
Breast Reconstruction by Exclusive Lipofilling after Total Mastectomy for Breast Cancer: Description of the Technique and Evaluation of Quality of Life

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
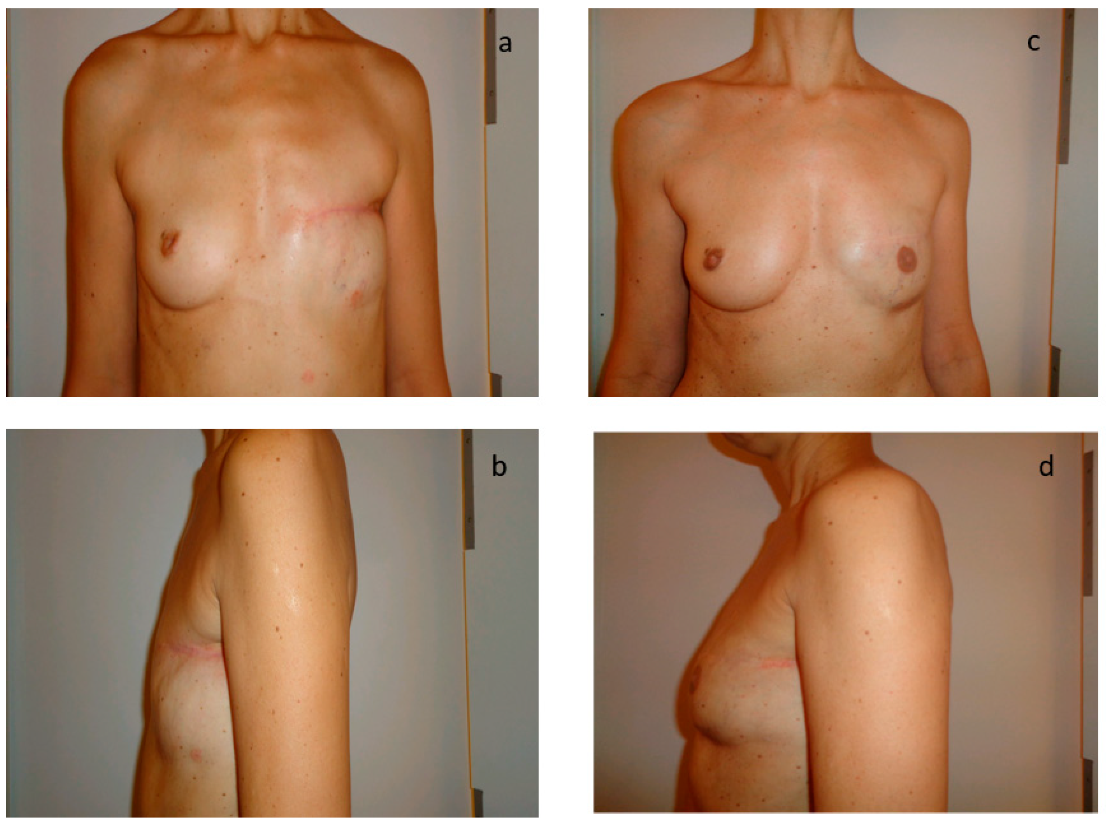
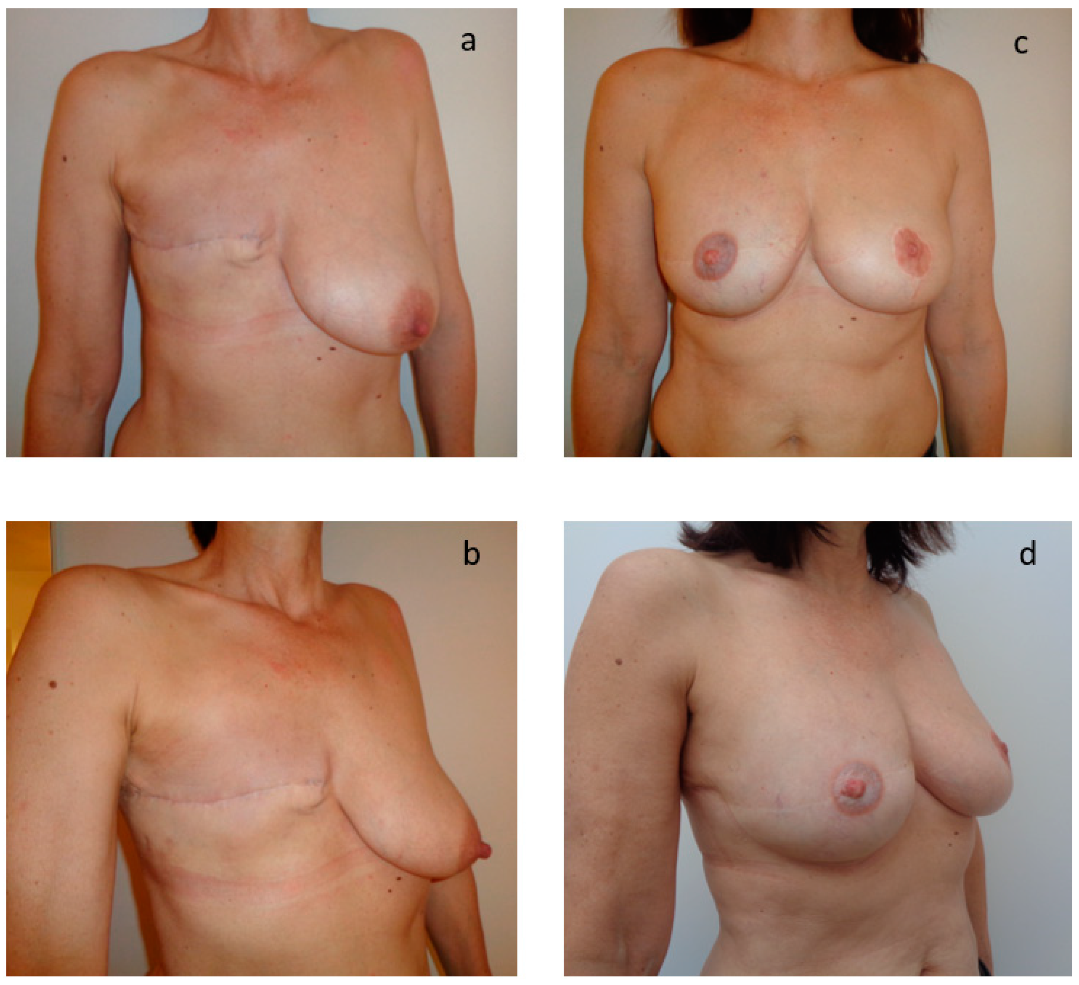
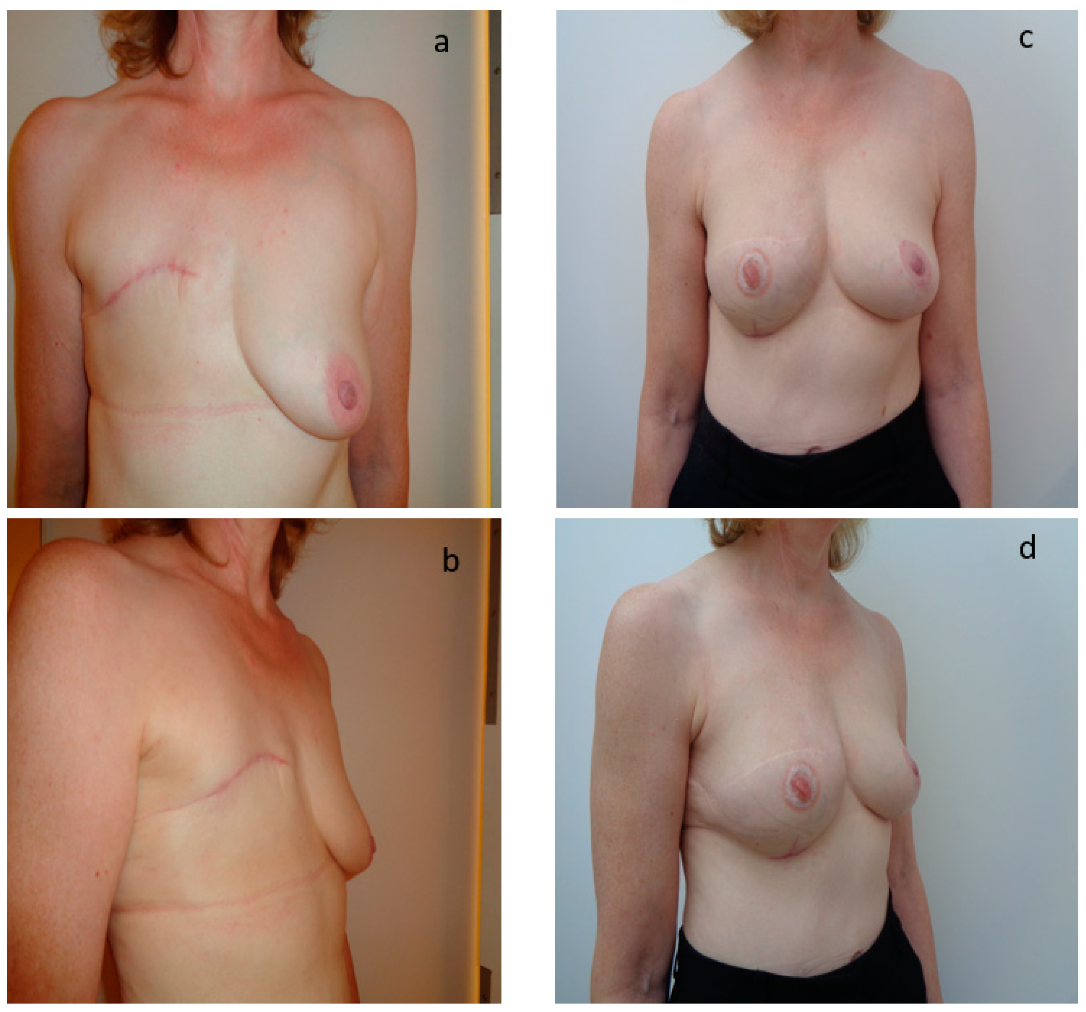
2.2. Surgical Technique
