

A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methodology
2.1. Stage 1: Source of Information
2.2. Stage 2: Search Stratergy
2.3. Stage 3: Process of Selection
2.4. Eligibility Criteria
2.5. Data Charting
2.6. Data Items
3. Results
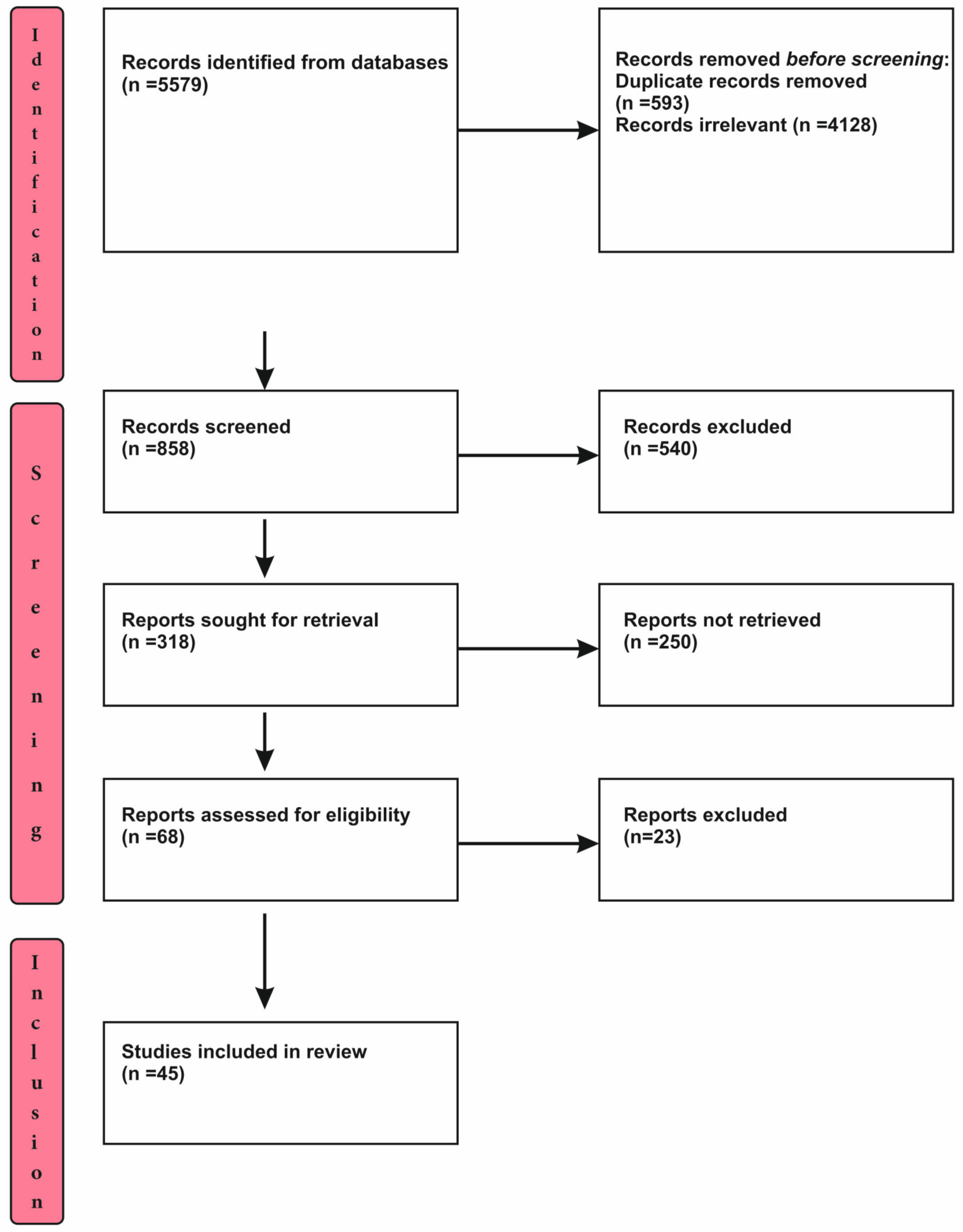
3.1. Selection of Source of Evidence
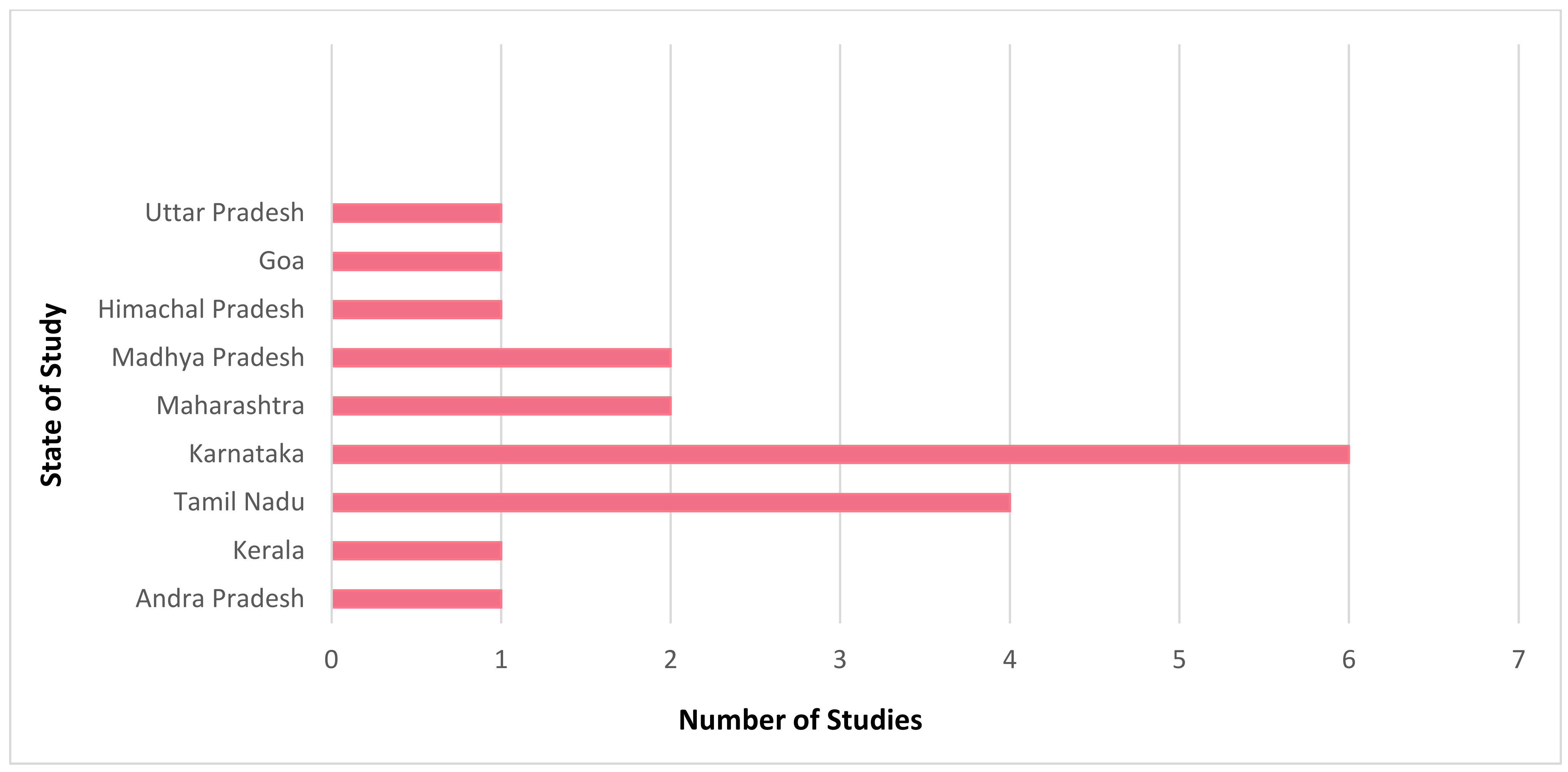
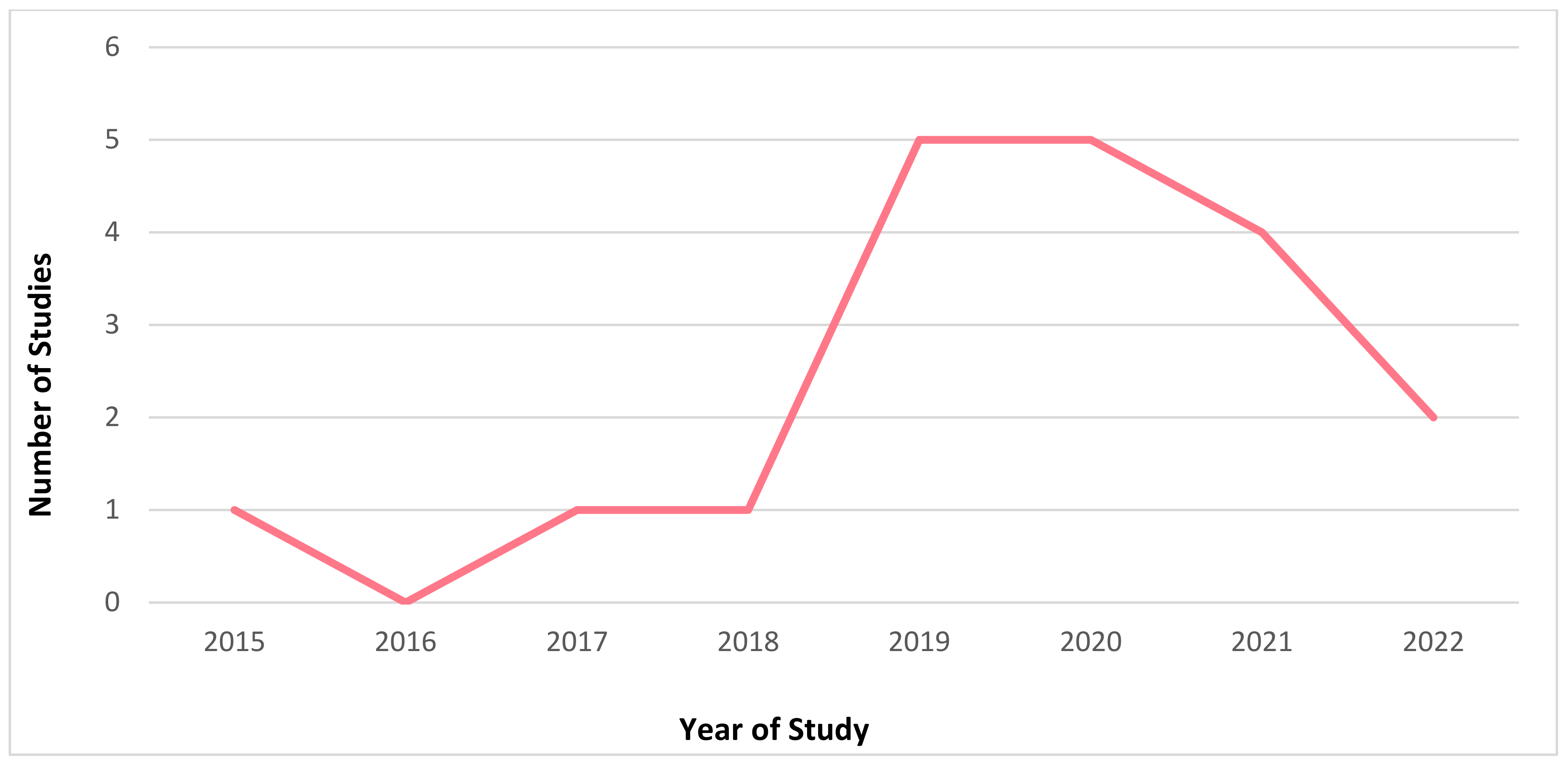
