
Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Examinations
2.3. Diagnostic Criteria
2.4. Statistical Analysis
2.5. Machine Learning
3. Results
3.1. Participants’ Characteristics
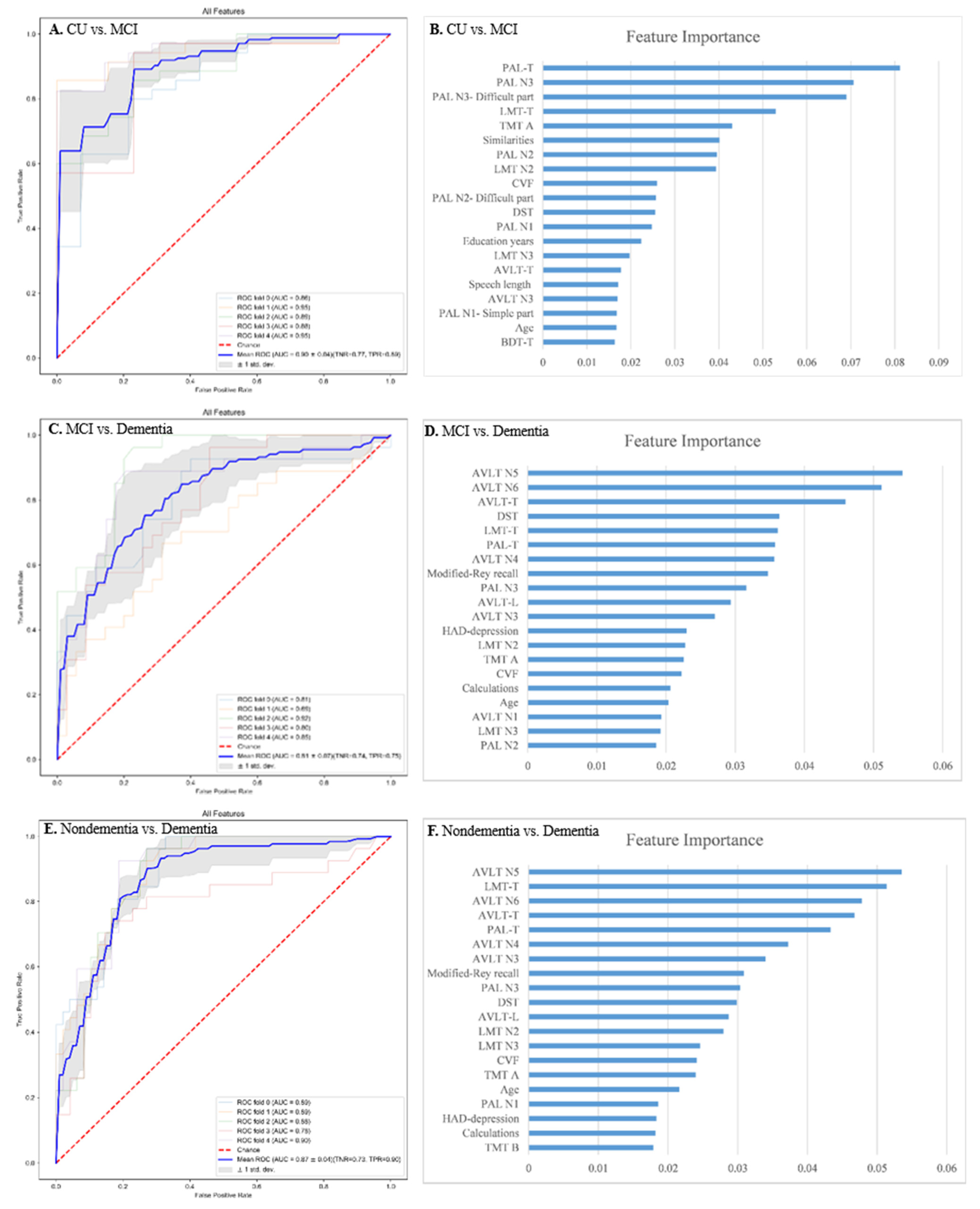
3.2. Assessment of Feature Importance
3.3. Performance of Various Classification Models
3.4. Selecting the Optimal Neuropsychological Tests to Establish Diagnostic Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Roberts, R.O.; Knopman, D.S.; Mielke, M.M.; Cha, R.H.; Pankratz, V.S.; Christianson, T.J.; Geda, Y.E.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology 2014, 82, 317–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olazarán, J.; Reisberg, B.; Clare, L.; Cruz, I.; Peña-Casanova, J.; Del Ser, T.; Woods, B.; Beck, C.; Auer, S.; Lai, C.; et al. Nonpharmacological Therapies in Alzheimer’s Disease: A Systematic Review of Efficacy. Dement. Geriatr. Cogn. Disord. 2010, 30, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 1, CD011145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 764–785. [Google Scholar] [CrossRef]
- Breton, A.; Casey, D.; Arnaoutoglou, N.A. Cognitive tests for the detection of mild cognitive impairment (MCI), the prodromal stage of dementia: Meta-analysis of diagnostic accuracy studies. Int. J. Geriatr. Psychiatry 2019, 34, 233–242. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Jia, J.; Yang, Z. Mini-Mental State Examination in Elderly Chinese: A Population-Based Normative Study. J. Alzheimer’s Dis. 2016, 53, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.P.; Li, N.; Gao, J.; Wang, L.-N.; Zhao, Y.-M.; Yu, B.-C.; Du, W.; Zhang, W.-J.; Cui, L.-Q.; Wang, Q.-S.; et al. Optimal Cutoff Scores for Dementia and Mild Cognitive Impairment of the Montreal Cognitive Assessment among Elderly and Oldest-Old Chinese Population. J. Alzheimer’s Dis. 2014, 43, 1403–1412. [Google Scholar] [CrossRef]
- Chiu, P.Y.; Tang, H.; Wei, C.Y.; Zhang, C.; Hung, G.U.; Zhou, W. NMD-12: A new machine-learning derived screening instrument to detect mild cognitive impairment and dementia. PLoS ONE 2019, 14, e0213430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davatzikos, C. Machine learning in neuroimaging: Progress and challenges. NeuroImage 2019, 197, 652–656. [Google Scholar] [CrossRef]
- Shigemizu, D.; Akiyama, S.; Asanomi, Y.; Boroevich, K.; Sharma, A.; Tsunoda, T.; Sakurai, T.; Ozaki, K.; Ochiya, T.; Niida, S. A comparison of machine learning classifiers for dementia with Lewy bodies using miRNA expression data. BMC Med. Genom. 2019, 12, 150. [Google Scholar] [CrossRef]
- Shehzad, A.; Rockwood, K.; Stanley, J.; Dunn, T.; Howlett, S.E. Use of Patient-Reported Symptoms from an Online Symptom Tracking Tool for Dementia Severity Staging: Development and Validation of a Machine Learning Approach. J. Med. Internet Res. 2020, 22, e20840. [Google Scholar] [CrossRef]
- Yim, D.; Yeo, T.Y.; Park, M.H. Mild cognitive impairment, dementia, and cognitive dysfunction screening using machine learning. J. Int. Med. Res. 2020, 48, 300060520936881. [Google Scholar] [CrossRef]
