
New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient


 ,
,  , , ,
, , , 
Abstract
:1. Introduction
1.1. Physiology of Lung Interstices and Alveolar, the Role of Local Regenerative Mechanisms
1.2. The Rationale Uses of Autologous Peripheral Blood Plasma and Stem Cells in COVID-19
2. Materials and Methods
The In Vivo Plasma Procedure
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keith, P.; Day, M.; Perkins, L.; Moyer, L.; Hewitt, K.; Wells, A. A novel treatment approach to the novel coronavirus: An argument for the use of therapeutic plasma exchange for fulminant COVID-19. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S.; et al. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, e1–e6. [Google Scholar] [CrossRef]
- Pham, V.H.; Gargiulo Isacco, C.; Nguyen, K.C.D.; Le, S.H.; Tran, D.K.; Nguyen, Q.V.; Pham, H.T.; Aityan, S.; Pham, S.T.; Cantore, S.; et al. Rapid and Sensitive Diagnostic Procedure for Multiple Detection of Pandemic Coronaviridae Family Members SARS-CoV-2, SARS-CoV, MERS-CoV and HCoV: A Translational Research and Cooperation between the Phan Chau Trinh University in Vietnam and University of Bari “Aldo Moro” in Italy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7173–7191. [Google Scholar] [CrossRef]
- Gargiulo, C.; Pham, V.H.; Hai, N.T.; Nguyen, K.C.D.; Kim, N.D.; Van, T.N.; Tuan, A.L.; Abe, K.; Flores, V.; Shiffman, M. Autologous Peripheral Blood Stem Cells and γ/δ T Cells May Improve Immunity in Treating Secondary Bacteremic Infection in HIV Infected Patient. Stem Cell Discov. 2015, 5, 48–61. [Google Scholar] [CrossRef] [Green Version]
- Tiberghien, P.; De Lamballerie, X.; Morel, P.; Gallian, P.; Lacombe, K.; Yazdanpanah, Y. Collecting and evaluating convalescent plasma for COVID-19 treatment: Why and how? Vox Sang. 2020, 115, 488–494. [Google Scholar] [CrossRef]
- Tanne, J.H. Covid-19: FDA approves use of convalescent plasma to treat critically ill patients. BMJ 2020, 368, m1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.-A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef]
