
Pharmacogenomics of Cancer Pain Treatment Outcomes in Asian Populations: A Review

 , ,
, ,
Abstract
:1. Introduction
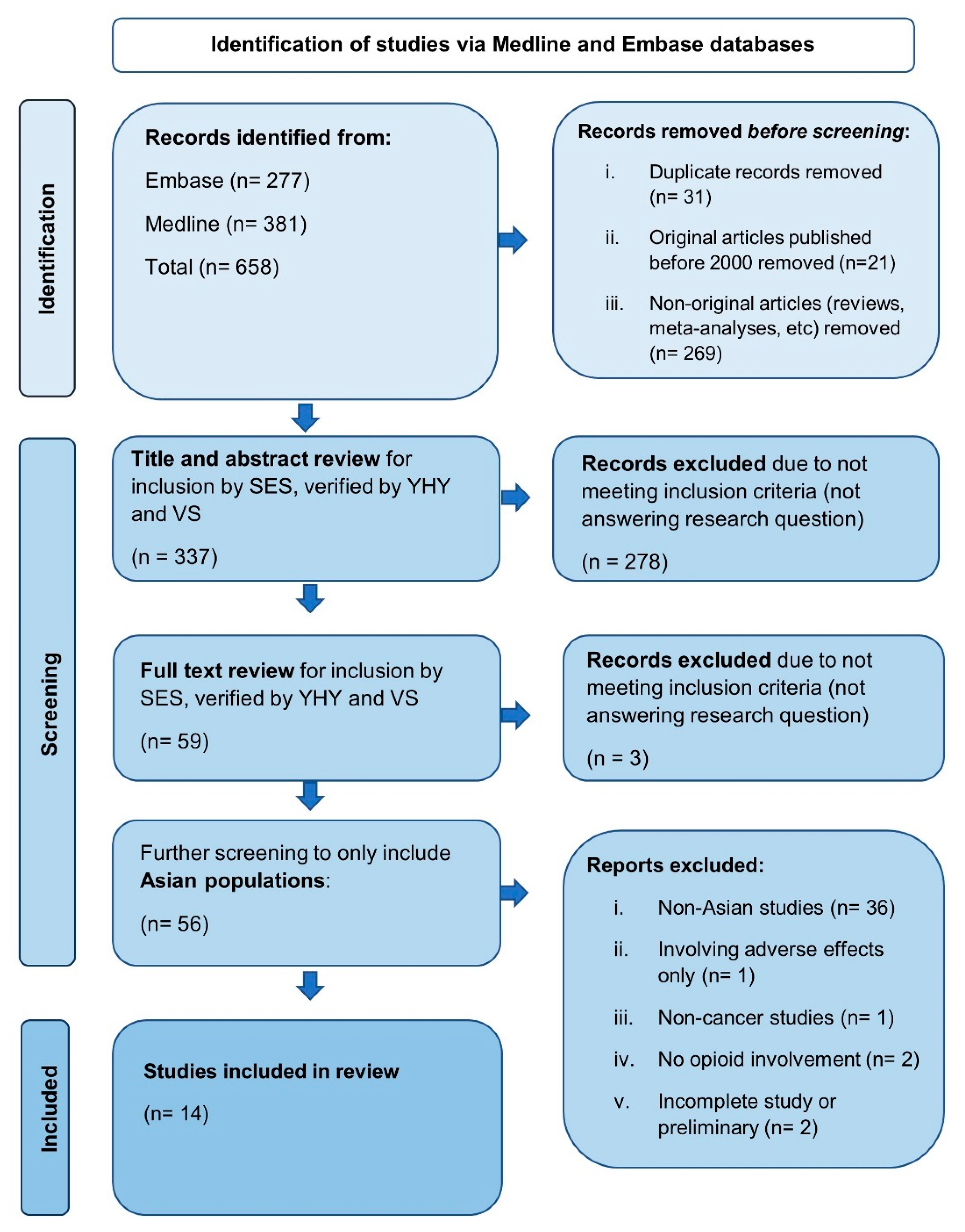
2. Materials and Methods
3. Results
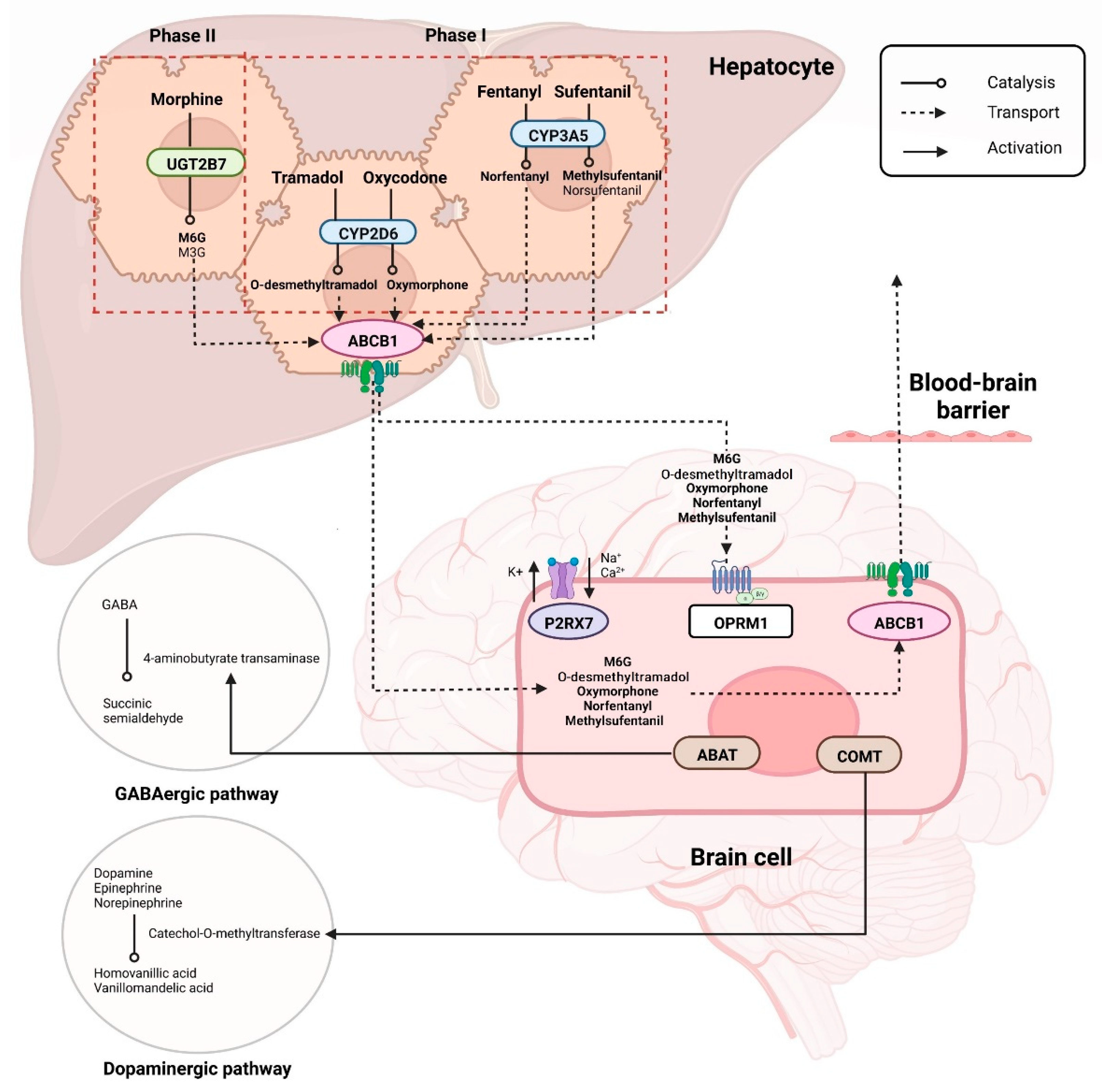
3.1. Phase I Opioid Metabolism: Cytochrome P450 Enzyme-Coding Genes
3.1.1. CYP2D6
- Tramadol
- Fentanyl
3.1.2. CYP3A5
3.2. Phase II Opioid Metabolism: UGT Enzyme-Coding Genes
UGT2B7
- Morphine
- Oxycodone
3.3. Opioid Receptor Gene
OPRM1
- Morphine
- Tramadol/Paracetamol combination
- Sufentanil
3.4. Neurotransmitter-Metabolizing Enzyme-Coding Genes
3.4.1. COMT
- Morphine
3.4.2. ABAT
- Multiple opioids
3.5. Drug Transporter Gene
ABCB1
- FentanylTakashina et al. investigated the impact of ABCB1 1236TT (rs1128503) on fentanyl pharmacokinetics among 60 Japanese cancer patients undergoing conversion to transdermal fentanyl from previous treatment of either oral morphine or oxycodone [25]. They showed that rescue medication was needed by fewer patients with the TT genotype compared to the other genotypes (p = 0.036) [25].
- SufentanilA study conducted among 225 Han Chinese patients with lung cancer reported the association of ABCB1 SNPs, rs2032582 and rs1128503 with the analgesic effect and dose of sufentanil taken for pain relief [30]. The doses of sufentanil required by double heterozygous patients at 6, 24 and 48 h were significantly higher than those consumed by patients who were wild type for both SNPs [30]. However, another SNP, wild type rs1045642 in ABCB1 did not show any significance (p > 0.05). There were no significant differences in the VAS scores at the three time points nor association with adverse effects [30].
- Multiple opioidsGong et al. evaluated the influence of ABCB1 C3435T (rs1045642) polymorphism on opioid requirements among 112 Chinese patients [34]. In this study, morphine, tramadol, sustained-release morphine, oxycodone, transdermal fentanyl and paracetamol were dosed according to the intensity of the cancer pain. The authors reported that compared with CC/CT genotypes, patients homozygous for the T allele received higher 24 h- and weight-surface area-adjusted-24 h- opioids doses (p = 0.057 and 0.028, respectively) [34].