2.3. Statistical Analysis
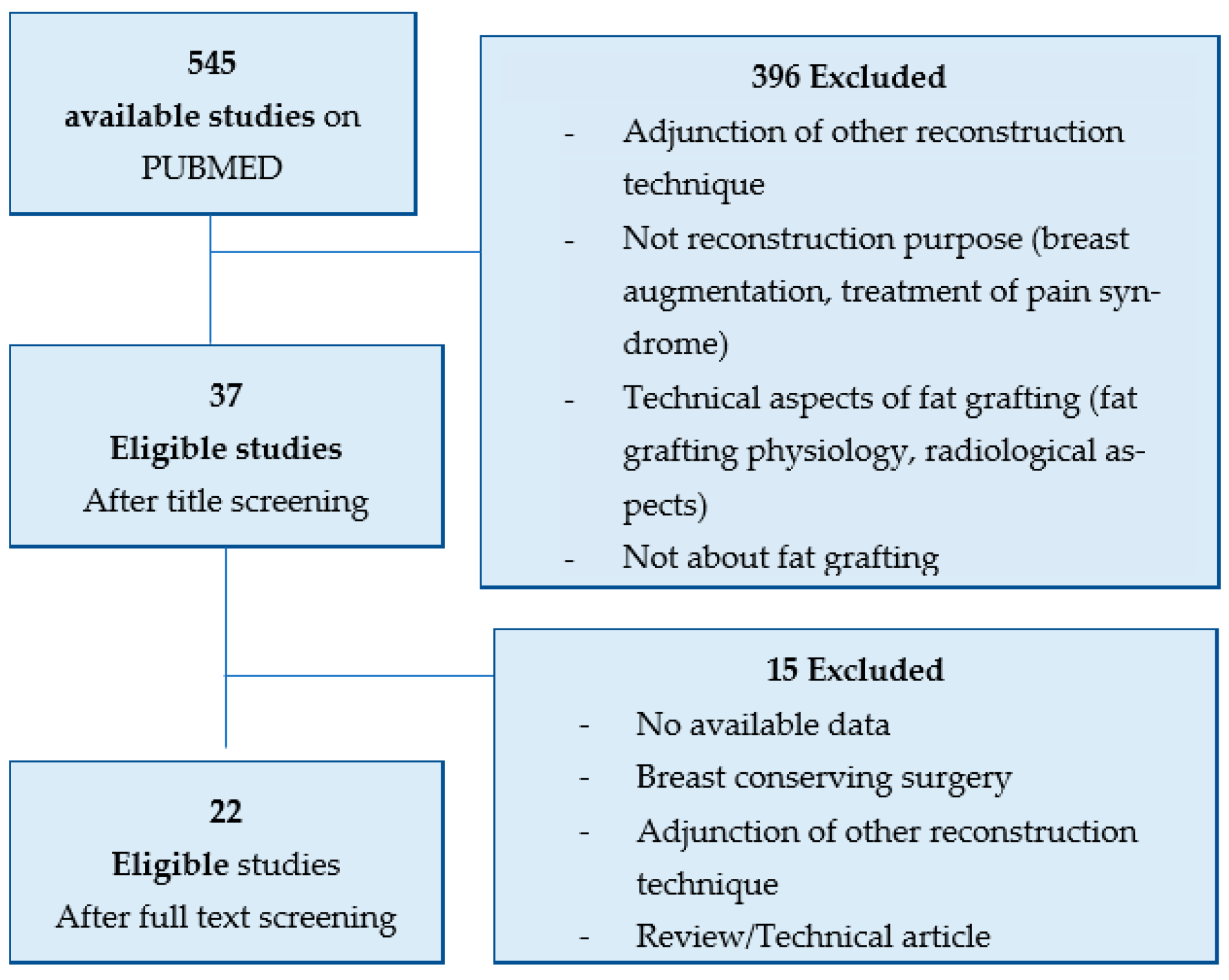
2.4. Literature Research
3. Results
3.1. General Results
3.2. Oncological Aspects
3.3. Technical Aspects
3.4. Patient Quality of Life and Satisfaction
3.5. Survival Outcome
3.6. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer. Breast Cancer Fact Sheets; Globocan: Lyon, France, 2020. [Google Scholar]
- Institut National de Cancer. Available online: https://www.e-cancer.fr (accessed on 6 January 2021).
- La Vie Deux Ans Après un Diagnostic de Cancer. Collection Études et Enquêtes, INCa. July 2014. Available online: file:///C:/Users/MDPI/Downloads/La-vie-2-ans-apres-un-diagnostic-de-cancer-2014-V2%20(1).pdf. (accessed on 6 January 2021).
