
The Patient-Specific Combined Target Zone for Morpho-Functional Planning of Total Hip Arthroplasty
 , ,
, , 
Abstract
:1. Introduction
- How can we calculate suitable THA implant and implantation parameters for a specific patient considering the most relevant criteria?
- Are the resulting target zones inside conventional safe zones?
- Do patients with implantations fulfilling these combined criteria have a better outcome score?
2. Material and Methods
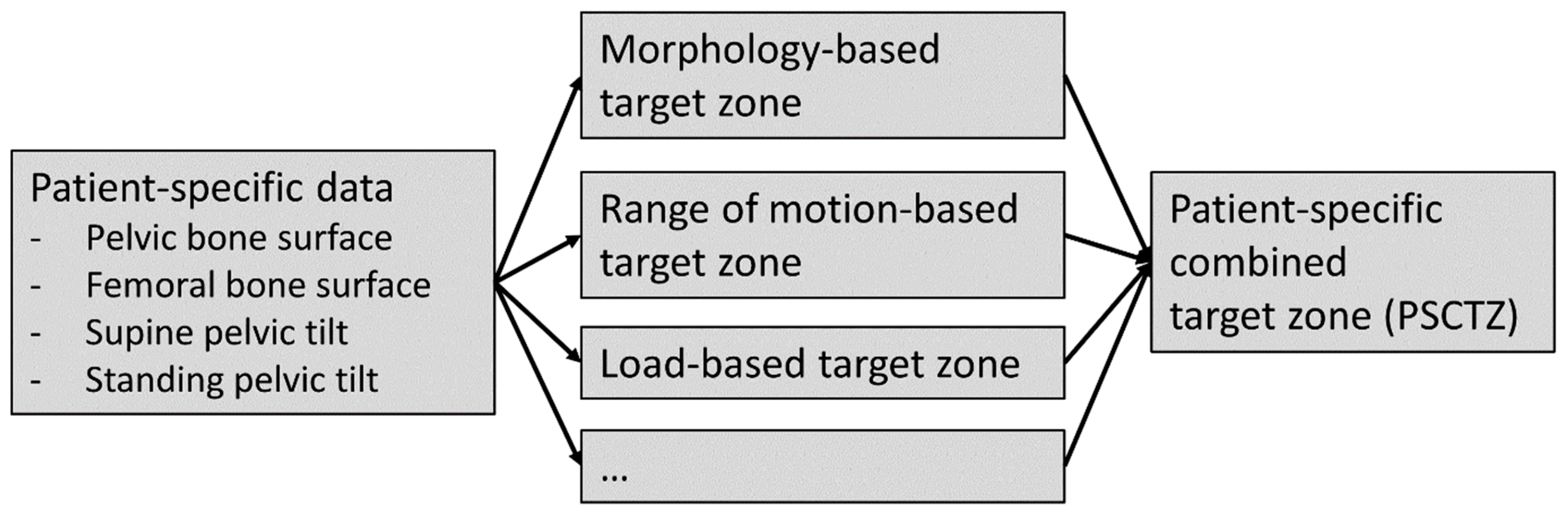
2.1. Patient-Specific Target Zone Calculation
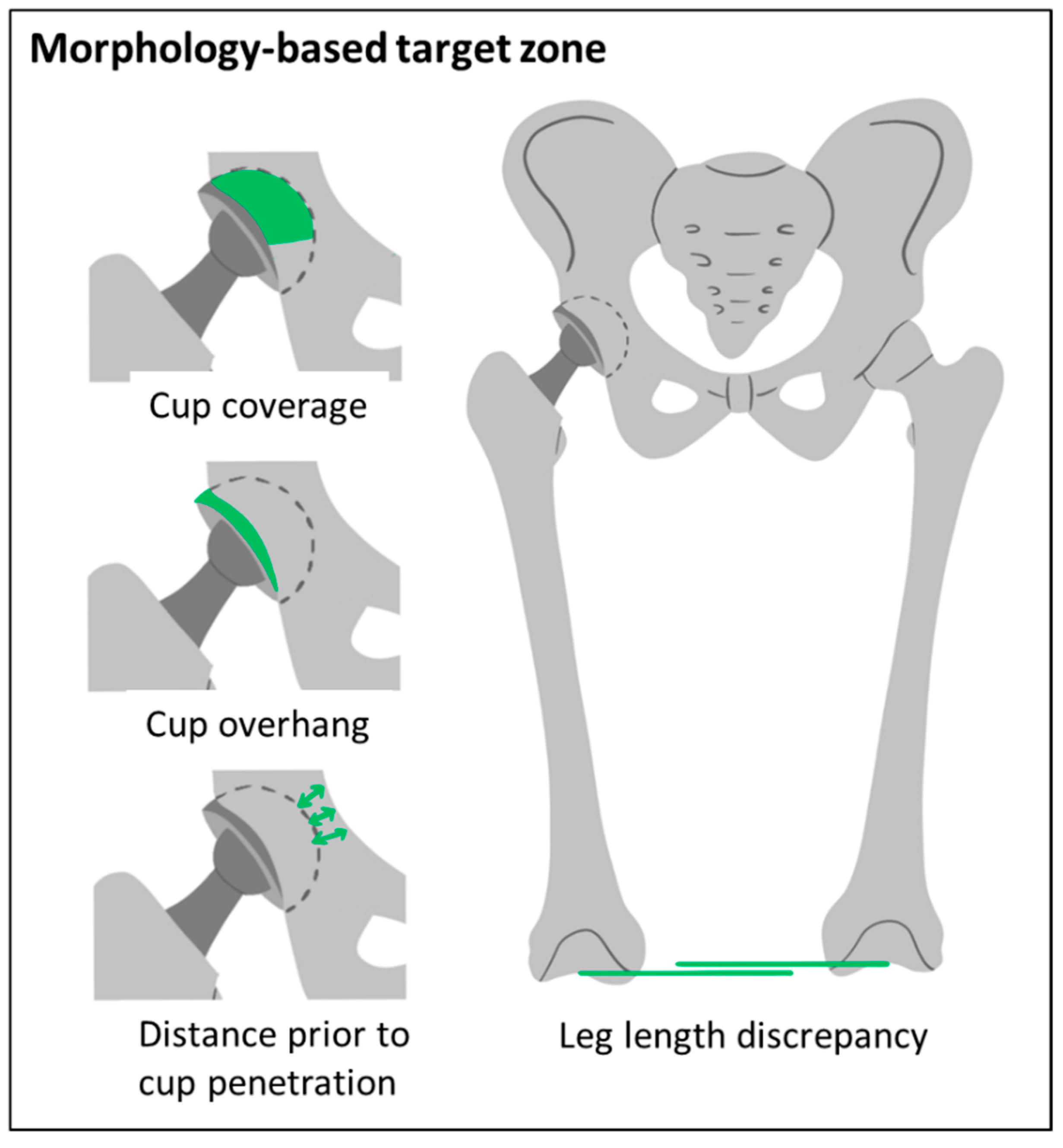
2.1.1. Morphology-Based Target Zone
- A bony coverage of at least 65%.
