
The Psychiatric Consequences of Long-COVID: A Scoping Review

 and
and 
Abstract
:1. Introduction
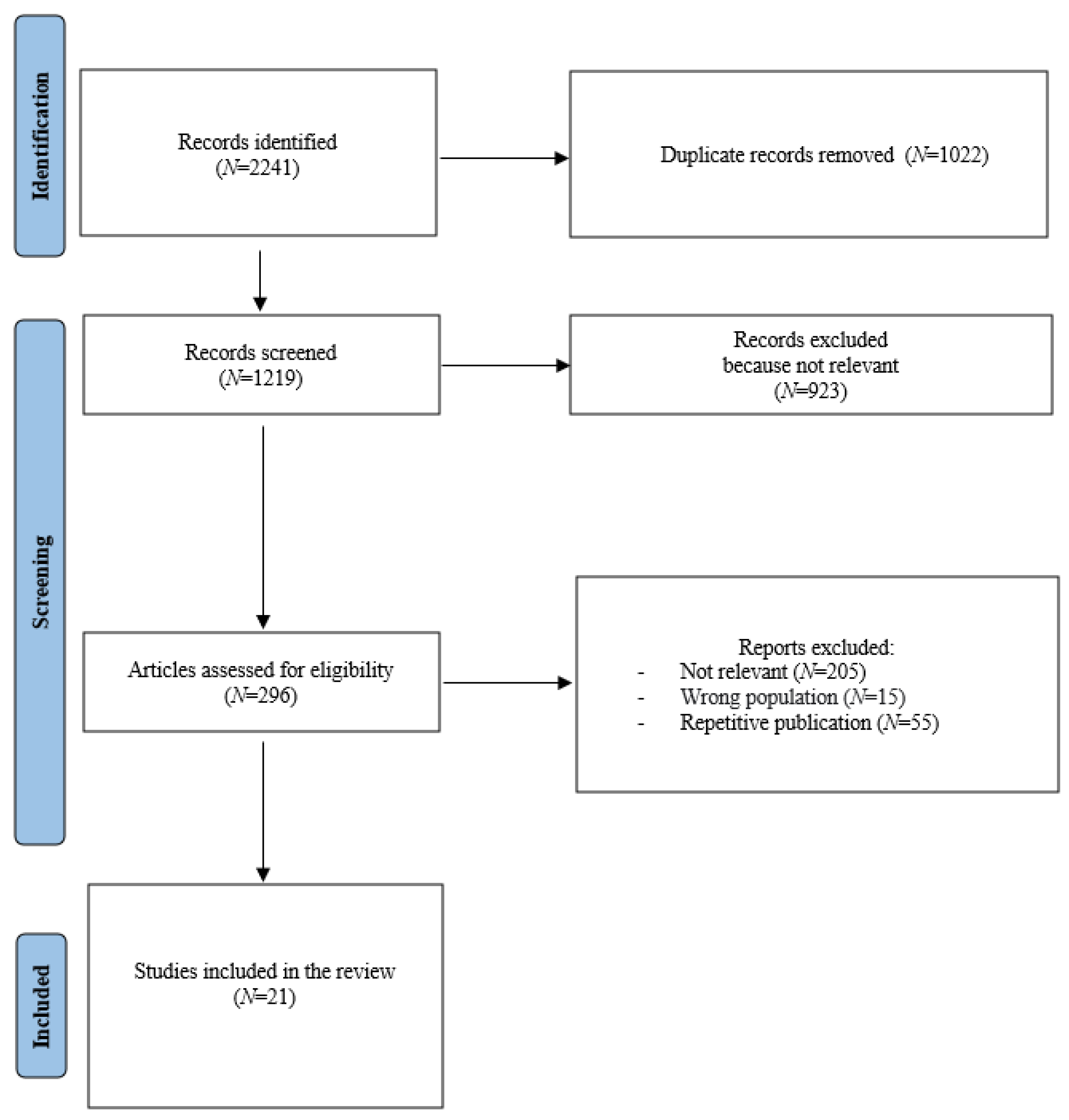
2. Materials and Methods
Study Selection and Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Unützer, J.; Kimmel, R.J.; Snowden, M. Psychiatry in the age of COVID-19. World Psychiatry 2020, 19, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Bridgland, V.M.E.; Moeck, E.K.; Green, D.M.; Swain, T.L.; Nayda, D.M.; Matson, L.A.; Hutchison, N.P.; Takarangi, M.K.T. Why the COVID-19 pandemic is a traumatic stressor. PLoS ONE 2021, 16, e0240146. [Google Scholar] [CrossRef] [PubMed]
- Horesh, D.; Brown, A.D. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychol. Trauma 2020, 12, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Rooksby, M.; Furuhashi, T.; McLeod, H.J. Hikikomori: A hidden mental health need following the COVID-19 pandemic. World Psychiatry 2020, 19, 399–400. [Google Scholar] [CrossRef]
- Sampogna, G.; Pompili, M.; Fiorillo, A. Mental Health in the Time of COVID-19 Pandemic: A Worldwide Perspective. Int. J. Environ. Res. Public Health 2021, 19, 161. [Google Scholar] [CrossRef]
- Wasserman, D.; van der Gaag, R.; Wise, J. The term “physical distancing” is recommended rather than “social distancing” during the COVID-19 pandemic for reducing feelings of rejection among people with mental health problems. Eur. Psychiatry 2020, 63, e52. [Google Scholar] [CrossRef]
- Alonzi, S.; La Torre, A.; Silverstein, M.W. The psychological impact of preexisting mental and physical health conditions during the COVID-19 pandemic. Psychol. Trauma 2020, 12, S236–S238. [Google Scholar] [CrossRef]
- Duarte, C.S.; Monk, C.; Weissman, M.M.; Posner, J. Intergenerational psychiatry: A new look at a powerful perspective. World Psychiatry 2020, 19, 175–176. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [Green Version]
- Gorwood, P.; Fiorillo, A. One year after the COVID-19: What have we learnt, what shall we do next? Eur. Psychiatry 2021, 64, e15. [Google Scholar] [CrossRef]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef] [PubMed]
- Hodgkin, D.; Moscarelli, M.; Rupp, A.; Zuvekas, S.H. Mental health economics: Bridging research, practice and policy. World Psychiatry 2020, 19, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Karatzias, T.; Shevlin, M.; Hyland, P.; Ben-Ezra, M.; Cloitre, M.; Owkzarek, M.; McElroy, E. The network structure of ICD-11 complex post-traumatic stress disorder across different traumatic life events. World Psychiatry 2020, 19, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, P. COVID-19 health anxiety. World Psychiatry 2020, 19, 307–308. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Badinlou, F.; Buhrman, M.; Brocki, K.C. Psychological impact of COVID-19 in the Swedish population: Depression, anxiety, and insomnia and their associations to risk and vulnerability factors. Eur. Psychiatry 2020, 63, e81. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, B.; Viganò, C.; Conti, D.; Scarpa, C.; Casati, L.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Nanni, M.G.; et al. Insomnia and related factors in patients with pre-existing psychiatric disorders compared to the general population during the COVID-19 lockdown: Findings from the multicentric COMET study. Compr. Psychiatry 2022, 118, 152345. [Google Scholar] [CrossRef]
- Pompili, M.; Innamorati, M.; Sampogna, G.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Erbuto, D.; Luciano, M.; Nanni, M.G.; et al. The impact of Covid-19 on unemployment across Italy: Consequences for those affected by psychiatric conditions. J. Affect Disord. 2022, 296, 59–66. [Google Scholar] [CrossRef]
- Carrà, G.; Crocamo, C.; Bartoli, F.; Riboldi, I.; Sampogna, G.; Luciano, M.; Albert, U.; Carmassi, C.; Cirulli, F.; Dell’Osso, B.; et al. Were anxiety, depression and psychological distress associated with local mortality rates during COVID-19 outbreak in Italy? Findings from the COMET study. J. Psychiatr. Res. 2022, 152, 242–249. [Google Scholar] [CrossRef]