- Babin, G.; Commeny, J.; Fournier, M.; Rousvoal, A.; Kabbani, Y.; Debled, M.; Jaffre, A.; de Lara, C.T. Breast reconstruction in elderly patients: Studies of the practices at institut Bergonié during 2005–2015. Bull. Cancer 2017, 104, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Hu, G.; Biskup, E.; Qiu, X.; Zhang, H.; Zhang, H. Depression Induced by Total Mastectomy, Breast Conserving Surgery and Breast Reconstruction: A Systematic Review and Meta-analysis. World J. Surg. 2018, 42, 2076–2085. [Google Scholar] [CrossRef] [PubMed]
- Hughson, A.V.M.; Cooper, A.F.; McArdle, C.S.; Smith, D.C. Psychosocial consequences of mastectomy: Levels of morbidity and associated factors. J. Psychosom. Res. 1988, 32, 383–391. [Google Scholar] [CrossRef]
- Kiebert, G.M.; de Haes, J.C.; van de Velde, C.J. The impact of breast-conserving treatment and mastectomy on the quality of life of early-stage breast cancer patients: A review. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1991, 9, 1059–1070. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, E.; Emilee, G.; Ussher, J.M.; Perz, J. Sexuality after breast cancer: A review. Maturitas 2010, 66, 397–407. [Google Scholar] [CrossRef]
- Berterö, C.; Wilmoth, M.C. Breast cancer diagnosis and its treatment affecting the self: A meta-synthesis. Cancer Nurs. 2017, 30, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Miaja, M.; Platas, A.; Martinez-Cannon, B.A. Psychological Impact of Alterations in Sexuality, Fertility, and Body Image in Young Breast Cancer Patients and Their Partners. Rev. Investig. Clin. Organo. Hosp. Enferm. Nutr. 2017, 69, 204–209. [Google Scholar] [CrossRef]
- Aerts, L.; Christiaens, M.; Enzlin, P.; Neven, P.; Amant, F. Sexual functioning in women after mastectomy versus breast conserving therapy for early-stage breast cancer: A prospective controlled study. Breast Edinb. Scotl. 2014, 23, 629–636. [Google Scholar] [CrossRef]
- Bailey, C.R.; Ogbuagu, O.; Baltodano, P.A.; Simjee, U.F.; Manahan, M.A.; Cooney, D.S.; Jacobs, L.K.; Tsangaris, T.N.; Cooney, C.M.; Rosson, G.D. Quality-of-Life Outcomes Improve with Nipple Sparing Mastectomy and Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 219–226. [Google Scholar] [CrossRef]
- Schmidt, J.L.; Wetzel, C.M.; Lange, K.W.; Heine, N.; Ortmann, O. Patients’ experience of breast reconstruction after mastectomy and its influence on postoperative satisfaction. Arch. Gynecol. Obs. 2017, 296, 827–834. [Google Scholar] [CrossRef]
- Lee, G.K.; Sheckter, C.C. Breast Reconstruction Following Breast Cancer Treatment-2018. JAMA 2018, 320, 1277–1278. [Google Scholar] [CrossRef] [PubMed]
- Régis, C.; Le, J.; Chauvet, M.-P.; Le Deley, M.-C.; Le Teuff, G. Variations in the breast reconstruction rate in France: A nationwide study of 19,466 patients based on the French medico-administrative database. Breast Edinb. Scotl. 2018, 42, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Nègre, G.; Balcaen, T.; Sinna, R.; Chazard, E. Chazard b En France, une minorité de femmes bénéficient d’une reconstruction mammaire après mastectomie pour cancer du sein. Revue d’Epidémiologie Santé Publique 2018, 66 (Suppl. S1), S19. [Google Scholar]
- Strong, A.; Cederna, P.S.; Rubin, J.P.; Coleman, S.R.; Levi, B. The Current State of Fat Grafting: A Review of Harvesting, Processing, and Injection Techniques. Plast. Reconstr. Surg. 2015, 136, 897–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellenbogen, R. Free autogenous pearl fat grafts in the face—A preliminary report of a rediscovered technique. Ann. Plast. Surg. 1986, 16, 179–194. [Google Scholar] [CrossRef]
- Clauser, L.; Zavan, B.; Galiè, M.; Di Vittorio, L.; Gardin, C.; Bianchi, A.E. Autologous Fat Transfer for Facial Augmentation: Surgery and Regeneration. J. Craniofac. Surg. 2019, 30, 682–685. [Google Scholar] [CrossRef]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Klok, J.A.; Cordeiro, P.G.; Cano, S.J. Development of a new patient-reported outcome measure for breast surgery: The BREAST-Q. Plast. Reconstr. Surg. 2009, 124, 345–353. [Google Scholar] [CrossRef]