- Yilmaz, A.; Ustun, I.; Ugur, Z.; Akyol, S.; Hu, W.T.; Fiandaca, M.S.; Mapstone, M.; Federoff, H.; Maddens, M.; Graham, S.F. A Community-Based Study Identifying Metabolic Biomarkers of Mild Cognitive Impairment and Alzheimer’s Disease Using Artificial Intelligence and Machine Learning. J. Alzheimer’s Dis. 2020, 78, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Khatri, U.; Kwon, G.R. An Efficient Combination among sMRI, CSF, Cognitive Score, and APOE ε4 Biomarkers for Classification of AD and MCI Using Extreme Learning Machine. Comput. Intell. Neurosci. 2020, 2020, 8015156. [Google Scholar] [CrossRef] [PubMed]
- Bougea, A.; Efthymiopoulou, E.; Spanou, I.; Zikos, P. A Novel Machine Learning Algorithm Predicts Dementia with Lewy Bodies Versus Parkinson’s Disease Dementia Based on Clinical and Neuropsychological Scores. J. Geriatr. Psychiatry Neurol. 2021, 891988721993556. [Google Scholar] [CrossRef]
- Gurevich, P.; Stuke, H.; Kastrup, A.; Stuke, H.; Hildebrandt, H. Neuropsychological Testing and Machine Learning Distinguish Alzheimer’s Disease from Other Causes for Cognitive Impairment. Front. Aging Neurosci. 2017, 9, 114. [Google Scholar] [CrossRef]
- Zhang, Z.; Hong, X.; Li, H.; Zhao, J.H.; Huang, J.B.; Wei, J.; Wang, J.M.; Li, S.W.; Yang, E.L.; Wu, J.X. The mini-mental state examination in the Chinese residents population aged 55 years and over in the urban and rural areas of Beijing. Chin. J. Neurol. 1999, 32, 149–153. [Google Scholar]
- Katzman, R.; Zhang, M.Y.; Ouang, Y.Q.; Wang, Z.; Liu, W.T.; Yu, E.; Wong, S.-C.; Salmon, D.P.; Grant, I. A Chinese version of the mini-mental state examination; Impact of illiteracy in a Shanghai dementia survey. J. Clin. Epidemiol. 1988, 41, 971–978. [Google Scholar] [CrossRef]
- Xu, G.; Meyer, J.S.; Huang, Y.; Du, F.; Chowdhury, M.; Quach, M. Adapting Mini-Mental State Examination for dementia screening among illiterate or minimally educated elderly Chinese. Int. J. Geriatr. Psychiatry 2003, 18, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Yu, E.; He, Y. Tools for dementia epidemiological investigations and their applications. Shanghai Arch. Psychiatry 1995, 7, 1–62. [Google Scholar]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.S.; Poon, M.W. Performance of 7- to 95-year-old individuals in a Chinese version of the category fluency test. J. Int. Neuropsychol. Soc. 1999, 5, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y. Manual of Modified Wechsler Adult Intelligence Scale (WAIS-RC); Hunan Med College: Changsha, China, 1982; pp. 45–48. [Google Scholar]
- Gong, Y. The Chinese revision of Halstead-Reitan Neuropsychological Test Battery for Adults. Acta Psychol. Sin. 1986, 18, 433–442. [Google Scholar]
- Xu, S.; Wu, Z. The construction of “The Clinical Memory Test”. Acta Psychol. Sin. 1986, 18, 100–108. [Google Scholar]
- Gao, S.; Zhu, Y.; Shi, S.; Peng, Y. Standard Aphasia Battery of Chinese. Chin. Ment. Health J. 1992, 6, 125–128. [Google Scholar]