- Sampogna, G.; Del Vecchio, V.; Giallonardo, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Menculini, G.; et al. What Is the Role of Resilience and Coping Strategies on the Mental Health of the General Population during the COVID-19 Pandemic? Results from the Italian Multicentric COMET Study. Brain. Sci. 2021, 11, 1231. [Google Scholar] [CrossRef]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249–250. [Google Scholar] [CrossRef]
- Qiu, D.; Li, Y.; Li, L.; He, J.; Ouyang, F.; Xiao, S. Prevalence of post-traumatic stress symptoms among people influenced by coronavirus disease 2019 outbreak: A meta-analysis. Eur. Psychiatry 2021, 64, e30. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Lee, Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry 2020, 19, 250–251. [Google Scholar] [CrossRef] [PubMed]
- Alderdice, F. Supporting psychological well-being around the time of birth: What can we learn from maternity care? World Psychiatry 2020, 19, 332–333. [Google Scholar] [CrossRef] [PubMed]
- Brown, S. Perinatal mental health and the COVID-19 pandemic. World Psychiatry 2020, 19, 333–334. [Google Scholar] [CrossRef]
- Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Menculini, G.; et al. Loneliness in Young Adults During the First Wave of COVID-19 Lockdown: Results from the Multicentric COMET Study. Front. Psychiatry 2021, 12, 788139. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.S.; Nanjundaswamy, M.H. Pregnancy specific anxiety: An under-recognized problem. World Psychiatry 2020, 19, 336–337. [Google Scholar] [CrossRef]
- Chatterjee, S.S.; Barikar, C.M.; Mukherjee, A. Impact of COVID-19 pandemic on pre-existing mental health problems. Asian J. Psychiatr. 2020, 51, 102071. [Google Scholar] [CrossRef]
- Crocamo, C.; Viviani, M.; Famiglini, L.; Bartoli, F.; Pasi, G.; Carrà. Surveilling COVID-19 Emotional Contagion on Twitter by Sentiment Analysis. Eur. Psychiatry 2021, 64, e17. [Google Scholar] [CrossRef]
- Giallonardo, V.; Sampogna, G.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Nanni, M.G.; et al. The Impact of Quarantine and Physical Distancing Following COVID-19 on Mental Health: Study Protocol of a Multicentric Italian Population Trial. Front. Psychiatry 2020, 11, 533. [Google Scholar] [CrossRef]
- Glover, V. Prenatal mental health and the effects of stress on the foetus and the child. Should psychiatrists look beyond mental disorders? World Psychiatry 2020, 19, 331–332. [Google Scholar] [CrossRef]
- Kato, T.A.; Kanba, S.; Teo, A.R. Defining pathological social withdrawal: Proposed diagnostic criteria for hikikomori. World Psychiatry 2020, 19, 116–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squeglia, L.M. Alcohol and the developing adolescent brain. World Psychiatry 2020, 19, 393–394. [Google Scholar] [CrossRef]
- Wang, Q.; Xu, R.; Volkow, N.D. Increased risk of COVID-19 infection and mortality in people with mental disorders: Analysis from electronic health records in the United States. World Psychiatry 2021, 20, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Q.; Davis, P.B.; Volkow, N.D.; Xu, R. Increased risk for COVID-19 breakthrough infection in fully vaccinated patients with substance use disorders in the United States between December 2020 and August 2021. World Psychiatry 2022, 21, 124–132. [Google Scholar] [CrossRef] [PubMed]
- De Hert, M.; Mazereel, V.; Detraux, J.; Van Assche, K. Prioritizing COVID-19 vaccination for people with severe mental illness. World Psychiatry 2021, 20, 54–55. [Google Scholar] [CrossRef] [PubMed]
- Adhanom Ghebreyesus, T. Addressing mental health needs: An integral part of COVID-19 response. World Psychiatry 2020, 19, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Stahl, S.M. The relevance of COVID-19 pandemic to psychiatry. World Psychiatry 2020, 19, 261. [Google Scholar] [CrossRef]