- An anterior cup overhang of less than 12 mm.
- A distance prior to cup penetration of at least 1 mm,
- A maximal leg length discrepancy of ±8 mm.
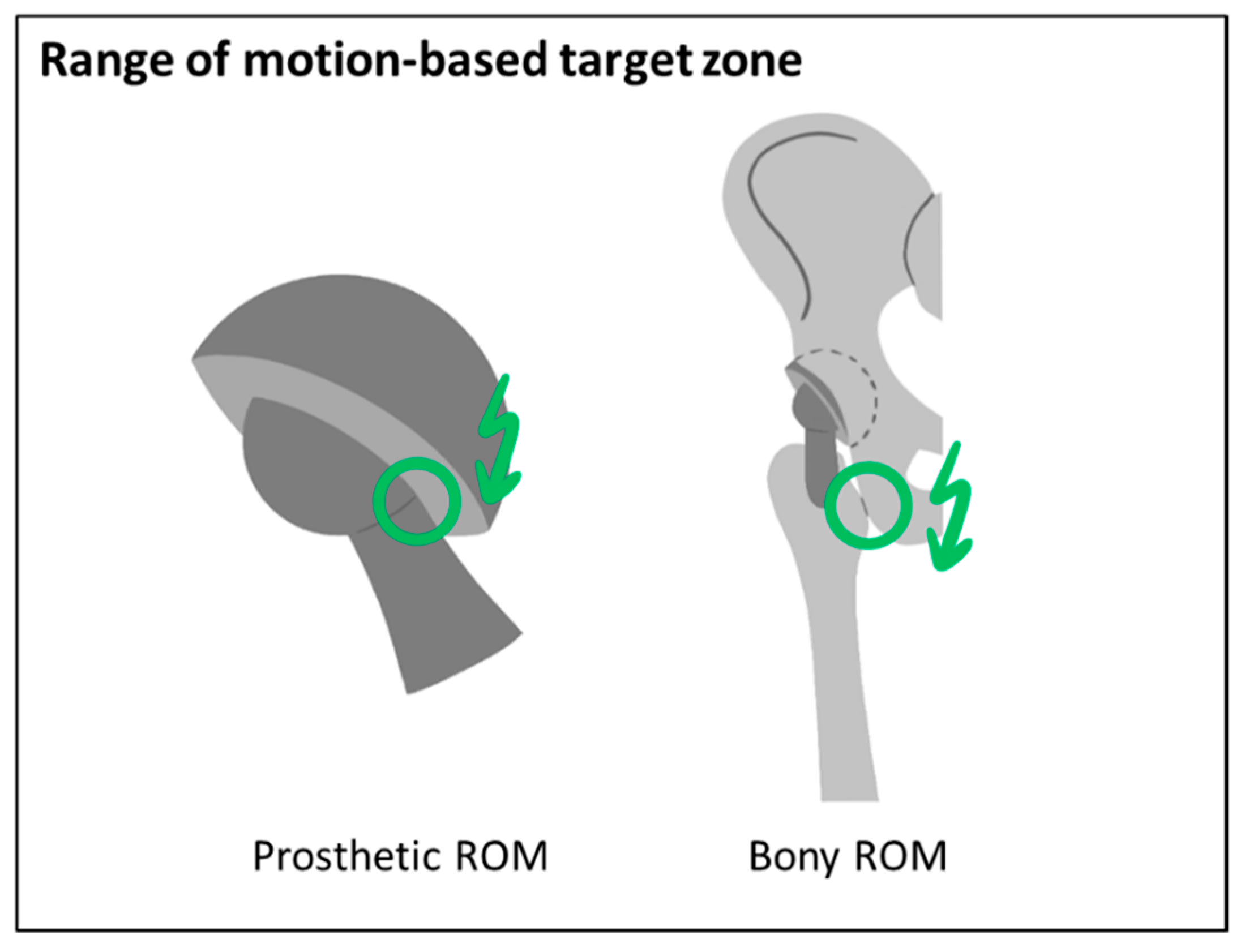
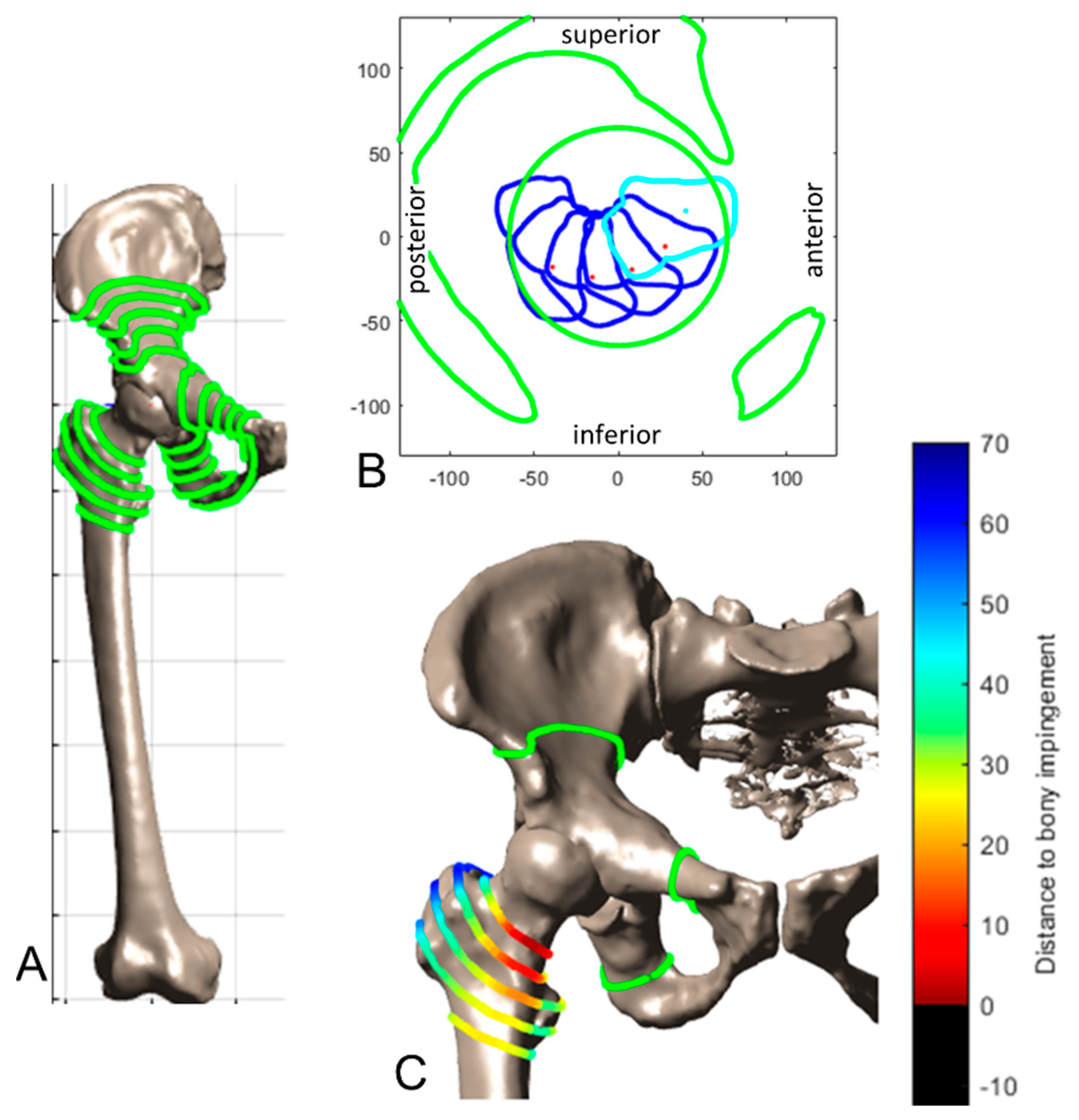
2.1.2. ROM-Based Target Zone
- No prosthetic impingement: distance to prosthetic impingement greater than 0°.