3.6. Ion Channel Gene
P2RX7
- FentanylThe correlation of rs1718125 in P2RX7 with postoperative fentanyl analgesia was investigated in an observational study among Han Chinese patients with lung cancer [35]. This SNP was found to be significantly associated with postoperative pain and fentanyl dose (p < 0.05). Patients carrying the GA and AA genotypes required more fentanyl doses for pain control within 48 h postoperatively (p < 0.05). The postoperative VAS score was also significantly higher in carriers of the GA genotype when compared to the GG genotype group in the period of analepsis after general anesthesia and 6 h post-surgery (p = 0.041 and p = 0.030, respectively). Meanwhile, the postoperative VAS score was significantly higher in the A homozygotes than in the period of analepsis after general anesthesia (p < 0.001), at 6 (p = 0.006) and 24 h (p = 0.016) post-surgery [35].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Henson, L.A.; Maddocks, M.; Evans, C.; Davidson, M.; Hicks, S.; Higginson, I.J. Palliative care and the management of common distressing symptoms in advanced cancer: Pain, breathlessness, nausea and vomiting, and fatigue. J. Clin. Oncol. 2020, 38, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Deandrea, S.; Montanari, M.; Moja, L.; Apolone, G. Prevalence of undertreatment in cancer pain. A review of published literature. Ann. Oncol. 2008, 19, 1985–1991. [Google Scholar] [CrossRef] [PubMed]
- Javier, F.O.; Irawan, C.; Mansor, M.B.; Sriraj, W.; Tan, K.H.; Thinh, D.H.Q. Cancer pain management insights and reality in Southeast Asia: Expert perspectives from six countries. J. Glob. Oncol. 2016, 2, 235–243. [Google Scholar] [CrossRef]
- Vallath, N.; Rajagopal, M.R.; Perera, S.; Khan, F.; Paudel, B.D.; Tisocki, K. Access to pain relief and essential opioids in the WHO South-East Asia Region: Challenges in implementing drug reforms. WHO South-East Asia J. Public Health 2018, 7, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Cancer Pain Relief: With a Guide to Opioid Availability, 2nd ed.; World Health Organization: Geneva, Switzerland, 1996. Available online: https://apps.who.int/iris/handle/10665/37896 (accessed on 23 October 2022).