- Alghamdi, H.Y.; Alrashed, A.M.; Jawhari, A.M.; Abdel-Moneim, A.S. Neuropsychiatric symptoms in post-COVID-19 long haulers. Acta Neuropsychiatr. 2022, 11, 1–12. [Google Scholar] [CrossRef]
- Feldman, R. What is resilience: An affiliative neuroscience approach. World Psychiatry 2020, 19, 132–150. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Petkova, E.; Bhui, K.S.; Schulze, T.G. A global needs assessment in times of a global crisis: World psychiatry response to the COVID-19 pandemic. BJPsych Open 2020, 6, e48. [Google Scholar] [CrossRef] [Green Version]
- Menculini, G.; Albert, U.; Bianchini, V.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Fabrazzo, M.; Perris, F.; Sampogna, G.; et al. Did we learn something positive out of the COVID-19 pandemic? Post-traumatic growth and mental health in the general population. Eur. Psychiatry 2022, 64, e79. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Clinical Excellence (NICE). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute of Clinical Excellence: London, UK, 2022. [Google Scholar]
- Sisó-Almirall, A.; Brito-Zerón, P.; Conangla Ferrín, L.; Kostov, B.; Moragas Moreno, A.; Mestres, J.; Sellarès, J.; Galindo, G.; Morera, R.; Basora, J.; et al. Long Covid-19: Proposed Primary Care Clinical Guidelines for Diagnosis and Disease Management. Int. J. Environ. Res. Public Health 2021, 18, 4350. [Google Scholar] [CrossRef] [PubMed]
- Mohamed-Hussein, A.A.R.; Amin, M.T.; Makhlouf, H.A.; Makhlouf, N.A.; Galal, I.; Abd-Elaal, H.K.; Abdeltawab, D.; Kholief, K.M.S.; Hashem, M.K. Non-hospitalised COVID-19 patients have more frequent long COVID-19 symptoms. Int. J. Tuberc. Lung Dis. 2021, 25, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Stefano, G.B.; Ptacek, R.; Ptackova, H.; Martin, A.; Kream, R.M. Selective Neuronal Mitochondrial Targeting in SARS-CoV-2 Infection Affects Cognitive Processes to Induce ‘Brain Fog’ and Results in Behavioral Changes that Favor Viral Survival. Med. Sci. Monit. 2021, 27, e930886. [Google Scholar] [CrossRef]
- Milton, D.C.; Ward, J.; Ward, E.; Lyall, D.M.; Strawbridge, R.J.; Smith, D.J.; Cullen, B. The association between C-reactive protein, mood disorder, and cognitive function in UK Biobank. Eur. Psychiatry 2021, 64, e14. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H. Psychiatric symptoms and cognitive impairment in “Long COVID”: The relevance of immunopsychiatry. World Psychiatry 2021, 20, 357–358. [Google Scholar] [CrossRef]
- Efstathiou, V.; Stefanou, M.I.; Demetriou, M.; Siafakas, N.; Makris, M.; Tsivgoulis, G.; Zoumpourlis, V.; Kympouropoulos, S.P.; Tsoporis, J.N.; Spandidos, D.A.; et al. Long COVID and neuropsychiatric manifestations (Review). Exp. Ther. Med. 2022, 23, 363. [Google Scholar] [CrossRef]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Tang, S.W.; Leonard, B.E.; Helmeste, D.M. Long COVID, neuropsychiatric disorders, psychotropics, present and future. Acta Neuropsychiatr. 2022, 34, 109–126. [Google Scholar] [CrossRef]
- Badenoch, J.B.; Rengasamy, E.R.; Watson, C.; Jansen, K.; Chakraborty, S.; Sundaram, R.D.; Hafeez, D.; Burchill, E.; Saini, A.; Thomas, L.; et al. Persistent neuropsychiatric symptoms after COVID-19: A systematic review and meta-analysis. Brain Commun. 2021, 4, fcab297. [Google Scholar] [CrossRef]
- Trapani, G.; Verlato, G.; Bertino, E.; Maiocco, G.; Vesentini, R.; Spadavecchia, A.; Dessì, A.; Fanos, V. Long COVID-19 in children: An Italian cohort study. Ital. J. Pediatr. 2022, 48, 83. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Ayuzo Del Valle, N.C.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. Long-COVID in children and adolescents: A systematic review and meta-analyses. Sci. Rep. 2022, 12, 9950. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/clinical-guidance/post-covid-19-conditions-in-children-and-adolescents/ (accessed on 23 October 2022).