- Charitos, I.A.; Del Prete, R.; Inchingolo, F.; Mosca, A.; Carretta, D.; Ballini, A.; Santacroce, L. What we have learned for the future about COVID-19 and healthcare management of it? Acta Bio Med. Atenei Parm. 2020, 91, e2020126. [Google Scholar] [CrossRef]
- Zhou, F.; Wang, Y.; Liu, Y.; Liu, X.; Gu, L.; Zhang, X.; Pu, Z.; Yang, G.; Liu, B.; Nie, Q.; et al. Disease severity and clinical outcomes of community-acquired pneumonia caused by non-influenza respiratory viruses in adults: A multicentre prospective registry study from the CAP-China Network. Eur. Respir. J. 2019, 54, 1802406. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Weibel, E.R. On the Tricks Alveolar Epithelial Cells Play to Make a Good Lung. Am. J. Respir. Crit. Care Med. 2015, 191, 504–513. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.; Barkauskas, C.E.; Takeda, N.; Bowie, E.; Aghajanian, H.; Wang, Q.; Padmanabhan, A.; Manderfield, L.J.; Gupta, M.; Li, D.; et al. Plasticity of Hopx+ type I alveolar cells to regenerate type II cells in the lung. Nat. Commun. 2015, 6, 1–11. [Google Scholar] [CrossRef]
- Flodby, P.; Li, C.; Liu, Y.; Wang, H.; Rieger, M.E.; Minoo, P.; Crandall, E.D.; Ann, D.K.; Borok, Z.; Zhou, B. Cell-specific expression of aquaporin-5 (Aqp5) in alveolar epithelium is directed by GATA6/Sp1 via histone acetylation. Sci. Rep. 2017, 7, 3473. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, M.I.; Millien, G.; Hinds, A.; Cao, Y.; Seldin, D.C.; Williams, M.C. T1α, a lung type I cell differentiation gene, is required for normal lung cell proliferation and alveolus formation at birth. Dev. Biol. 2003, 256, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, A.M.; Ingenito, E.P. Alveolar Epithelial Stem and Progenitor Cells: Emerging Evidence for their Role in Lung Regeneration. Curr. Med. Chem. 2012, 19, 6003–6008. [Google Scholar] [CrossRef] [PubMed]
