
Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review



Abstract
:1. Introduction
Background and Purpose
2. Materials and Methods
2.1. Background and Purpose
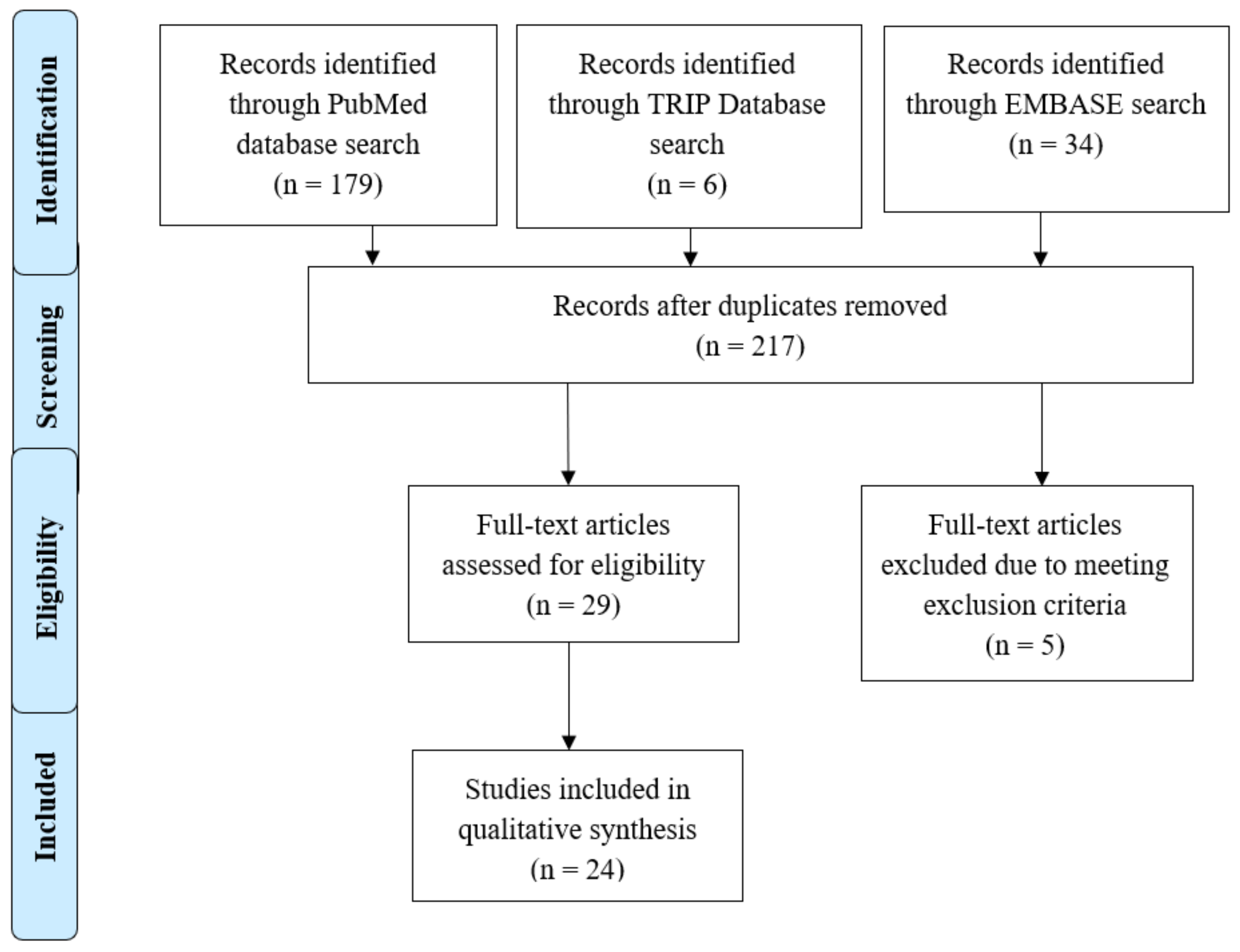
2.2. Database Identification and Selection
2.3. Selection of Studies
2.4. Data Extraction and Synthesis
- Author/year;
- Aims and purpose of the study;
- Number of participants tested;
- Number of patients surveyed or interviewed following genetic testing;
- Adult and/or pediatric population;
- Age range of participants;
- Gender (% females tested);
- Geographic region/location;
- Reporting of race or ethnicity;
- Disease;
- Genes or alleles examined;
- PRO/PROM instrument used (i.e., study design and data collection methods);
- PRO themes reported.