- Cohen, W.A.; Mundy, L.R.; Ballard, T.N.; Klassen, A.; Cano, S.J.; Browne, J.; Pusic, A.L. The BREAST-Q in surgical research: A review of the literature 2009-2015. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2016, 69, 149–162. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Babovic, S. Complete breast reconstruction with autologous fat graft—A case report. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2010, 63, e561–e563. [Google Scholar] [CrossRef]
- Bayti, T.; Panouilleres, M.; Tropet, Y.; Bonnetain, F.; Pauchot, J. Fat grafting in breast reconstruction. Retrospective study of satisfaction and quality of life about 68 patients]. Ann. Chir. Plast. Esthet. 2016, 61, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Panettiere, P.; Accorsi, D.; Marchetti, L.; Sgrò, F.; Sbarbati, A. Large-Breast Reconstruction Using Fat Graft Only after Prosthetic Reconstruction Failure. Aesthetic Plast. Surg. 2011, 35, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Ho Quoc, C.; Pires Novais Dias, L.; Freitas Melro Braghiroli, O.; Martella, N.; Vincenzo Giovinazzo, V.; Piat, J.-M. Oncological Safety of Lipofilling in Healthy BRCA Carriers After Bilateral Prophylactic Mastectomy: A Case Series. Eur. J. Breast Health 2019, 15, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Delaporte, T. Reconstruction mammaire par transfert graisseux exclusif : À propos de 15 cas consécutifs. Ann. Chir. Plast. Esthet. 2009, 54, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Fabiocchi, L.; Semprini, G.; Cattin, F.; Dellachiesa, L.; Fogacci, T.; Frisoni, G.; Samorani, D. ‘Reverse expansion’: A new technique of breast reconstruction with autologous tissue. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2017, 70, 1537–1542. [Google Scholar] [CrossRef] [Green Version]
- Fitoussi, A.; Pollet, A.G.; Couturaud, B.; Salmon, R.J. Secondary breast reconstruction using exclusive lipofilling. Ann. Chir. Plast. Esthet. 2009, 54, 374–378. [Google Scholar] [CrossRef]
- Hammer-Hansen, N.; Jensen, T.B.; Damsgaard, T.E. Delayed total breast reconstruction with brava. Case Rep. Surg. 2015, 2015, 601904. [Google Scholar] [CrossRef] [Green Version]
- Ho Quoc, C.; Piat, J.M.; Carrabin, N.; Meruta, A.; Faure, C.; Delay, E. Breast reconstruction with fat grafting and BRAVA((R)) pre-expansion: Efficacy evaluation in 45 cases. Ann. Chir. Plast. Esthet. 2016, 61, 183–189. [Google Scholar] [CrossRef]
- Chen, T.M.; Chen, S.G.; Teng, S.C. Using an external soft tissue expander before autologous fat grafting for non-irradiated breast reconstruction. J. Plast. Surg. Hand Surg. 2013, 47, 419–421. [Google Scholar] [CrossRef]
- Hoppe, D.L.; Ueberreiter, K.; Surlemont, Y.; Peltoniemi, H.; Stabile, M.; Kauhanen, S. Breast reconstruction de novo by water-jet assisted autologous fat grafting—A retrospective study. Ger. Med. Sci. GMS E-J. 2013, 11, Doc17. [Google Scholar]
- Jarrah, A.; Paloma, V.; Vernetta, O. Reconstrucción mamaria mediante lipoinfiltrado enriquecido con PRP. Use Lipofilling Enriched PRP Breast Reconstr. 2013, 39 (Suppl. S1), 65–73. [Google Scholar]
- Kellou, K.; Lequesne, J.; Georgescu, D.; De Gournay, E.; Bréard, H.; Carrilho, J.; Forestier, F.; Poteau, A.; Crouzet, A. Limitations of breast reconstruction using exclusive lipofilling: A retrospective study over 10 years. Gynecol. Obstet. Fertil. Senol. 2019, 47, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Longo, B.; Laporta, R.; Sorotos, M.; Pagnoni, M.; Gentilucci, M.; Santanelli di Pompeo, F. Total breast reconstruction using autologous fat grafting following nipple-sparing mastectomy in irradiated and non- irradiated patients. Aesthetic Plast. Surg. 2014, 38, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Manconi, A.; de Lorenzi, F.; Chahuan, B.; Berrino, V.; Berrino, P.; Zucca-Matthes, G.; Petit, J.Y.; Rietjens, M. Total Breast Reconstruction With Fat Grafting After Internal Expansion and Expander Removal. Ann. Plast. Surg. 2016, 78, 392–396. [Google Scholar] [CrossRef]
- Mestak, O.; Mestak, J.; Bohac, M.; Edriss, A.; Sukop, A. Breast Reconstruction after a Bilateral Mastectomy Using the BRAVA Expansion System and Fat Grafting. Plast. Reconstr. Surg. Glob. Open 2013, 1, e71. [Google Scholar] [CrossRef]