- AlRadini, F.A.; Alamri, F.; Aljahany, M.S.; Almuzaini, Y.; Alsofayan, Y.; Khan, A.; Albogami, N.; Abdulrahim, M.; Almogbil, A.; Alahmari, A. Post-acute COVID-19 condition in Saudi Arabia: A national representative study. J. Infect. Public Health 2022, 15, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, M.; Khan, A.; Jacobs, A.; D’Souza, V.; Consiglio, F.; Karmen, C.L.; Dornbush, R.; Hasnat, G.S.; Ferrando, S.J. Examining the Long-Term Sequelae of SARS-CoV2 Infection in Patients Seen in an Outpatient Psychiatric Department. Neuropsychiatr. Dis. Treat 2022, 18, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Iosifescu, A.L.; Hoogenboom, W.S.; Buczek, A.J.; Fleysher, R.; Duong, T.Q. New-onset and persistent neurological and psychiatric sequelae of COVID-19 compared to influenza: A retrospective cohort study in a large New York City healthcare network. Int. J. Methods Psychiatr. Res. 2022, 31, e1914. [Google Scholar] [CrossRef]
- Ohira, M.; Sano, T.; Takao, M. Clinical features of patients who visited the outpatient clinic for long COVID in Japan. eNeurologicalSci 2022, 28, 100418. [Google Scholar] [CrossRef]
- Jozuka, R.; Kimura, H.; Uematsu, T.; Fujigaki, H.; Yamamoto, Y.; Kobayashi, M.; Kawabata, K.; Koike, H.; Inada, T.; Saito, K.; et al. Severe and long-lasting neuropsychiatric symptoms after mild respiratory symptoms caused by COVID-19: A case report. Neuropsychopharmacol. Rep. 2022, 42, 114–119. [Google Scholar] [CrossRef]
- Calabria, M.; García-Sánchez, C.; Grunden, N.; Pons, C.; Arroyo, J.A.; Gómez-Anson, B.; Estévez García, M.D.C.; Belvís, R.; Morollón, N.; Vera Igual, J.; et al. Post-COVID-19 fatigue: The contribution of cognitive and neuropsychiatric symptoms. J. Neurol. 2022, 269, 3990–3999. [Google Scholar] [CrossRef]
- Cacciatore, M.; Raggi, A.; Pilotto, A.; Cristillo, V.; Guastafierro, E.; Toppo, C.; Magnani, F.G.; Sattin, D.; Mariniello, A.; Silvaggi, F.; et al. Neurological and Mental Health Symptoms Associated with Post-COVID-19 Disability in a Sample of Patients Discharged from a COVID-19 Ward: A Secondary Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4242. [Google Scholar] [CrossRef]
- Chen, A.K.; Wang, X.; McCluskey, L.P.; Morgan, J.C.; Switzer, J.A.; Mehta, R.; Tingen, M.; Su, S.; Harris, R.A.; Hess, D.C.; et al. Neuropsychiatric sequelae of long COVID-19: Pilot results from the COVID-19 neurological and molecular prospective cohort study in Georgia, USA. Brain Behav. Immun. Health 2022, 24, 100491. [Google Scholar] [CrossRef]
- Colizzi, M.; Peghin, M.; De Martino, M.; Bontempo, G.; Gerussi, V.; Palese, A.; Isola, M.; Tascini, C.; Balestrieri, M. Mental health symptoms one year after acute COVID-19 infection: Prevalence and risk factors. Rev. Psiquiatr. Salud. Ment. 2022. [Google Scholar] [CrossRef] [PubMed]
- Damanti, S.; Cilla, M.; Cilona, M.; Fici, A.; Merolla, A.; Pacioni, G.; De Lorenzo, R.; Martinenghi, S.; Vitali, G.; Magnaghi, C.; et al. Prevalence of Long COVID-19 Symptoms After Hospital Discharge in Frail and Robust Patients. Front. Med. 2022, 9, 834887. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Martín-Guerrero, J.D.; Cancela-Cilleruelo, I.; Moro-López-Menchero, P.; Rodríguez-Jiménez, J.; Pellicer-Valero, O.J. Trajectory curves of post-COVID anxiety/depressive symptoms and sleep quality in previously hospitalized COVID-19 survivors: The LONG-COVID-EXP-CM multicenter study. Psychol. Med. 2022, 10, 1–2. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef] [PubMed]
- Garout, M.A.; Saleh, S.A.K.; Adly, H.M.; Abdulkhaliq, A.A.; Khafagy, A.A.; Abdeltawab, M.R.; Rabaan, A.A.; Rodriguez-Morales, A.J.; Al-Tawfiq, J.A.; Alandiyjany, M.N. Post-COVID-19 syndrome: Assessment of short- and long-term post-recovery symptoms in recovered cases in Saudi Arabia. Infection 2022, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gasnier, M.; Choucha, W.; Radiguer, F.; Faulet, T.; Chappell, K.; Bougarel, A.; Kondarjian, C.; Thorey, P.; Baldacci, A.; Ballerini, M.; et al. Comorbidity of long COVID and psychiatric disorders after a hospitalisation for COVID-19: A cross-sectional study. J. Neurol. Neurosurg. Psychiatry 2022, 93, 1091–1098. [Google Scholar] [CrossRef]
- Magdy, R.; Elmazny, A.; Soliman, S.H.; Elsebaie, E.H.; Ali, S.H.; Abdel Fattah, A.M.; Hassan, M.; Yassien, A.; Mahfouz, N.A.; Elsayed, R.M.; et al. Post-COVID-19 neuropsychiatric manifestations among COVID-19 survivors suffering from migraine: A case-control study. J. Headache Pain 2022, 23, 101. [Google Scholar] [CrossRef]
- Matsumoto, K.; Hamatani, S.; Shimizu, E.; Käll, A.; Andersson, G. Impact of post-COVID conditions on mental health: A cross-sectional study in Japan and Sweden. BMC Psychiatry 2022, 22, 237. [Google Scholar]
- Rivera-Izquierdo, M.; Láinez-Ramos-Bossini, A.J.; de Alba, I.G.; Ortiz-González-Serna, R.; Serrano-Ortiz, Á.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Cervilla, J.A. Long COVID 12 months after discharge: Persistent symptoms in patients hospitalised due to COVID-19 and patients hospitalised due to other causes-a multicentre cohort study. BMC Med. 2022, 20, 92. [Google Scholar] [CrossRef]
- Stallmach, A.; Kesselmeier, M.; Bauer, M.; Gramlich, J.; Finke, K.; Fischer, A.; Fleischmann-Struzek, C.; Heutelbeck, A.; Katzer, K.; Mutschke, S.; et al. Comparison of fatigue, cognitive dysfunction and psychological disorders in post-COVID patients and patients after sepsis: Is there a specific constellation? Infection 2022, 50, 661–669. [Google Scholar] [CrossRef]
- Strahm, C.; Seneghini, M.; Güsewell, S.; Egger, T.; Leal, O.; Brucher, A.; Lemmenmeier, E.; Kleeb, D.M.; Möller, J.C.; Rieder, P.; et al. Symptoms Compatible with Long Coronavirus Disease (COVID) in Healthcare Workers With and Without Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection—Results of a Prospective Multicenter Cohort. Clin. Infect. Dis. 2022, 75, e1011–e1019. [Google Scholar] [CrossRef] [PubMed]