- Chapman, H.A.; Li, X.; Alexander, J.P.; Brumwell, A.; Lorizio, W.; Tan, K.; Sonnenberg, A.; Wei, Y.; Vu, T.H. Integrin α6β4 identifies an adult distal lung epithelial population with regenerative potential in mice. J. Clin. Investig. 2011, 121, 2855–2862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tata, P.R.; Rajagopal, J. Plasticity in the lung: Making and breaking cell identity. Development 2017, 144, 755–766. [Google Scholar] [CrossRef] [Green Version]
- Mohammadipoor, A.; Antebi, B.; Batchinsky, A.I.; Cancio, L.C. Therapeutic potential of products derived from mesenchymal stem/stromal cells in pulmonary disease. Respir. Res. 2018, 19, 1–14. [Google Scholar] [CrossRef]
- Gargiulo, C.; Pham, V.H.; Nguyen, K.C.; Kim, N.D.; Van, T.N.; Tuan, A.L.; Abe, K.; Shiffman, M. Toxoplasmosis Gondii Infection and Diabetes Mellitus Type 2 Treated by Using Autologous Peripheral Blood Stem Cells a Unique Case Report of a Caucasian 83 Year Old Lady. Biomed. Res. Ther. 2015, 2, 1–8. [Google Scholar] [CrossRef]
- Gargiulo, C.; Pham, V.H. Human Peripheral Blood Stem Cells can be a Solution to Diabetes Mellitus Type 2 a Preliminary Study on 14 Patients. J. Stem Cell Res. Ther. 2016, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Levesque, J.-P.; Winkler, I.G. Mobilization of hematopoietic stem cells: State of the art. Curr. Opin. Organ Transplant. 2008, 13, 53–58. [Google Scholar] [CrossRef]
- Ye, J.; Lee, S.Y.; Kook, K.H.; Yao, K. Bone marrow-derived progenitor cells promote corneal wound healing following alkali injury. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 246, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzog, E.L.; Van Arnam, J.; Hu, B.; Zhang, J.; Chen, Q.; Haberman, A.M.; Krause, D.S. Lung-specific nuclear reprogramming is accompanied by heterokaryon formation and Y chromosome loss following bone marrow transplantation and secondary inflammation. FASEB J. 2007, 21, 2592–2601. [Google Scholar] [CrossRef]