- A decrease of the bony ROM of less than 5° compared to the preoperative situation.
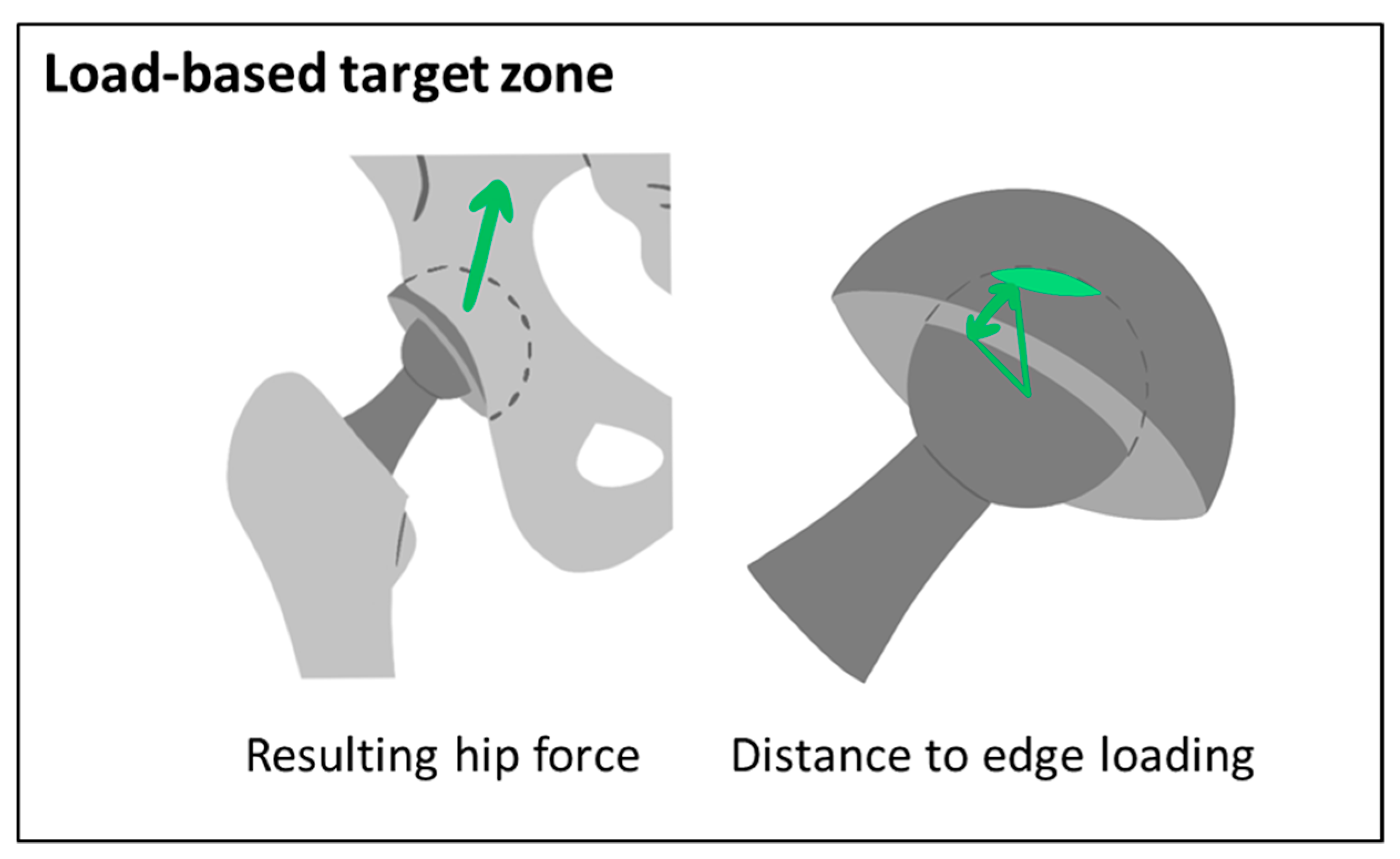
2.1.3. Load-Based Target Zone
- No edge loading: a minimal distance to edge loading greater than 0°.
- No increase of the resulting hip force: a decrease of the resulting hip force compared to the preoperative situation.