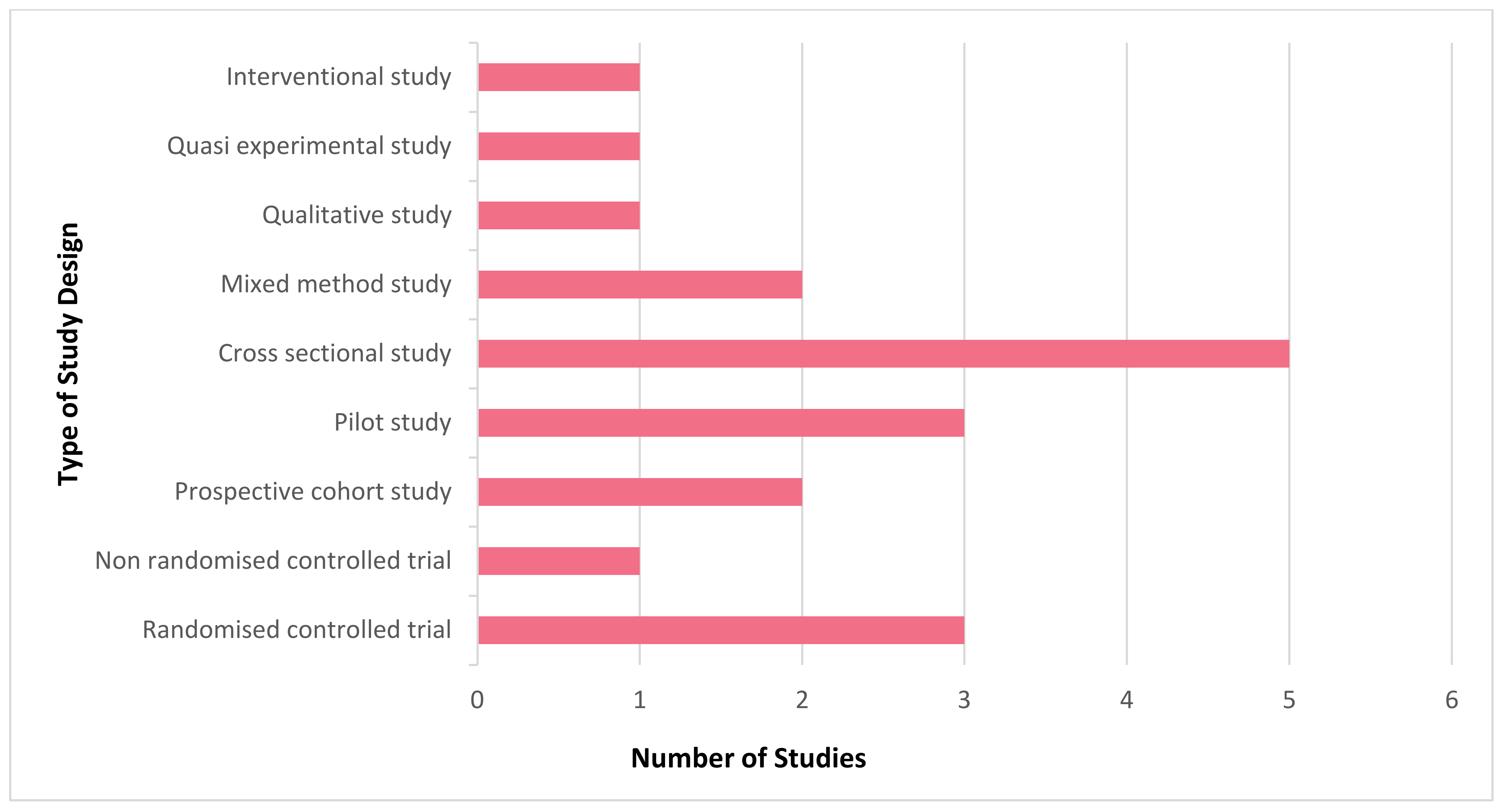
3.2. Characteristics and Results of Source of Evidence
3.3. Summary of Charted Data
4. Discussion
5. Knowledge Gaps
6. Limitations
7. Directions for Future Research
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Health & Human Services; Centers for Disease Control and Prevention. Tuberculosis, Basic TB Facts. Available online: https://www.cdc.gov/tb/topic/basics/default.htm (accessed on 29 July 2022).
- World Health Organization. Tuberculosis. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 30 July 2022).
- Minsitry of Health and Family Welfare; Central Tuberculosis Divison; Government of India. National Tuberculosis Elimination Programme. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=1&sublinkid=5613&lid=3658 (accessed on 29 July 2022).