- Shi, C.; Liu, J.; Hu, J.; Chen, X.; Xie, J.; Luo, J.; Wang, C.; Wang, H.; Yuan, Q.; Zhu, H.; et al. Genetic and clinical factors associated with opioid response in Chinese Han patients with cancer pain: An exploratory cross-sectional study. Pain Ther. 2022, 11, 269–288. [Google Scholar] [CrossRef]
- Mejin, M.; Keowmani, T.; Abdul Rahman, S.; Liew, J.; Lai, J.; Chua, M.; Che Wan, I. Prevalence of pain and treatment outcomes among cancer patients in a Malaysian palliative care unit. Pharm. Pract. 2019, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Campa, D.; Gioia, A.; Tomei, A.; Poli, P.; Barale, R. Association of ABCB1/MDR1 and OPRM1 gene polymorphisms with morphine pain relief. Clin. Pharmacol. Ther. 2008, 83, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Wiffen, P.J.; Wee, B.; Moore, R.A. Oral morphine for cancer pain. Cochrane Database Syst. Rev. 2016, 4, 1–31. [Google Scholar]
- Droney, J.M.; Gretton, S.K.; Sato, H.; Ross, J.R.; Branford, R.; Welsh, K.I.; Welsh, K.I.; Cookson, W.; Riley, J. Analgesia and central side-effects: Two separate dimensions of morphine response. Br. J. Clin. Pharmacol. 2013, 75, 1340–1350. [Google Scholar] [CrossRef] [Green Version]
- Solhaug, V.; Molden, E. Individual variability in clinical effect and tolerability of opioid analgesics—Importance of drug interactions and pharmacogenetics. Scand J. Pain 2017, 17, 193–200. [Google Scholar] [CrossRef]
- Pasternak, G.W. Opiate pharmacology and relief of pain. J. Clin. Oncol. 2014, 32, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, C.; Graff, C.L.; Pollack, G.M. Variable modulation of opioid brain uptake by P-glycoprotein in mice. Biochem. Pharmacol. 2004, 67, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Chaves, C.; Remiao, F.; Cisternino, S.; Decleves, X. Opioids and the blood-brain barrier: A dynamic interaction with consequences on drug disposition in brain. Curr. Neuropharmacol. 2017, 15, 1156–1173. [Google Scholar] [CrossRef] [PubMed]
- Paller, C.J.; Campbell, C.M.; Edwards, R.R.; Dobs, A.S. Sex-based differences in pain perception and treatment. Pain Med. 2009, 10, 289–299. [Google Scholar] [CrossRef]
- Planelles, B.; Margarit, C.; Inda, M.D.; Ballester, P.; Muriel, J.; Barrachina, J.; Ajo, R.; Esteban, M.D.; Peiró, A.M. Gender based differences, pharmacogenetics and adverse events in chronic pain management. Pharm. J. 2020, 20, 320–328. [Google Scholar] [CrossRef]
- Gibson, S.J.; Helme, R.D. Age-related differences in pain perception and report. Clin. Geriatr. Med. 2001, 17, 433–456. [Google Scholar] [CrossRef]
- Klepstad, P.; Fladvad, T.; Skorpen, F.; Bjordal, K.; Caraceni, A.; Dale, O.; Davies, A.; Kloke, M.; Lundström, S.; Maltoni, M.; et al. Influence from genetic variability on opioid use for cancer pain: A European genetic association study of 2294 cancer pain patients. Pain 2011, 152, 1139–1145. [Google Scholar] [CrossRef]
- Nielsen, L.M.; Olesen, A.E.; Branford, R.; Christrup, L.L.; Sato, H.; Drewes, A.M. Association between human pain-related genotypes and variability in opioid analgesia: An updated review. Pain Pract. 2015, 15, 580–594. [Google Scholar] [CrossRef]
- Bell, G.C.; Donovan, K.A.; McLeod, H.L. Clinical implications of opioid pharmacogenomics in patients with cancer. Cancer Control. 2015, 22, 426–432. [Google Scholar] [CrossRef]
- Yu, Z.; Wen, L.; Shen, X.; Zhang, H. Effects of the OPRM1 A118G polymorphism (rs1799971) on opioid analgesia in cancer pain. Clin. J. Pain 2019, 35, 77–86. [Google Scholar] [CrossRef]