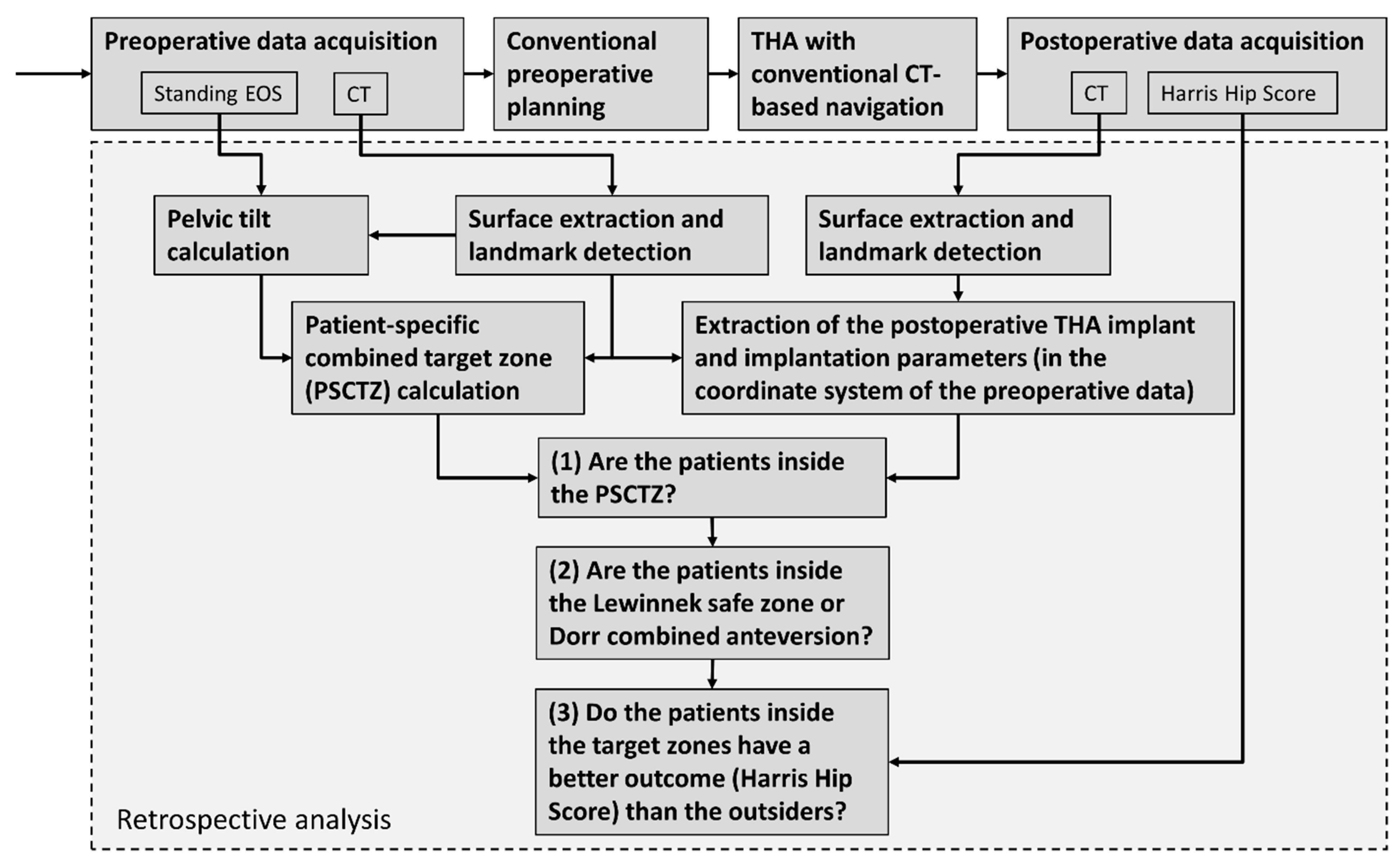
2.2. Retrospective Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The epidemiology of revision total hip arthroplasty in the United States. J. Bone Jt. Surg. 2009, 91, 128–133. [Google Scholar] [CrossRef]
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef]
- Opperer, M.; Lee, Y.Y.; Nally, F.; Perez, A.B.; Goudarz-Mehdikhani, K.; Della Valle, A.G. A critical analysis of radiographic factors in patients who develop dislocation after elective primary total hip arthroplasty. Int. Orthop. 2016, 40, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Kuijpers, M.F.L.; Hannink, G.; Vehmeijer, S.B.W.; van Steenbergen LNSchreurs, B.W. The risk of revision after total hip arthroplasty in young patients depends on surgical approach, femoral head size and bearing type; an analysis of 19,682 operations in the Dutch arthroplasty register. BMC Musculoskelet. Disord. 2019, 20, 385. [Google Scholar] [CrossRef] [Green Version]
- Corbett, K.L.; Losina, E.; Nti, A.A.; Prokopetz JJZKatz, J.N. Population-based rates of revision of primary total hip arthroplasty: A systematic review. PLoS ONE 2010, 5, e13520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere CLZimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Jt. Surg. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Callanan, M.C.; Jarrett, B.; Bragdon, C.R.; Zurakowski, D.; Rubash, H.E.; Freiberg, A.A.; Malchau, H. The John Charnley Award: Risk factors for cup malpositioning: Quality improvement through a joint registry at a tertiary hospital. Clin. Orthop. Relat. Res. 2011, 469, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Seagrave, K.G.; Troelsen, A.; Malchau, H.; Husted, H.; Gromov, K. Acetabular cup position and risk of dislocation in primary total hip arthroplasty: A systematic review of the literature. Acta Orthop. 2016, 88, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Abdel, M.P.; Roth, P.; von Jennings, M.T.; Hanssen, A.D.; Pagnano, M.W. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin. Orthop. Relat. Res. 2016, 474, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Fackler, C.D.; Poss, R. Dislocation in total hip arthroplasties. Clin. Orthop. Relat. Res. 1980, 151, 169–178. [Google Scholar] [CrossRef]
- Ali Khan, M.A.; Brakenbury, P.H.; Reynolds, I.S. Dislocation following total hip replacement. J. Bone Jt. Surg. 1981, 63, 214–218. [Google Scholar] [CrossRef] [Green Version]
- Dorr, L.D.; Wolf, A.W.; Chandler, R.; Conaty, J.P. Classification and treatment of dislocations of total hip arthroplasty. Clin. Orthop. Relat. Res. 1983, 173, 151–158. [Google Scholar] [CrossRef]
- Kohn, D.; Rühmann, O.; Wirth, C.J. Die Verrenkung der Hüfttotalendoprothese unter besonderer Beachtung verschiedener Zugangswege. Z. Orthop. Ihre. Grenzgeb. 1997, 135, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, R.; Tonin, A.; Krismer, M.; Rachbauer, F.; Eibl, G.; Stöckl, B. Reducing the risk of dislocation after total hip arthroplasty. The Effect of Orientation of the Acetabular Component. J. Bone Jt. Surg. 2005, 87, 762–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masaoka, T.; Yamamoto, K.; Shishido, T.; Katori, Y.; Mizoue, T.; Shirasu, H.; Nunoda, D. Study of hip joint dislocation after total hip arthroplasty. Int. Orthop. 2005, 30, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Dudda, M.; Gueleryuez, A.; Gautier, E.; Busato, A.; Röder, C. Risk factors for early dislocation after total hip arthroplasty: A matched case-control study. J. Orthop. Surg. 2010, 18, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Murphy, W.S.; Kowal, J.H.; Murphy, S.B. The Safe Zone for Acetabular Component Orientation. Orthop. Proc. 2013, 95-B (Suppl. 28), 44. [Google Scholar]
- Danoff, J.R.; Bobman, J.T.; Cunn, G.; Murtaugh, T.; Gorroochurn, P.; Geller, J.A.; Macaulay, W. Redefining the acetabular component safe zone for posterior approach total hip arthroplasty. J. Arthroplast. 2016, 31, 506–511. [Google Scholar] [CrossRef]
- Fujishiro, T.; Hiranaka, T.; Hashimoto, S.; Hayashi, S.; Kurosaka, M.; Kanno, T.; Masuda, T. The effect of acetabular and femoral component version on dislocation in primary total hip arthroplasty. Int. Orthop. 2016, 40, 697–702. [Google Scholar] [CrossRef]
- Ranawat, C.S.; Maynard, M.J. Modern technique of cemented total hip arthroplasty. Tech. Orthop. 1991, 6, 17–25. [Google Scholar] [CrossRef]