- Pereira, C.-F.; Terranova, R.; Ryan, N.K.; Santos, J.; Morris, K.J.; Cui, W.; Merkenschlager, M.; Fisher, A.G. Heterokaryon-Based Reprogramming of Human B Lymphocytes for Pluripotency Requires Oct4 but Not Sox2. PLoS Genet. 2008, 4, e1000170. [Google Scholar] [CrossRef] [PubMed]
- Baj-Krzyworzeka, M.; Szatanek, R.; Węglarczyk, K.; Baran, J.; Urbanowicz, B.; Brański, P.; Ratajczak, M.Z.; Zembala, M. Tumour-derived microvesicles carry several surface determinants and mRNA of tumour cells and transfer some of these determinants to monocytes. Cancer Immunol. Immunother. 2005, 55, 808–818. [Google Scholar] [CrossRef]
- Ratajczak, J.; Wysoczynski, M.; Hayek, F.; Janowskawieczorek, A.; Ratajczak, M.Z. Membrane-derived microvesicles: Important and underappreciated mediators of cell-to-cell communication. Leukemia 2006, 20, 1487–1495. [Google Scholar] [CrossRef]
- Aliotta, J.M.; Sanchez-Guijo, F.M.; Dooner, G.J.; Johnson, K.W.; Dooner, M.S.; Greer, K.A.; Greer, D.; Pimentel, J.; Kolankiewicz, L.M.; Puente, N.; et al. Alteration of marrow cell gene expression, protein production and engraftment into lung by lung-derived microvesicles: A novel mechanism for phenotype modulation. Stem Cells 2007, 25, 2245–2256. [Google Scholar] [CrossRef] [Green Version]
- Castillo Aleman, Y.M.; Villegas Valverde, C.A.; Ventura Carmenate, Y.; Abdel Hadi, L.; Rivero Jimenez, R.A.; Rezgui, R.; Alagha, S.H.; Shamat, S.; Bencomo Hernandez, A.A. Viability assessment of human peripheral blood-derived stem cells after three methods of nebulization. Am. J. Stem Cells 2021, 10, 68–78. [Google Scholar]
- Gargiulo, C.; Pham, V.P.; Hai, N.T.; Nguyen, K.C.D.; Van Phuc, P.; Abe, K.; Flores, V.; Shiffman, M. Isolation and Characterization of Multipotent and Pluripotent Stem Cells from Human Peripheral Blood. Stem Cell Discov. 2015, 5, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Gargiulo Isacco, C.; Inchingolo, F.; Nguyen, C.D.K.; Aityan, S.K.; Pham, H.; Dipalma, G.; Ballini, A.; Strong, D.M.; Filgueira, L.; Tran, T.; et al. Aging and Metabolic Disorders, the Role of Molecular Mechanisms Leading to Bone Degeneration as a Possible Cause of Implant and Graft Loss: A Review (Book); SignPost: New York, USA, 2019; ISBN 978-81-308-0585-6. [Google Scholar]
