



Polygenic Risk Score and Risk Factors for Preeclampsia and Gestational Hypertension

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Gestational Hypertension/Preeclampsia Cases
2.3. Genotype and Phenotype Data
2.4. Procedure for Learning the Polygenic Risk Scores
2.5. Mendelian Randomization
2.6. SNP Annotation
3. Results
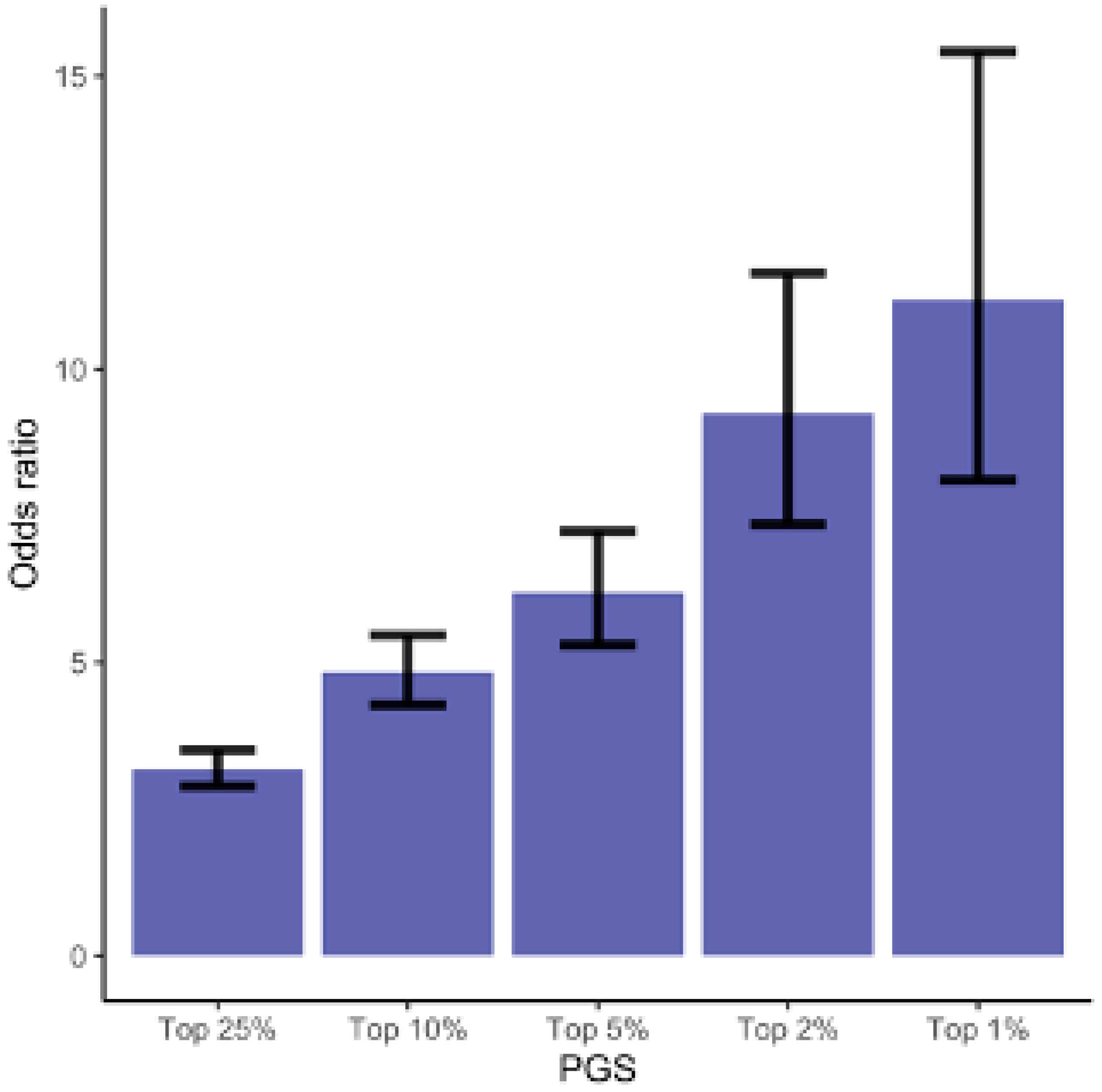
3.1. Polygenic Risk Score
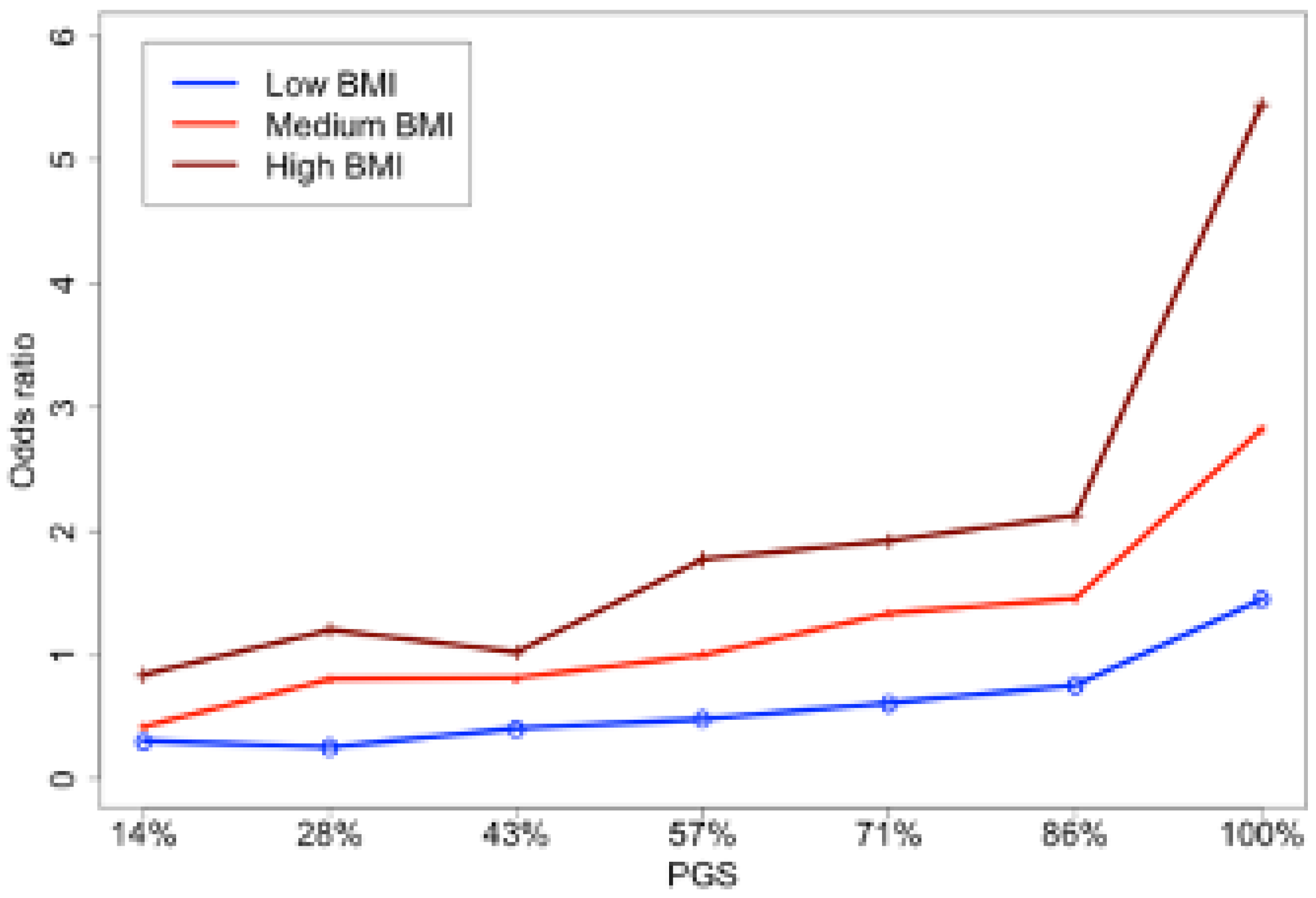
3.2. GHD Risk and BMI
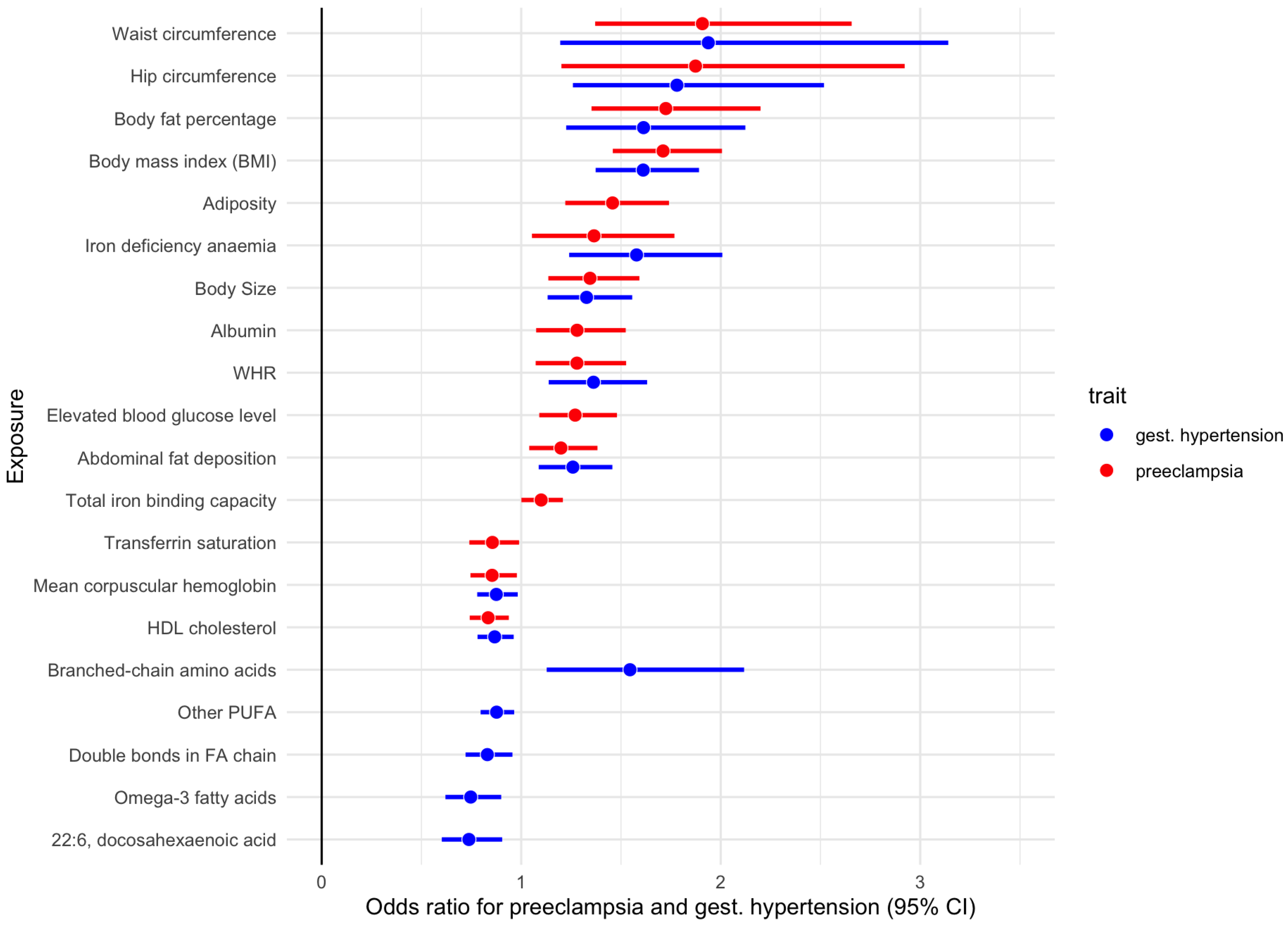
3.3. GHD Risk and Female-Specific Anthropometric Measures
3.4. GHD Risk and Other Biomarkers
4. Discussion
4.1. Functional Analysis
4.2. Risk Factors for GHD
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, K.; Brayboy, L.; Tripathi, A. Pre-eclampsia: A Scoping Review of Risk Factors and Suggestions for Future Research Direction. Regen. Eng. Transl. Med. 2022, 8, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Wisner, K. Gestational hypertension and preeclampsia. MCN Am. J. Matern. Nurs. 2019, 44, 170. [Google Scholar] [CrossRef]
- Jeyabalan, A. Epidemiology of preeclampsia: Impact of obesity. Nutr. Rev. 2013, 71, S18–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, T.F.; Gyamfi-Bannerman, C.; Manuck, T. Low-dose aspirin use during pregnancy. Obstet. Gynecol. 2018, 132, E44–E52. [Google Scholar]
- Visintin, C.; Mugglestone, M.A.; Fields, E.J.; Jacklin, P.; Murphy, M.S.; Pollard, A.J. Management of bacterial meningitis and meningococcal septicaemia in children and young people: Summary of NICE guidance. BMJ 2010, 340, c3209. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Wright, D.; Syngelaki, A.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; Greco, E.; Wright, A.; Maclagan, K.; et al. Comparison of diagnostic accuracy of early screening for pre-eclampsia by NICE guidelines and a method combining maternal factors and biomarkers: Results of SPREE. Ultrasound Obstet. Gynecol. 2018, 51, 743–750. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, T.M.; Walker, S.P.; Hannan, N.J.; Tong, S.; Kaitu’u-Lino, T.J. Clinical tools and biomarkers to predict preeclampsia. EBioMedicine 2022, 75, 103780. [Google Scholar] [CrossRef]