- United Nations. The 2030 Agenda and the Sustainable Development Goals: An Opportunity for Latin America and the Caribbean; LC/G.2681-P/Rev.3; United Nations Publication: Santiago, Chile, 2018. [Google Scholar]
- Global Sustainable Development Goals Indicator Platform. Available online: https://sdg.tracking-progress.org/indicator/3-3-2-tuberculosis-incidence/ (accessed on 30 July 2022).
- National Health Portal. National Tuberculosis Elimination Programme. Available online: https://www.nhp.gov.in/revised-national-tuberculosis-control-programme_pg (accessed on 28 July 2022).
- Galetsi, P.; Katsaliaki, K.; Kumar, S. Exploring benefits and ethical challenges in the rise of mHealth (mobile healthcare) technology for the common good: An analysis of mobile applications for health specialists. Technovation 2022, 102598, in press. [Google Scholar] [CrossRef]
- Price, M.; Yuen, E.K.; Goetter, E.M.; Herbert, J.D.; Forman, E.; Acierno, R.; Ruggiero, K.J. mHealth: A Mechanism to Deliver More Accessible, More Effective Mental Health Care. Clin. Psychol. Psychother. 2013, 21, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Ganapathy, K.; Aditi; Ravindra. mhealth: A Potential Tool for Health Care Delivery in India. Making the eHealth Connection. 2008. Available online: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.511.7287&rep=rep1&type=pdf (accessed on 30 July 2022).
- Bassi, A.; John, O.; Praveen, D.; Maulik, P.K.; Panda, R.; Jha, V. Current Status and Future Directions of mHealth Interventions for Health System Strengthening in India: Systematic Review. JMIR mHealth uHealth 2018, 6, e11440. [Google Scholar] [CrossRef] [PubMed]
- Tumuhimbise, W.; Musiimenta, A. A review of mobile health interventions for public private mix in tuberculosis care. Internet Interv. 2021, 25, 100417. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Handbook for the Use of Digital Technologies to Support Tuberculosis Medication Adherence; WHO: Paris, France, 2017; ISBN 978-92-4-000294-4. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Majella, M.G.; Thekkur, P.; Kumar, A.M.; Chinnakali, P.; Saka, V.K.; Roy, G. Effect of mobile voice calls on treatment initiation among patients diagnosed with tuberculosis in a tertiary care hospital of Puducherry: A randomized controlled trial. J. Postgrad. Med. 2021, 67, 205–212. [Google Scholar] [CrossRef]
- Nagaraja, S.B.; Kotur, N.; Murthy, N.; Kunjathur, S.M.; Sappandi, N.; Murthy, D.; Das, A.; Singarajipur, A. “Kill-TB” Drug Reminder Mobile Application for Tuberculosis Patients at Bengaluru, India: Effectiveness and Challenges. J. Tuberc. Res. 2020, 8, 1–10. [Google Scholar] [CrossRef]
- Zhang, W.; Dogar, M.E.; Jain, M.; Rodriges, E.; Pathak, S.; Bhargava, S.; Gupta, A.; Jain, M. Feasibility and Effectiveness of Mobile App for Active Case Finding for Tuberculosis in India. Telehealth Med. Today 2020, 5. [Google Scholar] [CrossRef]
- Fernandes, L.; Narvekar, A.; Lawande, D. Efficacy of smoking cessation intervention delivered through mobile tele-counseling among smokers with tuberculosis in a Revised National Tuberculosis Control Program. Indian J. Tuberc. 2022, 69, 207–212. [Google Scholar] [CrossRef]
- Velayutham, B.; Thomas, B.; Nair, D.; Thiruvengadam, K.; Prashant, S.; Kittusami, S.; Vijayakumar, H.; Chidambaram, M.; Shivakumar, S.V.B.Y.; Jayabal, L.; et al. The Usefulness and Feasibility of Mobile Interface in Tuberculosis Notification (MITUN) Voice Based System for Notification of Tuberculosis by Private Medical Practitioners—A Pilot Project. PLoS ONE 2015, 10, e0138274. [Google Scholar] [CrossRef] [Green Version]
- Thomas, B.; Kumar, J.; Onongaya, C.; Bhatt, S.; Galivanche, A.; Periyasamy, M.; Chiranjeevi, M.; Khandewale, A.; Ramachandran, G.; Shah, D.; et al. Explaining Differences in the Acceptability of 99DOTS, a Cell Phone–Based Strategy for Monitoring Adherence to Tuberculosis Medications: Qualitative Study of Patients and Health Care Providers. JMIR mHealth uHealth 2020, 8, e16634. Available online: https://mhealth.jmir.org/2020/7/e16634 (accessed on 29 July 2022). [CrossRef]
- Tyagi, H.; Sabharwal, M.; Dixit, N.; Pal, A.; Deo, S. Leveraging Providers’ Preferences to Customize Instructional Content in Information and Communications Technology–Based Training Interventions: Retrospective Analysis of a Mobile Phone–Based Intervention in India. JMIR mHealth uHealth 2020, 8, e15998. Available online: https://mhealth.jmir.org/2020/3/e15998 (accessed on 28 July 2022). [CrossRef] [PubMed]
- Gupta, A.; Bhardwaj, A.K.; Singh, H.; Kumar, S.; Gupta, R. Effect of ‘mHealth’ Interventions on adherence to treatment and outcomes in Tuberculosis patients of district Shimla, Himachal Pradesh, India: A Randomised Control Trial. Indian J. Prev. Soc. Med. 2020, 51, 125–136. Available online: http://www.ijpsm.co.in/index.php/ijpsm/article/view/278 (accessed on 30 July 2022).