- Balzanelli, G.M.; Distratis, P.; Amatulli, F.; Catucci, O.; Cefalo, A.; Lazzaro, R.; Palazzo, D.; Aityan, K.S.; Dipalma, G.; Inchingolo, F. Clinical Features in Predicting COVID-19. Biomed. J. Sci. Tech. Res. 2020, 29, 22921–22926. [Google Scholar] [CrossRef]
- Balzanelli, M.; Distratis, P.; Catucci, O.; Cefalo, A.; Lazzaro, R.; Inchingolo, F.; Tomassone, D.; Aityan, S.; Ballini, A.; Nguyen, K.; et al. Mesenchymal Stem Cells: The Secret Children’s Weapons against the SARS-CoV-2 Lethal Infection. Appl. Sci. 2021, 11, 1696. [Google Scholar] [CrossRef]
- Peng, H.; Gong, T.; Huang, X.; Sun, X.; Luo, H.; Wang, W.; Luo, J.; Luo, B.; Chen, Y.; Wang, X.; et al. A synergistic role of convalescent plasma and mesenchymal stem cells in the treatment of severely ill COVID-19 patients: A clinical case report. Stem Cell Res. Ther. 2020, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Charitos, I.A.; Ballini, A.; Bottalico, L.; Cantore, S.; Passarelli, P.C.; Inchingolo, F.; D’Addona, A.; Santacroce, L. Special Features of SARS-CoV-2 in Daily Practice. World J. Clin. Cases 2020, 8, 3920–3933. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-L.; Murakowski, D.K.; Bournazos, S.; Schoofs, T.; Sarkar, D.; Halper-Stromberg, A.; Horwitz, J.A.; Nogueira, L.; Golijanin, J.; Gazumyan, A.; et al. Enhanced clearance of HIV-1–infected cells by broadly neutralizing antibodies against HIV-1 in vivo. Science 2016, 352, 1001–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Li, J.; Qi, Y.; Zou, Y.; Liu, L.; Tang, X.; Duan, J.; Liu, H.; Zeng, G. Vitamin C promotes the proliferation of human adipose-derived stem cells via p53-p21 pathway. Organogenesis 2016, 12, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Ochiai-Shino, H.; Onodera, S.; Saito, A.; Shibahara, T.; Azuma, T. Promoting effect of 1,25(OH) 2 vitamin D 3 in osteogenic differentiation from induced pluripotent stem cells to osteocyte-like cells. Open Biol. 2015, 5, 140201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.; Cheng, H.; Gao, Y.; Shi, M.; Liu, Y.; Hu, Z.; Xu, J.; Qiu, L.; Yuan, W.; Leung, A.Y.