- Cnattingius, S.; Reilly, M.; Pawitan, Y.; Lichtenstein, P. Maternal and fetal genetic factors account for most of familial aggregation of preeclampsia: A population-based Swedish cohort study. Am. J. Med Genet. Part A 2004, 130, 365–371. [Google Scholar] [CrossRef]
- Miller, E.C.; Wilczek, A.; Bello, N.A.; Tom, S.; Wapner, R.; Suh, Y. Pregnancy, preeclampsia and maternal aging: From epidemiology to functional genomics. Ageing Res. Rev. 2022, 73, 101535. [Google Scholar] [CrossRef]
- Zhang, G.; Zhao, J.; Yi, J.; Luan, Y.; Wang, Q. Association between gene polymorphisms on chromosome 1 and susceptibility to pre-eclampsia: An updated meta-analysis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2016, 22, 2202. [Google Scholar] [CrossRef] [Green Version]
- Hillermann, R.; Carelse, K.; Gebhardt, G.S. The Glu298Asp variant of the endothelial nitric oxide synthase gene is associated with an increased risk for abruptio placentae in pre-eclampsia. J. Hum. Genet. 2005, 50, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Rouault, C.; Clément, K.; Zhu, W.; Degrelle, S.A.; Charles, M.A.; Heude, B.; Fournier, T. C1431T Variant of PPARγ Is Associated with Preeclampsia in Pregnant Women. Life 2021, 11, 1052. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.C.; Gomes, C.E.M.; Duggal, P.; De Paula Holanda, I.; de Lima, A.S.; do Nascimento, P.R.P.; Jeronimo, S.M.B. Genetic association of ERAP1 and ERAP2 with eclampsia and preeclampsia in northeastern Brazilian women. Sci. Rep. 2021, 11, 6764. [Google Scholar] [CrossRef]