- Voruz, P.; Cionca, A.; Jacot de Alcântara, I.; Nuber-Champier, A.; Allali, G.; Benzakour, L.; Thomasson, M.; Lalive, P.H.; Lövblad, K.O.; Braillard, O.; et al. Functional connectivity underlying cognitive and psychiatric symptoms in post-COVID-19 syndrome: Is anosognosia a key determinant? Brain Commun. 2022, 4, fcac057. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Salgado, J.; Allande-Cussó, R.; Domínguez-Salas, S.; García-Iglesias, J.J.; Coronado-Vázquez, V.; Ruiz-Frutos, C. Design of Fear and Anxiety of COVID-19 Assessment Tool in Spanish Adult Population. Brain Sci. 2021, 11, 328. [Google Scholar] [CrossRef] [PubMed]
- Rudroff, T.; Workman, C.D.; Bryant, A.D. Potential Factors That Contribute to Post-COVID-19 Fatigue in Women. Brain Sci. 2022, 12, 556. [Google Scholar] [CrossRef]
- Ortelli, P.; Ferrazzoli, D.; Sebastianelli, L.; Maestri, R.; Dezi, S.; Spampinato, D.; Saltuari, L.; Alibardi, A.; Engl, M.; Kofler, M.; et al. Altered motor cortex physiology and dysexecutive syndrome in patients with fatigue and cognitive difficulties after mild COVID-19. Eur. J. Neurol. 2022, 29, 1652–1662. [Google Scholar] [CrossRef]
- Tansey, C.M.; Louie, M.; Loeb, M.; Gold, W.L.; Muller, M.P.; de Jager, J.; Cameron, J.I.; Tomlinson, G.; Mazzulli, T.; Walmsley, S.L.; et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch. Intern. Med. 2007, 167, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, K.; Chan, D. The emergence of cognitive COVID. World Psychiatry 2021, 20, 52–53. [Google Scholar] [CrossRef]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 Affects the Brain. JAMA Psychiatry 2021, 78, 682–683. [Google Scholar] [CrossRef]
- de Erausquin, G.A.; Snyder, H.; Brugha, T.S.; Seshadri, S.; Carrillo, M.; Sagar, R.; Huang, Y.; Newton, C.; Tartaglia, C.; Teunissen, C.; et al. Chronic neuropsychiatric sequelae of SARS-CoV-2: Protocol and methods from the Alzheimer’s Association Global Consortium. Alzheimer’s Dement 2022, 8, e12348. [Google Scholar] [CrossRef]
- Son, G.; Jahanshahi, A.; Yoo, S.J.; Boonstra, J.T.; Hopkins, D.A.; Steinbusch, H.W.M.; Moon, C. Olfactory neuropathology in Alzheimer’s disease: A sign of ongoing neurodegeneration. BMB Rep. 2021, 54, 295–304. [Google Scholar] [CrossRef]
- Knapp, M.; Wong, G. Economics and mental health: The current scenario. World Psychiatry 2020, 19, 3–14. [Google Scholar] [CrossRef]
- Kuzman, M.R.; Curkovic, M.; Wasserman, D. Principles of mental health care during the COVID-19 pandemic. Eur. Psychiatry 2020, 63, e45. [Google Scholar] [CrossRef]
- McDaid, D. Viewpoint: Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry 2021, 64, e32. [Google Scholar] [CrossRef]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry 2020, 19, 406–407. [Google Scholar] [CrossRef]
- Wasserman, D.; Iosue, M.; Wuestefeld, A.; Carli, V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry 2020, 19, 294–306. [Google Scholar] [CrossRef]
- Menculini, G.; Tortorella, A.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Luciano, M.; Nanni, M.G.; Pompili, M.; et al. Access to Mental Health Care during the First Wave of the COVID-19 Pandemic in Italy: Results from the COMET Multicentric Study. Brain Sci. 2021, 11, 1413. [Google Scholar] [CrossRef]
- Volpe, U.; Fiorillo, A.; Luciano, M.; Del Vecchio, V.; Palumbo, C.; Calò, S.; Piras, S.; Signorelli, M.; Filippo, D.; Piselli, M.; et al. Pathways to mental health care in Italy: Results from a multicenter study. Int. J. Soc. Psychiatry 2014, 60, 508–513. [Google Scholar] [CrossRef] [Green Version]
- Serrano-Castro, P.J.; Estivill-Torrús, G.; Cabezudo-García, P.; Reyes-Bueno, J.A.; Ciano Petersen, N.; Aguilar-Castillo, M.J.; Suárez-Pérez, J.; Jiménez-Hernández, M.D.; Moya-Molina, M.Á.; Oliver-Martos, B.; et al. Impact of SARS-CoV-2 infection on neurodegenerative and neuropsychiatric diseases: A delayed pandemic? Neurologia 2020, 35, 245–251. [Google Scholar] [CrossRef]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Soh, H.L.; Ho, R.C.; Ho, C.S.; Tam, W.W. Efficacy of digital cognitive behavioural therapy for insomnia: A meta-analysis of randomised controlled trials. Sleep Med. 2020, 75, 315–325. [Google Scholar] [CrossRef]
- Reynolds, C.F. Optimizing personalized management of depression: The importance of real-world contexts and the need for a new convergence paradigm in mental health. World Psychiatry 2020, 19, 266–268. [Google Scholar] [CrossRef]


{kind=link}
| Spain | 5 |
| Saudi Arabia | 3 |
| Japan | 3 * |
| Italy | 3 |
| USA | 3 |
| Switzerland | 2 * |
| Egypt | 1 |
| France | 1 |
| Germany | 1 |
| Author(s), Year, Country, Study Design | Sample Size | Inclusion Criteria | Definition of Post-COVID Syndrome | Assessment Tools | Main Results |
|---|---|---|---|---|---|
| Alghamdi et al. (2022), Saudi Arabia [38] Online survey | N = 2218 participants | Laboratory-confirmed SARS-CoV-2 infection, as evidenced by a positive real-time reverse transcriptase-polymerase chain reaction test result. | Persistent neuropsychiatric disorders and conditions affecting the peripheral nerves from <1 to >6 months after COVID-19 infection. | Ad hoc questionnaire | Post-COVID neuropsychiatric symptoms, including altered cognitive skills, anosmia and dysgeusia, tinnitus, depression, and sleep disorders, were recorded in 18.9–63.9% of the participants with COVID-19. |
| Alradini et al. (2022), Saudi Arabia [55] Multicenter, retrospective cross-sectional study | N = 1000 participants | All patients with confirmed SARS-CoV-2 infection diagnosed At least 18 years old | Signs and symptoms that developed during or after an infection consistent with COVID-19, continuing for more than 12 weeks, and not explained by an alternative diagnosis. | Clinical records/telephone interview | Most common-to-late symptoms include loss of smell, loss of taste, fatigue, shortness of breath, and cough (52.4%, 31.1%, 11.5%, 10.2%, and 8.9% of patients with late symptoms, respectively). |