- Wang, G.X.; Zhang, H.; He, F.F.; Fang, X.M. Effect of the CYP2D6*10 C188T polymorphism on postoperative tramadol analgesia in a Chinese population. Eur. J. Clin. Pharmacol. 2006, 62, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.B.; Cai, L.N.; Yang, X.H.; Fu, H.G.; Sun, K.; Yuan, F.; Dong, T.L. Impact of CYP2D6 polymorphisms on postoperative fentanyl analgesia in gastric cancer patients. Genet. Test. Mol. Biomark. 2015, 19, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Naito, T.; Sato, H.; Hiraide, T.; Yamada, Y.; Kawakami, J. Impact of CYP genotype and inflammatory markers on the plasma concentrations of tramadol and its demethylated metabolites and drug tolerability in cancer patients. Eur. J. Clin. Pharmacol. 2018, 74, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Takashina, Y.; Naito, T.; Mino, Y.; Yagi, T.; Ohnishi, K.; Kawakami, J. Impact of CYP3A5 and ABCB1 gene polymorphisms on fentanyl pharmacokinetics and clinical responses in cancer patients undergoing conversion to a transdermal system. Drug Metab. Pharmacokinet. 2012, 27, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, M.; Tao, Y.; Hu, X.; Guo, L.; Ni, J.; Hu, J.; Shen, H.; Chen, Y. Roles of UGT2B7 C802T gene polymorphism on the efficacy of morphine treatment on cancer pain among the Chinese han population. Niger. J. Clin. Pract. 2019, 22, 1319–1323. [Google Scholar] [PubMed]
- Li, J.; Peng, P.; Mei, Q.; Xia, S.; Tian, Y.; Hu, L.; Chen, Y. The impact of UGT2B7 C802T and CYP3A4*1G polymorphisms on pain relief in cancer patients receiving oxycontin. Support. Care Cancer 2018, 26, 2763–2767. [Google Scholar] [CrossRef]
- Hajj, A.; Halepian, L.; El Osta, N.; Chahine, G.; Kattan, J.; Rabbaa Khabbaz, L. OPRM1 c.118A>G polymorphism and duration of morphine treatment associated with morphine doses and quality-of-life in palliative cancer pain settings. Int. J. Mol. Sci. 2017, 18, 669. [Google Scholar] [CrossRef]
- Liu, Y.C.; Wang, W.S. Human mu-opioid receptor gene A118G polymorphism predicts the efficacy of tramadol/acetaminophen combination tablets (Ultracet) in oxaliplatin-induced painful neuropathy. Cancer 2012, 118, 1718–1725. [Google Scholar] [CrossRef]
- Zhao, Z.; Lv, B.; Zhao, X.; Zhang, Y. Effects of OPRM1 and ABCB1 gene polymorphisms on the analgesic effect and dose of sufentanil after thoracoscopic-assisted radical resection of lung cancer. Biosci. Rep. 2019, 39, 1–15. [Google Scholar] [CrossRef]
- Matsuoka, H.; Arao, T.; Makimura, C.; Takeda, M.; Kiyota, H.; Tsurutani, J.; Fujita, Y.; Matsumoto, K.; Kimura, H.; Otsuka, M.; et al. Expression changes in arrestin β 1 and genetic variation in catechol-O-methyltransferase are biomarkers for the response to morphine treatment in cancer patients. Oncol. Rep. 2012, 27, 1393–1399. [Google Scholar]
- Matsuoka, H.; Makimura, C.; Koyama, A.; Fujita, Y.; Tsurutani, J.; Sakai, K.; Sakamoto, R.; Nishio, K.; Nakagawa, K. Prospective replication study implicates the catechol-o-methyltransferase val158met polymorphism as a biomarker for the response to morphine in patients with cancer. Biomed. Rep. 2017, 7, 380–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoshima, Y.; Sumitani, M.; Nishizawa, D.; Nagashima, M.; Ikeda, K.; Kato, R.; Hozumi, J.; Abe, H.; Azuma, K.; Tsuchida, R.; et al. Gamma-aminobutyric acid transaminase genetic polymorphism is a candidate locus for responsiveness to opioid analgesics in patients with cancer pain: An exploratory study. Neuropsychopharmacol. Rep. 2018, 38, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.D.; Wang, J.Y.; Liu, F.; Yuan, H.H.; Zhang, W.Y.; Guo, Y.H.; Jiang, B. Gene polymorphisms of OPRM1 A118G and ABCB1 C3435T may influence opioid requirements in Chinese patients with cancer pain. Asian Pacific J. Cancer Prev. 2013, 14, 2937–2943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Li, W.; Chai, Q.; Tan, X.; Zhang, K. Correlation of P2RX7 gene rs1718125 polymorphism with postoperative fentanyl analgesia in patients with lung cancer. Medicine 2019, 98, e14445. [Google Scholar] [CrossRef]
- Brennan, M.J. The clinical implications of cytochrome P450 interactions with opioids and strategies for pain management. J. Pain Symptom. Manag. 2012, 44, S15–S22. [Google Scholar] [CrossRef]
- Bertilsson, L.; Dahl, M.L.; Dalén, P.; Al-Shurbaji, A. Molecular genetics of CYP2D6: Clinical relevance with focus on psychotropic drugs. Br. J. Clin. Pharmacol. 2002, 53, 111–122. [Google Scholar] [CrossRef] [Green Version]
- PharmVar. Available online: https://www.pharmvar.org/gene/CYP2D6 (accessed on 8 November 2022).