- Niddam, J.; Durazzo, A.; Meningaud, J.P. Breast reconstruction by exclusive fat grafting: What about the breast projection? Br. J. Plast. Surg. 2017, 70, 1146–1147. [Google Scholar] [CrossRef]
- Serra-Renom, J.M.; Munoz-Olmo, J.; Serra-Mestre, J.M. Breast reconstruction with fat grafting alone. Ann. Plast. Surg. 2011, 66, 598–601. [Google Scholar] [CrossRef]
- Stillaert, F.B.J.L.; Sommeling, C.; D’Arpa, S.; Creytens, D.; van Landuyt, K.; Depypere, H.; van den Broecke, R.; Monstrey, S.; Blondeel, P.N.; Morrison, W.A. Intratissular expansion-mediated, serial fat grafting: A step-by-step working algorithm to achieve 3D biological harmony in autologous breast reconstruction. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2016, 69, 1579–1587. [Google Scholar] [CrossRef]
- Zhang, X.; Cai, L.; Yin, B.; Han, X.; Li, F. Total breast reconstruction using large volume condensed and viable fat grafting after mastectomy. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 966–973. [Google Scholar] [CrossRef]
- HAS. Evaluation de la Sécurité et des Conditions de Réalisation de L’autogreffe de Tissu Adipeux Dans la Chirurgie Reconstructrice, Réparatrice et Esthétique du Sein; Haute Autorité de Santé: Saint-Denis, France, 2015. [Google Scholar]
- De Decker, M.; De Schrijver, L.; Thiessen, F.; Tondu, T.; Van Goethem, M.; Tjalma, W. Breast cancer and fat grafting: Efficacy, safety and complications-a systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 207, 100–108. [Google Scholar] [CrossRef]
- Delay, E.; Meruta, A.C.; Guerid, S. Indications and Controversies in Total Breast Reconstruction with Lipomodeling. Clin. Plast. Surg. 2018, 45, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Costantini, M.; Cipriani, A.; Belli, P.; Bufi, E.; Fubelli, R.; Visconti, G.; Salgarello, M.; Bonomo, L. Radiological findings in mammary autologous fat injections: A multi-technique evaluation. Clin. Radiol. 2013, 68, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ueberreiter, C.S.; Ueberreiter, K.; Mohrmann, C.; Herm, J.; Herold, C. Langzeitevaluation nach autologer Fetttransplantation zur Brustvergrößerung (Long-term evaluation after autologous fat transplantation for breast augmentation). Handchir. Mikrochir. Plast. Chir. 2021, 53, 149–158. (In German) [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Abu-Ghname, A.; Davis, M.J.; Winocour, S.J.; Hanson, S.E.; Chu, C.K. Fat Grafting in Breast Reconstruction. Semin. Plast. Surg. 2020, 34, 17–23. [Google Scholar] [CrossRef]
- Li, M.; Tang, S. Analysis of risk factors related to periprosthetic infection after breast augmentation. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi Zhongguo Xiufu Chongjian Waike Zazhi Chin. J. Reparative Reconstr. Surg. 2019, 33, 889–893. [Google Scholar] [CrossRef]
- Long, A.C.; Sue, G.R.; Chattopadhyay, B.A.; Veld, B.E.H.I.; Lee, G.K. Critical Evaluation of Risk Factors of Infection Following 2-Stage Implant-Based Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1386. [Google Scholar] [CrossRef]
- Hartrampf, C.R.; Scheflan, M.; Black, P.W. Breast reconstruction with a transverse abdominal island flap. Plast. Reconstr. Surg. 1982, 69, 216–225. [Google Scholar] [CrossRef]
- Koshima, I.; Soeda, S. Inferior epigastric artery skin flaps without rectus abdominis muscle. Br. J. Plast. Surg. 1989, 42, 645–648. [Google Scholar] [CrossRef]
- Watterson, P.A.; Bostwick, J.; Hester, T.R.; Bried, J.T.; Taylor, G.I. TRAM flap anatomy correlated with a 10-year clinical experience with 556 patients. Plast. Reconstr. Surg. 1995, 95, 1185–1194. [Google Scholar] [CrossRef]
- Cason, R.W.; Shammas, R.L.; Broadwater, G.; Glener, A.D.; Sergesketter, A.R.; Vernon, R.; Le, E.; Wickenheisser, V.A.; Marks, C.; Orr, J.; et al. The Influence of Fat Grafting on Breast Imaging after Postmastectomy Reconstruction: A Matched Cohort Analysis. Plast. Reconstr. Surg. 2020, 146, 1227–1236. [Google Scholar] [CrossRef]
- Groen, J.; Negenborn, V.; Twisk, D.; Rizopoulos, D.; Ket, J.C.; Smit, J.; Mullender, M. Autologous fat grafting in onco-plastic breast reconstruction: A systematic review on oncological and radiological safety, complications, volume retention and patient/surgeon satisfaction. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2016, 69, 742–764. [Google Scholar] [CrossRef] [PubMed]