- Luria, A.R. Higher Cortical Functions in Man; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Fogel, B.S.; Schiffer, R.B.; Rao, S.M. Synopsis of Neuropsychiatry; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Gong, Y.; Jiang, D.; Deng, J. Manual of Modified Wechsler Memory Scale (WMS); Hunan Med College: Changsha, China, 1989; Volume 19. [Google Scholar]
- Guo, Q.H.; Sun, Y.T.; Yu, P.M.; Hong, Z.; Lv, C.Z. Norm of auditory verbal learning test in the normal aged in Chinese community. Chin. J. Clin. Psychol. 2007, 15, 132–135. [Google Scholar]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Friedman, T.W.; Yelland, G.W.; Robinson, S.R. Subtle cognitive impairment in elders with Mini-Mental State Examination scores within the ‘normal’ range. Int. J. Geriatr. Psychiatry 2011, 27, 463–471. [Google Scholar] [CrossRef]
- Votruba, K.L.; Persad, C.; Giordani, B. Cognitive Deficits in Healthy Elderly Population with “Normal” Scores on the Mini-Mental State Examination. J. Geriatr. Psychiatry Neurol. 2016, 29, 126–132. [Google Scholar] [CrossRef]
- Graham, S.A.; Lee, E.E.; Jeste, D.V.; Van Patten, R.; Twamley, E.W.; Nebeker, C.; Yamada, Y.; Kim, H.-C.; Depp, C.A. Artificial intelligence approaches to predicting and detecting cognitive decline in older adults: A conceptual review. Psychiatry Res. 2019, 284, 112732. [Google Scholar] [CrossRef] [Green Version]
- Battista, P.; Salvatore, C.; Castiglioni, I. Optimizing Neuropsychological Assessments for Cognitive, Behavioral, and Functional Impairment Classification: A Machine Learning Study. Behav. Neurol. 2017, 2017, 1850909. [Google Scholar] [CrossRef] [Green Version]
- Sarica, A.; Cerasa, A.; Quattrone, A. Random Forest Algorithm for the Classification of Neuroimaging Data in Alzheimer’s Disease: A Systematic Review. Front. Aging Neurosci. 2017, 9, 329. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Kleiman, M.J.; Barenholtz, E.; Galvin, J.E. Screening for Early-Stage Alzheimer’s Disease Using Optimized Feature Sets and Machine Learning. J. Alzheimer’s Dis. 2021, 81, 355–366. [Google Scholar] [CrossRef]
- Battista, P.; Salvatore, C.; Berlingeri, M.; Cerasa, A.; Castiglioni, I. Artificial intelligence and neuropsychological measures: The case of Alzheimer’s disease. Neurosci. Biobehav. Rev. 2020, 114, 211–228. [Google Scholar] [CrossRef]
- Lins, A.; Muniz, M.T.C.; Garcia, A.N.M.; Gomes, A.V.; Cabral, R.M.; Bastos-Filho, C.J.A. Using artificial neural networks to select the parameters for the prognostic of mild cognitive impairment and dementia in elderly individuals. Comput. Methods Programs Biomed. 2017, 152, 93–104. [Google Scholar] [CrossRef]
- Quintana, M.; Guàrdia, J.; Sánchez-Benavides, G.; Aguilar, M.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Antúnez, C.; Martínez-Parra, C.; García, A.F.; et al. Using artificial neural networks in clinical neuropsychology: High performance in mild cognitive impairment and Alzheimer’s disease. J. Clin. Exp. Neuropsychol. 2012, 34, 195–208. [Google Scholar] [CrossRef]