- Yoo, H.D.; Lee, Y.B. Interplay of pharmacogenetic variations in ABCB1 transporters and cytochrome P450 enzymes. Arch. Pharmacal. Res. 2011, 34, 1817–1828. [Google Scholar] [CrossRef]
- Coffman, B.L.; Rios, G.R.; King, C.D.; Tephly, T.R. Human UGT2B7 catalyzes morphine glucuronidation. Drug Metab. Dispos. 1997, 25, 1–4. [Google Scholar]
- Sora, I.; Takahashi, N.; Funada, M.; Ujike, H.; Revay, R.S.; Donovan, D.M.; Miner, L.L.; Uhl, G.R. Opiate receptor knockout mice define μ receptor roles in endogenous nociceptive responses and morphine-induced analgesia. Proc. Natl. Acad. Sci. USA 1997, 94, 1544–1549. [Google Scholar] [CrossRef] [Green Version]
- van Esch, A.A.; de Vries, E.; Te Morsche, R.H.; van Oijen, M.G.; Jansen, J.B.; Drenth, J.P. Catechol-O-methyltransferase (COMT) gene variants and pain in chronic pancreatitis. Neth J. Med. 2011, 69, 330–334. [Google Scholar]
- Berthele, A.; Platzer, S.; Jochim, B.; Boecker, H.; Buettner, A.; Conrad, B.; Riemenschneider, M.; Toelle, T.R. COMT Val108/158Met genotype affects the mu-opioid receptor system in the human brain: Evidence from ligand-binding, G-protein activation and preproenkephalin mRNA expression. Neuroimage 2005, 28, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Enna, S.J.; McCarson, K.E. The role of GABA in the mediation and perception of pain. Adv. Pharmacol. 2006, 54, 1–27. [Google Scholar] [PubMed]
- Comitato, A.; Bardoni, R. Presynaptic inhibition of pain and touch in the spinal cord: From receptors to circuits. Int. J. Mol. Sci. 2021, 22, 414. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.J.; Koszdin, K.; Bernards, C.M. Opiate-induced analgesia is increased and prolonged in mice lacking p-glycoprotein. Anesthesiology 2000, 92, 1392–1399. [Google Scholar] [CrossRef]
- Kambur, O.; Kaunisto, M.A.; Winsvold, B.S.; Wilsgaard, T.; Stubhaug, A.; Zwart, J.A.; Kalso, E.; Nielsen, C.S. Genetic variation in P2RX7 and pain tolerance. Pain 2018, 159, 1064–1073. [Google Scholar] [CrossRef]
- Gaedigk, A. Complexities of CYP2D6 gene analysis and interpretation. Int. Rev. Psychiatry 2013, 25, 534–553. [Google Scholar] [CrossRef]
- Nakamura, K.; Ariyoshi, N.; Yokoi, T.; Ohgiya, S.; Chida, M.; Nagashima, K.; Inoue, K.; Kodama, T.; Shimada, N.; Kamataki, T. CYP2D6.10 present in human liver microsomes shows low catalytic activity and thermal stability. Biochem. Biophys. Res. Commun. 2002, 293, 969–973. [Google Scholar] [CrossRef]
- Dean, L.; Kane, M. Tramadol therapy and CYP2D6 genotype. In Medical Genetics Summaries [Internet]; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kane, M.S., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. Available online: https://www.ncbi.nlm.nih.gov/books/NBK315950/ (accessed on 25 July 2022).
- Long, T.; Cristofoletti, R.; Cicali, B.; Michaud, V.; Dow, P.; Turgeon, J.; Schmidt, S. Physiologically based pharmacokinetic modeling to assess the impact of CYP2D6-mediated drug-drug interactions on tramadol and o-desmethyltramadol exposures via allosteric and competitive inhibition. J. Clin. Pharmacol. 2022, 62, 76–86. [Google Scholar] [CrossRef]
- Dorji, P.W.; Tshering, G.; Na-Bangchang, K. CYP2C9, CYP2C19, CYP2D6 and CYP3A5 polymorphisms in South-East and East Asian populations: A systematic review. J. Clin. Pharm. Ther. 2019, 44, 508–524. [Google Scholar] [CrossRef] [Green Version]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Callaghan, J.T.; Samer, C.F.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 4, 888–896. [Google Scholar] [CrossRef]
- Leppert, W. CYP2D6 in the metabolism of opioids for mild to moderate pain. Pharmacology 2011, 87, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Kisoi, M.; Imai, M.; Yamamura, M.; Sakaguchi, Y.; Murata, S.; Ichikawa, A.; Kinoshita, K. Unique Genotyping Protocol of CYP2D6 Allele Frequency Using Real Time Quantitative PCR from Japanese Healthy Women. Biol. Pharm. Bull. 2020, 43, 904–907. [Google Scholar] [CrossRef]
- Grimsrud, K.N.; Ivanova, X.; Sherwin, C.M.; Palmieri, T.L.; Tran, N.K. Identification of Cytochrome P450 polymorphisms in burn patients and impact on fentanyl pharmacokinetics: A pilot study. J. Burn Care Res. 2019, 40, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Koolen, S.L.W.; van der Rijt, C.C.D. Is there a role for pharmacogenetics in the dosing of fentanyl? Pharmacogenomics 2017, 18, 417–419. [Google Scholar] [CrossRef]
- Yang, Z.Z.; Li, L.; Wang, L.; Yuan, L.M.; Xu, M.C.; Gu, J.K.; Jiang, H.D.; Yu, L.S.; Zeng, S. The regioselective glucuronidation of morphine by dimerized human UGT2B7, 1A1, 1A9 and their allelic variants. Acta Pharmacol. Sin. 2017, 38, 1184–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawyer, M.B.; Innocenti, F.; Das, S.; Cheng, C.; Ramirez, J.; Pantle-Fisher, F.H.; Wright, C.; Badner, J.; Pei, D.; Boyett, J.M.; et al. A pharmacogenetic study of uridine diphosphate–glucuronosyltransferase 2B7 in patients receiving morphine. Clin. Pharmacol. Ther. 2003, 73, 566–574. [Google Scholar] [CrossRef]
- Eiselt, É.; Otis, V.; Belleville, K.; Yang, G.; Larocque, A.; Régina, A.; Demeule, M.; Sarret, P.; Gendron, L. Use of a noninvasive brain-penetrating peptide-drug conjugate strategy to improve the delivery of opioid pain relief medications to the brain. J. Pharmacol. Exp. Ther. 2020, 374, 52–61. [Google Scholar] [CrossRef] [Green Version]
- UGT2B7. Available online: https://www.pharmgkb.org/gene/PA361/clinicalAnnotation (accessed on 14 July 2022).