| Cacciatore et al. (2022), Italy [61] Cohort study | N = 105 patients | Patients who survived COVID-19 and were discharged from the COVID-19 Unit of the ASST Spedali Civili Hospital | No clear definition | WHODAS-12 Hospital Anxiety and Depression Scale (HADS) Pittsburgh Sleep Quality Index (PSQI) Montreal Cognitive Assessment (MoCA) Cumulative Illness Rating Scale (CIRS) COVID-19 severity | The most common symptoms at follow-up were sleep disturbances, cognitive dysfunctions, and fatigue. Cognitive dysfunction, anxiety, fatigue, and hyposmia/hypogeusia explained 28.8% of WHODAS-12 variation. |
| Calabria et al. (2022), Spain [60] Cross-sectional study | N = 136 patients with subjective cognitive complaints after SARS-CoV-2 infection | Having had COVID-19 symptoms and confirmed positive for SARS-CoV-2 via polymerase chain reaction (PCR) and/or serology (anti-SARS-CoV2 IgM or IgG) Being referred for neuropsychological assessment after reporting subjective cognitive complaints Being 18 + years old | No specific definition | Modified Fatigue Impact Scale Anxiety and Depression Scale (HADS) Frontal Systems Behavior Scale (FrSBe) European Quality of Life-5 Dimensions (EQ-5D) Brunnsviken Brief Quality of life scale (BBQ) World Health Organization Quality of Life—BREF (WHOQOL-BREF) | A total of 82.3% of individuals reported clinically significant levels of fatigue. Patients with clinically significant fatigue showed worse quality of life and poor daily functioning. Depressive symptoms and anxiety were reported in 23.5% and 35.3% of patients, respectively. |
| Chen et al. (2022), USA [62] Case-control study | Conga cohort: N = 200 COVID patients Control cohort; N = 342 patients. | Conga cohort: Patients testing positive for COVID-19 infection by respiratory swab or saliva sample RT-PCR with a minimum of four weeks from the date of confirmed COVID-19 infection or four weeks after the patient was discharged from the hospital Older than 18 years old Control cohort: patients enrolled in either the Georgia Cardiovascular Twin Study or the Georgia Stress and Heart study | Patients who were on a minimum of four weeks from the date of confirmed COVID-19 infection or four weeks after the patient was discharged from the hospital | Montreal Cognitive Assessment (MoCA) NIH Toolbox (NIH-TB) for the Assessment of Neurological and Behavioral Function studies. A University of Pennsylvania Smell Identification Test (UPSIT) A Waterless Empirical Taste Test (WETT) Patient Health Questionnaire-9 (PHQ-9) Generalized Anxiety Disorder-7 (GAD-7) | The most commonly reported COVID-19 symptom was fatigue (68.5%). In 25% of cases PHQ-9 criteria for depression were met. In 18% of cases GAD-7 criteria for anxiety were met. A total of 47% of patients met the criteria for mild cognitive impairment at MoCA. |
| Colizzi et al. (2022), Italy [63] Prospective study | N = 479 adult patients. | Consecutive patients, aged 18 years or older, admitted or seen on an outpatient basis at the hospital Infectious Disease Department, with a confirmed diagnosis of COVID-19. | “Post-COVID” symptoms had to be developed during or after COVID-19, and not to be explained by an alternative diagnosis in a follow-up period of 12 months after COVID-19 onset | Ad hoc questionnaire for evaluating clinical conditions | Significant increase was observed only for symptoms of psychiatric disorders (10.2%) and lack of concentration and focus (20%) |
| Damanti et al. (2022), Italy [64] Cross-sectional study | Three hundred and eighty-two patients | Patients aged 65 years or older, who attended a dedicated post-COVID-19 outpatient clinic. These patients were previously hospitalized for SARS-CoV-2 pneumonia in the Internal Medicine Department of the San Raffaele University Hospital, Milan, Italy and were discharged alive | Lack of specific definition | Medical examination, anthropometric measurements, strength assistance with walking, rising from a chair, climbing stairs, and falls (SARC-F) Short Physical Performance Battery (SPPB) test Mini Nutritional Assessment Short Form (MNA-SF) questionnaire EuroQol Group Health Questionnaire 5D-3L Visual Analog Scale (VAS) | Frailty was significantly associated with confusion, malnutrition, risk of sarcopenia, impaired muscle performance, complaints in mobility, in self-care, and in performing usual activities of daily life |
| De las Penas et al. (2022a), Spain [65] Multicenter cohort study | From 2000 patients randomly selected, 1593 (80.9%) were assessed at T1 and T2 months after hospital discharge | Individuals with a diagnosis of SARS-CoV-2 by RT-PCR technique and radiological findings hospitalized during the first wave of the pandemic | No clear definition of timeframe for evaluating post-COVID syndrome | The Hospital Anxiety and Depression Scale (HADS) The Pittsburgh Sleep Quality Index (PSQI) | Although the prevalence of post-COVID anxiety and depressive symptoms was considerable, a potential recovery over the following months was observed, explaining the downward prevalence trend |
| De las Penas et al. (2022b), Spain [66] Multicenter cohort study | From 2000 patients randomly selected, a total of 1969 participants (Mean age: 61, SD: 16 years, 46.4% women) were finally included | Individuals with a diagnosis of SARS-CoV-2 by RT-PCR technique and radiological findings hospitalized during the first wave of the pandemic | No clear definition of timeframe for evaluating post-COVID syndrome | The Hospital Anxiety and Depression Scale (HADS) The Pittsburgh Sleep Quality Index (PSQI) | The number of post-COVID symptoms was 2.25 for females and 1.5 for males. After adjusting by all variables, female gender was associated with 3 post-COVID symptoms, the presence of post-COVID fatigue, dyspnea, pain, hair loss, ocular problems, depressive levels, and worse sleep quality |