- Oudejans, C.; Michel, O.; Janssen, R.; Habets, R.; Poutsma, A.; Sistermans, E.; Weiss, M.; Incarnato, D.; Oliviero, S.; Kleiverda, G.; et al. Susceptibility allele-specific loss of miR-1324-mediated silencing of the INO80B chromatin-assembly complex gene in pre-eclampsia. Hum. Mol. Genet. 2015, 24, 118–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zusterzeel, P.L.; Peters, W.H.; De Bruyn, M.A.; Knapen, M.F.; Merkus, H.M.; Steegers, E.A. Glutathione S-transferase isoenzymes in decidua and placenta of preeclamptic pregnancies. Obstet. Gynecol. 1999, 94, 1033–1038. [Google Scholar] [PubMed]
- Xin, Q.; Han, Y.; Jiang, W.; Wang, J.; Luan, Y.; Ji, Q.; Sun, W. Genetic susceptibility analysis of FGF5 polymorphism to preeclampsia in Chinese Han population. Mol. Genet. Genom. 2022, 297, 791–800. [Google Scholar] [CrossRef]
- Uz, E.; Dolen, I.; Al, A.R.; Ozcelik, T. Extremely skewed X-chromosome inactivation is increased in pre-eclampsia. Hum. Genet. 2007, 121, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Che, G.; Liu, F.; Chang, L.; Jiang, Y. Association of IL-10-819C/T, -592A/C polymorphisms with the risk of preeclampsia: An updated meta-analysis. Medicine 2021, 100, 41. [Google Scholar] [CrossRef]
- Hong, X.; Rosenberg, A.Z.; Zhang, B.; Binns-Roemer, E.; David, V.; Lv, Y.; Hjorten, R.C.; Reidy, K.J.; Chen, T.K.; Wang, G.; et al. Joint associations of maternal-fetal APOL1 genotypes and maternal country of origin with preeclampsia risk. Am. J. Kidney Dis. 2021, 77, 879–888. [Google Scholar] [CrossRef]
- Tyrmi, J.S.; Kaartokallio, T.; Lokki, A.I.; Jääskeläinen, T.; Kortelainen, E.; Ruotsalainen, S.S.; Karjalainen, J.; Ripatti, S.; Laisk, T.; Kettunen, J.; et al. GWAS of preeclampsia and hypertensive disorders of pregnancy uncovers genes related to cardiometabolic, endothelial and placental function. medRxiv 2022. [Google Scholar] [CrossRef]
- Steinthorsdottir, V.; McGinnis, R.; Williams, N.O.; Stefansdottir, L.; Thorleifsson, G.; Shooter, S.; Fadista, J.; Sigurdsson, J.K.; Auro, K.M.; Berezina, G.; et al. Genetic predisposition to hypertension is associated with preeclampsia in European and Central Asian women. Nat. Commun. 2020, 11, 5976. [Google Scholar] [CrossRef] [PubMed]