- Pathan, H.; Williams, J. Basic opioid pharmacology: An update. Br. J. Pain 2012, 6, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Senese, N.B.; Kandasamy, R.; Kochan, K.E.; Traynor, J.R. Regulator of G-Protein signaling (RGS) protein modulation of opioid receptor signaling as a potential target for pain management. Front. Mol. Neurosci. 2020, 13, 5. [Google Scholar] [CrossRef] [Green Version]
- Halikere, A.; Moore, J.; Hart, R.; Tischfield, J.; Pang, Z. Synaptic mechanism of A118G OPRM1 gene variants in human neurons. Eur. Neuropsychopharmacol. 2019, 29, S732–S733. [Google Scholar] [CrossRef]
- Levran, O.; Kreek, M.J. Population-specific genetic background for the OPRM1 variant rs1799971 (118A>G): Implications for genomic medicine and functional analysis. Mol. Psychiatry 2020, 26, 3169–3177. [Google Scholar] [CrossRef] [PubMed]
- Chidambaran, V.; Mavi, J.; Esslinger, H.; Pilipenko, V.; Martin, L.J.; Zhang, K.; Sadhasivam, S. Association of OPRM1 A118G variant with risk of morphine-induced respiratory depression following spine fusion in adolescents. Pharm. J. 2015, 15, 255–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oertel, B.G.; Kettner, M.; Scholich, K.; Renné, C.; Roskam, B.; Geisslinger, G.; Schmidt, P.H.; Lötsch, J. A common human μ-opioid receptor genetic variant diminishes the receptor signaling efficacy in brain regions processing the sensory information of pain. J. Biol. Chem. 2009, 284, 6530–6535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elton, A.; Smith, C.T.; Parrish, M.H.; Boettiger, C.A. COMT Val158Met polymorphism exerts sex-dependent effects on fMRI measures of brain function. Front. Hum. Neurosci. 2017, 11, 578. [Google Scholar] [CrossRef]
- Hooten, W.M.; Hu, D.; Cunningham, J.M.; Black, J.L. Effect of catechol-O-methyltransferase (rs4680) single-nucleotide polymorphism on opioid-induced hyperalgesia in adults with chronic pain. Mol. Pain 2019, 15, 1744806919848929. [Google Scholar] [CrossRef] [Green Version]
- Mir, R.; Bhat, M.; Javid, J.; Jha, C.; Saxena, A.; Banu, S. Potential impact of COMT-rs4680 G > a gene polymorphism in coronary artery disease. J. Cardiovasc. Dev. Dis. 2018, 5, 38. [Google Scholar] [CrossRef] [Green Version]
- Rakvåg, T.T.; Klepstad, P.; Baar, C.; Kvam, T.M.; Dale, O.; Kaasa, S.; Krokan, H.E.; Skorpen, F. The Val158Met polymorphism of the human catechol-O-methyltransferase (COMT) gene may influence morphine requirements in cancer pain patients. Pain 2005, 116, 73–78. [Google Scholar] [CrossRef]
- Lucenteforte, E.; Vannacci, A.; Crescioli, G.; Lombardi, N.; Vagnoli, L.; Giunti, L.; Cetica, V.; Coniglio, M.L.; Pugi, A.; Bonaiuti, R.; et al. Opioid response in paediatric cancer patients and the Val158Met polymorphism of the human catechol-O-methyltransferase (COMT) gene: An Italian study on 87 cancer children and a systematic review. BMC Cancer 2019, 19, 113. [Google Scholar] [CrossRef]
- Hu, B.; Zhang, X.; Xu, G.; Zhang, Q.; Qian, P.; Liu, S.; Zhu, J.; Shen, R. Association between COMT polymorphism Val158Met and opioid consumption in patients with postoperative pain: A meta-analysis. Neurosignals 2018, 26, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Hoffmeyer, S.; Burk, O.; Von Richter, O.; Arnold, H.P.; Brockmöller, J.; Johne, A.; Cascorbi, I.; Gerloff, T.; Roots, I.; Eichelbaum, M.; et al. Functional polymorphisms of the human multidrug-resistance gene: Multiple sequence variations and correlation of one allele with P-glycoprotein expression and activity in vivo. Proc. Natl. Acad. Sci. USA 2000, 97, 3473–3478. [Google Scholar] [CrossRef]
- Kadiev, E.; Patel, V.; Rad, P.; Thankachan, L.; Tram, A.; Weinlein, M.; Woodfin, K.; Raffa, R.B.; Nagar, S. Role of pharmacogenetics in variable response to drugs: Focus on opioids. Expert Opin. Drug Metab. Toxicol. 2007, 4, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Jamroziak, K.; Robak, T. Pharmacogenomics of MDR1/ABCB1 gene: The influence on risk and clinical outcome of haematological malignancies. Hematology 2013, 9, 91–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, C.; Wang, J.; Xie, S. P2RX7 Gene rs1718125 Polymorphism is Related with Postoperative Pain and Fentanyl Intake in Esophageal Cancer Patients. Pharmgenom. Pers. Med. 2020, 13, 585–589. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gene | Polymorphism(s) | Parameters with Significant Association | Ref. |
|---|---|---|---|
| CYP2D6 | *10 | Opioid dose requirements, pain control | [22,23] |
| *2, *5, *10, *14 | Pharmacokinetics | [24] | |
| CYP3A5 | *3 | Pharmacokinetics | [25] |