2.5. Assessment of Methodological Quality
3. Results
3.1. Article Characteristics
3.2. Study and Participant Population Characteristics
3.3. PROs from Validated PROM Instruments
3.4. PROs from Validated Surveys
3.5. PROs from Qualitative Studies and Studies with Unreported PRO Data Collection Methods
3.6. Overall CASP Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rotenstein, L.S.; Huckman, R.S.; Wagle, N.W. Making Patients and Doctors Happier—The Potential of Patient-Reported Outcomes. N. Engl. J. Med. 2017, 377, 1309–1312. [Google Scholar] [CrossRef]
- Deshpande, P.R.; Rajan, S.; Sudeepthi, B.L.; Abdul Nazir, C.P. Patient-Reported Outcomes: A New Era in Clinical Research. Perspect. Clin. Res. 2011, 2, 137–144. [Google Scholar] [CrossRef]
- STAT. The Future of Healthcare Requires a Direct Connection to Patients to Better Understand Their Lived Experiences. Available online: https://www.mdpi.com/2075-4426/10/4/264/htm (accessed on 16 July 2021).
- Kozma, C.M.; Reeder, C.E.; Schulz, R.M. Economic, Clinical, and Humanistic Outcomes: A Planning Model for Pharmacoeconomic Research. Clin. Ther. 1993, 15, 1121–1132; discussion 1120. [Google Scholar] [PubMed]
- Cella, D.; Hahn, E.A.; Jensen, S.E.; Butt, Z.; Nowinski, C.J.; Rothrock, N.; Lohr, K.N. Types of Patient-Reported Outcomes; Research Triangle Park (North Carolina, USA) RTI Press: Research Triangle, NC, USA, 2015. [Google Scholar]
- Kohler, J.N.; Turbitt, E.; Biesecker, B.B. Personal Utility in Genomic Testing: A Systematic Literature Review. Eur. J. Hum. Genet. 2017, 25, 662–668. [Google Scholar] [CrossRef]
- Tiller, J.; Morris, S.; Rice, T.; Barter, K.; Riaz, M.; Keogh, L.; Delatycki, M.B.; Otlowski, M.; Lacaze, P. Genetic Discrimination by Australian Insurance Companies: A Survey of Consumer Experiences. Eur. J. Hum. Genet. 2020, 28, 108–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunnik, E.M.; Janssens, A.C.J.W.; Schermer, M.H.N. Personal Utility in Genomic Testing: Is There Such a Thing? J. Med. Ethics 2015, 41, 322–326. [Google Scholar] [CrossRef]
- David, S.P.; Palaniappan, L. Clinical and Personal Utility of Genetic Risk Testing. AFP 2018, 97, 600–602. [Google Scholar]
- McAllister, M.; Dearing, A. Patient Reported Outcomes and Patient Empowerment in Clinical Genetics Services. Clin. Genet. 2015, 88, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Hendricks-Sturrup, R.M.; Clark-LoCascio, J.; Lu, C.Y. A Global Review on the Utility of Genetic Testing for Familial Hypercholesterolemia. J. Pers. Med. 2020, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Murray, M.F.; Evans, J.P.; Angrist, M.; Chan, K.; Uhlmann, W.R.; Doyle, D.L.; Fullerton, S.M.; Ganiats, T.G.; Hagenkord, J.; Imhof, S.; et al. A Proposed Approach for Implementing Genomics-Based Screening Programs for Healthy Adults. NAM Perspect. 2018, 1–16. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Seyedfatemi, N.; Salsali, M.; Rezaee, N.; Rahnavard, Z. Women’s Health Concept: A Meta-Synthesis Study. Iran. J. Public Health 2014, 43, 1335–1344. [Google Scholar]
- Fisher, E.R.; Pratt, R.; Esch, R.; Kocher, M.; Wilson, K.; Lee, W.; Zierhut, H.A. The Role of Race and Ethnicity in Views toward and Participation in Genetic Studies and Precision Medicine Research in the United States: A Systematic Review of Qualitative and Quantitative Studies. Mol. Genet. Genom. Med. 2020, 8, e1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.K.; Rahm, A.K.; Manickam, K.; Butry, L.; Lazzeri, A.; Corcoran, T.; Komar, D.; Josyula, N.S.; Pendergrass, S.A.; Sturm, A.C.; et al. Healthcare Utilization and Patients’ Perspectives After Receiving a Positive Genetic Test for Familial Hypercholesterolemia. Circ. Genom. Precis. Med. 2018, 11, e002146. [Google Scholar] [CrossRef]
- Pang, J.; Martin, A.C.; Bates, T.R.; Hooper, A.J.; Bell, D.A.; Burnett, J.R.; Norman, R.; Watts, G.F. Parent–Child Genetic Testing for Familial Hypercholesterolaemia in an Australian Context. J. Paediatr. Child Health 2018, 54, 741–747. [Google Scholar] [CrossRef]
- deWit, A.C.D.; Duivenvoorden, H.J.; Passchier, J.; Niermeijer, M.F.; Tibben, A. Course of Distress Experienced by Persons at Risk for an Autosomal Dominant Inheritable Disorder Participating in a Predictive Testing Program: An Explorative Study. Psychosom. Med. 1998, 60, 543–549. [Google Scholar] [CrossRef]