- Navin, K.; Vadivu, G.; Maharaj, A.; Thomas, T.; Lavanya, S. A Mobile Health Intervention to Support TB Eradication Programme for Adherence to Treatment and a Novel QR Code Based Technique to Monitor Patient–DOTS Provider Interaction. In Advanced Computational and Communication Paradigms; Lecture Notes in Electrical Engineering; Bhattacharyya, S., Gandhi, T., Sharma, K., Dutta, P., Eds.; Springer: Singapore, 2018; Volume 475. [Google Scholar] [CrossRef]
- Pande, T.; Saravu, K.; Temesgen, Z.; Seyoum, A.; Rai, S.; Rao, R.; Mahadev, D.; Pai, M.; Gagnon, M.P. Evaluating clinicians’ user experience and acceptability of LearnTB, a smartphone application for tuberculosis in India. mHealth 2017, 3, 30. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.A.; De Costa, A.; Das, A.; Srinivasa, G.; D’Souza, G.; Rodrigues, R. Mobile Health for Tuberculosis Management in South India: Is Video-Based Directly Observed Treatment an Acceptable Alternative? JMIR mHealth uHealth 2019, 7, e11687. [Google Scholar] [CrossRef] [PubMed]
- Santra, S.; Garg, S.; Basu, S.; Sharma, N.; Singh, M.M.; Khanna, A. The effect of a mhealth intervention on anti-tuberculosis medication adherence in Delhi, India: A quasi-experimental study. Indian J. Public Health 2021, 65, 34–38. Available online: https://www.ijph.in/text.asp?2021/65/1/34/311528 (accessed on 30 July 2022).
- Open Science Framework. Acceptability of Video Observed Treatment vs. Directly Observed Treatment for Tuberculosis: A Comparative Analysis between South and Central India. Available online: https://wellcomeopenresearch.org/articles/7-152 (accessed on 30 July 2022). [CrossRef]
- Cox, S.N.; Elf, J.; Lokhande, R.; Ogale, Y.P.; DiAndreth, L.; Dupuis, E.; Milovanovic, M.; Mpungose, N.; Mave, V.; Suryavanshi, N.; et al. Mobile phone access and comfort: Implications for HIV and Tuberculosis care in India and South Africa. Int. J. Tuberc. Lung Dis. 2019, 23, 865–872. [Google Scholar] [CrossRef]
- Jose, N.K.; Vaz, C.; Chai, P.R.; Rodrigues, R. The Acceptability of Adherence Support via Mobile Phones for Antituberculosis Treat7ment in South India: Exploratory Study. JMIR Form. Res. 2022, 6, e37124. [Google Scholar] [CrossRef]
- Kodali, P.B.; Das, S. Acceptance of mHealth technologies among Auxiliary; Nurse Midwives in Andhra Pradesh, India: A mixed method study. Med. Sci. 2021, 25, 1052–1060. [Google Scholar]
- Holzman, S.B.; Atre, S.; Sahasrabudhe, T.; Ambike, S.; Jagtap, D.; Sayyad, Y.; Kakrani, A.L.; Gupta, A.; Mave, V.; Shah, M.; et al. Use of Smartphone-Based Video Directly Observed Therapy (vDOT) in Tuberculosis Care: Single-Arm, Prospective Feasibility Study. JMIR Form. Res. 2019, 3, e13411. [Google Scholar] [CrossRef]
- Shivalli, S.; Hondappagol, A.; Akshaya, K.M.; Nirgude, A.; Varun, N.; Reddy, R.H.R.; Sharath, B.N. Does mobile phone instructional video demonstrating sputum expectoration improve the sputum sample quality and quantity in presumptive pulmonary TB cases? Protocol for a prospective pragmatic non-randomised controlled trial in Karnataka state, India. BMJ Open 2020, 10, e032991. [Google Scholar] [CrossRef] [Green Version]
- Nagaraj, K.; Prithviraj, R.; Ramesh, R.M.; Maheswaran, R.; Narasimhaiah, S.; Akshaya, K.M. Effectiveness of Health Education Video in Improving Treatment Adherence among Patients with Tuberculosis: An Interventional Study from Bengaluru, India. J. Tuberc. Res. 2019, 7, 159–169. [Google Scholar] [CrossRef]
- Osei, E.; Mashamba-Thompson, T.P. Mobile health applications for disease screening and treatment support in low and middle income countries: A narrative review. Heliyon 2021, 7, e06639. [Google Scholar] [CrossRef] [PubMed]
- Keshri, V.R. Leveraging mHealth Intervention to Ensure Initiation of Treatment for Tuberculosis. J. Postgrad. Med. 2021, 67, 194–195. Available online: https://www.jpgmonline.com/text.asp?2021/67/4/194/331273 (accessed on 28 July 2022). [CrossRef] [PubMed]
- Turimumahoro, P.; Tucker, A.; Gupta, A.J.; Tampi, R.P.; Babirye, D.; Ochom, E.; Ggita, J.M.; Ayakaka, I.; Sohn, H.; Katamba, A.; et al. A cost analysis of implementing mobile health facilitated tuberculosis contact investigation in a low-income setting. PLoS ONE 2022, 17, e0265033. [Google Scholar] [CrossRef]
- Narasimhadevara, A.; Rambhatla, R. Chapter 9: mHealth for Better Quality of Life, Healthier Lifestyles, and More Meaningful Lives. In Technology and Global Public Health; Murthy, P., Ansehl, A., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Lee, Y.; Raviglione, M.C.; Flahault, A. Use of Digital Technology to Enhance Tuberculosis Control: Scoping Review. J. Med. Internet Res. 2020, 22, e15727. [Google Scholar] [CrossRef]
- Pai, R.R.; Alathur, S. Determinants of individuals’ intention to use mobile health: Insights from India. Trans. Gov. People Process Policy 2019, 13, 306–326. [Google Scholar] [CrossRef]