- Santosa, K.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Long-term Patient-Reported Outcomes in Postmastectomy Breast Reconstruction. JAMA Surg. 2018, 153, 891–899. [Google Scholar] [CrossRef]
- Largo, R.D.; Tchang, L.A.; Mele, V.; Scherberich, A.; Harder, Y.; Wettstein, R.; Schaefer, D.J. Efficacy, safety and complications of autologous fat grafting to healthy breast tissue: A systematic review. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2014, 67, 437–448. [Google Scholar] [CrossRef] [PubMed]
- El-Sabawi, B.; Sosin, M.; Carey, J.N.; Nahabedian, M.Y.; Patel, K.M. Breast reconstruction and adjuvant therapy: A systematic review of surgical outcomes. J. Surg. Oncol. 2015, 112, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Kronowitz, S.J.; Mandujano, C.; Liu, J.; Kuerer, H.M.; Smith, B.; Garvey, P.; Jagsi, R.; Hsu, L.; Hanson, S.; Valero, V. Lipofilling of the Breast Does Not Increase the Risk of Recurrence of Breast Cancer: A Matched Controlled Study. Plast. Reconstr. Surg. 2016, 137, 385–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva-Vergara, C.; Fontdevila, J.; Descarrega, J.; Burdio, F.; Yoon, T.-S.; Grande, L. Oncological outcomes of lipofilling breast reconstruction: 195 consecutive cases and literature review. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2016, 69, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Wazir, U.; Chehade, H.E.H.; Headon, H.; Oteifa, M.; Kasem, A.; Mokbel, K. Oncological Safety of Lipofilling in Patients with Breast Cancer: A Meta-analysis and Update on Clinical Practice. Anticancer Res. 2016, 36, 4521–4528. [Google Scholar] [CrossRef] [Green Version]
- Krastev, T.K.; Schop, S.; Hommes, J.; Piatkowski, A.A.; Heuts, E.M.; van der Hulst, R.R.W.J. Meta-analysis of the oncological safety of autologous fat transfer after breast cancer. Br. J. Surg. 2018, 105, 1082–1097. [Google Scholar] [CrossRef]
- Sorrentino, L.; Regolo, L.; Scoccia, E.; Petrolo, G.; Bossi, D.; Albasini, S.P.; Caruso, A.; Vanna, R.; Morasso, C.; Mazzucchelli, S.; et al. Autologous fat transfer after breast cancer surgery: An exact-matching study on the long-term oncological safety. Eur. J. Surg. Oncol. J. Cancer Surg. 2019, 45, 1827–1834. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Age (years) | 48.3 (10.2) |
| BMI (kg/m²) | 23.9 (5.2) |
| Active smoking | 10 (27%) |
| Type 2 diabetes | 2 (5.4%) |
| Depression | 2 (5.4%) |
| High blood pressure | 4 (10.1%) |
| Chest size (cm) | 75.2 (7.4) |
| Bra cup size | |
| A | 7 (18.9%) |
| B | 22 (59.4%) |
| C | 6 (16.2%) |
| D | 1 (2.7%) |
| F | 1 (2.7%) |
| N (%) | |
|---|---|
| Histological types | |
| Ductal carcinoma invasive (DCI) | 23 (62.1%) |
| Ductal carcinoma in situ (DCIS) | 6 (16.2%) |
| Lobular carcinoma invasive (LCI) | 5 (13.5%) |
| Combined breast cancer * | 2 (5.4%) |
| Other | 1 (2.7%) |
| Hormonal receptors | 25 (67.5%) |
| HER 2+ | 23 (62%) |
| Tumor size according to TNM classification | |
| Tis | 4 (10.8%) |
| T1 | 17 (45.9%) |
| T2 | 11 (29.7%) |
| T3 | 3 (8.1%) |
| T4 | 2 (5.4%) |
| Axillary lymph node disease | 16 (43.2%) |
| Visceral metastases | 3 (8.1%) |
| Chemotherapy | 21 (56.7%) |
| Radiotherapy | 19 (51.3%) |
| Hormotherapy | 21 (56.7%) |
| Axillary node management | |
| No | 1 (2.7%) |
| Sentinel node | 15 (40.5%) |
| Axillary Lymph node Dissection | 21 (56.7%) |
| N (37) | |
|---|---|
| Time of breast reconstruction | |
| Immediate | 4 (10.8%) |
| Delayed | 33 (89.2%) |
| Symmetrisation procedure | 17 (45.9%) |
| Fat volume collected per patient | |
| Total (mL) | 1144.6 (726.8) |
| Per session (mL) | 520.2 (81.7) |
| Fat volume transferred per patient | |
| Total (mL) | 566.4 (441.6) |
| Per procedure (mL) | 257.4 (46.7) |
| Number of procedures | 2.2 (1.1) |
| 1 | 11 (29.7%) |
| 2 | 10 (27.0%) |
| 3 | 12 (32.4%) |
| 4 | 3 (8.1%) |
| 6 | 1 (2.7%) |
| Staggered reconstruction (months) | 6.8 (6.9) |
| Interval between surgery/radiotherapy–lipofilling (months) * | 14.8 (8.9) |