- Broadstock, M.; Michie, S.; Marteau, T. Psychological Consequences of Predictive Genetic Testing: A Systematic Review. Eur. J. Hum. Genet. 2000, 8, 731–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croyle, R.T.; Smith, K.R.; Botkin, J.R.; Baty, B.; Nash, J. Psychological Responses to BRCA1 Mutation Testing: Preliminary Findings. Health Psychol. 1997, 16, 63–72. [Google Scholar] [CrossRef]
- Beri, N.; Patrick-Miller, L.J.; Egleston, B.L.; Hall, M.J.; Domchek, S.M.; Daly, M.B.; Ganschow, P.; Grana, G.; Olopade, O.I.; Fetzer, D.; et al. Preferences for In-Person Disclosure: Patients Declining Telephone Disclosure Characteristics and Outcomes in the Multicenter Communication Of GENetic Test Results by Telephone Study. Clin. Genet. 2019, 95, 293–301. [Google Scholar] [CrossRef]
- Bradbury, A.R.; Egleston, B.L.; Patrick-Miller, L.J.; Rustgi, N.; Brandt, A.; Brower, J.; DiGiovanni, L.; Fetzer, D.; Berkelbach, C.; Long, J.M.; et al. Longitudinal Outcomes with Cancer Multigene Panel Testing in Previously Tested BRCA1/2 Negative Patients. Clin. Genet. 2020, 97, 601–609. [Google Scholar] [CrossRef]
- Esplen, M.J.; Wong, J.; Aronson, M.; Butler, K.; Rothenmund, H.; Semotiuk, K.; Madlensky, L.; Way, C.; Dicks, E.; Green, J.; et al. Long-Term Psychosocial and Behavioral Adjustment in Individuals Receiving Genetic Test Results in Lynch Syndrome. Clin. Genet. 2015, 87, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Hallowell, N.; Foster, C.; Eeles, R.; Ardern-Jones, A.; Watson, M. Accommodating Risk: Responses to BRCA1/2 Genetic Testing of Women Who Have Had Cancer. Soc. Sci. Med. 2004, 59, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Hughes Halbert, C.H.; Stopfer, J.E.; McDonald, J.; Weathers, B.; Collier, A.; Troxel, A.B.; Domchek, S. Long-Term Reactions to Genetic Testing for BRCA1 and BRCA2 Mutations: Does Time Heal Women’s Concerns? J. Clin. Oncol. 2011, 29, 4302–4306. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-C.; Bernhardt, B.A.; Helzlsouer, K.J. Utilization of BRCA1/2 Genetic Testing in the Clinical Setting. Cancer 2002, 94, 1876–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerman, C. BRCA1 Testing in Families With Hereditary Breast-Ovarian Cancer: A Prospective Study of Patient Decision Making and Outcomes. JAMA 1996, 275, 1885. [Google Scholar] [CrossRef]
- Lerman, C.; Hughes, C.; Lemon, S.J.; Main, D.; Snyder, C.; Durham, C.; Narod, S.; Lynch, H.T. What You Don’t Know Can Hurt You: Adverse Psychologic Effects in Members of BRCA1-Linked and BRCA2-Linked Families Who Decline Genetic Testing. J. Clin. Oncol. 1998, 16, 1650–1654. [Google Scholar] [CrossRef]
- Luba, D.G.; DiSario, J.A.; Rock, C.; Saraiya, D.; Moyes, K.; Brown, K.; Rushton, K.; Ogara, M.M.; Raphael, M.; Zimmerman, D.; et al. Community Practice Implementation of a Self-Administered Version of PREMM1,2,6 to Assess Risk for Lynch Syndrome. Clin. Gastroenterol. Hepatol. 2018, 16, 49–58. [Google Scholar] [CrossRef] [Green Version]
- MacLeod, R.; Beach, A.; Henriques, S.; Knopp, J.; Nelson, K.; Kerzin-Storrar, L. Experiences of Predictive Testing in Young People at Risk of Huntington’s Disease, Familial Cardiomyopathy or Hereditary Breast and Ovarian Cancer. Eur. J. Hum. Genet. 2014, 22, 396–401. [Google Scholar] [CrossRef] [Green Version]
- Mallen, A.R.; Conley, C.C.; Fuzzell, L.; Ketcher, D.; Augusto, B.M.; McIntyre, M.; Barton, L.V.; Townsend, M.K.; Fridley, B.L.; Tworoger, S.S.; et al. “I Think That a Brief Conversation from Their Provider Can Go a Very Long Way”: Patient and Provider Perspectives on Barriers and Facilitators of Genetic Testing after Ovarian Cancer. Support Care Cancer 2021, 29, 2663–2677. [Google Scholar] [CrossRef]
- Manchanda, R.; Burnell, M.; Gaba, F.; Desai, R.; Wardle, J.; Gessler, S.; Side, L.; Sanderson, S.; Loggenberg, K.; Brady, A.F.; et al. Randomised Trial of Population-Based BRCA Testing in Ashkenazi Jews: Long-Term Outcomes. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 364–375. [Google Scholar] [CrossRef] [Green Version]