| Farooqui et al. (2022), USA [56] Retrospective study | N = 30 individuals with documented COVID-19 illness | Adult patients referred and assessed for psychiatric complications at a university hospital-based post-COVID-19 Recovery Program | Lack of definition of post-COVID syndrome | Physical Health Questionnaire-9 (PHQ-9) Generalized Anxiety Disorder-7 (GAD-7) Columbia Suicide Severity Rating Scale (C-SSRS) Fatigue Severity Scale (FSS) Montreal Cognitive Assessment (MOCA) | A total of 68% of the patient population had a combination of depression and/or anxiety in addition to reported complaints of fatigue and cognitive problems. Out of these, 14 (47%) met the criteria for a primary depressive disorder, followed by 17% (n = 5) who met the criteria for a primary anxiety disorder and 7% (n = 2) who met the clinical criteria for both a depressive disorder and an anxiety disorder |
| Garout et al. (2022), Saudi Arabia [67] Online survey | N = 744 participants who recovered from COVID-19 disease | Participants declared that they have been diagnosed with COVID-19 by confirmed (SARS-CoV-2) polymerase chain reaction (PCR) Participants who have had COVID-19 at least 2 months before the questionnaire | Post-COVID syndrome defined as having been infected by COVID-19 at least 2 months before | COVID-19 Yorkshire Rehabilitation Screening (C19-YRS) | Out of 744 participants, in 21.4% (N = 189) experienced continual symptoms including anxiety in 13.2% (N = 98) and depression in 9.5% (N = 70) |
| Gasnier et al. (2022), France [68] Cross-sectional study | N = 170 patients | Age ≥18 years old Hospitalized for >24 h primarily related to COVID-19, with a SARS-CoV-2 infection admitted in intensive care unit during acute phase and/or with at least one long COVID complaint (screened by telephone consultation 4 months after acute COVID-19) | Complaints had to have appeared or worsened since acute COVID-19 infection, and to persist since hospital discharge | Insomnia Severity Index (ISI) Hospital Anxiety and Depression Scale-Anxiety subscale (HAD-A) Beck Depression Inventory-13 items (BDI) PTSD CheckList for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (PCL-5) | Fatigue (44.1%), respiratory complaints (43.5%), cognitive complaints (23.7%), and paraesthesia (20.9%) were the most common long COVID complaints. The number of long COVID complaints was significantly associated with insomnia, anxiety, depression, and post-traumatic stress symptoms. The number of long COVID complaints was greater in patients with a psychiatric disorder, in those with a new-onset psychiatric disorder and in those with a significant suicide risk compared with patients without any past or current psychiatric disorder |
| Iosifescu et al. (2022), USA [57] Retrospective study | N = 18,811 COVID-19 patients N= 5772 flu patients | COVID-19 patients with neuro-Post Acute Syndrome COVID (PASC) Symptoms COVID-19 patients without neuro-PASC symptoms Flu patients with neurological and neuropsychiatric symptoms | Persistence of symptoms: at least 2 weeks past the date of COVID-19 or flu diagnosis | Clinical records/clinical assessment | Common neuro-PASC symptoms were anxiety (30%), depression (27%), dizziness (22%), altered mental status (17%), chronic headaches (17%), and nausea (11%). The average time to neuro-PASC onset was 138 days |
| Jozuka et al. (2021), Japan [59] Case report | 55-year-old female with COVID-19 accompanied by mild respiratory symptoms showed delusion, psychomotor excitement, and poor communication ability during quarantine outside the hospital. | Not applicable | Lack of specific definition | Clinical records | Case was severe and long-lasting. Neuropsychiatric symptoms after mild respiratory symptoms caused by COVID-19. Numerous residual neuropsychiatric symptoms, such as insomnia, fatigue, loss of concentration, and unsteadiness while walking, which have been reported as neuropsychiatric sequelae of COVID-19. These symptoms were associated also with slow EEG waves, postural tachycardia, and disturbed frontal lobe function |
| Magdy et al. (2022), Egypt [69] Case–control study | N = 408 patients Group 1: N = 204 COVID-19 survivors with a confirmed history of pre- COVID episodic migraine (migraine headache sufferers) Group 2: N = 204 COVID-19 survivors with no history of any primary headache disorders preceding COVID-19 infection (control) | Older than 18 years Confirmed history of COVID-19 diagnosis by reverse transcription-polymerase chain reaction (RT-PCR) by nasal and oropharynx swabs | After 3 months of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection | A detailed general, neurological and otolaryngological examination was done for all patients who attended the face-to-face interview. The diagnostic and Statistical Manual of Mental Disorders (DSM-5) was applied for diagnosing insomnia, depression, and anxiety disorders The Montreal Cognitive Assessment (MoCA) The post-COVID-19 Functional Status scale | The reported significant post-COVID-19 neuropsychiatric symptoms in migraine patients compared to controls were fatigue, anosmia/hyposmia, cacosmia, depression, anxiety, insomnia, and headache. There was no statistically significant difference between migraine patients and controls regarding the post-COVID-19 functional status score |
| Matsumoto et al. (2022), Japan and Sweden [70] International and collaborative cross-sectional study (online). | N = 763 total participants N = 135 infected with COVID-19. N = 628 never been infected with COVID-19 | At least 18 years old Data collection carried out through Asmark companies in Japan and Prolific in Sweden online research platforms | Lack of definition of post-COVID syndrome | Ad hoc questionnaire for collecting data on COVID-19 The Fear of COVID-19 Scale (FCV-19S) Patient Health Questionnaire-9 (PHQ-9) General Anxiety Disorder-7 -item (GAD-7) Impact of Event Scale-Revised (IES-R) | For clinically significant syndromes of COVID-19-related anxiety, depression, general anxiety, and PTSD, the proportion of the participants, who exceeded the cut-off on each clinical symptom rating scale, were significantly high in the group that had developed COVID-19 with post-COVID conditions |