- Subbaraman, R.; De Mondesert, L.; Musiimenta, A.; Pai, M.; Mayer, K.H.E.; Thomas, B.; Haberer, J. Digital adherence technologies for the management of tuberculosis therapy: Mapping the landscape and research priorities. BMJ Glob. Health 2018, 3, e001018. [Google Scholar] [CrossRef]
- Danasekaran, R.; Raja, T.; Kumar, M.B. mHealth: A Newer Perspective in Healthcare through Mobile Technology. J. Compr. Health 2019, 7, 67–68. [Google Scholar] [CrossRef]
- Chadha, S.; Trivedi, A.; Nagaraja, S.B.; Sagili, K. mHealth to enhance TB referrals: Challenge in scaling up: In reply; International Union against Tuberculosis and Lung Disease. Public Health Action 2018, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Margineanu, I.; Louka, C.; Vincenti-Gonzalez, M.; Saktiawati, A.; Schierle, J.; Abass, K.; Akkerman, O.; Alffenaar, J.; Ranchor, A.; Stienstra, Y. Patients and Medical Staff Attitudes Toward the Future Inclusion of eHealth in Tuberculosis Management: Perspectives from Six Countries Evaluated using a Qualitative Framework. JMIR mHealth uHealth 2020, 8, e18156. Available online: https://mhealth.jmir.org/2020/11/e18156 (accessed on 29 July 2022). [CrossRef]
- Das Gupta, D.; Patel, A.; Saxena, D.; Koizumi, N.; Trivedi, P.; Patel, K.; Raval, D.; King, A.; Chandler, K. Choice-Based Reminder Cues: Findings From an mHealth Study to Improve Tuberculosis (TB) Treatment Adherence Among the Urban Poor in India. World Med. Health Policy 2020, 12, 163–181. [Google Scholar] [CrossRef]
- Gashu, K.D.; Gelaye, K.A.; Mekonnen, Z.A.; Lester, R.; Tilahun, B. Does phone messaging improves tuberculosis treatment success? A systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Suryavanshi, N.; Dhumal, G.; Cox, S.; Sangle, S.; DeLuca, A.; Santre, M.; Gupta, A.; Chander, G.; Hutton, H. Acceptability, Adaptability, and Feasibility of a Novel Computer-Based Virtual Counselor–Delivered Alcohol Intervention: Focus Group and In-depth Interview Study Among Adults with HIV or Tuberculosis in Indian Clinical Settings. JMIR Form Res. 2022, 6, e35835. Available online: https://formative.jmir.org/2022/5/e35835 (accessed on 30 July 2022). [CrossRef] [PubMed]
- Asres, A.; Jerene, D.; Deressa, W. Delays to anti-tuberculosis treatment intiation among cases on directly observed treatment short course in districts of southwestern Ethiopia: A cross sectional study. BMC Infect. Dis. 2019, 19, 481. [Google Scholar] [CrossRef]
- Daftary, A.; Satyanaraya, S.; Jha, N. Can Community Pharmacist Improve Tuberculosis Case Finding? A Mixed Methods Intervention Study in India. BMJ Glob. Health 2019, 4, e001417. Available online: https://gh.bmj.com/content/4/3/e001417.abstract (accessed on 29 July 2022). [CrossRef]
- Thangaraj, P.; Hemalatha, K. Tuberculosis Notification: Facilitators and Barriers among Private Practitioners in Trichy, South India. 2021, 26, pp. 81–85. Available online: https://www.jmgims.co.in/article.asp?issn=0971- (accessed on 28 July 2022).
- Keutzer, L.; Wicha, S.G.; Simonsson, U.S. Mobile Health Apps for Improvement of Tuberculosis Treatment: Descriptive Review. JMIR mHealth uHealth 2020, 8, e17246. [Google Scholar] [CrossRef]
- Guo, P.; Qiao, W.; Sun, Y.; Liu, F.; Wang, C. Telemedicine Technologies and Tuberculosis Management: A Randomized Controlled Trial. Telemed. J. E Health 2020, 26, 1150–1156. [Google Scholar] [CrossRef]
- Basu, S. mHealth to enhance TB referrals: Challenge in scaling up; International Union against Tuberculosis and Lung Disease. Public Health Action 2018, 8, 29. [Google Scholar] [CrossRef]
- Okolo, C.T.; Kamath, S.; Dell, N.; Vashistha, A. “It cannot do all of my work”: Community Health Worker Perceptions of AI -Enabled Mobile Health Applications in Rural India. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems (CHI’21), Yokohama, Japan, 8–13 May 2021; Association for Computing Machinery: New York, NY, USA, 2021. Article 701. pp. 1–20. [Google Scholar] [CrossRef]
- Choudhury, P.; Devadutta, K.; Dash, A.K.; Mohapatra, A. Modeling a Monitoring System for TB Patients Using RFID Technique with SMS Access. In Smart Intelligent Computing and Applications; Smart Innovation, Systems and Technologies; Satapathy, S., Bhateja, V., Mohanty, J., Udgata, S., Eds.; Springer: Singapore, 2020; Volume 159. [Google Scholar] [CrossRef]
- Thomas, B.E.; Velayutham, B.; Thiruvengadam, K.; Nair, D.; Barman, S.B.; Jayabal, L.; Ovung, S.; Swaminathan, S. Perceptions of Private Medical Practitioners on Tuberculosis Notification: A Study from Chennai, South India. PLoS ONE 2016, 11, e0147579. [Google Scholar] [CrossRef]
- Pai; Rajesh, R. A select of Mobile Health Applications in Indian Context. 2020. Available online: https://idr.nitk.ac.in/jspui/handle/123456789/16887 (accessed on 28 July 2022).