-H.; et al. Antioxidant N-acetyl-l-cysteine increases engraftment of human hematopoietic stem cells in immune-deficient mice. Blood 2014, 124, e45–e48. [Google Scholar] [CrossRef] [Green Version]
- Wimalawansa, S.J. Vitamin D Deficiency: Effects on Oxidative Stress, Epigenetics, Gene Regulation, and Aging. Biology 2019, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afarid, M.; Sanie-Jahromi, F. Mesenchymal Stem Cells and COVID-19: Cure, Prevention, and Vaccination. Stem Cells Int. 2021, 2021, 1–12. [Google Scholar] [CrossRef]
- Wu, X.; Kwong, A.C.; Rice, C.M. Antiviral resistance of stem cells. Curr. Opin. Immunol. 2018, 56, 50–59. [Google Scholar] [CrossRef]
- Eggenberger, J.; Blanco-Melo, D.; Panis, M.; Brennand, K.J.; Tenoever, B.R. Type I interferon response impairs differentiation potential of pluripotent stem cells. Proc. Natl. Acad. Sci. USA 2019, 116, 1384–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The CBC Parameters at the Time of the Admission on 18 November 2020 | Clinical Laboratory Values |
| White cell count (WCC) | 11.66 (normal range 3.5–10) |
| Neutrophils | 89.6% (normal range 35–75) |
| Lymphocytes | 7.5% (normal range 20–55) |
| C-reactive Protein (CRP) | 80.4 mg/L (normal range up to 3.5) |
| Erythrocyte sedimentation rate (ESR) | 88 mm/h (normal range 1–10) |
| Fibrinogen | 643 mg/dL (normal range 200–400) |
| IL-6 | 66.9 pg/mL (normal range up to 3) |
| Vitamin D | 14.1 ng/mL (<30 insuff; 30–50 suff; >50–100 optimal) |
| The ABG Parameters (Arterial Blood Gas) 18 November 2020 | Clinical Laboratory Values |
| pH | 7.5 (normal range 7.35–7.45) |
| PaCO2 | 33 mmHg (normal range 35–45) |
| PaO2 | 65% mmHg (normal range 75–100) |
| FO2Hb | 93.4% (normal range 94–97) |
| Glucose | 119 mg/dL (normal range 80–115) |
| Lac | 1.24 mmol/L (normal range 0.50–2.00) |