| UGT2B7 | rs7439366 | Pharmacokinetics, pain control | [26] |
| Pain control | [27] | ||
| OPRM1 | rs1799971 | Opioid dose requirements | [28] |
| Pain control | [29] | ||
| Opioid dose requirements | [30] | ||
| rs1323040 | Opioid dose requirements | [30] | |
| COMT | rs4680 | Opioid dose requirements, Pharmacokinetics | [31] |
| Opioid dose requirements, pain control | [32] | ||
| ABAT | rs1641025 | Opioid dose requirements, pain control | [33] |
| ABCB1 | rs1128503 | Opioid dose requirements | [25,30] |
| rs2032582 | Opioid dose requirements | [30] | |
| rs1045642 | Opioid dose requirements | [34] | |
| P2RX7 | rs1718125 | Opioid dose requirements | [35] |
| Normal metabolizer (NM) | *1*1, *1*2, *1*5, *1*10, *1*14, *2*2, *2*5, *2*10, or *2*14 |
| Intermediate metabolizer (IM) | *5*10, *10*10, or *10*14 |
| Poor metabolizer (PM) | *5*5, *5*14, or *14*14 |
| Gene (SNP) | Genotype (%) | Findings | p-Value | Population (n) | Opioid | Cancer Type | Ref. |
|---|---|---|---|---|---|---|---|
| CYP2D6 (CYP2D6*2, *5, *10, *14) | NM 1 IM 2 PM 3 | Plasma concentration of O-desmethyltramadol and its ratio to tramadol were lower in the CYP2D6 IM + PM group than in the n NM group. | <0.05 | Japanese (70) | Tramadol | NA | [24] |
| CYP3A5 (CYP3A5*3) | *1*1 (8.3) *1*3 (33.3) *3*3 (58.3) | Plasma concentration of fentanyl normalized with the measured absorption rate was higher in the CYP3A5*3/*3 group than in the *1/*1 and *1/*3 groups | 0.048; 0.021 | Japanese (60) | Fentanyl | Solid tumors | [25] |
| UGT2B7 (C802T) | CC (13.33) CT (45) TT (41.67) | Plasma concentration of morphine for patients with CC genotype was significantly lower than that in patients with CT or TT genotype | 0.05 | Han Chinese (120) | Morphine | Solid tumors | [26] |
| COMT (G472A, rs4680) | GG GA AA | Plasma concentration of patients with AA genotype was lower compared to patients with AG and GG genotype on day 1 | 0.008 | Japanese (48) | Morphine | Solid tumors | [31] |
| Gene (SNP) | Genotype (%) | MEDD (mg) | Findings | p-Value | Population (n) | Opioid | Cancer Type | Ref. |
|---|---|---|---|---|---|---|---|---|
| CYP2D6 (CYP2D6*10) | Group I 1 (27) Group II 1 (41.3) Group III 1 (31.7) | 459.5 ± 70.3 476.8 ± 99.2 532.7 ± 92.6 | Tramadol consumption in group III was higher compared to group I or II at 4, 24, and 48 h. Tramadol consumption in group I and II did not differ. | <0.05 | Chinese (70) | Tramadol | Gastric cancer | [22] |
| CYP2D6 (CYP2D6*10) | WW 2 (21) WM 2 (54) MM 2 (25) | 587.7 ± 132.0 600.4 ± 104.5 657.8 ± 185.2 (24 h after surgery) | Cumulative fentanyl consumption was higher in the MM group compared to the WW group at 6, 12, and 24 h postoperatively. | 0.018 | Chinese (207) | Fentanyl | Gastric cancer | [23] |
| OPRM1 (rs1799971) | AA AG | 29.97 51.37 | Morphine mean dose decreased with age but increased with morphine treatment duration. Morphine dose requirements for patients with AG genotype was higher compared to patients with AA genotype. | 0.043; 0.029 <0.001 | Lebanese (89) | Morphine | Various 3 | [28] |
| OPRM1 (rs1799971) | AA (31) AG (58) GG (10) | NA | Tramadol/paracetamol combination treatment response was lower in patients with AG or GG genotypes than in patients with AA genotype. The requirement for rescue analgesia was also higher for patients with G allele variants. | <0.01 <0.01 | Chinese (96) | Tramadol/PCM combination | Colorectal carcinoma | [29] |
| OPRM1 (rs1799971) | AA (51) AG (35) GG (14) | 64.35 ± 5.12 67.59 ± 4.89 71.52 ± 5.03 (24 h after surgery) | The consumption of sufentanil in the patient groups carrying the GG genotype was significantly increased compared to that of the AA and AG genotypes groups. | <0.05 | Han Chinese (225) | Sufentanil | Lung cancer | [30] |
| OPRM1 (rs1323040) | CC (55) CT (35) TT (10) | 63.54 ± 4.87 67.71 ± 4.19 75.24 ± 3.98 (24 h after surgery) | The consumption of sufentanil in the patient groups carrying the TT genotype was significantly increased compared to that of the CC and CT genotypes groups. | <0.05 | Han Chinese (225) | Sufentanil | Lung cancer | [30] |
| COMT (rs4680) | GG GA AA | 43.0 ± 21.4 28.9 ± 3.2 30.0 ± 0.0 | Morphine dose requirement of patients with AA genotype was lower compared to patients with AG and GG genotypes on day 1 | 0.03 | Japanese (48) | Morphine | Solid tumors | [31] |
| COMT (rs4680) | GG (58) GA (38) AA (4) | 35.2 ± 11.5 29.5 ± 2.3 25.0 ± 7.1 | Morphine dose requirement of patients with GG genotype was higher compared to patients with AA and AG genotypes on day 1. | 0.013 | Japanese (50) | Morphine | Solid tumors | [32] |