- Meiser, B.; Quinn, V.F.; Mitchell, G.; Tucker, K.; Watts, K.J.; Rahman, B.; Peate, M.; Saunders, C.; Geelhoed, E.; Gleeson, M.; et al. Psychological Outcomes and Surgical Decisions after Genetic Testing in Women Newly Diagnosed with Breast Cancer with and without a Family History. Eur. J. Hum. Genet. 2018, 26, 972–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mella, S.; Muzzatti, B.; Dolcetti, R.; Annunziata, M.A. Emotional Impact on the Results of BRCA1 and BRCA2 Genetic Test: An Observational Retrospective Study. Hered. Cancer Clin. Pract. 2017, 15, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmquist, A.E.L.; Koehly, L.M.; Peterson, S.K.; Shegog, M.; Vernon, S.W.; Gritz, E.R. “The Cancer Bond”: Exploring the Formation of Cancer Risk Perception in Families with Lynch Syndrome. J. Genet. Couns. 2010, 19, 473–486. [Google Scholar] [CrossRef] [Green Version]
- Schneider, J.L.; Goddard, K.A.B.; Muessig, K.R.; Davis, J.V.; Rope, A.F.; Hunter, J.E.; Peterson, S.K.; Acheson, L.S.; Syngal, S.; Wiesner, G.L.; et al. Patient and Provider Perspectives on Adherence to and Care Coordination of Lynch Syndrome Surveillance Recommendations: Findings from Qualitative Interviews. Hered. Cancer Clin. Pract. 2018, 16, 11. [Google Scholar] [CrossRef] [Green Version]
- Underhill-Blazey, M.; Blonquist, T.; Chittenden, A.; Pozzar, R.; Nayak, M.; Lansang, K.; Hong, F.; Garber, J.; Stopfer, J.E. Informing Models of Cancer Genetics Care in the Era of Multigene Panel Testing with Patient-Led Recommendations. J. Genet. Couns. 2020, 30, 268–282. [Google Scholar] [CrossRef] [PubMed]
- Voorwinden, J.S.; Jaspers, J.P.C.; ter Beest, J.; Kievit, Y.; Sijmons, R.H.; Oosterwijk, J.C. The Introduction of a Choice to Learn Pre-Symptomatic DNA Test Results for BRCA or Lynch Syndrome Either Face-to-Face or by Letter. Clin. Genet. 2012, 81, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Werner-Lin, A.; Hoskins, L.M.; Doyle, M.H.; Greene, M.H. ‘Cancer Doesn’t Have an Age’: Genetic Testing and Cancer Risk Management in BRCA1/2 Mutation-Positive Women Aged 18–24. Health 2012, 16, 636–654. [Google Scholar] [CrossRef]
- Patrick-Miller, L.; Egleston, B.L.; Daly, M.; Stevens, E.; Fetzer, D.; Forman, A.; Bealin, L.; Rybak, C.; Peterson, C.; Corbman, M.; et al. Implementation and Outcomes of Telephone Disclosure of Clinical BRCA1/2 Test Results. Patient Educ. Couns. 2013, 93, 413–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieterse, A.H.; van Dulmen, A.M.; Beemer, F.A.; Bensing, J.M.; Ausems, M.G.E.M. Cancer Genetic Counseling: Communication and Counselees’ Post-Visit Satisfaction, Cognitions, Anxiety, and Needs Fulfillment. J. Genet. Couns. 2007, 16, 85–96. [Google Scholar] [CrossRef] [Green Version]
- Bradbury, A.R.; Patrick-Miller, L.J.; Egleston, B.L.; DiGiovanni, L.; Brower, J.; Harris, D.; Stevens, E.M.; Maxwell, K.N.; Kulkarni, A.; Chavez, T.; et al. Patient Feedback and Early Outcome Data with a Novel Tiered-Binned Model for Multiplex Breast Cancer Susceptibility Testing. Genet. Med. 2016, 18, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Underhill-Blazey, M.; Stopfer, J.; Chittenden, A.; Nayak, M.M.; Lansang, K.; Lederman, R.; Garber, J.; Gundersen, D.A. Development and Testing of the KnowGene Scale to Assess General Cancer Genetic Knowledge Related to Multigene Panel Testing. Patient Educ. Couns. 2019, 102, 1558–1564. [Google Scholar] [CrossRef]
- Dobrozsi, S.; Panepinto, J. Patient-Reported Outcomes in Clinical Practice. Hematol. Am. Soc. Hematol. Educ. Program Book 2015, 2015, 501–506. [Google Scholar] [CrossRef] [Green Version]
- Victorson, D. Patient Reported Outcomes (PROs) Tools for Measurement of Health Related Quality of Life|National Institute of Dental and Craniofacial Research. Available online: https://www.nidcr.nih.gov/grants-funding/grant-programs/behavioral-social-sciences-research-program/patient-reported-outcomes-tools-for-measurement-of-health-related-quality-of-life (accessed on 16 July 2021).
- PROMIS. Available online: https://www.healthmeasures.net/explore-measurement-systems/promis?AspxAutoDetectCookieSup=%27 (accessed on 16 July 2021).
- PROMs Lists|Australian Commission on Safety and Quality in Health Care. Available online: https://www.safetyandquality.gov.au/our-work/indicators-measurement-and-reporting/patient-reported-outcomes/proms-lists (accessed on 16 July 2021).