- Perisic, M.M.; Vladimir, K.; Storga, M.; Mostashari, A.; Khanin, R. Polygenic Risk Score and Risk Factors for Gestational Diabetes. J. Pers. Med. 2022, 12, 1381. [Google Scholar] [CrossRef] [PubMed]
- Oscanoa, J.; Sivapalan, L.; Gadaleta, E.; Dayem Ullah, A.Z.; Lemoine, N.; Chelala, C. SNPnexus: A web server for functional annotation of human genome sequence variation (2020 update). Nucleic Acids Res. 2020, 48, W185–W192. [Google Scholar] [CrossRef] [PubMed]
- Dayem Ullah, A.Z.; Oscanoa, J.; Wang, J.; Nagano, A.; Lemoine, N.R.; Chelala, C. SNPnexus: Assessing the functional relevance of genetic variation to facilitate the promise of precision medicine. Nucleic Acids Res. 2018, 46, W109–W113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Taskesen, E.; van Bochoven, A.; Posthuma, D. Functional mapping and annotation of genetic associations with FUMA. Nat. Commun. 2017, 8, 1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motedayen, M.; Rafiei, M.; Tavirani, M.R.; Sayehmiri, K.; Dousti, M. The relationship between body mass index and preeclampsia: A systematic review and meta-analysis. Int. J. Reprod. Biomed. 2019, 17, 463. [Google Scholar] [CrossRef]
- Kazemian, E.; Sotoudeh, G.; Dorosty-Motlagh, A.R.; Eshraghian, M.R.; Bagheri, M. Maternal obesity and energy intake as risk factors of pregnancy-induced hypertension among Iranian women. J. Health Popul. Nutr. 2014, 32, 486. [Google Scholar] [CrossRef]
- Said, M.A.; Verweij, N.; van der Harst, P. Associations of combined genetic and lifestyle risks with incident cardiovascular disease and diabetes in the UK Biobank Study. JAMA Cardiol. 2018, 3, 693–702. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, E.; Glymour, M.M.; Holmes, M.V.; Kang, H.; Morrison, J.; Munafò, M.R.; Palmer, T.; Schooling, C.M.; Wallace, C.; Zhao, Q.; et al. Mendelian randomization. Nat. Rev. Methods Prim. 2022, 2, 1–21. [Google Scholar] [CrossRef]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7, e34408. [Google Scholar] [CrossRef]