- Jolles, B.M.; Zangger, P.; Leyvraz, P.-F. Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J. Arthroplast. 2002, 17, 282–288. [Google Scholar] [CrossRef]
- Dorr, L.D.; Malik, A.; Dastane, M.; Wan, Z. Combined anteversion technique for total hip arthroplasty. Clin. Orthop. Relat. Res. 2009, 467, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Jaramaz, B.; DiGioia, A.M., III; Blackwell, M.; Nikou, C. Computer assisted measurement of cup placement in total hip replacement. Clin. Orthop. Relat. Res. 1998, 354, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Barrack, R.L.; Lavernia, C.; Ries, M.; Thornberry, R.; Tozakoglou, E. Virtual reality computer animation of the effect of component position and design on stability after total hip arthroplasty. Orthop. Clin. N. Am. 2001, 32, 569–577. [Google Scholar] [CrossRef]
- Ezquerra, L.; Quilez, M.P.; Pérez, M.Á.; Albareda, J.; Seral, B. Range of Movement for Impingement and Dislocation Avoidance in Total Hip Replacement Predicted by Finite Element Model. J. Med. Biol. Eng. 2017, 37, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, K.-H. The Impingement-free, Prosthesis-specific, and Anatomy-adjusted Combined Target Zone for Component Positioning in THA Depends on Design and Implantation Parameters of both Components. Clin. Orthop. Relat. Res. 2020, 478, 1904–1918. [Google Scholar] [CrossRef] [PubMed]
- Herrlin, K.; Selvik, G.; Pettersson, H. Space orientation of total hip prosthesis. A method for three-dimensional determination. Acta Radiol. Diagn. 1986, 27, 619–627. [Google Scholar] [CrossRef]
- Hsu, J.; de La Fuente, M.; Radermacher, K. Calculation of impingement-free combined cup and stem alignments based on the patient-specific pelvic tilt. J. Biomech. 2019, 82, 193–203. [Google Scholar] [CrossRef]
- Yoshimine, F. The safe-zones for combined cup and neck anteversions that fulfill the essential range of motion and their optimum combination in total hip replacements. J. Biomech. 2006, 39, 1315–1323. [Google Scholar] [CrossRef]
- Pedersen, D.R.; Callaghan, J.J.; Brown, T.D. Activity-dependence of the “safe zone” for impingement versus dislocation avoidance. Med. Eng. Phys. 2005, 27, 323–328. [Google Scholar] [CrossRef]
- Elkins, J.M.; Callaghan, J.J.; Brown, T.D. The 2014 Frank Stinchfield Award: The ‘landing zone’ for wear and stability in total hip arthroplasty is smaller than we thought: A computational analysis. Clin. Orthop. Relat. Res. 2015, 473, 441–452. [Google Scholar] [CrossRef] [Green Version]
- Kessler, O.; Patil, S.; Stefan, W.; Mayr, E.; Colwell, C.W., Jr.; D’Lima, D.D. Bony impingement affects range of motion after total hip arthroplasty: A subject-specific approach. J. Orthop. Res. 2008, 26, 443–452. [Google Scholar] [CrossRef]
- Kurtz, W.B.; Ecker, T.M.; Reichmann, W.M.; Murphy, S.B. Factors affecting bony impingement in hip arthroplasty. J. Arthroplast. 2010, 25, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Bunn, A.; Colwell, C.W.; D’lima, D.D. Bony impingement limits design-related increases in hip range of motion. Clin. Orthop. Relat. Res. 2012, 470, 418–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoji, T.; Yamasaki, T.; Izumi, S.; Kenji, M.; Sawa, M.; Yasunaga, Y.; Adachi, N. The effect of cup medialization and lateralization on hip range of motion in total hip arthroplasty. Clin. Biomech. 2018, 57, 121–128. [Google Scholar] [CrossRef] [PubMed]
- DiGioia, A.M.; Jaramaz, B.; Blackwell, M.; Simon, D.A.; Morgan, F.; Moody, J.E.; Nikou, C.; Colgan, B.D.; Aston, C.A.; Labarca, R.S.; et al. The Otto Aufranc Award. Image guided navigation system to measure intraoperatively acetabular implant alignment. Clin. Orthop. Relat. Res. 1998, 355, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Widmer, K.-H. Containment versus impingement: Finding a compromise for cup placement in total hip arthroplasty. Int. Orthop. 2007, 31, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, T.; Kabata, T.; Kajino, Y.; Ohmori, T.; Yoshitani, J.; Tsuchiya, H. Three-Dimensional Host Bone Coverage Required in Total Hip Arthroplasty for Developmental Dysplasia of the Hip and Its Relationship With 2-Dimensional Coverage. J. Arthroplast. 2019, 34, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, M.; Nakashima, Y.; Nakamura, T.; Ito, Y.; Hara, T. Minimum Lateral Bone Coverage Required for Securing Fixation of Cementless Acetabular Components in Hip Dysplasia. BioMed Res. Int. 2017, 2017, 4937151. [Google Scholar] [CrossRef] [PubMed]