- A Roadmap for Developing Study Endpoints in Real-World Settings. Available online: https://healthpolicy.duke.edu/publications/roadmap-developing-study-endpoints-real-world-settings (accessed on 16 July 2021).
- Garrison, L.P.; Neumann, P.J.; Erickson, P.; Marshall, D.; Mullins, C.D. Using Real-World Data for Coverage and Payment Decisions: The ISPOR Real-World Data Task Force Report. Value Health 2007, 10, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulini, A.A.; Caetano, G.M.; Clautiaux, H.; Vergeron, L.; Pitts, P.J.; Katz, G. Impact of Real-World Data on Market Authorization, Reimbursement Decision & Price Negotiation. Innov. Regul. Sci. 2021, 55, 228–238. [Google Scholar] [CrossRef]
- Basch, E.; Barbera, L.; Kerrigan, C.L.; Velikova, G. Implementation of Patient-Reported Outcomes in Routine Medical Care. Am. Soc. Clin. Oncol. Educ. Book 2018, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Hendricks-Sturrup, R. Patient-Reported Outcomes: A Privacy-Centric and Federated Approach to Machine Learning. HSYS 2020. Available online: https://drive.google.com/file/d/1Ep3-CX8hI38-1RSjGdfEezPZGq1txi3q/view?usp=sharing (accessed on 16 July 2021).
- Kothari, C.; Wack, M.; Hassen-Khodja, C.; Finan, S.; Savova, G.; O’Boyle, M.; Bliss, G.; Cornell, A.; Horn, E.J.; Davis, R.; et al. Phelan-McDermid Syndrome Data Network: Integrating Patient Reported Outcomes with Clinical Notes and Curated Genetic Reports. Am. J. Med Genet. Part B Neuropsychiatr. Genet. 2018, 177, 613–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bargon, C.A.; Batenburg, M.C.T.; van Stam, L.E.; Mink van der Molen, D.R.; van Dam, I.E.; van der Leij, F.; Baas, I.O.; Ernst, M.F.; Maarse, W.; Vermulst, N.; et al. Impact of the COVID-19 Pandemic on Patient-Reported Outcomes of Breast Cancer Patients and Survivors. JNCI Cancer Spectr. 2021, 5, pkaa104. [Google Scholar] [CrossRef] [PubMed]
- Baffert, K.-A.; Darbas, T.; Lebrun-Ly, V.; Pestre-Munier, J.; Peyramaure, C.; Descours, C.; Mondoly, M.; Latrouite, S.; Bignon, E.; Nicouleau, S.; et al. Quality of Life of Patients With Cancer During the COVID-19 Pandemic. Vivo 2021, 35, 663–670. [Google Scholar] [CrossRef]


{kind=link}
| PRO Category | Main Characteristics | Main Strengths | Main Limitations |
|---|---|---|---|
| Health-related quality of life (HRQL) | - Is multidimensional - Can be generic or condition-specific | - Yields a global summary of well-being | - May not be considered a sufficiently specific construct |
| Functional status | - Reflects ability to perform specific activities | - Can be used in addition to performance-based measures of function | - May reflect variations in self-reported capability and actual performance of activities |
| Symptoms and symptom burden | - Are specific to type of symptom of interest - May identify symptoms not otherwise captured by medical workup | - Are best assessed through self-report | - May fail to capture general, global aspects of well-being considered important to patients |
| Health behaviors | - Are specific to type of behavior - Typically measure frequency of behavior | - Target specific behavior categories | - Validity may be affected by social desirability - May produce potential patient discomfort in reporting socially undesirable behaviors |
| Patient Experience | - Concerns satisfaction with health care delivery, treatment recommendations, and medications (or other therapies) - Reflects actual experiences with health care services- Fosters patient activation | - Is an essential component of patient-centered care - Is valued by patients, families, and policymakers - Relates to treatment adherence - Relates to health behaviors and health outcomes | - May be a complex, multidimensional construct - Requires confidentiality to ensure patient comfort in disclosing negative experiences - Does not provide sufficient evidence that activation enhances health care decision making |
| Study ID | Country | Genetic Disease Focus | Qualitative/ Quantitative/ Mixed Methods |
|---|---|---|---|
| Beri et al. (2019) [21] | USA | Breast and ovarian cancer | Quantitative |
| Bradbury et al. (2020) [22] | USA | Breast and ovarian cancer | Quantitative |
| Croyle et al. (1997) [20] | USA | Breast and ovarian cancer | Quantitative |
| deWit et al. (1998) [18] | Netherlands | Breast and ovarian cancer | Quantitative |
| Esplen et al. (2015) [23] | Canada | Lynch syndrome | Quantitative |
| Hallowell et al. (2004) [24] | UK | Breast and ovarian cancer | Qualitative |
| Hughes Halbert et al. (2011) [25] | USA | Breast and ovarian cancer | Quantitative |
| Jones et al. (2018) [16] | USA | Familial hypercholesterolemia | Qualitative |
| Lee et al. (2002) [26] | USA | Breast and ovarian cancer | Not Reported |
| Lerman et al. (1996) [27] | USA | Breast and ovarian cancer | Mixed methods |
| Lerman et al. (1998) [28] | Canada/USA | Breast and ovarian cancer | Mixed methods |
| Luba et al. (2018) [29] | USA | Lynch syndrome | Quantitative |
| MacLeod et al. (2014) [30] | UK | Breast and ovarian cancer | Qualitative |
| Mallen et al. (2021) [31] | USA | Breast and ovarian cancer | Qualitative |