- Gadicherla, S.; Krishnappa, L.; Madhuri, B.; Mitra, S.G.; Ramaprasad, A.; Seevan, R.; Sreeganga, S.D.; Thodika, N.K.; Mathew, S.; Suresh, V. Envisioning a learning surveillance system for tuberculosis. PLoS ONE 2020, 15, e0243610. [Google Scholar] [CrossRef]
- Mitchell, E.; Adejumo, O.; Abdur-Razzaq, H.; Ogbudebe, C.; Chukwueme, N.; Olorunju, S.; Gidado, M. Hybrid Approach to Estimation of Underreporting of Tuberculosis Case Notification in High-Burden Settings with Weak Surveillance Infrastructure: Design and Implementation of an Inventory Study. JMIR Public Health Surveill 2021, 7, e22352. Available online: https://publichealth.jmir.org/2021/3/e22352 (accessed on 29 July 2022). [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Inclusion | Exclusion |
|---|---|---|
| Language | English | All other languages |
| Year | From 2015 | Before 2015 |
| Type of study | Quantitative, qualitative and mixed methods | |
| Country | India | All other countries |
| Publication status | Articles under peer review, grey literature, indexed journals, abstracts | |
| Study theme | mHealth interventions for Tuberculosis management | Manual methods of management |
| Intervention | Mobile health apps, Short Message Service (SMS) | Physical modes of diagnosis, management, or treatment |
| S. No. | Author | Year | State/City | Aim of Study | Study Design | Study Population |
|---|---|---|---|---|---|---|
| 1 | Majella et al. [14] | 2021 | Puducherry | To evaluate the use of mobile voice calls to remind Tuberculosis (TB) patients regarding follow up | Randomised controlled trial | Newly diagnosed TB patients |
| 2 | Nagaraja et al. [15] | 2020 | Karnataka | To observe missed doses during treatment in TB patients with or without mobile application | Prospective cohort study | 694 adult TB patients |
| 3 | Zhang et al. [16] | 2020 | Bhopal and Indore | To study the feasibility of the smart phone app | Pilot study | 18,706 patients |
| 4 | Fernandes et al. [17] | 2021 | Goa | To determine the effectiveness of tele-counselling to quit smoking in TB patients | Randomised controlled trial | 80 individuals |
| 5 | Velayutham et al. [18] | 2015 | Chennai | To ascertain the usefulness and affordability of mobile interface in TB notification | Pilot study | 184 private medical practitioners |
| 6 | Thomas et al. [19] | 2020 | Chennai and Vellore | To determine the factors affecting the acceptance of 99DOTS (Directly Observed Treatment, Short course) in TB patients and healthcare providers | Qualitative study | 93 patients |
| 7 | Tyagi et al. [20] | 2020 | Not specified | To explore the preferences of healthcare providers on the content of information and communication technology for TB | Mixed method study | 24,949 private practitioners |
| 8 | Gupta et al. [21] | 2020 | Shimla | To analyse the outcomes of mHealth interventions in tuberculosis care | Randomised control trial | 312 patients |
| 9 | Navin et al. [22] | 2018 | Chennai | To investigate the application and utility of an mHealth intervention for supporting tuberculosis treatment | Prospective cohort study | TB patients |
| 10 | Pande et al. [23] | 2017 | Manipal | To investigate the utilisation of a smartphone app among clinicians for tuberculosis | Cross sectional study | 101 clinicians |
| 11 | Kumar et al. [24] | 2019 | Bangalore | To explore the usage of mobile apps and mHealth support regarding tuberculosis management among patients | Cross sectional study | 185 TB patients |
| 12 | Santra et al. [25] | 2021 | Delhi | To assess the potency of mHealth intervention on medication follow up among TB patients | Quasi experimental study | 220 TB patients |
| 13 | Rao et al. [26] | 2022 | Bengaluru and Ujjain | To analyse the usage of mobile phones for the anti-tuberculosis regimen among patients | Cross sectional study | 351 TB patients |
| 14 | Cox et al. [27] | 2019 | Pune | To investigate the access to mobile phones and mHealth technology for management of tuberculosis | Cross sectional study | 136 Indian TB patients |
| 15 | Jose et al. [28] | 2022 | Kerala | To analyse the acceptance of mHealth interventions for the anti-tuberculosis treatment. | Cross sectional study | 100 TB patients |
| 16 | Kodali et al. [29] | 2021 | Andhra Pradesh | To study the approved practice of mHealth technology among auxiliary nurse midwives | Mixed method study | 272 auxiliary nurse midwives |
| 17 | Holzman et al. [30] | 2019 | Pune | To investigate the feasibility and utilisation of mobile apps for video-based Directly Observed Therapy (DOT) among TB patients | Pilot study | 25 TB patients |
| 18 | Shivalli et al. [31] | 2019 | Karnataka | To access the efficacy of mobile based video instructions on sputum expectoration in order to enhance the quality and quantity of sputum sampling for tuberculosis patients | Non-randomised controlled trial | 7341 presumptive pulmonary tuberculosis PTB patients of which 311 patients were diagnosed with TB |
| 19 | Nagaraj et al. [32] | 2019 | Bengaluru | To understand the adherence of patients to mobile based educational videos for regimen care to enhance tuberculosis treatment | Interventional study | 100 TB patients |
| S. No. | Type of Interventions | Name of app/Interventions | Available Languages | Target | Result |
|---|---|---|---|---|---|
| 1 | Voice calls [14] | Not mentioned | Tamil | Treatment | Mobile voice calls are effective interventions to reduce Pretreatment loss to follow-up PTLFU among TB patients |
| 2 | Mobile phone app [15] | Kill TB | Not mentioned | Treatment | mHealth app enhances the patient’s treatment adherence and improves treatment outcomes |