- Pierrepont, J.W.; Stambouzou, C.Z.; Miles, B.P.; O’Connor, P.B.; Walter, L.; Ellis, A.; Molnar, R.; Baré, J.V.; Solomon, M.; McMahon, S.; et al. Patient Specific Component Alignment in Total Hip Arthroplasty. Recon. Rev. 2016, 6, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Mellon, S.J.; Grammatopoulos, G.; Andersen, M.S.; Pandit, H.G.; Gill, H.S.; Murray, D.W. Optimal acetabular component orientation estimated using edge-loading and impingement risk in patients with metal-on-metal hip resurfacing arthroplasty. J. Biomech. 2015, 48, 318–323. [Google Scholar] [CrossRef] [Green Version]
- Clarke, I.; Lazennec, J.-Y. Margin-of-safety Algorithm Used with EOS Imaging to Interpret MHRA Warning for 46-48mm MOM Arthroplasty. Recon. Rev. 2015, 5, 13–21. [Google Scholar] [CrossRef]
- Babisch, J.W.; Layher, F.; Ritter, B.; Venbrocks, R.A. Computer-assisted Biomechanically Based Two-dimensional Planning of Hip Surgery. Transl. Orthopädische Prax. 2001, 37, 29–38. [Google Scholar]
- Maratt, J.D.; Esposito, C.I.; McLawhorn, A.S.; Jerabek, S.A.; Padgett, D.E.; Mayman, D.J. Pelvic tilt in patients undergoing total hip arthroplasty: When does it matter? J. Arthroplast. 2015, 30, 387–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thelen, T.; Thelen, P.; Demezon, H.; Aunoble, S.; Le Huec, J.-C. Normative 3D acetabular orientation measurements by the low-dose EOS imaging system in 102 asymptomatic subjects in standing position: Analyses by side, gender, pelvic incidence and reproducibility. Orthop. Traumatol. Surg. Res. 2017, 103, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Pierrepont, J.; Hawdon, G.; Miles, B.P.; Connor, B.O.; Baré, J.; Walter, L.R.; Marel, E.; Solomon, M.; McMahon, S.; Shimmin, A.J. Variation in functional pelvic tilt in patients undergoing total hip arthroplasty. Bone Jt. J. 2017, 99, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Dardenne, G.; Dusseau, S.; Hamitouche, C.; Lefèvre, C.; Stindel, E. Toward a dynamic approach of THA planning based on ultrasound. Clin. Orthop. Relat. Res. 2009, 467, 901–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutter, E.G.; Wellman, S.S.; Bolognesi, M.P.; Seyler, T.M. A Geometric Model to Determine Patient-Specific Cup Anteversion Based on Pelvic Motion in Total Hip Arthroplasty. Adv. Orthop. 2019, 2019, 4780280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannast, M.; Langlotz, U.; Siebenrock, K.A.; Wiese, M.; Bernsmann, K.; Langlotz, F. Anatomic referencing of cup orientation in total hip arthroplasty. Clin. Orthop. Relat. Res. 2005, 436, 144–150. [Google Scholar] [CrossRef]
- Babisch, J.W.; Layher, F.; Amiot, L.-P. The rationale for tilt-adjusted acetabular cup navigation. J. Bone Jt. Surg. 2008, 90, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Lembeck, B.; Mueller, O.; Reize, P.; Wuelker, N. Pelvic tilt makes acetabular cup navigation inaccurate. Acta Orthop. 2005, 76, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Jolles, B.M.; Genoud, P.; Hoffmeyer, P. Computer-assisted Cup Placement Techniques in Total Hip Arthroplasty Improve Accuracy of Placement. Clin. Orthop. Relat. Res. 2004, 426, 174–179. [Google Scholar] [CrossRef]
- Osmani, F.A.; Thakkar, S.; Ramme, A.; Elbuluk, A.; Wojack, P.; Vigdorchik, J.M. Variance in predicted cup size by 2-dimensional vs 3-dimensional computerized tomography-based templating in primary total hip arthroplasty. Arthroplast. Today 2017, 3, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Huppertz, A.; Radmer, S.; Asbach, P.; Juran, R.; Schwenke, C.; Diederichs, G.; Hamm, B.; Sparmann, M. Computed tomography for preoperative planning in minimal-invasive total hip arthroplasty: Radiation exposure and cost analysis. Eur. J. Radiol. 2011, 78, 406–413. [Google Scholar] [CrossRef]
- Imai, N.; Ito, T.; Suda, K.; Miyasaka, D.; Endo, N. Pelvic Flexion Measurement From Lateral Projection Radiographs is Clinically Reliable. Clin. Orthop. Relat. Res. 2013, 471, 1271–1276. [Google Scholar] [CrossRef] [Green Version]
- Fischer, M.C.M.; Tokunaga, K.; Okamoto, M.; Habor, J.; Radermacher, K. Preoperative factors improving the prediction of the postoperative sagittal orientation of the pelvis in standing position after total hip arthroplasty. Sci. Rep. 2020, 10, 15944. [Google Scholar] [CrossRef]