- Ardissino, M.; Slob, E.A.; Millar, O.; Reddy, R.K.; Lazzari, L.; Patel, K.H.K.; Ryan, D.; Johnson, M.R.; Gill, D.; Ng, F.S. Maternal Hypertension Increases Risk of Preeclampsia and Low Fetal Birthweight: Genetic Evidence From a Mendelian Randomization Study. Hypertension 2022, 79, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Sulc, J.; Sonrel, A.; Mounier, N.; Auwerx, C.; Marouli, E.; Darrous, L.; Draganski, B.; Kilpeläinen, T.O.; Joshi, P.; Loos, R.J.; et al. Composite trait Mendelian randomization reveals distinct metabolic and lifestyle consequences of differences in body shape. Commun. Biol. 2021, 4, 1064. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Zingheim, R.W.; King, I.B.; Zebelman, A.M. Omega-3 fatty acids in maternal erythrocytes and risk of preeclampsia. Epidemiology 1995, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Young, M.F.; Oaks, B.M.; Tandon, S.; Martorell, R.; Dewey, K.G.; Wendt, A.S. Maternal hemoglobin concentrations across pregnancy and maternal and child health: A systematic review and meta-analysis. Ann. N. Y. Acad. Sci. 2019, 1450, 47–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afrose, D.; Chen, H.; Ranashinghe, A.; Liu, C.C.; Henessy, A.; Hansbro, P.M.; McClements, L. The diagnostic potential of oxidative stress biomarkers for preeclampsia: Systematic review and meta-analysis. Biol. Sex Differ. 2022, 13, 26. [Google Scholar] [CrossRef]
- Chaemsaithong, P.; Sahota, D.S.; Poon, L.C. First trimester preeclampsia screening and prediction. Am. J. Obstet. Gynecol. 2020, 226, S1071–S1097.e2. [Google Scholar] [CrossRef]
- Benny, P.A.; Alakwaa, F.M.; Schlueter, R.J.; Lassiter, C.B.; Garmire, L.X. A review of omics approaches to study preeclampsia. Placenta 2020, 92, 17–27. [Google Scholar] [CrossRef]
- Adeyemo, A.; Balaconis, M.K.; Darnes, D.R.; Fatumo, S.; Granados Moreno, P.; Hodonsky, C.J.; Inouye, M.; Kanai, M.; Kato, K.; Knoppers, B.M.; et al. Responsible use of polygenic risk scores in the clinic: Potential benefits, risks and gaps. Nat. Med. 2021, 27, 1876–1884. [Google Scholar] [CrossRef]