| Manchanda et al. (2019) [32] | UK | Breast and ovarian cancer | Quantitative |
| Meiser et al. (2018) [33] | Australia | Breast and ovarian cancer | Quantitative |
| Mella et al. (2017) [34] | Italy | Breast and ovarian cancer | Quantitative |
| Palmquist et al. (2010) [35] | USA | Lynch Syndrome | Qualitative |
| Pang et al. (2018) [17] | Australia | Familial hypercholesterolemia | Not reported |
| Schneider et al. (2018) [36] | USA | Lynch syndrome | Qualitative |
| Tiller et al. (2020) [7] | Australia | Lynch syndrome Breast and ovarian cancer | Mixed methods |
| Underhill-Blazey et al. (2020) [37] | USA | Breast, ovarian, and endometrial/uterine cancer | Mixed methods |
| Voorwinden et al. (2012) [38] | Netherlands | Lynch syndromeBreast and ovarian cancer | Quantitative |
| Werner-Lin et al. (2012) [39] | USA | Breast and ovarian cancer | Qualitative |
| Study ID | Genetic Disease | PROM Instrument Used |
|---|---|---|
| Beri et al. (2019) [21] | Breast and ovarian cancer | - Cancer Genetics Knowledge Scale - State-Trait Anxiety Inventory - Hospital Anxiety and Depression Scale - Impact of Event Scale - Multidimensional Impact of Cancer Risk Assessment |
| Croyle et al. (1997) | Breast and ovarian cancer | - State-Trait Anxiety Inventory - Impact of Event Scale |
| deWit et al. (1998) [18] | Breast and ovarian cancer | - Impact of Event Scale |
| Esplen et al. (2015) [23] | Lynch syndrome | - Center for Epidemiologic Studies for Depression Scale - State-Trait Anxiety Inventory - Impact of Event Scale - Perception of Lifetime Risk for Colorectal Cancer - Colonoscopy Screening - Ways of Coping Questionnaire - Social Support Questionnaire - Quality of Life Index - Demographic and Medical Information Questionnaire |
| Hughes Halbert et al. (2011) [25] | Breast and ovarian cancer | - Multidimensional Impact of Cancer Risk Assessment |
| Lerman et al. (1996) [27] | Breast and ovarian cancer | - Center for Epidemiologic Studies for Depression Scale - Medical Outcomes Study |
| Lerman et al. (1998) [28] | Breast and ovarian cancer | - Center for Epidemiologic Studies for Depression Scale - Intrusion Subscale of the Revised Impact of Event Scale |
| Manchanda et al. (2019) [32] | Breast and ovarian cancer | - Hospital Anxiety and Depression Scale - Health Anxiety Inventory - Multidimensional Impact of Cancer Risk Assessment - SF12 questionnaire (Physical Health Component Scale and Mental Health Component Scale) |
| Meiser et al. (2018) [33] | Breast and ovarian cancer | - Impact of Event Scale - Hospital Anxiety and Depression Scale - Decision Regret Scale (genetic testing choice and surgery choice) |
| Mella et al. (2017) [34] | Breast and ovarian cancer | - Hospital Anxiety and Depression Scale - Profile of Mood States - Emotional Thermometers (ad hoc instrument) |
| Underhill-Blazey et al. (2020) [37] | Breast, ovarian, and endometrial/uterine cancer | - Multidimensional Impact of Cancer Risk Assessment |
| Voorwinden et al. (2012) [38] | Lynch syndrome Breast and ovarian cancer | - General Health Questionnaire-12 - Cancer Worry Scale |
| Study ID | Genetic Disease | Survey Measures |
|---|---|---|
| Beri et al. (2019) [21] | Breast and ovarian cancer | - Perceptions of genetic counseling and testing experience (Patrick-Miller et al. 2013 and Pieterse et al. 2007) [40,41] - Intent to utilize services (mammography, breast MRI, colonoscopy, prophylactic surgeries [e.g. mastectomy and oophorectomy]) |
| Bradbury et al. (2020) [22] | Breast and ovarian cancer | - Self-Regulation Theory of Health Behavior |
| Lerman et al. (1996) [27] | Breast and ovarian cancer | - Impact of receipt of BRCA1 test results on decisions about prophylactic mastectomy and prophylactic oophorectomy |
| Luba et al. (2018) [29] | Lynch syndrome | - Satisfaction |
| Meiser et al. (2018) [33] | Breast and ovarian cancer | - Test-Related Distress - Positive Experiences - Uptake of bilateral mastectomy or risk-reducing bilateral salpingo-oophorectomy |
| Underhill-Blazey et al. (2020) | Breast, ovarian, and endometrial/uterine cancer | - Genetic Counseling and Testing Satisfaction (Bradbury et al., 2016) [42] - KnowGene (Underhill-Blazey et al., 2019) [43] |
| Voorwinden et al. (2012) [38] | Lynch syndrome; Breast and ovarian cancer | - Knowledge - Risk perception - Decision-making |
| Study ID | Genetic Disease | Data Collection Method | PROs Reported |
|---|---|---|---|
| Hallowell et al. (2004) [24] | Breast and ovarian cancer | Qualitative interviews | - Reflecting on the past: the impact of a cancer diagnosis on self-identity - Looking to the future: genetic risk and identity - Accounting for the past and predicting the future: women’s motivations for undergoing genetic testing - Intrusion - Avoidance |
| Jones et al. (2018) [16] | FH | Qualitative interviews | - Understanding of FH (i.e., the inherited nature of FH) - Concerns about increased risk for heart attacks - Confusion and uncertainty for future medical care - Importance of genetic test results for family members. - Communicating with family members to understand family history of heart disease. - Feelings of shock from incidental genetic test findings (i.e., non-paternity) |
