | Patients on 81 mg ASA (n = 40) | |
| Mean (SD) | ||
| Age (yrs) | 58 (19) | 68 (9) |
| Platelet Count (108/mL) | 186 (62) | 209 (70.47) |
| WBC (108/mL) | 6.2 (2.0) | 6.8 (1.7) |
| HCT | 0.380 (0.04) | 0.384 (0.03) |
| Frequency (%) | ||
| Sex (male) | 15 (75) | 28 (70) * |
| Hypertension | 8 (40) | 28 (70) * |
| Hyperlipidemia | 8 (40) | 32 (80) * |
| Diabetes | 2 (10) | 15 (37) * |
| Smoking | 7 (35) | 30 (75) * |
| CAD | 0 (0) | 12 (30) * |
| PAD | 5 (13) | 24 (60) * |
| Medication (%) | ||
| Statin | 9 (45) | 33 (83) * |
| ACEi/ARB | 6 (30) | 21 (53) * |
| B-blockers | 1 (5) | 9 (23) * |
| Validation Phase | |
|---|---|
| Patient Demographics | Patients on 81 mg ASA (n = 40) |
| Mean (SD) | |
| Age (yrs) | 68 (11) |
| Platelet Count (108/mL) | 185.3 (48) |
| WBC (108/mL) | 6.8 (1.9) |
| HCT | 0.3832 (0.03) |
| Frequency (%) | |
| Sex (male) | 24 (60) |
| Hypertension | 27 (68) |
| Hyperlipidemia | 33 (83) |
| Diabetes | 20 (50) |
| Smoking | 29 (73) |
| CAD | 13 (33) |
| PAD | 22 (55) |
| Medications (Frequency, %) | |
| Statin | 34 (85) |
| ACEi/ARB | 20 (50) |
| B-blockers | 9 (23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, H.; Jain, S.; Gallant, R.C.; Syed, M.H.; Zamzam, A.; Al-Omran, M.; Rand, M.L.; Ni, H.; Abdin, R.; Qadura, M. Plateletworks® as a Point-of-Care Test for ASA Non-Sensitivity. J. Pers. Med. 2021, 11, 813. https://doi.org/10.3390/jpm11080813
Khan H, Jain S, Gallant RC, Syed MH, Zamzam A, Al-Omran M, Rand ML, Ni H, Abdin R, Qadura M. Plateletworks® as a Point-of-Care Test for ASA Non-Sensitivity. Journal of Personalized Medicine. 2021; 11(8):813. https://doi.org/10.3390/jpm11080813
Chicago/Turabian StyleKhan, Hamzah, Shubha Jain, Reid C. Gallant, Muzammil H. Syed, Abdelrahman Zamzam, Mohammed Al-Omran, Margaret L. Rand, Heyu Ni, Rawand Abdin, and Mohammad Qadura. 2021. "Plateletworks® as a Point-of-Care Test for ASA Non-Sensitivity" Journal of Personalized Medicine 11, no. 8: 813. https://doi.org/10.3390/jpm11080813
APA StyleKhan, H., Jain, S., Gallant, R. C., Syed, M. H., Zamzam, A., Al-Omran, M., Rand, M. L., Ni, H., Abdin, R., & Qadura, M. (2021). Plateletworks® as a Point-of-Care Test for ASA Non-Sensitivity. Journal of Personalized Medicine, 11(8), 813. https://doi.org/10.3390/jpm11080813