| 3 | Mobile phone app [16] | Not specified | Not mentioned | Treatment and diagnosis | The use of smart phone application can boost diagnosis and follow up of patients |
| 4 | Voice calls [17] | Not mentioned | Not mentioned | Prevention | Mobile tele-counselling is a feasible intervention to encourage smoking cessation |
| 5 | Voice based system for notification [18] | Mobile interface in TB notification (MITUN) | Not mentioned | Prevention and treatment | The effectiveness of Mobile interface in TB notification (MITUN) was found to be suboptimal |
| 6 | Short Message Service (SMS) and voice calls [19] | 99DOTS (Directly Observed Treatment, Short course) | Not mentioned | Treatment | Poor cell phone accessibility, cellular signal and literacy are some of the factors contributing to non-adherence to 99DOTS |
| 7 | Mobile phone app [20] | Think TB | Not mentioned | Informative | Providers had inherent preferences for instructional content |
| 8 | Short Message Service (SMS) and voice calls [21] | Not specified | Hindi | Treatment | These mHealth technologies are easier to access and provide effective means of communication when physical presence couldnot be offered for every reminder. |
| 9 | Mobile phone app with unique Quck Response (QR) scanning [22] | TB track | Not mentioned | Treatment | A Quick Response (QR) tracking system provides unique monitoring of patients. Reminders for medication intake, reporting symptoms and tracking of progress are effectively well monitored. |
| 10 | Mobile phone app [23] | LearnTB | English | Informative | The overall utility of the app was very good which advocates the fact that mHealth technologies are more efficient and accessible. |
| 11 | Short Message Service (SMS) and voice calls [24] | Not specified | English | Treatment and prevention | Mobile communication received a high optimistic response among the participants. Reminders regarding medications, medical appointments, follow up and general preventive information was well appreciated to be received as SMS and voice calls |
| 12 | Short Message Service (SMS) and voice calls [25] | Not specified | Hindi | Treatment | mHealth technologies offer a supportive hand for daily regimen reminders of TB patients and weekly follow up. Future studies are essential in making these interventions accessible to all |
| 13 | Short Message Service (SMS) and voice calls, video based Directly Observed Therapy (DOT) [26] | Not specified | Not mentioned | Treatment | Short Message Service (SMS) and voice call preference was higher among frequent mobile users and video-based Directly Observed Therapy (DOT) was on high demand as it is cost effective, requires less travelling and convenient for users. |
| 14 | Short Message Service (SMS) reminders [27] | Not specified | Not mentioned | Treatment | Acceptability towards text messages was suboptimal among patients. Literacy, employment status and frequency of mobile usage were found to affect the acceptance rate |
| 15 | Short Message Service (SMS) and voice calls [28] | Not specified | Malayalam and English | Treatment | Voice calls were preferred to SMS reminders. However, a quarter of the participants accepted the usage of mobile phones for effective treatment reminders. |
| 16 | Mobile phone app [29] | Not specified | Telugu and English | Informative | mHealth acceptance was found to be less among the midwives, which can be attributed to less technological awareness and less exposure to newer methods of information transmission. |
| 17 | Mobile phone app [30] | Emocha Mobile Health Inc. | Marathi and English | Treatment | Video based Directly Observed Therapy (DOT) are identified to be feasible and affordable means of follow up of treatment and it can be used as a reliable monitoring tool among TB patients |
| 18 | Instructional videos [32] | Not specified | Kannada | Sample collection | SMS and voice calls are rapidly used for TB management in India. However, implementation of higher standard technologies may be costly and adhering people to these interventions may be a challenge as very fewstudies have been conducted in regard to video explanations. |
| 19 | Informational video [32] | Not specified | Kannada | Informative and treatment | The video-based technological support was found to have greater adherence and enhanced the awareness of TB patients about the importance of diagnosis, side effects and available treatment facilities to promote better health conditions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Needamangalam Balaji, J.; Prakash, S.; Park, Y.; Baek, J.S.; Shin, J.; Rajaguru, V.; Surapaneni, K.M. A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India. J. Pers. Med. 2022, 12, 1599. https://doi.org/10.3390/jpm12101599
Needamangalam Balaji J, Prakash S, Park Y, Baek JS, Shin J, Rajaguru V, Surapaneni KM. A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India. Journal of Personalized Medicine. 2022; 12(10):1599. https://doi.org/10.3390/jpm12101599
Chicago/Turabian StyleNeedamangalam Balaji, Jyotsna, Sreenidhi Prakash, Youngmok Park, Joon Sang Baek, Jaeyong Shin, Vasuki Rajaguru, and Krishna Mohan Surapaneni. 2022. "A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India" Journal of Personalized Medicine 12, no. 10: 1599. https://doi.org/10.3390/jpm12101599
APA StyleNeedamangalam Balaji, J., Prakash, S., Park, Y., Baek, J. S., Shin, J., Rajaguru, V., & Surapaneni, K. M. (2022). A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India. Journal of Personalized Medicine, 12(10), 1599. https://doi.org/10.3390/jpm12101599