| Lee et al. (2002) [26] | Breast and ovarian cancer | Not reported | - Concern about insurance discrimination - Cost (free/self-pay/insurance) |
| Lerman et al. (1996) [27] | Breast and ovarian cancer | Telephone interview assessment | - Knowledge of genetic disease - Disbelief in cancer prevention - Worry about losing insurance coverage - Concern about accuracy of test results - Distrust in trust modern medicine - Curiosity about need for increased screening - Planning for the future for reassurance (i.e., making surgery and/or childbearing decisions, understanding children’s risk) - Poor emotional coping |
| MacLeod et al. (2014) [30] | Breast and ovarian cancer | Qualitative interviews | - Expecting to be gene-positive; preparing for possibility of bad news - Not a difficult decision; relieve uncertainty - Time for action; alter course of disease - Parental attitudes to testing; parental best interests at heart - Initial shock |
| Mallen et al. (2021) | Breast and ovarian cancer | Qualitative interviews | - Knowledge of genetic testing availability to learn disease risk - Beliefs and attitudes; inquiry and advocacy - Insurance coverage and out-of-pocket cost - Knowledge about genetic risks to self or family - Emotional reactions to the idea of learning about genetic risk may deter the pursuit of genetic testing - Positive appraisal; focusing on something favorable about their situation - Results not shared widely; shared only with a small immediate circle of close friends and family - Family impact of test results |
| Palmquist et al. (2010) [35] | Lynch Syndrome | Qualitative interviews | - Understanding the link between risk perception and cancer prevention - Understanding disease risk - Family history and cancer experiences in the formation of risk perception - Availability and accessibility to genetic testing |
| Pang et al. (2018) [17] | FH | Not reported | - Concern about the stigmatization of genetic testing - Reasons why parents did not provide consent for genetic testing: (i) wished children to make their own decision regarding testing after age 18 years; (ii) both parents could not reach unanimous decision |
| Schneider et al. (2018) [36] | Lynch syndrome | Qualitative interviews | - Facilitators and barriers to care coordination and receipt - Familiarity with Lynch syndrome and engagement with screening recommendations - Approach to and support with surveillance recommendations - Informing and communicating with family members - Appreciation for being able to inform family members - Relief - Gratitude - Regret - Fear - Feeling emotional |
| Tiller et al. (2020) [7] | Lynch syndrome; breast and ovarian cancer | Qualitative interviews | - Difficulty accessing insurance |
| Underhill-Blazey et al. (2020) [37] | Breast, ovarian, and endometrial/uterine cancer | Focus group interviews | - Genetic knowledge - Understanding complex genetic testing results - Communicate novel developments and recommendations to patients who receive a variant of unknown significance test result - Satisfaction - Preparing to communicate genetic test results to family members- Facilitating cascade testing (when necessary) - Psychosocial impact |
| Werner-Lin et al. (2012) [39] | Breast and ovarian cancer | Qualitative interviews | - Still learning - Feeling vulnerable to an impending cancer diagnosis and pressure to act before crossing a threshold into territory perceived as unsafe - Making active lifestyle choices to support healthy living since learning their mutation status - Navigating to and through genetic counseling and/or testing and risk management decision making - Actively seeking readily accessible resources to clarify and facilitate risk management |
| Study ID | Was There a Clear Statement of the Aims of the Research? | Is a Qualitative Methodology Appropriate? | Was the Research Design Appropriate to Address the Aims of The Research? | Was the Recruitment Strategy Appropriate to the Aims of The Research? | Were the Data Collected in a Way That Addressed the Research Issue? | Has the Relationship between Researcher and Participants Been Adequately Considered? | Have Ethical Issues Been Taken into Consideration? | Was the Data Analysis Sufficiently Rigorous? | Is There a Clear Statement of Findings? | How Valuable Is the Research? |
|---|---|---|---|---|---|---|---|---|---|---|
| Beri et al. (2019) [21] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Bradbury et al. (2020) [22] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Croyle et al. (1997) | Yes | No | Yes | Yes | Yes | Cannot Tell | Yes | Yes | Yes | Major |
| deWit et al. (1998) [18] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Esplen et al. (2015) [23] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Hallowell et al. (2004) [24] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Hughes Halbert et al. (2011) [25] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Jones et al. (2018) [16] | Yes | Yes | Cannot tell | Yes | Cannot tell | Yes | Yes | Yes | Yes | Major |