- Weakley, A.; Williams, J.A.; Schmitter-Edgecombe, M.; Cook, D.J. Neuropsychological test selection for cognitive impairment classification: A machine learning approach. J. Clin. Exp. Neuropsychol. 2015, 37, 899–916. [Google Scholar] [CrossRef] [Green Version]
- Tunvirachaisakul, C.; Supasitthumrong, T.; Tangwongchai, S.; Hemrunroj, S.; Chuchuen, P.; Tawankanjanachot, I.; Likitchareon, Y.; Phanthumchinda, K.; Sriswasdi, S.; Maes, M. Characteristics of Mild Cognitive Impairment Using the Thai Version of the Consortium to Establish a Registry for Alzheimer’s Disease Tests: A Multivariate and Machine Learning Study. Dement. Geriatr. Cogn. Disord. 2018, 45, 38–48. [Google Scholar] [CrossRef]
- Lv, S.; Wang, X.; Cui, Y.; Jin, J.; Sun, Y.; Tang, Y.; Bai, Y.; Wang, Y.; Zhou, L. Application of attention network test and demographic information to detect mild cognitive impairment via combining feature selection with support vector machine. Comput. Methods Programs Biomed. 2009, 97, 11–18. [Google Scholar] [CrossRef]
- Reverberi, C.; Cherubini, P.; Baldinelli, S.; Luzzi, S. Semantic fluency: Cognitive basis and diagnostic performance in focal dementias and Alzheimer’s disease. Cortex 2014, 54, 150–164. [Google Scholar] [CrossRef]
- Clark, D.G.; Kapur, P.; Geldmacher, D.S.; Brockington, J.; Harrell, L.; DeRamus, T.; Blanton, P.; Lokken, K.; Nicholas, A.; Marson, D. Latent information in fluency lists predicts functional decline in persons at risk for Alzheimer disease. Cortex 2014, 55, 202–218. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Lv, Y.; Zhou, Y.; Hong, Z.; Guo, Q. Short-Term Delayed Recall of Auditory Verbal Learning Test Is Equivalent to Long-Term Delayed Recall for Identifying Amnestic Mild Cognitive Impairment. PLoS ONE 2012, 7, e51157. [Google Scholar] [CrossRef]
- Yu, H.; Guo, Q.; Hong, Z.; Lv, C. Logic Memory Test in early detection of Alzheimer’s disease. Nerve Dis. Ment. Hygeine 2005, 5, 89–91. [Google Scholar]
- Curiel, R.E.; Crocco, E.; Rosado, M.; Duara, R.; Greig, M.T.; Raffo, A.; Loewenstein, D.A. A Brief Computerized Paired Associate Test for the Detection of Mild Cognitive Impairment in Community-Dwelling Older Adults. J. Alzheimer’s Dis. 2016, 54, 793–799. [Google Scholar] [CrossRef] [Green Version]
- Duchek, J.M.; Cheney, M.; Ferraro, F.R.; Storandt, M. Paired Associate Learning in Senile Dementia of the Alzheimer Type. Arch. Neurol. 1991, 48, 1038–1040. [Google Scholar] [CrossRef]
- Wang, L.; Nie, K.; Zhao, X.; Feng, S.; Xie, S.; He, X.; Ma, G.; Wang, L.; Huang, Z.; Huang, B.; et al. Characteristics of gray matter morphological change in Parkinson’s disease patients with semantic abstract reasoning deficits. Neurosci. Lett. 2018, 673, 85–91. [Google Scholar] [CrossRef]


{kind=link}
| Total n = 375 | CU n = 67 | MCI n = 174 | Dementia n = 134 | χ2/F a | Post Hoc Tests b,c | |
|---|---|---|---|---|---|---|
| Age (years) | 65.51 ± 11.46 | 63.24 ± 12.00 | 64.16 ± 11.61 | 68.41 ± 10.44 | 7.05 ** | 1 = 2 < 3 |