| K+ | 3.43 mmol/L (normal range 3.5–5.3) |
| C++ | 1.10 mmol/L (normal range 1.12–1.32) |
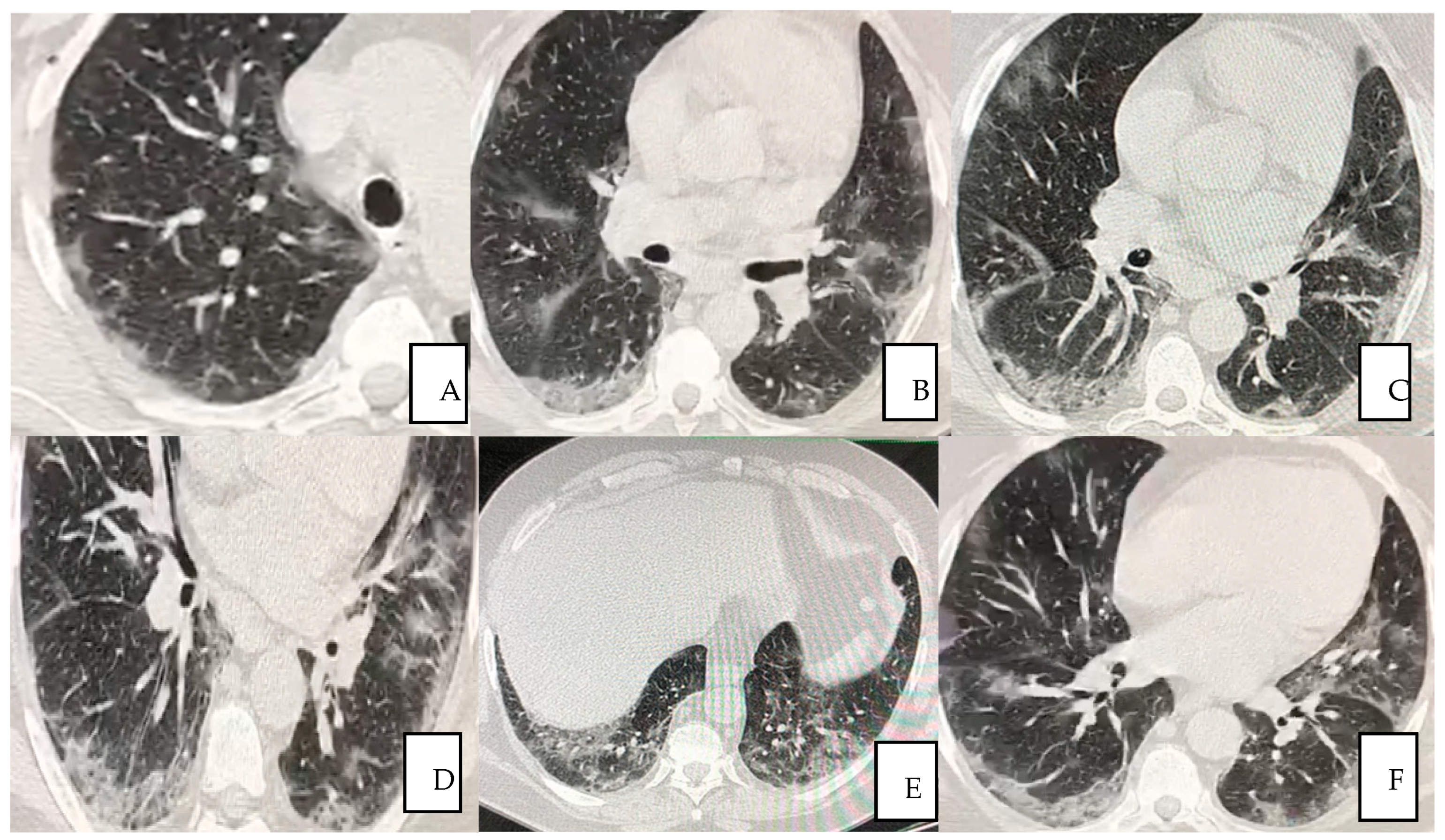
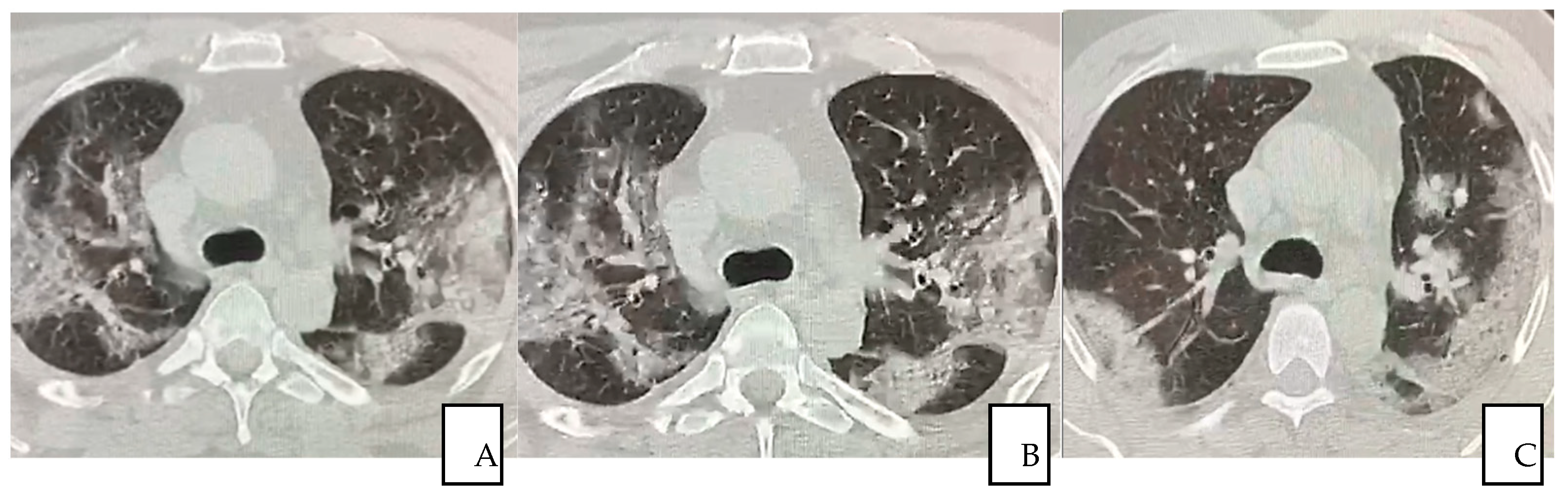
| Pulmonary High-resolution Computed tomography (HRCT) 18 November 2020 | Diagnosis |
| Positive with ground-glass opacities indicating a bilateral, multisegmental, mid-basal and interstitial involvement, suggestive of 35% injury of the total lung surface, as shown in Figure 1. |
| Home Oral Therapy | Drug Posology |
|---|---|
| Ramipril (ACE inhibitor) | 10 mg, 1 cpr day |
| Fleiderina (anti-atrial fibrillation) | 200 mg, 1 cpr day |
| Lobivon (anti-hypertension) | 5 mg, 1 cpr day |
| Hospital therapy | Timeline |
| Kcl retard (oral) 600 mg | from 18 to 25 November |
| Norvasc (oral) 5 mg 1 cp | from 20 November in replacing Lobivon |
| Clexane (ID) 6000 1 fl day | from 20 November to 1 December |
| Pantorc (IV) 40 mg 1 fl day | from 18 November to 1 December |
| Decadron (IV) 8 mg 1 fl × 2 | from 18 to 26 November |
| Decadron (IV) 4 mg 1 fl × 2 | from 27 November to 1 December |
| Rocefin (IV) 2 g 1 fl | from 18 November to 1 December |
| Veklury (IV) 100 mg 2 fl + S.F. 250 mL in 2 h | from 15 November to 19 November |
| Veklury (IV) 100 mg 1 fl + S.F. 250 mL in 2 h | from 20 November to 23 November |
| O2 in CPAP (peep 10 cm H2O) + FiO2 | O2 Supplementation (%) |
| 60% (day 18 November) 50% (days from 20 to 25 November) 40% (day from 26 to 29 November) On 30 November, O2 supplementation ended. |
| The CBC Parameters on Dismissing 1 December 2020 | Clinical Laboratory Values |
| White cell count (WCC) | 5.14 (normal range 3.5–10) |
| Neutrophils | 82.8% (normal range 35–75) |
| Lymphocytes | 711.02% (normal range 20–55) |
| C-reactive protein (CRP) | 2.9 mg/L (normal range up to 3.5) |
| Erythrocyte sedimentation rate (ESR) | 18 mm/h (normal range 1–10) |
| Fibrinogen | 458 mg/dL (normal range 200–400) |
| IL-6 | 2.7 pg/mL (normal range up to 3) |
| Vitamin D | 42.1 ng/mL (<30 insuff; 30–50 suff.; >50–100 optimal) |