| Lee et al. (2002) [26] | Yes | Cannot tell | Cannot tell | Yes | Cannot tell | Yes | Yes | Cannot tell | Yes | Minor |
| Lerman et al. (1996) [27] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Lerman et al. (1998) [28] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Luba et al. (2018) [29] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| MacLeod et al. (2014) [30] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Mallen et al. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Manchanda et al. (2019) [32] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Meiser et al. (2018) [33] | Yes | No | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Major |
| Mella et al. (2017) [34] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Palmquist et al. (2010) [35] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Pang et al. (2018) [17] | Yes | Cannot tell | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Minor |
| Schneider et al. (2018) [36] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Tiller et al. (2020) [7] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Underhill-Blazey et al. (2020) [37] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Voorwinden et al. (2012) [38] | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Werner-Lin et al. (2012) [39] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Major |
| Study ID | Genetic Disease | Survey Measures |
|---|---|---|
| Beri et al. (2019) [21] | Breast and ovarian cancer | - Perceptions of genetic counseling and testing experience (Patrick-Miller et al. 2013 and Pieterse et al. 2007) [40,41] - Intent to utilize services (mammography, breast MRI, colonoscopy, prophylactic surgeries (e.g., mastectomy and oophorectomy)) |
| Bradbury et al. (2020) [22] | Breast and ovarian cancer | - Self-Regulation Theory of Health Behavior |
| Lerman et al. (1996) [27] | Breast and ovarian cancer | - Impact of receipt of BRCA1 test results on decisions about prophylactic mastectomy and prophylactic oophorectomy |
| Luba et al. (2018) [29] | Lynch syndrome | - Satisfaction |
| Meiser et al. (2018) [33] | Breast and ovarian cancer | - Test-related distress - Positive experiences - Uptake of bilateral mastectomy or risk-reducing bilateral salpingo-oophorectomy |
| Underhill-Blazey et al. (2020) [37] | Breast, ovarian, and endometrial/uterine cancer | - Genetic counseling and testing satisfaction (Bradbury et al., 2016) [42] - KnowGene (Underhill-Blazey et al., 2019) [43] |
| Voorwinden et al. (2012) [38] | Lynch syndrome; breast and ovarian cancer | - Knowledge - Risk perception - Decision-making |
| Validated Patient-Reported Outcome Measure Surveys | General Surveys | Qualitative Interviews and Focus Groups | Kohler et al. |
|---|---|---|---|
| Psychological, mood, emotional function or state (i.e., feelings of anxiety, depression, distress, regret, and worry) | Psychological and emotional feeling of intrusion, avoidance, shock, disbelief, distrust, curiosity, emotional coping, feeling emotional, psychosocial impact, relief, gratitude, regret, and fear | ||
| Knowledge and perceptions of their lifetime or genetic disease risk, uncertainty about managing their genetic disease risk, and health screening behaviors | Self-regulation and decision making (e.g., utilization of risk-mitigating procedures such as prophylactic surgery) Distress, knowledge, and risk perception | Genetic disease awareness and knowledge gain | Mental preparation Feelings of responsibility Value of information Knowledge of condition Self-knowledge Curiosity |
| Coping style or mechanisms, social functioning and support, quality of life, genetic testing satisfaction, functional health, and medical outcomes | Experience and satisfaction with the genetic testing process | Feelings of satisfaction or readiness about future personal and family communication and planning | To enhance coping Improved spiritual well-being Ability for future planning Reproductive autonomy Communication with relatives Change in social support |
| Concern about insurance discrimination and stigmatization Concern about cost of testing or care | Concern about discrimination and stigma Concern about privacy | ||
| Research altruism |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendricks-Sturrup, R.M.; Joseph, L.; Lu, C.Y. Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review. J. Pers. Med. 2021, 11, 850. https://doi.org/10.3390/jpm11090850
Hendricks-Sturrup RM, Joseph L, Lu CY. Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review. Journal of Personalized Medicine. 2021; 11(9):850. https://doi.org/10.3390/jpm11090850
Chicago/Turabian StyleHendricks-Sturrup, Rachele M., Lucson Joseph, and Christine Y. Lu. 2021. "Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review" Journal of Personalized Medicine 11, no. 9: 850. https://doi.org/10.3390/jpm11090850
APA StyleHendricks-Sturrup, R. M., Joseph, L., & Lu, C. Y. (2021). Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review. Journal of Personalized Medicine, 11(9), 850. https://doi.org/10.3390/jpm11090850