| Gender (% female) | 214 (57.1%) | 43 (64.2%) | 99 (56.9%) | 72 (53.7%) | 1.99 | - |
| Education years | 12.28 ± 3.91 | 13.88 ± 3.34 | 11.93 ± 3.98 | 11.96 ± 3.92 | 6.63 ** | 1 > 2 = 3 |
| MMSE | 27.80 ± 1.31 | 28.70 ± 1.17 | 27.95 ± 1.22 | 27.15 ± 1.17 | 40.42 ** | 1 > 2 > 3 |
| MoCA-P | 24.35 ± 3.08 | 27.18 ± 1.65 | 24.64 ± 2.77 | 22.54 ± 2.82 | 71.52 ** | 1 > 2 > 3 |
| ADL | 24.34 ± 4.57 | 21.78 ± 2.05 | 22.26 ± 2.53 | 28.31 ± 4.85 | 136.32 ** | 1 = 2 < 3 |
| IADL | 11.39 ± 3.30 | 9.45 ± 1.82 | 9.82 ± 1.99 | 14.39 ± 3.11 | 160.18 ** | 1 = 2 < 3 |
| BADL | 12.95 ± 1.92 | 12.33 ± 0.73 | 12.45 ± 1.01 | 13.93 ± 2.69 | 31.29 ** | 1 = 2 < 3 |
| HAD-anxiety | 4.66 ± 3.38 | 4.45 ± 3.15 | 4.48 ± 3.52 | 5.01 ± 3.29 | 1.06 | - |
| HAD-depression | 4.88 ± 3.48 | 4.50 ± 3.50 | 4.46 ± 3.44 | 5.64 ± 3.41 | 4.86 * | 1 = 2 < 3 |
| Accuracy | Precision | Recall | F1 Score | ROC-AUC | |
|---|---|---|---|---|---|
| Logistic Regression | 60.53 | 60.80 | 60.08 | 60.12 | 79.62 |
| Decision Tree | 59.73 | 60.48 | 60.86 | 60.21 | 69.55 |
| SVM | 62.40 | 65.37 | 59.29 | 61.17 | 80.87 |
| XGBoost | 66.40 | 67.78 | 66.15 | 66.70 | 81.61 |
| Random Forest | 68.00 | 71.09 | 66.73 | 68.02 | 85.17 |
| New Diagnosis Models | Subtests of Interest | Number of Features | ROC AUC for CU vs. MCI (Sensitivity, Specificity) | ROC AUC for MCI vs. Dementia (Sensitivity, Specificity) | ROC AUC for Dementia vs. Nondementia (Sensitivity, Specificity) |
|---|---|---|---|---|---|
| Model-1 | PAL, AVLT-H, Modified-Rey | 19 | 0.86 (0.79, 0.84) | 0.77 (0.68, 0.76) | 0.84 (0.72, 0.81) |
| Model-2 | PAL, AVLT-H, Modified-Rey, LMT | 20 | 0.87 (0.78, 0.84) | 0.79 (0.76, 0.66) | 0.83 (0.70, 0.83) |
| Model-3 | PAL, AVLT-H, Modified-Rey, LMT, DST | 21 | 0.87 (0.83, 0.84) | 0.79 (0.81, 0.65) | 0.84 (0.84, 0.71) |
| Model-4 | PAL, AVLT-H, Modified-Rey, LMT, DST, TMT A | 22 | 0.89 (0.92, 0.74) | 0.79 (0.84, 0.63) | 0.84 (0.85, 0.73) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Wang, Z.; Liu, N.; Liu, C.; Mao, C.; Dong, L.; Li, J.; Huang, X.; Lei, D.; Chu, S.; et al. Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores. J. Pers. Med. 2022, 12, 37. https://doi.org/10.3390/jpm12010037
Wang J, Wang Z, Liu N, Liu C, Mao C, Dong L, Li J, Huang X, Lei D, Chu S, et al. Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores. Journal of Personalized Medicine. 2022; 12(1):37. https://doi.org/10.3390/jpm12010037
Chicago/Turabian StyleWang, Jie, Zhuo Wang, Ning Liu, Caiyan Liu, Chenhui Mao, Liling Dong, Jie Li, Xinying Huang, Dan Lei, Shanshan Chu, and et al. 2022. "Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores" Journal of Personalized Medicine 12, no. 1: 37. https://doi.org/10.3390/jpm12010037
APA StyleWang, J., Wang, Z., Liu, N., Liu, C., Mao, C., Dong, L., Li, J., Huang, X., Lei, D., Chu, S., Wang, J., & Gao, J. (2022). Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores. Journal of Personalized Medicine, 12(1), 37. https://doi.org/10.3390/jpm12010037