- Marques, C.J.; Martin, T.; Fiedler, F.; Weber, M.; Breul, V.; Lampe, F.; Kozak, J. Intra- and Inter-rater Reliability of Navigated Ultrasound in the Assessment of Pelvic Tilt in Symptom-Free Young Adults. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2018, 37, 2333–2342. [Google Scholar] [CrossRef]
- Dardenne, G.; Pluchon, J.P.; Letissier, H.; Guezou-Philippe, A.; Gerard, R.; Lefevre, C.; Stindel, E. Accuracy and Precision of an Ultrasound-Based Device to Measure the Pelvic Tilt in Several Positions. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2020, 39, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Hartel, M.J.; Petersik, A.; Schmidt, A.; Kendoff, D.; Nüchtern, J.; Rueger, J.M.; Lehmann, W.; Grossterlinden, L.G. Determination of Femoral Neck Angle and Torsion Angle Utilizing a Novel Three-Dimensional Modeling and Analytical Technology Based on CT Datasets. PLoS ONE 2016, 11, e0149480. [Google Scholar] [CrossRef] [PubMed]
- Cyteval, C.; Sarrabère, M.P.; Cottin, A.; Assi, C.; Morcos, L.; Maury, P.; Taourel, P. Iliopsoas Impingement on the Acetabular Component: Radiologic and Computed Tomography Findings of a Rare Hip Prosthesis Complication in Eight Cases. J. Comput. Assist. Tomogr. 2003, 27, 183–188. [Google Scholar] [CrossRef]
- Otomaru, I.; Kobayashi, K.; Okada, T.; Nakamoto, M.; Kagiyama, Y.; Takao, M.; Sugano, N.; Tada, Y.; Sato, Y. Expertise modeling for automated planning of acetabular cup in total hip arthroplasty using combined bone and implant statistical atlases. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2009; Volume 2009, pp. 532–539. [Google Scholar]
- Kagiyama, Y.; Otomaru, I.; Takao, M.; Sugano, N.; Nakamoto, M.; Yokota, F.; Tomiyama, N.; Tada, Y.; Sato, Y. CT-based automated planning of acetabular cup for total hip arthroplasty (THA) based on hybrid use of two statistical atlases. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 2253–2271. [Google Scholar] [CrossRef]
- Pathak, P.K.; Gupta, R.K.; Meena, H.S.; Fiske, R. Limb length discrepancy after total hip arthroplasty: A systematic review. Int. J. Res. Orthop. 2018, 4, 690. [Google Scholar] [CrossRef]
- Turley, G.A.; Ahmed, S.M.Y.; Williams, M.A.; Griffin, D.R. Establishing a range of motion boundary for total hip arthroplasty. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2011, 225, 769–782. [Google Scholar] [CrossRef] [PubMed]
- Sugano, N.; Tsuda, K.; Miki, H.; Takao, M.; Suzuki, N.; Nakamura, N. Dynamic measurements of hip movement in deep bending activities after total hip arthroplasty using a 4-dimensional motion analysis system. J. Arthroplast. 2012, 27, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.C.M.; Damm, P.; Habor, J.; Radermacher, K. Effect of the underlying cadaver data and patient-specific adaptation of the femur and pelvis on the prediction of the hip joint force estimated using static models. J. Biomech. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Imado, K.; Kido, Y.; Miyagawa, H. A method of calculation for contact pressure between femoral head and cup of artificial hip joint. Tribol. Trans. 2005, 48, 230–237. [Google Scholar] [CrossRef]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Jt. Surg. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- Fischer, M.C.M.; Krooß, F.; Habor, J.; Radermacher, K. A robust method for automatic identification of landmarks on surface models of the pelvis. Sci. Rep. 2019, 9, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, M.C.M.; Grothues, S.A.G.A.; Habor, J.; de La Fuente, M.; Radermacher, K. A robust method for automatic identification of femoral landmarks, axes, planes and bone coordinate systems using surface models. Sci. Rep. 2020, 10, 20859. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.W. The definition and measurement of acetabular orientation. J. Bone Jt. Surg. 1993, 75, 228–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belzunce, M.A.; Henckel, J.; Di Laura, A.; Hart, A. Uncemented femoral stem orientation and position in total hip arthroplasty: A CT study. J. Orthop. Res. 2020, 38, 1486–1496. [Google Scholar] [CrossRef] [PubMed]
- Habor, J. The Patient-specific Combined Target Zone for Total Hip Arthroplasty Planning; Shaker Verlag: Düren, Germany, 2020. [Google Scholar]
- Gagnier, J.J.; Huang, H.; Mullins, M.; Marinac-Dabic, D.; Ghambaryan, A.; Eloff, B.; Mirza, F.; Bayona, M. Measurement Properties of Patient-Reported Outcome Measures Used in Patients Undergoing Total Hip Arthroplasty: A Systematic Review. JBJS Rev. 2018, 6, e2. [Google Scholar] [CrossRef]