| The ABG parameters (arterial blood gas) 1 December 2020 | Clinical Laboratory Values |
| pH | 7.4 (normal range 7.35–7.45) |
| PaCO2 | 35.8 mmHg (normal range 35–45) |
| PaO2 | 85 mmHg (normal range 75–100) |
| FO2Hb | 95.3% mg/dL (normal range 94–97) |
| Glucose | 240 mg/dL (normal range 80–115) |
| Lac | 3.38 mmol/L (normal range 0.50–2.00) |
| K+ | 3.80 mmol/L (normal range 3.5–5.3) |
| C++ | 1.23 mmol/L (normal range 1.12–1.32) |
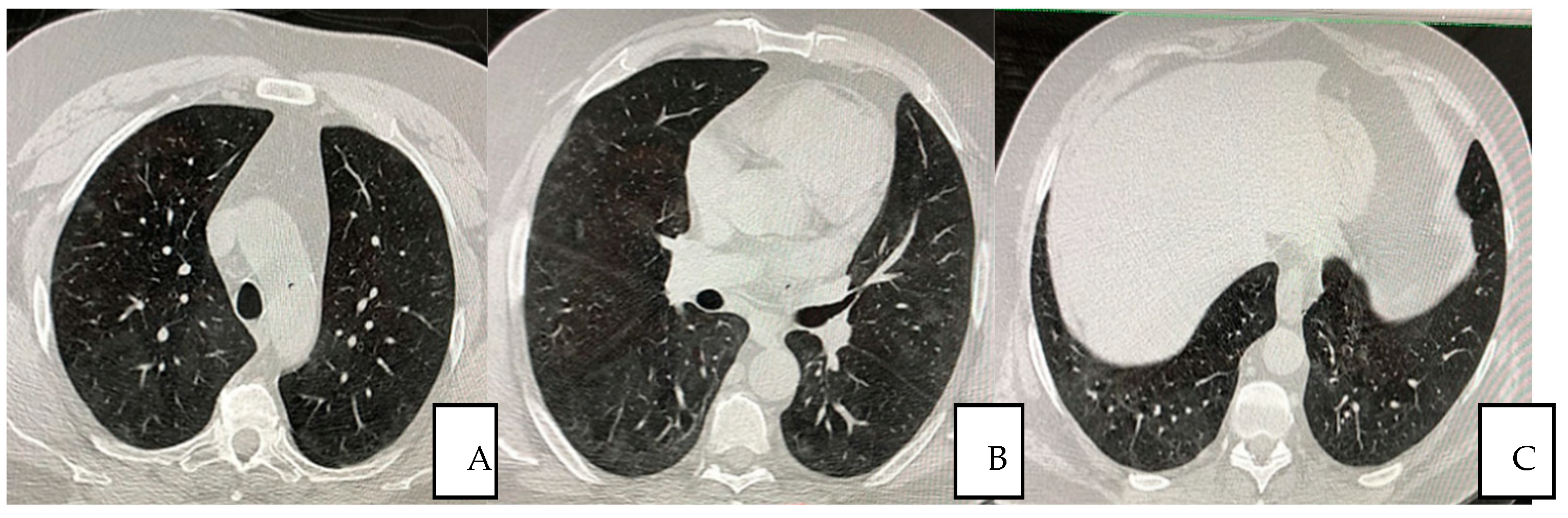
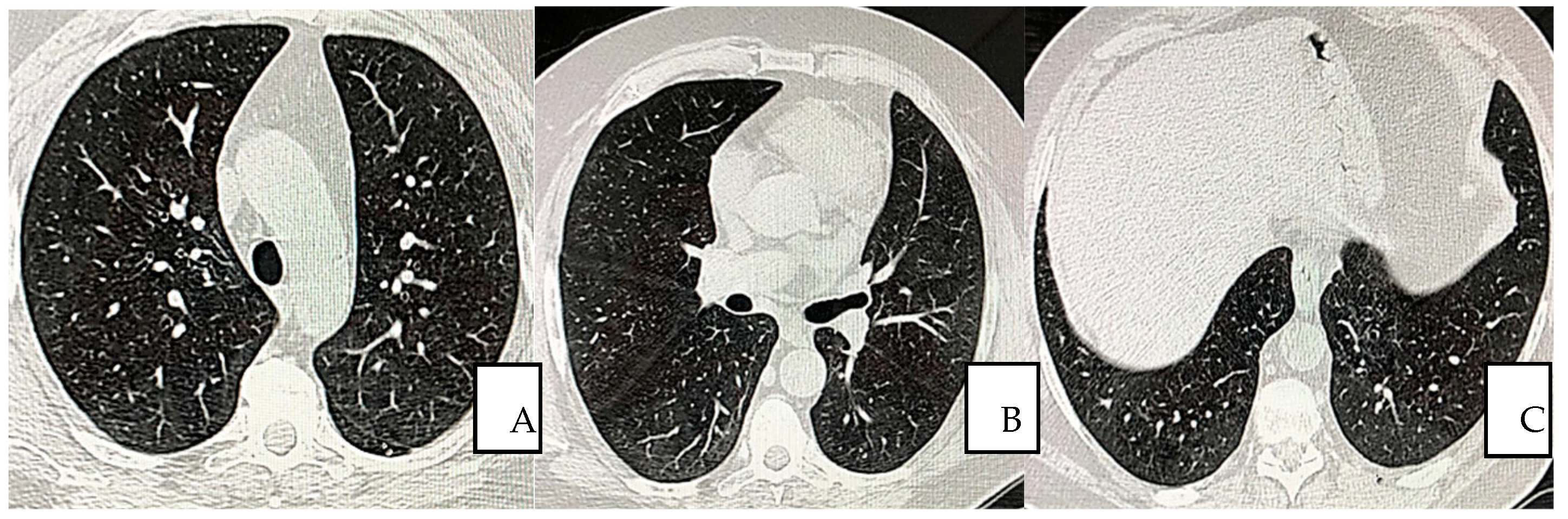
| Pulmonary HRCT 15 December 2020 | Diagnosis |
| In complete resolution any ground-glass opacities were seen indicating healing process of 98%. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; D’Ettorre, E.; Nico, A.; Inchingolo, F.; Dipalma, G.; Tomassone, D.; Serlenga, E.M.; Dalagni, G.; et al. New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient. J. Pers. Med. 2022, 12, 85. https://doi.org/10.3390/jpm12010085
Balzanelli MG, Distratis P, Lazzaro R, D’Ettorre E, Nico A, Inchingolo F, Dipalma G, Tomassone D, Serlenga EM, Dalagni G, et al. New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient. Journal of Personalized Medicine. 2022; 12(1):85. https://doi.org/10.3390/jpm12010085
Chicago/Turabian StyleBalzanelli, Mario Giosuè, Pietro Distratis, Rita Lazzaro, Ernesto D’Ettorre, Andrea Nico, Francesco Inchingolo, Gianna Dipalma, Diego Tomassone, Emilio Maria Serlenga, Giancarlo Dalagni, and et al. 2022. "New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient" Journal of Personalized Medicine 12, no. 1: 85. https://doi.org/10.3390/jpm12010085
APA StyleBalzanelli, M. G., Distratis, P., Lazzaro, R., D’Ettorre, E., Nico, A., Inchingolo, F., Dipalma, G., Tomassone, D., Serlenga, E. M., Dalagni, G., Ballini, A., Nguyen, K. C. D., & Isacco, C. G. (2022). New Translational Trends in Personalized Medicine: Autologous Peripheral Blood Stem Cells and Plasma for COVID-19 Patient. Journal of Personalized Medicine, 12(1), 85. https://doi.org/10.3390/jpm12010085