| ABAT (rs1641025) | CC (59) CT (32) TT (8) | Before vs. after increased opioid dosage 1.9 ± 2.3 vs. 1.1 ± 1.5 6.5 ± 17.7 vs. 4.3 ± 16.4 8.0 ± 9.5 vs. 55.2 ± 100 | Opioid dose requirement was lower in patient with CC genotype compared to patients with CT and TT genotype for both before and after increasing opioid dosage. | <0.001 | Japanese (71) | Combination of opioids | NA | [33] |
| ABCB1 (1236TT rs1128503) | CC (21.7) CT (40) TT (38.3) | NA | Rescue medication was needed by fewer patients with TT genotype compared to patients with CT and CC genotype | 0.036 | Japanese (60) | Fentanyl | Solid tumors | [25] |
| ABCB1(rs1128503 | CC (58) CT (28) TT (14) | 62.98 ± 5.68 67.89 ± 4.26 73.42 ± 3.97 (24 h after surgery) | The consumption of sufentanil in the patient groups carrying the TT genotype was significantly increased compared to that of the CC and CT genotypes groups. | <0.05 | Han Chinese (225) | Sufentanil | Lung cancer | [30] |
| ABCB1 (rs2032582) | GG (48.4) GA (37.8) AA (13.8) | NA | Sufentanil dose received was higher in patients with AA genotype compared to patients with AG and GG genotype at time points 6, 24, and 48 h. | <0.05 | Han Chinese (225) | Sufentanil | Lung cancer | [30] |
| ABCB1 (C3435Trs1045642) | CC (40.2) CT (43.7) TT (16.1) | NA | 24 h and weight-surface-area-adjusted-24 h opioid dose received was higher in patients with TT genotype compared to patients with CC and CT genotypes. | 0.057; 0.028 | Han Chinese (112) | Various opioids 4 | NA | [34] |
| P2RX7 (rs1718125) | GG (46.2) GA (44.96) AA (8.82) | 9.27 ± 3.06 10.45 ± 2.99 11.69 ± 3.40 (24 h post-operation) | Fentanyl dose requirement to control postoperative pain was higher in patients with GA and AA genotypes than in GG genotype. | <0.05 | Han Chinese (238) | Hydromorphone | Lung cancer | [35] |
| Gene (SNP) | Genotype (%) | Findings | p-Value | Population (n) | Opioid | Cancer Type | Ref. |
|---|---|---|---|---|---|---|---|
| CYP2D6 (CYP2D6*10) | WW 1 (21) WM 1 (54) MM 1 (25) | Pain score in the MM group was higher than in the WW group 6 h postoperatively | <0.05 | Chinese (207) | Fentanyl | Gastric cancer | [23] |
| UGT2B7 (rs7439366) | CC (13.33) CT (45) TT (41.6) | Pain score of patients with CT or TT genotypes were higher than patients with CC genotype | <0.05 | Han Chinese (120) | Morphine | Solid tumors | [26] |
| UGT2B7 (rs7439366) | CC (59.6) CT (31.6) TT (8.8 | Pain score of patients with TT genotype was higher than patients with CC genotype | <0.05 | Han Chinese (47) | Oxycodone | Tumors | [27] |
| OPRM1 (rs1799971) | AA (31) AG (58) GG (10) | The difference in pre-treatment and post-treatment pain scores for patients with AA genotype was more significant than patients with AG or GG genotype. AA genotype patients showed lowered pain scores after receiving tramadol/paracetamol combination treatment | <0.01 | Chinese (96) | Tramadol/PCM Combination | Colorectal carcinoma | [29] |
| ABAT (rs1641025) | CC (59.1) CT (32.4) TT (8.5) | Pain severity mean was lowest in patients with CT genotype compared to patients with CC or TT genotype after opioid dosage increment | <0.001 | Japanese (71) | Combination of opioids | NA | [33] |
| P2RX7 (rs1718125) | GG (46.2) GA (44.96) AA (8.82) | Carriers of the GA genotype had higher postoperative VAS scores than GG genotype carriers after general anesthesia and 6 h after surgery. Carriers of the AA genotype group had higher postoperative VAS scores than GG genotype carriers after general anesthesia, 6 h and 24 h after surgery | 0.041; 0.030 <0.001; 0.006; 0.016 | Han Chinese (238) | Fentanyl | Lung cancer | [4] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satkunananthan, S.E.; Suppiah, V.; Toh, G.-T.; Yow, H.-Y. Pharmacogenomics of Cancer Pain Treatment Outcomes in Asian Populations: A Review. J. Pers. Med. 2022, 12, 1927. https://doi.org/10.3390/jpm12111927
Satkunananthan SE, Suppiah V, Toh G-T, Yow H-Y. Pharmacogenomics of Cancer Pain Treatment Outcomes in Asian Populations: A Review. Journal of Personalized Medicine. 2022; 12(11):1927. https://doi.org/10.3390/jpm12111927
Chicago/Turabian StyleSatkunananthan, Shobha Elizabeth, Vijayaprakash Suppiah, Gaik-Theng Toh, and Hui-Yin Yow. 2022. "Pharmacogenomics of Cancer Pain Treatment Outcomes in Asian Populations: A Review" Journal of Personalized Medicine 12, no. 11: 1927. https://doi.org/10.3390/jpm12111927
APA StyleSatkunananthan, S. E., Suppiah, V., Toh, G. -T., & Yow, H. -Y. (2022). Pharmacogenomics of Cancer Pain Treatment Outcomes in Asian Populations: A Review. Journal of Personalized Medicine, 12(11), 1927. https://doi.org/10.3390/jpm12111927