- Ishida, T.; Inaba, Y.; Kobayashi, N.; Iwamoto, N.; Yukizawa, Y.; Choe, H.; Saito, T. Changes in pelvic tilt following total hip arthroplasty. J. Orthop. Sci. 2011, 16, 682–688. [Google Scholar] [CrossRef]
- Parratte, S.; Pagnano, M.W.; Coleman-Wood, K.; Kaufman, K.R.; Berry, D.J. The 2008 Frank Stinchfield award: Variation in postoperative pelvic tilt may confound the accuracy of hip navigation systems. Clin. Orthop. Relat. Res. 2009, 467, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoji, T.; Yamasaki, T.; Izumi, S.; Murakami, H.; Mifuji, K.; Sawa, M.; Yasunaga, Y.; Adachi, N.; Ochi, M. Factors affecting the potential for posterior bony impingement after total hip arthroplasty. Bone Jt. J. 2017, 99, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Palit, A.; King, R.; Hart, Z.; Gu, Y.; Pierrepont, J.; Elliott, M.T.; Williams, M.A. Bone-to-Bone and Implant-to-Bone Impingement: A Novel Graphical Representation for Hip Replacement Planning. Ann. Biomed. Eng. 2020, 48, 1354–1367. [Google Scholar] [CrossRef] [Green Version]
- Matziolis, G.; Krakow, L.; Layher, F.; Sander, K.; Bossert, J.; Brodt, S. Patient-Specific Contact Stress Does Not Predict Polyethylene Wear Rate in a Specific Pressfit Cup. J. Arthroplast. 2017, 32, 3802–3805. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inside | Outside | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Median (Min., Max.) | Percentage of Insiders below a HHS of 95 (%) | n | Median (Min., Max.) | Percentage of Insiders below a HHS of 95 (%) | p | |||
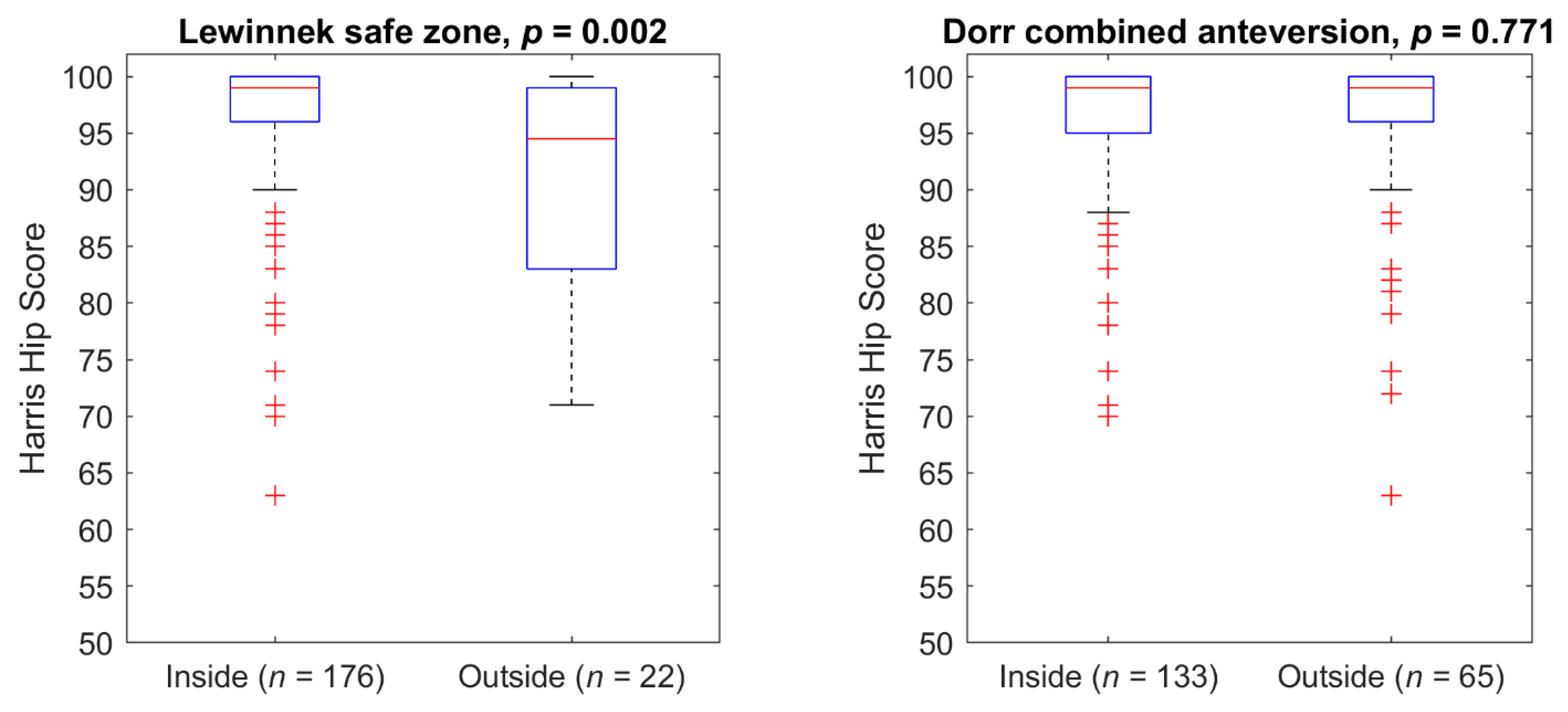
| Lewinnek safe zone | 176 | HHS | 99 (63, 100) | 20 | 22 | HHS | 95 (71, 100) | 50 | 0.002 |
| Age | 62 (34, 91) | Age | 70 (54, 85) | 0.000 | |||||
| Dorr combined anteversion | 133 | HHS | 99 (70, 100) | 24 | 65 | HHS | 99 (63, 100) | 23 | 0.771 |
| Age | 63 (34, 87) | Age | 62 (38, 91) | 0.600 | |||||
| Patient-specific target zones | |||||||||
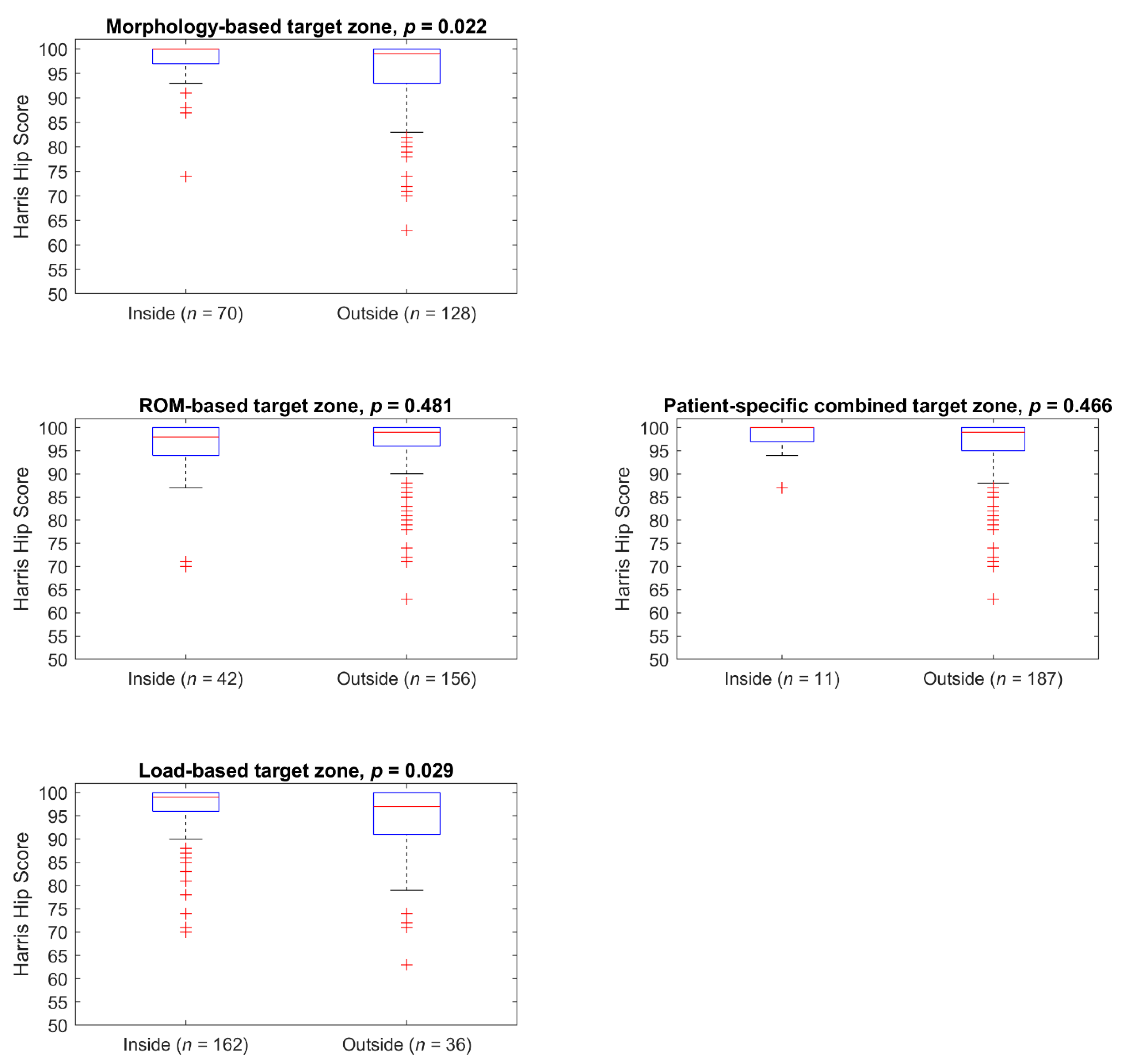
| Morphology-based | 70 | HHS | 100 (74, 100) | 14 | 128 | HHS | 99 (63, 100) | 29 | 0.022 |
| Age | 62 (38, 87) | Age | 63 (34, 91) | 0.256 | |||||
| ROM-based | 42 | HHS | 98 (70, 100) | 26 | 156 | HHS | 99 (63, 100) | 23 | 0.481 |
| Age | 67 (51, 82) | Age | 63 (34, 91) | 0.110 | |||||
| Load-based | 162 | HHS | 99 (70, 100) | 20 | 36 | HHS | 97 (63, 100) | 39 | 0.029 |
| Age | 62 (34, 87) | Age | 70 (38, 91) | 0.008 | |||||
| PSCTZ | 11 | HHS | 100 (87, 100) | 18 | 187 | HHS | 99 (63, 100) | 24 | 0.466 |
| Age | 62 (52, 82) | Age | 63 (34, 91) | 0.972 | |||||
| Criterion | Median (Q1 to Q3, Min. to Max.) | Mean ± SD |
|---|---|---|
| Cup coverage (%) | 79.6 (72.0 to 86.6, 49.8 to 97.7) | 78.7 ± 9.8 |
| Max. Anterior cup overhang (mm) | 9.1 (4.4 to 14.8, 0.0 to 38.5) | 9.9 ± 7.2 |
| Distance prior to cup penetration (mm) | 2.0 (0.4 to 3.7, −4.5 to 9.1) | 2.0 ± 2.6 |
| Leg length discrepancy (mm) | 0.8 (−3.8 to 5.2, −48.1 to 27.0) | 0.8 ± 8.4 |
| Distance to prosthetic impingement (°) | −0.4 (−4.1 to 2.2, −17.1 to 10.6) | −1.1 ± 5.1 |
| Decrease of bony ROM (°) | 0.6 (−4.6 to 6.3, −32.7 to 18.3) | −0.2 ± 8.9 |
| Min. distance to edge loading (°) | 5.6 (1.6 to 8.7, −14.9 to 21.6) | 5.1 ± 6.3 |
| Decrease of the resulting hip force (%BW) | −0.6 (−1.0 to −0.3, −8.7 to 2.4) | −0.7 ± 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habor, J.; Fischer, M.C.M.; Tokunaga, K.; Okamoto, M.; Radermacher, K. The Patient-Specific Combined Target Zone for Morpho-Functional Planning of Total Hip Arthroplasty. J. Pers. Med. 2021, 11, 817. https://doi.org/10.3390/jpm11080817
Habor J, Fischer MCM, Tokunaga K, Okamoto M, Radermacher K. The Patient-Specific Combined Target Zone for Morpho-Functional Planning of Total Hip Arthroplasty. Journal of Personalized Medicine. 2021; 11(8):817. https://doi.org/10.3390/jpm11080817
Chicago/Turabian StyleHabor, Juliana, Maximilian C. M. Fischer, Kunihiko Tokunaga, Masashi Okamoto, and Klaus Radermacher. 2021. "The Patient-Specific Combined Target Zone for Morpho-Functional Planning of Total Hip Arthroplasty" Journal of Personalized Medicine 11, no. 8: 817. https://doi.org/10.3390/jpm11080817
APA StyleHabor, J., Fischer, M. C. M., Tokunaga, K., Okamoto, M., & Radermacher, K. (2021). The Patient-Specific Combined Target Zone for Morpho-Functional Planning of Total Hip Arthroplasty. Journal of Personalized Medicine, 11(8), 817. https://doi.org/10.3390/jpm11080817