| Nipple reconstruction ** | 12 (32.4%) |
| Number of complications | 7 (18.9%) |
| Author | Year | Design | Number of Patients | Number of Sessions | Total volume Injected (mL) | Volume Per Session (mL) | Expansion System | Complications | Health Quality of Life |
|---|---|---|---|---|---|---|---|---|---|
| Babin [4] | 2017 | Case report | 1 | 3 | 500 | 166 | None | Infection | “Satisfied” |
| Babovic [23] | 2010 | Case report | 1 | 6 | 1615 | 403.9 | None | 0 | “Satisfied” |
| Bayti [24] | 2015 | Retrospective | 22 | 4.9 | 1421 | NR | BRAVA | 18.2% cytosteatonecrosis | Breast Q: 98% “very satisfied” |
| 4.5% hematoma | |||||||||
| 13.6% donor site irregularity | |||||||||
| Cheng [25] | 2013 | Case report | 1 | 2 | 430 | 215 | BRAVA | 0 | - |
| Costantini [26] | 2013 | Prospective | 2 | 2 | 302 | 100.48 | None | - | - |
| Delaporte [27] | 2009 | Retrospective | 15 | 3 | 600 | - | None | 20% cytosteatonecrosis | 66.7% “very good” |
| Fabiocchi [28] | 2017 | Retrospective | 57 | 3.6 | 640 | 318 | Expander | 0.75% hemorrhage donor site | 64.8% “excellent” |
| 0.75% surgical site infection | |||||||||
| Fitoussi [29] | 2009 | Case report | 1 | 2 | 380 | - | None | - | - |
| Hammer-Hansen [30] | 2015 | Case report | 1 | 7 | 957 | 136.71 | BRAVA | Rash | - |
| Ho Quoc [31] | 2016 | Retrospective | 6 | 790 | - | BRAVA | - | 82% “satisfied” | |
| Ho Quoc [32] | 2019 | Retrospective | 2 | 4 | 474 | 118 | None | - | - |
| Hoppe [33] | 2013 | Retrospective | 28 | 5 | 1020 | 159 | None | 2.59% cytosteatonecrosis | 96% “high |
| 0.74% infection | satifaction” | ||||||||
| 0.74% granuloma | |||||||||
| Jarrah [34] | 2013 | Case report | 1 | 3 | 720 | 240 | None | - | - |
| Kellou [35] | 2019 | Retrospective | 22 | 5.86 | 1490.6 | - | None | 50% hematoma donor site | |
| 22.7% lipolysis, | - | ||||||||
| 44.4% puncture site burn, | |||||||||
| 11% lymphocele (donor site) | |||||||||
| 11% hip phlyctene | |||||||||
| Longo [36] | 2014 | Prospective | 21 | 4 | 439 | 137 | None | - | - |
| Manconi [37] | 2017 | Retrospective | 12 | 3 | 417 | 214 | Expander | 3.2 | - |
| Mestak [38] | 2013 | Case report | 1 | 3 | 815 | 271 | BRAVA | 0 | - |
| Niddam [39] | 2017 | Retrospective | 25 | - | - | - | None | - | Satisfaction rate: 5.8/10 |
| Pannettiere [25] | 2011 | Case report | 1 | 9 | 700 | 78 | None | 0 | - |
| Serra-Renom [40] | 2011 | Case series | 8 | 3 | 400 | 133 | None | 0 | - |
| Stillaert [41] | 2016 | Case series | 8 | 4 | 644 | 160 | Expander | 1 cyst | - |
| Zhang [42] | 2020 | Retrospective | 30 | 3,3 | - | 230.5 | +/− BRAVA | 3% cellulitis 27% cysts 3% palpable nodules | 90% “very satisfied” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piffer, A.; Aubry, G.; Cannistra, C.; Popescu, N.; Nikpayam, M.; Koskas, M.; Uzan, C.; Bichet, J.-C.; Canlorbe, G. Breast Reconstruction by Exclusive Lipofilling after Total Mastectomy for Breast Cancer: Description of the Technique and Evaluation of Quality of Life. J. Pers. Med. 2022, 12, 153. https://doi.org/10.3390/jpm12020153
Piffer A, Aubry G, Cannistra C, Popescu N, Nikpayam M, Koskas M, Uzan C, Bichet J-C, Canlorbe G. Breast Reconstruction by Exclusive Lipofilling after Total Mastectomy for Breast Cancer: Description of the Technique and Evaluation of Quality of Life. Journal of Personalized Medicine. 2022; 12(2):153. https://doi.org/10.3390/jpm12020153
Chicago/Turabian StylePiffer, Alexandre, Gabrielle Aubry, Claudio Cannistra, Nathalie Popescu, Maryam Nikpayam, Martin Koskas, Catherine Uzan, Jean-Christophe Bichet, and Geoffroy Canlorbe. 2022. "Breast Reconstruction by Exclusive Lipofilling after Total Mastectomy for Breast Cancer: Description of the Technique and Evaluation of Quality of Life" Journal of Personalized Medicine 12, no. 2: 153. https://doi.org/10.3390/jpm12020153
APA StylePiffer, A., Aubry, G., Cannistra, C., Popescu, N., Nikpayam, M., Koskas, M., Uzan, C., Bichet, J. -C., & Canlorbe, G. (2022). Breast Reconstruction by Exclusive Lipofilling after Total Mastectomy for Breast Cancer: Description of the Technique and Evaluation of Quality of Life. Journal of Personalized Medicine, 12(2), 153. https://doi.org/10.3390/jpm12020153