| Ohira et al., (Japan), 2022 [58] Descriptive case series study | N = 90 long COVID patients (39 male, 51 female) | Electronic medical records and clinical summaries of patients who visited the clinic and reported symptoms after recovering from the acute phase of COVID-19 All patients were over 15 years old at the time of their visit At least 2 months had elapsed since the diagnosis of COVID-19 or the end of hospitalization | At least 2 months had elapsed since the diagnosis of COVID-19 or the end of hospitalization | All patients were examined by physicians who were each certified as a Fellow of the Japanese Society of Internal Medicine, and board-certified neurologists of the Japanese Society of Neurology MRI scans were performed using a 3-Tesla MR scanner Olfactory acuity tests used the T&T olfactometer threshold test | The most common chief complaint was disturbance of smell and/or taste (38.9%), followed by memory disturbance (24.4%), fatigue (31.1%), headache (18.9%), hair loss (16.7%), and sleeping problems, including insomnia (13.3%) |
| Rivera-Izquierdo et al. (2022), Spain [71] Case-control study | N = 906 adult patients. N = 453 patients hospitalized due to COVID-19. N = 453 hospitalized due to other causes. | Randomly selected sample from all hospitalized patients, with laboratory-confirmed SARS-CoV-2 infection through PCR-positive samples | Modified version of the open-access Case Report Form of the Clinical Characterization Protocol for Severe Emerging Infections of the International Severe Acute Respiratory and Emerging Infection Consortium (ISARIC) Medical records | Most frequently occurring symptoms in the COVID-19 cohort were persistent pharyngeal symptoms, confusion or memory loss, thrombotic events, and anxiety. Patients hospitalized due to COVID-19 showed a higher prevalence of respiratory, neurological, and anxiety symptoms after adjusting for sex, age, ICU admission, and baseline comorbidities | |
| Stallmach et al. (2022), Germany [72] Prospective cohort study | N = 355 patients | Symptomatic post-COVID patients who visited out-patient clinics for post COVID-19 care | No clear definition of post-COVID syndrome | Fatigue Assessment Scale, FAS Brief Fatigue Inventory, BFI Depression module of the Patient Health Questionnaire, PHQ-9 Montreal Cognitive Assessment (MoCA) screening) Structured examination consisting of the evaluation of current and initial symptoms, treatment of the SARS-CoV-2 infection, body examination, and amnestic information | Fatigue or signs of depression were reported in 320 patients (90.1% of all patients). Chronic fatigue was found in 93.2% of patients. Depression was reported in 81.3% of patients. Cognitive dysfunction was found in 23.5% of patients |
| Strahm et al. (2022), Switzerland [73] Prospective observational study | N = 3346 participants. | Hospital employees from 23 healthcare institutions located in northern and eastern Switzerland | “Long post-COVID” = 13 to 24 weeks “Persistent post-COVID” = more than 24 weeks | Rivermead Post Concussion Questionnaire (RMEAD) score 9-item Fatigue Severity Scale (FSS) 8-item Patient Health Questionnaire (PHQ) 7-item General Anxiety Disorder (GAD) score | Symptoms included exhaustion/burnout in 33% of patients, nasopharyngeal swap (NPS)-positive vs. 25% in only seropositive and weakness/tiredness (34% and 25%, respectively). Clinically relevant fatigue was found in 10.6% of the sample |
| Voruz et al. (2022), Spain [74] Cross-sectional study | N = 102 patients. N = 26 anosognosics patients. N = 76 non-anosognosics patients. | Participants were recruited either via admission lists provided by their treating doctors or from the COVID-COG cohort. | Not a defined time frame for considering a post--COVID condition. | Beck Depression Inventory-Second Edition State–Trait Anxiety Inventory Apathy Motivation Index Posttraumatic Stress Disorder Checklist for DSM-5 Goldberg Mania Inventory Dissociative Experience Scale Perceived Stress Scale | Patients were first divided into two groups according to the to the presence or absence of anosognosia for memory deficits Only 15.6% of patients who presented a mild disease displayed anosognosia for memory dysfunction, compared with 32.4% of patients with a moderate presentation and 34.8% of patients with severe disease. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampogna, G.; Di Vincenzo, M.; Giallonardo, V.; Perris, F.; Volpicelli, A.; Del Vecchio, V.; Luciano, M.; Fiorillo, A. The Psychiatric Consequences of Long-COVID: A Scoping Review. J. Pers. Med. 2022, 12, 1767. https://doi.org/10.3390/jpm12111767
Sampogna G, Di Vincenzo M, Giallonardo V, Perris F, Volpicelli A, Del Vecchio V, Luciano M, Fiorillo A. The Psychiatric Consequences of Long-COVID: A Scoping Review. Journal of Personalized Medicine. 2022; 12(11):1767. https://doi.org/10.3390/jpm12111767
Chicago/Turabian StyleSampogna, Gaia, Matteo Di Vincenzo, Vincenzo Giallonardo, Francesco Perris, Antonio Volpicelli, Valeria Del Vecchio, Mario Luciano, and Andrea Fiorillo. 2022. "The Psychiatric Consequences of Long-COVID: A Scoping Review" Journal of Personalized Medicine 12, no. 11: 1767. https://doi.org/10.3390/jpm12111767
APA StyleSampogna, G., Di Vincenzo, M., Giallonardo, V., Perris, F., Volpicelli, A., Del Vecchio, V., Luciano, M., & Fiorillo, A. (2022). The Psychiatric Consequences of Long-COVID: A Scoping Review. Journal of Personalized Medicine, 12(11), 1767. https://doi.org/10.3390/jpm12111767