- Ren, M.; Ng, F.L.; Warren, H.R.; Witkowska, K.; Baron, M.; Jia, Z.; Cabrera, C.; Zhang, R.; Mifsud, B.; Munroe, P.B.; et al. The biological impact of blood pressure-associated genetic variants in the natriuretic peptide receptor C gene on human vascular smooth muscle. Hum. Mol. Genet. 2018, 27, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Burchakov, D.I.; Kuznetsova, I.V.; Uspenskaya, Y.B. Omega-3 long-chain polyunsaturated fatty acids and preeclampsia: Trials say “no,” but is it the final word? Nutrients 2017, 9, 1364. [Google Scholar] [CrossRef] [Green Version]
- Konuma, T.; Okada, Y. Statistical genetics and polygenic risk score for precision medicine. Inflamm. Regen. 2021, 41, 18. [Google Scholar] [CrossRef] [PubMed]
- Aghamohammadi, A.; Zafari, M.; Tofighi, M. High maternal hemoglobin concentration in first trimester as risk factor for pregnancy induced hypertension. Casp. J. Intern. Med. 2011, 2, 194. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Term | Estimate | std.error | Statistic | p-Value | Overlapped Gene | Nearest Upstream Gene | Nearest Downstream Gene |
|---|---|---|---|---|---|---|---|
| rs1173743 | 0.1453 | 0.031 | 4.712 | NPR3 | |||
| rs4660586 | −0.1570 | 0.034 | −4.603 | HIVEP3 | |||
| rs77979097 | 0.3020 | 0.071 | 4.266 | CSMD1 | |||
| rs29282 | 0.2175 | 0.053 | 4.128 | FMR1 | |||
| rs144401118 | 0.5282 | 0.130 | 4.068 | RP11-102N11.1 | SMLR1 | ||
| rs167479 | −0.1247 | 0.031 | −4.000 | 0.0001 | RGL3 | ||
| rs193168008 | 1.1161 | 0.282 | 3.965 | 0.0001 | LINC01019 | IRX1 | |
| rs534036441 | 0.9111 | 0.234 | 3.901 | 0.0001 | RNU6-163P | LINC00704 | |
| rs537363408 | 1.0705 | 0.275 | 3.893 | 0.0001 | RAD51B | ||
| rs190092234 | 1.1370 | 0.294 | 3.865 | 0.0001 | OSBPL6 | ||
| rs141667164 | 1.2467 | 0.326 | 3.830 | 0.0001 | DEF6 | PPARD | |
| rs115654387 | 0.4269 | 0.112 | 3.811 | 0.0001 | RP11-329N22.1 | RP11-334L9.1 | |
| rs544149038 | 1.3523 | 0.360 | 3.753 | 0.0002 | C14orf177 | AL132796.1 | |
| rs113046103 | 0.2230 | 0.060 | 3.703 | 0.0002 | SHANK2 | ||
| rs561028558 | 1.1228 | 0.303 | 3.700 | 0.0002 | TOP2A | ||
| rs191614564 | 0.4953 | 0.137 | 3.607 | 0.0003 | SCRT2 | SLC52A3 | |
| rs72674615 | 0.6124 | 0.170 | 3.604 | 0.0003 | LINC00609; PTCSC3 | ||
| rs113882455 | 0.4979 | 0.143 | 3.474 | 0.0005 | U40455.1 | RPL7L1P11 | |
| rs28558138 | 0.1080 | 0.031 | 3.452 | 0.0006 | TBC1D19 | STIM2 | |
| rs71519836 | 0.2241 | 0.065 | 3.447 | 0.0006 | MYOM2 | AC133633.2 | |
| rs80043362 | 0.1698 | 0.050 | 3.413 | 0.0006 | JPH2 | ||
| rs183374245 | 0.4377 | 0.129 | 3.400 | 0.0007 | CACNA2D1 | ||
| rs2409532 | −0.0991 | 0.030 | −3.342 | 0.0008 | AP000330.8 | ||
| rs145385264 | 0.2780 | 0.083 | 3.333 | 0.0009 | RP11-344P13.4 | ||
| rs558954655 | 0.7364 | 0.222 | 3.311 | 0.0009 | SPON2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perišić, M.M.; Vladimir, K.; Karpov, S.; Štorga, M.; Mostashari, A.; Khanin , R. Polygenic Risk Score and Risk Factors for Preeclampsia and Gestational Hypertension. J. Pers. Med. 2022, 12, 1826. https://doi.org/10.3390/jpm12111826
Perišić MM, Vladimir K, Karpov S, Štorga M, Mostashari A, Khanin R. Polygenic Risk Score and Risk Factors for Preeclampsia and Gestational Hypertension. Journal of Personalized Medicine. 2022; 12(11):1826. https://doi.org/10.3390/jpm12111826
Chicago/Turabian StylePerišić, Marija Majda, Klemo Vladimir, Sarah Karpov, Mario Štorga, Ali Mostashari, and Raya Khanin . 2022. "Polygenic Risk Score and Risk Factors for Preeclampsia and Gestational Hypertension" Journal of Personalized Medicine 12, no. 11: 1826. https://doi.org/10.3390/jpm12111826
APA StylePerišić, M. M., Vladimir, K., Karpov, S., Štorga, M., Mostashari, A., & Khanin , R. (2022). Polygenic Risk Score and Risk Factors for Preeclampsia and Gestational Hypertension. Journal of Personalized Medicine, 12(11), 1826. https://doi.org/10.3390/jpm12111826